eating well for older people - the caroline walker trust · eating well for older people second...
TRANSCRIPT

Practical and nutritional guidelines for food in residential and nursing homes and for
community meals
REPORT OF AN EXPERT WORKING GROUP
THE CAROLINE WALKER TRUST
Eating well forolder people
SECOND EDITION

Practical and nutritional guidelines for food in residential and nursing homes and for
community meals
REPORT OF AN EXPERT WORKING GROUP
REPORT OF ANEXPERT
WORKING GROUP
THE CAROLINE WALKER TRUST
Eating well forolder people
SECOND EDITION

2
Acknowledgements
The Expert Working Group would like to thank DGAAHomelife, the Department of Health, and Tesco plc, forproviding the financial support which made the first edition ofthis report possible.
© The Caroline Walker Trust, 1995This edition printed in 2004. ISBN 1 897820 18 6First edition printed in 1995 (ISBN 1 897820 02 X)
The Caroline Walker TrustPO Box 61St Austell PL26 6YL
Registered charity number: 328580
Further copies of this report are available from:The Caroline Walker Trust22 Kindersley WayAbbots LangleyHerts WD5 0DQ
Price £15 (including postage and packing). Please make cheque payable to ‘The Caroline Walker Trust’.
Edited and produced by Wordworks, London W4 4DB.Design by Information Design Workshop.Illustrations by Frances Lloyd.
The text and tables contained in this report (except for materialreproduced with permission from other organisations) can bephotocopied by all those involved in providing food for olderpeople.
Also available:
The CORA Menu PlannerA computer program to help plan nutritionally balanced menusfor older people in residential and nursing homes. Includes adatabase of over 800 recipes. Available on CD ROM or 31/2”disks. Price £50. Send a cheque, payable to ‘The Caroline WalkerTrust’, to: The Caroline Walker Trust, 22 Kindersley Way, AbbotsLangley, Herts WD5 0DQ.
Eating Well for Older People with DementiaA good practice guide for residential and nursing homes andothers involved in caring for older people with dementia. Available from VOICES. Price £12.99. Send a cheque, payable to‘VOICES’, to: VOICES, Unicorn House, Station Close, Potters Bar,Herts EN6 3JW. Phone: 01707 651777.

Members of the Expert Working Group on NutritionalGuidelines for Food Prepared for Older People
These are the members of the Expert Working Group which produced the firstedition of this report. Their affiliations are as at 1995 when the first edition waspublished.
Anne Dillon Roberts (Chair) Director of Public Affairs, National Farmers Union of England and Wales; Trustee of TheCaroline Walker Trust
Dame Barbara Clayton Honorary Research Professor in Metabolism,University of Southampton
June Copeman Chair of the Nutrition Advisory Group for Elderly People, the British Dietetic Association; Senior Lecturer in Nutrition andDietetics, Leeds Metropolitan University
Dr Louise Davies Consultant in Gerontology Nutrition and Honorary Senior Lecturer, Royal FreeHospital School of Medicine, London
Mandy Downes Director of Food Services, Women’s Royal Voluntary Service
Dr Anthea Lehmann Consultant Geriatrician, Homerton Hospital,Hackney, London
Dorothy Newman National Chair, Advisory Body for Social Services Catering, Bradford
Maggie Sanderson Principal Lecturer in Nutrition, University of North London; Chair of The Caroline WalkerTrust
Professor Aubrey Sheiham Professor of Dental Public Health, University College, London
Kiran Shukla District Dietitian, Thameside Community NHS Trust, Essex
Elizabeth Walker Health Care Divisional Dietitian, Gardner Merchant, Northwich, Cheshire
Observers
Dr Petra Clarke Senior Medical Officer, Department of Health, London
Sylvia Stenhouse Matron/Manager, DGAA Homelife, Rush Court Nursing Home, Wallingford,Oxfordshire
Dr Jennifer Woolfe Senior Scientific Officer, Food Safety Directorate, Ministry of Agriculture,Fisheries and Food, London
The first edition of this report was researched by Dr Katia Herbst.This edition was researched and updated by Dr Helen Crawley.


Contents
Foreword 7
Summary and recommendations 9
Chapter 1 Why nutritional guidelines are needed 14
Chapter 2 Food prepared for older people: who provides it, and who eats it? 17Food prepared for older people in residential and nursing homesCommunity meals
Chapter 3 How a good diet can contribute to the health of older people 21How the body changes with ageingMalnutritionCommon health problems that can be improved by diet
Chapter 4 Nutritional requirements of older people 29
Chapter 5 Nutritional guidelines for food prepared for older people 40Food prepared for people in residential and nursing homesCommunity meals
Chapter 6 Examples of menus which meet the nutritional guidelines 46Example menus for older people living in residential or nursing homesExample menus for community meals
Chapter 7 Nutritional assessments 51How to identify older people who might be at risk of malnutritionAssessing food provision
Chapter 8 Exciting the appetite 60Providing variety and choiceTiming and frequency of mealsFood presentationSocial occasionsPhysical activity
Appendix 1 Recommendations of the COMA report on The Nutrition of Elderly People 63
Appendix 2 Care Homes for Older People: National Minimum Standards 64
Appendix 3 Good sources of nutrients 65
Appendix 4 Portion guide 69
Appendix 5 Sample nutritional assessment methods for use in the community 70
Appendix 6 Useful addresses and further reading 74

6
List of Tables and Figures
Table 1 Nutritional requirements of older people 30
Table 2 Nutritional guidelines for food prepared for older people in residential or nursing homes 41
Table 3 Nutritional guidelines for community meals for older people 44
Table 4 Example menus for older people living in residential or nursing homes 47
Table 5 Example menus for community meals for older people 49
Table 6 Examples of community meals suitable for older people from Asian and Afro-Caribbean backgrounds 50
Table 7 Weight loss score 56
Figure 1 Estimating height from ulna length 52
Figure 2 Measuring from mid upper arm circumference 53
Figure 3 The Malnutrition Universal Screening Tool (MUST) 54
Figure 4 BMI score (and BMI) 55

7
Foreword The Caroline Walker Trust isdedicated to the improvementof public health by means of
good food. Established in 1988 tocontinue the work of Caroline Walker,and in particular to protect the qualityof food, it is a charitable trust whosework is wholly dependent on grantsand donations.
The Trust has produced a number ofpublications, training materials andcomputer packages which providepractical guidance on eating well forthose who care for vulnerable peoplein our society. The Trust’s first ExpertReport Nutritional Guidelines forSchool Meals,1 published in 1992, hasbeen widely used as the basis forquantitative standards for school mealsand is provided as guidance by theDepartment for Education and Skills inits nutritional guidelines for schoollunches.2 Practical and nutritionalguidelines have also been produced forunder-5s in child care3 in 1998, and forlooked after children and youngpeople4 in 2001. More informationabout these documents and theiraccompanying training packs andsoftware can be found on the CarolineWalker Trust website: www.cwt.org.uk.
In 1995 the Trust produced the firstedition of this publication – EatingWell for Older People.5 Members of theworking group responsible for thatreport were also involved in theVOICES report Eating Well for OlderPeople with Dementia,6 produced in1998. A computer program called theCORA Menu Planner,7 produced inresponse to the publication of the firstedition of Eating Well for Older People,has provided a practical tool for thoseplanning menus for older people and isnow extensively used across the UK.
Since this report was first published, ithas been widely used in residential andnursing homes, and in the community,both to raise the profile of eating wellfor older people and to providepractical guidance for those who workin this sector and for those who adviseand support them.
When the first edition of the report waspublished in 1995, the last nationalsurvey of the nutrition of older peopleavailable to the Expert Working Groupwas over 20 years old. The Committee
on Medical Aspects of Food andNutrition Policy (COMA) hadrecognised this lack of information intheir reports on Dietary ReferenceValues8 and on the Nutrition of ElderlyPeople.9 The Government respondedto COMA’s recommendations, andcommissioned a nutrition survey ofpeople aged 65 years and over inGreat Britain as part of the NationalDiet and Nutrition Survey (NDNS)programme. The results werepublished in 1998,10, 11 after the firstedition of this report had beenpublished. More recently, theGovernment has also published aNational Service Framework for olderpeople.12
This report on Eating Well for OlderPeople remains in high demand. It isnow five years since the NDNS surveyof people aged 65 years and over waspublished. The Trust recognised that itwould be appropriate to ensure thatthe report took account of this morerecent information and of the NationalService Framework for older people,and therefore decided to produce anew edition.
The Trust is delighted that many of itsrecommendations have beenincorporated into the new NationalMinimum Standards for Care Homesfor Older People13 and this new reportwill hopefully be a good starting pointfrom which nutritional standards canbe further improved.
The Trustees would like to thank theoriginal Expert Working Group, andparticularly Anne Dillon Roberts theChair, for their work in compiling thefirst edition of this report. They wouldalso like to thank Dr Helen Crawleyand Rosie Leyden for updating thisreport and June Copeman and AnitaBerkley for their useful comments onthe text for this edition.
We hope that this second edition ofthis report will be as well used as itspredecessor and provide practicaladvice to all those who have animportant role to play in the care ofolder people.
Professor Martin WisemanChair, Caroline Walker Trust

Foreword
8
References
1 Sharp I. 1992. Nutritional Guidelinesfor School Meals. Report of an ExpertWorking Group. London: The CarolineWalker Trust.
2 Available from: www.dfes.gov.uk
3 The Caroline Walker Trust. 1998. EatingWell for Under-5s in Child Care.London: The Caroline Walker Trust.
4 The Caroline Walker Trust. 2001. EatingWell for Looked After Children andYoung People. London: The CarolineWalker Trust.
5 The Caroline Walker Trust. 1995. EatingWell for Older People. 1st edition.London: The Caroline Walker Trust.
6 VOICES. 1998. Eating Well for OlderPeople with Dementia. London:VOICES.
7 The Caroline Walker Trust. CORA MenuPlanner. London: DGAA Homelife.Available from The Caroline WalkerTrust (www.cwt.org.uk).
8 Department of Health. 1991. DietaryReference Values for Food Energy andNutrients for the United Kingdom.Report on Health and Social SubjectsNo. 41. Report of the Panel on DietaryReference Values of the Committee onMedical Aspects of Food Policy.London: HMSO.
9 Department of Health. 1992. TheNutrition of Elderly People. Report onHealth and Social Subjects No. 43.Report of the Working Group on theNutrition of Elderly People of theCommittee on Medical Aspects ofFood Policy. London: HMSO.
10 Finch S, Doyle W, Lowe C, Bates CJ etal. 1998. National Diet and NutritionSurvey: People Aged 65 Years andOver. Volume 1: Report of the Diet andNutrition Survey. London: TheStationery Office.
11 Steele JG, Sheiham A, Marcenes W,Walls AWG. 1998. National Diet andNutrition Survey: People Aged 65Years and Over. Volume 2: Report ofthe Oral Health Survey. London: TheStationery Office.
12 Department of Health. 2001. NationalService Framework for Older People.London: The Stationery Office.Available from: www.dh.gov.uk
13 Department of Health. 2002. CareHomes for Older People: NationalMinimum Standards. London: TheStationery Office. Available from:www.dh.gov.uk

9
Summary and recommendations
Chapter 1 Why nutritional guidelines are needed
The Caroline Walker Trust Expert Working Group regards the provision ofcommunity meals – including meals delivered to the home and meals served ata lunch club or day centre – as a vital component of community care.
Adequate nutritional standards of food in residential care accommodation –including both residential and nursing homes – are crucial to the well-being ofresidents and patients.
The Working Group makes the following recommendations:
• The nutritional guidelines in this report (see Tables 2 and 3 onpages 41 and 44) should become minimum standards for foodprepared for older people in residential care accommodation andfor community meals. Cost considerations should not overridethe need for adequate nutritional content in the planning andpreparation of food for older people.
• Local authorities should adopt these nutritional guidelines andinsist on them being maintained in residential and nursing homeswith which they contract for long-term care, and in the provisionof community meals.
Chapter 2 Food prepared for older people: who providesit, and who eats it?
In 2001, 341,200 older people lived in residential care accommodation and afurther 186,000 people in nursing homes. About a quarter of people over 85years of age live in long-stay care. The percentage of the population in long-term care has remained steady but the actual number has been rising becauseof the increase in population in these age groups. That growth is set to continuebecause of the particularly rapid increase in the number of over-85s.
Many older people in residential care accommodation are undernourished,either through previous poverty, social isolation, or personal or psychologicalproblems, or due to the effects on appetite of illness or medication.
Since this report was originally published there have been a number ofrecommendations made relating to food service to older people in residentialand nursing care. These recommendations are welcomed but there is still aneed to provide practical information to managers of residential or nursinghomes on how they can achieve appropriate nutritional content in the foodthey serve.
Community meals, whether delivered to people’s own homes or eaten in lunchclubs or day centres, are a very important source of nutritious food for olderpeople living in their own homes and unable to cook adequately forthemselves.
The Working Group makes the following recommendations:
• Residential and nursing homes applying for registration should berequired to meet the nutritional guidelines for food prepared forolder people as part of the registration process. Monitoring of thenutritional standard of meals should be carried out regularly, and

Summary and recommendations
10
homes which do not meet the guidelines should receiveappropriate advice and help to meet the standards, or forfeitregistration.
• In residential care accommodation, at least £18 per resident perweek (2004 prices) should be spent on food ingredients to ensurethat food of sufficient nutritional content can be made available.
• Individuals, their relatives or advocates should enquire about aprospective home’s commitment to nutritional standards andshould ask how much money per resident per week is spent onfood ingredients.
• Those providing community meals need to take into account theneeds and wishes of older people from black and ethnicminorities who do not have access to an appropriate lunch club.
• Lunch clubs should be developed for older people in any settingwhere it is already the custom for older people to gather.
Chapter 3 How a good diet can contribute to the healthof older people
The ageing process affects people at different rates. A good diet and physicalactivity help to minimise potential health problems and accelerate recoveryfrom episodes of illness.
As activity lessens, calorie requirements fall. However, if insufficient food iseaten, the level of nutrients in the diet can become dangerously low, leading toa vicious circle of muscle loss, even less activity, and even lower appetite.
Mouth problems and swallowing difficulties may also lead to low food intake.The importance of regular care of the teeth and mouth is stressed.
There are more underweight than overweight older people and, in old age,being underweight poses far greater risks to health than being overweight.
Poor nutrition can contribute to a number of health problems including:constipation and other digestive disorders; anaemia; diabetes mellitus; muscleand bone disorders including osteoporosis, osteomalacia and osteoarthritis;overweight; and coronary heart disease and stroke. Poor diet may alsocontribute to other health problems such as declining mental health, changes tothe nervous system and the immune system, cataract and some cancers.
In addition to the nutritional guidelines given in Chapter 5, the Working Groupmakes the following recommendations:
• Older people should be encouraged to undertake regular physicalactivity, such as walking, as this strengthens and builds upmuscle and bone, and increases calorie requirements, whichincreases appetite. Even chair-bound people should beencouraged to do regular leg and arm movements.
• Facilities should be provided for regular dental check-ups. Thismeans taking people to the dental surgery, either from their ownhomes or from residential homes, or having community dentistsvisit the home.
• Architects designing accommodation for older people should beencouraged to take account of the need for residents to haveregular exposure to sunlight, which is a source of vitamin D.Features could include windows that allow UV light to passthrough the glass, sheltered alcoves on the south side of

Summary and recommendations
11
Chapter 5 Nutritional guidelines for food prepared forolder people
The Dietary Reference Values are translated into nutritional guidelines for foodprepared for older people in residential care accommodation and forcommunity meals.
The Working Group recommends that:
• The average day’s food, over a one-week period, for people livingin residential care accommodation, should meet the COMAreport’s Estimated Average Requirement for energy and theReference Nutrient Intakes for selected nutrients. Quantifiednutritional guidelines for food prepared for older people inresidential or nursing homes are given in Table 2 on page 41.
In relation to community meals, the Working Group recommends that:
• The average community meal should provide a minimum of 33%of the Dietary Reference Values prepared by COMA in 1991,except for energy and certain key nutrients, which should beprovided at higher levels.
• In view of the common occurrence of undernutrition inhousebound older people living in their own homes, providersshould increase the energy, calcium, iron and zinc content ofcommunity meals to 40% of the Dietary Reference Values, and thefolate and vitamin C content to 50%. Quantified nutritionalguidelines for community meals are given in Table 3 on page 44.
• Research is needed to find out how much of the meal is eaten bythose who receive community meals, and how the service canbest meet the needs of its users. Alternative methods of providingfood – such as smaller meals and snacks which together comprisethe nutrients more usually associated with a conventional meal –also need to be evaluated.
Chapter 4 Nutritional requirements of older people
This chapter discusses the intake levels for food energy and nutrients andconcludes that:
• The Dietary Reference Values prepared by COMA (the Committeeon the Medical Aspects of Food Policy) in 1991 should be used asthe basis for the nutritional guidelines for food prepared for olderpeople.
buildings, and well-paved paths with hand rails and no steps.
• Older people living in residential and nursing homes who rarelygo outside are likely to need vitamin D supplements and shouldconsume a diet which provides sufficient calcium. Advice onsupplements should be taken from a GP.

Summary and recommendations
12
Chapter 6 Examples of menus which meet thenutritional guidelines
This chapter gives examples of menus both for meals prepared for older peoplein residential care accommodation and for community meals, to demonstratethat it is possible to meet the nutritional guidelines proposed in Chapter 5,easily and cost-effectively.
Chapter 7 Nutritional assessments
The importance of nutritional assessment is discussed.
The Working Group makes the following recommendations:
• Vulnerable older people living in the community should have anutritional assessment, and the results should help inform thedesign of the person’s care package. The assessment could becarried out by a member of the care management team or theprimary health care team.
• All older people entering residential care accommodation shouldhave their food and fluid needs assessed in the first week afteradmission, and should be monitored regularly thereafter.
• All residential and nursing homes should have weighing scales,preferably sitting scales, for monthly weight checks. The scalesshould be checked regularly.
• The weight of each resident or patient should be recorded in theperson’s care plan at least once a month.
• Care managers and service providers need to ensure that routinereassessments are made. All people found to be at risk in theinitial screening should be reassessed at frequent intervals.Thereafter, reassessments will be necessary with changingcircumstances.
Chapter 8 Exciting the appetite
The importance of appetite should be given a high profile. It is no goodproducing nutritious meals unless they are eaten.
The Working Group makes the following recommendations:
• Older people living in residential care accommodation orreceiving community meals should be offered a variety and somechoice of food.
• Records of the food preferences of each person should be kept.
• Every effort should be made to make the eating environment asattractive and as culturally appropriate as possible.
• In residential care accommodation, residents should beencouraged to invite guests in either for a simple meal, or for teaor coffee.
• Residents should be encouraged to go on trips and outingsoutside the residential care home. This may stimulate appetite byproviding exercise, fresh air and a change of food choice.

Summary and recommendations
13
• Snacks should be provided in between more formal mealtimes or,in the case of community meals, be delivered with the main meal,thereby ensuring that, if they wish, older people can eat a little ata time, but more frequently.
• Advice should be sought from an occupational therapist orspeech and language therapist, for those who may need specialaids or help with eating or drinking.
• Physical activity routines, even of a very modest nature, shouldbe established for all older people living in residential careaccommodation.
• Staff or volunteers at lunch clubs should encourage physicalactivity among older people, either by providing information orby organising simple activities at the club.

Chapter 1
Whynutritionalguidelinesare needed
14
The number of older people inthe UK is rising rapidly, dueto a surge in the birth rate
after the First World War combinedwith a much reduced rate of infantmortality and far better health caresince the introduction of the NationalHealth Service.
Life expectancy has now risen toover 75 years for men and over 80years for women, and continues torise, although the rate of increase ismore gradual than that seen over thefirst 70 years of the last century.1
However, while life expectancy hasincreased, years of disability-free lifehas not. The total prevalence ofserious disability among thepopulation aged over 65 years isestimated at 16%.2 A quarter of over-80-year-olds living at home and 70%of over-80-year-olds in residentialcare report serious long-standingdisability.2
These factors have combined tocreate a rapidly growing careindustry of residential careaccommodation – including bothresidential homes and nursing homes– and an increased demand for carein people’s own homes. TheCommunity Care Act which cameinto force in 1993 had, as one of itsmain objectives, to enable people tostay in their own homes for as longas possible. This has beenaccompanied by a decrease in theproportion of older people inresidential and nursing care over thepast 10 years, particularly among thevery old, with 5% fewer of thoseaged over 85 now in residential ornursing care. The absolute numbersof older people in residential care,however, is increasing with theageing population in the UK. In 2001there were 1.1 million people aged85 and older in the UK – three timesas many as in 1961.3 Projections fromrecent census data suggest that, overthe next 30 years, the number ofpeople aged 65 and over will exceedthe numbers aged under 16 by 2014,and those in the over-85 age groupwill more than double. Thisincreasingly ageing populationmeans that the demand for long-termresidential care accommodation will
remain strong. There will also be anincreasing demand for home-basedcare, including both the delivery ofmeals and support with eating wellfor dependent people in their ownhomes.
The body starts to age from about theage of 20. Many people reach ‘a ripeold age’ still alert and taking greatenjoyment from life. The rate atwhich people age and become frailor disabled is influenced by theirgenetic make-up. However, manyoutside influences – such asinvolvement in the local communityor special interest group, hobbies,the family or social circle – all play animportant part in maintainingphysical and mental resilience andenjoyment of life.4
This report focuses on the dailyinfluence of diet and activity on olderpeople. Food and eating bring shapeto a day and facilitate socialinteraction, as well as providingessential energy and nutrients. Muchof the evidence collated in the firstedition of this report was taken fromthe 1992 Department of HealthCommittee on Medical Aspects ofFood Policy (COMA) report on TheNutrition of Elderly People.5 Thisreport summarised research evidenceat that time and maderecommendations on how olderpeople can maintain adequatenutritional status. While new data
Food and eating bringshape to a day and
facilitate social interaction,as well as providingessential energy and
nutrients.

Chapter 1 Why nutritional guidelines are needed
15
have been reported in many areas ofnutrition and health since then,including a National Diet andNutrition Survey of people aged 65years and over,6, 7 a further review ofthe nutrition of older people has notbeen completed, and therefore therecommendations of the COMAreport on The Nutrition of ElderlyPeople are still reproduced in thissecond edition (see Appendix 1).
When this report was first publishedin 1995, there were no clearguidelines on food and nutrition forpeople in residential care. The Trustidentified a need for practicalguidelines on nutrition for use bythose who are responsible forcatering for older people either inresidential care accommodation or bythe provision of community meals,including meals delivered to thehome and meals served at lunchclubs and day centres. The Trustbrought together an Expert WorkingGroup to produce this report (seepage 3 for a list of members of theExpert Working Group) and ispleased to find almost 10 years laterthat the recommendations made thenhave been widely incorporated intoguidance in other publications.
The Caroline Walker Trust isdelighted that several recent policyreviews and recommendations haveincluded food and nutrition and aimto improve the health and well-beingof older people in the UK. TheNational Service Framework (NSF)for Older People, launched in 2001,relates particularly to hospital andprimary care initiatives.8 Of mostsignificance to the residential caresector are the National MinimumStandards for Care Homes for OlderPeople9 which came into force in2002, and the Scottish National CareStandards: Care Homes for OlderPeople,10 also operational from 2002.Both sets of standards provide clearguidelines relating to food choiceand food service as well as arequirement for nutritionalassessment of residents. A summaryof the standards for England andWales which relate to food andnutrition is given in Appendix 2.Scottish nursing home care standards
go further in their requirement thatall nursing homes demonstrate thattheir menus meet specified quantifiednutritional guidelines – a requirementwhich is particularly welcomed bythe Caroline Walker Trust.11
The recognition that good nutritionand good food are essential for boththe current and future health andwell-being of older people inresidential care is very welcome butthe need for clear, scientificallyaccurate and practically useful adviceon how to implement theserecommendations remains essential.There is still much to be done toencourage and support residentialand nursing homes to fulfil thesenew guidelines and to effectivelyencourage an increasingly frail,elderly population group to eat well.The nutritional contribution ofcommunity meals and meals servedin lunch clubs and day centres willbecome ever more important asincreasing numbers of frail, olderpeople remain in their own homes.
The aims of this updated reportremain the same as those of the firstedition:
• To provide clear, referenced,background information showingthe relationship between goodnutrition and health among olderpeople.
• To look at the current nutritionalintake of older people andhighlight potential inadequacies.
• To provide practical guidelines to
enable caterers, manager/matrons,cooks/chefs, residential caremanagers and managers of servicesproviding meals at home, todevelop suitable menus to achievea good nutritional balance in thefood they provide and to showhow to develop this informationinto practical action.
• To act as a resource document forthose working for better standardsof nutrition both for people inlong-term residential or nursingcare and for those in receipt ofcommunity meals.
The Working Group recognises thesevere financial pressures on serviceproviders. It regards the provision ofcommunity meals as a vitalcomponent of community care. Thenutritional standard of food inresidential care accommodation iscrucial to the well-being of residentsand patients. The Working Grouphopes that the nutritional guidelinescontained in this report becomeminimum standards, and that costconsiderations do not override theneed for adequate nutritional contentin the planning and preparation offood for older people. Itrecommends that local authoritiesshould adopt the nutritionalguidelines in this report and shouldinsist on them being maintained inresidential and nursing homes withwhich they contract for long-termcare, and in the provision ofcommunity meals.
The nutritional standard of food in residential careaccommodation is crucial to the well-being of
residents and patients.

Chapter 1 Why nutritional guidelines are needed
16
References
1 Office for National Statistics. 2003.Social Trends. Available from:www.ons.gov.uk
2 Department of Health. 2000. HealthSurvey for England: The Health ofOlder People. Available from:www.dh.gov.uk/public/healtholderpeople200press.htm
3 Office for National Statistics. 2001.Census data. Available from:www.ons.gov.uk/census
4 Glass TA, Mendes de Leon C, MarottoliRA et al. 1999. Population based studyof social and productive activities aspredictors of survival among elderlyAmericans. British Medical Journal;319: 478-83.
5 Department of Health. 1992. TheNutrition of Elderly People. Report ofthe Working Group on the Nutrition ofElderly People of the Committee onMedical Aspects of Food policy.London: HMSO.
6 Finch S, Doyle W, Lowe C, Bates CJ etal. 1998. National Diet and NutritionSurvey: People Aged 65 Years andOver. Volume 1: Report of the Diet andNutrition Survey. London: TheStationery Office.
7 Steele JG, Sheiham A, Marcenes W,Walls AWG. 1998. National Diet andNutrition Survey: People Aged 65Years and Over. Volume 2: Report ofthe Oral Health Survey. London: TheStationery Office.
8 Department of Health. 2001. NationalService Framework for Older People.London: The Stationery Office.Available from: www.dh.gov.uk
9 Department of Health. 2002. CareHomes for Older People: NationalMinimum Standards. London: TheStationery Office. Available from:www.dh.gov.uk
Recommendations• The nutritional guidelines in this report (see Tables 2 and
3 on pages 41 and 44) should become minimumstandards for food prepared for older people in residentialcare accommodation and for community meals. Costconsiderations should not override the need for adequatenutritional content in the planning and preparation of foodfor older people.
• Local authorities should adopt these nutritional guidelinesand insist on them being maintained in residential andnursing homes with which they contract for long-termcare, and in the provision of community meals.
10 Scottish Executive. 2002. National CareStandards: Care Homes for OlderPeople. Edinburgh: Scottish Executive.Available from: www.scotland.gov.uk
11 NHS MEL (1999) 54 section 6 (ScottishExecutive document) on NursingHomes Scotland Care Standards forNutritional Care.

Chapter 2 Food prepared for older people: who provides it, and who eats it?
17
Chapter 2
Foodprepared for olderpeople:whoprovides it,and whoeats it?
This chapter gives background information on foodprepared for older people in residential homes andnursing homes, and on community meals. In this report,the term ‘community meals’ includes meals delivered topeople’s homes, meals provided for people living insheltered accommodation, and meals served in lunchclubs.
Food prepared forolder people inresidential andnursing homes
Who lives in careaccommodation?There are approximately 9.3 millionpeople aged over 65 years in the UK(2001 census figures),1 of whom 4.4million are aged over 75 years and1.1 million are aged over 85 years. In2001, 341,200 older people lived inresidential care accommodation anda further 186,800 people in nursinghomes – in 24,100 registered homesand 5,700 nursing homes, clinics andprivate hospitals.2 About a quarter ofpeople over 85 years of age live in aresidential or nursing home or along-stay hospital.3 The number ofolder people in the UK, particularlythe over-85s, is set to risedramatically as people live longer,and it is estimated that numbers willgo on increasing rapidly, peaking atover 3 million over-85-year-olds bythe year 2056.3
In 2001, 92% of all homes and 85% ofplaces in residential care homes wereprovided by the independent sector.2
After a rise in the number of places inresidential care accommodation inthe 1990s, between 2000 and 2001there were decreases in the numberof homes and the number of placesof around 700 (3%) and 4,700 (1%)respectively. This particularly affectedthe South East where 200 homes and1,000 places have been lost.2
More recent figures for 2001-02suggest that the number of placesavailable continues to fall as both the
number of new care homesdeveloped slows and the demand forplaces from local authorities declines.This is due both to an increasedattempt by local authorities to keepolder people in their own homes andto a reduction in the number ofresidents eligible with preservedrights to income support. BetweenNovember 2000 and November 2001the number of care home residentsfunded by either local authorities orincome support fell by 8,000.3 Thebiggest increase in provision hasbeen in independent sector placesfor people with mental healthproblems, with 15,000 new placescreated between 1996 and 2001.4
The net effect of these changesmeans that those in residential andnursing care are increasingly frail andvulnerable, and unable to liveindependently in their own homeseven with substantial support. Datafrom the Health Survey for Englandpublished in 2000 reported thatthree-quarters of all residents inprivate and voluntary careaccommodation are women. It alsoreports that 69% of men and 70% ofwomen in residential care arereported to have serious or multipledisabilities.5 In care homes the mostcommonly reported type of seriousdisability is locomotor disability,affecting 65% of older people. Justover a half of residents reportedpersonal care disability and almost aquarter reported communication andhearing disability. The Health Surveyfor England also reported that olderpeople in residential accommodationare more likely to have a long-standing illness, to have consulted aGP in the past two weeks or to haveexperienced a major accident in thepast six months compared with those

Chapter 2 Food prepared for older people: who provides it, and who eats it?
18
of a similar age living in their ownhomes. It is difficult to estimate thelevel of mental illness amongresidential care home residents, butthe Health Survey for Englandreported that while about 18% ofresidents had scores in cognitivefunction tests which suggesteddifficulties, a further 40% wereincapable of completing theinterview, suggesting that about halfof all residents may have some formof dementia. There are currently750,000 people in the UK diagnosedwith dementia, and 1 in 5 peopleaged over 80 will develop thedisease.6
The older, more frail and moredisabled population of older peoplenow in residential care means thatthe majority are highly dependent,with many requiring maximum care.There is evidence that many olderpeople living in residential andnursing care are clinicallyundernourished, with data from theHealth Survey for England suggestingthat up to 20% of people inresidential homes are malnourishedcompared with 1 in 7 elderly peoplein Britain overall.5
There are several reasons for this:
• Older people often enterresidential care after a period ofpoverty, social isolation, personaland psychological problems anddifficulty in preparing their ownmeals.
• Illness – which can increase theneed for calories but does notincrease appetite – and the effectsof medication often play a role.
• Some older people may havedifficulties in chewing andswallowing, and insufficientsupport may be available to helpthose with eating difficulties to eatwell.
• Some residents may not like thefood that has been prepared forthem.
• Older people with dementia mayhave a number of difficultiesrelated to physical, physiologicaland emotional/cognitive disease-related changes which impact ontheir ability to eat well.7
Catering regulationsThe catering in residential carehomes is undertaken either by thehome itself, by the local authoritycatering services or by a contractcaterer. The National MinimumStandards for Care Homes for OlderPeople8 which came into force in2002 provide new standards for allaspects of care, including issuesaround food and drink, and it isstated that residents “should receivea wholesome, appealing balanceddiet in pleasing surroundings attimes convenient to them”. Guidanceon how this can be achieved is givenin nine individual standards outlinedin Appendix 2. (This Caroline WalkerTrust report is included in thebibliography of the NationalMinimum Standards document as asource of guidance.) While theacknowledgement of the importanceof good food in residential carehomes in the standards is welcomed,the regulations still do not define thenutritional content of meals neededto sustain and improve the health ofresidents. The Working Group whichproduced the first edition of thisCaroline Walker Trust report believedthat the quantitative nutritionalguidelines it recommended shouldbe adopted by all social servicesdepartments and health authorities asthe basis for registration andinspection of homes, and thisremains the case in this secondedition.
It is recognised that many residentialcare homes have made enormousstrides in improving the food andnutrition of residents, and manyhomes use this report and the CORAMenu Planner software developed toaid the implementation of thenutritional recommendations (see
page 46). However, it is recognisedthat improving nutritional statusamong residents requires a multi-disciplinary approach, with inputfrom community dietitians andcommunity speech and languagetherapists as well as increased stafftraining for residential home workersin supporting good nutrition.
It has been reported that for olderpeople food and nutrition remain apriority among the factors theyassociate with good personal care,and people aged 85 and over andthose with disabilities ranked foodand nutrition as the most importantaspect of their personal care.9
Catering costsLittle new data about the spendingon food in residential and nursinghomes has been published since thefirst draft of this report. While thetotal cost of providing residential careis a subject of much debate andcontroversy, the majority of costs arefor staff and buildings, with estimatesfor food usually included with allother non-staffing costs. In theprevious report, based on theWorking Group’s own research, itwas suggested that in 1994 it wouldbe difficult to provide food ofsufficient nutritional content if lessthan £15 per resident was spent onfood ingredients. Allowing forincreased food costs, it would beprudent to increase that estimate to aminimum of £18 per resident perweek (at 2004 prices). It should alsobe acknowledged, however, that thecosts of improving nutrition involvemore than just the cost of the food,since encouraging eating well alsorequires staff time and training.
The Working Group recommendsthat individuals, their relatives oradvocates should enquire about aprospective home’s commitment tonutritional standards and should askhow much money per resident perweek is spent on food ingredients.
It is recognised thatimproving nutritionalstatus among residents
requires a multi-disciplinary approach.

Chapter 2 Food prepared for older people: who provides it, and who eats it?
19
Community meals
Meals delivered topeople’s homesIt is estimated that 5% of elderlypeople in their own homes cannotcook a main meal, and that 1 in 12people receive community meals,and 1 in 4 receive home help.10
Others are referred to lunch clubs orhave help from family and friends. In2001, 195,000 older people receivedcommunity meals (often called‘meals-on-wheels’) in their ownhomes at an average cost of £13.50per person per week.11 Communitymeals are available to older peoplewho cannot shop for, cook orprovide a hot main meal forthemselves. They are organised bylocal authorities through their owncatering resources, from privatecontractors and from the WRVS,which delivers 9 million meals a year.Clients are referred to the appropriatecommunity meals scheme by socialservices through doctors, districtnurses, health visitors, shelteredhousing managers and socialworkers, following an assessment todetermine how many meals a clientis eligible for. This can vary fromonce or twice a week to every day,with 7-days-a-week services usuallyreserved for those with no relativesliving in the immediate area. Clientspay to cover some of the cost of themeal, which usually consists of amain course and a pudding. Theprice paid varies in each area but isgenerally around £2.10 per meal.12
The delivery of community mealsvaries depending on both thecontract with the provider and thewishes of the client. Traditionally ahot meal is delivered daily atlunchtime, but increasingly frozenmeals are delivered weekly or every
two weeks for regeneration daily bythe client in a microwave.
The importance of home careservices has increased as the numberof vulnerable older people remainingin their own homes increases, andthere is a need for research toevaluate how changes in serviceprovision for community meals iscatering for the needs of thisvulnerable group.
Meals provided for peoplein shelteredaccommodationSheltered accommodation usuallytakes the form of self-contained flatsor bungalows with a warden on callfor emergencies. There are about500,000 sheltered accommodationunits in England alone and about 5%of older households live in shelteredaccommodation.13 Very shelteredhousing schemes with accommodationand services similar to shelteredaccommodation but which also offertwo cooked meals a day (lunch andtea) are being established around theUK. Residents are able to eat theirtwo main meals in a communaleating area and prepare additionalfood and drinks in their ownaccommodation.
Current legislation requires olderpeople themselves to bear much ofthe cost of services in shelteredaccommodation and many areprepared to do so in return for themix of independence and securitythat this type of housing provides.There are little recent data on foodintake among older people in thistype of accommodation, but earlierstudies have shown that poornutrition was widespread. In a two-year study of older people living insheltered accommodation inScotland, almost all the tenantssurveyed were deficient in somevitamins and 41% were below theacceptable weight for their height.14
Women were at greater risk than menand 22% of residents could not easilyprepare their own meals. Those whoattended lunch clubs generally hadfewer nutritional deficiencies. It islikely that older people on low
incomes are at greater risk ofundernutrition and all those involvedin supporting older people in thecommunity should be alert to this.Residents in very shelteredaccommodation have been found tohave widely varying dietary intakesboth from the food eaten in theirown flats and from the mealsprovided for them. The communalmeals may provide the majority ofthe daily food eaten for veryvulnerable residents.15
Cooking and cateringarrangements
People living in shelteredaccommodation may have their ownfacilities for cooking and preparingfood. The amount of help they getwith cooking or preparing their fooddepends on the facilities built intothe sheltered accommodationcomplex and on the role of thewarden. Some complexes havecommunal eating areas, and somehave kitchens where food can beprepared for communal eating. Notall complexes have wardens who areallowed to or are prepared toprovide such a service.
Residents also have access to theservices offered to other peopleliving in their own homes. Forexample, they may have mealsdelivered to them once or twice aweek or more frequently. Somecomplexes have communal orindividual freezers and microwaveovens, allowing for frozen meals tobe delivered in bulk. Lunch clubsmay be provided, or at leastorganised, by the warden inconjunction with a local religious orvoluntary organisation or socialservices department (see below).
Meals served in lunchclubsLunch clubs are places where olderor disabled people living in theirown homes can go to have a mealprepared for them and served in thecompany of other people. They areorganised by a range of voluntaryorganisations, black, ethnic andreligious groups and statutoryauthorities – both through social
The community mealsservice is an importantmeans of encouraging
people to remainindependent and in theirown homes for as long as
possible.

Chapter 2 Food prepared for older people: who provides it, and who eats it?
20
services departments and throughlocal health authorities.
It is difficult to collect statistics on thetotal number of lunch clubs in theUK or on the number of people whouse them. In 2003, the WRVSestimated that it ran 1,000 socialclubs in the UK, providing meals orrefreshments for approximately40,000 club members. Data from theGeneral Household Survey of peopleaged over 65 years in 1998-99reported that 11% of older peopleliving alone visited lunch clubscompared with only 2% of those wholived with others.10
Black and ethnic lunch clubs makean important contribution to the well-being of older people from thesegroups. However, such lunch clubsare only provided where there areenough people locally to justifyspecial arrangements. Thoseproviding community meals need totake into account the needs andwishes of those older people fromblack and ethnic minorities who donot have access to an appropriatelunch club.
The importance of lunch clubs to theoverall diet of older people (as wellas the social benefits to be derivedfrom going out and being withothers) has been recognised fordecades. While some older peoplemay choose to eat alone, for otherseating meals alone makes eatingseem more like an obligation than apleasurable activity, and can result ina lack of interest in food.
Lunch clubs should be developed inany appropriate setting. For example,one company allows their pensionersand guests to use the company’ssubsidised canteens, therebyproviding an invaluable service to thelocal community at a negligibleincrease in overhead cost. TheWorking Group suggests that largeemployers consider this as part oftheir contribution to their localcommunities. In addition, foodretailers, who already subsidisetransport to their supermarkets orsuperstores which already havecatering facilities, could considersetting up subsidised lunch clubs.
Recommendations• Residential and nursing homes applying for registration
should be required to meet the nutritional guidelines forfood prepared for older people as part of the registrationprocess. Monitoring of the nutritional standard of mealsshould be carried out regularly, and homes which do notmeet the guidelines should receive appropriate advice andhelp to meet the standards, or forfeit registration.
• In residential care accommodation, at least £18 perresident per week (2004 prices) should be spent on foodingredients to ensure that food of sufficient nutritionalcontent can be made available.
• Individuals, their relatives or advocates should enquireabout a prospective home’s commitment to nutritionalstandards and should ask how much money per residentper week is spent on food ingredients.
• Those providing community meals need to take intoaccount the needs and wishes of older people from blackand ethnic minorities who do not have access to anappropriate lunch club.
• Lunch clubs should be developed for older people in anysetting where it is already the custom for older people togather.
References
1 Office for National Statistics. 2001.Census data. Available from:www.ons.gov.uk/census
2 Department of Health. Department ofHealth Statistical Bulletin: CommunityCare Statistics 2001. Available from:www.dh.gov.uk
3 Laing and Buisson. 2002. Care ofElderly People: Market Survey. 15thedition. London: Laing and Buisson.Available from:www.laingbuisson.co.uk
4 Office for National Statistics 2003.Social Trends 2003. Available from:www.ons.gov.uk
5 Department of Health. 2000. HealthSurvey for England. Available from:www.dh.gov.uk
6 Statistics from the Alzheimer’s Society,2003. Available from:www.alzheimers.org.uk
7 VOICES. 1998. Eating Well for OlderPeople with Dementia. London:VOICES. For details see:www.cwt.org.uk
8 Department of Health. 2002. CareHomes for Older People: National
Minimum Standards. London: TheStationery Office. Available from:www.dh.gov.uk
9 Personal Social Services ResearchUnit, 2002. OPUS: A Measure of SocialCare Outcome for Older People.Available from: www.ukc.ac.uk/PSSRU
10 Office for National Statistics. 2001.General Household Survey: PeopleAged 65 Years and Over: 1998-1999.Available from: www.ons.gov.uk
11 Office for National Statistics. 2001.Personal Social Service Expenditure2000-2001. Available from:www.ons.gov.uk
12 Data accessed in 2003 from:www.wrvs.co.uk/about/housebound/meals.htm
13 Data accessed in 2003 from:www.housing.odpm.gov.uk
14 Caughey P, Seaman C, Parry D, FarquarD, McNennan WJ. 1994. Nutrition ofold people in sheltered housing.Journal of Human Nutrition andDietetics; 7: 263-68.
15 Personal communication with AnitaBerkley.

Chapter 3 How a good diet can contribute to the health of older people
21
Chapter 3
How agood dietcancontributeto thehealth ofolderpeople
How the bodychanges withageingMany people remain well as they getolder, but they undergo:
• changes in organ systems, and
• changes in body composition andin metabolism.1, 2
These changes happen at verydifferent rates in different people.Older people may also have morefrequent episodes of ill health andtake longer to recuperate fromillnesses. To help minimise potentialhealth problems, a good diet andphysical activity are essential.
Changes in organ systems Disorders affecting the digestivesystem, heart and circulation,endocrine system, kidneys, brain andnervous system become increasinglycommon. In some older people, theimmune system begins to functionless well. The senses of sight,hearing, taste and smell may alsodeteriorate.
Changes in bodycomposition andmetabolism As people get older, they are usuallyless active and therefore use upfewer calories.1, 3-5 Muscle fibres mayget weaker, and bone lossaccelerates.6 Old people tend to losemuscle and their proportion of bodyfat increases.7 As they use up lessenergy, so they have less need anddrive to eat calories. Energyexpenditure decreases progressivelywith age, even if the person does nothave any illness.1
It is quite normal for people – of anyage – to eat less food if their calorierequirements fall. However, at verylow levels of calorie intake, as lessfood is eaten, there is a greaterpossibility that the level of intakes ofsome nutrients in the diet willbecome dangerously low. This canlead to muscle loss, weakness and afurther decrease in activity generally,which further exacerbates bone and
muscle loss. Weak muscle power canmake some older people feelunsteady on their feet, and fear offalling may deter them from trying tobe more active.
MalnutritionMalnutrition includes bothundernutrition and overnutrition. Themain cause for concern among olderpeople in the UK is that they are noteating enough to maintain goodnutrition. Among the population ofolder people in residential care thereare many more underweight peoplethan there are overweight or obesepeople, and in old age beingunderweight poses a far greater riskto health than being overweight.8
The most recent information on thenutritional status of older people inBritain was reported in the NationalDiet and Nutrition Survey (NDNS) ofpeople aged 65 years and over in1998.9 In this survey, 3% of men and6% of women living at home wereunderweight, while comparablefigures for those in residential carewere 16% and 15% respectively. It issuggested, however, that risk ofundernutrition is still not adequatelyidentified in older people10 and thatundernutrition is often associatedwith hospitalisation and poor healthstatus.10-12 The level of undernutritionamong older people with dementiain residential care is likely to be evenhigher, with estimates that as many as50% of older people with dementiahave inadequate energy intakes.13
Undernutrition is related to increasedmortality, increased risk of fracture,increased risk of infections andincreased risk of specific nutrientdeficiencies leading to a variety ofhealth-related conditions that cangreatly affect the quality of life.8
Disease can also exert a potentinfluence on malnutrition as medicalconditions can reduce food intakeand impair digestion and absorptionof nutrients as well as affect how thebody metabolises and utilises them.14
The causes of undernutrition in olderpeople in residential care are oftenmulti-factorial: low income, living

Chapter 3 How a good diet can contribute to the health of older people
22
alone, limited mobility, and lack offacilities and social network can leadto undernutrition before admission,and this is often exacerbated bydepression, bereavement andconfusion.15 Factors that have beenassociated with undernutrition incare situations include: lack ofpalatability of food and inflexibletiming of meals,16 lack of assistancewith eating or loss of independencein eating,17 lack of acceptability offood provided to ethnic minorities,18
and lack of awareness of the need forassessment and documentation ofolder people at risk ofundernutrition.19
Common healthproblems that canbe improved bydietMalnutrition can contribute to anumber of health problemsincluding:
• constipation and other digestivedisorders
• anaemia
• diabetes mellitus
• muscle and bone disorders,including osteoporosis,osteomalacia and osteoarthritis
• mouth problems
• swallowing difficulties
• overweight, and
• coronary heart disease and stroke.
Further details on these, and on howdiet can help, are given below.
Constipation and otherdigestive disordersConstipation plagues and perplexesmany older people. One in five
people in Britain have problemsassociated with constipation whichimpair their quality of life,particularly if their mobility isaffected.20 Constipation is mostcommon in those who are very oldand frail and therefore likely to beliving in residential care.21 Most atrisk are those who do not getsufficient exercise, those confined tobed and those who have severedifficulties in moving and gettingabout.
Recent evidence suggests thatnursing home residents are threetimes more likely to receive a laxativeto treat constipation than olderpeople living at home.22 Chronic useof laxatives is discouraged, however,as over-use can lead to dehydrationand mineral imbalance, particularlypotassium deficiency. There is alsoan association between calorie intakeand the consumption of a smallernumber of meals and an increasedrisk of constipation23 suggesting thatthere is a potential for constipationwhenever overall food consumptiondeclines.
Constipation may be caused byinadequate fluid intake, inadequatefibre intake, low mobility andsometimes as a side effect ofmedication. Chronic disease, changesin food habits and psychologicaldistress also contribute toconstipation.24
Low fibre intake has been shown tobe associated with older people whohave chewing difficulties due tohaving no teeth or poorly fittingdentures.25
What can helpAn adequate intake of fluid isessential in preventing constipation –1,500ml is recommended, equivalentto 8-10 teacups a day.26 Adequateintake of fibre and increased physicalactivity can also help to preventconstipation.27 Sources of fibre arewhole grain cereals (found forexample in wholemeal bread), wholegrain breakfast cereals, pulses (peas,beans and lentils), fresh and driedfruit, vegetables and salads. Forpeople who have difficulty chewing,fruits, vegetables and pulses can be
puréed and added to dishes (see alsoMouth problems on page 24). Higherfibre white bread may be moreacceptable to older people who areunaccustomed to or dislikewholemeal bread.
Increasing the fibre intake of olderpeople, particularly those with smallappetites, should always be doneslowly and cautiously and inconjunction with increased fluid.
Older people with gastrointestinalproblems should have regular mealsand snacks, and good nutrition canbe part of the management plan fordiverticulitis. Those with bowel ormalabsorption disorders are likely toneed expert advice from a doctor ordietitian.
Raw wheat bran should never beadded to the diet. Although rawwheat bran is high in fibre, itcontains phytates, which interferewith the absorption of importantnutrients such as calcium and iron.
AnaemiaThere are several different causes ofanaemia. It might be caused byinsufficient dietary iron, especially iflittle meat is eaten. It can also becaused by folate deficiency. In olderpeople folate deficiency anaemia isusually the result of undernutrition,particularly among those who livealone, are depressed, drink too muchalcohol or have dementia. Perniciousanaemia is a disorder where vitaminB12 is not absorbed from food andthis condition is treated withinjections. However, anaemia inolder people may also be a sign ofinternal disease which has causedsmall repeated losses of blood. Adietary cause should only bediagnosed after excluding suchdiseases.28 Anaemia often progressesslowly and increasing paleness andtiredness are often left untreated.Anaemia is also associated withbreathlessness on exertion andpalpitations and people with anaemiamay be more prone to infections dueto changes in immune function.29 Ina large American study, low serumiron status was also shown to be apredictor of death from all causes,
In old age beingunderweight poses a far
greater risk to health thanbeing overweight.
Chapter 3 How a good diet can contribute to the health of older people
23
particularly coronary heart diseaseamong men and women over 70years.30 Iron status in older peoplehas also been shown to be positivelyassociated with intakes of vitamin C,protein, iron, fibre and alcohol.31
What can helpTo help prevent anaemia, peopleshould be encouraged to eat iron-rich foods such as liver, kidney, redmeat, oily fish, pulses and nuts(including nuts which have beenground and used in cooking). Foods,particularly fruit and vegetables, adrink rich in vitamin C and moderateamounts of alcohol taken at the samemeal will help iron absorption. Olderpeople should also be encouraged toeat folate-rich foods such as greenleafy vegetables and salads, orangesand other citrus fruits, liver, fortifiedbread and breakfast cereals and yeastextract. Yeast extract provides asignificant amount of folate even ifsmall quantities are eaten. (SeeAppendix 3 for other sources of ironand folate.)
Iron preparations should only begiven if prescribed by a medicalpractitioner.
High doses of folic acid supplements(more than 1mg daily) should beavoided unless prescribed by amedical practitioner.
Diabetes mellitusIt is estimated that between 7% and10% of elderly people in residentialand nursing care have diabetes, butthis may increase to as many as 25%in some areas.32
Dietary treatment of diabetes haslong been seen as the cornerstone ofmanagement of this illness and canhelp to prevent complications.33 Therestrictions on carbohydrate whichused to be recommended are nolonger advised. Diets for diabeticsshould follow the healthy eatingadvice for the general population –more fruits and vegetables, less fat,especially saturated fat, less sugarand more fibre. This will allow plentyof scope for a full range of attractivefood.
What can helpAdvice for residential and nursinghome care staff on the managementof diabetes among residents is givenin the Diabetes UK publicationGuidelines of Practice for Residentswith Diabetes in Care Homes,32
which can be found on their websitewww.diabetes.org.uk
Muscle and bonedisordersSixty-five per cent of older people inresidential and nursing care havedisabilities which hinder moving andgetting about.34 These disabilities areusually caused by disorders such asosteoarthritis, osteoporosis,osteomalacia (the adult form ofrickets) and stroke. Loss of musclestrength and reduced bone densitycontribute to falls and fractures. Thecurrent rate of over 200,000 fracturesa year, the majority of which occur inolder people, costs the NHS over£940 million a year. Fracture ratesincrease with age and there is anincrease in age-specific fracture riskrelated to vitamin D insufficiency.35
Low body weight is a major riskfactor for hip fracture among frail,older women.36
Physical activity is extremelyimportant for maintaining bonestrength. It can also improve musclestrength thus helping to prevent fallswhich can cause fractures.
Vitamin D is essential for maintainingbone and muscle integrity. The mainsource of vitamin D for most peopleis that formed in the skin by theaction of summer sunlight betweenApril and October. However,exposure to the sun is limited formany older people in residential andnursing care and the ability toconvert vitamin D to its active form isimpaired with ageing. As few foodscontain vitamin D, there may be verylittle vitamin D in an older person’sdiet.
The specific value of calciumsupplements for bone health in oldage is debated,35 but it is sensible toensure that older people have anadequate calcium intake.
What can helpPhysical activityIt is important to encourage olderpeople to undertake regular physicalactivity, such as walking, as thisstrengthens and builds up muscleand bone and increases calorierequirements, which in turn increasesappetite. Increased activity isassociated with reduced levels ofosteoporotic fracture37 and reducedmortality from all causes38 as well asgiving psychological benefits whichincrease the sense of well-being andencourage the maintenance ofactivities of daily living.39 Many olderpeople in residential care may findeven a 10-minute walk beyond theirfunctional ability and in suchcircumstances it is more appropriateto encourage specific activities tohelp to improve mobility andmuscular strength particularly toprevent falls.40 Even chair-boundpeople should be encouraged to doregular leg and arm movements. Staffin residential care accommodationcan help residents to do things forthemselves rather than doing the jobsfor them. People who have sufferedinjuries or who have been ill shouldbe encouraged to regain mobility asthey recover. Resources to help staffencourage activity in residential carecan be found on page 76.
Vitamin D and calciumIt is now suggested that it isimpossible for most older people toget enough vitamin D from the dietalone and that older people inresidential and nursing homes whorarely go out should receive vitaminD supplements.35 Advice onsupplementation should be takenfrom a medical practitioner.Increasing intakes of vitamin D andcalcium in residential care and in thecommunity has been shown toreduce fracture rates.41, 42 Vitamin Dsupplements can also be used to treatosteomalacia.
Measures to give older people moreaccess to summer sunlight should,however, be encouraged andarchitects designing accommodationfor older people should beencouraged to take account of the

Chapter 3 How a good diet can contribute to the health of older people
24
need for residents to have regularexposure to sunlight. Features couldinclude the use of glass in windowswhich allows UV light to passthrough, sheltered alcoves on thesouth side of buildings, and well-paved paths with hand rails and nosteps.
Ensure adequate calcium intakes byencouraging intakes of dairyproducts such as milk, cheese andyoghurt and other good sources ofcalcium such as green vegetables,tinned fish (eaten with the bones)and cereal products. Good sources ofnutrients are shown in Appendix 3.
Mouth problemsIt has been shown that the presence,number and distribution of naturalteeth are related to the ability to eatcertain foods, and that havingdifficulty with chewing affects thenutrient intakes of older people.43,44
There is evidence that people whocannot chew or bite comfortably areless likely to consume high fibrefoods such as bread, fruit andvegetables, thereby risking reducingtheir intake of essential nutrientssuch as fibre, iron and vitamin C.43
Chewing ability is highly correlatedwith number of teeth. Edentulouspeople (those with no natural teethwho usually rely on completedentures) are more affected thandentate people and the goal for oralhealth for older people is to have atleast 20 teeth: 10 in the top jaw and10 in the lower jaw, free from painand discomfort. If older people havefalse teeth these should becomfortable and well fitting, shouldlook good and should allow thebearer to bite and chew all types offood. Dentures may become loose ifthere is substantial weight loss.
People with xerostomia (dry mouth),which affects about 20% of olderpeople,44 also have difficulties eatingcertain foods.45, 46 Mouth ulcers andthrush can also cause mouth painand can be treated with anti-fungalmouthwash.
What can helpOral health should be promoted at allages by eating sugary foods lessoften (see Non-milk extrinsic sugarsin chapter 4), using a fluoridetoothpaste or a fluoride mouth rinse,and by stopping smoking. Toothcleaning can be improved by using asmall-headed toothbrush which iseasy to manipulate. Older peoplewho cannot brush their own teethshould be helped to do so every day.
Older people should have a fulldental check-up when they first enterresidential accommodation and atleast every three years thereafter.Facilities are needed to take theperson to the dental surgery whenappropriate. Alternatively,community dentists could bring theirequipment to the home for routinecheck-ups. Older people shoulddemand attention for dental pain.
Special attention should be given tosensitivity and discomfort of the teethand mouth as these conditions canrestrict choice of food and lead toloss of social confidence.47
Replacement of missing teeth shouldbe limited to front teeth and pre-molars to enhance chewing and self-esteem. Badly fitting dentures shouldbe relined rather than replaced withnew ones, which old people mayfind it difficult to adapt to. Usefulinformation on dental care can befound in the Relatives Associationpublication Dental Care for OlderPeople in Homes.47
Swallowing difficultiesAfter a stroke many older peopleexperience delayed or diminishedswallowing reflex and this may alsooccur in older people with dementia,with cancers of the head or neck, orwhere there are diseases such asParkinson’s disease or multiplesclerosis. Swallowing difficulties maymake eating or drinking moredifficult. Lack of co-ordination inchewing and swallowing can resultin choking, which can be a veryfrightening experience. It isimportant that all staff working witholder people should be trained in
what to do if someone chokes.Information and advice on what todo if someone chokes can be foundin Eating Well for Older People withDementia (see page 2). Swallowingdifficulties always need professionalassessment and food and drinkintakes can often be improved whensuitable modifications are made tofood and drink consistency.
What can helpOlder people who complain ofpainful eating and swallowing shouldask their doctor for advice urgently.The cause can often be found andswallowing disorders are much moreeasily treated if dealt with quickly. Aspeech and language therapist willbe able to assess problems withswallowing and make suggestionsabout the appropriate texture of foodto offer. It is essential that the olderperson gets enough calories andnutrient-rich foods. Food that ismashed, liquidised or diluted maynot contain enough energy. It may beworth using a prescribable thickeningagent to modify texture. Informationon altered texture diets and helpingpeople with swallowing difficulties toeat well can be found in Eating Wellfor Older People with Dementia (seepage 2).
OverweightSome over-75-year-olds who areconcerned about being overweightmay want to lose weight, especially ifthis would improve their mobility.However, eating less food may resultin them getting an inadequatenutrient intake. It is possible to beoverweight and still be deficient incertain nutrients. Older people whohave been advised by their doctor tolose weight should therefore begiven information – either by thedoctor or a dietitian – on how tomaintain the nutrient content of theirdiet while reducing calorie intake.
In younger adults, obesity isassociated with heart disease, highblood pressure and diabetes. Afterthe age of 75, this relationship is lessclearly defined.

Chapter 3 How a good diet can contribute to the health of older people
25
What can helpOlder people should be encouragedto maintain their weight, unless theyare very overweight.
Those who are overweight and whoalso suffer from arthritis and impairedmobility should be given information– either by their doctor or by adietitian – on how to lose someweight, as obesity can increase jointpain.
Coronary heart diseaseand strokeForty per cent of all deaths amongover-65-year-olds are caused bycoronary heart disease or stroke. Anystrategies for limiting these majorhealth problems will reduce disabilityamong older people and increase lifeexpectancy. Risk of cardiovasculardisease rises incrementally withincreasing levels of blood pressureand cholesterol concentration,48 andreducing blood pressure andcholesterol concentrations in olderpeople could have a substantialeffect on reducing cardiovasculardisease. Reducing the amount ofsaturated fat and the amount of saltin the diet have been shown togreatly affect cardiovascular risk in alarge number of studies.49, 50
Evidence also shows that increasingfruit and vegetable intakes by 1-2portions a day may decreasecardiovascular risk51 and increasingintakes of oily fish has also beenshown to reduce cardiovasculardeath.52
It would therefore be prudent toencourage older people to eat a dietrich in fruits and vegetables, leanmeat and fish, and to reduce intakesof saturated fats in fatty meats, full-fatdairy products, cakes and biscuits.There will, however, be some veryold, very frail or ill older people whohave small appetites and who needto be encouraged to eat whateverfoods they can. High salt intakesshould be discouraged, but it isacknowledged that as people getolder their sense of taste diminishesand they may want more salt toflavour foods.
What can helpOlder people should be encouragedto eat more fruit, vegetables and fishand more starchy foods such asbread. Older people who are thinshould be encouraged to eatwhatever foods they can, but olderpeople with a good appetite shouldlimit their intakes of saturated fatsfrom fatty meat, full-fat dairy foodsand cakes and biscuits.
Where possible herbs, spices, lemonjuice, mustard, onion and celeryshould be used to flavour foodsrather than just salt.
Recovery from illness andsurgeryOlder people’s recovery from illnessand the incidence of post-operativecomplications depend on theirnutritional status.53 The relationshipbetween undernutrition andprolonged hospital stay has beendemonstrated and there have beenmany reports outlining the particularproblems patients have in obtainingadequate nutrition while inhospital.12, 54 Many older peopleneed to undergo surgery and goodnutrition has been shown to play animportant part in the prevention ofcomplications such as infection andto assist in the healing process.14
What can helpOlder people who are going intohospital should be encouraged to eatand drink well in preparation forsurgery. They may wish to considerhow they can be supported byfamily, friends or carers to maintaintheir nutritional status while inhospital.
Following surgery, appetites of olderpeople may take time to recover andnutritionally dense meals should beprovided. This can be either throughenriching the energy content ofmeals served by adding cream, butterand sugar to foods, or through thecareful use of energy and proteinsupplements. The hospital doctor orGP may prescribe supplements post-operatively, but these should not beseen as long-term substitutes for
meals. Supplements should be usedin addition to enriched meals.
Special attention should be paid tothe energy requirements of olderpeople who have had an amputation.
Other health problemsThere is still debate about whetherdiet can be considered causative inother health problems in olderpeople such as mental health andnervous system decline or cataracts,but there is increasing evidence forthe role of diet in the prevention ofsome cancers and in maintaining theimmune system. For many diseasesthere is not sufficient evidence to make highly specificrecommendations for prevention, butthere is overwhelming evidence thatparticular dietary patterns do seem torelate to healthy aging.55
Mental health The causes of dementia ordepression in older people arecomplex and malnutrition maycontribute, especially where there isa deficiency of B vitamins.Malnutrition may itself result fromlack of interest or difficulties inpreparing and eating food, creating a‘vicious cycle’ of malnutrition anddecline. Inadequate energy intakehas been found in as many as 50% ofpeople with dementia in nursingcare, residential care or hospital,55, 56
and older people with dementia aremore likely to be deficient in certainvitamins and minerals than otherolder people.57 Some studies havefound that, compared with otherolder people, those with dementiaare more likely to have low levels offolate, zinc, vitamin B12 and iron.58, 59
The importance of good nutrition forolder people with dementia has beenrecognised, and detailed practicaladvice on how individuals can beencouraged to eat well can be foundin Eating Well for Older People withDementia (see page 2).
The nervous systemThe nervous system which controlsmovement and feeling depends on a

Chapter 3 How a good diet can contribute to the health of older people
26
satisfactory nutritional state,especially with regard to adequate Bvitamins. Extreme circumstancesleading to conditions such as beri-beri are most unlikely, but lesserdegrees of deficiency may play a partin unsteadiness of movement.
CataractCataract may be related toundernutrition and it has beensuggested that good nutrition canprotect against cataracts.60 Higherintakes of some nutrients includingprotein, vitamin A, carotenoids,vitamin C, niacin, thiamin andriboflavin during adulthood havebeen suggested as being protectiveagainst cataract in a number ofstudies61, 62 but not consistently.Other nutrients such as selenium,zinc, calcium and folic acid have alsobeen suggested as potentiallypreventative, but some studies haveshown that other non-dietary factorsare confounding relationshipsbetween diet and cataractdevelopment. Further research isrequired to identify preventativestrategies in this area.
CancersAbout 25% of deaths of people aged75-84, and 14% of deaths of peopleover 85, are caused by cancers.63 Therelationship between nutrition andthe development of cancer iscomplex, but there is considerableevidence that particular elements inthe diet may promote or retard thegrowth of specific canceroustumours.64 The dietary advice for theprevention of cancer includeschoosing a diet rich in plant-basedfoods, eating plenty of vegetablesand fruits and choosing foods low insalt and fat. In addition, maintaininga healthy body weight, drinkingalcohol in moderation and ensuringfoods are stored and prepared safelyare important preventativestrategies.65
Good nutrition plays an importantrole in the care of people withcancer. Specialist advice from adietitian is recommended.
The immune systemThe body’s ability to fight infectionand disease through its immunesystem probably diminishes with age.This is likely to be one reason for thegreater frequency of illnesses in olderpeople.29 However, not all olderpeople are affected and degenerationof the immune system is notinevitable.66 Maintaining goodnutritional status will contribute tokeeping healthy body defences aspeople get older. Research showsthat improving the nutritional statusof older people greatly enhancestheir ability to fight off infection.67, 68
The effect of drugs onnutritionMany older people take a number ofdifferent drugs, both over-the-counter drugs and those prescribedby medical practitioners. The use ofdrugs may influence appetite, food
intake and body weight. Some drugscan cause loss of appetite and somecause adverse responses to food,such as nausea, dry mouth or loss oftaste. Some drugs may also alterbowel function causing constipationor diarrhoea, and if drugs causedrowsiness this can cause olderpeople to miss meals and snacks.
The effect of nutrition onthe action of drugs It is also important to recognise thatpoor nutritional status can impairdrug metabolism and older peoplewho are dehydrated or have hadrecent weight loss may experiencegreater side effects.53
It can be helpful to ask for regulardrugs reviews for older people inresidential care and to be alert to sideeffects when new drugs areprescribed.69
RecommendationsIn addition to the nutritional guidelines given in Chapter 5,the Working Group makes the following recommendations:
• Older people should be encouraged to undertake regularphysical activity, such as walking, as this strengthens andbuilds up muscle and bone, and increases calorierequirements, which in turn increases appetite. Evenchair-bound people should be encouraged to do regularleg and arm movements.
• Facilities should be provided for regular dental check-ups.This means taking people to the dental surgery, eitherfrom their own homes or from residential homes, orhaving community dentists visit the home.
• Architects designing accommodation for older peopleshould be encouraged to take account of the need forresidents to have regular exposure to sunlight, which is asource of vitamin D. Features could include windowswhich allow UV light to pass through the glass, shelteredalcoves on the south side of buildings, and well-pavedpaths with hand rails and no steps.
• Older people living in residential and nursing homes whorarely go outside are likely to need vitamin D supplementsand should consume a diet which provides sufficientcalcium. Advice on supplements should be taken from aGP.

Chapter 3 How a good diet can contribute to the health of older people
27
management program. Journal ofGerontological Nursing; 20: 32-34.
28 Finch CA. 1989. Nutritional anaemia.In: Horwitz et al (eds.) Nutrition in theElderly. Published on behalf of theWorld Health Organization by OxfordUniversity Press.
29 Chandra RK. 1992. Effect of vitaminand trace-element supplementation onimmune responses and infection inelderly subjects. The Lancet; 340:1124-26.
30 Corti MC, Guralnik JM, Salive ME et al.1997. Serum iron level, coronary heartdisease and all cause mortality in oldermen and women. American Journal ofCardiology; 79: 120-27.
31 Doyle W, Crawley H, Robert H et al.1999. Iron deficiency in older people:Interactions between food and nutrientintakes with biochemical measures ofiron: further analysis of the NationalDiet and Nutrition Survey of peopleaged 65 years and over. EuropeanJournal of Clinical Nutrition; 53: 552-59.
32 Diabetes UK. 1999. Guidelines ofPractice for Residents with Diabetes inCare Homes. Available from:www.diabetes.org.uk
33 Ruoff G. 1993. The management ofnon-insulin dependent diabetesmellitus in the elderly. Journal of theFamily Practitioner; 36: 329-35.
34 Department of Health. 2000. HealthSurvey for England: The Health ofOlder People. Available from:www.dh.gov.uk/public/healtholderpeople2000press.htm
35 Department of Health. 1998. Nutritionand Bone Health. London: TheStationery Office.
36 Bernstein J, Grisso J, Kaplan F. 1999.Body mass and fracture risk: a study of330 patients. Clinical Orthopaedics;364: 227-30.
37 Wickham CAC, Walsh K, Barker DJP etal. 1989. Dietary calcium, physicalactivity and risk of hip fracture: aprospective study. British MedicalBulletin; 299: 889-92.
38 Blair SN, Kohl HW, Paffenbarger RS etal. 1989. Physical fitness and all causemortality: a prospective study ofhealthy men and women. Journal ofthe American Medical Association;262: 2395-401.
39 Bennett K, Morgan K. 1992. Activityand morale in later life: preliminaryanalyses from the NottinghamLongitudinal Study of Activity andAgeing. In: Norgan NG (ed.) Nutritionand Physical Activity. Cambridge:Cambridge University Press: pages129-42.
40 Health Development Agency. 1999.Active for Life: Promoting PhysicalActivity with Older People. London:
15 Morley JE, Kraenzle D. 1994. Causesof weight loss in a community nursinghome. Journal of the AmericanGeriatrics Society; 42: 563-85.
16 Stephen AD, Beigg CL, Elliot ET et al.1997. Food provision, wastage andintake in medical surgery and elderlyhospitalised patients. Clinical Nutrition;16: 4.
17 McLaren SM, Dickerson JW, Wright J.1997. Nursing support offered to strokepatients at mealtimes: a direct non-participant observation study.Proceedings of the Nutrition Society;56: 255A.
18 McGlone PC, Davies GJ, Murcott A etal. 1997. Foods consumed by a Bengalipopulation in a British hospital.Proceedings of the Nutrition Society;56: 28.
19 Lennard-Jones J, Arrowsmith H,Davison C et al. 1995. Screeningnurses and junior doctors to detectmalnutrition when patients are firstassessed in hospital. Clinical Nutrition;14: 336-40.
20 Cummings JH, Bingham SA. 1992.Towards a recommended intake ofdietary fibre. In: Eastwood M, EdwardsC, Parry D (eds.) Human Nutrition: AContinuing Debate. Symposiumentitled ‘Nutrition in the Nineties’.London: Chapman Hall.
21 Kinnunen O. 1991. Study ofconstipation in a geriatric hospital, dayhospital, old people’s home and athome. Aging; 3: 161-70.
22 Fahey T, Montgomery A, Barnes J,Protheroe J. 2003. Quality of care forelderly residents in nursing homes andelderly people living at home: acontrolled observational study. BritishMedical Journal; 326: 580-85.
23 Towers A, Burgio K, Locher J et al.1994. Constipation in the elderly:influence of dietary, psychological andphysiological factors. Journal of theAmerican Geriatrics Society; 42: 701-06.
24 Sandman PO, Adolfsson R, Hallmans Get al. 1983. Treatment of constipationwith bread in long term care ofseverely demented elderly patients.Journal of the American GeriatricsSociety; 31: 289-93.
25 Brodeur JM, Laurin D, Vallee R,Lachapelle D. 1993. Nutrient intake andgastrointestinal disorders related tomasticatory performance in theedentulous elderly. Journal ofProsthetic Dentistry; 70: 468-73.
26 EURONUT-SENECA (Lisette CPGM etal, eds.) 1991. Nutrition and the elderlyin Europe. European Journal of ClinicalNutrition; 45 (Suppl 3): 1-196.
27 Karam SE, Nies DM. 1994. Studentstaff collaboration: a pilot bowel
References
1 Hodkinson HM. 1990. Nutrition andillness in the aged. In: Harrison GA,Waterlow JC (eds.) Diet and Disease inTraditional and Developing Societies.Society for the Study of HumanBiology. Symposium 30. Cambridge:Cambridge University Press.
2 Prentice AM. 1992. Energy expenditurein the elderly. European Journal ofClinical Nutrition; 46, Suppl 3: S21-S28.
3 Zheng JJ, Rosenburg IH. 1989. What isthe nutritional status of the elderly?Geriatrics; 44 (6): 57-58, 60, 63-64.
4 Shock NW. 1972. Energy metabolism,caloric intake and physical activity ofthe aging. In: Carlson LA (ed). Nutritionin Old Age. Symposia of the SwedishNutrition Foundation X. Uppsala:Almqvist and Wiksell.
5 Reilly JJ, Lord A, Bunker VW et al.1993. Energy balance in healthy elderlywomen. British Journal of Nutrition;69: 21-27.
6 Widdowson EM. 1992. Physiologicalprocesses of aging: are there specialnutritional requirements for elderlypeople? Do McCay’s findings apply tohumans? American Journal of ClinicalNutrition; 55 (6 suppl): 1246s-1249s.
7 Hoffman N. 1993. Diet in the elderly.Needs and risks. Medical Clinics ofNorth America; 77: 745-56.
8 Lehmann AB. 1991. Nutrition in oldage: an update and questions forfuture research. Part 1. Reviews inClinical Gerontology; 1: 135-45.
9 Finch S, Doyle W, Lowe C, Bates CJ etal. 1998. National Diet and NutritionSurvey: People Aged 65 Years andOver. Volume 1: Report of the Diet andNutrition Survey. London: TheStationery Office.
10 Margetts BM, Thompson RE, Elia M,Jackson AA. 2003. Prevalence of riskof undernutrition is associated withpoor health status in older people inthe UK. European Journal of ClinicalNutrition; 57: 69-74.
11 McWhirter JP, Pennington CR. 1994.Incidence and recognition ofmalnutrition in hospital. British MedicalJournal; 308: 945-48.
12 Pennington CR. 1998. Diseaseassociated malnutrition in the year2000. Postgraduate Medical Journal;74: 65-71.
13 Bucht G, Sandman P. 1990. Nutritionalaspects of dementia, especiallyAlzheimer’s disease. Age and Ageing;19: 32-36.
14 McLaren S, Crawley H. 2000.Managing Nutritional Risks in OlderAdults. Nursing Times ClinicalMonographs No. 44. London: NTBooks.

Chapter 3 How a good diet can contribute to the health of older people
28
Health Development Agency. Availablefrom: www.hda-online.gov.uk
41 Chapuy MC, Arlot ME, Duboeuf F et al.1992. Vitamin D3 and calcium toprevent hip fractures in elderly women.New England Journal of Medicine;327: 1637-42.
42 Trivedi DP, Doll R, Khaw KT. 2003.Effect of four monthly oral vitamin D(cholecalciferol) supplementation onfractures and mortality in men andwomen living in the community:randomised double blind controlledtrial. British Medical Journal; 326: 469-74.
43 Sheiham A, Steele J. 2001. Does thecondition of the mouth and teeth affectthe ability to eat certain foods, nutrientand dietary intake and nutritional statusamongst older people? Public HealthNutrition; 4 (3): 797-803.
44 Steele JG, Sheiham A, Marcenes W,Walls AWG. 1998. National Diet andNutrition Survey: People Aged 65Years and Over. Volume 2: Report ofthe Oral Health Survey. London: TheStationery Office.
45 Locker D. 1993. Subjective reports oforal dryness in an older adultpopulation. Community Dental OralEpidemiology; 21: 165-68.
46 Gilbert GH, Heft MW, Duncan RP.1993. Mouth dryness as reported byolder Floridians. Community DentalOral Epidemiology; 21: 390-97.
47 The Relatives Association. 1995. DentalCare for Older People in Homes.London: The Relatives Association.
48 Qizilbash N, Lewington S, Duffy S et al.1995. Cholesterol, diastolic bloodpressure and stroke: 13,000 strokes in450,000 people in 45 prospectivestudies. The Lancet; 346: 1647-53.
49 Clarke R, Frost C, Collins R et al. 1997.Dietary lipids and blood cholesterol:quantitative meta-analysis of metabolicward studies. British Medical Journal;314: 112-17.
50 Scientific Advisory Committee onNutrition. 2003. Salt and Health.London: The Stationery Office.
51 Gillman MW, Cupples LA, Gagnon D etal. 1995. Protective effect of fruits andvegetables on development of strokein men. Journal of the AmericanMedical Association; 273: 1113-17.
52 Department of Health. 1994. Diet andCardiovascular Disease. London:HMSO.
53 British Nutrition Foundation. 2003.Undernutrition in the UK. London:British Nutrition Foundation.
54 Lennard-Jones JE (ed.) 1992. APositive Approach to Nutrition asTreatment. London: King’s Fund.
55 Khaw KT. 1997. Healthy Aging. BritishMedical Journal; 315: 1090-96.
56 Sandman PO, Adolfsson R, Nygren Cet al. 1987. Nutritional status anddietary intake in institutionalisedpatients with Alzheimers disease anddementia. Journal of the AmericanGeriatrics Society; 35: 31-38.
57 Silver AJ, Morley JE, Strome LS et al.1988. Nutritional status in an academicnursing home. Journal of the AmericanGeriatrics Society; 36: 487-91.
58 Greer A, McBride DH, Shenkin A.1986. Comparison of the nutritionalstate of new and long term patients ina psychogeriatric unit. British Journal ofPsychiatry; 149: 738-41.
59 Renvall MJ, Spindler AA, Ramsdell JWet al. 1989. Nutritional status of free-living Alzheimers patients. AmericanJournal of Medical Science; 90: 433-35.
60 Taylor A, Jacques PF, Chylack LT et al.2002. Long-term intake of vitamins andcarotenoids and odds of early agerelated cortical and posteriorsubscapular lens opacities. AmericanJournal of Clinical Nutrition; 75: 540-49.
61 Hankinson SE, Stampfer MJ, SneddonJM et al. 1992. Nutrient intake andcataract extraction in women: aprospective study. British MedicalJournal; 305: 335-39.
62 Cumming RG, Mitchell P, Smith W.2000. Diet and cataract: the BlueMountains eye study. Ophthalmology;107, 450-56.
63 Office for National Statistics. HealthStatistics 2002. Available from:www.ons.gov.uk
64 Department of Health. 1998.Nutritional Aspects of theDevelopment of Cancer. London: TheStationery Office.
65 World Cancer Research Fund. 1997.Food, Nutrition and the Prevention ofCancer: A Global Perspective. London:World Cancer Research Fund.
66 Chandra RK. 1993. Influence ofnutrition on immunocompetence in theelderly. In: Cunningham-Rundles (ed).Nutrient Modulation of the ImmuneResponse. New York: Dekke.
67 Roebothan BV, Chandra RK. 1994.Relationship between nutritional statusand immune function of elderly people.Age and Ageing; 23: 49-53.
68 Woo J, Ho SC, Mak YT et al. 1994.Nutritional status of elderly peopleduring recovery from chest infectionand the role of nutritionalsupplementation assessed by aprospective randomised single-blindtrial. Age and Ageing; 23: 40-48.
69 Rochon P, Gurwitz JH. 1997. Optimisingdrug treatment for elderly people: theprescribing cascade. British MedicalJournal; 315: 1096-99.

Chapter 4 Nutritional requirements of older people
29
Chapter 4
Nutritionalrequirementsof olderpeople
Among older people, lowweight, a small appetiteand low food intakes are
more common and cause moreproblems than overweight. Manyolder people have problems witheating and chewing, as a result ofbadly fitting dentures or lost teeth.They also have a higher risk ofpoor absorption of nutrients. Thosewho are on medication may haveless appetite than normal. (SeeChapters 2 and 3.) As a result, manyolder people in the UK have lowintakes of energy, many mineralsand vitamins, and fibre.
The question ‘What are desirableintakes of energy and nutrients forolder people?’ has been a subject ofdebate for some time.
In 1991 the Department of Healthpublished a report on the DietaryReference Values (DRVs) for FoodEnergy and Nutrients for the
population of the UK,1 prepared bythe Committee on Medical Aspectsof Food Policy (COMA). (DietaryReference Values are quantifiednutritional guidelines for energyand various nutrients, separatelystated for women and men. For afuller explanation, see box below.)The DRVs were examined by theCOMA Working Group on theNutrition of Elderly People andwere endorsed in their report onThe Nutrition of Elderly People.2
The Caroline Walker Trust ExpertWorking Group has therefore usedthe DRVs as the basis of this report.
The main COMA recommendationsfor older people are given in theleft-hand columns on pages 30-37,followed by a summary of the basisfor those recommendations. Thecomplete COMA recommendationsare given in Appendix 1.
DIETARY REFERENCE VALUES (DRVs)
Dietary Reference Values (or DRVs) are quantified nutritionalguidelines for energy and nutrients. They apply to groups of people;they are not intended for assessing individual diets. The COMA reportgives three figures for requirements for most nutrients:
Reference Nutrient Intake (RNI) The amount of a nutrient which is sufficient to meet the dietaryrequirements for about 97% of the people in a group. Intakes abovethis amount will almost certainly be adequate.
Estimated Average Requirement (EAR) The amount which satisfies 50% of people in a group.
Lowest Reference Nutrient Intake (LRNI) The amount of the nutrient which is sufficient for about the 3% ofpeople in a population who have the lowest needs. Anyone regularlyeating less than the LRNI may be at risk of deficiency.

Chapter 4 Nutritional requirements of older people
30
Table 1 Nutritional requirements of older people
The text in black in the left-hand columns on pages 30-37 show recommendations of the COMA report on Dietary Reference Values for FoodEnergy and Nutrients for the United Kingdom.1
Reference Nutrient Intake = The amount of a nutrient which is sufficient tomeet the dietary requirements for about 97% of the people in a group. Intakesabove this amount will almost certainly be adequate.
Estimated Average Requirement = The amount which satisfies 50% of people ina group.
Energy (calories)
Estimated Average Requirement
WOMEN aged 75 and over:1,810kcal (7.61MJ*) a day
MEN aged 75 and over:2,100kcal (8.77MJ*) a day
The 1992 COMA report on The Nutrition of Elderly People2 emphasised theneed for monitoring the energy (calorie intake) of older people. Those olderpeople who are relatively inactive require fewer calories because they use lessenergy. However, although the energy requirements of such people may belower, their requirements for other nutrients will not have changed and maywell have increased. Their diet therefore should be one of quality rather thanquantity.
On the other hand, some older people, especially those who have long-standing chronic illness such as heart disease or lung disease and thosesuffering from dementia or other related disorders, have increased energyrequirements. These people are more likely to be living in residential homesand therefore present a particular challenge to caterers, because they not onlyhave an increased energy requirement but in many cases also have poorappetites. In such cases, nutrient-dense foods (foods which contain aconcentration of nutrients) may be suitable, for example fortified milkpuddings, or milky drinks.
Housebound older people have energy intakes up to one-third lower thanthose of free-living older people.3 When calorie intakes are reduced below1,200kcals it is difficult to achieve a diet that is sufficient in all nutrients.
Fat
The contribution of fat tothe diet
35% of food energy
WOMEN aged 75 and over:70g a day
MEN aged 75 and over:82g a day
Fat provides the most concentrated form of energy (calories). Saturated fats aremainly derived from animal sources, and are found for example in meat, butterand cheese. Unsaturated fats are mainly from plant and fish sources, and arefound for example in some margarines and oils.
It is recommended that fat should contribute about 35% of the food energy inthe diet. For many people this means reducing the amount of fat they now eat.It is also recommended that the types of fat should be varied so that no morethan 11% of food energy comes from saturated fats. Reducing the risk of heartdisease by moderating fat intake is also a worthwhile goal for older people.
The proportion of fat in the diet must be tailored to meet the needs of theindividual. For thin older people who need additional energy but who have apoor appetite, fat may both add flavour to food and provide an additionaluseful source of calories.
COMA RECOMMENDATIONS
Sources of fatSources of fat include fats and oil added to food when cooking or frying;butter, margarine and low-fat spreads; and the fat incorporated in manymanufactured foods such as biscuits, cakes, pastry and chocolate. Fattymeats and whole milk are also sources of fat.
MJ = megajoules1 MJ = approx. 239kcal
kcal = kilocalories1 kcal = 1 Calorie
* Megajoules and kilocalories areboth measurements of energy.
thes

Chapter 4 Nutritional requirements of older people
31
Carbohydrates
The contribution ofcarbohydrates to the diet
50% of food energy
The term carbohydrates includes both starches and sugars. COMA recommendsthat, for the population as a whole, carbohydrates should provide about 50% offood energy: 39% from starch and intrinsic and milk sugars (the sugar in fruit,vegetables and milk), and only about 11% from non-milk extrinsic sugars (egtable sugar and sugar added to foods).
Starch and intrinsicand milk sugars
The contribution of starchand intrinsic and milksugars to the diet
39% of food energy
WOMEN aged 75 and over:188g a day
MEN aged 75 and over:218g a day
Starchy foods are a good source of calories and can also provide importantnutrients, such as fibre and some B vitamins. Many people need to reduce theirfat intake and COMA recommends that eating more starchy foods shouldrestore the resulting loss in calories. However, for frail people who havedifficulty in eating large amounts of food, it is not always appropriate to reducefat intake (see page 30), or to eat large quantities of starchy foods, which maymake the diet bulky and less nutrient-dense.
COMA RECOMMENDATIONS
Sources of starchSources of starch include bread, pitta bread, chapatis, potatoes, pasta, rice,breakfast cereals, yams and plantains.
Sources of intrinsic and milk sugarsFruit and vegetables that contain sugars; and milk.
Non-milk extrinsicsugars(NME sugars)
The contribution of NMEsugars to the diet
11% of food energy
WOMEN aged 75 and over:53g a day
MEN aged 75 and over:62g a day
In the past sugars have often been referred to as ‘added sugars’ or ‘naturalsugars’. As the interpretation of these two terms often led to a great deal ofconfusion and misleading information on the health consequences, COMA triedto remedy this by defining the different groups of sugars to identify their effectson health, particularly dental health.
Non-milk extrinsic sugars, or ‘NME sugars’, are sugars which have beenextracted from the root, stem or fruit of a plant and are no longer incorporatedinto the cellular structure of food. NME sugars include table sugar, sugar addedto recipes, and honey, and are found in foods such as confectionery, cakes,biscuits, soft drinks and fruit juices.
The general population has been advised to reduce their intake of NME sugars.This advice has been made on the basis of the relationship between frequencyof sugar intakes and dental decay. Older people who do not have teeth are notat risk of dental decay but, as more older people retain their own teeth, dentaldecay is an increasingly important issue in this age group.
Sugar provides calories but contains no nutrients. Older people require a dietthat maintains a high nutrient intake, and eating a large amount of food rich inNME sugars may depress their appetite for a more varied and nutrient-rich diet.The advice given in the COMA report on The Nutrition of Elderly People2
therefore is that older people should keep their consumption of sugars in linewith the recommendations for the rest of the population.
Sources of NME sugarsSources of NME sugars include table sugar, honey, confectionery, cakes,biscuits, soft drinks and fruit juices.

Chapter 4 Nutritional requirements of older people
32
Fibre(Non-starch polysaccharides,or NSP)
Dietary Reference Value
18g a day
Fibre is important in the prevention of constipation. The quality of life for manyolder people is impaired by the symptoms of constipation. A high fibre diet canprevent over-use of laxatives.
An adequate fluid intake (11/2 litres of non-alcoholic fluid each day) aids theaction of fibre and can thus help prevent or alleviate constipation. Increasingthe intake of fruits, including dried fruit, vegetables and pulses will increase theamount of fibre consumed.
Although raw wheat bran is high in fibre, it contains phytates which interferewith the absorption of important nutrients such as calcium and iron. Raw wheatbran should therefore not be added to the diet of older people.
COMA RECOMMENDATIONS
Sources of fibreSources of dietary fibre include: wholemeal bread, wholemeal biscuits,whole grain breakfast cereals, pulses (peas, beans and lentils), fruit andvegetables. These foods provide useful sources of other nutrients too.
Protein
Reference Nutrient Intake
WOMEN:46.5g a day
MEN:53.3g a day
Protein is needed for building and for repairing body tissues. As people getolder, worn out tissue and injured tissue are replaced more slowly, and woundsheal more slowly and are more vulnerable to infection. The diet of older peopleshould provide adequate protein. This is most easily derived from animalsources but can also be obtained by combining different vegetable sources ofprotein such as pulses and cereals.
There is still debate about the amounts of protein older people can absorb anduse successfully.4 The COMA recommendations therefore set a balancebetween providing sufficient protein for repair of tissue and not overburdeningthe kidneys.
Some older people, especially those with infections or bedsores or those whoare less mobile, may require a higher level of protein,5-7 but advice shouldalways be sought from a dietitian or doctor if it is thought that extra protein isrequired.
People with known severe kidney failure sometimes need to be on a lowprotein diet.
Sources of proteinSources of protein include: meat, poultry and fish; pulses such as peas,beans and lentils; eggs and cheese. Milk can also be a useful source. Severalprotein supplements are available in ready-to-drink or powdered form.

Chapter 4 Nutritional requirements of older people
33
B vitamins (thiamin, riboflavin, niacin)
Reference Nutrient Intake
WOMEN:Thiamin 0.8mg a day Riboflavin 1.1mg a dayNiacin 12mg a day (women aged 50 and over)
MEN:Thiamin 0.9mg a dayRiboflavin 1.3mg a day Niacin 16mg a day (men aged 50 and over)
The body needs the B vitamins – thiamin, riboflavin and niacin – to be able toutilise the energy in the diet. B vitamins are particularly important for the brainand nervous system. There is a possibility that lack of the B vitamins maycontribute to confusion in older people.
Data from the National Diet and Nutrition Survey of people aged 65 years andover showed that 40% of older people both in residential care and in thecommunity had low biochemical status for riboflavin, and 10%-15% of bothgroups had low thiamin status.8 Older people in residential care were also morelikely to have lower intakes of B vitamins. It is therefore important to ensurethat older people have a varied diet and include good sources of riboflavin andthiamin in their diet every day.
People who have a history of alcohol abuse or are presently abusing alcoholmay need more than the recommended minimum amount given on the left.
COMA RECOMMENDATIONS
Sources of B vitaminsSources of thiamin and niacin include bread and other foods made with flour(such as bread, pasta and biscuits), breakfast cereals, pork (including baconand ham), kidney, liver, potatoes, yeast extract and fish.
Sources of riboflavin include milk and milk products (such as yoghurt),poultry, meat, oily fish such as herring, mackerel, canned sardines, tuna andsalmon, and eggs. For more details on sources of B vitamins, see Appendix 3.
Folate
Reference Nutrient Intake
200 micrograms a day
Folate deficiency leads to a particular type of anaemia known as megaloblasticanaemia. Folate is essential for many vital metabolic processes.
Low folate status has been shown in 40% of older people in residential care andvery low intakes of folate have been observed in about 5% of this group.8
People with dementia have particularly low levels of folate and this has beenpartly attributed to a lower consumption of fruits and vegetables.9
People who are taking certain drugs or who are drinking excessive amounts ofalcohol may also be at risk of folate deficiency, as are some people with boweldiseases such as coeliac disease.
It is possible for older people to achieve an adequate intake of folate quiteeasily provided they eat a varied diet with plenty of vegetables. However, folateis destroyed by prolonged heating – for example by overcooking food or byheating and keeping it for long periods – and particular care should be takenpreparing vegetables for mealtimes. Folate supplements may be needed, butshould be given under medical supervision.
Sources of folateSources of folate include Brussels sprouts and other green leafy vegetablesand salads, oranges and other citrus fruits, fortified bread, fortified breakfastcereals, liver, and yeast extract. Yeast extract provides a significant amount offolate even if only small quantities are eaten. For more details on sources offolate see Appendix 3.

Chapter 4 Nutritional requirements of older people
34
Vitamin C
Reference Nutrient Intake
40mg a day
Vitamin C has an important role in preventing disease and maintaining goodhealth. Low vitamin C intakes are associated with susceptibility to pressuresores10 and infection.11 Vitamin C can also help the absorption of dietary iron,and intakes of vitamin C have been positively associated with iron status inolder people.12
Data from the National Diet and Nutrition Survey8 suggested that 40% of olderpeople in residential care had low vitamin C status and intakes of vitamin Cdecrease with age and energy intake, suggesting that particular care should betaken to maintain vitamin C intakes among older frailer residents who havesmall appetites.
The use of drinks fortified with vitamin C offers a practical alternative source. Ifincluded daily in the diet, these could ensure an adequate vitamin C intake forolder people.
Preparing vegetables long before they are cooked can lead to loss of vitamin C.Prolonged cooking or storage of fruit and vegetables can also lead to substantialloss of vitamin C content, so it is wise to cook these foods for as short a time aspossible, and not to keep them hot for too long. This practice is not alwaysused in the provision of meals in residential care accommodation andcommunity meals, so a change in practice may be required.
Sources of vitamin CFruit and fruit juices, potatoes and other vegetables are all sources of vitaminC. Some drinks are fortified with vitamin C – for example blackcurrant andorange squashes and juice drinks. For more details on sources of vitamin Csee Appendix 3.
Vitamin A(retinol equivalents)
Reference Nutrient Intake
WOMEN:600 micrograms a day
MEN:700 micrograms a day
Vitamin A comes in two forms: retinol, which is found only in animal products,and carotene – the yellow or orange pigment found in fruit and vegetables –which can be converted to retinol by the body. If a food contains both retinoland carotene, the total vitamin A content is expressed as units of retinolequivalents.
Vitamin A is often thought of as the ‘anti-infection’ vitamin as it plays animportant role in maintaining the immune system.
Sources of vitamin ASources of retinol are liver, and fat spreads such as margarine. As very fewfoods provide vitamin A naturally in the diet, all margarines in the UK are bylaw fortified with vitamin A (and vitamin D). Many low-fat spreads are alsofortified, so it is worth checking the labels.
Carotene is found in leafy green vegetables, carrots, orange-fleshed sweetpotato, and fruits such as apricots, canned or fresh peaches, plums, prunes,mangoes and papayas. For more details on sources of vitamin A seeAppendix 3.
COMA RECOMMENDATIONS

Chapter 4 Nutritional requirements of older people
35
Vitamin D
Reference Nutrient Intake
10 micrograms a day*
* to be supplied either through thediet or as a supplement
Vitamin D is needed for healthy bones and to maintain muscle strength. Lack ofvitamin D contributes to bone disorders leading to bone fractures, including hipfractures, and bone pains.
The action of summer sunlight on skin can produce enough vitamin D to meetthe needs of most adults in the UK. However, older people are more likely tostay indoors and, if outside, they may be fully covered with thick clothes.Furthermore, the skin is less able to make vitamin D as people age, and thekidneys are less able to convert vitamin D into its active form.
COMA recommends a daily intake of 10 micrograms of vitamin D. For olderpeople in residential care who rarely go outside it is likely that supplements ofvitamin D will be needed as it is impossible for most people to get sufficientvitamin D from the diet alone.13 Advice on vitamin D supplementation shouldbe taken from a GP.
Osteomalacia is the adult form of rickets. It is a painful bone disorder in adultsresulting from low vitamin D and it may still be something to look out for inAsian communities and housebound older people. Osteomalacia can beprevented by an adequate vitamin D intake. Poor vitamin D status may alsocontribute to the development of osteoporosis.
Sources of vitamin DDietary sources of vitamin D include oily fish such as mackerel, herring,tuna, salmon and pilchards. Margarine and several breakfast cereals have thisvitamin added. Extra vitamin D can be given as tablets taken regularly or inan injection given once every few months, under medical supervision. Toomuch vitamin D can be harmful. For more details on sources of vitamin Dsee Appendix 3.
Calcium
Reference Nutrient Intake
700mg a day
One of the most common disorders among older people, especially olderwomen, is osteoporosis – the loss of minerals which causes thinning andweakening of the bones. Taking additional calcium in old age can help toincrease bone mass in some older people.13 It is prudent to maintain a gooddaily calcium intake as well as ensuring that vitamin D status is adequate as thisis needed for the body to absorb calcium.
Recent evidence has also pointed out the importance of physical activity toolder people as a protection against osteoporosis (see page 23).
Sources of calciumSources of calcium include: milk and foods made with milk, such as yoghurt,cheese, milky drinks, custards and milk puddings; and foods made withwhite or brown flour such as bread, pasta and biscuits. Other sources arecanned pilchards, sardines, and salmon (if the soft bones of the fish are alsoeaten). For more details on sources of calcium see Appendix 3.
COMA RECOMMENDATIONS

Chapter 4 Nutritional requirements of older people
36
Iron
Reference Nutrient Intake
8.7mg a day
Iron is an essential part of haemoglobin, which carries oxygen in the red bloodcells. A deficiency in iron will cause anaemia.
Iron status among older people in residential care was measured in the NationalDiet and Nutrition Survey8 and it was found that 52% of men and 39% ofwomen had low haemoglobin levels and about 10% of older people inresidential care had low serum ferritin levels. Intakes of iron were low for asubstantial proportion of older people in residential care with only 6% of ironprovided from ‘haem’ or animal sources (the form of iron absorbed best by thebody – see below).
In older people the gut may not be as effective at absorbing iron as in youngerpeople and therefore the iron needs to be in a form that is readily absorbed.The iron in meat, offal and oily fish is the most readily absorbed. The iron incereals, pulses and vegetables tends to be more difficult to absorb, butabsorption is enhanced if vitamin C is present at the meal. Evidence suggeststhat iron status in older people is positively enhanced by alcohol, vitamin C,protein and fibre in the diet.12 A varied diet containing meat, poultry, fish,vegetables and fruit and moderate intakes of alcohol may make a positivecontribution to the iron status of older people. While tannins in tea and phyticacid in cereal grains have been shown to affect iron absorption from non-haemsources in the intestine, tea-drinking and fibre intake were not shown tocorrelate with low iron status in the National Diet and Nutrition Survey.12
Sources of ironSources of iron include liver, kidney, red meat, oily fish, pulses and nuts(including nuts which have been ground for use in cooking). Ironpreparations should only be given if prescribed by a medical practitioner.For more details on sources of iron see Appendix 3.
Zinc
Reference Nutrient Intake
WOMEN: 7mg a dayMEN: 9.5mg a day
Zinc plays a major role in the functioning of every organ in the body. It isneeded for normal metabolism of protein, fat and carbohydrate and isassociated with the hormone insulin which regulates the body’s energy. Zinc isalso involved in the immune system, the use of vitamin A and in woundhealing. Average intakes of zinc among older people in the UK have beenfound to be below the Reference Nutrient Intake8 and older people with lowerblood measures of zinc have been shown to be at greater risk ofundernutrition.14
Sources of zincSources of zinc include liver, kidney, lean meat, corned beef, whole graincereals, canned sardines, nuts, eggs, milk and pulses. For more details onsources of zinc see Appendix 3.
COMA RECOMMENDATIONS

Chapter 4 Nutritional requirements of older people
37
Sodium
Not more than 2,400mgsodium (6g salt) a day
The most common form of sodium in the diet is salt (sodium chloride). Sodiumis also found in taste-enhancers such as monosodium glutamate, in sodiumbicarbonate, and in sodium nitrate (a preservative found in bacon).
The recent report of the Scientific Advisory Committee on Nutrition (SACN) onsalt and health15 recommends that people of all ages should reduce their saltintake to help prevent high blood pressure, strokes and coronary heart disease.Older people are no exception to this advice. The average intake of salt in theUK is 9g a day and the advice is to reduce this to 6g a day. In the National Dietand Nutrition Survey salt was usually added at table by half of men and a thirdof women in residential care. Reducing habitual salting of foods already saltedin cooking may need to be considered.
However, any severe reduction in salt should be made only on the basis ofmedical advice. Low intakes of salt in the diet can lead to sodium depletion,especially in those over the age of 85, the majority of whom are on salt-losingwater tablets. Low intake of salt can lead to confused mental states. Also, lowsalt diets tend to be very bland and may well depress an already poor appetite.
If salty foods are being restricted, it is important to ensure that the food is stilltasty and appetising. Imaginative use of herbs, spices, lemon juice, mustard,onion and celery to flavour food can help reduce the amount of salt needed.
Sources of sodiumSources of sodium include table salt and cooking salt, processed meats (suchas ham and bacon), cheeses and salted smoked foods, and manymanufactured foods, especially soups and sauces. For more information onfoods that are high in salt, see Appendix 3.
Potassium
Reference Nutrient Intake
350mg a day
Lack of potassium is probably more common in older people than is generallyrealised. In the National Diet and Nutrition Survey, average intakes of potassiumamong people in residential care were below the Reference Nutrient Intake,and two-thirds of older people in residential care had very low intakes ofpotassium (below the Lower Reference Nutrient Intake).8
Low potassium intake leads to depression, muscular weakness, mentalconfusion, and loss of appetite. One of the major causes of potassium lossamong older people is the use of drugs to control either blood pressure oroedema (fluid retention). Patients taking these drugs should be regularlymonitored by blood tests. This is important to ensure that they do not becomeshort of potassium.
Sources of potassiumSources of potassium include fruit (especially bananas and all dried fruits),coffee (both instant coffee and ground coffee beans), fruit juices, potatoesand other vegetables. For more details on sources of potassium, seeAppendix 3.
COMA RECOMMENDATIONS
RECOMMENDATIONS

Chapter 4 Nutritional requirements of older people
38
Fluids
1.5 litres a day (just over 21/2 pints, orabout 8 teacups)
A regular and adequate intake of fluids is extremely important for older people.It helps prevent dehydration, which can lead to confused states; helps toprevent and alleviate the symptoms of constipation; and helps to ‘flush thesystem’, carrying away toxins.
Older people should aim to drink about eight cups of non-alcoholic fluid aday.16 Tea and coffee are sociable and relatively cheap drinks. Milky drinks areeasy to digest and an excellent source of nutrients, especially calcium. Fruitjuices contain vitamin C. Fruit squashes could also be used to increase totalfluid intake.
Many older people have a fading sense of thirst and therefore forget to drink.Also, some may be frightened to drink because of fear of incontinence. Thesepeople need individual consideration, perhaps with a timetable of which timessuit best for their drinks: for example not just before bedtime.
For people with renal failure there may be specific limits to fluid intake.
Alcohol
Some older people drink to excess, but this is rare for those in residential careaccommodation. The Royal College of Psychiatrists acknowledges that “a drinkor two may revive a jaded appetite”.17 In residential homes and nursing homes,having the opportunity to meet and have a drink before a meal will often helppeople socialise, which in itself can stimulate the appetite. Moderate alcoholintakes have also been shown to enhance iron status in older people.12
Alcohol has a dehydrating effect, so older people who drink alcohol should beadvised to drink extra fluid to compensate. Excessive alcohol intake isassociated with undernutrition and deficiencies of some vitamins and minerals,particularly thiamin, folate and vitamin C.18 Sources of advice on alcohol abusecan be found in Appendix 6. Less healthy older people should be advised todrink alcohol sparingly or not at all.
RECOMMENDATIONS

Chapter 4 Nutritional requirements of older people
39
References
1 Department of Health. 1991. DietaryReference Values for Food Energy andNutrients for the United Kingdom.Report on Health and Social SubjectsNo. 41. Report of the Panel on DietaryReference Values of the Committee onMedical Aspects of Food Policy.London: HMSO.
2 Department of Health. 1992. TheNutrition of Elderly People. Report onHealth and Social Subjects No. 43.Report of the Working Group on theNutrition of Elderly People of theCommittee on Medical Aspects ofFood Policy. London: HMSO.
3 Bunker VV, Clayton B. 1989. Researchreview: Studies in the nutrition ofelderly people with particular referenceto essential trace elements. Age andAgeing; 18: 422-29.
4 Widdowson EM. 1992. Physiologicalprocesses of aging: are there specialnutritional requirements for elderlypeople? Do McCay’s findings apply tohumans? American Journal of ClinicalNutrition; 55 (6 suppl): 1246s-1249s.
5 Lehmann AB. 1991. Nutrition in oldage: an update and questions forfuture research. Part 1. Reviews inClinical Gerontology; 1: 135-45.
6 Mobarhan S, Trumbore LS. 1991.Nutritional problems of the elderly.Clinical Geriatric Medicine; 7 (2): 191-214.
7 Sullivan DH, Walls RC. 1994. Impact ofnutritional status on morbidity in apopulation of geriatric rehabilitationpatients. Journal of the AmericanGeriatrics Society; 42: 471-77.
8 Finch S, Doyle W, Lowe C, Bates CJ etal. 1998. National Diet and NutritionSurvey: People Aged 65 Years andOver. Volume 1: Report of the Diet andNutrition Survey. London: TheStationery Office.
9 Nes M, Sem SW, Rousseau B et al.1988. Dietary intakes and nutritionalstatus of old people with dementialiving at home in Oslo. EuropeanJournal of Clinical Nutrition; 42: 581-93.
10 Goode HF, Burns E, Walker BE. 1992.Vitamin C depletion and pressuresores in elderly patients with femoralfracture. British Medical Journal; 305:925-27.
11 Chandra RK. 1992. Effect of vitaminand trace element supplementation onimmune responses and infection inelderly subjects. The Lancet; 340:1124-27.
12 Doyle W, Crawley H, Robert H et al.1999. Iron deficiency in older people:Interactions between food and nutrientintakes with biochemical measures ofiron: further analysis of the NationalDiet and Nutrition Survey of peopleaged 65 years and over. EuropeanJournal of Clinical Nutrition; 53: 552-59.
13 Department of Health. 1998. Nutritionand Bone Health. London: TheStationery Office.
14 Margetts BM, Thompson RL, Elia M etal. 2003. Prevalence of risk ofundernutrition is associated with poorhealth status in older people in the UK.European Journal of Clinical Nutrition;57: 69-74.
15 Scientific Advisory Committee onNutrition. 2003. Salt and Health.London: The Stationery Office.
16 EURONUT-SENECA; Lisette CPGM etal (eds). 1991. Nutrition and the elderlyin Europe. European Journal of ClinicalNutrition, 45 (Suppl 3): 1-196.
17 Royal College Physicians. 1986.Alcohol: Our Favourite Drug. London:Tavistock Publications.
18 Dunn FJ. 1994. Misuse of alcohol anddrugs by elderly people. BritishMedical Journal; 308: 608-09.

40
Chapter 5
Nutritionalguidelinesfor foodprepared forolder people
This chapter provides nutritional guidelines for foodprepared for older people, recommended by the CarolineWalker Trust Expert Working Group. It looks first at foodprepared for people living in residential and nursinghomes, and then at community meals.
The Working Group recognisesthat simply providing foodthat meets these guidelines
will not necessarily mean that olderpeople consume the necessarynutrients. It is important to create theright sort of environment for eating,and to provide food which tastesgood, looks good and is wellpresented, in order to increase thelikelihood that the older person willeat the complete meal. Portion sizesare also important: serving portionsthat are too large may be offputting,while portions that are too small mayleave the older person still feelinghungry afterwards. These issues arediscussed in more detail in Chapter 8.
In many cases cost can be the mainconsideration when providing food,and caterers are often expected tomeet low cost targets which may wellresult in the nutritional content beingcompromised. It is vital, therefore,that cost considerations should notoverride the need for adequatenutritional content in the planningand preparation of food for olderpeople.
Food prepared for people inresidential andnursing homes People living in residential andnursing homes have, in many cases,100% of their food provided by thehome. Evidence suggests that there iscause for concern about thenutritional status of people who livein residential care, particularly thosewho are very old.1 The WorkingGroup therefore recommends thatthe average day’s food over a one-week period for people in residentialand nursing homes should meet theCOMA report’s2 Estimated AverageRequirement for energy and
Reference Nutrient Intakes for selectednutrients. (See page 29 for anexplanation of these terms.) Asummary of these guidelines is givenin Table 2 on the next page.
Regular monitoring to ensure thatresidents are well nourished is animportant part of the nutritionalprogramme. Older people’s nutritionalrequirements may change from time totime depending on their state ofhealth, so their dietary intake mayneed to change to reflect this. Somesimple and reliable methods ofassessing nutritional well-being aregiven in Chapter 7 and in Appendix 5.
In order to meet the nutritionalguidelines set out on the next page,the Working Group recommends thatadequate financial provision is madeto ensure that residents’ meals are ofsufficient nutrient quality.
Some example one-week menus forolder people living in residential careaccommodation, which meet thesenutritional guidelines, are given inChapter 6.
Notes on Table 2
SodiumThe Reference Nutrient Intake for sodium(1,600mg a day) indicates the amount neededphysiologically by most of the population. Mostof the sodium in the diet comes from salt andmost diets provide salt intakes greatly in excessof this figure. The current recommendation forsalt intakes for all adults is 6g a day3 and thecurrent daily intake by adults is approximately9g. Caterers in residential care accommodationshould attempt to reduce the use of highlysalted foods and salt in cooking, as acontribution to reducing current intakes.
Vitamin DIt is impossible for most older adults to obtainthe full daily requirement of 10 micrograms ofvitamin D from the diet alone. It is likely thatolder adults in residential accommodation whorarely go outside will need vitamin Dsupplements.4 They should seek medical adviceabout this (see page 35).

Chapter 5 Nutritional guidelines for food prepared for older people
41
ENERGY (calories) EAR WOMEN aged 75 and over: 1,810kcal (7.6MJ) MEN aged 75 and over: 2,100kcal (8.8MJ)
FAT 35% of food energyWOMEN aged 75 and over: 70g MEN aged 75 and over: 82g
STARCH AND INTRINSIC 39% of food energyAND MILK SUGARS WOMEN aged 75 and over: 188g
MEN aged 75 and over: 218g
NME SUGARS 11% of food energyWOMEN aged 75 and over: 53g MEN aged 75 and over: 62g
FIBRE DRV 18g(non-starch polysaccharides, or NSP)
PROTEIN RNI WOMEN: 46.5g MEN: 53.3g
B VITAMINS Thiamin RNI WOMEN: 0.8mgMEN: 0.9mg
Riboflavin RNI WOMEN 1.1mg MEN 1.3mg
Niacin RNI WOMEN: 12mg MEN: 16mg
FOLATE RNI 200 micrograms
VITAMIN C RNI 40mg
VITAMIN A (retinol equivalents) RNI WOMEN: 600 microgramsMEN: 700 micrograms
CALCIUM RNI 700mg
IRON RNI 8.7mg
ZINC RNI WOMEN: 7mgMEN: 9.5mg
POTASSIUM RNI 350mg
SODIUM Not more than 2,400mg sodium (6g salt)
Table 2 Nutritional guidelines for foodprepared for older people inresidential or nursing homesThese guidelines provide figures for therecommended nutrient content of an average day’sfood for an older person over a one-week period.
EAR = Estimated Average RequirementDRV = Dietary Reference ValueRNI = Reference Nutrient IntakeFor an explanation of these terms see page 29.
See also the notes on Sodium and Vitamin D atthe bottom of page 40.
These nutritional guidelines have been preparedby The Caroline Walker Trust Expert WorkingGroup, and are based on the COMA report onDietary Reference Values for Food Energy andNutrients for the United Kingdom.2

Chapter 5 Nutritional guidelines for food prepared for older people
42
Community mealsIn this report the term ‘communitymeals’ includes:
• meals delivered to people’s homes
• meals provided for those living insheltered accommodation
• meals served in lunch clubs.
The number of community mealsserved to an individual each weekvaries from one meal to seven mealsa week. Most meals provided atlunch clubs or delivered to people’shomes are the ‘main meal of the day’.In many local authorities thenutritional content of communitymeals is based either on theguidelines of the Advisory Body forSocial Service Catering (now theNational Association of CareCatering: NACC)5 or on thenutritional guidelines for communitymeals for older people published bythe Caroline Walker Trust WorkingGroup in the first edition of thisreport. The rationale for the CarolineWalker Trust guidelines published inthis report is explained below.
Conventionally a main meal wouldbe expected to provide 33% of theEstimated Average Requirement forenergy and 33% of the ReferenceNutrient Intakes for other nutrients.Among vulnerable housebound olderpeople, however, community mealsare likely to need to provide a greaterproportion of nutrients,1 especially ifthese meals are not provided everyday. In order to ensure thatcommunity meals make a significantcontribution to the nutritional needsof those vulnerable older peoplewho are likely to be the recipients ofthese meals, the Working Grouprecommends that the proportion ofrequirements be increased from 33%to 40% for energy, calcium, iron andzinc, and to 50% for folate andvitamin C. This should enablecommunity meals to deliver as muchnutritional benefit as possible, whilekeeping meals attractive. This may bebest achieved among those withsmaller appetites by providing a mealand a snack. A summary of theseguidelines is given in Table 3 onpage 44.
It has been suggested that increasingthe nutritional content of communitymeals will place an additionalfinancial burden on a service whichis already financially stretched.However, although increasing thenutritional content of the meal mightincrease the cost of the food, therewould be only a minor increase inthe costs of overheads ofpreparation, packaging and delivery,which represent a substantialproportion of the total cost ofproviding the meals.
Changes in the provision ofcommunity meals in some areas hasled to the use of less frequent (oftenfortnightly) frozen meal deliveries toolder people for regeneration inmicrowaves. The evaluation of theeffectiveness of meal provision in thisway needs to be investigated as amatter of urgency. Research isneeded to find out how much of themeal is eaten by those receivingcommunity meals and how theservice can best meet the needs of itsusers. For some older people theperson who delivers the communitymeal will be the only person theywill see that day. Community mealsproviders can therefore act as the‘eyes and ears’ of social services andcan report back any individualproblems. The wider implications ofrecent changes to meal service alsoneed to be investigated.
Alternative methods of providingfood – such as smaller meals andsnacks which together comprise thenutrients more usually associatedwith a main meal – also need to beevaluated. Suggestions as to how thecommunity meals delivery servicecan be usefully extended are givenon page 50.
For those residents living in verysheltered housing accommodationwho are provided with two meals aday, which may form the majority oftheir nutrient intake, it would beprudent for each meal to fufil therecommendations given here for acommunity meal. This would ensurethat these residents receive at least80% of average energy needs and100% of the current ReferenceNutrient Intake for folate and vitaminC from the food provided.
Most older people who receivecommunity meals get only two orthree such meals a week. It istherefore recommended that, forenergy and for the five nutrientslisted below, an average communitymeal should provide more than just33% of the recommendation for anaverage day’s food.This will enablethe community meal to deliver asmuch nutritional benefit as possibleand still remain attractive andappetising.
ENERGY Not less than 40% of theEstimated AverageRequirement
The importance of maintaining anadequate energy intake has beenstressed by the COMA WorkingGroup on the Nutrition of theElderly. The ‘thin, frail, old lady’ isusually an undernourished personwhose smallness represents severalyears of progressive weight loss.Such a person has no reserves forfuture episodes of ill health. Peoplewho are ill need more calories, andextra care needs to be taken bothbefore and after illness to ensure thatincreased nutritional needs are met.6
Since being ill is often one of thecriteria for receiving communitymeals at home, this group mayrequire more calories than theirsedentary lifestyles may at firstindicate. Increasing the calorie intakeof a community meal would alsoenable more nutrients to be providedand help to compensate for the dayswhen no community meal isprovided and lower energy intakesare likely.
FOLATENot less than 50% of theReference Nutrient Intake
Folate deficiency is associated with aparticular form of anaemia and boththe intakes of folate and folate statushave been found to be low in someolder people both in residential careand living in their own homes.1 Lowfolate status is also more commonamong older people with dementia,many of whom live in their own

Chapter 5 Nutritional guidelines for food prepared for older people
43
homes and receive communitymeals. The amount of folaterecommended to be provided by acommunity meal has increased sincethe first edition of this report (from40% to 50% of the Reference NutrientIntake) to reflect continuing evidenceof low folate status among vulnerableolder people.
VITAMIN C Not less than 50% of theReference Nutrient Intake
Low vitamin C intakes have beenreported both among older people inresidential care and among thoseliving in their own homes.1 Sufficientvitamin C with meals is alsoimportant to aid iron absorption.
CALCIUMNot less than 40% of theReference Nutrient Intake
Low intakes of calcium among someolder people living in their ownhomes have been reported1 andtherefore it would seem prudent toensure that the community mealprovided sufficient calcium to offersome protection against low intakes.
IRONNot less than 40% of theReference Nutrient Intake
Low iron status has been reportedboth among people in residentialcare and among those living in theirown homes, and low iron statusincreases with increasing age.1 Sincethe majority of people receivingcommunity meals will be both veryold and frail and at increased risk oflow iron status, community mealsshould aim to offer at least 40% ofthe daily Reference Nutrient Intakefor iron. Ensuring sufficient vitamin Cwith meals is also important.
Older people are vulnerable to irondeficiencies for three main reasons.Firstly, they tend to have a reducedintake of iron-rich foods. Secondly, insome older people the gut mayabsorb nutrients less efficiently.Thirdly, some older people mayconsume smaller amounts of vitamin
C rich foods which can help iron tobe absorbed.
ZINCNot less than 40% of theReference Nutrient Intake
Average intakes of zinc among olderpeople have been shown to be lowerthan the Reference Nutrient Intake.Zinc plays an important role inmaintaining the immune system andin wound healing and low intakesmay be contributory to other chronicdiseases and undernutrition in olderpeople.

Chapter 5 Nutritional guidelines for food prepared for older people
44
ENERGY (calories) Not less than 40% of EAR WOMEN aged 75 and over: 724kcal (3MJ)MEN aged 75 and over: 840kcal (3.5MJ)
FAT 35% of food energyWOMEN aged 75 and over: 28g MEN aged 75 and over: 33g
STARCH AND INTRINSIC 39% of food energyAND MILK SUGARS WOMEN aged 75 and over: 75g
MEN aged 75 and over: 87g
NME SUGARS 11% of food energyWOMEN aged 75 and over: 21g MEN aged 75 and over: 24g
FIBRE Not less than 33% of DRV 6g(Non-starch polysaccharides, or NSP)
PROTEIN Not less than 33% of RNI WOMEN: 15gMEN: 18g
B VITAMINS
Thiamin Not less than 33% of RNI 0.3mg
Riboflavin Not less than 33% of RNI 0.4mg
Niacin Not less than 33% of RNI WOMEN: 4mg MEN: 5mg
FOLATE Not less than 50% of RNI 100 micrograms
VITAMIN C Not less than 50% of RNI 20mg
VITAMIN A Not less than 33% of RNI WOMEN: 200 micrograms(retinol equivalents) MEN: 230 micrograms
CALCIUM Not less than 40% of RNI 280mg
IRON Not less than 40% of RNI 3.5mg
ZINC Not less than 40% of RNI WOMEN: 2.8mg MEN: 3.8mg
POTASSIUM Not less than 33% of RNI 115mg
SODIUM Not more than 40% of the 960mg sodium (equivalent to 2.4g salt) recommended maximum intake of 2,400mg sodium a day (6g salt a day)
Table 3 Nutritional guidelines for communitymeals for older peopleThese guidelines provide figures for the recommendednutrient content of community meals for an older personover a one- or two-week period.
EAR = Estimated Average RequirementDRV = Dietary Reference ValueRNI = Reference Nutrient IntakeFor an explanation of these terms see page 29.
See also the notes on Sodium and Vitamin D at thebottom of page 45.
These nutritional guidelines have been prepared byThe Caroline Walker Trust Expert Working Group, andare based on the COMA report on Dietary ReferenceValues for Food Energy and Nutrients for the UnitedKingdom.2

Chapter 5 Nutritional guidelines for food prepared for older people
45
Notes on Table 3
SodiumThe Reference Nutrient Intake for sodium(1,600mg a day) indicates the amount neededphysiologically by most of the population. Mostof the sodium in the diet comes from salt andmost diets provide salt intakes greatly in excessof this figure. The current recommendation forsalt intakes for all adults is 6g a day3 and thecurrent daily intake by adults is approximately9g. Caterers in residential care accommodationshould attempt to reduce the use of highlysalted foods and salt in cooking, as acontribution to reducing current intakes.
Vitamin DIt is impossible for most older adults to obtainthe full daily requirement of 10 micrograms ofvitamin D from the diet alone. It is likely thatolder adults in residential accommodation whorarely go outside will need vitamin Dsupplements.4 They should seek medical adviceabout this (see page 35).
Recommendations• The average day’s food, over a one-week period, for
people living in residential care accommodation, shouldmeet the COMA report’s Estimated Average Requirementfor energy and the Reference Nutrient Intakes for selectednutrients. Quantified nutritional guidelines for foodprepared for older people in residential or nursing homesare given in Table 2 on page 41.
In relation to community meals, the Working Grouprecommends that:
• The average community meal should provide a minimumof 33% of the Dietary Reference Values prepared byCOMA in 1991, except for energy and certain keynutrients, which should be provided at higher levels.
• In view of the common occurrence of undernutrition inhousebound older people living in their own homes,providers should increase the energy, calcium, iron andzinc content of community meals to 40% of the DietaryReference Values, and the folate and vitamin C content to50%. Quantified nutritional guidelines for communitymeals are given in Table 3 on page 44.
• Research is needed to find out how much of the meal iseaten by those who receive community meals, and howthe service can best meet the needs of its users.Alternative methods of providing food – such as smallermeals and snacks which together comprise the nutrientsmore usually associated with a conventional meal – alsoneed to be evaluated.
References1 Finch S, Doyle W, Lowe C, Bates CJ et
al. 1998. National Diet and NutritionSurvey: People Aged 65 Years andOver. Volume 1: Report of the Diet andNutrition Survey. London: TheStationery Office.
2 Department of Health. 1991. DietaryReference Values for Food Energy andNutrients for the United Kingdom.Report of the Panel on DietaryReference Values of the Committee onMedical Aspects of Food Policy.London: HMSO.
3 Scientific Advisory Committee onNutrition. 2003. Salt and Health.London: The Stationery Office.
4 Department of Health. 1998. Nutritionand Bone Health. London: TheStationery Office.
5 National Association of Care Catering.2003. A Recommended Standard forCommunity Meals. Seewww.carecatering.org.uk
6 McLaren S, Crawley H. 2000.Managing nutritional risks in olderadults. Nursing Times ClinicalMonographs No. 44. London: NTBooks.

46
Chapter 6
Examples ofmenus whichmeet thenutritionalguidelines
Table 4 on pages 47-48 givessome example one-weekmenus for older people living
in residential or nursing homes.Table 5 on page 49 gives someexample menus for communitymeals.
These menus may not be suitable forsome older people from black andethnic minorities, and differentmenus may need to be designed.When devising menus, it is importantnot to generalise, but rather to askclients about their preferences. Thecommunity meals given in Table 6are very general examples to showthat Asian or Afro-Caribbean mealscan meet the nutritional guidelines.
Excellent resources on Afro-Caribbean foods and menus suitablefor use in care homes have beenproduced by the Relatives andResidents Association AfricanCaribbean Elders Project. Details ofthese can be found on page 76.
When planning and preparing meals,it is important that fruit andvegetables are not stored or cookedfor too long, as this leads to loss ofvitamin C. Older people who havedifficulty eating whole fruit andvegetables can have them stewed,puréed or made into soups. Try andensure that older people have at leastfive portions of a wide variety offruits and vegetables every day.
In order to stimulate an interest infood, it is important to avoid over-repetition of menus. Popular mealscan of course be provided at frequentintervals, but the ‘shepherd’s pieevery Wednesday’ syndrome shouldbe avoided. A five-week menu cycle,which is changed every three monthsor so, offers scope for variety andchoice. This pattern is already usedin many residential and nursinghomes.
Many older people enjoy meatdishes, but future generations willneed a much broader menu,including vegetarian meals, pastadishes and curries.
Menu planning softwareFollowing the publication of the firstedition of this report, the CarolineWalker Trust developed the CORAMenu Planner computer program1
which helps residential and nursinghomes to plan nutritionally balancedmenus for groups of older people.The menu planner can analyse thenutritional value of a weekly menuand displays the findings on an easy-to-read bar chart.
The program contains a recipe librarydatabase of over 800 dishes, snacksand drinks, complete with anutritional analysis of each item andrecipes where appropriate. Somerecipes for ethnic foods are alsoincluded. Additional dishes can alsobe added if a nutritional analysis canbe provided. The program provides ablank weekly menu planner and themenu can be easily built up bychoosing foods and drinks from thedatabase to make 7-day menus forone to eight complete weeks. Youcan then assess how the nutritionalcontent of your menus compareswith the guidelines in this report. Ifyour menus are too high or too lowin particular nutrients, the programcan identify alternative dishes whichwill help you meet the nutritionalguidelines. It will also help you lookat the frequency of dishes served, toavoid repetitive menus.
The CORA Menu Planner is avaluable tool for residential andnursing homes as it allows you toeasily plan and prepare interestingand nutritionally balanced menus. Itis also a useful tool to help staffunderstand more about food andnutrients and to provide all thoseinvolved in food provision with abetter understanding of how eatingwell can be achieved.
The CORA Menu Planner can beobtained from The Caroline WalkerTrust at a cost of £50 (see page 2).
This chapter demonstrates that it is not difficult toproduce uncomplicated menus which meet thenutritional guidelines given in Chapter 5.

Chapter 6 Examples of menus which meet the nutritional guidelines
47
BREAKFAST
MID-MORNING
LUNCH
MID-AFTERNOON
EVENINGMEAL
BEDTIME
Table 4 Example menus for older people livingin residential or nursing homes
MONDAY
Fruit juice
Steak andkidney pie
Mixedvegetables
Cauliflower
Mashedpotato
Trifle
Water
Tea or coffeewith milk
Toastedteacake withbutter or poly- unsaturatedmargarine
Kedgeree
Canned peas
Instantdessert
Fresh apple
Water or fruit juice
TUESDAY
Fruit juice
Chickenfricassee
Carrots
Broccoli
Mashedpotato
Apple pie and custard
Water
Tea or coffeewith milk
Fruit sconewith butter or poly-unsaturatedmargarine
Scrambledegg
Toast and butter
Chocolateeclair
Banana
Water or fruit juice
WEDNESDAY
Fruit juice
Roast pork and applesauce
Cabbage
Sweetcorn
Roastpotatoes
Rhubarbcrumble and custard
Water
Tea or coffeewith milk
Jam sponge
Fish cakes and tomato
Cherry pie
Fresh orange
Water or fruit juice
THURSDAY
Fruit juice
Braised liver
Swede
Sprouts
Mashedpotato
Lemonmeringue pie
Water
Tea or coffeewith milk
Plain sconewith butter or poly- unsaturatedmargarineand jam
Cheese andtomatoquiche
Spaghettihoops
Arctic roll
Fresh apple
Water or fruit juice
FRIDAY
Fruit juice
Fried haddock
Peas
Chippedpotatoes
Bread andbutter pudding
Water
Tea or coffeewith milk
Shortbread
Tomato soup
Roast beefsandwich
Lemon sorbet
Fresh orange
Water or fruit juice
SATURDAY
Fruit juice
Lancashire hot pot
Green beans
Cauliflower
Mashedpotato
Plum tart and custard
Water
Tea or coffeewith milk
Pancake withbutter or poly- unsaturatedmargarine and jam
Macaronicheese withsliced ham
Cannedpeaches and ice cream
Banana
Water or fruit juice
SUNDAY
Fruit juice
Roast beef and Yorkshirepudding
Cabbage
Carrots
Roast potatoes
Rice puddingand jam
Water
Tea or coffeewith milk
Madeira cake
Chicken soup
Egg andcresssandwich
Creme caramel
Fresh apple
Water or fruit juice
Prunes
Porridge or high fibre cereal with milk
Toast (white or wholemeal) with butter/polyunsaturated margarine and marmalade or jam
Tea or coffee with milk*
Tea or coffee with milk and digestive biscuit
Milky drink: Horlicks, Ovaltine, hot chocolate, milky tea or milk shake
NB Residents should be offered additional drinks after meals: 8 cups of fluid a day are recommended.

Chapter 6 Examples of menus which meet the nutritional guidelines
48
BREAKFAST
MID-MORNING
LUNCH
MID-AFTERNOON
EVENINGMEAL
BEDTIME
MONDAY
Chickencasserole
Newpotatoes
Broccoli
Banana flan
Water or fruitjuice
Carrot soup
Welsh rarebit
Tinnedmandarinswith crèmefraîche
Water or fruitjuice
TUESDAY
Baked spicedgammon
Parsley sauce
Mashedpotato
Peas
Stewed pearsand fromagefrais
Water or fruitjuice
Cream ofcelery soup
Corned beefand tomatosandwich
Banana
Water or fruitjuice
WEDNESDAY
Kidney turbigo
Braised rice
Celery
Green beans
Queen ofpuddings andcustard
Water or fruitjuice
Lentil soup
Smokedmackerel pâtéand toast
Fruit yoghurt
Water or fruitjuice
THURSDAY
Haricot oflamb
Croquettepotatoes
Carrots
Apricot condé
Water or fruitjuice
Tomato soup
Tunamayonnaisesandwich
Fresh orange
Water or fruitjuice
FRIDAY
Fish cakes
Homemadeoven chips
Mange-touts
Cheese cake
Water or fruitjuice
Leek andparsley soup
Poached eggon toast
Gooseberryfool
Water or fruitjuice
SATURDAY
Pasta bakedwithmushroomsand cheese
Mixed salad
Ice cream andchocolatesauce
Water or fruitjuice
Mushroomsoup
Chickensandwich
Rosy pears
Water or fruitjuice
SUNDAY
Roast lamb
Gravy
Baked slicedpotatoes
Courgettes
Swede
Lemonmeringue pie
Water or fruitjuice
Vegetablesoup
Cheese andham flan
Mixed beansalad
Butterscotchmousse
Water or fruitjuice
Choice of porridge or high fibre cereals (eg wheat bisks, bran flakes, muesli, shredded wheat)
Fresh citrus juice or cranberry juice
Scrambled eggs, or baked beans, or grilled bacon, or grilled kipper, or grilled tomatoes with toast
Tea or coffee
Choice of fresh fruit slices (apple, pear, banana, orange, melon etc, as in season)
Tea or coffee
Tea or coffee
Choice of: apple and cinnamon cake, banana tea bread, date and raisin tea bread, farmhouse sultana cake, fruit
scones with butter, sticky prune cake or lemon cake
Milky drink: Horlicks, Ovaltine, hot chocolate, milky tea or milk shake
This sample menu uses options from the CORA Menu Planner.1
NB Residents should be offered additional drinks after meals: 8 cups of fluid a day are recommended.

Chapter 6 Examples of menus which meet the nutritional guidelines
49
LUNCH
MID-AFTERNOON
MONDAY
Fruit juice
Steak andkidney pie
Mixedvegetables
Cauliflower
Mashedpotato
Trifle
Tea or coffeewith milk
Toastedteacake
TUESDAY
Fruit juice
Chickenfricassee
Carrots
Broccoli
Mashedpotato
Apple pie and custard
Tea or coffeewith milk
Fruit scone
WEDNESDAY
Fruit juice
Roast porkand applesauce
Cabbage
Sweetcorn
Roastpotatoes
Rhubarbcrumble and custard
Tea or coffeewith milk
Jam sponge
THURSDAY
Fruit juice
Braised liver
Swede
Sprouts
Mashedpotato
Lemonmeringue pie
Tea or coffeewith milk
Plain sconewith jam
FRIDAY
Fruit juice
Fried haddock
Peas
Chippedpotatoes
Bread andbutter pudding
Tea or coffeewith milk
Shortbread
SATURDAY
Fruit juice
Lancashire hot pot
Green beans
Cauliflower
Mashedpotato
Plum tartand custard
Tea or coffeewith milk
Pancakewith jam
SUNDAY
Fruit juice
Roast beef and Yorkshirepudding
Cabbage
Carrots
Roast potatoes
Rice puddingand jam
Tea or coffeewith milk
Madeira cake
NB A drink of water or fruit juice should be offered with the main meal.
Table 5Example menus for community mealsfor older people
The Working Group recommends that the average nutrient content of community meals served over a one- or two-week period should meetthe nutritional guidelines shown on page 44. Individual meals do not have to meet the guidelines in every respect, as long as the average mealdoes meet them.

Chapter 6 Examples of menus which meet the nutritional guidelines
50
LUNCH
AFTERNOONSNACK
South Asianvegetarianmeal
Red lentildhal
Spinach andchick peacurry
Yoghurt raita
Side salad
Rice orchapatiwithout fat
Banana
South Asiannon-vegetarianmeal
Chicken curry
Rice orchapatiwithout fat
Yoghurt raita
Side salad
Grapes
Afro-Caribbeanmeal
Rice andpeas
Jamaicanfricaseedchicken
Sweet potato
Side salad
Semolinapudding
Afro-Caribbeanvegetarianmeal
Cornchowder
Fried yamcakes
Dumplings
Creamedspinach
Tinnedpineapple andcream
MiddleEastern meal
Shammi(lamb) kebabs
Spicy pilaurice
Tabbouleh
Green salad
Halva
Asian meal
Indonesianfish curry
Rice
Stir-friedvegetables
Bananafritters
Asianvegetarianmeal
Sweet andsourvegetables
Rice
Fried tofu
Rice pudding
NB A drink of water or fruit juice should be offered with the main meal.
Table 6Examples of community meals suitable for older peoplefrom Asian and Afro-Caribbean backgrounds*
Tea or coffee with: spiced bread pudding, carrot cake, frosted coconut cake, honey cake, malted fruit loaf, orangeand cinnamon cake or gingerbread.
* The menus in Table 6 are just examples for particular groups of people. The Working Group recognises that menus have to be adapted tosuit different cooking styles and tastes. The Working Group recommends that the average nutrient content of community meals served overa one- or two-week period should meet the nutritional guidelines shown on page 44. Individual meals do not have to meet the guidelines inevery respect, as long as the average meal does meet them.
Delivering informationand advice with thecommunity meals service
Local authorities should considerways of extending the communitymeals delivery service to providegreater support to vulnerable olderpeople living in their own homes.
• Information could be provided onsnacks and easy-to-prepare meals.Some useful leaflets are producedby NAGE (see page 75).
• Information on shopping services,local food deliveries, food co-ops,community cafés and otherinitiatives could be provided.
• Older people could be encouragedto keep a ‘food store’ of cans orfrozen foods which can be used tomeet unexpected needs, forexample if the person is ill.Checking food stores to ensure
foods are not out of date is alsoimportant.
• Those delivering community mealsare in the unique position of beingable to offer advice and support onother key areas related to thehealth and well-being of olderpeople, for example: encouragingphysical activity, advising onkeeping warm, encouragingmaintenance of social intereststhrough lunch clubs, communitycentres or books on wheelsservices.
• Local authorities should alsoconsider basic training on nutritionfor those who deliver communitymeals so that they can offer goodadvice and be alert to signs ofnutritional deterioration amongvulnerable older people.
Reference1 The Caroline Walker Trust. CORA Menu
Planner. London: DGAA Homelife.Available from The Caroline WalkerTrust (www.cwt.org.uk).

Chapter 7 Nutritional assessments
51
Chapter 7
Nutritionalassessments
This chapter provides guidelines on:
• how to identify older people – living either inresidential care accommodation or in thecommunity – who might be at risk of malnutritionand in need of some form of intervention, and
• how to assess whether food provision forvulnerable older people is adequate andappropriate.
Malnutrition is rarelydiagnosed in olderpeople living at home
and undoubtedly this cause of illhealth, debility and depression is often missed. Risk ofundernutrition is reported to berelated to having a long-standingillness, being more than 85 yearsold, having recently beenhospitalised, or living inresidential care.1 The clinicalsigns of malnutrition, however,may appear only very late, oftenas a sudden illness such aspneumonia, or as a fracture.Before then, there could havebeen long periods of poor dietand low food consumption. Thisemphasises the need to identifyspeedily those older people whoare vulnerable and to treat thembefore they becomemalnourished. It is possible toprevent malnutrition if thecircumstances likely to lead topoor eating and drinking arerecognised and if appropriatecommunity services are there tohelp.
A considerable amount of workon nutritional assessment of olderpeople has been done since thefirst edition of this report waspublished. Nutritional screeningon admission and on a periodicbasis, and weight measurement,are now regulatory in care homes(see Appendix 2).
A clinically validated tool toidentify older people who aremalnourished, called theMalnutrition Universal ScreeningTool (MUST),2 has beendeveloped and evaluated. This
tool is suitable for use in thecommunity and in residential care.It is recommended by The CarolineWalker Trust and has also beenendorsed by the Registered NursingHome Association. Any assessmentmethod should be easy and quickto use and easy to interpret, andthose carrying out the assessmentsneed training. This chapter providessome guidelines on the use of theMUST tool for identifyingmalnutrition and also gives detailsof a simple food-based nutritionalassessment, and assessment of theadequacy of food provision.

Chapter 7 Nutritional assessments
52
How to identifyolder people whomight be at risk ofmalnutritionThe MUST toolThe most important way to identifyolder people who might be at risk ofmalnutrition – for older people livingeither in residential careaccommodation or in the community– is by regular weighing, and byobserving and reporting changes inweight. The MUST tool can detectboth overnutrition (overweight andobesity) and undernutrition. Itprimarily uses measurements ofweight and height, and weightchange.
Measuring weightAccurate and reliable weighing scalesare essential for accurate weightmeasurements. The Caroline WalkerTrust Expert Working Grouprecommends that all residential careestablishments should have weighingscales – preferably sitting scales – for
Men (<65 years) 1.94 1.93 1.91 1.89 1.87 1.85 1.84 1.82 1.80 1.78 1.76 1.75 1.73 1.71
Men (>65 years) 1.87 1.86 1.84 1.82 1.81 1.79 1.78 1.76 1.75 1.73 1.71 1.70 1.68 1.67
Ulna length (cm) 32.0 31.5 31.0 30.5 30.0 29.5 28.5 28.0 27.5 27.0 26.5 26.5 26.0 25.5
Women (<65 years) 1.84 1.83 1.81 1.80 1.79 1.77 1.76 1.75 1.73 1.72 1.70 1.69 1.68 1.66
Women (>65 years) 1.84 1.83 1.81 1.79 1.78 1.76 1.75 1.73 1.71 1.70 1.68 1.66 1.65 1.63
Men (<65 years) 1.69 1.67 1.66 1.64 1.62 1.60 1.58 1.57 1.55 1.53 1.51 1.49 1.48 1.46
Men (>65 years) 1.65 1.63 1.62 1.60 1.59 1.57 1.56 1.54 1.52 1.51 1.49 1.48 1.46 1.45
Ulna length (cm) 25.0 24.5 24.0 23.5 23.0 22.5 22.0 21.5 21.0 20.5 20.0 19.5 19.0 18.5
Women (<65 years) 1.65 1.63 1.62 1.61 1.59 1.58 1.56 1.55 1.54 1.52 1.51 1.50 1.48 1.47
Women (>65 years) 1.61 1.60 1.58 1.56 1.55 1.53 1.52 1.50 1.48 1.47 1.45 1.44 1.42 1.40
Reproduced with permission of the British Association of Parenteral and Enteral Nutrition (BAPEN).
Figure 1Estimating height from ulnalength
Measure between the point of theelbow (olecranon process) and themidpoint of the prominent bone ofthe wrist (styloid process) (left side ifpossible).
carrying out monthly weight checks.The scales should be regularlychecked (calibrated) to make surethat they give an accurate reading.Weight can be measured in eitherimperial measurements (stones andpounds) or metric measurements(kilograms).
Measuring heightTo measure height effectivelyrequires a stadiometer (a height-measuring tool that is either placedagainst a wall or is free-standing).Measurements can be taken inimperial measurements (feet andinches) or metric measurements(metres and centimetres).
However, it can be difficult to getaccurate height measurements forolder people, especially those whoare unable to stand. If you are unableto get a standing heightmeasurement, it is possible toestimate height from the length of thearm between the wrist and the elbow(called the ulna length). See Figure 1below. While this method allowssome estimation of height to bemade, the estimations may be less
appropriate for very elderly peopleand people of different ethnicbackgrounds and should always beused cautiously for the prediction ofBMI (body mass index).
Sometimes, however, it may bedifficult to get either of thesemeasurements – for example ifsomeone is unable to stand orstraighten their arm. If themeasurement cannot be easily made ineither of these ways, then an estimatecan be made from the mid upper armcircumference, as shown in Figure 2.
It is important to remember that poorestimation of height and weight canlead to misleading figures for BMI inolder people, which may misclassifysome older people who are at risk ofmalnutrition.Where it is difficult toobtain height and weight data, moreimportant indicators of risk may beweight loss, illness and leaving food onplates at mealtimes. Difficulties inheight and weight measurementshould always be flagged up on aresident’s care plan and more frequentobservations made of eating anddrinking patterns and any weight lossobserved.
HEI
GH
T(m
)H
EIG
HT
(m)
HEI
GH
T(m
)H
EIG
HT
(m)

Chapter 7 Nutritional assessments
53
Reproduced with permission of the BritishAssociation of Parenteral and EnteralNutrition (BAPEN).
Figure 2Measuring from mid upper armcircumference
The subject’s left arm should be bentat the elbow at a 90o angle, with theupper arm held parallel to the side ofthe body. Measure the distancebetween the bony protrusion on theshoulder (acromion) and the point ofthe elbow (olecranon process). Markthe mid-point.
Ask the subject to let arm hang looseand measure around the upper armat the mid-point, making sure thatthe tape measure is snug but nottight.
Using the MUST toolThe five steps of the MUST tool areshown in detail in Figure 3 on page54.
Step 1 Measuring height and weightto get a BMI score
The height and weight measurementsare used to estimate a BMI scoreusing the chart shown in Figure 4.
Step 2Noting the percentageunplanned weight loss
Unplanned weight loss is a keyindicator of malnutrition. Table 7 (onpage 56) helps to assess weight lossthrough a simple scoring method.Either imperial or metricmeasurements can be used. Thinner
people are at risk with even a smallamount of weight loss. Older peoplewho are overweight or obese canalso be at risk of malnutrition if theyhave significant unplanned weightloss.
Step 3 Establish acute disease effectscore
If an older person is very ill and hasnot eaten for more than five days, orif they are waiting for treatmentwhich requires them to spend severaldays without food, then they are atrisk of malnutrition. Older peoplewho have had surgery and whocannot eat for five days or morefollowing their treatment are also atrisk.
Steps 1-3 of the MUST tool allow arisk score to be identified using the
simple steps outlined (see Figure 3on page 54). The MUST tool alsooffers management guidelines foreach risk group to ensure that theappropriate response is made to anymalnutrition risk.
For further explanation of MUST andadditional information on how tointerpret information for people whohave amputations or plaster casts forexample, contact the MalnutritionAdvisory Group of the BritishAssociation of Parenteral and EnteralNutrition (BAPEN)(www.bapen.org.uk). To obtain aMUST Starter Pack, contact BAPENon 01527 457850.

Chapter 7 Nutritional assessments
54
Figure 3The Malnutrition Universal Screening Tool (MUST)
The Malnutrition Universal Screening Tool (MUST) is a five-step screening tool to identifyadults who are malnourished, at risk of malnutrition (undernutrition), or obese. It is for use inhospitals, in the community and other care settings and can be used by all care workers.
Re-assess subjects identified as at risk as they move through care settings. See The ‘MUST’ Explanatory Booklet for further details and The ‘MUST’ Report for supporting evidence.Reproduced with permission of the British Association of Parenteral and Enteral Nutrition (BAPEN).
If unable to obtain height and weight,see page 52 for alternativemeasurementsand use of subjective criteria.
BMI kg/m2 Score>20(>30 Obese) = 0
18.5 -20 = 1
<18.5 = 2
0Low Risk
Routine clinical care
• Repeat screening Hospital – weekly Care Homes – monthlyCommunity – annually for special groups e.g. those >75 yrs
All risk categories:
• Treat underlying condition and provide help and adviceon food choices, eating and drinking when necessary.
• Record malnutrition risk category.
• Record need for special diets and follow local policy.
Obesity:
• Record presence of obesity. For those withunderlying conditions, these are generallycontrolled before the treatment of obesity.
1Medium Risk
Observe
• Document dietary intake for 3 daysif subject in hospital or care home
• If improved or adequate intake –little clinical concern; if noimprovement – clinical concern -follow local policy
• Repeat screening Hospital – weekly Care Home – at least monthlyCommunity – at least every 2-3months
2 or moreHigh Risk
Treat*
• Refer to dietitian, NutritionalSupport Team or implementlocal policy
• Improve and increase overallnutritional intake
• Monitor and review care planHospital – weekly Care Home – monthlyCommunity – monthly
* Unless detrimental or no benefit is expected from nutritional support e.g. imminent death.
Add Scores together to calculate overall risk of malnutrition.
Score 0 Low Risk Score 1 Medium Risk Score 2 or more High Risk
Unplanned weight lossin past 3-6 months
% Score<5 = 05-10 = 1>10 = 2
If patient is acutely illand there has been or islikely to be no nutritional
intake for >5 daysScore 2
Step 2Weight loss score
Step 4Overall risk of malnutrition
Step 1BMI score
+ + Step 3Acute disease effect score
Step 5Management guidelines

Chapter 7 Nutritional assessments
55
Figure 4BMI score (and BMI)
This chart shows the BMI scores to be used in the Malnutrition Universal Screening Tool (MUST).2
Height (feet and inches)
100 46 44 43 42 41 40 39 38 37 36 35 35 34 33 32 32 31 30 30 29 28 28 15 1099 45 44 43 42 41 40 39 38 37 36 35 34 33 33 32 31 31 30 29 29 28 27 15 898 45 44 42 41 40 39 38 37 36 36 35 34 33 32 32 31 30 30 29 28 28 27 15 697 44 43 42 41 40 39 38 37 36 35 34 34 33 32 31 31 30 29 29 28 27 27 15 496 44 43 42 40 39 38 38 37 36 35 34 33 32 32 31 30 30 29 28 28 27 27 15 295 43 42 41 40 39 38 37 36 35 34 34 33 32 31 31 30 29 29 28 27 27 26 15 94 43 42 41 40 39 38 37 36 35 34 33 33 32 31 30 30 29 28 28 27 27 26 14 1193 42 41 40 39 38 37 36 35 35 34 33 32 31 31 30 29 29 28 27 27 26 26 14 992 42 41 40 39 38 37 36 35 34 33 33 32 31 30 30 29 28 28 27 27 26 25 14 791 42 40 39 38 37 36 36 35 34 33 32 31 31 30 29 29 28 27 27 26 26 25 14 590 41 40 39 38 37 36 35 34 33 33 32 31 30 30 29 28 28 27 27 26 25 25 14 289 41 40 39 38 37 36 35 34 33 32 32 31 30 29 29 28 27 27 26 26 25 25 14 88 40 39 38 37 36 35 34 34 33 32 31 30 30 29 28 28 27 27 26 25 25 24 13 1287 40 39 38 37 36 35 34 33 32 32 31 30 29 29 28 27 27 26 26 25 25 24 13 1086 39 38 37 36 35 34 34 33 32 31 30 30 29 28 28 27 27 26 25 25 24 24 13 885 39 38 37 36 35 34 33 32 32 31 30 29 29 28 27 27 26 26 25 25 24 24 13 684 38 37 36 35 35 34 33 32 31 30 30 29 28 28 27 27 26 25 25 24 24 23 13 383 38 37 36 35 34 33 32 32 31 30 29 29 28 27 27 26 26 25 25 24 23 23 13 182 37 36 35 35 34 33 32 31 30 30 29 28 28 27 26 26 25 25 24 24 23 23 12 1381 37 36 35 34 33 32 32 31 30 29 29 28 27 27 26 26 25 24 24 23 23 22 12 1180 37 36 35 34 33 32 31 30 30 29 28 28 27 26 26 25 25 24 24 23 23 22 12 879 36 35 34 33 32 32 31 30 29 29 28 27 27 26 26 25 24 24 23 23 22 22 12 678 36 35 34 33 32 31 30 30 29 28 28 27 26 26 25 25 24 24 23 23 22 22 12 477 35 34 33 32 32 31 30 29 29 28 27 27 26 25 25 24 24 23 23 22 22 21 12 176 35 34 33 32 31 30 30 39 28 28 27 26 26 25 25 24 23 23 22 22 22 21 11 1375 34 33 32 32 31 30 29 29 28 27 27 26 25 25 24 24 23 23 22 22 21 21 11 1174 34 33 32 31 30 30 29 28 28 27 26 26 25 24 24 23 23 22 22 21 21 20 11 973 33 32 32 31 30 29 29 28 27 26 26 25 25 24 24 23 23 22 22 21 21 20 11 772 33 32 31 30 30 29 28 27 27 26 26 25 24 24 23 23 22 22 21 21 20 20 11 471 32 32 31 30 29 28 28 27 26 26 25 25 24 23 23 22 22 21 21 21 20 20 11 370 32 31 30 30 29 28 27 27 26 25 25 24 24 23 23 22 22 21 21 20 20 19 1169 32 31 30 29 28 28 27 26 26 25 24 24 23 23 22 22 21 21 20 20 20 19 10 1168 31 30 29 29 28 27 27 26 25 25 24 24 23 22 22 21 21 21 20 20 19 19 10 1067 31 30 29 28 28 27 26 26 25 24 24 23 23 22 22 21 21 20 20 19 19 19 10 766 30 29 29 28 27 26 26 25 25 24 23 23 22 22 21 21 20 20 19 19 19 18 10 665 30 29 28 27 27 26 25 25 24 24 23 22 22 21 21 21 20 20 19 19 18 18 10 364 29 28 28 27 26 26 25 24 24 23 23 22 22 21 21 20 20 19 19 18 18 18 10 163 29 28 27 27 26 25 25 24 23 23 22 22 21 21 20 20 19 19 19 18 18 17 9 1362 28 28 27 26 25 25 24 24 23 22 22 21 21 20 20 20 19 19 18 18 18 17 9 1061 28 27 26 26 25 24 24 23 23 22 22 21 21 20 20 19 19 18 18 18 17 17 9 860 27 27 26 25 25 24 23 23 22 22 21 21 20 20 19 19 19 18 18 17 17 17 9 659 27 26 26 25 24 24 23 22 22 21 21 20 20 19 19 19 18 18 17 17 17 16 9 458 26 26 25 24 24 23 23 22 22 21 21 20 20 19 19 18 18 18 17 17 16 16 9 157 26 25 25 24 23 23 22 22 21 21 20 20 19 19 18 18 18 17 17 16 16 16 956 26 25 24 24 23 22 22 21 21 20 20 19 19 18 18 18 17 17 17 16 16 16 8 1155 25 24 24 23 23 22 21 21 20 20 19 19 19 18 18 17 17 17 16 16 16 15 8 854 25 24 23 23 22 22 21 21 20 20 19 19 18 18 17 17 17 16 16 16 15 15 8 753 24 24 23 22 22 21 21 20 20 19 19 18 18 18 17 17 16 16 16 15 15 15 8 452 24 23 23 22 21 21 20 20 19 19 18 18 18 17 17 16 16 16 15 15 15 14 8 351 23 23 22 22 21 20 20 19 19 19 18 18 17 17 16 16 16 15 15 15 14 14 8 050 23 22 22 21 21 20 20 19 19 18 18 17 17 17 16 16 15 15 15 14 14 14 7 1349 22 22 21 21 20 20 19 19 18 18 17 17 17 16 16 15 15 15 14 14 14 14 7 1048 22 21 21 20 20 19 19 18 18 17 17 17 16 16 15 15 15 14 14 14 14 13 7 747 21 21 20 20 19 19 18 18 17 17 17 16 16 16 15 15 15 14 14 14 13 13 7 646 21 20 20 19 19 18 18 18 17 17 16 16 16 15 15 15 14 14 14 13 13 13 7 345 21 20 19 19 18 18 18 17 17 16 16 16 15 15 15 14 14 14 13 13 13 12 7 144 20 20 19 19 18 18 17 17 16 16 16 15 15 15 14 14 14 13 13 13 12 12 6 1343 20 19 19 18 18 17 17 16 16 16 15 15 15 14 14 14 13 13 13 12 12 12 6 1142 19 19 18 18 17 17 16 16 16 15 15 15 14 14 14 13 13 13 12 12 12 12 6 841 19 18 18 17 17 16 16 16 15 15 15 14 14 14 13 13 13 12 12 12 12 11 6 640 18 18 17 17 16 16 16 15 15 15 14 14 14 13 13 13 12 12 12 12 11 11 6 439 18 17 17 16 16 16 15 15 15 14 14 13 13 13 13 12 12 12 12 11 11 11 6 138 17 17 16 16 16 15 15 14 14 14 13 13 13 13 12 12 12 11 11 11 11 11 637 17 16 16 16 15 15 14 14 14 13 13 13 13 12 12 12 11 11 11 11 10 10 5 1136 16 16 16 15 15 14 14 14 13 13 13 12 12 12 12 11 11 11 11 10 10 10 5 935 16 16 15 15 14 14 14 13 13 13 12 12 12 12 11 11 11 11 10 10 10 10 5 734 16 15 15 14 14 14 13 13 13 12 12 12 11 11 11 11 10 10 10 10 10 9 5 5
1.48 1.50 1.52 1.54 1.56 1.58 1.60 1.62 1.64 1.66 1.68 1.70 1.72 1.74 1.76 1.78 1.80 1.82 1.84 1.86 1.88 1.90
4’101/2 4’11 5’0 5’01/2 5’11/2 5’2 5’3 5’4 5’41/2 5’51/2 5’6 5’7 5’71/2 5’81/2 5’91/2 5’10 5’11 5’111/2 6’01/2 6’1 6’2 6’3
Score 0
(obese)
Score 0
Score 1
Score 2
Height (m)
Weight (stones and pounds)
Wei
ght
(kg)

Chapter 7 Nutritional assessments
56
Table 7Weight loss score This chart shows the weight loss scores to be used in the Malnutrition Universal Screening Tool (MUST).2
Reproduced with permission of the British Association of Parenteral and Enteral Nutrition (BAPEN).
34 kg36 kg38 kg40 kg42 kg44 kg46 kg48 kg50 kg52 kg54 kg56 kg58 kg60 kg62 kg64 kg66 kg68 kg70 kg72 kg74 kg76 kg78 kg80 kg82 kg84 kg86 kg88 kg90 kg92 kg94 kg96 kg98 kg
100 kg102 kg104 kg106 kg108 kg110 kg112 kg114 kg116 kg118 kg120 kg122 kg124 kg126 kg
Score 0Wt Loss <5%
<1.70<1.80<1.90<2.00<2.10<2.20<2.30<2.40<2.50<2.60<2.70<2.80<2.90<3.00<3.10<3.20<3.30<3.40<3.50<3.60<3.70<3.80<3.90<4.00<4.10<4.20<4.30<4.40<4.50<4.60<4.70<4.80<4.90<5.00<5.10<5.20<5.30<5.40<5.50<5.60<5.70<5.80<5.90<6.00<6.10<6.20<6.30
Score 1Wt Loss 5-10%
1.70 – 3.401.80 – 3.601.90 – 3.802.00 – 4.002.10 – 4.202.20 – 4.402.30 – 4.602.40 – 4.802.50 – 5.002.60 – 5.202.70 – 5.402.80 – 5.602.90 – 5.803.00 – 6.003.10 – 6.203.20 – 6.403.30 – 6.603.40 – 6.803.50 – 7.003.60 – 7.203.70 – 7.403.80 – 7.603.90 – 7.804.00 – 8.004.10 – 8.204.20 – 8.404.30 – 8.604.40 – 8.804.50 – 9.004.60 – 9.204.70 – 9.404.80 – 9.604.90 – 9.805.00 – 10.005.10 – 10.205.20 – 10.405.30 – 10.605.40 – 10.805.50 – 11.005.60 – 11.205.70 – 11.405.80 – 11.605.90 – 11.806.00 – 12.006.10 – 12.206.20 – 12.406.30 – 12.60
Score 2Wt Loss >10%
>3.40>3.60>3.80>4.00>4.20>4.40>4.60>4.80>5.00>5.20>5.40>5.60>5.80>6.00>6.20>6.40>6.60>6.80>7.00>7.20>7.40>7.60>7.80>8.00>8.20>8.40>8.60>8.80>9.00>9.20>9.40>9.60>9.80>10.00>10.20>10.40>10.60>10.80>11.00>11.20>11.40>11.60>11.80>12.00>12.20>12.40>12.60
5st 4lb5st 7lb5st 11lb6st 6st 4lb6st 7lb6st 11lb7st7st 4lb7st 7lb7st 11lb8st8st 4lb8st 7lb8st 11lb9st9st 4lb9st 7lb9st 11lb10st10st 4lb10st 7lb10st 11lb11st11st 4lb11st 7lb11st 11lb12st12st 4lb12st 7lb12st 11lb13st13st 4lb13st 7lb13st 11lb14st14st 4lb14st 7lb14st 11lb15st15st 4lb15st 7lb15st 11lb16st16st 4lb16st 7lb
Score 0Wt Loss <5%
<4lb<4lb<4lb<4lb<4lb<5lb<5lb<5lb<5lb<5lb<5lb<6lb<6lb<6lb<6lb<6lb<7lb<7lb<7lb<7lb<7lb<7lb<8lb<8lb<8lb<8lb<8lb<8lb<9lb<9lb<9lb<9lb<9lb<9lb
<10lb<10lb<10lb<10lb<10lb<11lb<11lb<11lb<11lb<11lb<11lb<12lb
Score 1Wt Loss 5-10%
4lb – 7lb4lb – 8lb4lb – 8lb4lb – 8lb4lb – 9lb5lb – 9lb5lb – 10lb5lb – 10lb5lb – 10lb5lb – 11lb5lb – 11lb6lb – 11lb6lb – 12lb6lb – 12lb6lb – 12lb6lb – 13lb7lb – 13lb7lb – 13lb7lb – 1st 0lb7lb – 1st 0lb7lb – 1st 0lb7lb – 1st 1lb8lb – 1st 1lb8lb – 1st 1lb8lb – 1st 2lb8lb – 1st 2lb8lb – 1st 3lb8lb – 1st 3lb9lb – 1st 3lb9lb – 1st 4lb9lb – 1st 4lb9lb – 1st 4lb9lb – 1st 5lb9lb – 1st 5lb10lb – 1st 5lb10lb – 1st 6lb10lb – 1st 6lb10lb – 1st 6lb10lb – 1st 7lb11lb – 1st 7lb11lb – 1st 7lb11lb – 1st 8lb11lb – 1st 8lb11lb – 1st 8lb11lb – 1st 9lb12lb – 1st 9lb
Score 2Wt Loss >10%
>7lb>8lb>8lb>8lb>9lb>9lb>10lb>10lb>10lb>11lb>11lb>11lb>12lb>12lb>12lb>13lb>13lb>13lb>1st 0lb>1st 0lb>1st 0lb>1st 1lb>1st 1lb>1st 1lb>1st 2lb>1st 2lb>1st 3lb>1st 3lb>1st 3lb>1st 4lb>1st 4lb>1st 4lb>1st 5lb>1st 5lb>1st 5lb>1st 6lb>1st 6lb>1st 6lb>1st 7lb>1st 7lb>1st 7lb>1st 8lb>1st 8lb>1st 8lb>1st 9lb>1st 9lb
Weight before weight loss (kg) Weight before weight loss (st lb)

Chapter 7 Nutritional assessments
57
Assessing new residentsMany older people are alreadysuffering from malnutrition whenthey enter residential careaccommodation. It is thereforeimportant to carry out an assessmentof all new residents and to make surethat they are eating and drinking wellin their first weeks.
The Care Homes for Older PeopleNational Minimum Standards (seeAppendix 2) requires a full needsassessment on admission whichincludes details of the weight, dietand dietary preferences and oralhealth of each individual. Anyunexplained swallowing disorder orother eating problems should beassessed by an appropriate healthadvisor such as a speech andlanguage therapist, doctor or dentist.
In the early days in the home thereshould be regular checks to look atthe resident’s food and beveragelikes and dislikes, food and drinkwastage and access to secondhelpings. Extra time should beallowed for slow eaters. Newresidents may be depressed anduninterested, and helping friendshipsto develop can bring improvementsin eating and drinking.
Residential and nursing care staff andcare management staff should alsowatch out for the following warningsignals:
• changes in eating habits, forexample whether a person iseating or drinking more or lessthan usual
• food or drinks left over atmealtimes and at between-mealsnacks
• loss of independence in eating
• difficulties with swallowing
• visible signs, for example loose ortight clothing which can be a signof weight loss or gain
• verbal signals, for example if anolder person says “I’ve got noenergy” or “I just can’t get round todoing things.”
Assessing nutritionalstatus among olderpeople in the communityAppendix 5 outlines two samplenutritional assessment methodswhich have been developed for usein the community to identify olderpeople who may be at nutritionalrisk. They look more specifically atfactors related to changes in food anddrink consumption and relate theseto other lifestyle risk factors whichare known to contribute tomalnutrition.
The Single Assessment Process (SAP)for older people in the community,introduced in the National ServiceFramework for Older People,4 cameinto force in 2004. Its purpose is toensure that older people receiveappropriate, effective and timelyresponses to their health and socialcare needs, and evaluation of foodand drink intake is part of theassessment process. Further details ofthe SAP can be found on theDepartment of Health websitewww.dh.gov.uk
Assessing foodprovisionIt is also important to assess whetherfood and drink provision forvulnerable older people is adequateand appropriate.
Better standards of food can beensured if:
• Social Services Departments rejectsuppliers or caterers who do notmeet the nutritional guidelines,food safety standards, andstandards for client acceptability(as judged by taste, smell andpresentation of food).
• The suppliers and caterers set theirown high production standards.
• The person delivering or servingthe meals reports any unfavourablereactions to the food.
• Environmental health officers visitresidential and nursing homes toensure that the food hygieneregulations are observed.
• Consumers should also commenton the acceptability of meals, butthey may have low expectations, orbe reluctant to complain.3 Inresidential care accommodation,one good way of finding out aboutresidents’ opinions is through theresidents’ committee.
• Heads of homes and inspectorsfrom the National Care StandardsCommission and the Scottish CareCommission should use theregulatory framework now in placeto encourage and support homesto fulfil the national minimumstandards for meals and mealtimes.
The checklist on the next page mayalso be useful for all those providingprepared food for older people.

Chapter 7 Nutritional assessments
58
Checklist to assess the quality of food andequipmentThis checklist can be used by those planning and providing food for olderpeople in residential care accommodation.
Photocopy the checklist and use the space on the right to note any action youcould take to make improvements.
Mealtimes
Appearance andtexture of food
Aroma
Temperature
Cultural andreligiousrequirements
Special diets
Presentation andhelp with eating
Drinks
Snacks
Second helpings
Utensils andequipment
Furniture
Room temperatureand ambience
Is everyone offered three full meals a day (one of which is cooked) at intervalsof not more than 5 hours?Is the interval between the evening snack and breakfast no more than 12hours?Are mealtimes flexible to meet the needs of all residents?Do all residents have information about the choice of meals available to them?
Does the food look attractive and appealing? Is there an interesting combination of textures, flavour and colours?Do puréed meals look attractive and appealing?
Does the food smell appetising? Do unpleasant smells interfere with eating?
Is the food served at the correct temperature even for slow eaters?
Is the food acceptable and in keeping with the cultural and religious foodrequirements of individual residents?Is food available for special occasions for all religious and cultural groups?
Are special therapeutic diets as advised by health care and dietetic staffprovided where necessary?
Are staff ready to offer assistance in eating where necessary, discreetly,sensitively and individually?Are residents encouraged to eat independently even if they find using a knifeand fork difficult?Are mealtimes unhurried, with everyone given sufficient time to eat?
Are cups filled too full, resulting in spillage by older people with a tremor? Are hot and cold drinks available at all times? Is the tea reasonably freshly brewed rather than stewed? Are people given drinks in appropriate cups or mugs?Are there small tables in the sitting room where they can put their drinks? Are milk and sugar added to taste for each resident?
Are snacks regularly available at all times and offered regularly?
Are second helpings on offer without any rush?
Are the appropriate utensils available? For example, are special utensilsprovided for people with arthritis? Is a slip mat provided where needed – eg for single-handed eaters?
Does the dining room look inviting? Are people offered the choice of sitting either in a wheelchair or an ordinarychair?
Is the temperature in the dining room at a comfortable level?Is the dining room quiet and calm?Are distractions such as radio and television kept to a minimum?
ACTION

Chapter 7 Nutritional assessments
59
Recommendations• Vulnerable older people living in the community should
have a nutritional assessment, and the results should helpinform the design of the person’s care package. Theassessment could be carried out by a member of the caremanagement team or the primary health care team.
• All older people entering residential care accommodationshould have their food and fluid needs assessed in thefirst week after admission, and these should be monitoredregularly thereafter.
• All residential and nursing homes should have weighingscales, preferably sitting scales, for monthly weightchecks. The scales should be checked regularly.
• The weight of each resident or patient should be recordedin the person’s care plan at least once a month.
• Care managers and service providers need to ensure thatroutine reassessments are made. All people found to be atrisk in the initial screening should be reassessed atfrequent intervals. Thereafter, reassessments will benecessary with changing circumstances.
References1 Margetts BM, Thompson RE, Elia M,
Jackson AA. 2003. Prevalence of riskof undernutrition is associated withpoor health status in older people inthe UK. European Journal of ClinicalNutrition; 57: 69-74.
2 British Association for Parenteral andEnteral Nutrition (BAPEN). 2003.Malnutrition Universal Screening Tool(MUST). Materials can be downloadedfrom the BAPEN websitewww.bapen.org.uk or can be orderedfrom BAPEN on 01527 457850.
3 Davies L. 1992. Opportunities forBetter Health in the Elderly throughMass Catering. EUR/NUT 120. WorldHealth Organization Regional OfficeEurope.
4 Department of Health. 2001. NationalService Framework for Older People.London: The Stationery Office.Available from: www.dh.gov.uk
Useful contactsAll those involved in providing foodfor older people – for examplemanager/matrons of residentialhomes and nursing homes, providersof community meals, and cateringcompanies – should have a list ofuseful local contacts, including:
• the local nutrition and dieteticservice
• community meals services,including lunch clubs
• shops offering free delivery offood, and
• where to obtain advice for each ofthe ethnic and religious groups inrelation to food.
For more information on usefulcontacts, see Appendix 6.

60
Chapter 8
Exciting theappetite
Even if the nutritional content of a meal isappropriate, it is of no value unless it is eaten. Makingthe meal look good and taste good, and encouragingthe older person to want to eat, are just as important.This chapter gives some ideas on how to do this.
Providing varietyand choiceAll those in residential careaccommodation and all those whoreceive community meals should beoffered variety and some choice offood. The right to exercise choice –particularly with regard to food – ispart of guidance and regulation forcare homes1 and is an underlyingprinciple for all aspects of care ofolder people.2 The particular likesand dislikes of all residents, orrecipients of community meals,should be ascertained, respected andmet wherever possible. This isparticularly important where theremay be ethnic, religious and culturalrequirements. Records of suchpreferences should be kept foreveryone – preferably in the kitchen.Wherever possible, residents shouldbe encouraged to contribute theirown recipes.
Timing andfrequency of mealsSince many older people have smallappetites, it is important not tooverface people with too much foodat a time, but to provide frequentopportunities for eating. Too largehelpings, apart from being wasteful,may even deter an older person fromeating at all.
It is essential to provide nutritioussnacks in between more formalmealtimes: for example, at mid-morning, mid-afternoon and a milkydrink in the late evening. Hot drinksshould be available during the night.
It is also important to allow for theproper spacing of meals. Breakfastshould be available at a timeacceptable to residents, for example7.30am - 9.00am. Suppers should be
as late as possible in the evening butearly enough to leave time for asnack before bedtime. Regulationsnow state that meals should not bespaced more than 5 hours apart andthat no more than 12 hours shouldelapse between the last food at nightand breakfast the followingmorning.1 Ensuring appropriatespacing between meals may requireresidential and nursing homes toreview care and catering staff rotasand shift patterns.
There should be proper andattractive ways of keeping the foodwarm for those who take a long timeto eat. Mealtimes must not be rushed– everyone should have enough timeto eat. Allowing enough time forpeople to eat, and offering all olderfrail people encouragement to eat,may help to correct problems ofundernutrition.3
Food presentation
In residential careaccommodation and atlunch clubsThe atmosphere created in the diningroom or lunch club, the presentationof tray meals, the way the food lookson the plate, and the attitude of thestaff may all influence whether or notthe food gets eaten.
The eating place should be culturallyappropriate, attractive, warm, well-litand with comfortable chairs. Whereappropriate, flowers, tablecloths andnapkins could be used to create apleasant environment. The ultimategoal is to provide a home from homewhere people are happy. Diningcompanions should be compatiblewherever possible. Wheelchair usersshould be transferred to dining roomchairs if they wish, unless thephysiotherapist has advised againstthis. Those who want to eat their

Chapter 8 Exciting the appetite
61
food in places other than the diningroom should be allowed to do so,but they should be encouraged tohave one meal a day in the diningroom.
People who need help from care staffto be able to eat and drink should beasked about their preferences andshould also benefit from wellpresented food. Staff should sit downand be prepared to spend time withthem. If it is essential to purée food,the different items of food should bepuréed separately and servedattractively on an appropriate dish orplate.
In residential care accommodation ithelps if the care staff both serve andclear away the food, as this providesvaluable information about the foodthat residents are not eating.
Cups and cutlery should not be tooheavy. Knives should be sharp orserrated to make it easier for cuttingmeat. Aids to encourageindependence in eating and drinkingshould be introduced discreetly.Appropriate advice about aids can befound either from a localoccupational therapy department orfrom the Disabled Living Foundation(see Appendix 6.)
In general then, the followingfeatures of food presentation willencourage older people to eat theirfood:
• ensuring that it is culturallyappropriate and similar to whatthey would eat in their own homeenvironment
• the proper and hygienic use ofcutlery and crockery
• a kindly and dignified service
• providing food that is appetising inamount, colour, freshness, tasteand smell
• arranging the food attractively onthe plate, and with appropriategarnishes
• providing appropriate drinks toaccompany the food.
Community mealsThe community meals delivered topeople at home should be in
packages which look good as well asproviding proper insulation at theright temperature. Packaging shouldbe easy to open, disposable andsuitable for transporting food. ARecommended Standard forCommunity Meals,4 published by theNational Association of Care Cateringin 2003, provides information forcaterers on the nutritional aspects ofcatering for older people anddisabled people in their own homes.
The meal should be delivered withenthusiasm and interest. The deliveryshould be part of the socialinteraction which stimulates appetite.Also, those delivering food should beencouraged to report back on anyvisible changes in the well-being ofthe client (see Chapter 7).
Social occasionsFood plays an important part insocial life and activity. It can be usedto mark welcomes and farewells,celebrations, birthdays and otherspecial days. Building on suchoccasions can help encourage eating,release memories, and stimulateconversation among older people.
In residential care accommodation,residents should be encouraged toinvite guests in either for a simplemeal or just for tea or coffee andbiscuits. The Residents Committee ina residential care home can find outwhat trips and outings residentswould enjoy. Outings, however local,which encourage some physicalactivity, exposure to sunlight andfresh air or a change of food choicecan all encourage better eating byresidents.
Physical activityOne of the most consistent findingsof all research into the nutrition ofolder people is that they eat lesswhile at the same time, and at leastpartly because, they do less.5 If olderpeople could be encouraged to bemore physically active, their energyrequirements and their appetitewould increase. Physical activity has
many other health benefits includingreduction in the risk of coronaryheart disease and stroke, theprevention or control of high bloodpressure, the prevention ofosteoporosis, improvement in jointmobility and strength, a reduction inaccidental falls, and reducing the riskof diabetes.6, 7 There is also ampleevidence of the psychological andsocial benefits of physical activity forolder people including a reduction indepression and improvements inmental alertness and sleep quality.8
Evidence suggests that current fitnesslevels among older people are low.The National Fitness Survey foundthat only a very limited number ofolder people take enough exercise to maintain their functionalindependence.9 In those aged 65-74,30% of men and 56% women hadthigh muscle strength below thatrequired to stand up from a chairunaided; and 45% of men and 79% ofwomen were not fit enough tosustain continuous walking at anormal pace. Many older people donot have the flexibility or musclestrength to perform normal everydaytasks such as hair-washing andclimbing the stairs, and women aretypically less strong than men of thesame age and more likely to haveincreased disability because of theirreduced fitness.9
It is, however, possible to reverseage-related and activity-relateddecline relatively quickly. Amongpeople over 75 years, 15 years’rejuvenation of muscle strength(27%) can be regained in threemonths through strength trainingwith one supervised class a weekand some home exercises.10 Frailolder people with multipledisabilities and illnesses can derivebenefits from regular physical activityand, among those who are immobile,regular movement of the legs andarms can help to prevent severeconstipation, swelling of the legs,pressure sores and deep veinthrombosis.11 Even previouslysedentary older people can beginexercising at an advanced age.12
High intensity resistance exercisetraining is a feasible and effective

Chapter 8 Exciting the appetite
62
way of counteracting muscleweakness and physical frailty in olderpeople.13 The development of yogadesigned especially for older peoplein a residential setting – even thechair-bound – is to be commended.14
Other exercises such as T’ai Chi andhome-based exercise programmesinvolving balance, strength andwalking exercises have also shownpositive results among olderpeople.7,15
Advice about appropriate exerciseroutines for older people may befound at the local leisure centre orfitness centre or through the localAge Concern. It is not necessary tocreate sophisticated programmes.Encouraging everyone who can, towalk to their meals, or serving coffeeand tea in another room, can providea little light and regular exercise.Fresh air is an excellent appetitestimulant.
Resources to encourage activityamong older people can be found onpage 76.
Recommendations• Older people living in residential care accommodation or
receiving community meals should be offered variety andsome choice of food.
• Records of the food preferences of each person should bekept.
• Every effort should be made to make the eatingenvironment as attractive and as culturally appropriate aspossible.
• In residential care accommodation, residents should beencouraged to invite guests in either for a simple meal, orfor tea or coffee.
• Residents should be encouraged to go on trips andoutings outside the residential care home. This maystimulate appetite by providing exercise, fresh air and achange of food choice.
• Snacks should be provided in between more formalmealtimes or, in the case of community meals, bedelivered with the main meal, thereby ensuring that, ifthey wish, older people can eat a little at a time, but morefrequently.
• Advice should be sought from an occupational therapistor speech and language therapist, for those who mayneed special aids or help with eating or drinking.
• Physical activity routines, even of a very modest nature,should be established for all older people living inresidential care accommodation.
• Staff or volunteers at lunch clubs should encouragephysical activity among older people, either by providinginformation or by organising simple activities at the club.
References1 Department of Health. 2002. Care
Homes for Older People: NationalMinimum Standards. London: TheStationery Office. Available from:www.dh.gov.uk
2 Department of Health. 2001. NationalService Framework for Older People.London: The Stationery Office.
3 Prentice AM et al. 1992. Energyexpenditure in the elderly. EuropeanJournal of Clinical Nutrition; 46 (Suppl3): S21-S28.
4 National Association of Care Catering.2003. A Recommended Standard forCommunity Meals. See:www.carecatering.org.uk.
5 Cunningham DA, Montoye HJ, MetzerHL et al. 1969. Physical activity at workand leisure as related to occupation.Medicine and Science in Sports andExercise; 1: 165-70.
6 Health Development Agency. 1999.Active for Life: Promoting PhysicalActivity with Older People. London:Health Development Agency.
7 Campbell AJ, Robertson MC, GardnerMM et al. 1997. Randomised controlledtrial of a general practice programmeof home based exercise to preventfalls in elderly women. British MedicalJournal; 315: 1065-69.
8 Fox K. 1999. The influence of physicalactivity on mental well-being. PublicHealth Nutrition; 2(3a): 411-18.
9 Skelton DA, Young A, Walker A et al.1999. Physical Activity in Later Life:Further Analysis of the Allied DunbarNational Fitness Survey and the HealthEducation Authority Survey of Activityand Health. London: Health EducationAuthority.
10 Skelton DA, McLaughlin AW. 1996.Training functional ability in old age.Physiotherapy; 82: 159-67.
11 World Health Organization. 1996. TheHeidelberg Guidelines for PromotingPhysical Activity Among OlderPersons. Geneva: World HealthOrganization.
12 Edwards KE, Larson EB. 1992. Benefitsof exercise for older adults. Clinics inGeriatric Medicine; 8: 35-50.
13 Fiatrone MA, O’Neill EF, Doyle RN etal. 1994. Exercise training andnutritional supplementation for physicalfrailty in very elderly people. NewEngland Journal of Medicine; 330:1769-75.
14 Graham M. 1988. Keep Moving, KeepYoung. Gentle Yoga Exercises for theElderly. London: Unwin.
15 Province MA, Hadley EC, HornbrookMC et al. 1995. The effects of exerciseon falls in elderly patients: a pre-planned meta-analysis of the FICSITtrials. Journal of the American MedicalAssociation; 273: 1341-47.

63
Reference1 Department of Health. 1992. The
Nutrition of Elderly People. Report onHealth and Social Subjects No. 43.Report of the Working Group on theNutrition of Elderly People of theCommittee on Medical Aspects ofFood Policy. London: HMSO.
Appendix 1Recommendations of the COMAreport on The Nutrition of ElderlyPeople
Recommendations tomaintain good nutritionalstatus in elderly people1
1 The [COMA] Working Groupendorsed the recommendationsfor people aged over 50 years inthe Government publicationDietary Reference Values forFood Energy and Nutrients forthe United Kingdom.
2 Recommendations for dietaryenergy intakes of elderly peopleshould tend to the generous,except for those who are obese.
3 Elderly people should derive theirdietary intakes from a dietcontaining a variety of nutrientdense foods.
4 An active life style, with promptresumption after episodes ofintercurrent illness, isrecommended as contributing inseveral ways to good health.
5 Steps should be taken to increasethe awareness by healthprofessionals of the importance ofboth overweight and underweightin elderly people.
6 For the majority of elderly people,the same recommendationsconcerning the dietary intake ofnon-milk extrinsic sugars apply asfor the younger adult population.
7 Intakes of non-starch-polysaccharides comparable tothose recommended for thegeneral population are advisedfor most elderly people. Foodswith high phytate content,especially raw bran, should beavoided or used sparingly.
8 The statutory fortification ofyellow fats other than butter with
vitamin A and D should continue,and manufacturers areencouraged to fortify other fatspreads voluntarily.
9 Elderly people should beencouraged to increase theirdietary intakes of vitamin C.
10 Adequate intakes of vitamin Cneed to be ensured for elderlypeople who are dependent oninstitutional catering.
11 Elderly people, in common withthose of all ages, should beadvised to eat more freshvegetables, fruit, and whole graincereals.
12 Elderly people should beencouraged to adopt diets whichmoderate their plasma cholesterollevels.
13 There should be encouragementof elderly people to consume oilyfish and to maintain physicalactivity in order to reduce the riskof thrombosis.
14 The [COMA] Working Groupendorsed the WHOrecommendation that 6g/dsodium chloride would be areasonable average intake for theelderly population in the UK, andrecommends that the presentaverage dietary salt intakes bereduced to meet this level.
15 The calcium intakes of elderlypeople in the UK should bemonitored.
16 Doorstep deliveries of milk forelderly people should bemaintained.
17 All elderly people should beencouraged to expose some skinto sunlight regularly during themonths May to September.
18 If adequate exposure to sunlightis not possible, vitamin Dsupplementation should beconsidered especially during thewinter and early spring.
19 Health professionals should bemade aware of the impact ofnutritional status on thedevelopment of and recoveryfrom illness.
20 Health professionals should beaware of the often inadequatefood intake of elderly people ininstitutions.
21 Assessment of nutritional statusshould be a routine aspect ofhistory taking and clinicalexamination when an elderlyperson is admitted to hospital.

64
Appendix 2Care Homes for Older People:National Minimum Standards
The following standards which relateto food and nutrition came into forcein 2002.1 The wording of thestandards is taken directly from thepublished document which isavailable at www.dh.gov.uk/ncsc.Explanations of terms used below(eg ‘registered person’) can be foundin that document.
These standards apply to Englandand Wales. Similar care standards forScotland are outlined atwww.scotland.gov.uk/publications.Similar standards for Northern Irelandare expected in 2005.
1 Needs assessment• New service users are admitted
only on the basis of a fullassessment undertaken by peopletrained to do so, and to which theprospective service user, his/herrepresentative (if any) and relevantprofessionals have been party.
• For individuals referred throughCare Management arrangements,the registered person obtains asummary of the Care Management(health and social services)assessment and a copy of the careplan produced for caremanagement purposes.
• For individuals who are self-funding and without a CareManagement assessment/CarePlan, the registered person carriesout a needs assessment covering:– Personal care and physical well-
being– Diet and weight, including
dietary preferences– Sight, hearing and
communication– Oral health– Foot care– Mobility and dexterity– History of falls– Continence
– Medication usage– Mental state and cognition– Social interests, hobbies,
religious and cultural needs– Personal safety and risk– Carer and family involvement
and other social contacts/relationships
2 Health care• Nutritional screening is undertaken
on admission and subsequently ona periodic basis, a recordmaintained of nutrition, includingweight gain or loss, andappropriate action taken.
• Opportunities are given forappropriate exercise and physicalactivity; appropriate interventionsare carried out for service usersidentified as at risk of falling.
• Care staff maintain the personaland oral hygiene of each serviceuser and wherever possible,support the service user’s owncapacity for self-care.
3 Meals and mealtimes• The registered person ensures that
service users receive a varied,appealing, wholesome andnutritious diet, which is suited toindividual assessed and recordedrequirements, and that meals aretaken in a congenial setting and atflexible times.
• Each service user is offered threefull meals each day (at least one ofwhich must be cooked) at intervalsof not more than five hours.
• Hot and cold drinks and snacks areavailable at all times and offeredregularly. A snack meal should beoffered in the evening and theinterval between this and breakfastthe following morning should beno more than 12 hours.
• Food, including liquefied meals, ispresented in a manner which isattractive and appealing in terms oftexture, flavour and appearance, inorder to maintain appetite andnutrition.
• Special therapeutic diets/feeds areprovided when advised by healthcare and dietetic staff, includingadequate provision of calcium andvitamin D.
• Religious or cultural dietary needsare catered for as agreed atadmission and recorded in the careplan and food for special occasionsis available.
• The registered person ensures thatthere is a menu (changedregularly) offering a choice ofmeals in written or other formats tosuit the capacities of all serviceusers, which is given, read orexplained to service users.
• The registered person ensures thatmealtimes are unhurried withservice users given sufficient timeto eat.
• Staff are ready to offer assistance ineating where necessary, discreetly,sensitively and individually, whileindependent eating is encouragedfor as long as possible.
4 Staff complement• Staffing numbers and skill mix of
qualified/unqualified staff areappropriate to the assessed needsof the service users, the size, layoutand purpose of the home, at alltimes.
• Domestic staff are employed insufficient numbers to ensure thatstandards relating to food, mealsand nutrition are fully met, and thatthe home is maintained in a cleanand hygienic state, free from dirtand unpleasant odours.
Reference1 Department of Health. 2002. Care
Homes for Older People: NationalMinimum Standards. London: TheStationery Office. Available from:www.dh.gov.uk

65
Appendix 3Good sources of nutrients
EXCELLENT
liver liver pâtépork, bacon and hamfortified breakfast cerealsmalted drinks
liverkidney
fortified breakfast cerealscanned salmon, tunapilchardschicken
most fortified breakfastcereals, eg cornflakes,branflakes, crisped riceliverspinach
blackcurrantsorange (and orange juice) strawberriescanned guavaspring greensgreen and red peppers(raw)
GOOD
wholemeal breadyeast extractoatcakescurrant bunsnutspotatoes
milkmalted drinksfortified breakfast cerealsalmonds
lean meatsausageskidneysherringssardines
yeast extractcabbagespinachBrussels sproutsbroccolipeasorangemelonkidney
broccolicabbagecauliflowerspinachtomatoBrussels sproutswatercresskiwi fruitmangograpefruit
USEFUL
lean meatchicken and other poultryeggswhite or brown breadsemi-sweet biscuits
lean meat or poultrybaconmackerel, tuna, salmonsardines, pilchardscheese yoghurteggs
wholemeal breadpeanut butteryeast extractbaconliver sausage
wholemeal bread/flourwheat biskscauliflowerbeefrunner beanstomatoesparsnippotatoesgreen leafy saladsackeepeanuts
potatoesgreen beanspeassatsumaseating applesnectarinespeachesraspberriesblackberries
B VITAMINS
Thiamin
Riboflavin
Niacin
FOLATE
VITAMIN C
This table shows a number of foods and drinks which are important sources ofcertain vitamins and minerals. These are based on average servings.
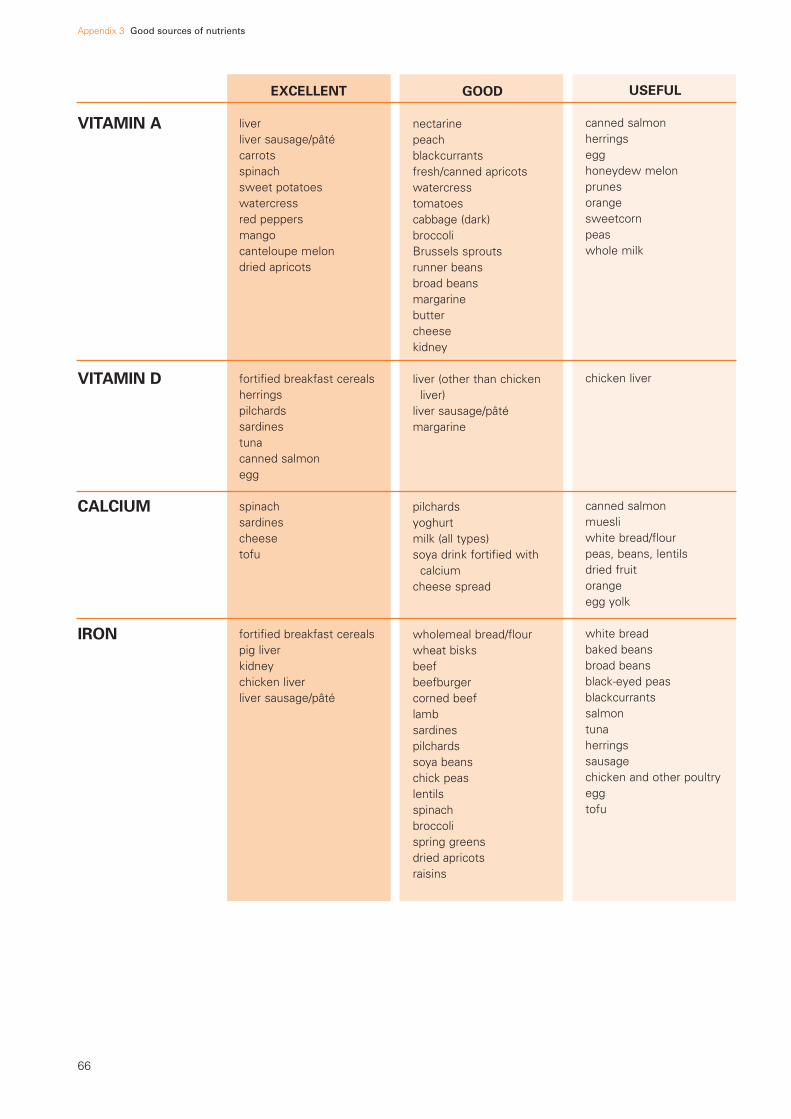
Appendix 3 Good sources of nutrients
66
EXCELLENT
liverliver sausage/pâtécarrotsspinachsweet potatoeswatercressred peppersmangocanteloupe melondried apricots
fortified breakfast cerealsherringspilchardssardinestunacanned salmonegg
spinachsardinescheesetofu
fortified breakfast cerealspig liverkidneychicken liverliver sausage/pâté
GOOD
nectarinepeachblackcurrantsfresh/canned apricotswatercresstomatoescabbage (dark)broccoliBrussels sproutsrunner beansbroad beansmargarinebuttercheese kidney
liver (other than chicken liver)
liver sausage/pâtémargarine
pilchardsyoghurtmilk (all types)soya drink fortified with
calciumcheese spread
wholemeal bread/flourwheat bisksbeefbeefburgercorned beeflambsardinespilchardssoya beanschick peaslentilsspinachbroccolispring greensdried apricotsraisins
USEFUL
canned salmonherringsegghoneydew melonprunesorangesweetcornpeaswhole milk
chicken liver
canned salmonmuesliwhite bread/flourpeas, beans, lentilsdried fruitorangeegg yolk
white breadbaked beansbroad beansblack-eyed peasblackcurrantssalmontunaherringssausagechicken and other poultryeggtofu
VITAMIN A
VITAMIN D
CALCIUM
IRON

Appendix 3 Good sources of nutrients
67
EXCELLENT
liverkidneylean meatcorned beef
whole grain / wholewheat breakfast cereals suchas bran flakes, wheatbisks, shreddies,shredded wheat, sultana bran
wholemeal breadwholemeal pitta breadbaked beanschick peas, kidney beans
(and most beans)lentilsdried apricotsdried figsdried prunes
jacket potatoeschipsroast potatoesvegetable soupdried fruit cerealsmilkbananastomato juice
GOOD
baconhampoultrycanned sardinesshrimps and prawnstofuwhole grain breakfast
cereals, eg puffed wheat, branflakes, wheat bisks
nuts
muesliwholemeal pastabrown breadwheatgerm breadrye breadwhite bread with added
fibrebaked potato with skinchipssweet potatobroad beansfresh and frozen peassweetcornbroccoliBrussels sproutsokraquornavocadoblackberriesdried datesalmondshazelnutspeanutstwiglets
parsnipsmelonorange juicedried fruitcoffeeBrussels sproutstomatoesmeatbaconsausagesfish
USEFUL
sausagescold cooked meatscanned tuna or pilchardseggsmilkcheesebeans and lentilsbrown or wholemeal
breadplain popcornsesame seeds
puffed wheat cerealbrown ricewhite pitta breadpizzapotatoesyamhoumouscanned peascabbagecarrotsplantainbananamangoraisinssunflower seedspotato crisps
fresh fruitcanned fruitfresh vegetablescanned vegetablesbread
ZINC
FIBRE(non-starchpolysaccharides –NSP)
POTASSIUM

Appendix 3 Good sources of nutrients
68
VERY HIGH
canned and packet soupsbacon and hamsalted savoury snackssmoked sausage,
smoked cheese or smoked fish
sauces and condiments some ready prepared
dishes (Check the label:dishes which containmore than 0.5g sodiumper 100g, or more than1g sodium per portion,are high in sodium.)
Some breakfast cereals are high in sodium: lookfor lower sodiumalternatives.
MODERATELY HIGH
breadcheesefishmarmitemilk
LOW
fresh and frozen meatfresh and frozen chickenfresh fruit, canned fruit,
dried fruitfresh and frozen
vegetablesfruit juicesshredded wheat, puffed
wheattea, coffee
SODIUM

69
Appendix 4Portion guide
The table below is only a guide. Individual needs must beconsidered when deciding on appropriate portion sizes.
(C) = cooked (R) = raw (L) = ladle
‘Breakfast foods’grapefruit segments 4oz 120gporridge 5oz (L) 150gfruit juice 100mlcereal 1oz 30gprunes 3oz (5 prunes) 90gbutter 1/2 oz 15gbread 11/2 oz 45gjam/marmalade 2/3 oz 20gbacon (middle/back) 3oz (R) 90gblack pudding 3oz (R) 90gscrambled egg 2 eggspoached egg 1 egg
Milk 1 pt 600 ml
Meat/fish/eggsroast meat 4oz (R) 3oz (C) 120g (R) 90g (C)chop 4oz (R) 3oz (C) 120g (R) 90g (C)braised steak 4oz (R) 3oz (C) 120g (R) 90g (C)liver 4oz (R) 3oz (C) 120g (R) 90g (C)casseroled meat(eg chicken) 4oz (R) 3oz (C) 120g (R) 90g (C)tripe 3oz (R) 90gomelette 2 eggsbreaded fish 4-5oz (R) 120-150g (R)poached fish 4-5oz (R) 120-150g (R)cold meats for salads 3oz (C) 90g (C)
Vegetablesbaked beans 2.5oz (C) 80gbroccoli 2.5oz (C) 80gcabbage 2.5oz (C) 80gcanned tomatoes 2.5oz (R) 80gcarrots 2.5oz (C) 80ggreen beans 2.5oz (C) 80g
Potatoes and other starchy foodscreamed potatoes 3oz(C) 90gboiled potatoes 3oz(C) 90groast potatoes 3oz(C) 90gchipped potatoes 4oz(C) 120gsauté potatoes 4oz(C) 120gduchesse potatoes 4oz(C) 120grice 4oz (C) 120gspaghetti/pasta 6oz (C) 160g
Sweetsmilk pudding 4oz (L) 120gsponge 3oz 90gjelly 4oz 120gtart 3-4oz 90-120gtrifle 4oz 120gstewed fruit 3oz 90gcustard sauce 3oz 90gcrumble 3-4oz 90-120gcanned fruit 3oz 90gice cream 2 scoops 60gapple/pear/orange 4oz 120gbanana 3oz 90g
Cheese and biscuits 1oz cheese 30g cheese+ 3 biscuits + 3 biscuits
Sandwichescheese 11/2 oz 45gmeat 1oz (C) 30gfish 11/2 oz 45g
Cakes and biscuits1 digestive biscuit 1/2 oz 15gtea cake 2oz 60gfruit scone 2oz 60gjam sponge 11/2 -2oz 45-60gshortbread 1oz 30gmadeira cake 2oz 60g

70
Appendix 5Sample nutritional assessmentmethods for use in the community
This Appendix gives some sampleassessment methods for identifyingolder people living in the communitywho might be at risk of malnutrition:
• the Assessment Grid, and
• the Nutrition Assessment Checklist.
See also The MUST tool on page 52.
Assessment gridThe Assessment Grid on the nextpage can be used by those mostfrequently in touch with the olderperson living in the community: forexample, relatives, neighbours,friends, home care workers ormedical practitioners. Theseprofessionals and lay people mightbenefit from some training bydietitians on how to makeobservations and when to make areferral or take other appropriatesteps.
The Assessment Grid helps to identifyknown risk factors – circumstancesthat increase the risk of malnutritionamong older people living in thecommunity.1 These should beevaluated in the light of anyobserved warning signals –circumstances which, if leftunchecked, might cause an ‘at risk’person to become malnourished. Themain warning signals related to eachrisk factor are marked by blankcircles in the grid.
To use the grid, first tick the riskfactor(s) that apply to the individual(for example, ‘housebound’, ‘noregular cooked meals’ etc). Olderpeople with four or more risk factorsare at considerable risk ofmalnutrition. If you are worried that adiagnosed medical condition may beaffecting the patient’s nutritionalstatus, check all the warning signalslisted on the grid and report your
observations to the medicalpractitioner.
Having a risk factor does notnecessarily mean that an olderperson is suffering from malnutrition.For example, being housebound is arisk factor, but this does not meanthat all housebound people aremalnourished. However, olderpeople who are housebound andshow signs of any of the warningsignals which are marked with ablank circle in the ‘housebound’column (eg ‘recent unintendedweight change ...’ or ‘physicaldisability affecting food shopping...’), are more likely to bemalnourished. If the person is alsoliving alone, or has any other riskfactor, the blank circles in thosecolumns also need to be observed.For more details on how to use thisgrid, see the journal article Warningsignals for malnutrition in theelderly.2
An adequate income is no guaranteethat an older person is wellnourished. Bereavement, mentalconfusion, physical disability andpoor nutritional knowledge canaffect both rich and poor alike, andeach of these is a warning signal.
Warning signals are interrelated andcumulative, so each one needs to beevaluated in relation to the others.For example, ‘food wastage/rejection’may just be a sign of an over-large orunpopular meal, but if there is alsodepression, lack of sunlight andinsufficient food stores at home,there may be good reason toundertake a more detailedassessment so that appropriate actioncan be taken.
Taking action
• If the older person has had a recent
unintended gain or loss of 3kg(7lb) or more, he/she should bereferred for a medical assessment,and a management plan put inplace.
• Consider what immediate, practicalthings could be done to preventnutritional problems fromdeveloping. These can be simpleand inexpensive, and will dependon the needs and wishes of theindividual: for example, help withshopping and preparing food, anoccasional accompanied visit to theshops, transport to lunch clubs orday centres, or contacting a localcommunity meals service. Or itcould be action not directly food-related: for example help with awalking aid, or specialised kitchengadgets to help a disabled personbecome more independent, orbereavement counselling.
This community-based approachdoes not disregard the morestructured care of the social andhealth services. It is simply a way inwhich lay people, and professionals,can pass on their observations tothose who can assess the need foraction, and implement it.

Appendix 5 Sample nutritional assessment methods for use in the community
71
Based on a grid produced in: Davies L, Knutson KC. 1991. Warning signals for malnutrition in the elderly. Journal of the American Dietetic Association; 91 (11): 1413-1417.
Recent unintended weight change + or - 3kg (7lb)
Physical disability affecting food shopping, preparation or intake
Lack of sunlight
Bereavement and/or observed depression/loneliness
Mental confusion affecting eating
High alcohol consumption
Polypharmacy/long-term medication
Missed meals/snacks/fluids
Food wastage/rejection
Insufficient food stores at home
Lack of fruit/juices/vegetables
Low budget for food
Poor nutritional knowledge
livin
g al
one
hous
ebou
nd
no r
egul
ar c
ooke
d m
eals
low
men
tal t
est
scor
e
clin
ical
dia
gnos
is o
f de
pres
sion
chro
nic
bron
chiti
s/em
phys
ema
gast
rect
omy
poor
den
titio
n an
d/or
diff
icul
ty in
sw
allo
win
g
RIS
KFA
CTO
RS
NAME
ADDRESS
DATE
Relevant risk factors and observed warning signals
WARNING SIGNALS
Assessment grid

Appendix 5 Sample nutritional assessment methods for use in the community
72
NutritionAssessmentChecklistThe Nutrition Assessment Checklistopposite was developed by stateregistered dietitians to help communitycare workers (health and socialservices) to recognise nutrition-relatedproblems among older people living inthe community. It is a simple screeningtool to identify possible nutrientdeficiencies.
It is important to ask the five ‘Generalquestions’ first. The answers to thesequestions will influence subsequentadvice and action. For example, if theclient has had unintended weight lossor gain you would want to ensure thatthe person has been referred to adoctor for further investigation inparallel to whatever other advice wasgiven.
Next ask the questions in sections 1-4.Circle the score for each answer. Iftwice as much is eaten, double thescore for that question. Add up thescore for each section. If the personhas a score of under 10 in any section,he/she is at risk of developing, or mayhave already developed, a deficiencyin that nutrient.
Taking action
Practical suggestions on how tocounteract deficiencies, and whichfoods can help, are given in theguidance notes3 which are availablefrom NAGE (see page 75). See alsoChapter 4 of this report. For furtherinformation and specific advice,contact your local Nutrition andDietetic Department (in the telephonedirectory under the name of yourprimary care trust).
General questions
Nutrition Assessment Checklist
1 Do you usually eat
Breakfast yes no
Mid-day lunch/dinner yes no
Tea/evening meal yes no
2 Have you lost or gained much weight (more than 1 stone) inthe last year, without trying to?
Gained weight yes no
Lost weight yes no
3 Are you on a special diet? (eg diabetic, high fibre, reducing)
yes no Type
4 Are you taking any food/drink supplements? (eg Complan, Bengers, Build Up)
yes no If yes, what?
5 Are you taking any laxatives, vitamin supplements, cod liver oil, iron tablets etc?
yes no If yes, what?
Please consider the answers to questions 1 to 5 when using the checklistas they will influence your advice and action.
NAME
ADDRESS
COMPLETED BY
DATE
Guidance notes on how to usethis Nutrition AssessmentChecklist are available fromNAGE (address on page 75).
References1 DHSS. 1979. Nutrition and Health in Old
Age. Report on Health and SocialSubjects No 16. London: HMSO.
2 Davies L, Knutson KC. 1991. Warningsignals for malnutrition in the elderly.Journal of the American DieteticAssociation; 91 (11): 1413-17.
3 NAGE: The Nutrition AssessmentChecklist: Guidance Notes and Advice.Birmingham: NAGE (see page 75 forcontact details).

Appendix 5 Sample nutritional assessment methods for use in the community
73
How often do you eat ... Weekly Alternate days DailyCitrus fruit, eg oranges 2 5 10Soft fruit, eg strawberries, blackcurrants (not tinned) 2 5 10Grapefruit/orange/tomato juice (not tinned) 1 3 6Vitamin C enriched cordial, eg blackcurrant 1 3 6Potatoes, including instant 1 3 6Green veg/tomato/salad 1 2 3Banana/tinned mandarins 1 2 3
Total
Total
Total
Total
Section 1 Vitamin C
How often do you eat ... Weekly Alternate days DailyHalf a pint of milk (drinks/cereal) 1 3 6Sardines/pilchards 2 4 8Cheese (1oz) 1 2 4Yoghurt/ice-cream 1 2 3Milk pudding/custard/evaporated milk 1 2 3
Section 2 Calcium/vitamin D
How often do you eat ... Weekly Alternate days DailyWholegrain breakfast cereals 3 4 5Wholemeal bread/roll (3 slices) 2 3 4Wholegrain biscuits/crackers/crispbread (3-6) 1 2 3Pulses including baked beans 1 2 3Fruit 0 1 2Vegetables/salad 0 1 2White bread 0 0 1Chapati/rice/pasta 0 0 1
Section 3 Fibre
How often do you eat ... Weekly Alternate days DailyBlack pudding 4 10 20Liver, kidney, heart 3 6 12Liver pâté/sausage/faggots 2 4 8Red meat, corned beef 2 4 8Egg 1 2 4Breakfast cereal 1 2 4Wholemeal bread – 3 slices 0 1 3Dark green vegetables 0 1 3Pulses, eg lentils 0 1 3
Section 4 Iron
NOTE: As you ask the questions in Sections 1-4, circle the score for eachanswer. If twice as much is eaten, double the score and if eaten less oftenthan once a week or never, score zero (0). If the score is under 10 in anysection please consult the relevant information in the guidance notes.3
It is important to drink at least 8 cups of fluid a day.

74
Appendix 6Useful addresses andfurther reading
Citizens Advice BureauxMyddelton House115-123 Pentonville RoadLondon N1 9LZPhone: 0207 833 2181www.citizensadvice.org.uk
Counsel and CareTwyman House16 Bonny StreetLondon NW1 9PGPhone: 020 7241 8555Advice line: 0845 300 7585 (Callscharged at local rate.)Email: [email protected]
Diabetes UK10 ParkwayLondon NW1 7AAPhone: 020 7424 1000Helpline: 020 7424 1030Email: [email protected]
DIAL UK (Disability Information andAdvice Line services)St Catherine’s Tickhill RoadDoncaster DN4 8QNPhone: 01302 310 123Email: [email protected]
Disability WalesWernddu CourtCaerphilly Business ParkVan RoadCaerphilly CF83 3EDPhone: 029 2088 7325Email: [email protected]
Disabled Living Foundation380-384 Harrow RoadLondon W9 2HUPhone: 020 7289 6111Helpline: 0845 130 9177 (Calls chargedat local rate.)Email: [email protected]
Help the Aged England207-221 Pentonville RoadLondon N1 9UZPhone: 020 7278 1114Email: [email protected]
Help the Aged Northern IrelandAscot House24-30 Shaftesbury SquareBelfast BT2 7DBPhone: 02890 230 666Email: [email protected]
Useful addressesAge ConcernAge Concern EnglandAstral House1268 London RoadLondon SW16 4ERPhone: 020 8765 7200Email: [email protected]
Age Concern Cymru (Wales)1 Cathedral RoadCardiff CF11 9SDPhone: 029 2037 1566Email: [email protected]
Age Concern Northern Ireland3 Lower CrescentBelfast BT7 1NRPhone: 02890 245729Email: [email protected]
Age Concern Scotland113 Rose StreetEdinburgh EH2 3DTPhone: 0131 220 3345Email: [email protected]
Alcohol ConcernWaterbridge House32-36 Loman StreetLondon SE1 0EEPhone: 020 7928 7377 Email:[email protected]
Alzheimer Scotland – Action onDementia22 Drumsheugh GardensEdinburgh EH3 7RNPhone: 0131 243 1453Email: [email protected]
Alzheimer’s SocietyGordon House10 Greencoat PlaceLondon SW1P 1PHPhone: 020 7306 0606Email: [email protected]
Alzheimer’s Society Food for Thought ProjectCromwell House31 MicklegateYork YO1 6JHPhone: 01904 633640Email: [email protected]
Arthritis Care18 Stephenson WayLondon NW1 2HDPhone: 020 7380 6500Helpline: 0808 800 4050www.arthritiscare.co.uk
British Dental Health FoundationSmile House2 East Union StreetRugbyWarwickshire CV22 6AJPhone: 0870 770 4000Helpline: 0845 063 1188Email: [email protected]
British Dietetic Association5th floor, Charles House148/9 Great Charles Street QueenswayBirmingham B3 3HTPhone: 0121 200 8080Email: [email protected]
British Geriatrics SocietyMarjory Warren House31 St John’s SquareLondon EC1M 4DNPhone: 020 7608 1369Email: [email protected]
British Heart Foundation14 Fitzhardinge StreetLondon W1H 6DHPhone: 020 7935 0185Heart Information Line: 08450 70 80 70(Calls charged at local rate.)Email: [email protected]
Carers UK20/25 Glasshouse YardLondon EC1A 4JTPhone: 020 7490 8818Email: [email protected]

Appendix 6 Useful addresses and further reading
75
Help the Aged Scotland11 Granton SquareEdinburgh EH5 1HXPhone: 0131 551 6331Email: [email protected]
Help the Aged Wales12 Cathedral RoadCardiff CF11 9LJPhone: 02920 346 550Email: [email protected]
NAGE (Nutrition Advisory Group forElderly People)A group of dietitians who work witholder peoplec/o the British Dietetic Association5th floorCharles House148/9 Great Charles StreetQueenswayBirmingham B3 3HTPhone: 0121 200 8080Email: [email protected]
National Association of Care Catering45 Palace ViewBromley BR1 3EJPhone: 020 8460 4477Email: [email protected]
National Care Homes Association45/49 Leather LaneLondon EC1N 7TJPhone: 020 7831 7090Email: [email protected]
National Osteoporosis SocietyCamertonBath BA2 0PJPhone: 01761 471771 Helpline: 0845 450 0230Email: [email protected]
RADAR (Royal Association for Disabilityand Rehabilitation)12 City Forum250 City RoadLondon EC1V 8AFPhone: 020 7250 3222Email: [email protected]
Registered Nursing Home Association15 Highfield RoadEdgbastonBirmingham B15 3DUPhone: 0121 454 2511Email: [email protected]
The Relatives and Residents Association24 The Ivories6-18 Northampton StreetLondon N1 2HYPhone: 020 7359 8148Adviceline: 020 7359 8136Email: [email protected]
Royal College of Nursing20 Cavendish SquareLondon W1G 0RNPhone: 020 7409 3333Email: via websitewww.rcn.org.uk
Royal College of Speech and LanguageTherapists2 White Hart YardLondon SE1 1NXPhone: 020 7378 1200Email: [email protected]
Voluntary Organisations Involved inCaring in the Elderly Sector (VOICES)c/o the Association of Charity OfficersUnicorn HouseStation ClosePotters BarHerts EN6 3JWPhone: 01707 651777www.aco.uk.net
Women’s Royal Voluntary Service(WRVS)Garden HouseMilton HillSteventonAbingdonOxfordshire OX13 6ADPhone: 01235 442900Email: [email protected]
Further reading andresources
FOOD AND EATING
Eating Matters – A Resource forImproving Dietary Care in HospitalsPublished by the Centre for HealthServices Research, University ofNewcastle upon Tyne, 21 Claremont,Newcastle upon Tyne NE2 4AA.Phone: 0191 222 7044
Nutritional care for older peopleBy June Copeman. Published by AgeConcern, London (1999).
Eating Well for Older People withDementiaPublished by VOICES (1998).Details from the Caroline Walker Trustwebsite www.cwt.org.uk
Food, Drink and DementiaHow to help people with dementia eatwell. By Helen Crawley (2002).Available from: Dementia ServicesDevelopment Centre, University ofStirling. Phone: 01786 467740www.stir.ac.uk/dsdc
Publications by NAGE
(NAGE is the Nutrition Advisory Groupfor Elderly People of the British DieteticAssociation.)NAGEBritish Dietetic Association5th floor Charles House148/9 Great Charles Street QueenswayBirmingham B3 3HTPhone: 0121 200 8080Email: [email protected]
Eating through the 90sEating Well and Keeping Well with
Diabetes Have You Got a Small Appetite? Nutrition Assessment Checklist and
Guidance Notes Taking Steps to Tackle Eating Problems
VideosFibre Keeps You Fit Stimulating a Small AppetiteSupermarket Shopping and the Store
Cupboard
USEFUL WEBSITES
Information on food and health forolder people can be found on the

Appendix 6 Useful addresses and further reading
76
following websites:www.food.gov.ukwww.nutrition.org.uk
EXERCISE AND PHYSICALACTIVITY
Active for Later LifeBy the British Heart FoundationNational Centre for Physical Activityand Health.Published by the British HeartFoundation, London.A resource for agencies andorganisations promoting physicalactivity with older people.
Alive and Kicking – The Carer’s Guideto Exercises for Older PeopleBy J Sobczack (2001).Published by Age Concern BooksEngland.
Easy Exercises for the Older PersonBy MP File and T File (1999).Published by Springfield Books. Price£4.95.
Keep Moving, Keep Young: Gentle YogaExercises for the ElderlyBy M Graham (1988).Published by Unwin, London.
More Active, More OftenA video explaining the practicalbenefits of setting up regular chair-based movement to music sessions forolder people, and advice on how to setup the sessions. Published by Research Into Ageing,Baird House, 15-17 St Cross Street,London EC1N 8UN.Phone: 020 7404 6878
You Can Do It! – Exercises for OlderPeople By Margaret Ruddlesden.Published by Hawker Publications Ltd,13 Park House, 140 Battersea ParkRoad, London SW11 4NB.
CATERING
Catering for HealthProduced by the Food StandardsAgency and Department of Health.Available free from PO Box 369, Hayes,Middlesex UB3 1UT.Phone: 0845 6060667
Easy Cooking For One or Two andMore Easy Cooking For One or TwoBy Louise Davies.Published by Penguin Books.
Food in CareBy Diane Sandy.Published by MacMillan Press (1997).
Good Practice Guide on AfricanCaribbean foodsPublished by the Relatives andResidents Association (2002).Available from the Relatives andResidents Association (details on page75).
SUPPLIERS OF SPECIALTABLEWARE
Kapitex HealthcareKapitex House1 Sandbeck WayWetherby LS22 7GHPhone: 01937 580 211
Nottingham RehabLudlow Hill RoadWest BridgfordNottingham NG2 6HDPhone: 0115 945 2345
Smith and Nephew HomecraftSidings RoadLowmoor Road Industrial EstateKirkby in Ashfield NG17 7JZPhone: 01623 721 000
FOOD SAFETY AND HYGIENE
Food Standards Agencypublications
The publications below are availablefrom:Food Standards AgencyPO Box 359Hayes Middlesex UB3 1UTPhone: 0845 606 0667Minicom (for people with hearingdisabilities) 0845 606 0678Email: [email protected]
Food Allergy and Other UnpleasantReactions to Food PB1696
Food Safety PB0551
The Food Safety Act and You. Bookletsummarising the Food Safety Act.PB2507
Keeping Food Cool and Safe PB1649
Ten Tips for Food Safety: LeafletPB1684; Posters in A4 or A2 sizes
ADVICE AND SUPPORT FORRELATIVES
The Relatives and Residents Association24 The Ivories6-18 Northampton StreetLondon N1 2HYPhone: 020 7359 8148Adviceline: 020 7359 8136
Publications from the Relatives andResidents Association:Dental Care for Older People in HomesA Relative’s PerspectiveRelative ViewsSetting up Relatives’ Groups in Homes Good Practice Guide on African
Caribbean FoodsGood Practice Guide on Activities and
Leisure
COURSES
Eating Well for Older People
and
Eating Well for Older People withDementia
For details of these courses contact TheCaroline Walker Trust.Phone: 01726 844107
Nourishing the Elderly in ResidentialCare
For details of one-day courses onNourishing the Elderly in ResidentialCare, contact the Royal Institute ofPublic Health and Hygiene, 28 PortlandPlace, London W1N 4DE.Phone: 020 7580 2731
COMPUTER SOFTWARE
CORA Menu PlannerA computer program which cananalyse the nutritional value of aweekly menu and displays the findingson an easy-to-read bar chart. For moredetails see page 2 or visit the CarolineWalker Trust website: www.cwt.org.uk

A good diet can help reduce older people’s risk of a
wide variety of health problems including constipation
and other digestive disorders, anaemia, diabetes mellitus,
muscle and bone disorders, overweight, and coronary
heart disease and stroke. Nutrition also plays an
important part in achieving a good recovery from illness
and surgery. Adequate nutritional standards of food
prepared in residential and nursing accommodation, and
of community meals, are therefore crucial to the well-
being of older people.
This report, by an Expert Working Group convened by
The Caroline Walker Trust, sets out nutritional guidelines
both for food prepared for older people in residential
and nursing accommodation, and for community meals.
Based on current dietary recommendations, the
guidelines are intended for caterers, manager/matrons,
cooks, chefs, and residential care managers, as well as
managers of services providing meals at home.
THE CAROLINE WALKER TRUST
The Caroline Walker Trust
PO Box 61
St Austell PL26 6YL
£15 including postage and packing
ISBN 1 897820 18 6