ec.europa.euec.europa.eu/health/documents/community-register/2013/... · at-1020 wien . austria...
TRANSCRIPT

ANNEX I
LIST OF THE NAMES, PHARMACEUTICAL FORMS, STRENGTHS OF THE MEDICINAL PRODUCTS, ROUTE OF ADMINISTRATION, MARKETING AUTHORISATION HOLDERS
IN THE MEMBER STATES
1

Member State EU/EEA
Marketing authorisation holder
Invented Name Strength Pharmaceutical form
Route of administration
Content (concentration)
Austria Novartis Pharma GmbH Stella-Klein-Löw-Weg 17 AT-1020 Wien Austria
Sandimmun - Neoral 10 mg Kapseln
10 mg Capsule, soft Oral use
Austria Novartis Pharma GmbH Stella-Klein-Löw-Weg 17 AT-1020 Wien Austria
Sandimmun - Neoral 25 mg Kapseln
25 mg Capsule, soft Oral use
Austria Novartis Pharma GmbH Stella-Klein-Löw-Weg 17 AT-1020 Wien Austria
Sandimmun - Neoral 50 mg Kapseln
50 mg Capsule, soft Oral use
Austria Novartis Pharma GmbH Stella-Klein-Löw-Weg 17 AT-1020 Wien Austria
Sandimmun - Neoral 100 mg Kapseln
100 mg Capsule, soft Oral use
Austria Novartis Pharma GmbH Stella-Klein-Löw-Weg 17 AT-1020 Wien Austria
Sandimmun - Neoral 100 mg/ml - Trinklösung
100 mg/ml Oral solution Oral use 100 mg/ml
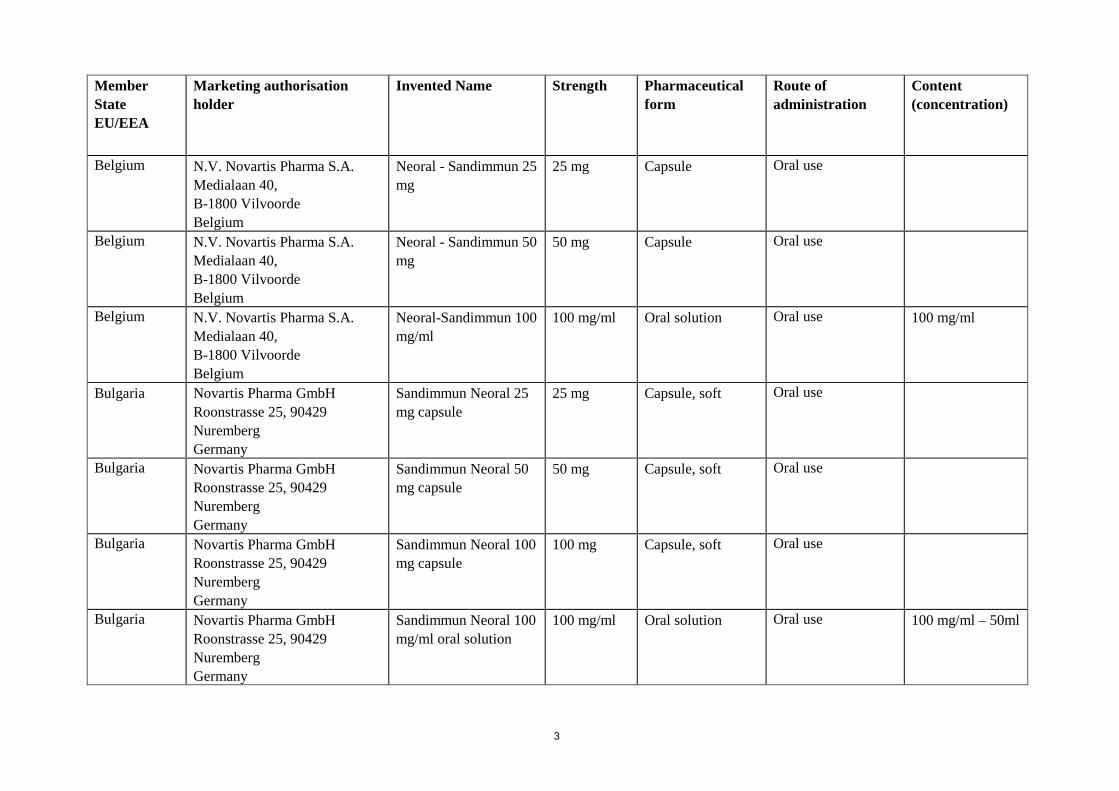
Belgium N.V. Novartis Pharma S.A. Medialaan 40, B-1800 Vilvoorde Belgium
Neoral - Sandimmun 10 mg
10 mg Capsule Oral use
Belgium N.V. Novartis Pharma S.A. Medialaan 40, B-1800 Vilvoorde Belgium
Neoral-Sandimmun 100 mg
100 mg Capsule Oral use
2
Member State EU/EEA
Marketing authorisation holder
Invented Name Strength Pharmaceutical form
Route of administration
Content (concentration)
Belgium N.V. Novartis Pharma S.A. Medialaan 40, B-1800 Vilvoorde Belgium
Neoral - Sandimmun 25 mg
25 mg Capsule Oral use
Belgium N.V. Novartis Pharma S.A. Medialaan 40, B-1800 Vilvoorde Belgium
Neoral - Sandimmun 50 mg
50 mg Capsule Oral use
Belgium N.V. Novartis Pharma S.A. Medialaan 40, B-1800 Vilvoorde Belgium
Neoral-Sandimmun 100 mg/ml
100 mg/ml Oral solution Oral use 100 mg/ml
Bulgaria Novartis Pharma GmbH Roonstrasse 25, 90429 Nuremberg Germany
Sandimmun Neoral 25 mg capsule
25 mg Capsule, soft Oral use
Bulgaria Novartis Pharma GmbH Roonstrasse 25, 90429 Nuremberg Germany
Sandimmun Neoral 50 mg capsule
50 mg Capsule, soft Oral use
Bulgaria Novartis Pharma GmbH Roonstrasse 25, 90429 Nuremberg Germany
Sandimmun Neoral 100 mg capsule
100 mg Capsule, soft Oral use
Bulgaria Novartis Pharma GmbH Roonstrasse 25, 90429 Nuremberg Germany
Sandimmun Neoral 100 mg/ml oral solution
100 mg/ml Oral solution Oral use 100 mg/ml – 50ml
3

Member State EU/EEA
Marketing authorisation holder
Invented Name Strength Pharmaceutical form
Route of administration
Content (concentration)
Cyprus Novartis Pharmaceuticals UNITED KINGDOM Ltd Frimley Business Park Frimley, Camberley Surrey GU16 7SR United Kingdom
Sandimmun Neoral 25 mg
25 mg Capsule, soft Oral use
Cyprus Novartis Pharmaceuticals UNITED KINGDOM Ltd Frimley Business Park Frimley, Camberley Surrey GU16 7SR United Kingdom
Sandimmun Neoral 50 mg
50 mg Capsule, soft Oral use
Cyprus Novartis Pharmaceuticals UNITED KINGDOM Ltd Frimley Business Park Frimley, Camberley Surrey GU16 7SR United Kingdom
Sandimmun Neoral 100 mg
100 mg Capsule, soft Oral use
Cyprus Novartis Pharmaceuticals UNITED KINGDOM Ltd Frimley Business Park Frimley, Camberley Surrey GU16 7SR United Kingdom
Sandimmun Neoral Oral Solution 100 mg/ ml
100 mg/ml Oral Solution Oral use 100 mg/ml
Czech Republic
Novartis s.r.o. Na Pankráci 1724/129 140 00 Prague 4 - Nusle Czech Republic
Sandimmun Neoral 25 mg
25 mg Capsule, soft Oral use
4

Member State EU/EEA
Marketing authorisation holder
Invented Name Strength Pharmaceutical form
Route of administration
Content (concentration)
Czech Republic
Novartis s.r.o. Na Pankráci 1724/129 140 00 Prague 4 - Nusle Czech Republic
Sandimmun Neoral 50 mg
50 mg Capsule, soft Oral use
Czech Republic
Novartis s.r.o. Na Pankráci 1724/129 140 00 Prague 4 - Nusle Czech Republic
Sandimmun Neoral 100 mg
100 mg Capsule, soft Oral use
Czech Republic
Novartis s.r.o. Na Pankráci 1724/129 140 00 Prague 4 - Nusle Czech Republic
Sandimmun Neoral 100 mg/ml
100 mg/ml Oral solution Oral use 100 mg/ml
Denmark
Novartis Healthcare A/S Lyngbyvej 172 DK-2100 Copenhagen Denmark
Sandimmun Neoral 10 mg Capsule, soft Oral use
Denmark Novartis Healthcare A/S Lyngbyvej 172 DK-2100 Copenhagen Denmark
Sandimmun Neoral 25 mg Capsule, soft Oral use
Denmark Novartis Healthcare A/S Lyngbyvej 172 DK-2100 Copenhagen Denmark
Sandimmun Neoral 50 mg Capsule, soft Oral use
Denmark Novartis Healthcare A/S Lyngbyvej 172 DK-2100 Copenhagen Denmark
Sandimmun Neoral 100 mg Capsule, soft Oral use
5

Member State EU/EEA
Marketing authorisation holder
Invented Name Strength Pharmaceutical form
Route of administration
Content (concentration)
Denmark Novartis Healthcare A/S Lyngbyvej 172 DK-2100 Copenhagen Denmark
Sandimmun Neoral 100 mg/ml Oral solution Oral use 100 mg/ml
Estonia Novartis Finland OY Metsänneidonkuja 10 FIN-02130 Espoo Finland
Sandimmun Neoral 25 mg Capsule, soft Oral use
Estonia Novartis Finland OY Metsänneidonkuja 10 FIN-02130 Espoo Finland
Sandimmun Neoral 50 mg Capsule, soft Oral use
Estonia Novartis Finland OY Metsänneidonkuja 10 FIN-02130 Espoo Finland
Sandimmun Neoral 100 mg Capsule, soft Oral use
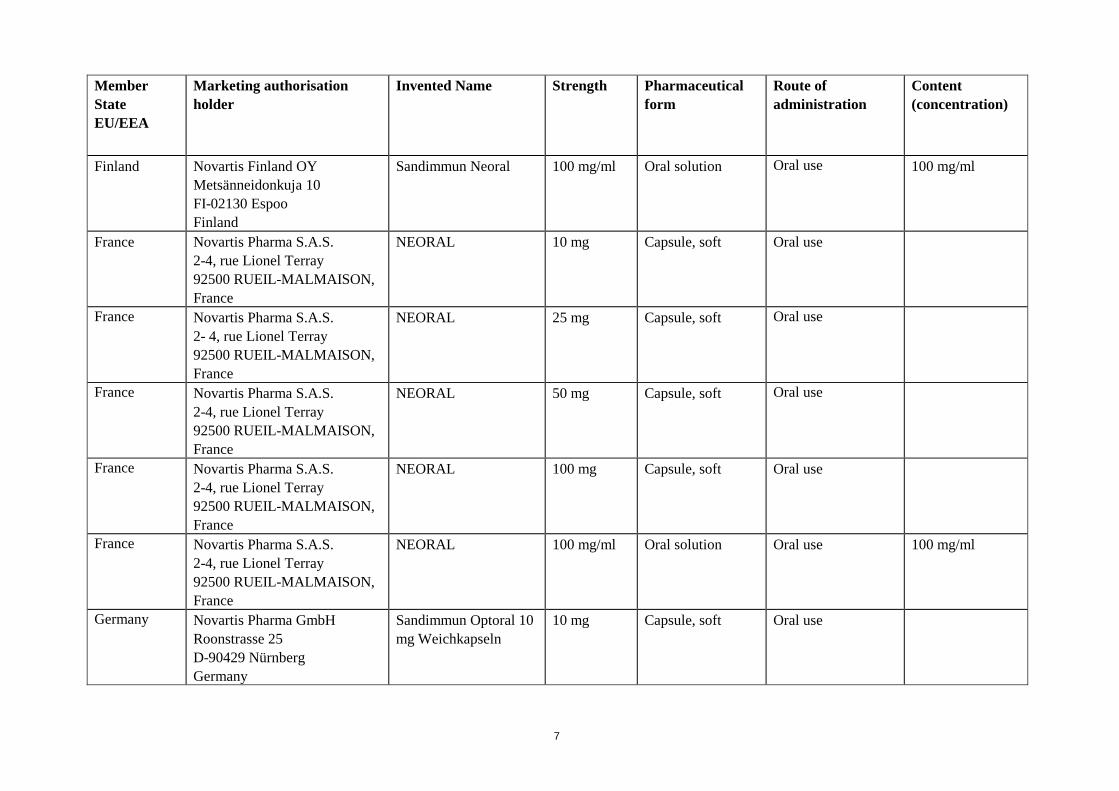
Finland Novartis Finland OY Metsänneidonkuja 10 FI-02130 Espoo Finland
Sandimmun Neoral
25 mg Capsule, soft Oral use
Finland Novartis Finland OY Metsänneidonkuja 10 FI-02130 Espoo Finland
Sandimmun Neoral 50 mg Capsule, soft Oral use
Finland Novartis Finland OY Metsänneidonkuja 10 FI-02130 Espoo Finland
Sandimmun Neoral 100 mg Capsule, soft Oral use
6
Member State EU/EEA
Marketing authorisation holder
Invented Name Strength Pharmaceutical form
Route of administration
Content (concentration)
Finland Novartis Finland OY Metsänneidonkuja 10 FI-02130 Espoo Finland
Sandimmun Neoral
100 mg/ml Oral solution Oral use 100 mg/ml
France Novartis Pharma S.A.S. 2-4, rue Lionel Terray 92500 RUEIL-MALMAISON, France
NEORAL
10 mg Capsule, soft Oral use
France Novartis Pharma S.A.S. 2- 4, rue Lionel Terray 92500 RUEIL-MALMAISON, France
NEORAL 25 mg Capsule, soft Oral use
France Novartis Pharma S.A.S. 2-4, rue Lionel Terray 92500 RUEIL-MALMAISON, France
NEORAL 50 mg Capsule, soft Oral use
France Novartis Pharma S.A.S. 2-4, rue Lionel Terray 92500 RUEIL-MALMAISON, France
NEORAL 100 mg Capsule, soft Oral use
France Novartis Pharma S.A.S. 2-4, rue Lionel Terray 92500 RUEIL-MALMAISON, France
NEORAL 100 mg/ml Oral solution Oral use 100 mg/ml
Germany Novartis Pharma GmbH Roonstrasse 25 D-90429 Nürnberg Germany
Sandimmun Optoral 10 mg Weichkapseln
10 mg Capsule, soft Oral use
7
Member State EU/EEA
Marketing authorisation holder
Invented Name Strength Pharmaceutical form
Route of administration
Content (concentration)
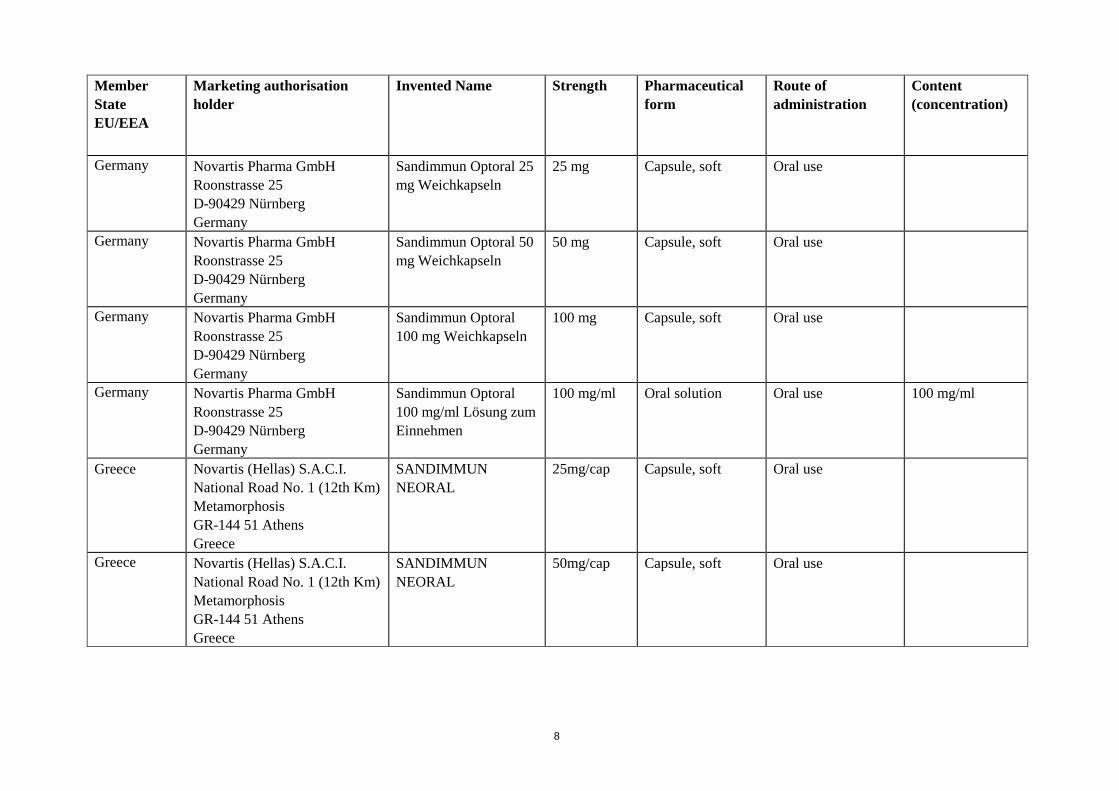
Germany Novartis Pharma GmbH Roonstrasse 25 D-90429 Nürnberg Germany
Sandimmun Optoral 25 mg Weichkapseln
25 mg Capsule, soft Oral use
Germany Novartis Pharma GmbH Roonstrasse 25 D-90429 Nürnberg Germany
Sandimmun Optoral 50 mg Weichkapseln
50 mg Capsule, soft Oral use
Germany Novartis Pharma GmbH Roonstrasse 25 D-90429 Nürnberg Germany
Sandimmun Optoral 100 mg Weichkapseln
100 mg Capsule, soft Oral use
Germany Novartis Pharma GmbH Roonstrasse 25 D-90429 Nürnberg Germany
Sandimmun Optoral 100 mg/ml Lösung zum Einnehmen
100 mg/ml Oral solution Oral use 100 mg/ml
Greece Novartis (Hellas) S.A.C.I. National Road No. 1 (12th Km) Metamorphosis GR-144 51 Athens Greece
SANDIMMUN NEORAL
25mg/cap Capsule, soft Oral use
Greece Novartis (Hellas) S.A.C.I. National Road No. 1 (12th Km) Metamorphosis GR-144 51 Athens Greece
SANDIMMUN NEORAL
50mg/cap Capsule, soft Oral use
8

Member State EU/EEA
Marketing authorisation holder
Invented Name Strength Pharmaceutical form
Route of administration
Content (concentration)
Greece Novartis (Hellas) S.A.C.I. National Road No. 1 (12th Km) Metamorphosis GR-144 51 Athens Greece
SANDIMMUN NEORAL
100mg/cap Capsule, soft Oral use
Greece Novartis (Hellas) S.A.C.I. National Road No. 1 (12th Km) Metamorphosis GR-144 51 Athens Greece
SANDIMMUN NEORAL
500mg/5ml Oral solution Oral use 100 mg/ml
Hungary Novartis Hungária Kft. Pharma részlege Bartók Béla út 43-47 H-1114 Budapest Hungary
Sandimmun Neoral 10 mg lágy kapszula
10 mg Capsule, soft Oral use
Hungary Novartis Hungária Kft. Pharma részlege Bartók Béla út 43-47 H-1114 Budapest Hungary
Sandimmun Neoral 25 mg lágy kapszula
25 mg Capsule, soft Oral use
Hungary Novartis Hungária Kft. Pharma részlege Bartók Béla út 43-47 H-1114 Budapest Hungary
Sandimmun Neoral 50 mg lágy kapszula
50 mg Capsule, soft Oral use
9

Member State EU/EEA
Marketing authorisation holder
Invented Name Strength Pharmaceutical form
Route of administration
Content (concentration)
Hungary Novartis Hungária Kft. Pharma részlege Bartók Béla út 43-47 H-1114 Budapest Hungary
Sandimmun Neoral 100 mg lágy kapszula
100 mg Capsule, soft Oral use
Hungary Novartis Hungária Kft. Pharma részlege Bartók Béla út 43-47 H-1114 Budapest Hungary
Sandimmun Neoral 100 mg/ml belsőleges oldat
100 mg/ml Oral solution Oral use 100 mg/ml
Iceland Novartis Healthcare A/S Edward Thomsens Vej 14 2003 Köbenhavn S Denmark
Sandimmun Neoral 25 mg Capsule, soft Oral use
Iceland Novartis Healthcare A/S Edward Thomsens Vej 14 2003 Köbenhavn S Denmark
Sandimmun Neoral 50 mg Capsule, soft Oral use
Iceland Novartis Healthcare A/S Edward Thomsens Vej 14 2003 Köbenhavn S Denmark
Sandimmun Neoral 100 mg Capsule, soft Oral use
Iceland Novartis Healthcare A/S Edward Thomsens Vej 14 2003 Köbenhavn S Denmark
Sandimmun Neoral 100 mg/ml Oral solution Oral use 100 mg/ml
Ireland Novartis Pharmaceuticals UNITED KINGDOM Ltd Frimley Business Park Frimley, Camberley Surrey GU16 7SR United Kingdom
Neoral 25 mg Capsule, soft Oral use
10

Member State EU/EEA
Marketing authorisation holder
Invented Name Strength Pharmaceutical form
Route of administration
Content (concentration)
Ireland Novartis Pharmaceuticals UNITED KINGDOM Ltd Frimley Business Park Frimley, Camberley Surrey GU16 7SR United Kingdom
Neoral 50 mg Capsule, soft Oral use
Ireland Novartis Pharmaceuticals UNITED KINGDOM Ltd Frimley Business Park Frimley, Camberley Surrey GU16 7SR United Kingdom
Neoral 100 mg Capsule, soft Oral use
Ireland Novartis Pharmaceuticals UNITED KINGDOM Ltd Frimley Business Park Frimley, Camberley Surrey GU16 7SR United Kingdom
Neoral 100 mg/ml Oral solution Oral use 100 mg/ml
Italy Novartis Europharm Limited Wimblehurst Road Horsham West Sussex, RH12 5AB United Kingdom
Sandimmun Neoral 10 mg Capsule, soft Oral use
Italy Novartis Europharm Limited Wimblehurst Road Horsham West Sussex, RH12 5AB United Kingdom
Sandimmun Neoral 25 mg Capsule, soft Oral use
11

Member State EU/EEA
Marketing authorisation holder
Invented Name Strength Pharmaceutical form
Route of administration
Content (concentration)
Italy Novartis Europharm Limited Wimblehurst Road Horsham West Sussex, RH12 5AB United Kingdom
Sandimmun Neoral 50 mg Capsule, soft Oral use
Italy Novartis Europharm Limited Wimblehurst Road Horsham West Sussex, RH12 5AB United Kingdom
Sandimmun Neoral 100 mg Capsule, soft Oral use
Italy Novartis Europharm Limited Wimblehurst Road Horsham West Sussex, RH12 5AB United Kingdom
Sandimmun Neoral 100 mg/ml Oral solution Oral use 100 mg/ml
Latvia Novartis Finland OY Metsänneidonkuja 10 FIN-02130 Espoo Finland
Sandimmun Neoral
25 mg mīkstās kapsulas 25 mg Capsule, soft Oral use
Latvia Novartis Finland OY Metsänneidonkuja 10 FIN-02130 Espoo Finland
Sandimmun Neoral 50 mg mīkstās kapsulas
50 mg Capsule, soft Oral use
Latvia Novartis Finland OY Metsänneidonkuja 10 FIN-02130 Espoo Finland
Sandimmun Neoral 100 mg mīkstās kapsulas
100 mg Capsule, soft Oral use
12

Member State EU/EEA
Marketing authorisation holder
Invented Name Strength Pharmaceutical form
Route of administration
Content (concentration)
Lithuania Novartis Finland Oy Metsänneidonkuja 10 FIN-02130 Espoo Finland
Sandimmun Neoral 25 mg Capsule, soft Oral use
Lithuania Novartis Finland Oy Metsänneidonkuja 10 FIN-02130 Espoo, Finland
Sandimmun Neoral 50 mg Capsule, soft Oral use
Lithuania Novartis Finland Oy Metsänneidonkuja 10 FIN-02130 Espoo Finland
Sandimmun Neoral 100 mg Capsule, soft Oral use
Luxembourg Novartis Pharma GmbH Roonstrasse 25 D-90429 Nürnberg Germany
Sandimmun Optoral 10 mg Weichkapseln
10 mg Capsule, soft Oral use
Luxembourg Novartis Pharma GmbH Roonstrasse 25 D-90429 Nürnberg Germany
Sandimmun Optoral 25 mg Weichkapseln
25 mg Capsule, soft Oral use
Luxembourg Novartis Pharma GmbH Roonstrasse 25 D-90429 Nürnberg Germany
Sandimmun Optoral 50 mg Weichkapseln
50 mg Capsule, soft Oral use
Luxembourg Novartis Pharma GmbH Roonstrasse 25 D-90429 Nürnberg Germany
Sandimmun Optoral 100 mg Weichkapseln
100 mg Capsule, soft Oral use
13
Member State EU/EEA
Marketing authorisation holder
Invented Name Strength Pharmaceutical form
Route of administration
Content (concentration)
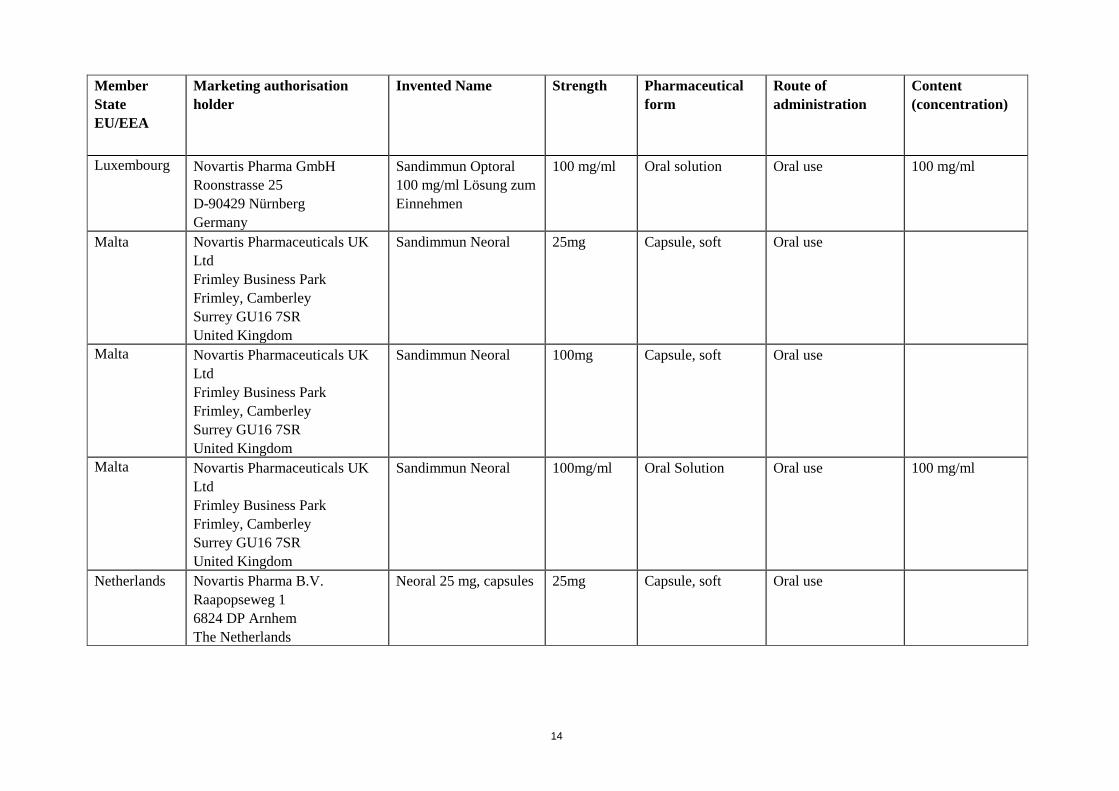
Luxembourg Novartis Pharma GmbH Roonstrasse 25 D-90429 Nürnberg Germany
Sandimmun Optoral 100 mg/ml Lösung zum Einnehmen
100 mg/ml Oral solution Oral use 100 mg/ml
Malta Novartis Pharmaceuticals UK Ltd Frimley Business Park Frimley, Camberley Surrey GU16 7SR United Kingdom
Sandimmun Neoral 25mg Capsule, soft Oral use
Malta Novartis Pharmaceuticals UK Ltd Frimley Business Park Frimley, Camberley Surrey GU16 7SR United Kingdom
Sandimmun Neoral
100mg Capsule, soft Oral use
Malta Novartis Pharmaceuticals UK Ltd Frimley Business Park Frimley, Camberley Surrey GU16 7SR United Kingdom
Sandimmun Neoral 100mg/ml
Oral Solution Oral use 100 mg/ml
Netherlands Novartis Pharma B.V. Raapopseweg 1 6824 DP Arnhem The Netherlands
Neoral 25 mg, capsules 25mg Capsule, soft Oral use
14

Member State EU/EEA
Marketing authorisation holder
Invented Name Strength Pharmaceutical form
Route of administration
Content (concentration)
Netherlands Novartis Pharma B.V. Raapopseweg 1 6824 DP Arnhem The Netherlands
Neoral 100 mg, capsules
100mg Capsule, soft Oral use
Netherlands Novartis Pharma B.V. Raapopseweg 1 6824 DP Arnhem The Netherlands
Neoral 100 mg/ml, drank
100mg/ml
Oral Solution Oral use 100 mg/ml
Norway Novartis Norge AS Nydalen Alle 37A P.O Box 4284 Nydalen, N-0401 Oslo Norway
Sandimmun Neoral 25 mg Capsule, soft Oral use
Norway Novartis Norge AS Nydalen Alle 37A P.O Box 4284 Nydalen, N-0401 Oslo Norway
Sandimmun Neoral 50 mg Capsule, soft Oral use
Norway Novartis Norge AS Nydalen Alle 37A P.O Box 4284 Nydalen, N-0401 Oslo Norway
Sandimmun Neoral 100 mg Capsule, soft Oral use
Norway Novartis Norge AS Nydalen Alle 37A P.O Box 4284 Nydalen, N-0401 Oslo Norway
Sandimmun Neoral 100 mg/ml Oral solution Oral use 100 mg/ml
15

Member State EU/EEA
Marketing authorisation holder
Invented Name Strength Pharmaceutical form
Route of administration
Content (concentration)
Poland Novartis Pharma GmbH Roonstrasse 25 D-90429 Nürnberg Germany
Sandimmun Neoral 10 mg Capsule, soft Oral use
Poland Novartis Pharma GmbH Roonstrasse 25 D-90429 Nürnberg Germany
Sandimmun Neoral 25 mg Capsule, soft Oral use
Poland Novartis Pharma GmbH Roonstrasse 25 D-90429 Nürnberg Germany
Sandimmun Neoral 50 mg Capsule, soft Oral use
Poland Novartis Pharma GmbH Roonstrasse 25 D-90429 Nürnberg Germany
Sandimmun Neoral 100 mg Capsule, soft Oral use
Poland Novartis Pharma GmbH Roonstrasse 25 D-90429 Nürnberg Germany
Sandimmun Neoral 100 mg/ml Oral solution Oral use 100 mg/ml
Portugal Novartis Farma - Produtos Farmacêuticos S.A. Rua do Centro Empresarial, Edificio 8 Quinta da Beloura P-2710-444 Sintra Portugal
Sandimmun Neoral 25 mg Capsule, soft Oral use
16

Member State EU/EEA
Marketing authorisation holder
Invented Name Strength Pharmaceutical form
Route of administration
Content (concentration)
Portugal Novartis Farma - Produtos Farmacêuticos S.A. Rua do Centro Empresarial, Edificio 8 Quinta da Beloura P-2710-444 Sintra Portugal
Sandimmun Neoral 50 mg Capsule, soft Oral use
Portugal Novartis Farma - Produtos Farmacêuticos S.A. Rua do Centro Empresarial, Edificio 8 Quinta da Beloura P-2710-444 Sintra Portugal
Sandimmun Neoral 100 mg Capsule, soft Oral use
Portugal Novartis Farma - Produtos Farmacêuticos S.A. Rua do Centro Empresarial, Edificio 8 Quinta da Beloura P-2710-444 Sintra Portugal
Sandimmun Neoral 100 mg/ml Oral solution Oral use 100 mg/ml
Romania Novartis Pharma GmbH Roonstrasse 25 D-90429 Nürnberg Germany
SANDIMMUN NEORAL capsule moi, 25 mg
25 mg Capsule, soft Oral use
Romania Novartis Pharma GmbH Roonstrasse 25 D-90429 Nürnberg Germany
SANDIMMUN NEORAL,capsule moi, 50 mg
50 mg Capsule, soft Oral use
17

Member State EU/EEA
Marketing authorisation holder
Invented Name Strength Pharmaceutical form
Route of administration
Content (concentration)
Romania Novartis Pharma GmbH Roonstrasse 25 D-90429 Nürnberg Germany
SANDIMMUN NEORAL, solutie orala, 100 mg/ml
100 mg/ml Oral solution Oral use 100 mg /ml
Slovak Republic
Novartis s.r.o. Na Pankráci 1724/129 Prague 140 00 Czech Republic
Sandimmun Neoral 25 mg
25 mg Capsule, soft Oral use
Slovak Republic
Novartis s.r.o. Na Pankráci 1724/129 Prague 140 00 Czech Republic
Sandimmun Neoral 50 mg
50 mg Capsule, soft Oral use
Slovak Republic
Novartis s.r.o. Na Pankráci 1724/129 Prague 140 00 Czech Republic
Sandimmun Neoral 100 mg
100 mg Capsule, soft Oral use
Slovak Republic
Novartis s.r.o. Na Pankráci 1724/129 Prague 140 00 Czech Republic
Sandimmun Neoral 100 mg/ml
100 mg/ml Oral solution Oral use 100 mg/ml
Slovenia Novartis Pharma GmbH Roonstrasse 25 D-90429 Nürnberg Germany
Sandimmun Neoral 25 mg mehke kapsule
25 mg Capsule, soft Oral use
Slovenia Novartis Pharma GmbH Roonstrasse 25 D-90429 Nürnberg Germany
Sandimmun Neoral 50 mg mehke kapsule
50 mg Capsule, soft Oral use
18

Member State EU/EEA
Marketing authorisation holder
Invented Name Strength Pharmaceutical form
Route of administration
Content (concentration)
Slovenia Novartis Pharma GmbH Roonstrasse 25 D-90429 Nürnberg Germany
Sandimmun Neoral 100 mg mehke kapsule
100 mg Capsule, soft Oral use
Slovenia Novartis Pharma GmbH Roonstrasse 25 D-90429 Nürnberg Germany
Sandimmun Neoral 100 mg/ml peroralna raztopina
100 mg/ml Oral solution Oral use 100 mg/ml
Spain Novartis Farmacéutica S.A. Gran Via de les Corts Catalanes, 764 E-08013 Barcelona Spain
Sandimmun Neoral 25 mg cápsulas blandas
25 mg Capsule, soft Oral use
Spain Novartis Farmacéutica S.A. Gran Via de les Corts Catalanes, 764 E-08013 Barcelona Spain
Sandimmun Neoral 50 mg cápsulas blandas
50 mg Capsule, soft Oral use
Spain Novartis Farmacéutica S.A. Gran Via de les Corts Catalanes, 764 E-08013 Barcelona Spain
Sandimmun Neoral 100 mg cápsulas blandas
100 mg Capsule, soft Oral use
Spain Novartis Farmacéutica S.A. Gran Via de les Corts Catalanes, 764 E-08013 Barcelona Spain
Sandimmun Neoral 100 mg/ml solución oral
100 mg/ml Oral solution Oral use 100 mg/ml
19

Member State EU/EEA
Marketing authorisation holder
Invented Name Strength Pharmaceutical form
Route of administration
Content (concentration)
Sweden Novartis Sverige AB Kemistvägen 1B / Box 1150 SE-183 11 Täby Sweden
Sandimmun Neoral 10 mg Capsule, soft Oral use
Sweden Novartis Sverige AB Kemistvägen 1B / Box 1150 SE-183 11 Täby Sweden
Sandimmun Neoral 25 mg Capsule, soft Oral use
Sweden Novartis Sverige AB Kemistvägen 1B / Box 1150 SE-183 11 Täby Sweden
Sandimmun Neoral 50 mg Capsule, soft Oral use
Sweden Novartis Sverige AB Kemistvägen 1B / Box 1150 SE-183 11 Täby Sweden
Sandimmun Neoral 100 mg Capsule, soft Oral use
Sweden Novartis Sverige AB Kemistvägen 1B / Box 1150 SE-183 11 Täby Sweden
Sandimmun Neoral 100 mg/ml Oral solution Oral use 100 mg/ml
United Kingdom
Novartis Pharmaceuticals UK Ltd Frimley Business Park Frimley, Camberley Surrey GU16 7SR United Kingdom
Neoral Soft Gelatin Capsules 10mg
10 mg Capsule, soft Oral use
20

Member State EU/EEA
Marketing authorisation holder
Invented Name Strength Pharmaceutical form
Route of administration
Content (concentration)
United Kingdom
Novartis Pharmaceuticals UK Ltd Frimley Business Park Frimley, Camberley Surrey GU16 7SR United Kingdom
Neoral Soft Gelatin Capsules 25mg
25 mg Capsule, soft Oral use
United Kingdom
Novartis Pharmaceuticals UK Ltd Frimley Business Park Frimley, Camberley Surrey GU16 7SR United Kingdom
Neoral Soft Gelatin Capsules 50mg
50 mg Capsule, soft Oral use
United Kingdom
Novartis Pharmaceuticals UK Ltd Frimley Business Park Frimley, Camberley Surrey GU16 7SR United Kingdom
Neoral Soft Gelatin Capsules 100mg
100 mg Capsule, soft Oral use
United Kingdom
Novartis Pharmaceuticals UK Ltd Frimley Business Park Frimley, Camberley Surrey GU16 7SR United Kingdom
Neoral Oral solution 100 mg/ml Oral Solution Oral use 100 mg/ml
21

Annex II
Scientific conclusions and grounds for the variation to the terms of the Marketing Authorisation
22

Scientific conclusions Overall summary of the scientific evaluation of Sandimmun Neoral and associated names (see Annex I) Sandimmun Neoral is a microemulsified formulation of ciclosporin. Ciclosporin is a potent immunosuppressive agent used in human solid organ and bone marrow transplantation to prevent graft rejection and in Graft Versus Host Disease (GVHD). Ciclosporin is also used in a variety of conditions that are known, or may be considered, to be of autoimmune origin (endogenous uveitis, nephrotic syndrome, rheumatoid arthritis, psoriasis and atopic dermatitis). In comparison to Sandimmun (oil-based formulation of ciclosporin), Sandimmun Neoral (microemulsified formulation) provides improved dose linearity of ciclosporin exposure, a more consistent absorption profile and shows less influence from concomitant food intake and from diurnal rhythm. Overall, these properties result in lower within-patient variability in the pharmacokinetics of ciclosporin and a stronger correlation between trough concentrations and total exposure. As a consequence of these additional advantages, Sandimmun Neoral can be administered independently of mealtimes. In addition, Sandimmun Neoral produces a more uniform exposure to ciclosporin throughout the day and from day to day on a maintenance regimen. Sandimmun Neoral was first registered in Germany in February 1993 and is available in the EU as 10 mg, 25 mg, 50 mg, 100 mg soft gelatin capsules and 100 mg/ml oral solution. The registration of Sandimmun Neoral was based on efficacy and safety data from clinical studies performed with the oil-based formulation (Sandimmun), first registered in Switzerland in December 1982. Additional pharmacokinetics and pharmacodynamics studies, as well as non clinical trials were performed with Sandimmun Neoral medicinal product to support its registration. In the European Union (EU), Sandimmum and Sandimmun Neoral are registered via national procedures. Sandimmun Neoral is available as Sandimmun Neoral soft gelatin capsules (10 mg, 25 mg, 50 mg and 100 mg) and Sandimmun Neoral oral solution, 100 mg/ml. Sandimmun is available as Sandimmun soft gelatin capsules (25 mg, 50 mg and 100 mg), Sandimmun oral solution, 100 mg/ml and Sandimmum concentrate for solution for infusion, 50mg/ml. Not all strengths and pharmaceutical forms are registered in each country. Furthermore, not all indications are approved in each country. In October 2010, Sandimmun Neoral was included in the list of products for Summary of Product Characteristics (SmPC) harmonization, requested by the CMD(h), in accordance with Article 30(2) of Directive 2001/83/EC, as amended. Due to the divergent national decisions taken by Member States (MS) concerning the authorization of Sandimmun Neoral (and associated names), the European Commission (EC) notified the EMA/CHMP secretariat of an official referral under Article 30(2) of Directive 2001/83/EC as amended, to resolve divergences amongst the nationally authorised Sandimmun Neoral SmPCs across the EU/EEA region.
• Clinical aspects
To achieve a harmonized SmPC, the MAH used the wording that is common to national SmPCs in the majority of MSs and the MAH’s Core Data Sheet (CDS) for Sandimmun Neoral (dated 13 February 2012), as well as submitted legacy studies and literature references. The agreed Core Safety profile (CSP) from the last PSUR 13 work sharing procedure (EE/H/PSUR/0007/001) and the public AR from the paediatric article 45 procedure (CZ/W/04/pdWS/01, 2010) were also used. A number of areas of disharmony in the Product Information have been considered as follows: Section 4.1 – Therapeutic indications
Transplantation indications
23

• Solid organ transplantation:
In line with the overall above mentioned strategy, the MAH proposed an indication wording which is already approved as proposed in 21 EU national labels. The CHMP questioned the MAH’s justification with regards to the listing of specific organ transplantations in the indication. The MAH agreed with the CHMP that no specific organ transplantations should be mentioned in section 4.1 unless not appropriate to use. The wording was reviewed accordingly. With regards to the treatment of rejection, the main concerns reflected by the CHMP related to the switch from tacrolimus, treatment of humoral rejections with Cyclosporin and in case of chronic allograft injury, as this has been seen as chronic rejection. The CHMP requested the MAH to compile all available data on switch to ciclosporin in case of rejection with any other immunosuppressive agent, not only tacrolimus. The MAH addressed this concern; based on the submitted data the CHMP agreed with the MAH that the common practice is to change to another agent in case of rejection. Finally the inclusion of the term “cellular” rejection was also discussed since the diagnosis of humoral rejection episodes is controversial. The CHMP is of the view that introducing Sandimmun Neoral for the treatment of rejection is most appropriate for cellular rather than humoral rejection, based on the mechanism of action of CNI’s. The MAH agrees with the CHMP’s view. The proposed wording was reviewed and agreed accordingly.
• Bone marrow transplantation (BMT)
All MS except Norway have the indication bone marrow transplantation and GVHD approved. The efficacy of ciclosporin has been demonstrated in bone marrow transplant (BMT) recipients in eight studies carried out in Europe and US with a total of 227 patients. Seven trials were conducted for the prevention of graft-versus host disease (GVHD), one trial for the treatment of acute GVHD. The MAH is of the view that the efficacy of ciclosporin in bone marrow transplantation and GVHD is well established from the data in the original MAA, published clinical studies and extensive clinical use. The CHMP questioned though the benefit-risk of ciclosporin in “prevention of graft rejection following bone marrow transplantation”: the CHMP requested the MAH to submit data confirming a positive benefit-risk of ciclosporin in terms of frequency of stem cell engrafting/graft failure beyond the benefits/risk (B/R) of conditioning treatment. In their response the MAH confirmed that the data from these studies as well as extensive clinical experience are supportive of the indication “Prevention of graft rejection” for Ciclosporin. The CHMP is in agreement with the MAH’s position. In addition, a clarification of the B/R of ciclosporin in prevention of graft rejection after non-myloablative stem cell transplantation was also requested by the CHMP; the CHMP reviewed the MAH’s position and considered unnecessary to specify myeloablative vs. non-myeloablative stem cell transplantation in the Ciclosporin indication. Finally the CHMP also requested the MAH to discuss whether the heading “bone marrow transplantation” shall be updated to “allogenous stem cell transplantation”, i.e. independent from the source (else than non-host) of the stem cells and blasts. The MAH addressed the CHMP’s concerns; the CHMP is of the view that clinical experience supports the proposed additions in the indication. A wording was agreed accordingly. Non-transplantation indications
• Endogenous uveitis The MAH’s proposed indication wording for the uveitis and Behçet uveitis is approved in 14 EU countries.
24

The review of the original Sandimmun Dossiers from major markets such as France, the U.S. and UK which contains the clinical results from a total of 15 global studies has been performed. The dossier of Sandimmun was used as a basis of the review as the dossier supporting the approval of the new ciclosporin formulation (Sandimmun Neoral) was based on pharmacokinetics evaluation that demonstrated equivalence between the 2 forms of ciclosporin (oil-based formulation versus microemulsified formulation). The studies presented at renewals of marketing authorization in EU were also screened and reviewed. At the time of the submission of the oil-based formulation of ciclosporin, Sandimmun, in 1987, a comprehensive clinical data summary on endogenous uveitis was available (Nussenblatt 1987). Two types of studies, open and controlled masked, were carried out in order to evaluate the efficacy of ciclosporin in the treatment of severe sight-threatening intermediate and posterior uveitis. The CHMP noted that the majority of patients benefited from ciclosporin treatment in all reports. Although some patients experienced adverse reactions, mostly nephrotoxicity, hypertension and metabolic disorders, the CHMP noted that these adverse reactions are well known and could be managed in dose dependent manner. From the data provided and other published data the CHMP concluded that benefit-risk ratio for ciclosporin in treatment of endogenous refractory uveitis, including Behçet uveitis, is positive. The CHMP also raised questions regarding the risk of aggravation of the neurological manifestations of Behcet’s disease by Ciclosporin. Based on literature and supportive data the MAH is of the view that the data presented supports the positive benefit/risk of the indication while recommending using Ciclosporin as systemic therapy both for non-infectious uveitis and for the ocular manifestations of Behcet’s disease in patients without neurological manifestations. A wording was agreed accordingly.
• Nephrotic syndrome (NS) The MAH’s proposed indication wording for nephritic syndrome is approved in 16 EU countries. The efficacy of Sandimmun (oil based formulation of ciclosporin) has been demonstrated in 4 randomized controlled and 5 uncontrolled studies.The clinical results from these 9 clinical studies were analyzed using a pooling of data from all studies (controlled and uncontrolled). In parallel of these 9 performed studies, 2 double-blind placebo controlled multicenter studies and 1 multicenter study comparing ciclosporin with cyclophosphamide in steroidresistant patients had to be stopped prematurely because of a lack of suitable patients consenting to receive placebo or a cytostatic agent. Pediatric data from controlled and uncontrolled studies were also provided. At the time of submission, patients of 17 years of age maximum qualified as “children”. In view of the above dataset, the CHMP considered that the efficacy of Sandimmun (oil based formulation of ciclosporin) has been demonstrated in 4 randomized controlled and 5 uncontrolled studies as well as studies conducted in pediatric patients. Moreover, recent trials have confirmed the benefit of Sandimmun Neoral in different forms of nephrotic syndrome in children and adults. However the CHMP had concerns over the fact that current indication was too broad as use in secondary glomerulonephritis is controversial. The CHMP therefore requested the MAH to justify the positive benefit risk for all nephrotic conditions except the primary minimal change glomerulonephritis, primary focal segmental glomerulosclerosis, or primary membranous glomerulonephritis. The CHMP is of the view that the indication should be limited to primary glomerulonephritis cases as specified above. The MAH agreed with the CHMP’s opinion and a wording was agreed accordingly.
• Rheumatoid arthritis (RA)
25

The MAH’s proposed indication wording for rheumatoid arthritis is approved in 13 EU countries. The rationale given by the MAH for the proposed indication was based on the following data: the initial pilot study in active rheumatoid arthritis used a dose of 10 mg/kg/day, half the dose used in solid organ transplantation at that time. The promising benefit was offset by the renal dysfunction and hypertension. Subsequent, studies using lower doses showed a better risk-benefit ratio. European controlled double-blind trials used 5 mg/kg/d that allowed a downward titration to find the maximum tolerated dose. Renal dysfunction above the critical threshold, defined as creatinine increased by 30-50% over baseline, was less of a problem when starting with a dose of 2.5 mg/kg/day. The control groups were either using placebo, or azathioprine, or D-penicillamine. This data, along with ciclosporin experience in other nontransplant diseases, helped to design the four pivotal placebo-controlled double-blind Sandimmun (SIM) trials in severe RA in the US and Canada. The MAH presented respectively the clinical efficacy outcome of the US and Canada studies and then the European studies. Rheumatoid arthritis is an approved therapeutic indication in all EU countries. ciclosporin has been extensively studied in several clinical trials in patients with rheumatoid arthritis in whom conventional therapy is ineffective or inappropriate, as well as in many published studies reporting the use of ciclosporin in this indication. The CHMP is of the opinion that the available data confirms the use of ciclosporin in the following indication: “Treatment of severe, active rheumatoid arthritis.”
• Psoriasis The Psoriasis is an approved therapeutic indication in all EU countries. Based on the comprehensive clinical data summary on psoriasis and references provided by the MAH, the CHMP considers the argumentation made by the MAH acceptable and therefore agrees with the wording proposed by the MAH.
• Atopic dermatitis The MAH proposed the following wording for this indication: “Sandimmun Neoral is indicated in patients with severe atopic dermatitis when systemic therapy is required.” The MAH’s proposed indication wording for the Atopic dermatis is approved in 15 EU countries. Ciclosporin has been studied in several clinical trials in atopic dermatitis, although the studies by modern standards are considered small. 15 EU countries already have exactly the proposed label and in those which do not, the deviations are not considered large. Therefore, based on clinical data summary on atopic dermatitis and references provided by the MAH, the CHMP considers the argumentation made by the MAH acceptable and therefore agrees with the above mentioned wording.
• Aplastic Anemia The indication aplastic anemia is only approved in France. As recorded in the minutes of the pre-referral meeting held on 27 July 2011, regarding the approach to label harmonisation, the Agency agreed with the MAH’s proposal to use the SmPC wording that is common in the majority of the Members States, the Sandimmun and Sandimmun Neoral CDSs as justified by the review of legacy studies and literature references. In line with this agreement, the MAH did not include the indication of aplastic anemia in the harmonized label of Sandimmun and Sandimmun Neoral since this indication is approved in only one of 27 member states and is not listed in Sandimmun and Sandimmun Neoral CDSs. The CHMP endorses this proposal
26
Section 4.2 – Posology and method of administration This section contains general parts as well as separate sub-sections for each indication. In the following, the entire section 4.2 is reviewed, sub-section by sub-section. Posology: The MAH proposed the following wording for the posology: “The dose ranges given for oral administration are intended to serve as guidelines only. The daily doses of Neoral should always be given in two divided doses.” The MAH’s statement “The dose ranges given for oral administration are intended to serve as guidelines only” is endorsed by the CHMP. However the statement “The daily doses of Neoral should always be given in two divided doses” was partly endorsed by the CHMP since the word “always” should be omitted (in some cases, three times daily administration may be needed). In addition, the CHMP requested the MAH to specify in the SmPC whether Sandimmun/Sandimmun Neoral should be administered with or without food or if administration may be performed irrespective of concomitant food intake. Considering the narrow therapeutic window for ciclosporin, the CHMP requested the MAH to consider ciclosporin intake in order to reduce intra-individual variability. The MAH acknowledged that food affects the absorption of ciclosporin both from the Sandimmun formulation and, to a lesser extent, from the Sandimmun Neoral formulation. The MAH stated in their response package that the absolute changes may be considered small, but in view of the narrow therapeutic window for ciclosporin, standardised intake in relation to food intake would be preferable to reduce intra-individual variability. The MAH therefore agreed to revise the wording, recommending that Sandimmun Neoral should be administered on a consistent schedule with regard to time of day and relation to meals, as follows: “The daily doses of Sandimmun/Sandimmun Neoral always should be given in two divided doses equally distributed throughout the day, taken at the same time of the day, e.g., in the morning and in the evening. It is recommended that Sandimmun Neoral be administered on a consistent schedule with regard to time of day and relation to meals. ” This wording was endorsed by the CHMP. Lastly, based on the fact that ciclosporin is a potent active substance associated with serious safety concerns, the CHMP was of the opinion that the posology section should clearly state that Sandimmun/Sandimmun Neoral is a product to be handled by specialists within the respective therapeutic area; a general wording was agreed and included accordingly in section 4.2. General monitoring of posology.
The CHMP was of the opinion that a general message about the value of monitoring to guide posology was missing. This type of information is in line with SmPCs of several Member States. The CHMP was concerned by the fact that different approaches in monitoring proposals for transplantation and non-transplantation populations were proposed by the MAH, ignoring blood levels measurements in non-transplant indications. In response to the CHMP’S request, the MAH adjusted information by adding cautious reference to blood level monitoring options for non-transplant indications and additionally stressing the practice protocols for transplantation indications. This approach was acceptable to the CHMP and final wordings in sections 4.2 and 4.4.were agreed accordingly. Transplantation indications: The MAH proposed two different wordings for each of the paragraphs on transplantation:
• Solid organ transplantation Based on the most commonly approved wording in EU member states and the recent version of the company core data sheet (CDS) dated 13 February 2012, the MAH proposed a wording which is already approved in 13 EU MS.
27
In the original Sandimmun studies, initial doses in the range 14-18 mg/kg/day have been used and these were subsequently reduced to a maintenance dose in the range 6-10 mg/kg/day. The administration started within 2-20 hours prior to surgery. Based on the higher Cmax and AUC values achieved with Sandimmun Neoral compared to Sandimmun, the resulting individualized doses of Sandimmun Neoral were on average lower compared to Sandimmun. Hence, this supports the lower doses proposed for Sandimmun Neoral in the proposed SmPC. However, since the studies in the original Sandimmun dossier are old and the posology based on those data is therefore obsolete in comparison with the different transplantation regimens used today, the CHMP was of the view that the dosage should also be guided by monitoring of ciclosporin blood levels. The MAH agreed with the CHMP’s opinion and hence revised the wording of the posology in the solid organ transplantation indication accordingly.
• Bone marrow transplantation Extensive information was provided by the MAH, including the dosages used in clinical studies that supported the approval of Sandimmun and Sandimmun Neoral in the bone marrow transplant indications. After review of the dataset, the proposed posology in the bone marrow transplantation indication as approved in 16 EU MS was acceptable to the CHMP. Non-transplantation indications: The MAH proposed a new general wording to introduce the paragraph on non- transplantation indications, as general recommendations. The CHMP agreed that general information applicable to all these indications was relevant to include. However the CHMP considered that this paragraph should be complemented with recommendations for further controls to be made, e.g. of liver function, bilirubin, serum electrolytes and blood pressure and that it is preferred to use glomerular filtration rate determined by a reliable and reproducible method rather than serum creatinine. Furthermore, in addition to a strengthening of the monitoring of renal function, the CHMP was of the view that occasional monitoring of ciclosporin blood levels were also relevant in these indications. The MAH proposed a wording accordingly to include these recommendations, as requested by the CHMP. Lastly the MAH recommended oral administration in non-transplantation indications due to lack of data and potential risk for anaphylactic reactions with intravenous use; this was acknowledged by the CHMP. However, in case of a more prolonged inability to use oral ciclosporin, use of IV ciclosporin should be considered, provided that care is taken to administer an adequate IV dose. Thus, a wording was proposed by the MAH and agreed by the CHMP to address this matter. Further to this introduction paragraph on non-transplantation, the MAH proposed a posology for each of the non-transplantation indications (i.e. endogenous uveitis, nephrotic syndrome, rheumatoid arthritis, psoriasis, atopic dermatitis). Based on the assessment of the MAH’s proposal, the responses to the LoQ, LoOI and following the discussions of the committee, the CHMP agreed upon a harmonised wording of the section 4.2 accordingly for the non-transplantations indications. Switching from Sandimmun to Sandimmun Neoral The MAH proposed a wording for recommendations related to the switch between Sandimmun and Sandimmun Neoral in accordance with the approved wording of 9 countries. Since not all countries have such a text included in their national labels and in some countries only Sandimmun Neoral is available, the MAH recommended shortening the proposed text. The CHMP was in agreement with this approach and a revised wording was agreed consequently. Switching between oral ciclosporin formulations The wording proposed by the MAH is already approved in 24 countries and several other countries have very similar information. The MAH considered that the information included in the proposed harmonized label provided relevant information to the prescribing physician to optimize patient
28

management. However in view of the CHMP concerns the MAH revised and shortened the initially proposed text, leading for a final wording which was endorsed by the CHMP. Special populations Referring to the “non-transplantation indications” section, likewise, the MAH proposed a posology for each of the special populations (i.e. patients with renal impairment, patients with hepatic impairment, paediatric population, elderly population). Based on the assessment of the MAH’s proposal, the responses to the LoQ, LoOI and following the discussions of the committee, the CHMP agreed upon a harmonised wording of the section 4.2 accordingly for the special populations. Method of administration The MAH proposed the wording related to the method of oral administration which is approved in 12 EU countries. The proposed wording was acceptable to the CHMP.
Sections 4.3 to 4.9 – from “Contraindications” to “Overdose” The approach taken by the MAH to achieve a proposed harmonized SmPC with regard to the safety sections of the SmPC (sections 4.3 to 4.9) was to use as a basis the most recently updated MAH’s Core Data Sheet (CDS) of Sandimmun Neoral, dated 13 February 2012 (as justified by a review of submitted legacy studies, and identified literature references) and the finalized Core Safety profile (CSP) from the last PSUR 13 work sharing (WS) procedure (EE/H/PSUR/0007/001). According to the EU guideline on the implementation of the outcome of a PSUR WS procedure, the 29 EU countries have submitted, within a 4 month timeframe after the release of the CSP, a variation to implement the agreed CSP. Given the fact that a harmonized label was agreed among the EU community in February 2011 through the PSUR 13 WS procedure, the MAH’s position was to use the agreed CSP entirely (i.e. without any further changes). In November 2011, a full review of the company label (CDSs for both products Sandimmun and Sandimmun Neoral) was initiated. As an outcome of this full review, both CDSs were finalized with a release date of 13 February 2012. In that context, a thorough comparison of the Feb 2011 agreed CSP information and the safety sections of the newly released CDSs was performed by the MAH. To ensure that the Core Safety Information of the updated CDSs remains in line with the agreed CSP information, newly incorporated safety information into the CDS was proposed by the MAH for consideration into the agreed CSP, hence for the harmonized Eu SmPC safety related sections. Thus, the harmonized label for the safety section of the SmPC proposed by the MAH was based on the agreed CSP and enhanced with some newly added information from the full review of the MAH’s labels (CDSs). The CHMP was in agreement with the approach taken by the MAH. Sections 4.3 – Contraindications As stated above, the MAH proposed a following wording for the above-mentioned paragraph based on the wordings used in the CDS and CSP. Ciclosporin is contraindicated for some HMG-CoA reductase inhibitors (statins) due to the CYP3A4 and/or Pgp inhibitory potential of ciclosporin. The MAH discussed the need of a contraindication of statins for cyclosporin and the need of further contraindications for other medicinal products/herbals. The CHMP considered that the use of Hypericum perforatum (St. John's wort, SJW) products in the treatment of a mild depression was not considered to balance the potential risk of an acute organ rejection caused by SJW induction; the CHMP requested the introduction of a contraindication accordingly. However concerning HMG CoA reductase inhibitors (statins), the CHMP agreed that a
29

strict contraindication may not be warranted, however, information in section 4.4 should be strengthened. In addition, the CHMP considered that substrates for CYP3A4 and/or P-gp and for which elevated plasma levels are associated with serious safety concerns should not be combined with ciclosporin (e.g. dabigatran etexilate, bosentan, aliskiren). The MAH agreed to include the above mentioned contraindication. A wording was agreed accordingly.
Section 4.4 - Special Warnings and Precautions for Use With regards to the paragraphs concerning Medical supervision, Lymphomas and other malignancies, Geriatrics, Hyperkalaemia, Hypomagnesemia and Hyperuricaemia, Special excipients, the MAH proposed the CSP wording as the harmonised SmPC text. The CHMP agreed with the wording proposed by the MAH. Concerning the sub-sections on infections, renal toxicity and hepatotoxicity, monitoring ciclosporin levels in transplant patients, hypertension, blood lipids increased, live-attenuated vaccines and interactions, wordings were proposed by the MAH and intensively discussed and revisited as per CHMP requests. Similarly to the section 4.2, wordings for each of the sub-sections for the different non-transplantation indications were discussed and agreed between the CHMP and MAH. Section 4.5 - Interaction with Other Medicinal Products and Other Forms of Interaction The MAH proposed wordings for the sub-sections “Food interactions, Drug interactions, Drugs that decrease ciclosporin levels, Drugs that increase ciclosporin levels, Other relevant drug interactions, Recommendations, Paediatric population and Other relevant drug interactions.” The MAH proposed the CSP wording as the harmonized SmPC text for all sections except the additional text regarding interactions with bosentan/ ambrisentan and anthracycline antibiotics. The CHMP did not agree with the wording proposed by the MAH in this section. The CHMP provided the MAH with a detailed suggestion of a clearer structure and proposed text revisions accordingly. The CHMP also requested the MAH to provide more detailed information that could help the dose adjustments. Lastly the CHMP was of the view that further additions to the lists of interactants would be of value, based on an updated survey. Finally the MAH was also requested to update this section with more information concerning the inhibitory potential of ciclosporin on other transporters than P-gp. The MAH provided the requested data and clarifications accordingly. A harmonised wording was therefore agreed. Section 4.6 - Pregnancy and Lactation The MAH proposed a wording on which the CHMP agreed with the exception of one minor comment, which was taken into consideration subsequently by the MAH. A wording was agreed accordingly.
Section 4.7 - Effects on Ability to Drive and Use Machines The MAH proposed to harmonise the SmPC text along with the agreed CSP. The CHMP agreed with the wording proposed by the MAH. Section 4.8 - Undesirable Effects The MAH proposed wordings for the sub-sections Summary of the safety profile, Doses/side effects, Infections and infestations and Neoplasms, Other ADRs from post-marketing experience.
30

With regards to the sub-section Summary of the safety profile, the MAH proposed the inclusion of an overall summary of the principal adverse reactions which were most frequently reported in clinical trials. The CHMP agreed with the addition proposed by the MAH. Regarding the sub-sections Doses/side effects, Infections and infestations and Neoplasms, Other ADRs from post-marketing experience, the MAH proposed align the harmonized SmPC text with the agreed CSP. The CHMP was in agreement with this approach and related wordings as proposed by the MAH. Concerning the wording contained in the sub-section Tabulated summary of ADRs, the MAH made a complete revision of the ADR table and changed many of the frequency figure, in most cases based on the fact that several ADRs originated from post-marketing data and a denominator was missing for the estimation of a frequency. Whilst reviewing the MAH’s proposal, in view of the SmPC guideline, the CHMP considered that the category “not known” should only be used in exceptional cases; the MAH was requested to adhere to the classification according to the CSP unless adequately justified. More specifically, considering data on ADRs frequencies in clinical trials the CHMP requested the MAH to state the reasons to set different frequencies comparing to the ones that have been calculated and thus, proposals were made with regards to some ADRs such as hyperglycaemia, headache, migraine, abdominal discomfort and gingival hyperplasia. The MAH accepted the proposal to amend the ADRs as highlighted by the CHMP. Other changes were also introduced including several proposed downgraded positions; justifications were requested by the CHMP and provided by the MAH subsequently. In addition, the MAH clarified as requested why conjunctivitis, depression and hearing loss were not included in the ADR table. A revised wording was proposed by the MAH accordingly and endorsed by the CHMP. Finally in this section, the MAH proposed two additions to this section, under the format of two new sub-sections on Acute and chronic nephrotoxicity and Paediatric population. These paragraphs were not included in the CSP. The CHMP was of the view that the proposed text is relevant to include and therefore the CHMP agreed with the wordings as proposed by the MAH. Section 5.1 - Pharmacodynamic Properties The MAH proposed wording was in line with the overall strategy undertaken to propose a harmonized wording based on the most commonly approved label across the EU community. The CHMP therefore agreed with the approach taken by the MAH. However the CHMP considers that data of use in children in nephrotic syndrome should be included under the heading Paediatric population. This point was addressed by the MAH and a wording was agreed. In addition, the CHMP requested the MAH to provide a clear rationale for having slightly different description of pharmacodynamic section in Sandimmun (both oral and injection) vs Sandimmun Neoral versions of SmPCs. The MAH agreed to correct this and proposed a wording for Sandimmum and Sandimmum Neoral which was acceptable to the CHMP. Section 5.2 - Pharmacokinetic Properties The MAH proposed wordings for the sub-sections “Absorption, Distribution, Biotransformation and Elimination, Special populations and Paediatric population.” based on a harmonized text already approved in 13 EU countries. The MAH proposed’ wording was line with the overall strategy undertaken to propose a harmonized wording based on the most commonly approved label across the EU community. This was endorsed by the CHMP with the exceptions of some requests for clarifications, which were subsequently provided by the MAH with supportive data.
31

The MAH dedicated the whole sub-section to a comparison between Sandimmun and Sandimmun Neoral. This was supported since it is of interest in the states where both formulations are used. Section 5.3 - Preclinical Safety Data The MAH proposed a wording that was approved in between 18 an 24 MS, depending on sub-sections. Although the proposed text was already approved in the majority of EU countries, the CHMP is of the opinion that some structural modification of the text was needed. Furthermore, since ciclosporin from a non-clinical point of view is a well-known compound, the CHMP requested the MAH to delete the paragraph concerning clinical safety data on development of malignancy. The MAH addressed the points raised by the CHMP and proposed a final wording for this section on which the CHMP agreed. Section 6.3 - Shelf life The CHMP requested the MAH to clarify the discrepancy in the shelf life term; the CHMP was concerned by the different shelf-life periods. The MAH explained that shelf life periods were not harmonised and proposed to follow the safest approach to Sandimmun (to fix 36 months period) and the last reduced period for Sandimmun Neoral that is approved in EU countries via variation procedure. The CHMP was in agreement with the MAH’s proposal. Section 6.4 - Special precautions for storage The MAH confirmed that the storage conditions in the SmPCs of Sandimmun Neoral soft gelatin capsules and oral solutions are already aligned with the requirements set in the Guideline on Declaration of Storage Conditions (CPMP/QWP/609/96/Rev 2 dated 19 Nov 2007).
Recommendation
In conclusion, based on the assessment of the MAH’s proposal, the responses to the LoQ, LoOI and following the discussions of the committee, the CHMP agreed upon and adopted harmonised sets of PI documents for the various presentations of Sandimmun Neoral and associated names. Based on the above the CHMP considers the benefit/risk ratio of Sandimmun Neoral to be favourable and the harmonised PI to be approvable.
Grounds for amendment of the summary of product characteristics, labelling and package leaflet
Whereas • the scope of the referral was the harmonisation of the summary of products characteristics,
labelling and package leaflet
• the summary of products characteristic, labelling and package leaflet proposed by the marketing authorisation holders have been assessed based on the documentation submitted and the scientific discussion within the Committee
the CHMP has recommended the amendment of the marketing authorisations for which the summary of product characteristics, labelling and package leaflet are set out in Annex III for Sandimmum and associated names (see Annex I).
32

ANNEX III
SUMMARY OF PRODUCT CHARACTERISTICS, LABELLING AND PACKAGE LEAFLET
Note: This summary of product characteristics, labelling and package leaflet is the version valid at the time of Commission Decision. After the Commission Decision the National Competent Authorities will update the product information as required.
33

SUMMARY OF PRODUCT CHARACTERISTICS
34

1. NAME OF THE MEDICINAL PRODUCT Sandimmun Neoral and associated names (see Annex I) 10 mg soft capsules Sandimmun Neoral and associated names (see Annex I) 25 mg soft capsules Sandimmun Neoral and associated names (see Annex I) 50 mg soft capsules Sandimmun Neoral and associated names (see Annex I) 100 mg soft capsules [See Annex I – To be completed nationally] 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Each capsule contains 10 mg ciclosporin. Excipients with known effect: Ethanol: 10 mg/capsule. Sandimmun Neoral soft capsules contain 11.8% v/v ethanol (9.4% m/v). Propylene glycol: 10 mg/capsule. Macrogolglycerol hydroxystearate/Polyoxyl 40 hydrogenated castor oil: 40.5 mg/capsule. Each capsule contains 25 mg ciclosporin. Excipients with known effect: Ethanol: 25 mg/capsule. Sandimmun Neoral soft capsules contain 11.8% v/v ethanol (9.4% m/v). Propylene glycol: 25 mg/capsule. Macrogolglycerol hydroxystearate/Polyoxyl 40 hydrogenated castor oil: 101.25 mg/capsule. Each capsule contains 50 mg ciclosporin. Excipients with known effect: Ethanol: 50 mg/capsule. Sandimmun Neoral soft capsules contain 11.8% v/v ethanol (9.4% m/v). Propylene glycol: 50 mg/capsule. Macrogolglycerol hydroxystearate/Polyoxyl 40 hydrogenated castor oil: 202.5 mg/capsule. Each capsule contains 100 mg ciclosporin. Excipients with known effect: Ethanol: 100 mg/capsule. Sandimmun Neoral soft capsules contain 11.8% v/v ethanol (9.4% m/v). Propylene glycol: 100 mg/capsule. Macrogolglycerol hydroxystearate/Polyoxyl 40 hydrogenated castor oil: 405.0 mg/capsule. For the full list of excipients see section 6.1. 3. PHARMACEUTICAL FORM Capsule, soft Yellow-white, oval soft gelatin capsules, imprinted “NVR 10” in red. Blue-grey, oval soft gelatin capsules, imprinted with “NVR 25mg” in red. Yellow-white, oblong soft gelatin capsules, imprinted with “NVR 50mg” in red. Blue-grey, oblong soft gelatin capsules, imprinted with “NVR 100mg” in red. 4. CLINICAL PARTICULARS 4.1 Therapeutic indications Transplantation indications Solid organ transplantation Prevention of graft rejection following solid organ transplantation. Treatment of transplant cellular rejection in patients previously receiving other immunosuppressive agents.
35

Bone marrow transplantation Prevention of graft rejection following allogeneic bone marrow and stem cell transplantation. Prevention or treatment of graft-versus-host disease (GVHD). Non-transplantation indications Endogenous uveitis Treatment of sight-threatening intermediate or posterior uveitis of non-infectious aetiology in patients in whom conventional therapy has failed or caused unacceptable side effects. Treatment of Behçet uveitis with repeated inflammatory attacks involving the retina in patients without neurological manifestations. Nephrotic syndrome Steroid-dependent and steroid-resistant nephrotic syndrome, due to primary glomerular diseases such as minimal change nephropathy, focal and segmental glomerulosclerosis, or membranous glomerulonephritis. Sandimmun Neoral can be used to induce and maintain remissions. It can also be used to maintain steroid-induced remission, allowing withdrawal of steroids. Rheumatoid arthritis Treatment of severe, active rheumatoid arthritis. Psoriasis Treatment of severe psoriasis in patients in whom conventional therapy is inappropriate or ineffective. Atopic dermatitis Sandimmun Neoral is indicated in patients with severe atopic dermatitis when systemic therapy is required. 4.2 Posology and method of administration Posology The dose ranges given for oral administration are intended to serve as guidelines only. The daily doses of Sandimmun Neoral should be given in two divided doses equally distributed throughout the day. It is recommended that Sandimmun Neoral be administered on a consistent schedule with regard to time of day and in relation to meals. Sandimmun Neoral should only be prescribed by, or in close collaboration with, a physician with experience of immunosuppressive therapy and/or organ transplantation. Transplantation Solid organ transplantation Treatment with Sandimmun Neoral should be initiated within 12 hours before surgery at a dose of 10 to 15 mg/kg given in 2 divided doses. This dose should be maintained as the daily dose for 1 to 2 weeks post-operatively, being gradually reduced in accordance with blood levels according to local immunosuppressive protocols until a recommended maintenance dose of about 2 to 6 mg/kg given in 2 divided doses is reached. When Sandimmun Neoral is given with other immunosuppressants (e.g. with corticosteroids or as part of a triple or quadruple medicinal product therapy), lower doses (e.g. 3 to 6 mg/kg given in 2 divided doses for the initial treatment) may be used.
36

Bone marrow transplantation The initial dose should be given on the day before transplantation. In most cases, Sandimmun concentrate for solution for infusion is preferred for this purpose. The recommended intravenous dose is 3 to 5 mg/kg/day. Infusion is continued at this dose level during the immediate post-transplant period of up to 2 weeks, before a change is made to oral maintenance therapy with Sandimmun Neoral at daily doses of about 12.5 mg/kg given in 2 divided doses. Maintenance treatment should be continued for at least 3 months (and preferably for 6 months) before the dose is gradually decreased to zero by 1 year after transplantation. If Sandimmun Neoral is used to initiate therapy, the recommended daily dose is 12.5 to 15 mg/kg given in 2 divided doses, starting on the day before transplantation. Higher doses of Sandimmun Neoral, or the use of Sandimmun intravenous therapy, may be necessary in the presence of gastrointestinal disturbances which might decrease absorption. In some patients, GVHD occurs after discontinuation of ciclosporin treatment, but usually responds favourably to re-introduction of therapy. In such cases an initial oral loading dose of 10 to 12.5 mg/kg should be given, followed by daily oral administration of the maintenance dose previously found to be satisfactory. Low doses of Sandimmun Neoral should be used to treat mild, chronic GVHD. Non-transplantation indications When using Sandimmun Neoral in any of the established non-transplantation indications, the following general rules should be adhered to: Before initiation of treatment a reliable baseline level of renal function should be established by at least two measurements. The estimated glomerular filtration rate (eGFR) by the MDRD formula can be used for estimation of renal function in adults and an appropriate formula should be used to assess eGFR in paediatric patients. Since Sandimmun Neoral can impair renal function, it is necessary to assess renal function frequently. If eGFR decreases by more than 25% below baseline at more than one measurement, the dosage of Sandimmun Neoral should be reduced by 25 to 50%. If the eGFR decrease from baseline exceeds 35%, further reduction of the dose of Sandimmun Neoral should be considered. These recommendations apply even if the patient`s values still lie within the laboratory`s normal range. If dose reduction is not successful in improving eGFR within one month, Sandimmun Neoral treatment should be discontinued (see section 4.4). Regular monitoring of blood pressure is required. The determination of bilirubin and parameters that assess hepatic function are required prior to starting therapy and close monitoring during treatment is recommended. Determinations of serum lipids, potassium, magnesium and uric acid are advisable before treatment and periodically during treatment. Occasional monitoring of ciclosporin blood levels may be relevant in non-transplant indications, e.g. when Sandimmun Neoral is co-administered with substances that may interfere with the pharmacokinetics of ciclosporin, or in the event of unusual clinical response (e.g. lack of efficacy or increased drug intolerance such as renal dysfunction). The normal route of administration is by mouth. If the concentrate for solution for infusion is used, careful consideration should be given to administering an adequate intravenous dose that corresponds to the oral dose. Consultation with a physician with experience of use of ciclosporin is recommended. Except in patients with sight-threatening endogenous uveitis and in children with nephrotic syndrome, the total daily dose must never exceed 5 mg/kg.
37

For maintenance treatment the lowest effective and well tolerated dosage should be determined individually. In patients in whom within a given time (for specific information see below) no adequate response is achieved or the effective dose is not compatible with the established safety guidelines, treatment with Sandimmun Neoral should be discontinued. Endogenous uveitis For inducing remission, initially 5 mg/kg/day orally given in 2 divided doses are recommended until remission of active uveal inflammation and improvement in visual acuity are achieved. In refractory cases, the dose can be increased to 7 mg/kg/day for a limited period. To achieve initial remission, or to counteract inflammatory ocular attacks, systemic corticosteroid treatment with daily doses of 0.2 to 0.6 mg/kg prednisone or an equivalent may be added if Sandimmun Neoral alone does not control the situation sufficiently. After 3 months, the dose of corticosteroids may be tapered to the lowest effective dose. For maintenance treatment, the dose should be slowly reduced to the lowest effective level. During the remission phases, this should not exceed 5 mg/kg/day. Infectious causes of uveitis should be ruled out before immunosuppressants can be used. Nephrotic syndrome For inducing remission, the recommended daily dose is given in 2 divided oral doses. If the renal function (except for proteinuria) is normal, the recommended daily dose is the following: - adults: 5 mg/kg - children: 6 mg/kg In patients with impaired renal function, the initial dose should not exceed 2.5 mg/kg/day. The combination of Sandimmun Neoral with low doses of oral corticosteroids is recommended if the effect of Sandimmun Neoral alone is not satisfactory, especially in steroid-resistant patients. Time to improvement varies from 3 to 6 months depending on the type of glomerulopathy. If no improvement has been observed after this time to improvement period, Sandimmun Neoral therapy should be discontinued. The doses need to be adjusted individually according to efficacy (proteinuria) and safety, but should not exceed 5 mg/kg/day in adults and 6 mg/kg/day in children. For maintenance treatment, the dose should be slowly reduced to the lowest effective level. Rheumatoid arthritis For the first 6 weeks of treatment the recommended dose is 3 mg/kg/day orally given in 2 divided doses. If the effect is insufficient, the daily dose may then be increased gradually as tolerability permits, but should not exceed 5 mg/kg. To achieve full effectiveness, up to 12 weeks of Sandimmun Neoral therapy may be required. For maintenance treatment the dose has to be titrated individually to the lowest effective level according to tolerability. Sandimmun Neoral can be given in combination with low-dose corticosteroids and/or non-steroidal anti-inflammatory drugs (NSAIDs) (see section 4.4). Sandimmun Neoral can also be combined with low-dose weekly methotrexate in patients who have insufficient response to methotrexate alone, by
38

using 2.5 mg/kg Sandimmun Neoral in 2 divided doses per day initially, with the option to increase the dose as tolerability permits. Psoriasis Sandimmun Neoral treatment should be initiated by physicians with experience in the diagnosis and treatment of psoriasis. Due to the variability of this condition, treatment must be individualised. For inducing remission, the recommended initial dose is 2.5 mg/kg/day orally given in 2 divided doses. If there is no improvement after 1 month, the daily dose may be gradually increased, but should not exceed 5 mg/kg. Treatment should be discontinued in patients in whom sufficient response of psoriatic lesions cannot be achieved within 6 weeks on 5 mg/kg/day, or in whom the effective dose is not compatible with the established safety guidelines (see section 4.4). Initial doses of 5 mg/kg/day are justified in patients whose condition requires rapid improvement. Once satisfactory response is achieved, Sandimmun Neoral may be discontinued and subsequent relapse managed with re-introduction of Sandimmun Neoral at the previous effective dose. In some patients, continuous maintenance therapy may be necessary. For maintenance treatment, doses have to be titrated individually to the lowest effective level, and should not exceed 5 mg/kg/day. Atopic dermatitis Sandimmun Neoral treatment should be initiated by physicians with experience in the diagnosis and treatment of atopic dermatitis. Due to the variability of this condition, treatment must be individualised. The recommended dose range is 2.5 to 5 mg/kg/day given in 2 divided oral doses. If a starting dose of 2.5 mg/kg/day does not achieve a satisfactory response within 2 weeks, the daily dose may be rapidly increased to a maximum of 5 mg/kg. In very severe cases, rapid and adequate control of the disease is more likely to occur with a starting dose of 5 mg/kg/day. Once satisfactory response is achieved, the dose should be reduced gradually and, if possible, Sandimmun Neoral should be discontinued. Subsequent relapse may be managed with a further course of Sandimmun Neoral. Although an 8-week course of therapy may be sufficient to achieve clearing, up to 1 year of therapy has been shown to be effective and well tolerated, provided the monitoring guidelines are followed. Switching from Sandimmun to Sandimmun Neoral The available data indicate that after a 1:1 switch from Sandimmun to Sandimmun Neoral, the trough concentrations of ciclosporin in whole blood are comparable. In many patients, however, higher peak concentrations (Cmax) and increased exposure to the active substance (AUC) may occur. In a small percentage of patients these changes are more marked and may be of clinical significance. In addition, the absorption of ciclosporin from Sandimmun Neoral is less variable and the correlation between ciclosporin trough concentrations and exposure (in terms of AUC) is stronger than with Sandimmun. Since the switch from Sandimmun to Sandimmun Neoral may result in increased exposure to ciclosporin, the following rules must be observed: In transplant patients, Sandimmun Neoral should be started at the same daily dose as was previously used with Sandimmun. Ciclosporin trough concentrations in whole blood should be monitored initially within 4 to 7 days after the switch to Sandimmun Neoral. In addition, clinical safety parameters such as renal function and blood pressure must be monitored during the first 2 months after the switch. If the ciclosporin trough blood levels are beyond the therapeutic range, and/or worsening of the clinical safety parameters occurs, the dosage must be adjusted accordingly. In patients treated for non-transplantation indications, Sandimmun Neoral should be started with the same daily dose as was used with Sandimmun. Two, 4 and 8 weeks after the switch, renal function and blood pressure should be monitored. If blood pressure significantly exceed the pre-switch levels or if eGFR decreases by more than 25% below the value measured prior to Sandimmun therapy at more than one measurement, the dose should be reduced (see also ‘Additional precautions’ in section
39

4.4). In the event of unexpected toxicity or inefficacy of ciclosporin, blood trough levels should also be monitored. Switching between oral ciclosporin formulations The switch from one oral ciclosporin formulation to another should be made under physician supervision, including monitoring of blood levels of ciclosporin for transplantation patients. Special populations Patients with renal impairment All indications Ciclosporin undergoes minimal renal elimination and its pharmacokinetics are not extensively affected by renal impairment (see section 5.2). However, due to its nephrotoxic potential (see section 4.8), careful monitoring of renal function is recommended (see section 4.4). Non-transplantation indications With the exception of patients being treated for nephrotic syndrome, patients with impaired renal function should not receive ciclosporin (see subsection on additional precautions in non-transplantation indications in section 4.4). In nephrotic syndrome patients with impaired renal function, the initial dose should not exceed 2.5 mg/kg/day. Patients with hepatic impairment Ciclosporin is extensively metabolised by the liver. An approximate 2- to 3-fold increase in ciclosporin exposure may be observed in patients with hepatic impairment. Dose reduction may be necessary in patients with severe liver impairment to maintain blood levels within the recommended target range (see sections 4.4 and 5.2) and it is recommended that ciclosporin blood levels are monitored until stable levels are reached. Paediatric population Clinical studies have included children from 1 year of age. In several studies, paediatric patients required and tolerated higher doses of ciclosporin per kg body weight than those used in adults. Use of Sandimmun Neoral in children for non-transplantation indications other than nephrotic syndrome cannot be recommended (see section 4.4). Elderly population (age 65 years and above) Experience with Sandimmun Neoral in the elderly is limited. In rheumatoid arthritis clinical trials with ciclosporin, patients aged 65 or older were more likely to develop systolic hypertension on therapy, and more likely to show serum creatinine rises ≥50% above the baseline after 3 to 4 months of therapy. Dose selection for an elderly patient should be cautious, usually starting at the low end of the dosing range, reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or medication and increased susceptibility for infections. Method of administration Oral use Sandimmun Neoral capsules should be swallowed whole. 4.3 Contraindications Hypersensitivity to the active substance or to any of the excipients listed in section 6.1. Combination with products containing Hypericum perforatum (St John´s Wort) (see section 4.5).
40

Combination with medicines that are substrates for the multidrug efflux transporter P-glycoprotein or the organic anion transporter proteins (OATP) and for which elevated plasma concentrations are associated with serious and/or life-threatening events, e.g. bosentan, dabigatran etexilate and aliskiren (see section 4.5). 4.4 Special warnings and precautions for use Medical supervision Sandimmun Neoral should be prescribed only by physicians who are experienced in immunosuppressive therapy and can provide adequate follow-up, including regular full physical examination, measurement of blood pressure and control of laboratory safety parameters. Transplantation patients receiving this medicinal product should be managed in facilities with adequate laboratory and supportive medical resources. The physician responsible for maintenance therapy should receive complete information for the follow-up of the patient. Lymphomas and other malignancies Like other immunosuppressants, ciclosporin increases the risk of developing lymphomas and other malignancies, particularly those of the skin. The increased risk appears to be related to the degree and duration of immunosuppression rather than to the use of specific agents. A treatment regimen containing multiple immunosuppressants (including ciclosporin) should therefore be used with caution as this could lead to lymphoproliferative disorders and solid organ tumours, some with reported fatalities. In view of the potential risk of skin malignancy, patients on Sandimmun Neoral, in particular those treated for psoriasis or atopic dermatitis, should be warned to avoid excess unprotected sun exposure and should not receive concomitant ultraviolet B irradiation or PUVA photochemotherapy. Infections Like other immunosuppressants, ciclosporin predisposes patients to the development of a variety of bacterial, fungal, parasitic and viral infections, often with opportunistic pathogens. Activation of latent polyomavirus infections that may lead to polyomavirus associated nephropathy (PVAN), especially to BK virus nephropathy (BKVN), or to JC virus associated progressive multifocal leukoencephalopathy (PML), have been observed in patients receiving ciclosporin. These conditions are often related to a high total immunosuppressive burden and should be considered in the differential diagnosis in immunosuppressed patients with deteriorating renal function or neurological symptoms. Serious and/or fatal outcomes have been reported. Effective pre-emptive and therapeutic strategies should be employed, particularly in patients on multiple long-term immunosuppressive therapy. Renal toxicity A frequent and potentially serious complication, an increase in serum creatinine and urea, may occur during Sandimmun Neoral therapy. These functional changes are dose-dependent and are initially reversible, usually responding to dose reduction. During long-term treatment, some patients may develop structural changes in the kidney (e.g. interstitial fibrosis) which, in renal transplant patients, must be differentiated from changes due to chronic rejection. Frequent monitoring of renal function is therefore required according to local guidelines for the indication in question (see sections 4.2 and 4.8). Hepatotoxicity Sandimmun Neoral may also cause dose-dependent, reversible increases in serum bilirubin and in liver enzymes (see section 4.8). There have been solicited and spontaneous reports of hepatotoxicity and liver injury including cholestasis, jaundice, hepatitis and liver failure in patients treated with ciclosporin. Most reports included patients with significant co-morbidities, underlying conditions and other confounding factors including infectious complications and co-medications with hepatotoxic potential. In some cases, mainly in transplant patients, fatal outcomes have been reported (see section
41

4.8). Close monitoring of parameters that assess hepatic function is required and abnormal values may necessitate dose reduction (see sections 4.2 and 5.2). Elderly population (age 65 years and above) In elderly patients, renal function should be monitored with particular care. Monitoring ciclosporin levels (see section 4.2) When Sandimmun Neoral is used in transplant patients, routine monitoring of ciclosporin blood levels is an important safety measure. For monitoring ciclosporin levels in whole blood, a specific monoclonal antibody (measurement of parent compound) is preferred; a high-performance liquid chromatography (HPLC) method, which also measures the parent compound, can be used as well. If plasma or serum is used, a standard separation protocol (time and temperature) should be followed. For the initial monitoring of liver transplant patients, either the specific monoclonal antibody should be used, or parallel measurements using both the specific monoclonal antibody and the non-specific monoclonal antibody should be performed, to ensure a dosage that provides adequate immunosuppression. In non-transplant patients, occasional monitoring of ciclosporin blood levels is recommended, e.g. when Sandimmun Neoral is co-administered with substances that may interfere with the pharmacokinetics of ciclosporin, or in the event of unusual clinical response (e.g. lack of efficacy or increased drug intolerance such as renal dysfunction). It must be remembered that the ciclosporin concentration in blood, plasma, or serum is only one of many factors contributing to the clinical status of the patient. Results should therefore serve only as a guide to dosage in relationship to other clinical and laboratory parameters. Hypertension Regular monitoring of blood pressure is required during Sandimmun Neoral therapy. If hypertension develops, appropriate antihypertensive treatment must be instituted. Preference should be given to an antihypertensive agent that does not interfere with the pharmacokinetics of ciclosporin, e.g. isradipine (see section 4.5). Blood lipids increased Since Sandimmun Neoral has been reported to induce a reversible slight increase in blood lipids, it is advisable to perform lipid determinations before treatment and after the first month of therapy. In the event of increased lipids being found, restriction of dietary fat and, if appropriate, a dose reduction, should be considered. Hyperkalaemia Ciclosporin enhances the risk of hyperkalaemia, especially in patients with renal dysfunction. Caution is also required when ciclosporin is co-administered with potassium-sparing drugs (e.g. potassium-sparing diuretics, angiotensin converting enzyme (ACE) inhibitors, angiotensin II receptor antagonists) or potassium-containing medicinal products as well as in patients on a potassium rich diet. Control of potassium levels in these situations is advisable. Hypomagnesaemia Ciclosporin enhances the clearance of magnesium. This can lead to symptomatic hypomagnesaemia, especially in the peri-transplant period. Control of serum magnesium levels is therefore recommended in the peri-transplant period, particularly in the presence of neurological symptom/signs. If considered necessary, magnesium supplementation should be given. Hyperuricaemia Caution is required when treating patients with hyperuricaemia. Live-attenuated vaccines During treatment with ciclosporin, vaccination may be less effective. The use of live attenuated vaccines should be avoided (see section 4.5).
42

Interactions Caution should be observed when co-administering ciclosporin with drugs that substantially increase or decrease ciclosporin plasma concentrations, through inhibition or induction of CYP3A4 and/or P-glycoprotein (see section 4.5). Renal toxicity should be monitored when initiating ciclosporin use together with active substances that increase ciclosporin levels or with substances that exhibit nephrotoxic synergy (see section 4.5). Concomitant use of ciclosporin and tacrolimus should be avoided (see section 4.5). Ciclosporin is an inhibitor of CYP3A4, the multidrug efflux transporter P-glycoprotein and organic anion transporter proteins (OATP) and may increase plasma levels of co-medications that are substrates of this enzyme and/or transporter. Caution should be observed while co-administering ciclosporin with such drugs or concomitant use should be avoided (see section 4.5). Ciclosporin increases the exposure to HMG-CoA reductase inhibitors (statins). When concurrently administered with ciclosporin, the dosage of the statins should be reduced and concomitant use of certain statins should be avoided according to their label recommendations. Statin therapy needs to be temporarily withheld or discontinued in patients with signs and symptoms of myopathy or those with risk factors predisposing to severe renal injury, including renal failure, secondary to rhabdomyolysis (see section 4.5). Following concomitant administration of ciclosporin and lercanidipine, the AUC of lercanidipine was increased three-fold and the AUC of ciclosporin was increased 21%. Therefore the simultaneous combination of ciclosporin and lercanidipine should be avoided. Administration of ciclosporin 3 hours after lercanidipine yielded no change of the lercanidipine AUC, but the ciclosporin AUC was increased by 27%. This combination should therefore be given with caution with an interval of at least 3 hours. Special excipients: Polyoxyl 40 hydrogenated castor oil Sandimmun Neoral contains polyoxyl 40 hydrogenated castor oil, which may cause stomach upsets and diarrhoea. Special excipients: Ethanol Sandimmun Neoral contains around 12% vol. ethanol. A 500 mg dose of Sandimmun Neoral contains 500 mg ethanol, equivalent to nearly 15 ml beer or 5 ml wine. This may be harmful in alcoholic patients and should be taken into account in pregnant or breast-feeding women, in patients presenting with liver disease or epilepsy, or if the patients is a child. Additional precautions in non-transplantation indications Patients with impaired renal function (except nephrotic syndrome patients with a permissible degree of renal impairment), uncontrolled hypertension, uncontrolled infections, or any kind of malignancy should not receive ciclosporin. Before initiation of treatment a reliable baseline assessment of renal function should be established by at least two measurements of eGFR. Renal function must be assessed frequently throughout therapy to allow dosage adjustment (see section 4.2). Additional precautions in endogenous uveitis Sandimmun Neoral should be administered with caution in patients with neurological Behcet`s syndrome. The neurological status of these patients should be carefully monitored. There is only limited experience with the use of Sandimmun Neoral in children with endogenous uveitis. Additional precautions in nephrotic syndrome
43

Patients with abnormal baseline renal function should initially be treated with 2.5 mg/kg/day and must be monitored very carefully. In some patients, it may be difficult to detect Sandimmun Neoral-induced renal dysfunction because of changes in renal function related to the nephrotic syndrome itself. This explains why, in rare cases, Sandimmun Neoral-associated structural kidney alterations have been observed without increases in serum creatinine. Renal biopsy should be considered for patients with steroid-dependent minimal-change nephropathy, in whom Sandimmun Neoral therapy has been maintained for more than 1 year. In patients with nephrotic syndrome treated with immunosuppressants (including ciclosporin), the occurrence of malignancies (including Hodgkin's lymphoma) has occasionally been reported. Additional precautions in rheumatoid arthritis After 6 months of therapy, renal function needs to be assessed every 4 to 8 weeks depending on the stability of the disease, its co- medication, and concomitant diseases. More frequent checks are necessary when the Sandimmun Neoral dose is increased, or concomitant treatment with an NSAID is initiated or its dosage increased. Discontinuation of Sandimmun Neoral may also become necessary if hypertension developing during treatment cannot be controlled by appropriate therapy. As with other long-term immunosuppressive treatments, an increased risk of lymphoproliferative disorders must be borne in mind. Special caution should be observed if Sandimmun Neoral is used in combination with methotrexate due to nephrotoxic synergy. Additional precautions in psoriasis Discontinuation of Sandimmun Neoral therapy is recommended if hypertension developing during treatment cannot be controlled with appropriate therapy. Elderly patients should be treated only in the presence of disabling psoriasis, and renal function should be monitored with particular care. There is only limited experience with the use of Sandimmun Neoral in children with psoriasis. In psoriatic patients on ciclosporin, as in those on conventional immunosuppressive therapy, development of malignancies (in particular of the skin) has been reported. Skin lesions not typical for psoriasis, but suspected to be malignant or pre-malignant should be biopsied before Sandimmun Neoral treatment is started. Patients with malignant or pre-malignant alterations of the skin should be treated with Sandimmun Neoral only after appropriate treatment of such lesions, and if no other option for successful therapy exists. In a few psoriatic patients treated with Sandimmun Neoral, lymphoproliferative disorders have occurred. These were responsive to prompt discontinuation. Patients on Sandimmun Neoral should not receive concomitant ultraviolet B irradiation or PUVA photochemotherapy. Additional precautions in atopic dermatitis Discontinuation of Sandimmun Neoral is recommended if hypertension developing during treatment cannot be controlled with appropriate therapy. Experience with Sandimmun Neoral in children with atopic dermatitis is limited. Elderly patients should be treated only in the presence of disabling atopic dermatitis and renal function should be monitored with particular care. Benign lymphadenopathy is commonly associated with flares in atopic dermatitis and invariably disappears spontaneously or with general improvement in the disease.
44
Lymphadenopathy observed on treatment with ciclosporin should be regularly monitored. Lymphadenopathy which persists despite improvement in disease activity should be examined by biopsy as a precautionary measure to ensure the absence of lymphoma. Active herpes simplex infections should be allowed to clear before treatment with Sandimmun Neoral is initiated, but are not necessarily a reason for treatment withdrawal if they occur during therapy unless infection is severe. Skin infections with Staphylococcus aureus are not an absolute contraindication for Sandimmun Neoral therapy, but should be controlled with appropriate antibacterial agents. Oral erythromycin, which is known to have the potential to increase the blood concentration of ciclosporin (see section 4.5), should be avoided. If there is no alternative, it is recommended to closely monitor blood levels of ciclosporin, renal function, and for side effects of ciclosporin. Patients on Sandimmun Neoral should not receive concomitant ultraviolet B irradiation or PUVA photochemotherapy. Paediatric use in non-transplantation indications Except for the treatment of nephrotic syndrome, there is no adequate experience available with Sandimmun Neoral. Its use in children under 16 years of age for non-transplantation indications other than nephrotic syndrome cannot be recommended. 4.5 Interaction with other medicinal products and other forms of interaction Drug interactions Of the many drugs reported to interact with ciclosporin, those for which the interactions are adequately substantiated and considered to have clinical implications are listed below. Various agents are known to either increase or decrease plasma or whole blood ciclosporin levels usually by inhibition or induction of enzymes involved in the metabolism of ciclosporin, in particular CYP3A4. Ciclosporin is also an inhibitor of CYP3A4, the multidrug efflux transporter P-glycoprotein and organic anion transporter proteins (OATP) and may increase plasma levels of co-medications that are substrates of this enzyme and/or transporters. Medicinal products known to reduce or increase the bioavailability of ciclosporin: In transplant patients frequent measurement of ciclosporin levels and, if necessary, ciclosporin dosage adjustment is required, particularly during the introduction or withdrawal of the co-administered medication. In non-transplant patients the relationship between blood level and clinical effects is less well established. If medicinal products known to increase ciclosporin levels are given concomitantly, frequent assessment of renal function and careful monitoring for ciclosporin-related side effects may be more appropriate than blood level measurement. Drugs that decrease ciclosporin levels All inducers of CYP3A4 and/or P-glycoprotein are expected to decrease ciclosporin levels. Examples of drugs that decrease ciclosporin levels are: Barbiturates, carbamazepine, oxcarbazepine, phenytoin; nafcillin, intravenous sulfadimidine, probucol, orlistat, hypericum perforatum (St. John’s wort), ticlopidine, sulfinpyrazone, terbinafine, bosentan. Products containing Hypericum perforatum (St John´s Wort) must not be used concomitantly with Sandimmun Neoral due to the risk of decreased blood levels of ciclosporin and thereby reduced effect (see section 4.3).
45

Rifampicin induces ciclosporin intestinal and liver metabolism. Ciclosporin doses may need to be increased 3- to 5-fold during co-administration. Octreotide decreases oral absorption of ciclosporin and a 50% increase in the ciclosporin dose or a switch to intravenous administration could be necessary. Drugs that increase ciclosporin levels All inhibitors of CYP3A4 and/or P-glycoprotein may lead to increased levels of cyclosporine. Examples are: Nicardipine, metoclopramide, oral contraceptives, methylprednisolone (high dose), allopurinol, cholic acid and derivatives, protease inhibitors, imatinib, colchicine, nefazodone. Macrolide antibiotics: Erythromycin can increase ciclosporin exposure 4- to 7-fold, sometimes resulting in nephrotoxicity. Clarithromycin has been reported to double the exposure of ciclosporin. Azitromycin increases ciclosporin levels by around 20%. Azole antibiotics: Ketoconazole, fluconazole, itraconazole and voriconazole could more than double ciclosporin exposure. Verapamil increases ciclosporin blood concentrations 2- to 3-fold. Co-administration with telaprevir resulted in approximately 4.64-fold increase in ciclosporin dose normalised exposure (AUC). Amiodarone substantially increases the plasma ciclosporin concentration concurrently with an increase in serum creatinine. This interaction can occur for a long time after withdrawal of amiodarone, due to its very long half-life (about 50 days). Danazol has been reported to increase ciclosporin blood concentrations by approximately 50%. Diltiazem (at doses of 90 mg/day) can increase ciclosporin plasma concentrations by up to 50%. Imatinib could increase ciclosporin exposure and Cmax by around 20%. Food interactions The concomitant intake of grapefruit and grapefruit juice has been reported to increase the bioavailability of ciclosporin. Combinations with increased risk for nephrotoxicity Care should be taken when using ciclosporin together with other active substances that exhibit nephrotoxic synergy such as: aminoglycosides (including gentamycin, tobramycin), amphotericin B, ciprofloxacin, vancomycin, trimethoprim (+ sulfamethoxazole); fibric acid derivatives (e.g. bezafibrate, fenofibrate); NSAIDs (including diclofenac, naproxen, sulindac); melphalan histamine H2-receptor antagonists (e.g. cimetidine, ranitidine); methotrexate (see section 4.4). During the concomitant use of a drug that may exhibit nephrotoxic synergy, close monitoring of renal function should be performed. If a significant impairment of renal function occurs, the dosage of the co-administered medicinal product should be reduced or alternative treatment considered. Concomitant use of ciclosporin and tacrolimus should be avoided due to the risk for nephrotoxicity and pharmacokinetic interaction via CYP3A4 and/or P-gp (see section 4.4). Effects of ciclosporin on other drugs Ciclosporin is an inhibitor of CYP3A4, the multidrug efflux transporter P-glycoprotein (P-gp) and organic anion transporter proteins (OATP). Co-administration of drugs that are substrates of
46

CYP3A4, P-gp and OATP with ciclosporin may increase plasma levels of co-medications that are substrates of this enzyme and/or transporter. Some examples are listed below: Ciclosporin may reduce the clearance of digoxin, colchicine, HMG-CoA reductase inhibitors (statins) and etoposide. If any of these drugs are used concurrently with ciclosporin, close clinical observation is required in order to enable early detection of toxic manifestations of the medicinal products, followed by reduction of its dosage or its withdrawal. When concurrently administered with ciclosporin, the dosage of the statins should be reduced and concomitant use of certain statins should be avoided according to their label recommendations. Exposure changes of commonly used statins with ciclosporin are summarised in Table 1. Statin therapy needs to be temporarily withheld or discontinued in patients with signs and symptoms of myopathy or those with risk factors predisposing to severe renal injury, including renal failure, secondary to rhabdomyolysis. Table 1 Summary of exposure changes of commonly used statins with ciclosporin
Statin Doses available Fold change in
exposure with ciclosporin
Atorvastatin 10-80 mg 8-10 Simvastatin 10-80 mg 6-8 Fluvastatin 20-80 mg 2-4 Lovastatin 20-40 mg 5-8 Pravastatin 20-80 mg 5-10 Rosuvastatin 5-40 mg 5-10 Pitavastatin 1-4 mg 4-6
Caution is recommended when co-administering ciclosporin with lercanidipine (see section 4.4). Following concomitant administration of ciclosporin and aliskiren, a P-gp substrate, the Cmax of aliskiren was increased approximately 2.5-fold and the AUC approximately 5-fold. However, the pharmacokinetic profile of ciclosporin was not significantly altered. Co-administration of ciclosporin and aliskiren is not recommended (see section 4.3). Concomitant administration of dabigatran etexilate is not recommended due to the P-gp inhibitory activity of ciclosporin (see section 4.3). The concurrent administration of nifedipine with ciclosporin may result in an increased rate of gingival hyperplasia compared with that observed when ciclosporin is given alone. The concomitant use of diclofenac and ciclosporin has been found to result in a significant increase in the bioavailability of diclofenac, with the possible consequence of reversible renal function impairment. The increase in the bioavailability of diclofenac is most probably caused by a reduction of its high first-pass effect. If NSAIDs with a low first-pass effect (e.g. acetylsalicylic acid) are given together with ciclosporin, no increase in their bioavailability is to be expected. Elevations in serum creatinine were observed in the studies using everolimus or sirolimus in combination with full-dose ciclosporin for microemulsion. This effect is often reversible with ciclosporin dose reduction. Everolimus and sirolimus had only a minor influence on ciclosporin pharmacokinetics. Co-administration of ciclosporin significantly increases blood levels of everolimus and sirolimus. Caution is required with concomitant use of potassium-sparing medicinal products (e.g. potassium-sparing diuretics, ACE inhibitors, angiotensin II receptor antagonists) or potassium-containing medicinal products since they may lead to significant increases in serum potassium (see section 4.4).
47

Ciclosporin may increase the plasma concentrations of repaglinide and thereby increase the risk of hypoglycaemia. Co-administration of bosentan and ciclosporin in healthy volunteers increases the bosentan exposure several-fold and there was a 35% decrease in ciclosporin exposure. Co-administration of ciclosporin with bosentan is not recommended (see above subsection “Drugs that decrease ciclosporin levels” and section 4.3). Multiple dose administration of ambrisentan and ciclosporin in healthy volunteers resulted in an approximately 2-fold increase in ambrisentan exposure, while the ciclosporin exposure was marginally increased (approximately 10%). A significantly increased exposure to anthracycline antibiotics (e.g. doxorubicine, mitoxanthrone, daunorubicine) was observed in oncology patients with the intravenous co-administration of anthracycline antibiotics and very high doses of ciclosporin. During treatment with ciclosporin, vaccination may be less effective and the use of live attenuated vaccines should be avoided. Paediatric population Interaction studies have only been performed in adults. 4.6 Fertility, pregnancy and lactation Pregnancy Animal studies have shown reproductive toxicity in rats and rabbits. Experience with Sandimmun Neoral in pregnant women is limited. Pregnant women receiving immunosuppressive therapies after transplantation, including ciclosporin and ciclosporin-containing regimens, are at risk of premature delivery (<37 weeks). A limited number of observations in children exposed to ciclosporin in utero are available, up to an age of approximately 7 years. Renal function and blood pressure in these children were normal. However, there are no adequate and well-controlled studies in pregnant women and therefore Sandimmun Neoral should not be used during pregnancy unless the potential benefit to the mother justifies the potential risk to the foetus. The ethanol content of the Sandimmun Neoral formulations should also be taken into account in pregnant women (see section 4.4). Breast-feeding Ciclosporin passes into breast milk. The ethanol content of the Sandimmun Neoral formulations should also be taken into account in women who are breast-feeding (see section 4.4). Mothers receiving treatment with Sandimmun Neoral should not breast-feed because of the potential of Sandimmun Neoral to cause serious adverse drug reactions in breast-fed newborns/infants. A decision should be made whether to abstain from breast-feeding or to abstain from using the medicinal drug, taking into account the importance of the medicinal product to the mother. Fertility There is limited data on the effect of Sandimmun Neoral on human fertility (see section 5.3). 4.7 Effects on ability to drive and use machines No data exist on the effects of Sandimmun Neoral on the ability to drive and use machines.
48

4.8 Undesirable effects
Summary of the safety profile The principal adverse reactions observed in clinical trials and associated with the administration of ciclosporin include renal dysfunction, tremor, hirsutism, hypertension, diarrhoea, anorexia, nausea and vomiting. Many side effects associated with ciclosporin therapy are dose-dependent and responsive to dose reduction. In the various indications the overall spectrum of side effects is essentially the same; there are, however, differences in incidence and severity. As a consequence of the higher initial doses and longer maintenance therapy required after transplantation, side effects are more frequent and usually more severe in transplant patients than in patients treated for other indications. Anaphylactoid reactions have been observed following intravenous administration (see section 4.4). Infections and infestations Patients receiving immunosuppressive therapies, including ciclosporin and ciclosporin-containing regimens, are at increased risk of infections (viral, bacterial, fungal, parasitic) (see section 4.4). Both generalised and localised infections can occur. Pre-existing infections may also be aggravated and reactivation of polyomavirus infections may lead to polyomavirus-associated nephropathy (PVAN) or to JC virus associated progressive multifocal leukopathy (PML). Serious and/or fatal outcomes have been reported. Neoplasms benign, malignant and unspecified (including cysts and polyps) Patients receiving immunosuppressive therapies, including ciclosporin and ciclosporin containing regimens, are at increased risk of developing lymphomas or lymphoproliferative disorders and other malignancies, particularly of the skin. The frequency of malignancies increases with the intensity and duration of therapy (see section 4.4). Some malignancies may be fatal. Tabulated summary of adverse drug reactions from clinical trials Adverse drug reactions from clinical trials (Table 1) are listed by MedDRA system organ class. Within each system organ class, the adverse drug reactions are ranked by frequency, with the most frequent reactions first. Within each frequency grouping, adverse drug reactions are presented in order of decreasing seriousness. In addition the corresponding frequency category for each adverse drug reaction is based on the following convention (CIOMS III): very common (≥1/10); common (≥1/100, <1/10); uncommon (≥1/1,000, <1/100); rare (≥1/10,000, <1/1,000) very rare (<1/10,000), not known (cannot be estimated from the available data). Table 1: Adverse drug reactions from clinical trials Blood and lymphatic system disorders Common Leucopenia Uncommon Thrombocytopenia, anaemia Rare Haemolytic uraemic syndrome, microangiopathic haemolytic anaemia Not known* Thrombotic microangiopathy, thrombotic thrombocytopenic purpura Metabolism and nutrition disorders Very common Hyperlipidaemia Common Hyperglycaemia, anorexia, hyperuricaemia, hyperkalaemia, hypomagnesaemia Nervous system disorders Very common Tremor, headache Common Convulsions, paraesthesia
49

Uncommon Encephalopathy including Posterior Reversible Encephalopathy Syndrome (PRES), signs and symptoms such as convulsions, confusion, disorientation, decreased responsiveness, agitation, insomnia, visual disturbances, cortical blindness, coma, paresis and cerebellar ataxia
Rare Motor polyneuropathy Very rare Optic disc oedema, including papilloedema, with possible visual impairment
secondary to benign intracranial hypertension Not known* Migraine Vascular disorders Very common Hypertension Common Flushing Gastrointestinal disorders Common Nausea, vomiting, abdominal discomfort/pain, diarrhoea, gingival hyperplasia,
peptic ulcer Rare Pancreatitis Hepatobiliary disorders Common Hepatic function abnormal (see section 4.4) Not known* Hepatotoxicity and liver injury including cholestasis, jaundice, hepatitis and
liver failure with some fatal outcome (see section 4.4) Skin and subcutaneous tissue disorders Very common Hirsutism Common Acne, hypertrichosis Uncommon Allergic rashes Musculoskeletal and connective tissue disorders Common Myalgia, muscle cramps Rare Muscle weakness, myopathy Renal and urinary disorders Very common Renal dysfunction (see section 4.4) Reproductive system and breast disorders Rare Menstrual disturbances, gynaecomastia General disorders and administration site conditions Common Pyrexia, fatigue Uncommon Oedema, weight increase * Adverse events reported from post marketing experience where the ADR frequency is not known due to the lack of a real denominator. Other adverse drug reactions from post-marketing experience There have been solicited and spontaneous reports of hepatotoxicity and liver injury including cholestasis, jaundice hepatitis and liver failure in patients treated with ciclosporin. Most reports included patients with significant co-morbidities, underlying conditions and other confounding factors including infectious complications and co-medications with hepatotoxic potential. In some cases, mainly in transplant patients, fatal outcomes have been reported (see section 4.4). Acute and chronic nephrotoxicity Patients receiving calcineurin inhibitor (CNI) therapies, including ciclosporin and ciclosporin-containing regimens, are at increased risk of acute or chronic nephrotoxicity. There have been reports from clinical trials and from the post-marketing setting associated with the use of Sandimmun Neoral. Cases of acute nephrotoxicity reported disorders of ion homeostasis, such as hyperkalaemia, hypomagnesaemia, and hyperuricaemia. Cases reporting chronic morphological changes included arteriolar hyalinosis, tubular atrophy and interstitial fibrosis (see section 4.4). Paediatric population Clinical studies have included children from 1 year of age using standard ciclosporin dosage with a comparable safety profile to adults.
50

4.9 Overdose The oral LD50 of ciclosporin is 2,329 mg/kg in mice, 1,480 mg/kg in rats and > 1,000 mg/kg in rabbits. The intravenous LD50 is 148 mg/kg in mice, 104 mg/kg in rats, and 46 mg/kg in rabbits. Symptoms Experience with acute overdosage of ciclosporin is limited. Oral doses of ciclosporin of up to 10 g (about 150 mg/kg) have been tolerated with relatively minor clinical consequences, such as vomiting, drowsiness, headache, tachycardia and in a few patients moderately severe, reversible impairment of renal function. However, serious symptoms of intoxication have been reported following accidental parenteral overdosage with ciclosporin in premature neonates. Treatment In all cases of overdosage, general supportive measures should be followed and symptomatic treatment applied. Forced emesis and gastric lavage may be of value within the first few hours after oral intake. Ciclosporin is not dialysable to any great extent, nor is it well cleared by charcoal haemoperfusion. 5. PHARMACOLOGICAL PROPERTIES 5.1 Pharmacodynamic properties Pharmacotherapeutic group: Immunosuppressive agents, calcineurin inhibitors, ATC code: L04AD01 Ciclosporin (also known as ciclosporin A) is a cyclic polypeptide consisting of 11 amino acids. It is a potent immunosuppressive agent, which in animals prolongs survival of allogeneic transplants of skin, heart, kidney, pancreas, bone marrow, small intestine or lung. Studies suggest that ciclosporin inhibits the development of cell-mediated reactions, including allograft immunity, delayed cutaneous hypersensitivity, experimental allergic encephalomyelitis, Freund's adjuvant arthritis, graft-versus-host disease (GVHD), and also T-cell dependent antibody production. At the cellular level it inhibits production and release of lymphokines including interleukin 2 (T-cell growth factor, TCGF). Ciclosporin appears to block the resting lymphocytes in the G0 or G1 phase of the cell cycle, and inhibits the antigen-triggered release of lymphokines by activated T-cells. All available evidence suggests that ciclosporin acts specifically and reversibly on lymphocytes. Unlike cytostatic agents, it does not depress haemopoiesis and has no effect on the function of phagocytic cells. Successful solid organ and bone marrow transplantations have been performed in man using ciclosporin to prevent and treat rejection and GVHD. Ciclosporin has been used successfully both in hepatitis C virus (HCV) positive and HCV negative liver transplants recipients. Beneficial effects of ciclosporin therapy have also been shown in a variety of conditions that are known, or may be considered to be of autoimmune origin. Paediatric population: Ciclosporin has been shown to be efficacious in steroid-dependent nephrotic syndrome. 5.2 Pharmacokinetic properties Absorption Following oral administration of Sandimmun Neoral peak blood concentrations of ciclosporin are reached within 1-2 hours. The absolute oral bioavailability of ciclosporin following administration of Sandimmun Neoral is 20 to 50%. About 13 and 33% decrease in AUC and Cmax was observed when Sandimmun Neoral was administered with a high-fat meal. The relationship between administered dose and exposure (AUC) of ciclosporin is linear within the therapeutic dose range. The intersubject
51

and intrasubject variability for AUC and Cmax is approximately 10-20%. Sandimmun Neoral solution and soft gelatin capsules are bioequivalent. Sandimmun Neoral administration results in a 59% higher Cmax and approximately 29% higher bioavailability than Sandimmun. The available data indicate that following a 1:1 switch from Sandimmun soft gelatin capsules to Sandimmun Neoral soft gelatin capsules trough concentrations in whole blood are comparable and remain in the desired therapeutic range. Sandimmun Neoral administration improves dose linearity in ciclosporin exposure (AUCB). It provides a more consistent absorption profile with less influence from concomitant food intake or from diurnal rhythm than Sandimmun. Distribution Ciclosporin is distributed largely outside the blood volume, with an average apparent distribution volume of 3.5 l/kg. In the blood, 33 to 47% is present in plasma, 4 to 9% in lymphocytes, 5 to 12% in granulocytes, and 41 to 58% in erythrocytes. In plasma, approximately 90% is bound to proteins, mostly lipoproteins. Biotransformation Ciclosporin is extensively metabolised to approximately 15 metabolites. Metabolism mainly takes place in the liver via cytochrome P450 3A4 (CYP3A4), and the main pathways of metabolism consist of mono- and dihydroxylation and N-demethylation at various positions of the molecule. All metabolites identified so far contain the intact peptide structure of the parent compound; some possess weak immunosuppressive activity (up to one-tenth that of the unchanged drug). Elimination The excretion is primarily biliary, with only 6% of the oral dose excreted in the urine; only 0.1% is excreted in the urine as unchanged parent compound. There is a high variability in the data reported on the terminal half-life of ciclosporin depending on the assay applied and on the target population. The terminal half-life ranged from 6.3 hours in healthy volunteers to 20.4 hours in patients with severe liver disease (see sections 4.2 and 4.4). The elimination half-life in kidney-transplanted patients was approximately 11 hours, with a range between 4 and 25 hours. Special populations Patients with renal impairment In a study performed in patients with terminal renal failure, the systemic clearance was approximately two thirds of the mean systemic clearance in patients with normally functioning kidneys. Less than 1% of the administered dose is removed by dialysis. Patients with hepatic impairment An approximate 2- to 3-fold increase in ciclosporin exposure may be observed in patients with hepatic impairment. In a study performed in severe liver disease patients with biopsy-proven cirrhosis, the terminal half-life was 20.4 hours (range between 10.8 to 48.0 hours) compared to 7.4 to 11.0 hours in healthy subjects. Paediatric population Pharmacokinetic data from paediatric patients given Sandimmun Neoral
or Sandimmun
are very
limited. In 15 renal transplant patients aged 3 -16 years, ciclosporin whole blood clearance after intravenous administration of Sandimmun
was 10.6±3.7 ml/min/kg (assay: Cyclo-trac specific RIA).
In a study of 7 renal transplant patients aged 2-16 years, the ciclosporin clearance ranged from 9.8 to15.5 ml/min/kg. In 9 liver transplant patients aged 0.65-6 years, clearance was 9.3±5.4 ml/min/kg (assay: HPLC). In comparison to adult transplant populations, the differences in bioavailability between Sandimmun Neoral and Sandimmun in paediatrics are comparable to those observed in adults.
52

5.3 Preclinical safety data Ciclosporin gave no evidence of mutagenic or teratogenic effects in the standard test systems with oral application (rats up to 17 mg/kg/day and rabbits up to 30 mg/kg/day orally). At toxic doses (rats at 30 mg/kg/day and rabbits at 100 mg/kg/day orally), ciclosporin was embryo- and foetotoxic as indicated by increased prenatal and postnatal mortality, and reduced foetal weight together with related skeletal retardations. In two published research studies, rabbits exposed to ciclosporin in utero (10 mg/kg/day subcutaneously) demonstrated reduced numbers of nephrons, renal hypertrophy, systemic hypertension, and progressive renal insufficiency up to 35 weeks of age. Pregnant rats which received 12 mg/kg/day of ciclosporin intravenously (twice the recommended human intravenous dose) had foetuses with an increased incidence of ventricular septal defect. These findings have not been demonstrated in other species and their relevance for humans is unknown. No impairment in fertility was demonstrated in studies in male and female rats. Ciclosporin was tested in a number of in vitro and in vivo tests for genotoxicity with no evidence for a clincally relevant mutagenic potential. Carcinogenicity studies were carried out in male and female rats and mice. In the 78-week mouse study, at doses of 1, 4, and 16 mg/kg/day, evidence of a statistically significant trend was found for lymphocytic lymphomas in females, and the incidence of hepatocellular carcinomas in mid-dose males significantly exceeded the control value. In the 24-month rat study conducted at 0.5, 2, and 8 mg/kg/day, pancreatic islet cell adenomas significantly exceeded the control rate at the low dose level. The hepatocellular carcinomas and pancreatic islet cell adenomas were not dose related. 6. PHARMACEUTICAL PARTICULARS 6.1 List of excipients Capsule contents Alpha-tocopherol Ethanol anhydrous Propylene glycol Corn oil-mono-di-triglycerides Macrogolglycerol hydroxystearate / polyoxyl 40 hydrogenated castor oil. Capsule shell Titanium dioxide (E 171) Glycerol 85% Propylene glycol Gelatin Imprint Carminic acid (E 120) Capsule content Alpha-tocopherol Ethanol anhydrous Propylene glycol Corn oil-mono-di-triglycerides Macrogolglycerol hydroxystearate / polyoxyl 40 hydrogenated castor oil Capsule shell Iron oxide black (E172)
53

Titanium dioxide (E171) Glycerol 85% Propylene glycol Gelatin Imprint Carminic acid (E120) Capsule content Alpha-tocopherol Ethanol anhydrous Propylene glycol Corn oil-mono-di-triglycerides Macrogolglycerol hydroxystearate / polyoxyl 40 hydrogenated castor oil Capsule shell Titanium dioxide (E171) Glycerol 85% Propylene glycol Gelatin Imprint Carminic acid (E120) Capsule content Alpha-tocopherol Ethanol anhydrous Propylene glycol Corn oil-mono-di-triglycerides Macrogolglycerol hydroxystearate / polyoxyl 40 hydrogenated castor oil Capsule shell Iron oxide black (E172) Titanium dioxide (E 171) Glycerol 85% Propylene glycol Gelatin Imprint Carminic acid (E 120) 6.2 Incompatibilities Not applicable. 6.3 Shelf life 2 years 6.4 Special precautions for storage Sandimmun Neoral capsules may be stored at room temperature not exceeding 25°C. Increases in temperatures up to 30°C for a total maximum of 3 months do not affect the quality of the product. Sandimmun Neoral capsules should be left in the blister pack until required for use. When a blister is opened, a characteristic smell is noticeable. This is normal and does not mean that there is anything wrong with the capsule. 6.5 Nature and contents of container
54

Blister packs of double-sided aluminium consisting of aluminium foil on the bottom side and aluminium foil on the upper side. [To be completed nationally] 6.6 Special precautions for disposal No special requirements. Any unused medicinal product or waste material should be disposed of in accordance with local requirements. 7. MARKETING AUTHORISATION HOLDER [See Annex I - To be completed nationally] {Name and address} {tel} {fax} {e-mail} 8. MARKETING AUTHORISATION NUMBER(S) [To be completed nationally] 9. DATE OF FIRST AUTHORISATION/RENEWAL OF THE AUTHORISATION [To be completed nationally] 10. DATE OF REVISION OF THE TEXT [To be completed nationally] Detailed information on this medicinal product is available on the website of {name of MS/Agency}
55

1. NAME OF THE MEDICINAL PRODUCT Sandimmun Neoral and associated names (see Annex I) 100 mg/ml oral solution [See Annex I – To be completed nationally] 2. QUALITATIVE AND QUANTITATIVE COMPOSITION 1 ml oral solution contains 100 mg ciclosporin. Excipients with known effect: Ethanol: 94.70 mg/ml. Sandimmun Neoral oral solution contains 12% v/v ethanol (9.5% m/v). Propylene glycol: 94.70 mg/ml. Macrogolglycerol hydroxystearate: 383.70 mg/ml. For the full list of excipients, see section 6.1. 3. PHARMACEUTICAL FORM Oral solution Clear, faintly yellow to brownish yellow solution. The formulation of Sandimmun Neoral is a microemulsion preconcentrate. 4. CLINICAL PARTICULARS 4.1 Therapeutic indications Transplantation indications Solid organ transplantation Prevention of graft rejection following solid organ transplantation. Treatment of transplant cellular rejection in patients previously receiving other immunosuppressive agents. Bone marrow transplantation Prevention of graft rejection following allogeneic bone marrow and stem cell transplantation. Prevention or treatment of graft-versus-host disease (GVHD). Non-transplantation indications Endogenous uveitis Treatment of sight-threatening intermediate or posterior uveitis of non-infectious aetiology in patients in whom conventional therapy has failed or caused unacceptable side effects. Treatment of Behçet uveitis with repeated inflammatory attacks involving the retina in patients without neurological manifestations. Nephrotic syndrome Steroid-dependent and steroid-resistant nephrotic syndrome, due to primary glomerular diseases such as minimal change nephropathy, focal and segmental glomerulosclerosis, or membranous glomerulonephritis.
56

Sandimmun Neoral can be used to induce and maintain remissions. It can also be used to maintain steroid-induced remission, allowing withdrawal of steroids. Rheumatoid arthritis Treatment of severe, active rheumatoid arthritis. Psoriasis Treatment of severe psoriasis in patients in whom conventional therapy is inappropriate or ineffective. Atopic dermatitis Sandimmun Neoral is indicated in patients with severe atopic dermatitis when systemic therapy is required. 4.2 Posology and method of administration Posology The dose ranges given for oral administration are intended to serve as guidelines only. The daily doses of Sandimmun Neoral should be given in two divided doses equally distributed throughout the day. It is recommended that Sandimmun Neoral be administered on a consistent schedule with regard to time of day and in relation to meals. Sandimmun Neoral should only be prescribed by, or in close collaboration with, a physician with experience of immunosuppressive therapy and/or organ transplantation. Transplantation Solid organ transplantation Treatment with Sandimmun Neoral should be initiated within 12 hours before surgery at a dose of 10 to 15 mg/kg given in 2 divided doses. This dose should be maintained as the daily dose for 1 to 2 weeks post-operatively, being gradually reduced in accordance with blood levels according to local immunosuppressive protocols until a recommended maintenance dose of about 2 to 6 mg/kg given in 2 divided doses is reached. When Sandimmun Neoral is given with other immunosuppressants (e.g. with corticosteroids or as part of a triple or quadruple medicinal product therapy), lower doses (e.g. 3 to 6 mg/kg given in 2 divided doses for the initial treatment) may be used. Bone marrow transplantation The initial dose should be given on the day before transplantation. In most cases, Sandimmun concentrate for solution for infusion is preferred for this purpose. The recommended intravenous dose is 3 to 5 mg/kg/day. Infusion is continued at this dose level during the immediate post-transplant period of up to 2 weeks, before a change is made to oral maintenance therapy with Sandimmun Neoral at daily doses of about 12.5 mg/kg given in 2 divided doses. Maintenance treatment should be continued for at least 3 months (and preferably for 6 months) before the dose is gradually decreased to zero by 1 year after transplantation. If Sandimmun Neoral is used to initiate therapy, the recommended daily dose is 12.5 to 15 mg/kg given in 2 divided doses, starting on the day before transplantation. Higher doses of Sandimmun Neoral, or the use of Sandimmun intravenous therapy, may be necessary in the presence of gastrointestinal disturbances which might decrease absorption. In some patients, GVHD occurs after discontinuation of ciclosporin treatment, but usually responds favourably to re-introduction of therapy. In such cases an initial oral loading dose of 10 to 12.5 mg/kg
57

should be given, followed by daily oral administration of the maintenance dose previously found to be satisfactory. Low doses of Sandimmun Neoral should be used to treat mild, chronic GVHD. Non-transplantation indications When using Sandimmun Neoral in any of the established non-transplantation indications, the following general rules should be adhered to: Before initiation of treatment a reliable baseline level of renal function should be established by at least two measurements. The estimated glomerular filtration rate (eGFR) by the MDRD formula can be used for estimation of renal function in adults and an appropriate formula should be used to assess eGFR in paediatric patients. Since Sandimmun Neoral can impair renal function, it is necessary to assess renal function frequently. If eGFR decreases by more than 25% below baseline at more than one measurement, the dosage of Sandimmun Neoral should be reduced by 25 to 50%. If the eGFR decrease from baseline exceeds 35%, further reduction of the dose of Sandimmun Neoral should be considered. These recommendations apply even if the patient`s values still lie within the laboratory`s normal range. If dose reduction is not successful in improving eGFR within one month, Sandimmun Neoral treatment should be discontinued (see section 4.4). Regular monitoring of blood pressure is required. The determination of bilirubin and parameters that assess hepatic function are required prior to starting therapy and close monitoring during treatment is recommended. Determinations of serum lipids, potassium, magnesium and uric acid are advisable before treatment and periodically during treatment. Occasional monitoring of ciclosporin blood levels may be relevant in non-transplant indications, e.g. when Sandimmun Neoral is co-administered with substances that may interfere with the pharmacokinetics of ciclosporin, or in the event of unusual clinical response (e.g. lack of efficacy or increased drug intolerance such as renal dysfunction). The normal route of administration is by mouth. If the concentrate for solution for infusion is used, careful consideration should be given to administering an adequate intravenous dose that corresponds to the oral dose. Consultation with a physician with experience of use of ciclosporin is recommended. Except in patients with sight-threatening endogenous uveitis and in children with nephrotic syndrome, the total daily dose must never exceed 5 mg/kg. For maintenance treatment the lowest effective and well tolerated dosage should be determined individually. In patients in whom within a given time (for specific information see below) no adequate response is achieved or the effective dose is not compatible with the established safety guidelines, treatment with Sandimmun Neoral should be discontinued. Endogenous uveitis For inducing remission, initially 5 mg/kg/day orally given in 2 divided doses are recommended until remission of active uveal inflammation and improvement in visual acuity are achieved. In refractory cases, the dose can be increased to 7 mg/kg/day for a limited period. To achieve initial remission, or to counteract inflammatory ocular attacks, systemic corticosteroid treatment with daily doses of 0.2 to 0.6 mg/kg prednisone or an equivalent may be added if Sandimmun Neoral alone does not control the situation sufficiently. After 3 months, the dose of corticosteroids may be tapered to the lowest effective dose. For maintenance treatment, the dose should be slowly reduced to the lowest effective level. During the remission phases, this should not exceed 5 mg/kg/day.
58

Infectious causes of uveitis should be ruled out before immunosuppressants can be used. Nephrotic syndrome For inducing remission, the recommended daily dose is given in 2 divided oral doses. If the renal function (except for proteinuria) is normal, the recommended daily dose is the following: - adults: 5 mg/kg - children: 6 mg/kg In patients with impaired renal function, the initial dose should not exceed 2.5 mg/kg/day. The combination of Sandimmun Neoral with low doses of oral corticosteroids is recommended if the effect of Sandimmun Neoral alone is not satisfactory, especially in steroid-resistant patients. Time to improvement varies from 3 to 6 months depending on the type of glomerulopathy. If no improvement has been observed after this time to improvement period, Sandimmun Neoral therapy should be discontinued. The doses need to be adjusted individually according to efficacy (proteinuria) and safety, but should not exceed 5 mg/kg/day in adults and 6 mg/kg/day in children. For maintenance treatment, the dose should be slowly reduced to the lowest effective level. Rheumatoid arthritis For the first 6 weeks of treatment the recommended dose is 3 mg/kg/day orally given in 2 divided doses. If the effect is insufficient, the daily dose may then be increased gradually as tolerability permits, but should not exceed 5 mg/kg. To achieve full effectiveness, up to 12 weeks of Sandimmun Neoral therapy may be required. For maintenance treatment the dose has to be titrated individually to the lowest effective level according to tolerability. Sandimmun Neoral can be given in combination with low-dose corticosteroids and/or non-steroidal anti-inflammatory drugs (NSAIDs) (see section 4.4). Sandimmun Neoral can also be combined with low-dose weekly methotrexate in patients who have insufficient response to methotrexate alone, by using 2.5 mg/kg Sandimmun Neoral in 2 divided doses per day initially, with the option to increase the dose as tolerability permits. Psoriasis Sandimmun Neoral treatment should be initiated by physicians with experience in the diagnosis and treatment of psoriasis. Due to the variability of this condition, treatment must be individualised. For inducing remission, the recommended initial dose is 2.5 mg/kg/day orally given in 2 divided doses. If there is no improvement after 1 month, the daily dose may be gradually increased, but should not exceed 5 mg/kg. Treatment should be discontinued in patients in whom sufficient response of psoriatic lesions cannot be achieved within 6 weeks on 5 mg/kg/day, or in whom the effective dose is not compatible with the established safety guidelines (see section 4.4). Initial doses of 5 mg/kg/day are justified in patients whose condition requires rapid improvement. Once satisfactory response is achieved, Sandimmun Neoral may be discontinued and subsequent relapse managed with re-introduction of Sandimmun Neoral at the previous effective dose. In some patients, continuous maintenance therapy may be necessary. For maintenance treatment, doses have to be titrated individually to the lowest effective level, and should not exceed 5 mg/kg/day.
59

Atopic dermatitis Sandimmun Neoral treatment should be initiated by physicians with experience in the diagnosis and treatment of atopic dermatitis. Due to the variability of this condition, treatment must be individualised. The recommended dose range is 2.5 to 5 mg/kg/day given in 2 divided oral doses. If a starting dose of 2.5 mg/kg/day does not achieve a satisfactory response within 2 weeks, the daily dose may be rapidly increased to a maximum of 5 mg/kg. In very severe cases, rapid and adequate control of the disease is more likely to occur with a starting dose of 5 mg/kg/day. Once satisfactory response is achieved, the dose should be reduced gradually and, if possible, Sandimmun Neoral should be discontinued. Subsequent relapse may be managed with a further course of Sandimmun Neoral. Although an 8-week course of therapy may be sufficient to achieve clearing, up to 1 year of therapy has been shown to be effective and well tolerated, provided the monitoring guidelines are followed. Switching from Sandimmun to Sandimmun Neoral The available data indicate that after a 1:1 switch from Sandimmun to Sandimmun Neoral, the trough concentrations of ciclosporin in whole blood are comparable. In many patients, however, higher peak concentrations (Cmax) and increased exposure to the active substance (AUC) may occur. In a small percentage of patients these changes are more marked and may be of clinical significance.. In addition, the absorption of ciclosporin from Sandimmun Neoral is less variable and the correlation between ciclosporin trough concentrations and exposure (in terms of AUC) is stronger than with Sandimmun. Since the switch from Sandimmun to Sandimmun Neoral may result in increased exposure to ciclosporin, the following rules must be observed: In transplant patients, Sandimmun Neoral should be started at the same daily dose as was previously used with Sandimmun. Ciclosporin trough concentrations in whole blood should be monitored initially within 4 to 7 days after the switch to Sandimmun Neoral. In addition, clinical safety parameters such as renal function and blood pressure must be monitored during the first 2 months after the switch. If the ciclosporin trough blood levels are beyond the therapeutic range, and/or worsening of the clinical safety parameters occurs, the dosage must be adjusted accordingly. In patients treated for non-transplantation indications, Sandimmun Neoral should be started with the same daily dose as was used with Sandimmun. Two, 4 and 8 weeks after the switch, renal function and blood pressure should be monitored. If blood pressure significantly exceed the pre-switch levels or if eGFR decreases by more than 25% below the value measured prior to Sandimmun therapy at more than one measurement, the dose should be reduced (see also ‘Additional precautions’ in section 4.4). In the event of unexpected toxicity or inefficacy of ciclosporin, blood trough levels should also be monitored. Switching between oral ciclosporin formulations The switch from one oral ciclosporin formulation to another should be made under physician supervision, including monitoring of blood levels of ciclosporin for transplantation patients. Special populations Patients with renal impairment All indications Ciclosporin undergoes minimal renal elimination and its pharmacokinetics are not extensively affected by renal impairment (see section 5.2). However, due to its nephrotoxic potential (see section 4.8), careful monitoring of renal function is recommended (see section 4.4). Non-transplantation indications With the exception of patients being treated for nephrotic syndrome, patients with impaired renal function should not receive ciclosporin (see subsection on additional precautions in non-transplantation indications in section 4.4). In nephrotic syndrome patients with impaired renal function, the initial dose should not exceed 2.5 mg/kg/day.
60

Patients with hepatic impairment Ciclosporin is extensively metabolised by the liver. An approximate 2- to 3-fold increase in ciclosporin exposure may be observed in patients with hepatic impairment. Dose reduction may be necessary in patients with severe liver impairment to maintain blood levels within the recommended target range (see sections 4.4 and 5.2) and it is recommended that ciclosporin blood levels are monitored until stable levels are reached. Paediatric population Clinical studies have included children from 1 year of age. In several studies, paediatric patients required and tolerated higher doses of ciclosporin per kg body weight than those used in adults. Use of Sandimmun Neoral in children for non-transplantation indications other than nephrotic syndrome cannot be recommended (see section 4.4). Elderly population (age 65 years and above) Experience with Sandimmun Neoral in the elderly is limited. In rheumatoid arthritis clinical trials with ciclosporin, patients aged 65 or older were more likely to develop systolic hypertension on therapy, and more likely to show serum creatinine rises ≥50% above the baseline after 3 to 4 months of therapy. Dose selection for an elderly patient should be cautious, usually starting at the low end of the dosing range, reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or medication and increased susceptibility for infections. Method of administration Oral use Sandimmun Neoral oral solution should be diluted, preferably with orange or apple juice. However, other drinks, such as soft drinks, can be used accordingly to individual taste. The solution should be stirred well immediately before it is taken. Owing to its possible interference with the cytochrome P450-dependent enzyme system, grapefruit or grapefruit juice should be avoided for dilution (see section 4.5). The syringe should not come in contact with the diluent. If the syringe is to be cleaned, do not rinse it but wipe the outside with a dry tissue (see section 6.6). Precautions to be taken before handling or administering the medicinal product For instructions on dilution of the medicinal product before administration, see section 6.6. 4.3 Contraindications Hypersensitivity to the active substance or to any of the excipients listed in section 6.1. Combination with products containing Hypericum perforatum (St John´s Wort) (see section 4.5). Combination with medicines that are substrates for the multidrug efflux transporter P-glycoprotein or the organic anion transporter proteins (OATP) and for which elevated plasma concentrations are associated with serious and/or life-threatening events, e.g. bosentan, dabigatran etexilate and aliskiren (see section 4.5). 4.4 Special warnings and precautions for use Medical supervision Sandimmun Neoral should be prescribed only by physicians who are experienced in immunosuppressive therapy and can provide adequate follow-up, including regular full physical examination, measurement of blood pressure and control of laboratory safety parameters. Transplantation patients receiving this medicinal product should be managed in facilities with
61

adequate laboratory and supportive medical resources. The physician responsible for maintenance therapy should receive complete information for the follow-up of the patient. Lymphomas and other malignancies Like other immunosuppressants, ciclosporin increases the risk of developing lymphomas and other malignancies, particularly those of the skin. The increased risk appears to be related to the degree and duration of immunosuppression rather than to the use of specific agents. A treatment regimen containing multiple immunosuppressants (including ciclosporin) should therefore be used with caution as this could lead to lymphoproliferative disorders and solid organ tumours, some with reported fatalities. In view of the potential risk of skin malignancy, patients on Sandimmun Neoral, in particular those treated for psoriasis or atopic dermatitis, should be warned to avoid excess unprotected sun exposure and should not receive concomitant ultraviolet B irradiation or PUVA photochemotherapy. Infections Like other immunosuppressants, ciclosporin predisposes patients to the development of a variety of bacterial, fungal, parasitic and viral infections, often with opportunistic pathogens. Activation of latent polyomavirus infections that may lead to polyomavirus associated nephropathy (PVAN), especially to BK virus nephropathy (BKVN), or to JC virus associated progressive multifocal leukoencephalopathy (PML), have been observed in patients receiving ciclosporin. These conditions are often related to a high total immunosuppressive burden and should be considered in the differential diagnosis in immunosuppressed patients with deteriorating renal function or neurological symptoms. Serious and/or fatal outcomes have been reported. Effective pre-emptive and therapeutic strategies should be employed, particularly in patients on multiple long-term immunosuppressive therapy. Renal toxicity A frequent and potentially serious complication, an increase in serum creatinine and urea, may occur during Sandimmun Neoral therapy. These functional changes are dose-dependent and are initially reversible, usually responding to dose reduction. During long-term treatment, some patients may develop structural changes in the kidney (e.g. interstitial fibrosis) which, in renal transplant patients, must be differentiated from changes due to chronic rejection. Frequent monitoring of renal function is therefore required according to local guidelines for the indication in question (see sections 4.2 and 4.8). Hepatotoxicity Sandimmun Neoral may also cause dose-dependent, reversible increases in serum bilirubin and in liver enzymes (see section 4.8). There have been solicited and spontaneous reports of hepatotoxicity and liver injury including cholestasis, jaundice, hepatitis and liver failure in patients treated with ciclosporin. Most reports included patients with significant co-morbidities, underlying conditions and other confounding factors including infectious complications and co-medications with hepatotoxic potential. In some cases, mainly in transplant patients, fatal outcomes have been reported (see section 4.8). Close monitoring of parameters that assess hepatic function is required and abnormal values may necessitate dose reduction (see sections 4.2 and 5.2). Elderly population (age 65 years and above) In elderly patients, renal function should be monitored with particular care. Monitoring ciclosporin levels (see section 4.2) When Sandimmun Neoral is used in transplant patients, routine monitoring of ciclosporin blood levels is an important safety measure. For monitoring ciclosporin levels in whole blood, a specific monoclonal antibody (measurement of parent compound) is preferred; a high-performance liquid chromatography (HPLC) method, which also measures the parent compound, can be used as well. If plasma or serum is used, a standard separation protocol (time and temperature) should be followed.
62

For the initial monitoring of liver transplant patients, either the specific monoclonal antibody should be used, or parallel measurements using both the specific monoclonal antibody and the non-specific monoclonal antibody should be performed, to ensure a dosage that provides adequate immunosuppression. In non-transplant patients, occasional monitoring of ciclosporin blood levels is recommended, e.g. when Sandimmun Neoral is co-administered with substances that may interfere with the pharmacokinetics of ciclosporin, or in the event of unusual clinical response (e.g. lack of efficacy or increased drug intolerance such as renal dysfunction). It must be remembered that the ciclosporin concentration in blood, plasma, or serum is only one of many factors contributing to the clinical status of the patient. Results should therefore serve only as a guide to dosage in relationship to other clinical and laboratory parameters. Hypertension Regular monitoring of blood pressure is required during Sandimmun Neoral therapy. If hypertension develops, appropriate antihypertensive treatment must be instituted. Preference should be given to an antihypertensive agent that does not interfere with the pharmacokinetics of ciclosporin, e.g. isradipine (see section 4.5). Blood lipids increased Since Sandimmun Neoral has been reported to induce a reversible slight increase in blood lipids, it is advisable to perform lipid determinations before treatment and after the first month of therapy. In the event of increased lipids being found, restriction of dietary fat and, if appropriate, a dose reduction, should be considered. Hyperkalaemia Ciclosporin enhances the risk of hyperkalaemia, especially in patients with renal dysfunction. Caution is also required when ciclosporin is co-administered with potassium-sparing drugs (e.g. potassium-sparing diuretics, angiotensin converting enzyme (ACE) inhibitors, angiotensin II receptor antagonists) or potassium-containing medicinal products as well as in patients on a potassium rich diet. Control of potassium levels in these situations is advisable. Hypomagnesaemia Ciclosporin enhances the clearance of magnesium. This can lead to symptomatic hypomagnesaemia, especially in the peri-transplant period. Control of serum magnesium levels is therefore recommended in the peri-transplant period, particularly in the presence of neurological symptom/signs. If considered necessary, magnesium supplementation should be given. Hyperuricaemia Caution is required when treating patients with hyperuricaemia. Live-attenuated vaccines During treatment with ciclosporin, vaccination may be less effective. The use of live attenuated vaccines should be avoided (see section 4.5). Interactions Caution should be observed when co-administering ciclosporin with drugs that substantially increase or decrease ciclosporin plasma concentrations, through inhibition or induction of CYP3A4 and/or P-glycoprotein (see section 4.5). Renal toxicity should be monitored when initiating ciclosporin use together with active substances that increase ciclosporin levels or with substances that exhibit nephrotoxic synergy (see section 4.5). Concomitant use of ciclosporin and tacrolimus should be avoided (see section 4.5).
63

Ciclosporin is an inhibitor of CYP3A4, the multidrug efflux transporter P-glycoprotein and organic anion transporter proteins (OATP) and may increase plasma levels of co-medications that are substrates of this enzyme and/or transporter. Caution should be observed while co-administering ciclosporin with such drugs or concomitant use should be avoided (see section 4.5). Ciclosporin increases the exposure to HMG-CoA reductase inhibitors (statins). When concurrently administered with ciclosporin, the dosage of the statins should be reduced and concomitant use of certain statins should be avoided according to their label recommendations. Statin therapy needs to be temporarily withheld or discontinued in patients with signs and symptoms of myopathy or those with risk factors predisposing to severe renal injury, including renal failure, secondary to rhabdomyolysis (see section 4.5). Following concomitant administration of ciclosporin and lercanidipine, the AUC of lercanidipine was increased three-fold and the AUC of ciclosporin was increased 21%. Therefore the simultaneous combination of ciclosporin and lercanidipine should be avoided. Administration of ciclosporin 3 hours after lercanidipine yielded no change of the lercanidipine AUC, but the ciclosporin AUC was increased by 27%. This combination should therefore be given with caution with an interval of at least 3 hours. Special excipients: Polyoxyl 40 hydrogenated castor oil Sandimmun Neoral contains polyoxyl 40 hydrogenated castor oil, which may cause stomach upsets and diarrhoea. Special excipients: Ethanol Sandimmun Neoral contains around 12% vol. ethanol. A 500 mg dose of Sandimmun Neoral contains 500 mg ethanol, equivalent to nearly 15 ml beer or 5 ml wine. This may be harmful in alcoholic patients and should be taken into account in pregnant or breast-feeding women, in patients presenting with liver disease or epilepsy, or if the patients is a child. Additional precautions in non-transplantation indications Patients with impaired renal function (except nephrotic syndrome patients with a permissible degree of renal impairment), uncontrolled hypertension, uncontrolled infections, or any kind of malignancy should not receive ciclosporin. Before initiation of treatment a reliable baseline assessment of renal function should be established by at least two measurements of eGFR. Renal function must be assessed frequently throughout therapy to allow dosage adjustment (see section 4.2). Additional precautions in endogenous uveitis Sandimmun Neoral should be administered with caution in patients with neurological Behcet`s syndrome. The neurological status of these patients should be carefully monitored. There is only limited experience with the use of Sandimmun Neoral in children with endogenous uveitis. Additional precautions in nephrotic syndrome Patients with abnormal baseline renal function should initially be treated with 2.5 mg/kg/day and must be monitored very carefully. In some patients, it may be difficult to detect Sandimmun Neoral-induced renal dysfunction because of changes in renal function related to the nephrotic syndrome itself. This explains why, in rare cases, Sandimmun Neoral-associated structural kidney alterations have been observed without increases in serum creatinine. Renal biopsy should be considered for patients with steroid-dependent minimal-change nephropathy, in whom Sandimmun Neoral therapy has been maintained for more than 1 year. In patients with nephrotic syndrome treated with immunosuppressants (including ciclosporin), the occurrence of malignancies (including Hodgkin's lymphoma) has occasionally been reported.
64

Additional precautions in rheumatoid arthritis After 6 months of therapy, renal function needs to be assessed every 4 to 8 weeks depending on the stability of the disease, its co- medication, and concomitant diseases. More frequent checks are necessary when the Sandimmun Neoral dose is increased, or concomitant treatment with an NSAID is initiated or its dosage increased. Discontinuation of Sandimmun Neoral may also become necessary if hypertension developing during treatment cannot be controlled by appropriate therapy. As with other long-term immunosuppressive treatments, an increased risk of lymphoproliferative disorders must be borne in mind. Special caution should be observed if Sandimmun Neoral is used in combination with methotrexate due to nephrotoxic synergy. Additional precautions in psoriasis Discontinuation of Sandimmun Neoral therapy is recommended if hypertension developing during treatment cannot be controlled with appropriate therapy. Elderly patients should be treated only in the presence of disabling psoriasis, and renal function should be monitored with particular care. There is only limited experience with the use of Sandimmun Neoral in children with psoriasis. In psoriatic patients on ciclosporin, as in those on conventional immunosuppressive therapy, development of malignancies (in particular of the skin) has been reported. Skin lesions not typical for psoriasis, but suspected to be malignant or pre-malignant should be biopsied before Sandimmun Neoral treatment is started. Patients with malignant or pre-malignant alterations of the skin should be treated with Sandimmun Neoral only after appropriate treatment of such lesions, and if no other option for successful therapy exists. In a few psoriatic patients treated with Sandimmun Neoral, lymphoproliferative disorders have occurred. These were responsive to prompt discontinuation. Patients on Sandimmun Neoral should not receive concomitant ultraviolet B irradiation or PUVA photochemotherapy. Additional precautions in atopic dermatitis Discontinuation of Sandimmun Neoral is recommended if hypertension developing during treatment cannot be controlled with appropriate therapy. Experience with Sandimmun Neoral in children with atopic dermatitis is limited. Elderly patients should be treated only in the presence of disabling atopic dermatitis and renal function should be monitored with particular care. Benign lymphadenopathy is commonly associated with flares in atopic dermatitis and invariably disappears spontaneously or with general improvement in the disease. Lymphadenopathy observed on treatment with ciclosporin should be regularly monitored. Lymphadenopathy which persists despite improvement in disease activity should be examined by biopsy as a precautionary measure to ensure the absence of lymphoma. Active herpes simplex infections should be allowed to clear before treatment with Sandimmun Neoral is initiated, but are not necessarily a reason for treatment withdrawal if they occur during therapy unless infection is severe.
65
Skin infections with Staphylococcus aureus are not an absolute contraindication for Sandimmun Neoral therapy, but should be controlled with appropriate antibacterial agents. Oral erythromycin, which is known to have the potential to increase the blood concentration of ciclosporin (see section 4.5), should be avoided. If there is no alternative, it is recommended to closely monitor blood levels of ciclosporin, renal function, and for side effects of ciclosporin. Patients on Sandimmun Neoral should not receive concomitant ultraviolet B irradiation or PUVA photochemotherapy. Paediatric use in non-transplantation indications Except for the treatment of nephrotic syndrome, there is no adequate experience available with Sandimmun Neoral. Its use in children under 16 years of age for non-transplantation indications other than nephrotic syndrome cannot be recommended. 4.5 Interaction with other medicinal products and other forms of interaction Drug interactions Of the many drugs reported to interact with ciclosporin, those for which the interactions are adequately substantiated and considered to have clinical implications are listed below. Various agents are known to either increase or decrease plasma or whole blood ciclosporin levels usually by inhibition or induction of enzymes involved in the metabolism of ciclosporin, in particular CYP3A4. Ciclosporin is also an inhibitor of CYP3A4, the multidrug efflux transporter P-glycoprotein and organic anion transporter proteins (OATP) and may increase plasma levels of co-medications that are substrates of this enzyme and/or transporters. Medicinal products known to reduce or increase the bioavailability of ciclosporin: In transplant patients frequent measurement of ciclosporin levels and, if necessary, ciclosporin dosage adjustment is required, particularly during the introduction or withdrawal of the co-administered medication. In non-transplant patients the relationship between blood level and clinical effects is less well established. If medicinal products known to increase ciclosporin levels are given concomitantly, frequent assessment of renal function and careful monitoring for ciclosporin-related side effects may be more appropriate than blood level measurement. Drugs that decrease ciclosporin levels All inducers of CYP3A4 and/or P-glycoprotein are expected to decrease ciclosporin levels. Examples of drugs that decrease ciclosporin levels are: Barbiturates, carbamazepine, oxcarbazepine, phenytoin; nafcillin, intravenous sulfadimidine, probucol, orlistat, hypericum perforatum (St. John’s wort), ticlopidine, sulfinpyrazone, terbinafine, bosentan. Products containing Hypericum perforatum (St John´s Wort) must not be used concomitantly with Sandimmun Neoral due to the risk of decreased blood levels of ciclosporin and thereby reduced effect (see section 4.3). Rifampicin induces ciclosporin intestinal and liver metabolism. Ciclosporin doses may need to be increased 3- to 5-fold during co-administration. Octreotide decreases oral absorption of ciclosporin and a 50% increase in the ciclosporin dose or a switch to intravenous administration could be necessary. Drugs that increase ciclosporin levels All inhibitors of CYP3A4 and/or P-glycoprotein may lead to increased levels of cyclosporine. Examples are:
66

Nicardipine, metoclopramide, oral contraceptives, methylprednisolone (high dose), allopurinol, cholic acid and derivatives, protease inhibitors, imatinib, colchicine, nefazodone. Macrolide antibiotics: Erythromycin can increase ciclosporin exposure 4- to 7-fold, sometimes resulting in nephrotoxicity. Clarithromycin has been reported to double the exposure of ciclosporin. Azitromycin increases ciclosporin levels by around 20%. Azole antibiotics: Ketoconazole, fluconazole, itraconazole and voriconazole could more than double ciclosporin exposure. Verapamil increases ciclosporin blood concentrations 2- to 3-fold. Co-administration with telaprevir resulted in approximately 4.64-fold increase in ciclosporin dose normalised exposure (AUC). Amiodarone substantially increases the plasma ciclosporin concentration concurrently with an increase in serum creatinine. This interaction can occur for a long time after withdrawal of amiodarone, due to its very long half-life (about 50 days). Danazol has been reported to increase ciclosporin blood concentrations by approximately 50%. Diltiazem (at doses of 90 mg/day) can increase ciclosporin plasma concentrations by up to 50%. Imatinib could increase ciclosporin exposure and Cmax by around 20%. Food interactions The concomitant intake of grapefruit and grapefruit juice has been reported to increase the bioavailability of ciclosporin. Combinations with increased risk for nephrotoxicity Care should be taken when using ciclosporin together with other active substances that exhibit nephrotoxic synergy such as: aminoglycosides (including gentamycin, tobramycin), amphotericin B, ciprofloxacin, vancomycin, trimethoprim (+ sulfamethoxazole); fibric acid derivatives (e.g. bezafibrate, fenofibrate); NSAIDs (including diclofenac, naproxen, sulindac); melphalan histamine H2-receptor antagonists (e.g. cimetidine, ranitidine); methotrexate (see section 4.4). During the concomitant use of a drug that may exhibit nephrotoxic synergy, close monitoring of renal function should be performed. If a significant impairment of renal function occurs, the dosage of the co-administered medicinal product should be reduced or alternative treatment considered. Concomitant use of ciclosporin and tacrolimus should be avoided due to the risk for nephrotoxicity and pharmacokinetic interaction via CYP3A4 and/or P-gp (see section 4.4). Effects of ciclosporin on other drugs Ciclosporin is an inhibitor of CYP3A4, the multidrug efflux transporter P-glycoprotein (P-gp) and organic anion transporter proteins (OATP). Co-administration of drugs that are substrates of CYP3A4, P-gp and OATP with ciclosporin may increase plasma levels of co-medications that are substrates of this enzyme and/or transporter. Some examples are listed below: Ciclosporin may reduce the clearance of digoxin, colchicine, HMG-CoA reductase inhibitors (statins) and etoposide. If any of these drugs are used concurrently with ciclosporin, close clinical observation is required in order to enable early detection of toxic manifestations of the medicinal products, followed by reduction of its dosage or its withdrawal. When concurrently administered with ciclosporin, the dosage of the statins should be reduced and concomitant use of certain statins should be avoided according to their label recommendations. Exposure changes of commonly used statins
67

with ciclosporin are summarised in Table 1. Statin therapy needs to be temporarily withheld or discontinued in patients with signs and symptoms of myopathy or those with risk factors predisposing to severe renal injury, including renal failure, secondary to rhabdomyolysis. Table 1 Summary of exposure changes of commonly used statins with ciclosporin
Statin Doses available Fold change in
exposure with ciclosporin
Atorvastatin 10-80 mg 8-10 Simvastatin 10-80 mg 6-8 Fluvastatin 20-80 mg 2-4 Lovastatin 20-40 mg 5-8 Pravastatin 20-80 mg 5-10 Rosuvastatin 5-40 mg 5-10 Pitavastatin 1-4 mg 4-6
Caution is recommended when co-administering ciclosporin with lercanidipine (see section 4.4). Following concomitant administration of ciclosporin and aliskiren, a P-gp substrate, the Cmax of aliskiren was increased approximately 2.5-fold and the AUC approximately 5-fold. However, the pharmacokinetic profile of ciclosporin was not significantly altered. Co-administration of ciclosporin and aliskiren is not recommended (see section 4.3). Concomitant administration of dabigatran etexilate is not recommended due to the P-gp inhibitory activity of ciclosporin (see section 4.3). The concurrent administration of nifedipine with ciclosporin may result in an increased rate of gingival hyperplasia compared with that observed when ciclosporin is given alone. The concomitant use of diclofenac and ciclosporin has been found to result in a significant increase in the bioavailability of diclofenac, with the possible consequence of reversible renal function impairment. The increase in the bioavailability of diclofenac is most probably caused by a reduction of its high first-pass effect. If NSAIDs with a low first-pass effect (e.g. acetylsalicylic acid) are given together with ciclosporin, no increase in their bioavailability is to be expected. Elevations in serum creatinine were observed in the studies using everolimus or sirolimus in combination with full-dose ciclosporin for microemulsion. This effect is often reversible with ciclosporin dose reduction. Everolimus and sirolimus had only a minor influence on ciclosporin pharmacokinetics. Co-administration of ciclosporin significantly increases blood levels of everolimus and sirolimus. Caution is required with concomitant use of potassium-sparing medicinal products (e.g. potassium-sparing diuretics, ACE inhibitors, angiotensin II receptor antagonists) or potassium-containing medicinal products since they may lead to significant increases in serum potassium (see section 4.4). Ciclosporin may increase the plasma concentrations of repaglinide and thereby increase the risk of hypoglycaemia. Co-administration of bosentan and ciclosporin in healthy volunteers increases the bosentan exposure several-fold and there was a 35% decrease in ciclosporin exposure. Co-administration of ciclosporin with bosentan is not recommended (see above subsection “Drugs that decrease ciclosporin levels” and section 4.3).
68
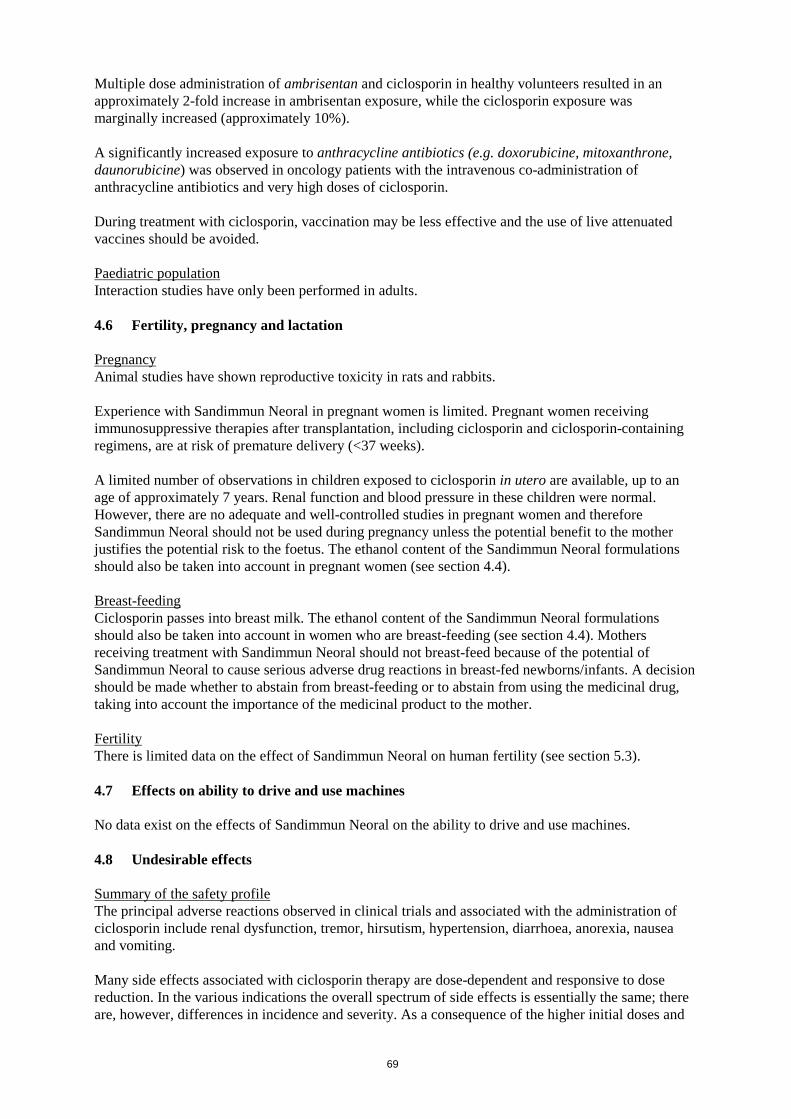
Multiple dose administration of ambrisentan and ciclosporin in healthy volunteers resulted in an approximately 2-fold increase in ambrisentan exposure, while the ciclosporin exposure was marginally increased (approximately 10%). A significantly increased exposure to anthracycline antibiotics (e.g. doxorubicine, mitoxanthrone, daunorubicine) was observed in oncology patients with the intravenous co-administration of anthracycline antibiotics and very high doses of ciclosporin. During treatment with ciclosporin, vaccination may be less effective and the use of live attenuated vaccines should be avoided. Paediatric population Interaction studies have only been performed in adults. 4.6 Fertility, pregnancy and lactation Pregnancy Animal studies have shown reproductive toxicity in rats and rabbits. Experience with Sandimmun Neoral in pregnant women is limited. Pregnant women receiving immunosuppressive therapies after transplantation, including ciclosporin and ciclosporin-containing regimens, are at risk of premature delivery (<37 weeks). A limited number of observations in children exposed to ciclosporin in utero are available, up to an age of approximately 7 years. Renal function and blood pressure in these children were normal. However, there are no adequate and well-controlled studies in pregnant women and therefore Sandimmun Neoral should not be used during pregnancy unless the potential benefit to the mother justifies the potential risk to the foetus. The ethanol content of the Sandimmun Neoral formulations should also be taken into account in pregnant women (see section 4.4). Breast-feeding Ciclosporin passes into breast milk. The ethanol content of the Sandimmun Neoral formulations should also be taken into account in women who are breast-feeding (see section 4.4). Mothers receiving treatment with Sandimmun Neoral should not breast-feed because of the potential of Sandimmun Neoral to cause serious adverse drug reactions in breast-fed newborns/infants. A decision should be made whether to abstain from breast-feeding or to abstain from using the medicinal drug, taking into account the importance of the medicinal product to the mother. Fertility There is limited data on the effect of Sandimmun Neoral on human fertility (see section 5.3). 4.7 Effects on ability to drive and use machines No data exist on the effects of Sandimmun Neoral on the ability to drive and use machines. 4.8 Undesirable effects Summary of the safety profile The principal adverse reactions observed in clinical trials and associated with the administration of ciclosporin include renal dysfunction, tremor, hirsutism, hypertension, diarrhoea, anorexia, nausea and vomiting. Many side effects associated with ciclosporin therapy are dose-dependent and responsive to dose reduction. In the various indications the overall spectrum of side effects is essentially the same; there are, however, differences in incidence and severity. As a consequence of the higher initial doses and
69

longer maintenance therapy required after transplantation, side effects are more frequent and usually more severe in transplant patients than in patients treated for other indications. Anaphylactoid reactions have been observed following intravenous administration (see section 4.4). Infections and infestations Patients receiving immunosuppressive therapies, including ciclosporin and ciclosporin-containing regimens, are at increased risk of infections (viral, bacterial, fungal, parasitic) (see section 4.4). Both generalised and localised infections can occur. Pre-existing infections may also be aggravated and reactivation of polyomavirus infections may lead to polyomavirus-associated nephropathy (PVAN) or to JC virus associated progressive multifocal leukopathy (PML). Serious and/or fatal outcomes have been reported. Neoplasms benign, malignant and unspecified (including cysts and polyps) Patients receiving immunosuppressive therapies, including ciclosporin and ciclosporin containing regimens, are at increased risk of developing lymphomas or lymphoproliferative disorders and other malignancies, particularly of the skin. The frequency of malignancies increases with the intensity and duration of therapy (see section 4.4). Some malignancies may be fatal. Tabulated summary of adverse drug reactions from clinical trials Adverse drug reactions from clinical trials (Table 1) are listed by MedDRA system organ class. Within each system organ class, the adverse drug reactions are ranked by frequency, with the most frequent reactions first. Within each frequency grouping, adverse drug reactions are presented in order of decreasing seriousness. In addition the corresponding frequency category for each adverse drug reaction is based on the following convention (CIOMS III): very common (≥1/10); common (≥1/100, <1/10); uncommon (≥1/1,000, <1/100); rare (≥1/10,000, <1/1,000) very rare (<1/10,000), not known (cannot be estimated from the available data). Table 1: Adverse drug reactions from clinical trials Blood and lymphatic system disorders Common Leucopenia Uncommon Thrombocytopenia, anaemia Rare Haemolytic uraemic syndrome, microangiopathic haemolytic anaemia Not known* Thrombotic microangiopathy, thrombotic thrombocytopenic purpura Metabolism and nutrition disorders Very common Hyperlipidaemia Common Hyperglycaemia, anorexia, hyperuricaemia, hyperkalaemia, hypomagnesaemia Nervous system disorders Very common Tremor, headache Common Convulsions, paraesthesia Uncommon Encephalopathy including Posterior Reversible Encephalopathy Syndrome
(PRES), signs and symptoms such as convulsions, confusion, disorientation, decreased responsiveness, agitation, insomnia, visual disturbances, cortical blindness, coma, paresis and cerebellar ataxia
Rare Motor polyneuropathy Very rare Optic disc oedema, including papilloedema, with possible visual impairment
secondary to benign intracranial hypertension Not known* Migraine Vascular disorders Very common Hypertension Common Flushing Gastrointestinal disorders Common Nausea, vomiting, abdominal discomfort/pain, diarrhoea, gingival hyperplasia,
peptic ulcer Rare Pancreatitis
70

Hepatobiliary disorders Common Hepatic function abnormal (see section 4.4) Not known* Hepatotoxicity and liver injury including cholestasis, jaundice, hepatitis and
liver failure with some fatal outcome (see section 4.4) Skin and subcutaneous tissue disorders Very common Hirsutism Common Acne, hypertrichosis Uncommon Allergic rashes Musculoskeletal and connective tissue disorders Common Myalgia, muscle cramps Rare Muscle weakness, myopathy Renal and urinary disorders Very common Renal dysfunction (see section 4.4) Reproductive system and breast disorders Rare Menstrual disturbances, gynaecomastia General disorders and administration site conditions Common Pyrexia, fatigue Uncommon Oedema, weight increase * Adverse events reported from post marketing experience where the ADR frequency is not known due to the lack of a real denominator. Other adverse drug reactions from post-marketing experience There have been solicited and spontaneous reports of hepatotoxicity and liver injury including cholestasis, jaundice hepatitis and liver failure in patients treated with ciclosporin. Most reports included patients with significant co-morbidities, underlying conditions and other confounding factors including infectious complications and co-medications with hepatotoxic potential. In some cases, mainly in transplant patients, fatal outcomes have been reported (see section 4.4). Acute and chronic nephrotoxicity Patients receiving calcineurin inhibitor (CNI) therapies, including ciclosporin and ciclosporin-containing regimens, are at increased risk of acute or chronic nephrotoxicity. There have been reports from clinical trials and from the post-marketing setting associated with the use of Sandimmun Neoral. Cases of acute nephrotoxicity reported disorders of ion homeostasis, such as hyperkalaemia, hypomagnesaemia, and hyperuricaemia. Cases reporting chronic morphological changes included arteriolar hyalinosis, tubular atrophy and interstitial fibrosis (see section 4.4). Paediatric population Clinical studies have included children from 1 year of age using standard ciclosporin dosage with a comparable safety profile to adults. 4.9 Overdose The oral LD50 of ciclosporin is 2,329 mg/kg in mice, 1,480 mg/kg in rats and > 1,000 mg/kg in rabbits. The intravenous LD50 is 148 mg/kg in mice, 104 mg/kg in rats, and 46 mg/kg in rabbits. Symptoms Experience with acute overdosage of ciclosporin is limited. Oral doses of ciclosporin of up to 10 g (about 150 mg/kg) have been tolerated with relatively minor clinical consequences, such as vomiting, drowsiness, headache, tachycardia and in a few patients moderately severe, reversible impairment of renal function. However, serious symptoms of intoxication have been reported following accidental parenteral overdosage with ciclosporin in premature neonates. Treatment In all cases of overdosage, general supportive measures should be followed and symptomatic treatment applied. Forced emesis and gastric lavage may be of value within the first few hours after
71

oral intake. Ciclosporin is not dialysable to any great extent, nor is it well cleared by charcoal haemoperfusion. 5. PHARMACOLOGICAL PROPERTIES 5.1 Pharmacodynamic properties Pharmacotherapeutic group: Immunosuppressive agents, calcineurin inhibitors, ATC code: L04AD01 Ciclosporin (also known as ciclosporin A) is a cyclic polypeptide consisting of 11 amino acids. It is a potent immunosuppressive agent, which in animals prolongs survival of allogeneic transplants of skin, heart, kidney, pancreas, bone marrow, small intestine or lung. Studies suggest that ciclosporin inhibits the development of cell-mediated reactions, including allograft immunity, delayed cutaneous hypersensitivity, experimental allergic encephalomyelitis, Freund's adjuvant arthritis, graft-versus-host disease (GVHD), and also T-cell dependent antibody production. At the cellular level it inhibits production and release of lymphokines including interleukin 2 (T-cell growth factor, TCGF). Ciclosporin appears to block the resting lymphocytes in the G0 or G1 phase of the cell cycle, and inhibits the antigen-triggered release of lymphokines by activated T-cells. All available evidence suggests that ciclosporin acts specifically and reversibly on lymphocytes. Unlike cytostatic agents, it does not depress haemopoiesis and has no effect on the function of phagocytic cells. Successful solid organ and bone marrow transplantations have been performed in man using ciclosporin to prevent and treat rejection and GVHD. Ciclosporin has been used successfully both in hepatitis C virus (HCV) positive and HCV negative liver transplants recipients. Beneficial effects of ciclosporin therapy have also been shown in a variety of conditions that are known, or may be considered to be of autoimmune origin. Paediatric population: Ciclosporin has been shown to be efficacious in steroid-dependent nephrotic syndrome. 5.2 Pharmacokinetic properties Absorption Following oral administration of Sandimmun Neoral peak blood concentrations of ciclosporin are reached within 1-2 hours. The absolute oral bioavailability of ciclosporin following administration of Sandimmun Neoral is 20 to 50%. About 13 and 33% decrease in AUC and Cmax was observed when Sandimmun Neoral was administered with a high-fat meal. The relationship between administered dose and exposure (AUC) of ciclosporin is linear within the therapeutic dose range. The intersubject and intrasubject variability for AUC and Cmax is approximately 10-20%. Sandimmun Neoral solution and soft gelatin capsules are bioequivalent. Sandimmun Neoral administration results in a 59% higher Cmax and approximately 29% higher bioavailability than Sandimmun. The available data indicate that following a 1:1 switch from Sandimmun soft gelatin capsules to Sandimmun Neoral soft gelatin capsules trough concentrations in whole blood are comparable and remain in the desired therapeutic range. Sandimmun Neoral administration improves dose linearity in ciclosporin exposure (AUCB). It provides a more consistent absorption profile with less influence from concomitant food intake or from diurnal rhythm than Sandimmun. Distribution Ciclosporin is distributed largely outside the blood volume, with an average apparent distribution volume of 3.5 l/kg. In the blood, 33 to 47% is present in plasma, 4 to 9% in lymphocytes, 5 to 12% in
72

granulocytes, and 41 to 58% in erythrocytes. In plasma, approximately 90% is bound to proteins, mostly lipoproteins. Biotransformation Ciclosporin is extensively metabolised to approximately 15 metabolites. Metabolism mainly takes place in the liver via cytochrome P450 3A4 (CYP3A4), and the main pathways of metabolism consist of mono- and dihydroxylation and N-demethylation at various positions of the molecule. All metabolites identified so far contain the intact peptide structure of the parent compound; some possess weak immunosuppressive activity (up to one-tenth that of the unchanged drug). Elimination The excretion is primarily biliary, with only 6% of the oral dose excreted in the urine; only 0.1% is excreted in the urine as unchanged parent compound. There is a high variability in the data reported on the terminal half-life of ciclosporin depending on the assay applied and on the target population. The terminal half-life ranged from 6.3 hours in healthy volunteers to 20.4 hours in patients with severe liver disease (see sections 4.2 and 4.4). The elimination half-life in kidney-transplanted patients was approximately 11 hours, with a range between 4 and 25 hours. Special populations Patients with renal impairment In a study performed in patients with terminal renal failure, the systemic clearance was approximately two thirds of the mean systemic clearance in patients with normally functioning kidneys. Less than 1% of the administered dose is removed by dialysis. Patients with hepatic impairment An approximate 2- to 3-fold increase in ciclosporin exposure may be observed in patients with hepatic impairment. In a study performed in severe liver disease patients with biopsy-proven cirrhosis, the terminal half-life was 20.4 hours (range between 10.8 to 48.0 hours) compared to 7.4 to 11.0 hours in healthy subjects. Paediatric population Pharmacokinetic data from paediatric patients given Sandimmun Neoral
or Sandimmun
are very
limited. In 15 renal transplant patients aged 3 -16 years, ciclosporin whole blood clearance after intravenous administration of Sandimmun
was 10.6±3.7 ml/min/kg (assay: Cyclo-trac specific RIA).
In a study of 7 renal transplant patients aged 2-16 years, the ciclosporin clearance ranged from 9.8 to15.5 ml/min/kg. In 9 liver transplant patients aged 0.65-6 years, clearance was 9.3±5.4 ml/min/kg (assay: HPLC). In comparison to adult transplant populations, the differences in bioavailability between Sandimmun Neoral and Sandimmun in paediatrics are comparable to those observed in adults. 5.3 Preclinical safety data Ciclosporin gave no evidence of mutagenic or teratogenic effects in the standard test systems with oral application (rats up to 17 mg/kg/day and rabbits up to 30 mg/kg/day orally). At toxic doses (rats at 30 mg/kg/day and rabbits at 100 mg/kg/day orally), ciclosporin was embryo- and foetotoxic as indicated by increased prenatal and postnatal mortality, and reduced foetal weight together with related skeletal retardations. In two published research studies, rabbits exposed to ciclosporin in utero (10 mg/kg/day subcutaneously) demonstrated reduced numbers of nephrons, renal hypertrophy, systemic hypertension, and progressive renal insufficiency up to 35 weeks of age. Pregnant rats which received 12 mg/kg/day of ciclosporin intravenously (twice the recommended human intravenous dose) had foetuses with an increased incidence of ventricular septal defect. These findings have not been
73

demonstrated in other species and their relevance for humans is unknown. No impairment in fertility was demonstrated in studies in male and female rats. Ciclosporin was tested in a number of in vitro and in vivo tests for genotoxicity with no evidence for a clincally relevant mutagenic potential. Carcinogenicity studies were carried out in male and female rats and mice. In the 78-week mouse study, at doses of 1, 4, and 16 mg/kg/day, evidence of a statistically significant trend was found for lymphocytic lymphomas in females, and the incidence of hepatocellular carcinomas in mid-dose males significantly exceeded the control value. In the 24-month rat study conducted at 0.5, 2, and 8 mg/kg/day, pancreatic islet cell adenomas significantly exceeded the control rate at the low dose level. The hepatocellular carcinomas and pancreatic islet cell adenomas were not dose related. 6. PHARMACEUTICAL PARTICULARS 6.1 List of excipients Alpha–tocopherol Ethanol anhydrous Propylene glycol Corn oil-mono–di–triglycerides Macrogolglycerol hydroxystearate / polyoxyl 40 hydrogenated castor oil 6.2 Incompatibilities Not applicable. 6.3 Shelf life 3 years 6.4 Special precautions for storage Sandimmun Neoral oral solution should be stored between 15 and 30°C, but preferably not below 20°C for more than 1 month as it contains oily components of natural origin which tend to solidify at low temperatures. A jelly-like formation may occur below 20°C, which is however reversible at temperatures up to 30°C. Minor flakes or slight sediment may still be observed. These phenomena do not affect the efficacy and safety of the product and the dosing by means of the pipette remains accurate. After opening, Sandimmun Neoral oral solution should be used within 2 months. 6.5 Nature and contents of container 50 ml amber glass bottles with an aluminium cap and rubber stopper. A dispenser set is also provided. [To be completed nationally] 6.6 Special precautions for disposal Sandimmun Neoral oral solution is provided with two syringes for measuring the doses. The 1-ml syringe is used to measure doses less than or equal to 1 ml (each graduation of 0.05 ml corresponds to 5 mg of ciclosporin). The 4-ml syringe is used to measure doses greater than 1 ml and up to 4 ml (each graduation of 0.1 ml corresponds to 10 mg of ciclosporin).
74

Initial use of Sandimmun Neoral oral solution 1. Raise the flap in the centre of the metal sealing ring.
2. Tear off the sealing ring completely.
3. Remove the black stopper and throw it away.
4. Push the tube unit with the white stopper firmly into the neck of
the bottle.
5. Choose the syringe depending on the prescribed volume. For
volume less than 1 ml or equal to 1 ml, use the 1-ml syringe. For volume greater than 1 ml, use the 4-ml syringe. Insert the nozzle of the syringe into the white stopper.
6. Draw up the prescribed volume of solution (position the lower
part of the plunger ring in front of the graduation corresponding to the prescribed volume).
75
7. Expel any large bubbles by depressing and withdrawing the plunger a few times before removing the syringe containing the prescribed dose from bottle. The presence of a few tiny bubbles is of no importance and will not affect the dose in any way.
8. Push the medicine out of the syringe into a small glass with
some liquid (not grapefruit juice). Avoid any contact between the syringe and the liquid in the glass. The medicine can be mixed just before it is taken. Stir and drink the entire mixture right away. Once mixed it should be taken immediately after preparation.
9. After use, wipe the syringe on the outside only with a dry tissue
and replace it in its cover. The white stopper and tube should remain in the bottle. Close the bottle with the cap provided.
Subsequent use Commence at point 5. Any unused medicinal product or waste material should be disposed of in accordance with local requirements. 7. MARKETING AUTHORISATION HOLDER [See Annex I - To be completed nationally] {Name and address} {tel} {fax} {e-mail} 8. MARKETING AUTHORISATION NUMBER(S) [To be completed nationally] 9. DATE OF FIRST AUTHORISATION/RENEWAL OF THE AUTHORISATION [To be completed nationally]
76

10. DATE OF REVISION OF THE TEXT [To be completed nationally] Detailed information on this medicinal product is available on the website of {name of MS/Agency}
77
LABELLING
78
PARTICULARS TO APPEAR ON THE OUTER PACKAGING CARTONS 1. NAME OF THE MEDICINAL PRODUCT Sandimmun Neoral and associated names (see Annex I) 10 mg soft capsules Sandimmun Neoral and associated names (see Annex I) 25 mg soft capsules Sandimmun Neoral and associated names (see Annex I) 50 mg soft capsules Sandimmun Neoral and associated names (see Annex I) 100 mg soft capsules [See Annex I - To be completed nationally] Ciclosporin 2. STATEMENT OF ACTIVE SUBSTANCE(S) Ciclosporin [To be completed nationally] 3. LIST OF EXCIPIENTS Contains ethanol (see leaflet for further information). [To be completed nationally] 4. PHARMACEUTICAL FORM AND CONTENTS Capsule, soft [To be completed nationally] 5. METHOD AND ROUTE(S) OF ADMINISTRATION Oral use Read the package leaflet before use. [To be completed nationally] 6. SPECIAL WARNING THAT THE MEDICINAL PRODUCT MUST BE STORED OUT
OF THE SIGHT AND REACH OF CHILDREN Keep out of the sight and reach of children. [To be completed nationally]
79

7. OTHER SPECIAL WARNING(S), IF NECESSARY [To be completed nationally] 8. EXPIRY DATE [To be completed nationally] 9. SPECIAL STORAGE CONDITIONS [To be completed nationally] 10. SPECIAL PRECAUTIONS FOR DISPOSAL OF UNUSED MEDICINAL PRODUCTS OR WASTE MATERIALS DERIVED FROM SUCH MEDICINAL PRODUCTS, IF APPROPRIATE [To be completed nationally] 11. NAME AND ADDRESS OF THE MARKETING AUTHORISATION HOLDER [See Annex I - To be completed nationally] {Name and Address} {tel} {fax} {e-mail} 12. MARKETING AUTHORISATION NUMBER(S) [To be completed nationally] 13. BATCH NUMBER [To be completed nationally] 14. GENERAL CLASSIFICATION FOR SUPPLY [To be completed nationally] 15. INSTRUCTIONS ON USE [To be completed nationally] 16. INFORMATION IN BRAILLE
80

[To be completed nationally]
81

MINIMUM PARTICULARS TO APPEAR ON BLISTERS OR STRIPS BLISTERS 1. NAME OF THE MEDICINAL PRODUCT Sandimmun Neoral and associated names (see Annex I) 10 mg soft capsules Sandimmun Neoral and associated names (see Annex I) 25 mg soft capsules Sandimmun Neoral and associated names (see Annex I) 50 mg soft capsules Sandimmun Neoral and associated names (see Annex I) 100 mg soft capsules [See Annex I - To be completed nationally] Ciclosporin 2. NAME OF THE MARKETING AUTHORISATION HOLDER [See Annex I - To be completed nationally] {Name} 3. EXPIRY DATE [To be completed nationally] 4. BATCH NUMBER [To be completed nationally] 5. OTHER [To be completed nationally]
82

PARTICULARS TO APPEAR ON THE OUTER PACKAGING AND THE IMMEDIATE PACKAGING CARTON AND BOTTLE LABEL 1. NAME OF THE MEDICINAL PRODUCT Sandimmun Neoral and associated names (see Annex I) 100 mg/ml oral solution [See Annex I - To be completed nationally] Ciclosporin 2. STATEMENT OF ACTIVE SUBSTANCE(S) Each ml contains 100 mg ciclosporin 3. LIST OF EXCIPIENTS Contains ethanol (see leaflet for further information). 4. PHARMACEUTICAL FORM AND CONTENTS Oral solution containing 100 mg ciclosporin per mL 5. METHOD AND ROUTE(S) OF ADMINISTRATION Oral use Read the package leaflet before use. [To be completed nationally] 6. SPECIAL WARNING THAT THE MEDICINAL PRODUCT MUST BE STORED OUT
OF THE SIGHT AND REACH OF CHILDREN Keep out of the sight and reach of children. [To be completed nationally] 7. OTHER SPECIAL WARNING(S), IF NECESSARY [To be completed nationally] 8. EXPIRY DATE [To be completed nationally]
83

9. SPECIAL STORAGE CONDITIONS [To be completed nationally] 10. SPECIAL PRECAUTIONS FOR DISPOSAL OF UNUSED MEDICINAL PRODUCTS OR WASTE MATERIALS DERIVED FROM SUCH MEDICINAL PRODUCTS, IF APPROPRIATE [To be completed nationally] 11. NAME AND ADDRESS OF THE MARKETING AUTHORISATION HOLDER [See Annex I - To be completed nationally] {Name and Address} {tel} {fax} {e-mail} 12. MARKETING AUTHORISATION NUMBER(S) [To be completed nationally] 13. BATCH NUMBER [To be completed nationally] 14. GENERAL CLASSIFICATION FOR SUPPLY [To be completed nationally] 15. INSTRUCTIONS ON USE [To be completed nationally] 16. INFORMATION IN BRAILLE [To be completed nationally]
84

PACKAGE LEAFLET
85

Package leaflet: Information for the patient
Sandimmun Neoral 10 mg soft capsules Sandimmun Neoral 25 mg soft capsules Sandimmun Neoral 50 mg soft capsules Sandimmun Neoral 100 mg soft capsules
ciclosporin
Read all of this leaflet carefully before you start taking this medicine because it contains important information for you. - Keep this leaflet. You may need to read it again. - If you have any further questions, ask your doctor or pharmacist. - This medicine has been prescribed for you only. Do not pass it on to others. It may harm them,
even if their signs of illness are the same as yours. - If you get any side effects, talk to your doctor or pharmacist. This includes any possible side
effects not listed in this leaflet. What is in this leaflet 1. What Sandimmun Neoral is and what it is used for 2. What you need to know before you take Sandimmun Neoral 3. How to take Sandimmun Neoral 4. Possible side effects 5. How to store Sandimmun Neoral 6. Contents of the pack and other information 1. What Sandimmun Neoral is and what it is used for What Sandimmun Neoral is The name of your medicine is Sandimmun Neoral. It contains the active substance ciclosporin. This belongs to a group of medicines known as immunosuppressive agents. These medicines are used to lower the body’s immune reactions. What Sandimmun Neoral is used for and how Sandimmun Neoral works • If you have had an organ transplant, bone marrow and stem cell transplantation, the
function of Sandimmun Neoral is to control your body’s immune system. Sandimmun Neoral prevents rejection of transplanted organs by blocking the development of certain cells which would normally attack the transplanted tissue.
• If you have an autoimmune disease, in which your body’s immune response attacks your body’s own cells, Sandimmun Neoral stops this immune reaction. Such diseases include eye problems which threaten your vision (endogenous uveitis, including Behçet's uveitis), severe cases of certain skin diseases (atopic dermatitis, or eczema and psoriasis), severe rheumatoid arthritis and a kidney disease called nephrotic syndrome.
2. What you need to know before you take Sandimmun Neoral If you are taking Sandimmun Neoral following a transplant it will only be prescribed for you by a doctor with experience in transplants and/or autoimmune diseases. The advice in this leaflet may vary depending on whether you are taking the medicine for a transplant or for an autoimmune disease.
86
Follow all your doctor’s instructions carefully. They may differ from the general information contained in this leaflet. Do not take Sandimmun Neoral: - if you are allergic to ciclosporin or any of the other ingredients of this medicine (listed in
section 6). - with products containing Hypericum perforatum (St John´s Wort). - with products containing dabigatran etexilate (used to avoid blood clots after surgery) or
bosentan and aliskiren (used to reduce high blood pressure). Do not take Sandimmun Neoral and tell your doctor if the above applies to you. If you are not sure, talk to your doctor before taking Sandimmun Neoral. Warnings and precautions Before and during treatment with Sandimmun Neoral, tell your doctor straight away: • if you have any signs of infection, such as fever or a sore throat. Sandimmun Neoral suppresses
the immune system and may also affect your body’s ability to fight against infection. • if you have liver problems. • if you have kidney problems. Your doctor will carry out regular blood tests and may change
your dose if necessary. • if you develop high blood pressure. Your doctor will check your blood pressure regularly and
may give you a medicine to lower blood pressure if necessary. • if you have low levels of magnesium in your body. Your doctor may give you magnesium
supplements to take, especially just after your operation if you have had a transplant. • if you have high levels of potassium in your blood. • if you have gout. • if you need to have a vaccination. If any of the above applies to you before or during treatment with Sandimmun Neoral, tell your doctor straight away. Sunlight and sun protection Sandimmun Neoral suppresses your immune system. This increases your risk of developing cancers, particularly of the skin and lymphoid system. You should limit your exposure to sunlight and UV light by: • Wearing appropriate protective clothing. • Often applying a sunscreen with a high protection factor.
Talk to your doctor before taking Sandimmun Neoral: • if you have or have had alcohol-related problems. • if you have epilepsy. • if you have any liver problems. • if you are pregnant. • if you are breast-feeding. • if this medicine is being prescribed for a child. If any of the above apply to you (or you are not sure), tell your doctor before taking Sandimmun Neoral. This is because this medicine contains alcohol (see section below “Sandimmun Neoral contains ethanol”). Monitoring during your treatment with Sandimmun Neoral Your doctor will check: • the levels of ciclosporin in your blood, especially if you have had a transplant, • your blood pressure before the start of your treatment and regularly during treatment, • how well your liver and kidneys are working, • your blood lipids (fats). If you have any questions about how Sandimmun Neoral works or why this medicine has been
87

prescribed for you, ask your doctor. In addition if you are taking Sandimmun Neoral for a non-transplant disease (intermediary or posterior uveitis and Behçet's uveitis, atopic dermatitis, severe rheumatoid arthritis or nephrotic syndrome), do not take Sandimmun Neoral: • if you have kidney problems (except for nephrotic syndrome). • if you have an infection which is not under control with medication. • if you have any type of cancer. • if you have high blood pressure (hypertension) which is not under control with medication. If
you get high blood pressure during treatment and it cannot be controlled, Sandimmun Neoral should be stopped by your doctor.
Do not take Sandimmun Neoral if any of the above applies to you. If you are not sure, talk to your doctor or pharmacist before taking Sandimmun Neoral. If you are being treated for Behçet`s uveitis, your doctor will monitor you particularly carefully if you have neurological symptoms (for example: increased forgetfulness, personality changes noticed over time, psychiatric or mood disorders, burning sensation in limbs, decreased sensation in limbs, tingling sensation in limbs, weakness of limbs, walking disturbances, headache with or without nausea and vomiting, vision disturbances including restricted movement of eyeball). Your doctor will closely monitor you if you are elderly and are being treated for psoriasis or atopic dermatitis. If you have been prescribed Sandimmun Neoral to treat your psoriasis or atopic dermatitis, you must not be exposed to any UVB-rays or phototherapy during treatment. Children and adolescents Sandimmun Neoral should not be given to children for a non-transplant disease, except for treatment of nephrotic syndrome. Elderly population (65 years of age and older) There is limited experience with Sandimmun Neoral in elderly patients. Your doctor should monitor how well your kidneys work. If you are over 65 and have psoriasis or atopic dermatitis, you should only be treated with Sandimmun Neoral if your condition is particularly severe. Other medicines and Sandimmun Neoral Tell your doctor or pharmacist if you are taking, have recently taken or might take any other medicines. In particular tell your doctor or pharmacist if you are taking any of the following medicines before or during Sandimmun Neoral treatment: • Medicines that may affect your potassium levels. These include medicines which contain
potassium, potassium supplements, water tablets (diuretics) called potassium-sparing diuretics and some medicines which lower your blood pressure.
• Methotrexate. This is used to treat tumours, severe psoriasis and severe rheumatoid arthritis. • Medicines which may increase or decrease the level of ciclosporin (the active substance of
Sandimmun Neoral) in your blood. Your doctor might check the level of ciclosporin in your blood when starting or stopping treatment with other medicines. - Medicines which may increase the level of ciclosporin in your blood include: antibiotics
(such as erythromycin or azythromycin), anti-fungals (voriconazole, itraconazole), medicines used for heart problems or high blood pressure (diltiazem, nicardipine, verapamil, amiodarone), metoclopramide (used to stop sickness), oral contraceptives, danazol (used to treat menstrual problems), medicines used to treat gout (allopurinol), cholic acid and derivatives (used to treat gallstones), protease inhibitors used to treat HIV, imatinib (used to treat leukaemia or tumours), colchicine, telaprevir (used to treat hepatitis C).
88

- Medicines which may decrease the level of ciclosporin in your blood include: barbiturates (used to help you to sleep), some anti-convulsant medicines (such as carbamazepine or phenytoine), octreotide (used to treat acromegaly or neuroendocrine tumours in the gut), anti-bacterial medicines used to treat tuberculosis, orlistat (used to help weight loss), herbal medicines containing St. John’s wort, ticlopidine (used after a stroke), certain medicines which lower blood pressure (bosentan), and terbinafine (an anti-fungal medicine used to treat infections of the toes and nails).
• Medicines which may affect your kidneys. These include: anti-bacterial medicines (gentamycin, tobramycin, ciprofloxacin), anti-fungal medicines which contain amphotericin B, medicines used for urinary tract infections which contain trimethoprim, medicines for cancer which contain melphalan, medicines used to lower the amount of acid in your stomach (acid secretion inhibitors of the H2-receptor antagonist type), tacrolimus, pain killers (non-steroid anti-inflammatory medicines such as diclofenac), fibric acid medicines (used to lower the amount of fat in the blood).
• Nifedipine. This is used to treat high blood pressure and heart pain. You might get swollen gums that might grow over your teeth if you are taking nifedipine during your treatment with ciclosporin.
• Digoxin (used to treat heart problems), medicines which lower cholesterol (HMG-CoA reductase inhibitors also called statins), prednisolone, etoposide (used to treat cancer), repaglinide (oral anti-diabetic medicine), immunosuppressives (everolimus, sirolimus), ambrisentan and specific anti-cancer medicines called anthracyclines (such as doxorubicin).
If any of the above applies to you (or you are not sure), talk to your doctor or pharmacist before taking Sandimmun Neoral. Sandimmun Neoral with food and drink Do not take Sandimmun Neoral with grapefruit or grapefruit juice. This is because these can affect how Sandimmun Neoral works. Pregnancy and breast-feeding Ask your doctor or pharmacist for advice before taking this medicine. Your doctor will discuss with you the potential risks of taking Sandimmun Neoral during pregnancy. • Tell your doctor if you are pregnant or intend to become pregnant. Experience with
Sandimmun Neoral in pregnancy is limited. In general, Sandimmun Neoral should not be taken during pregnancy. If it is necessary for you to take this medicine, your doctor will discuss with you the benefits and potential risks of taking it during pregnancy.
• Tell your doctor if you are breast-feeding. Breast-feeding is not recommended during treatment with Sandimmun Neoral. This is because ciclosporin, the active substance, passes into breast milk. This may affect your baby.
Driving and using machines Sandimmun Neoral contains alcohol. This may affect your ability to drive and use machines. Sandimmun Neoral contains ethanol Sandimmun Neoral contains approximately 12.0 vol. % ethanol (alcohol), which corresponds to up to 500 mg per dose used in transplant patients. This is equivalent to nearly 15 ml beer or 5 ml wine per dose. Alcohol may be harmful if you have alcohol-related problems, epilepsy, brain injury, liver problems or if you are pregnant or breast-feeding. It may also be harmful if this medicine is given to children. Sandimmun Neoral contains castor oil Sandimmun Neoral contains castor oil, which may cause stomach discomfort and diarrhoea. 3. How to take Sandimmun Neoral
89

Always take this medicine exactly as your doctor has told you. Check with your doctor if you are not sure. Do not take more than the recommended dose. The dose of this medicine will be carefully adjusted to your individual needs by your doctor. Too much of the medicine can affect your kidneys. You will have regular blood tests and visits to the hospital, especially after a transplant. This will give you the chance to talk to your doctor about your treatment and talk about any problems you may be having. How much Sandimmun Neoral to take Your doctor will work out the correct dose of Sandimmun Neoral for you. This depends on your body weight and what you are taking the medicine for. Your doctor will also tell you how often to take your medicine. • In adults:
Organ, bone marrow and stem cell transplantation - The total dose each day is usually between 2 mg and 15 mg per kilogram body weight.
This is divided in two doses. - Usually, higher doses are used before and just after your transplant. Lower doses are
used once your transplanted organ or bone marrow has stabilised. - Your doctor will adjust your dose to one that is ideal for you. To do this, your doctor may
need to do some blood tests. Endogenous uveitis - The total dose each day is usually between 5 mg and 7 mg per kilogram body weight.
This is divided in two doses. Nephrotic syndrome - The total dose each day for adults is usually 5 mg per kilogram body weight. This is
divided in two doses. In patients with kidney problems, the first dose taken each day should not be more than 2.5 mg per kilogram body weight.
Severe rheumatoid arthritis - The total dose each day is usually between 3 mg per kilogram of your body weight and
5 mg per kilogram body weight. This is divided in two doses. Psoriasis and atopic dermatitis - The total dose each day is usually between 2.5 mg per kilogram of your body weight and
5 mg per kilogram body weight. This is divided in two doses. • In children:
Nephrotic syndrome - The total dose each day for children is usually 6 mg per kilogram body weight. This is
divided in two doses. In patients with kidney problems, the first dose taken each day should not be more than 2.5 mg per kilogram body weight.
Follow your doctor's instructions exactly and never change the dose yourself, even if you feel well. Switch from Sandimmun to Sandimmun Neoral You may have already been taking another medicine called Sandimmun soft gelatin capsules or Sandimmun oral solution. Your doctor may decide to change to this medicine, Sandimmun Neoral soft gelatin capsules. • These medicines all contain ciclosporin as the active ingredient. • Sandimmun Neoral is a different, improved formulation of ciclosporin compared to
Sandimmun. Ciclosporin is absorbed into your blood better with Sandimmun Neoral and absorption is less likely to be affected by taking the medicine with food. This means that the levels of ciclosporin in your blood stay more constant with Sandimmun Neoral than with Sandimmun.
If your doctor changes you from Sandimmun to Sandimmun Neoral: • Do not go back to taking Sandimmun unless your doctor tells you to.
90

• Following your transfer from Sandimmun to Sandimmun Neoral, your doctor will monitor you more closely for a short time. This is because of the change in how ciclosporin is absorbed into your blood. Your doctor will make sure that you get the right dose for your individual needs.
• You may have some side effects. If this happens, tell your doctor or pharmacist. Your dose may need to be lowered. Never lower your dose yourself, unless a doctor has told you to.
If your doctor switches you from one oral formulation of ciclosporin to another After you change from one oral formulation of ciclosporin to another: • Your doctor will monitor you more closely for a short time. • You may have some side effects. If this happens, tell your doctor or pharmacist. Your dose may
need to be changed. Never change your dose yourself, unless a doctor has told you to. When to take Sandimmun Neoral Take Sandimmun Neoral at the same time every day. This is very important if you have had a transplant. How to take Sandimmun Neoral Your daily doses should always be taken in 2 divided doses. Remove the capsules from the blister. Swallow the capsules whole with water. How long to take Sandimmun Neoral Your doctor will tell you how long you need to take Sandimmun Neoral for. This depends on whether you are taking it after a transplant or for the treatment of a severe skin condition, rheumatoid arthritis, uveitis or nephrotic syndrome. For severe rash, the treatment usually lasts for 8 weeks. Keep taking Sandimmun Neoral for as long as your doctor tells you. If you have questions about how long to take Sandimmun Neoral, talk to your doctor or your pharmacist. If you take more Sandimmun Neoral than you should If you accidentally take too much of your medicine, tell your doctor immediately or go to your nearest hospital emergency unit. You may need medical attention. If you forget to take Sandimmun Neoral • If you forget to take a dose, take it as soon as you remember it. However, if it is almost time for
your next dose, skip the missed dose. Then go on as before. • Do not take a double dose to make up for a forgotten dose. If you stop taking Sandimmun Neoral Do not stop taking Sandimmun Neoral unless your doctor tells you to. Keep taking Sandimmun Neoral even if you feel well. Stopping your treatment with Sandimmun Neoral may increase the risk of your transplanted organ being rejected. If you have any further questions on the use of this medicine, ask your doctor or pharmacist. 4. Possible side effects Like all medicines, this medicine can cause side effects, although not everybody gets them.
91

Some side effects could be serious Tell your doctor straight away if you notice any of the following serious side effects: • Like other medicines that act on the immune system, ciclosporin may influence your body’s
ability to fight against infection and may cause tumours or other cancers, particularly of the skin. Signs of infection might be fever or sore throat.
• Changes in your sight, loss of coordination, being clumsy, memory loss, difficulty speaking or understanding what others say, and muscle weakness. These might be signs of an infection of the brain called progressive multifocal leukoencephalopathy.
• Brain problems with signs such as seizures, confusion, feeling disorientated, being less responsive, personality changes, feeling agitated, sleeplessness, changes to your sight, blindness, coma, paralysis of part or all of the body, stiff neck, loss of coordination with or without unusual speech or eye movements.
• Swelling at the back of the eye. This may be associated with blurred vision. It may also affect your sight because of the higher pressure inside your head (benign intracranial hypertension).
• Liver problems and damage with or without yellow skin and eyes, nausea, loss of appetite and dark urine.
• Kidney problems which may greatly reduce the amount of urine you produce. • Low level of red blood cells or platelets. The signs include pale skin, feeling tired, being
breathless, having dark urine (this is a sign of the breakdown of red blood cells), bruising or bleeding with no obvious reasons, feeling confused, feeling disorientated, being less alert and having kidney problems.
Other side effects include: Very common side effects: These side effects may affect more than 1 in 10 people. • Kidney problems. • High blood pressure. • Headache. • Shaking of your body which you cannot control. • Excessive growth of body and facial hair. • High level of lipids in your blood. If any of these affects you severely, tell your doctor. Common side effects: These side effects may affect between 1 and 10 in every 100 people. • Fits (seizures). • Liver problems. • High level of sugar in your blood. • Tiredness. • Loss of appetite. • Nausea (feeling sick), vomiting, abdominal pain, constipation, diarrhoea. • Excessive hair growth. • Acne, hot flushes. • Fever. • Low level of white blood cells. • Feeling numb or tingling. • Pain in your muscles, muscle spasm. • Stomach ulcer. • Gum tissue overgrowing and covering your teeth. • High level of uric acid or patassium in your blood, low levels of magnesium in your blood. If any of these affects you severely, tell your doctor.
92

Uncommon side effects: These side effects may affect between 1 and 10 in every 1,000 people. • Symptoms of brain disorders including sudden fits, mental confusion, sleeplessness,
disorientation, disturbance of vision, unconsciousness, sense of weakness in the limbs, impaired movements.
• Rash. • General swelling. • Weight gain. • Low level of red blood cells, low level of platelets in your blood which could increase the risk
of bleeding. If any of these affects you severely, tell your doctor. Rare side effects: These side effects may affect between 1 and 10 in every 10,000 people. • Nerve problems with numbness or tingling in fingers and toes. • Inflammation of the pancreas with severe upper stomach pain. • Muscle weakness, loss of muscle strength, pain in muscles of the legs or hands or anywhere in
the body. • Destruction of red blood cells, involving kidney problems with symptoms such as swelling of
the face, stomach, hands and/or feet, decreased urination, breathing difficulty, chest pain, fits, unconsciousness.
• Changes in menstrual cycle, breast enlargement in men. If any of these affects you severely, tell your doctor. Very rare side effects: These side effects may affect between 1 and 10 in every 100,000 people. • Swelling at the back of the eye which may be associated with an increase in pressure inside the
head and eyesight disturbances. If this affects you severely, tell your doctor. Other side effects with frequency not known: Frequency cannot be estimated from the available data. • Serious liver problems both with and without yellowing of the eyes or skin, nausea (feeling
sick), loss of appetite, dark coloured urine, swelling of the face, feet, hands and/or the whole body.
• Bleeding underneath the skin or purple skin patched, sudden bleeding with no apparent cause. • Migraine or severe headache often with feeling and being sick (nausea, vomiting) and being
sensitive to light. If any of these affects you severely, tell your doctor. If you get any side effects, talk to your doctor or pharmacist. This includes any possible side effects not listed in this leaflet. Additional side effects in children and adolescents There are no additional side effects to be expected in children and adolescents compared to adults. 5. How to store Sandimmun Neoral • Keep this medicine out of the sight and reach of children. • Do not use this medicine after the expiry date which is stated on the package. • Do not store your capsules in a hot place (maximum temperature 25°C). • Leave your capsules in the foil. Only remove them when it is time to take your medicine. • When a blister is opened, a characteristic smell is noticeable. This is normal and does not mean
that there is anything wrong with the capsules.
93

• Do not throw away any medicines via wastewater or household waste. Ask your pharmacist how to throw away medicines you no longer use. These measures will help to protect the environment.
6. Contents of the pack and other information What Sandimmun Neoral contains • The active substance is ciclosporin. Each capsule contains 10 mg ciclosporin. • The other ingredients are:
o Capsule contents: alpha-tocopherol, ethanol anhydrous, propylene glycol, corn oil-mono-di-triglycerides, macrogolglycerol hydroxystearate /polyoxyl 40 hydrogenated castor oil.
o Capsule shell: Titanium dioxide (E 171), glycerol 85%, propylene glycol, gelatin. o Imprint: carminic acid (E 120).
• The active substance is ciclosporin. Each capsule contains 25 mg ciclosporin. • The other ingredients are:
o Capsule contents: alpha-tocopherol, ethanol anhydrous, propylene glycol, corn oil-mono-di-triglycerides, macrogolglycerol hydroxystearate / polyoxyl 40 hydrogenated castor oil.
o Capsule shell: Black iron oxide (E172), titanium dioxide (E171), glycerol 85%, propylene glycol, gelatin.
o Imprint: carminic acid (E 120). • The active substance is ciclosporin. Each capsule contains 50 mg ciclosporin. • The other ingredients are:
o Capsule content: alpha-tocopherol, ethanol anhydrous, propylene glycol, corn oil-mono-di-triglycerides, macrogolglycerol hydroxystearate / polyoxyl 40 hydrogenated castor oil.
o Capsule shell: Titanium dioxide (E 171), glycerol 85%, propylene glycol, gelatin. o Imprint: carminic acid (E 120).
• The active substance is ciclosporin. Each capsule contains 100 mg of the active substance ciclosporin.
• The other ingredients are: o Capsule contents: alpha-tocopherol, ethanol anhydrous, propylene glycol, corn oil-mono-
di-triglycerides, macrogolglycerol hydroxystearate / polyoxyl 40 hydrogenated castor oil. o Capsule shell: Black iron oxide (E172), titanium dioxide (E171), glycerol 85%,
propylene glycol, gelatin. o Imprint: carminic acid (E 120).
What Sandimmun Neoral looks like and contents of the pack Sandimmun Neoral 10 mg soft capsules are yellow to white oval, and marked with “NVR 10” in red. Sandimmun Neoral 25 mg soft capsules are blue to grey oval and marked with “NVR 25mg” in red. Sandimmun Neoral 50 mg soft capsules are yellow to white oblong and marked with “NVR 50mg” in red. Sandimmun Neoral 100 mg soft capsules are blue to grey oblong and marked with “NVR 100mg” in red. Not all pack sizes may be available. Marketing Authorisation Holder and Manufacturer [To be completed nationally] {Name and address} {tel} {fax} {e-mail}
94

This medicinal product is authorised in the Member States of the EEA under the following names: {Name of the Member State} {Name of the medicinal product} {Name of the Member State} {Name of the medicinal product} This leaflet was last revised in {MM/YYYY} {month YYYY}. [To be completed nationally]
95

Package leaflet: Information for the patient
Sandimmun Neoral 100 mg/ml oral solution
ciclosporin
Read all of this leaflet carefully before you start taking this medicine because it contains important information for you. - Keep this leaflet. You may need to read it again. - If you have any further questions, ask your doctor or pharmacist. - This medicine has been prescribed for you only. Do not pass it on to others. It may harm them,
even if their signs of illness are the same as yours. - If you get any side effects, talk to your doctor or pharmacist. This includes any possible side
effects not listed in this leaflet. What is in this leaflet 1. What Sandimmun Neoral is and what it is used for 2. What you need to know before you take Sandimmun Neoral 3. How to take Sandimmun Neoral 4. Possible side effects 6. How to store Sandimmun Neoral 6. Contents of the pack and other information 1. What Sandimmun Neoral is and what it is used for What Sandimmun Neoral is The name of your medicine is Sandimmun Neoral. It contains the active substance ciclosporin. This belongs to a group of medicines known as immunosuppressive agents. These medicines are used to lower the body’s immune reactions. What Sandimmun Neoral is used for and how Sandimmun Neoral works • If you have had an organ transplant, bone marrow and stem cell transplantation, the
function of Sandimmun Neoral is to control your body’s immune system. Sandimmun Neoral prevents rejection of transplanted organs by blocking the development of certain cells which would normally attack the transplanted tissue.
• If you have an autoimmune disease, in which your body’s immune response attacks your body’s own cells, Sandimmun Neoral stops this immune reaction. Such diseases include eye problems which threaten your vision (endogenous uveitis, including Behçet's uveitis), severe cases of certain skin diseases (atopic dermatitis, or eczema and psoriasis), severe rheumatoid arthritis and a kidney disease called nephrotic syndrome.
2. What you need to know before you take Sandimmun Neoral If you are taking Sandimmun Neoral following a transplant it will only be prescribed for you by a doctor with experience in transplants and/or autoimmune diseases. The advice in this leaflet may vary depending on whether you are taking the medicine for a transplant or for an autoimmune disease. Follow all your doctor’s instructions carefully. They may differ from the general information contained in this leaflet. Do not take Sandimmun Neoral:
96

- if you are allergic to ciclosporin or any of the other ingredients of this medicine (listed in section 6).
- with products containing Hypericum perforatum (St John´s Wort). - with products containing dabigatran etexilate (used to avoid blood clots after surgery) or
bosentan and aliskiren (used to reduce high blood pressure). Do not take Sandimmun Neoral and tell your doctor if the above applies to you. If you are not sure, talk to your doctor before taking Sandimmun Neoral. Warnings and precautions Before and during treatment with Sandimmun Neoral, tell your doctor straight away: • if you have any signs of infection, such as fever or a sore throat. Sandimmun Neoral suppresses
the immune system and may also affect your body’s ability to fight against infection. • if you have liver problems. • if you have kidney problems. Your doctor will carry out regular blood tests and may change
your dose if necessary. • if you develop high blood pressure. Your doctor will check your blood pressure regularly and
may give you a medicine to lower blood pressure if necessary. • if you have low levels of magnesium in your body. Your doctor may give you magnesium
supplements to take, especially just after your operation if you have had a transplant. • if you have high levels of potassium in your blood. • if you have gout. • if you need to have a vaccination. If any of the above applies to you before or during treatment with Sandimmun Neoral, tell your doctor straight away. Sunlight and sun protection Sandimmun Neoral suppresses your immune system. This increases your risk of developing cancers, particularly of the skin and lymphoid system. You should limit your exposure to sunlight and UV light by: • Wearing appropriate protective clothing. • Often applying a sunscreen with a high protection factor.
Talk to your doctor before taking Sandimmun Neoral: • if you have or have had alcohol-related problems. • if you have epilepsy. • if you have any liver problems. • if you are pregnant. • if you are breast-feeding. • if this medicine is being prescribed for a child. If any of the above apply to you (or you are not sure), tell your doctor before taking Sandimmun Neoral. This is because this medicine contains alcohol (see section below “Sandimmun Neoral contains ethanol”). Monitoring during your treatment with Sandimmun Neoral Your doctor will check: • the levels of ciclosporin in your blood, especially if you have had a transplant, • your blood pressure before the start of your treatment and regularly during treatment, • how well your liver and kidneys are working, • your blood lipids (fats). If you have any questions about how Sandimmun Neoral works or why this medicine has been prescribed for you, ask your doctor.
97

In addition if you are taking Sandimmun Neoral for a non-transplant disease (intermediary or posterior uveitis and Behçet's uveitis, atopic dermatitis, severe rheumatoid arthritis or nephrotic syndrome), do not take Sandimmun Neoral: • if you have kidney problems (except for nephrotic syndrome). • if you have an infection which is not under control with medication. • if you have any type of cancer. • if you have high blood pressure (hypertension) which is not under control with medication. If
you get high blood pressure during treatment and it cannot be controlled, Sandimmun Neoral should be stopped by your doctor.
Do not take Sandimmun Neoral if any of the above applies to you. If you are not sure, talk to your doctor or pharmacist before taking Sandimmun Neoral. If you are being treated for Behçet`s uveitis, your doctor will monitor you particularly carefully if you have neurological symptoms (for example: increased forgetfulness, personality changes noticed over time, psychiatric or mood disorders, burning sensation in limbs, decreased sensation in limbs, tingling sensation in limbs, weakness of limbs, walking disturbances, headache with or without nausea and vomiting, vision disturbances including restricted movement of eyeball). Your doctor will closely monitor you if you are elderly and are being treated for psoriasis or atopic dermatitis. If you have been prescribed Sandimmun Neoral to treat your psoriasis or atopic dermatitis, you must not be exposed to any UVB-rays or phototherapy during treatment. Children and adolescents Sandimmun Neoral should not be given to children for a non-transplant disease, except for treatment of nephrotic syndrome. Elderly population (65 years of age and older) There is limited experience with Sandimmun Neoral in elderly patients. Your doctor should monitor how well your kidneys work. If you are over 65 and have psoriasis or atopic dermatitis, you should only be treated with Sandimmun Neoral if your condition is particularly severe. Other medicines and Sandimmun Neoral Tell your doctor or pharmacist if you are taking, have recently taken or might take any other medicines. In particular tell your doctor or pharmacist if you are taking any of the following medicines before or during Sandimmun Neoral treatment: • Medicines that may affect your potassium levels. These include medicines which contain
potassium, potassium supplements, water tablets (diuretics) called potassium-sparing diuretics and some medicines which lower your blood pressure.
• Methotrexate. This is used to treat tumours, severe psoriasis and severe rheumatoid arthritis. • Medicines which may increase or decrease the level of ciclosporin (the active substance of
Sandimmun Neoral) in your blood. Your doctor might check the level of ciclosporin in your blood when starting or stopping treatment with other medicines. - Medicines which may increase the level of ciclosporin in your blood include: antibiotics
(such as erythromycin or azythromycin), anti-fungals (voriconazole, itraconazole), medicines used for heart problems or high blood pressure (diltiazem, nicardipine, verapamil, amiodarone), metoclopramide (used to stop sickness), oral contraceptives, danazol (used to treat menstrual problems), medicines used to treat gout (allopurinol), cholic acid and derivatives (used to treat gallstones), protease inhibitors used to treat HIV, imatinib (used to treat leukaemia or tumours), colchicine, telaprevir (used to treat hepatitis C).
- Medicines which may decrease the level of ciclosporin in your blood include: barbiturates (used to help you to sleep), some anti-convulsant medicines (such as carbamazepine or phenytoine), octreotide (used to treat acromegaly or neuroendocrine tumours in the gut),
98

anti-bacterial medicines used to treat tuberculosis, orlistat (used to help weight loss), herbal medicines containing St. John’s wort, ticlopidine (used after a stroke), certain medicines which lower blood pressure (bosentan), and terbinafine (an anti-fungal medicine used to treat infections of the toes and nails).
• Medicines which may affect your kidneys. These include: anti-bacterial medicines (gentamycin, tobramycin, ciprofloxacin), anti-fungal medicines which contain amphotericin B, medicines used for urinary tract infections which contain trimethoprim, medicines for cancer which contain melphalan, medicines used to lower the amount of acid in your stomach (acid secretion inhibitors of the H2-receptor antagonist type), tacrolimus, pain killers (non-steroid anti-inflammatory medicines such as diclofenac), fibric acid medicines (used to lower the amount of fat in the blood).
• Nifedipine. This is used to treat high blood pressure and heart pain. You might get swollen gums that might grow over your teeth if you are taking nifedipine during your treatment with ciclosporin.
• Digoxin (used to treat heart problems), medicines which lower cholesterol (HMG-CoA reductase inhibitors also called statins), prednisolone, etoposide (used to treat cancer), repaglinide (oral anti-diabetic medicine), immunosuppressives (everolimus, sirolimus), ambrisentan and specific anti-cancer medicines called anthracyclines (such as doxorubicin).
If any of the above applies to you (or you are not sure), talk to your doctor or pharmacist before taking Sandimmun Neoral. Sandimmun Neoral with food and drink Do not take Sandimmun Neoral with grapefruit or grapefruit juice. This is because these can affect how Sandimmun Neoral works. Pregnancy and breast-feeding Ask your doctor or pharmacist for advice before taking this medicine. Your doctor will discuss with you the potential risks of taking Sandimmun Neoral during pregnancy. • Tell your doctor if you are pregnant or intend to become pregnant. Experience with
Sandimmun Neoral in pregnancy is limited. In general, Sandimmun Neoral should not be taken during pregnancy. If it is necessary for you to take this medicine, your doctor will discuss with you the benefits and potential risks of taking it during pregnancy.
• Tell your doctor if you are breast-feeding. Breast-feeding is not recommended during treatment with Sandimmun Neoral. This is because ciclosporin, the active substance, passes into breast milk. This may affect your baby.
Driving and using machines Sandimmun Neoral contains alcohol. This may affect your ability to drive and use machines. Sandimmun Neoral contains ethanol Sandimmun Neoral contains approximately 12.0 vol. % ethanol (alcohol), which corresponds to up to 500 mg per dose used in transplant patients. This is equivalent to nearly 15 ml beer or 5 ml wine per dose. Alcohol may be harmful if you have alcohol-related problems, epilepsy, brain injury, liver problems or if you are pregnant or breast-feeding. It may also be harmful if this medicine is given to children. Sandimmun Neoral contains castor oil Sandimmun Neoral contains castor oil, which may cause stomach discomfort and diarrhoea. 3. How to take Sandimmun Neoral Always take this medicine exactly as your doctor has told you. Check with your doctor if you are not sure.
99
Do not take more than the recommended dose. The dose of this medicine will be carefully adjusted to your individual needs by your doctor. Too much of the medicine can affect your kidneys. You will have regular blood tests and visits to the hospital, especially after a transplant. This will give you the chance to talk to your doctor about your treatment and talk about any problems you may be having. How much Sandimmun Neoral to take Your doctor will work out the correct dose of Sandimmun Neoral for you. This depends on your body weight and what you are taking the medicine for. Your doctor will also tell you how often to take your medicine. • In adults:
Organ, bone marrow and stem cell transplantation - The total dose each day is usually between 2 mg and 15 mg per kilogram body weight.
This is divided in two doses. - Usually, higher doses are used before and just after your transplant. Lower doses are
used once your transplanted organ or bone marrow has stabilised. - Your doctor will adjust your dose to one that is ideal for you. To do this, your doctor may
need to do some blood tests. Endogenous uveitis - The total dose each day is usually between 5 mg and 7 mg per kilogram body weight.
This is divided in two doses. Nephrotic syndrome - The total dose each day for adults is usually 5 mg per kilogram body weight. This is
divided in two doses. In patients with kidney problems, the first dose taken each day should not be more than 2.5 mg per kilogram body weight.
Severe rheumatoid arthritis - The total dose each day is usually between 3 mg per kilogram of your body weight and
5 mg per kilogram body weight. This is divided in two doses. Psoriasis and atopic dermatitis - The total dose each day is usually between 2.5 mg per kilogram of your body weight and
5 mg per kilogram body weight. This is divided in two doses. • In children:
Nephrotic syndrome - The total dose each day for children is usually 6 mg per kilogram body weight. This is
divided in two doses. In patients with kidney problems, the first dose taken each day should not be more than 2.5 mg per kilogram body weight.
Follow your doctor's instructions exactly and never change the dose yourself, even if you feel well. Switch from Sandimmun to Sandimmun Neoral You may have already been taking another medicine called Sandimmun soft gelatin capsules or Sandimmun oral solution. Your doctor may decide to change to this medicine, Sandimmun Neoral oral solution. • These medicines all contain ciclosporin as the active ingredient. • Sandimmun Neoral is a different, improved formulation of ciclosporin compared to
Sandimmun. Ciclosporin is absorbed into your blood better with Sandimmun Neoral and absorption is less likely to be affected by taking the medicine with food. This means that the levels of ciclosporin in your blood stay more constant with Sandimmun Neoral than with Sandimmun.
If your doctor changes you from Sandimmun to Sandimmun Neoral: • Do not go back to taking Sandimmun unless your doctor tells you to. • Following your transfer from Sandimmun to Sandimmun Neoral, your doctor will monitor you
more closely for a short time. This is because of the change in how ciclosporin is absorbed into your blood. Your doctor will make sure that you get the right dose for your individual needs.
100

• You may have some side effects. If this happens, tell your doctor or pharmacist. Your dose may need to be lowered. Never lower your dose yourself, unless a doctor has told you to.
If your doctor switches you from one oral formulation of ciclosporin to another After you change from one oral formulation of ciclosporin to another: • Your doctor will monitor you more closely for a short time. • You may have some side effects. If this happens, tell your doctor or pharmacist. Your dose may
need to be changed. Never change your dose yourself, unless a doctor has told you to. When to take Sandimmun Neoral Take Sandimmun Neoral at the same time every day. This is very important if you have had a transplant. How to take Sandimmun Neoral Your daily doses should always be taken in 2 divided doses. - For initial use, follow steps 1 to 9. - For subsequent use, follow steps 5 to 9. Starting a new bottle of Sandimmun Neoral oral solution 1. Lift the flap in the centre of the metal sealing ring.
2. Tear off the sealing ring completely.
3. Take off the black stopper and throw it away.
4. Push the tube unit with the white stopper firmly into the neck of
the bottle.
101

Measuring your dose 5. Choose the syringe depending on how much medicine you need
to measure: - For 1 ml or less of medicine, use the 1 ml syringe. - For more than 1 ml of medicine, use the 4 ml syringe. Push the nozzle of the syringe into the white stopper.
6. Pull up the plunger until you have drawn up the correct amount
of medicine. - The lower part of the plunger ring needs to be in front of
the mark on the syringe which shows the amount of medicine.
7. Push down and pull up the plunger a few times.
- This will get rid of any large air bubbles. It does not matter if there are a few tiny bubbles in the syringe. This will not affect the dose in any way.
Ensure that the correct amount of medicine is in the syringe. Then, take the syringe out of the bottle
8. Push the medicine out of the syringe into a small glass
containing liquid, preferably orange or apple juice. - Make sure that the syringe does not touch the liquid in
the glass. - Stir and drink the whole contents of the glass straight
away.
9. After use, wipe the syringe on the outside only with a dry tissue. - Then, put the syringe back in its cover. - Leave the white stopper and tube in the bottle. - Close the bottle with the cap provided.
How long to take Sandimmun Neoral Your doctor will tell you how long you need to take Sandimmun Neoral for. This depends on whether you are taking it after a transplant or for the treatment of a severe skin condition, rheumatoid arthritis, uveitis or nephrotic syndrome. For severe rash, the treatment usually lasts for 8 weeks. Keep taking Sandimmun Neoral for as long as your doctor tells you.
102

If you have questions about how long to take Sandimmun Neoral, talk to your doctor or your pharmacist. If you take more Sandimmun Neoral than you should If you accidentally take too much of your medicine, tell your doctor immediately or go to your nearest hospital emergency unit. You may need medical attention. If you forget to take Sandimmun Neoral • If you forget to take a dose, take it as soon as you remember it. However, if it is almost time for
your next dose, skip the missed dose. Then go on as before. • Do not take a double dose to make up for a forgotten dose. If you stop taking Sandimmun Neoral Do not stop taking Sandimmun Neoral unless your doctor tells you to. Keep taking Sandimmun Neoral even if you feel well. Stopping your treatment with Sandimmun Neoral may increase the risk of your transplanted organ being rejected. If you have any further questions on the use of this medicine, ask your doctor or pharmacist. 4. Possible side effects Like all medicines, this medicine can cause side effects, although not everybody gets them. Some side effects could be serious Tell your doctor straight away if you notice any of the following serious side effects: • Like other medicines that act on the immune system, ciclosporin may influence your body’s
ability to fight against infection and may cause tumours or other cancers, particularly of the skin. Signs of infection might be fever or sore throat.
• Changes in your sight, loss of coordination, being clumsy, memory loss, difficulty speaking or understanding what others say, and muscle weakness. These might be signs of an infection of the brain called progressive multifocal leukoencephalopathy.
• Brain problems with signs such as seizures, confusion, feeling disorientated, being less responsive, personality changes, feeling agitated, sleeplessness, changes to your sight, blindness, coma, paralysis of part or all of the body, stiff neck, loss of coordination with or without unusual speech or eye movements.
• Swelling at the back of the eye. This may be associated with blurred vision. It may also affect your sight because of the higher pressure inside your head (benign intracranial hypertension).
• Liver problems and damage with or without yellow skin and eyes, nausea, loss of appetite and dark urine.
• Kidney problems which may greatly reduce the amount of urine you produce. • Low level of red blood cells or platelets. The signs include pale skin, feeling tired, being
breathless, having dark urine (this is a sign of the breakdown of red blood cells), bruising or bleeding with no obvious reasons, feeling confused, feeling disorientated, being less alert and having kidney problems.
Other side effects include: Very common side effects: These side effects may affect more than 1 in 10 people. • Kidney problems. • High blood pressure. • Headache. • Shaking of your body which you cannot control.
103

• Excessive growth of body and facial hair. • High level of lipids in your blood. If any of these affects you severely, tell your doctor. Common side effects: These side effects may affect between 1 and 10 in every 100 people. • Fits (seizures). • Liver problems. • High level of sugar in your blood. • Tiredness. • Loss of appetite. • Nausea (feeling sick), vomiting, abdominal pain, constipation, diarrhoea. • Excessive hair growth. • Acne, hot flushes. • Fever. • Low level of white blood cells. • Feeling numb or tingling. • Pain in your muscles, muscle spasm. • Stomach ulcer. • Gum tissue overgrowing and covering your teeth. • High level of uric acid or patassium in your blood, low levels of magnesium in your blood. If any of these affects you severely, tell your doctor. Uncommon side effects: These side effects may affect between 1 and 10 in every 1,000 people. • Symptoms of brain disorders including sudden fits, mental confusion, sleeplessness,
disorientation, disturbance of vision, unconsciousness, sense of weakness in the limbs, impaired movements.
• Rash. • General swelling. • Weight gain. • Low level of red blood cells, low level of platelets in your blood which could increase the risk
of bleeding. If any of these affects you severely, tell your doctor. Rare side effects: These side effects may affect between 1 and 10 in every 10,000 people. • Nerve problems with numbness or tingling in fingers and toes. • Inflammation of the pancreas with severe upper stomach pain. • Muscle weakness, loss of muscle strength, pain in muscles of the legs or hands or anywhere in
the body. • Destruction of red blood cells, involving kidney problems with symptoms such as swelling of
the face, stomach, hands and/or feet, decreased urination, breathing difficulty, chest pain, fits, unconsciousness.
• Changes in menstrual cycle, breast enlargement in men. If any of these affects you severely, tell your doctor. Very rare side effects: These side effects may affect between 1 and 10 in every 100,000 people. • Swelling at the back of the eye which may be associated with an increase in pressure inside the
head and eyesight disturbances. If this affects you severely, tell your doctor. Other side effects with frequency not known: Frequency cannot be estimated from the available data. • Serious liver problems both with and without yellowing of the eyes or skin, nausea (feeling
sick), loss of appetite, dark coloured urine, swelling of the face, feet, hands and/or the whole body.
104

• Bleeding underneath the skin or purple skin patched, sudden bleeding with no apparent cause. • Migraine or severe headache often with feeling and being sick (nausea, vomiting) and being
sensitive to light. If any of these affects you severely, tell your doctor. If you get any side effects, talk to your doctor or pharmacist. This includes any possible side effects not listed in this leaflet. Additional side effects in children and adolescents There are no additional side effects to be expected in children and adolescents compared to adults. 5. How to store Sandimmun Neoral • Keep this medicine out of the sight and reach of children. • Do not use this medicine after the expiry date which is stated on the package. • Store at room temperature (15°C to 30°C). • Do not store in the refrigerator. Do not store below 20°C for more than 1 month. This is because
this product contains oils which can become solid at low temperatures. • If the medicine is put in the refrigerator by mistake, let it reach room temperature before using it
again. Flakes or small bits (sediments) in the medicine do not affect how the medicine works or how safe it is to use. The dose can still be measured correctly with the syringe.
• The content of the bottle is stable for 2 months after opening. After 2 months, you should use a new bottle.
• Do not throw away any medicines via wastewater or household waste. Ask your pharmacist how to throw away medicines you no longer use. These measures will help to protect the environment.
6. Contents of the pack and other information What Sandimmun Neoral contains • The active substance is ciclosporin. One ml oral solution contains 100 mg ciclosporin. • The other ingredients are: DL-alpha-tocopherol, ethanol anhydrous, propylene glycol, corn oil-
mono-di-triglyceride, macrogolglycerol hydroxystearate (Ph.Eur.)/polyoxyl 40 hydrogenated castor oil (USP).
What Sandimmun Neoral looks like and contents of the pack Sandimmun Neoral comes in the form of an oral solution. It is a clear, faintly yellow-brownish liquid. It is available in a 50 ml glass bottle, with two syringes for measuring the dose. • The 1 ml syringe is used to measure doses of 1 ml or smaller. Each mark on the syringe is
0.05 ml. This contains 5 mg of ciclosporin. • The 4 ml syringe is used to measure doses bigger than 1 ml and up to 4 ml. Each mark on the
syringe is 0.1 ml. This contains 10 mg of ciclosporin. Marketing Authorisation Holder and Manufacturer [To be completed nationally] {Name and address} {tel} {fax} {e-mail}
105

This medicinal product is authorised in the Member States of the EEA under the following names: {Name of the Member State} {Name of the medicinal product} {Name of the Member State} {Name of the medicinal product} This leaflet was last revised in {MM/YYYY} {month YYYY}. [To be completed nationally]
106