ectopic pregnancy
TRANSCRIPT

Ectopic Pregnancy
Lt.Dhirendra Kumar Tiwari

Case
• 26 years old lady, presented on 7th may 2014 at 1230 hrs with C/O of
– Amenorrhoea 4 weeks 6 days
– Irregular bleeding P/V 3-4 days
– Severe lower abdominal pain since morning
– Loss of consciousness(syncope) 01 episode since morning

HOPI
• G2P1 lady
• LMP 04 April 2014
• Underwent LSCS 2 years back, live baby delivered(indication-unfavorable cervix)
• No H/O of Tuberculosis in past
• No H/O DM or HTN
On Examination• Temp-98.6
.F
• Pulse-68/min• RR-20/min• BP-80/40mmHg rt.arm supine• SpO2 95%• Pallor +++• P/A
– Distension +– Tenderness over suprapubic region ++
• Other systems-NAD

P/S,P/V examination
• Bilateral adnexal tenderness
• Uterus bulky, cervical rocking ++
• Bleeding ++
• UPT +
• USG findings– No intra-uterine gestational sac
– Free fluid in abdomen present
Δ RUPTURE ECTOPIC PREGNANCY

Management
• Plan-Emergency Laparotomy
• (kept NPO, antibiotic prophylaxis, IV line,Shift to OT by 1400 hrs)
• Anaesthesia-Spinal anaesthesia
• Exploratory Laparotomy
• Pre OP findings– Hemoperitonium ++(300ml +200ml clot)
– Tubal pregnancy in ampulla region(Rt)
– Tube(Lt) +Ovaries healthy

• Surgery-Salpingectomy(Rt)
• Haemostasis ensured
• Intraperitonial drain placed
• 2U of blood transfused
• Post OP
– NPO
– IV fluids
– Antimicrobials,analgesics
– I/O chart
– TPR/BP monitoring
– Post OP period uneventful

Discussion

DIFFERENTIAL DIAGNOSIS
D/D of Acute Ectopic
1. Rupture corpus luteum of pregnancy
2. Rupture of chocolate cyst
3. Twisted ovarian cyst
4. Torsion / degeneration of pedunculated fibroid
5. Incomplete abortion
6. Acute Appendicitis
7. Perforated peptic ulcer
8. Renal colic
9. Splenic rupture

D/D OF CHRONIC (SUB ACUTE) ECTOPIC
1. Pelvic abscess
2. Pyosalpinx
3. Subserous uterine fibroid
4. Salpingintis
5. Retroverted gravid uterus
6. Appendicular lump

Introduction
• When Fertilized Ovum is implanted and develops outside the normal Endometrial Cavity
• Contributes significantly to maternal morbidity and mortality
• Prompt recognition and early aggressive intervention is of paramount importance

Is one in which fertilized ovum is implanted & develops outside normal uterine cavity

• IMPLANTATION SITES– EXTRA-UTERINE
• TUBAL(97%)
– AMPULLA(55%)
– ISTHMUS(25%)
– INFUNDIBULUM(2%)
– INTERSTITIAL(2%)
• OVARIAN(0.5%)
• ABDOMINAL(1%)
– PRIMARY(RARE)
– SECONDARY
» INTRAPERITONIAL(COMMON)
» EXTRAPERITONEAL(BROAD LIGAMENT)– UTERINE(1.5%)
• CERVICAL(<1%)
• ANGULAR
• CAESAREAN SCAR(<1%)

ETIOLOGY
CONGENITAL
– Tubal Hypoplasia
– Tortuosity
– Congenital diverticuli
– Accessory ostia
– Partial stenosis
– Elongation
– Intamural polyp

ACQUIREDPelvic Inflammatory disease (6-10 times)
Chlamydia is most common
Contraceptive FaliureCu T - 4%Progestasart -17%Minipills -4-10%Norplant -30%

Tubal sterilization faliure - 40%Depends on sterilization technique and age of the patient
Bipolar Cauterisation -65%
Unipolar Cautery -17%
Reversal of sterilisation- Depends on method of sterilization, Site of
tubal occlusion, residual tubal length.
- Reanastomosis of cauterised tube -15%
- Reversal of Pomeroy’s - < 3%

Tubal reconstructive surgery (4-5 times)
Assisted Reproductive technique(ART)- Ovulation induction, IVF-ET and GIFT (4-7%)
- Risk of heterotopic pregnancy(1%)
Previous Ectopic Pregnancy
- 7-15% chances of repeat ectopic pregnancy

Other Risk factors
Age 35-45 yrs
Previous induced abortion
Previous pelvic surgeries
Cigarette smoking
Infertility
Salpingitis Isthmica Nodosa
Genital Tuberculosis
Fundal Fibroid & Adenomyosis of tube
Transperitoneal migration of ovum

Fate of Pregnancy• Pregnancy is unable to survive due to poor blood
supply, thus resulting in
– a tubal abortion and resorption
– Expulsion from the fimbriated end into the abdominal cavity.
• Continues to grow until the over distended tube ruptures, resulting profuse intraperitoneal bleeding.
• Isthmic – 6-8 wks,
• Ampulla – 8-12wks,
• Interstitial -4 months
• Abortion is common in ampullarypregnancies,whereas rupture is in isthmic.

• Rarely, tubal pregnancy will be expelled from the
tube and seed onto sites in the abdominal cavity (e.g.
omentum, small or large bowel, or parietal
peritoneum), and gives rise to a viable abdominal
pregnancy.

CLINICAL APPROACH
• Diagnosis can be done by history, detail examination and judicious use of investigation.
• H/o past PID, tubal surgery, current contraceptive measures
• Wide spectrum of clinical presentation from asymptomatic pt. to others with acute abdomen and in shock.

ACUTE ECTOPIC PREGNANCY
• Classical triad is present in 50% of pt. with rupture ectopic.
- PAIN:- most constant feature in 95% pt- variable in severity and nature
- AMENORRHOEA:- 60-80% of pt- there may be delayed period or slight spotting at the time of expected menses.
- VAGINAL BLEEDING: - scanty dark brown
• Feeling of nausea, vomiting, fainting attack, syncope attack(10%) due to reflex vasomotor disturbance.

• O/E:- patient is restless in agony, looks blanched, pale, sweating with cold clammy skin.Features of shock, tachycardia, hypotension.
• P/A:- abdomen tense, tender mostly in lower abdomen, shifting dullness, rigidity may be present.
• P/S:- minimal bleeding may be present
• P/V:- uterus may be bulky, deviated to opposite side, fornix is tender, excitation pain on movement of cervix.POD may be full, uterus floats as if in water.

CHRONIC ECTOPIC PREGNANCY
• It can be diagnosed by high clinical suspicion.
• Previous attack of acute pain from which she has recovered.
• She may have– amenorrhoea
– vaginal bleeding with dull pain in abdomen
– bladder and bowel complaints like dysuria,frequency or retention of urine, rectal tenesmus.

• O/E:- patient look ill, varying degree of pallor,
slightly raised temperature. Features of shock
are absent.
• P/A:- Tenderness and muscle guard on the lower
abdomen.
A mass may be felt, irregular and tender.
• P/V:- Vaginal mucosa pale, uterus may be normal
in size or bulky, ill defined boggy tender
mass may be felt in one of the fornix.

UNRUPTURED ECTOPIC
• Diagnosed accidentally in Laparoscopy or Laparotomy
C/F – delayed period, spotting with discomfort in lower abdomen.
P/A – tenderness in lower abdomen
P/V – should be done gentlyuterus is normal size, firmsmall tender mass may be felt in the fornix

DIAGNOSIS
• Patient with acute ectopic can be diagnosed clinically.
• Blood should be drawn for Hb gm%, blood grouping and cross matching, DC and TWBC, BT, CT.
• Should be catheterized to know urine output.
Bed side test:-
1. Urine pregnancy test:- positive in 95% cases.ELISA is sensitive to 10-50 mlU/ml of β hCG and can be detected on 24th day after LMP.

2. Culdocentesis:- (70-90%)(OLD TECHNIQUE)
- Can be done with 16-18 G lumbar puncture needle through posterior fornix into POD.
- Positive tap is 0.5ml of non clotting blood.
• Other Investigations:-
1. Ultra Sonography
a) Transvaginal Sonography (TVS):- Is more sensitive- It detect intrauterine gestational sac at 4-5wks and at S-β hCG level as low as 1500 IU/L .

b) Color Doppler Sonography(TV-CDS):
- Improve the accuracy.
-Identify the placental shape (ring-
of-fire pattern) and blood flow
outside the uterine cavity.
c) Transabdominal Sonography:
- can identify gestational sac at 5-6 wks
- S-β hCG level at which intrauterine gestational
sac is seen by TAS is 1800 IU/L.

2. β-HCG Assay
a) Single β-HCG: little value
b) Serial β-HCG: is required when result of initial USG is confusing.
- When hCG level < 2000 IU/L doubling time help to predict viable Vs nonviable pregnancy(hCG level doubles by 48 hrs in normal pregnancy)
-Rise of β-HCG <66% in 48 hrs indicate ectopic pregnancy or nonviable intrauterine pregnancy .
-Biochemical pregnancy is applied to those women who have two β-HCG values >10 IU/L

3. Serum Progesterone
- level >25 ngm/ml is suggestive of normal
intrauterine pregnancy.
- level <15 ngm/ml is suggestive of ectopic
pregnancy.
- level <5 ngm/ml indicates nonviable
pregnancy, irrespective of its location.
4. Diagnostic Laparoscopy (Gold standard)
- Can be done only when patient is
haemodynamically stable.
-It confirms the diagnosis and removal of
ectopic mass can be done at the same time.

5. Dilatation & Curettage - Is recommended in suspected case of
incomplete abortion vs ectopic pregnancy.- Identification of decidua without chorionic
villi is suggestive of extra uterine pregnancy.
6. Other hormonal Tests - Placenta protein (PP14) decrease in EP
- PAPPA (Pregnancy Associated Plasma Protein A),PAPPC (schwangerchaft protein 1) has low value in EP
- CA-125, Maternal serum creatine kinase, Maternal serum AFP elevated in ectopic pregnancy.

SUSPECTED ECTOPIC PREGNANCYUrine Pregnancy test positive
Transvaginal USG
IU sac No IU sacQuantitative S-hCG+ S progesterone
< 66% rise in 48 hr orS progesterone < 5-10 ng/ml
D & C
Villi present Villi absent
Incomplete abortion
Laparoscopy
>66% rise in 48 hr orS progesterone > 5-10 ng/ml
Repeat S-hCG in 48 hrstill USG discrimination zone
No sac IU sac
Continue to monitor

MANAGEMENT
Expectant management
Medicalmanagement
Surgicalmanagement
Local Systemic(USG or Laparoscopic)
salpingocentesis
- Methotrexate- Potassium chloride- Prostagladin(PGF2α)- Hypersmolar glucose- Actinomycin D- Mifepristone
Methotrexate
Radical
Salpingectomy
Conservative
-Salpingostomy
-Salpingotomy
- Segmental resection
-Milking or fimbrialexpression

MANAGEMENT OF RUPTURED ECTOPIC
PRINCIPLE: Resuscitation and Laparotomy
ANTI SHOCK TREATEMENT:
- IV line made patent, crystalloid is started
- Blood sample for Hb, blood grouping & cross matching, PT,PTTK,INR
- Catheterization done
- Colloids for volume replacement
LAPAROTOMY:
Principle is ‘Quick in and Quick out’
- Rapid exploration of abdominal cavity is done
- Salpingectomy is the definitive surgery (sent for HPE)
- Blood transfusion to be given

MANAGEMENT OF UNRUPTURED ECTOPIC PREGNANCY
OPTIONS: -
• SURGICAL
• SURGICALLY ADMINISTERED MEDICAL (SAM)
TREATMENT
• MEDICAL TREATMENT
• EXPECTANT MANAGEMENT

EXPECTANT MANAGEMENTIDENTIFICATION CRITERIA (Ylostalo et al , 1993)- :
1. Tubal ectopic pregnancies only
2. Haemodynamically stable
3. Haemoperitoneum < 50ml
4. Adnexal mass of < 3.5 cm without heart beat.
5. Initial β HCG <1000 IU/L and falling in titre
SUCCESS RATE - Upto 60%
PROTOCOL:- Hospitalization with strict monitoring of clinical symptom
- Daily Hb estimation
- Serum β HCG monitoring 3-4 days until it is <10 IU/L
- TVS to be done twice a week.

MEDICAL MANAGEMENT
Surgery-mainstay of management worldwideMedical management-tried in selected cases
CANDIDATES FOR METHOTREXATE (MTX) Unruptured sac < 3.5cm without cardiac activity S-hCG < 10,000 IU/L Persistant Ectopic after conservative surgery
PHYSICIAN CHECK LIST CBC, LFT, RFT, S-hCG Transvaginal USG within 48 hrs Obtain informed consent Anti-D Ig if pt is Rh negative Follow up on day1, 4 and 7.

MEDICAL MANAGEMENT
METHOTREXATE:
• Oral/intramuscular /intravenous usually along with folinic acid.
• Mostly used for early resolution of placental tissue in abdominal pregnancy. Can also be used for tubal pregnancy.
• Mechanism of action
– Methotrexate-folic acid antagonist that inactivates the enzyme dihydrofolate reductase
– Interferes with the DNA synthesis by inhibiting the synthesis of pyrimidines leading to trophoblastic cell death
– Auto enzymes and maternal tissues then absorb the trophoblast.

• Advantages –
– Minimal Hospitalisation.Usually outdoor treatment
– Quick recovery
– 90% success if cases are properly selected
• Disadvantages-
– Side effects like GI & Skin
– Monitoring is essential- Total blood count, LFT & serum HCG once weekly till it becomes negative

SURGICALLY ADMINISTERED MEDICAL(SAM) TREATMENT
• Aim- Trophoblastic destruction without systemic side effects
• Technique- Injection of trophotoxic substance into the ectopic pregnancy sac or into the affected tube by-
– Laparoscopy or
– Ultrasonographically guided
• Transabdominal (Porreco, 1992)
• Transvaginal (Feichtingar, 1987)
– With Falloposcopic control (Kiss, 1993)

Trophotoxic substances used-Methtrexate (Pansky, 1989)Potassium Chloride (Robertson, 1987) Mifiprostone (RU 486)PGF2 (Limblom, 1987)Hyper osmolar glucose solutionActinomycin D
Advantage of local MTX :- Increase tissue concentration at local site- Decrease systemic side effects- Decrease hospitalization- Greater preservation of fertility
Follow up: - Serum β HCG twice weekly till < 10 IU/L- TVS weekly for 4-6 weeks- HCG after 6 months for tubal patency
SURGICALLY ADMINISTERED MEDICAL Tt (SAM)

SURGICAL MANAGEMENT OF ECTOPIC
Conservative Surgery
Can be done Laparoscopically or by microsurgical laparotomy
INDICATION:- Patient desires future fertility
- Contralateral tube is damaged or surgically removed previously
CHOICE OF TECHNIQUE: depends on
- Location and size of gestational sac
- Condition of tubes
- Accessibility

VARIOUS CONSERVATIVE SURGERIES
1.Linear Salpingostomy:
- Indicated in unruptured ectopic <2cm in ampullary region.
- Linear incision given on antimesentric border over the site
and product removed by fingers, scalpel handle or gentle
suction and irrigation.
- Incision line kept open (heals by secondary intention)
2. Linear Salpingotomy :
- Incision line is closed in two layers with 7-0 interrupted
vicryl sutures.
3. Segmental Resection & Anastomosis:
- Indicated in unruptured isthmic pregnancy
- End to end anastomosis is done immediately or at later
date

4. Milking or fimbrial Expression:
- This is ideal in distal ampullary or infundibular pregnancy.
- It has got increased risk of persistent ectopic pregnancy.
ADVANTAGES OF LAPAROSCOPY
- It helps in diagnosis, evaluation, and treatment .
- Diagnose other causes of infertility.
- Decreased hospitalization, operative time, recovery period,
analgesic requirement.
Follow up after conservative surgery
- With weekly Serum β HCG titre till it is negative.
- If titre increases methotrexate can be given.

SALPINGECTOMY VS
SALPINGOSTOMY / SALPINGOTOMY
All tubal pregnancies can be treated by partial or total Salpingectomy
Salpingostomy / Salpingotomy is only indicated when:
1. The patient desires to conserve her fertility2. Patient is haemodinamically stable3. Tubal pregnancy is accessible4. Unruptured and < 5Cm. In size5. Contralateral tube is absent or damaged

Laparotomy Vs Laparoscopy
- Laparoscopy is reserved for pt.who are
hemodynamically stable.
- Ruptured Ectopic does not necessarily require
Laparotomy, but if large clots are present
Laparotomy should be considered.
Reproductive outcome
Is similar in pt. treated with either Laparoscopy or Laparotomy.

Discussion



OVARIAN ECTOPIC PREGNANCYIncidence: 1:40,000
Risk factor: - IUCD
- Endometriosis on surface of ovary
Course:
C/F are same as tubal pregnancy
ruptures within 2-3 wks
Diagnosis: On Laparotomy
Spiegelberg’s Criteria
1. Ipsilateral tube is intact and separate from sac
2. Sac occupies the position of the ovary
3. Connected to uterus by ovarian ligament
4. Ovarian tissue found on its wall on HP study
M/MRuptured
Laparotomy
Oophorectomy
Unruptured
Ovarian wedge resection
Ovarian Cystectomy
ABDOMINAL PREGNANCY
Incidence: Rarest
MMR : 7-8 times > tubal ectopic
90 times > Intrauterine pregnancy
H/O : - Irregular bleeding, spotting
- Nausea, vomiting, flatulence, constipation,
diarrhoea, abdominal pain.
- Fetal movement may be painful and high in
the abdomen
O/E : - Abnormal fetal position, easy in palpating
fetal parts.
- uterus palpated separate from sac
- no uterine contraction after oxytocin
infusion

FATE OF SECONDARY ABDOMINAL PREGNANCY :
1. Death of ovum – complete absorption
2. Placental separation – massive intraperitoneal
haemorrhage
3. Infection – fistulous communication with intestine,
bladder, vagina, or umbilicus
4. Fetus dies (majority) – mummification, adipocere
formation, or calcified to lithopaedion
5. Rarely – continue to term (malformation)
M/M:
- Urgent Laparatomy irrespective of period of gestation
- Ideal to remove entire sac fetus, placenta, membrane
- Placenta may be left if attached to vital organs, get
absorbed by aseptic autolysis

CERVICAL PREGNANCY
Implantation occurs in cervical canal at or below internal Os.
Incidence: 1 in 18,000
RISK FACTORS :
- Previous induced abortion
- Previous caesarean delivery
- Asherman’s syndrome
- IVF
- DES exposure
- Leiomyoma

MANAGEMENT
SurgicalMainstay therapy in past
Radical surgery
Hysterectomy
Conservative
D & C(risk of torrential bleeding)
- Cerclage Bernstein ≈ Mc Donald’sWharton ≈ Shirodkar’s
-Transvaginal ligation of Cx branch ofuterine artery
- Angiographic uterine A embolisation
- Intracervical vasopressin inj- Foley’s catheter as tamponade
MedicalRecently proposed
Single or CombinationOR
Adjunct to surgery
- Methotrexate
- Actinomycin
- KCl
- Etoposide
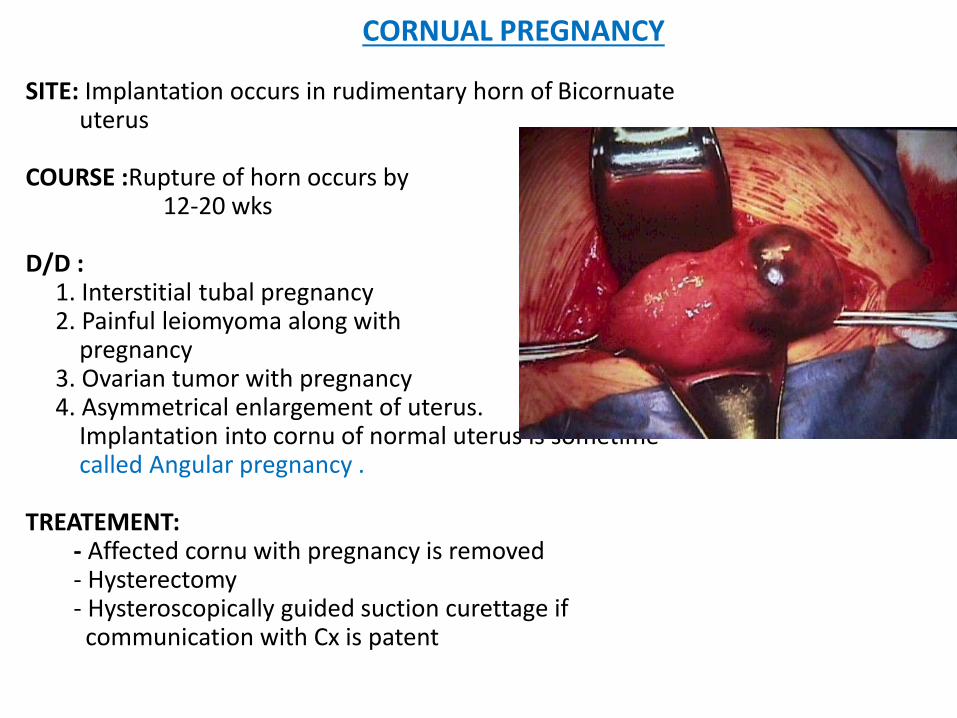
CORNUAL PREGNANCY
SITE: Implantation occurs in rudimentary horn of Bicornuateuterus
COURSE :Rupture of horn occurs by12-20 wks
D/D : 1. Interstitial tubal pregnancy2. Painful leiomyoma along with
pregnancy3. Ovarian tumor with pregnancy4. Asymmetrical enlargement of uterus.
Implantation into cornu of normal uterus is sometime called Angular pregnancy .
TREATEMENT:- Affected cornu with pregnancy is removed- Hysterectomy- Hysteroscopically guided suction curettage if communication with Cx is patent

INTERSTITAL PREGNANCY (2%)
It ruptures late at 3-4 months gestation.
Fatal rupture – severe bleeding as both uterine &
ovarian artery supply.
Early & Unruptured – Local or IM MTX with followup
Cornual resection by Laparotomy may be done.
There is high risk of uterine rupture in
subsequent pregnancy.
Rupture – Hysterectomy is indicated

CAESAREAN SCAR ECTOPIC PREGNANCY
Recently reported
USG slows on empty uterine cavity and gestational sac attached low to the lower segment caesarean scar.
C/F : similar to threatened or inevitable abortion
Diagnosis : Doppler imaging confirms
T/t : Methotrexate injection
Hysterectomy in a multiparous women.
In young pt resection & suturing of scar may be
done (high risk of rupture).

Discussion