east-escalate user workshop - cytel
TRANSCRIPT

East-Escalate User Workshop®
JSM 2015, Seattle
Hrishikesh Kulkarni, Charles Liu
Aug, 2015
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 1 / 68

Outline
1 Phase 1 Dose Finding
2 References
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 2 / 68

Phase 1 Dose Finding
Sequence of K fixed doses: d1, d2, ...dK
Each dose i has toxicity probability pi
Monotonicity assumption
Maximum Sample Size, cohort size, starting dose
Method for sequentially assigning doses to cohorts
Find MTD: highest dose with toxicity less than target pT
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 3 / 68

Dose Assignment Rules
In Phase 1 trial designs, why not assign patients equally at each dose?
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 4 / 68

Ethical Requirement
”The major difficulty in phase I trial design and conduct is the ethicalrequirement that the number of patients in the trial who experiencetoxicity must be limited.”
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 5 / 68

Phase I Trial Challenges
Under-dosing (risk of absence of any anti-tumour activity).
Over-dosing (risk of severe toxicity).
Minimize sample size (unproven agent).
Maximize information (on toxicity and PK profile).
Paoletti et al. (2006). European Journal of Cancer, 42(10), 1362–8.
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 6 / 68

Bayesian
Prior: uninformative, or published literature / experts
Likelihood: observed data
Posterior: updated evidence
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 7 / 68
Rule-based vs Model-based
Rule-based / Algorithmic (eg., 3+3) vs Model-based (CRM, BLRM)
mTPI is a mixture of both
Why model-based?
more flexible (eg., different cohort sizes)Bayesian statistical inferencesBut, more complex (need for user-friendly software!)
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 8 / 68

3+3 (Prevalence)
Over 98% of published Phase 1 trials (1991-2006) use variations of 3+3
(Rotgako et al., 2007)
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 9 / 68

3+3 (Prevalence)
Over 96% of published Phase 1 trials (2007-2008) use variations of 3+3
(LeTourneau et al., 2009)
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 10 / 68

East ESCALATE
http://www.youtube.com/watch?v=6txAE3eGOk8
Two modes: (1) Simulation; (2) Interim Monitoring
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 11 / 68

3 + 3 H (implicit pT = 1/3)
http://www.mdanderson.org/education-and-research/departments-programs-and-labs/departments-and-divisions/division-of-quantitative-sciences/lectures-and-seminars/peter-f.-thall-presentation.pdf
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 12 / 68

3 + 3 L (more common, implicit pT = 1/6)
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 13 / 68

Simulation Parameters
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 14 / 68

Response Generation Info
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 15 / 68

Create Multiple Profiles
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 16 / 68

Simulation Control Info
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 17 / 68

Output Summary
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 18 / 68

Subject-wise Dose Allocation
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 19 / 68

Dose-wise Summary
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 20 / 68

MTD Selected
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 21 / 68

Limitations of 3+3
Alessandro Matano, Novartis, http://www.smi-online.co.uk/pharmaceuticals/archive/4-2013/conference/adaptive-designs
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 22 / 68

Confidence Interval?
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 23 / 68

Target Toxicity?
Common misconception target toxicity is fixed (eg., 17%, or 33%).
He et al. (2006) showed via simulation that the expected toxicity level at theMTD for the 3+3 is between 19-22%.
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 24 / 68

Workshop Exercise (Simulation)
Adapted from Thall & Lee (2003):
”Patients with renal cell carcinoma (RCC) that was progressive after previoustreatment with interferon were eligible. Treatment consisted of fixed doses of5-FU and interferon, plus one of six doses of gemcitabine (GEM): 100, 200,300, 400, 500, or 600 mg/m2. Toxicity was defined as grade 3 or 4 diarrhea,mucositis, or hematological toxicity. A total of 36 patients were treated incohorts of size 3, with the first cohort given 200 mg/m2 of GEM.”
Enter relevant inputs into East
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 25 / 68

Response Generation Info
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 26 / 68

Simulation Control Info
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 27 / 68

Output Details
For each scenario...
1 ...which dose is selected most often (and how often) as the MTD by 3+3?
2 ...how often does 3+3 fail to select an MTD?
3 ...what are the median and mean sample sizes?
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 28 / 68

modified Toxicity Probability Interval (mTPI)
mTPI is rule-based like 3+3 but Bayesian like CRM and BLRM
Challenges for model-based methods: complexity (esp for non-statisticians);sensitivity to priors
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 29 / 68

modified Toxicity Probability Interval (mTPI)
“...almost all phase I oncology trials conducted at Merck in past 2 years havebeen based on the mTPI design”
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 30 / 68

modified Toxicity Probability Interval (mTPI)
Probability of toxicity at each dose modeled by independent Beta distributions
Set of decision intervals specified (like in BLRM)
Dosing decisions determined by ’normalized’ posterior probability in eachinterval at the current dose di :
Escalate to di+1 if di is ’underdosing’Stay at di if ’proper dosing’De-escalate to di−1 if di is ’overdosing’
Compute UPM for each interval. The one with largest UPM implies thedecision.
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 31 / 68

mTPI Priors
“[W]e believe that for phase I trials with small sample sizes...the dependenceintroduced by prior models will have a strong influence on the operatingcharacteristics...The independent prior models performs quite well comparedto existing approaches.”
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 32 / 68

Equivalence Intervals
The Equivalence Interval (EI) is defined as [pT − ε1, pT + ε2]
pT − ε1 is the lowest toxicity probability that the physician would becomfortable using to treat future patients without dose escalation
pT + ε2 is the highest toxicity probability that the physician would becomfortable using to treat future patients without dose de-escalation
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 33 / 68

Unit Probability Mass
UPM(interval) = Post Pr(interval) / length(interval)
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 34 / 68

Trial Monitoring Table (for Clinicians)
E=Escalate, S=Stay, D=De-escalate, DU=De-escalate & Unacceptable
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 35 / 68

mTPI Dose Exclusion / Stopping Rule
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 36 / 68

Regulatory Guidelines
FDA Guidance (Clinical Considerations for Therapeutic Cancer Vaccines)
EMEA / CHMP Guideline on Clinical Trials in Small Populations
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 37 / 68
Continual Reassessment Method (CRM)
Bayesian model-based method (O’Quigley et al. 1990)
Uses all available information from doses to guide assignment
Inputs to specify:
target toxicity pT (e.g., 0.3)one-parameter (θ) dose-toxicity curveprior distribution for θprior mean probabilities at each dose (“skeleton”)
Next recommended dose: posterior toxicity probability closest to target
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 38 / 68

Modified CRM
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 39 / 68

Modified CRM
Differences:
Can start at lowest doseAllow multiple patients per cohortRestrict escalation to one dose (do not allow skipping when escalating)
“The unmodified CRM...produces only modest increases in accuracy overthe modified CRM, but at the price of greater toxicity, and, mostimportant, clinical acceptability.”
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 40 / 68

CRM Simulation Parameters
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 41 / 68

CRM Dose Toxicity Curves & Priors
Logistic: p(di ) = expc+diθ
1+expc+diθ, c fixed
Hyperbolic Tangent: p(di ) =(
tan(di )+12
)θ
Power: p(di ) = (pi )θ
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 42 / 68

CRM Stopping Rules
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 43 / 68

CRM Interim Monitoring
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 44 / 68

Bayesian Logistic Regression Model (BLRM)
Two-parameter logistic: logit(p(di )) = logα + β log(di/d∗)
d∗ is the “reference dose”: logit(p(d∗)) = logα.
The approach is recommending a range of doses instead of just one dose.
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 45 / 68

Uncertainty in toxicity rate
CRM relies on point estimate (posterior mean) , ignores uncertainty andcould be misleading.BLRM uses entire posterior distribution at each dose.eg, Two beta distributions with same posterior mean but very differentvariances. Pr(Overdosing), Pr(p > 0.6) = 0.168 vs 0.002
X-axis - probability of observing DLT
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 46 / 68

Escalation With Overdose Control (EWOC)
Choose dose that maximizes targeted toxicity probability, given notoverdosing.
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 47 / 68

Bayes Risk
Choose dose that minimizes posterior expected loss.
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 48 / 68

Prior Specification (direct vs indirect)
Enter directly bivariate normal for log(α) and log(β) OR
Enter “best guess” for p(d1) and MTD
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 49 / 68

Prior Specification (indirect)
1 Assuming logits of toxicity are linear, calculate prior probabilities of toxicity(predicted median) at each dose level
2 Assign a “minimally informative unimodal” Beta distribution at each doselevel (Neuenschwander et al., 2008 Appendix A)
3 Generate n sets of logits from Beta distributions, to obtain n estimates oflog(α) and log(β) using least squares
4 Use sample means, variance, correlation for bivariate normal
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 50 / 68

Posterior Sampling Methods
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 51 / 68

BLRM Stopping Rules
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 52 / 68

BLRM Interim Monitoring
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 53 / 68

Interval Probabilities by Dose
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 54 / 68

BLRM Final Inference
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 55 / 68

BLRM Example
First in-Human study on advanced solid tumors.Primary endpoint - frequency of DLTDoses - 1, 2 , 4, 8, 15, 30, 40.Weak Prior Informationd* set to 10BVN prior for log(α) and log(β)
means = (-0.693, 0), sd = (2, 1), corr = 0
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 56 / 68
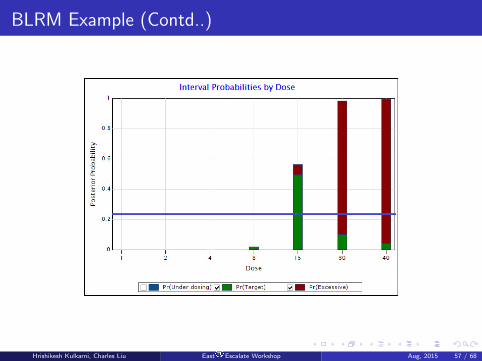
BLRM Example (Contd..)
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 57 / 68

Workshop Exercise (Interim Monitoring)
Adapted from Neuenschwander (2008):
”This study is an open-label, multicenter, non-comparative, dose-escalationcancer trial designed to characterize the safety, tolerability, andpharmacokinetic profile of a drug and to determine its MTD. The pre-defineddoses were 1, 2.5, 5, 10, 15, 20, 25, 30, 40, 50, 75, 100, 150, 200 and 250mg.”
“Currently in our trials the dose recommendation relies on maximizing theprobability of target toxicity while controlling the probability of excessive orunacceptable toxicity at 25 per cent.”
Enter relevant inputs into East
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 58 / 68

Simulation Parameters
”The best matching bivariate normal prior for the two-parameter logisticmodel had parameters µ1 = 2.15, µ2 = 0.52, σ1 = 0.84, σ2 = 0.8, ρ = 0.2”
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 59 / 68

Response Generation Info
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 60 / 68

Simulation Control Info
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 61 / 68

Simulation Stage Plots in Library
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 62 / 68

Interim Monitoring
“It was decided....not to skip dose levels during dose escalation.”
“The first cohort of patients was treated at 1 mg. No DLTs were observed forthe first four cohorts of patients, and the clinical team then decided to skiptwo dose levels...At 25 mg, two DLTs were seen in two patients. The datafrom the fifth cohort led to discussion about the dose for the next cohort.”
Enter these data into East. On the basis of information from the InterimMonitoring Dashboard, what dose would you recommend next?
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 63 / 68

Final Inference
“Eventually, the trial was continued with a dose of 20 mg, a total of ninepatients were enrolled at that dose, and two DLTs occurred. Then the trialwas stopped and 20 mg was declared as the MTD.
Enter and click “Final Inference”
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 64 / 68

Summary
Almost all trials to date have used rule-based methods
Rule-based methods (eg., 3+3) are easy to implement and simple to explain
Model-based methods (eg., CRM, BLRM) are more flexible and efficient, butperformance may depend on prior information
mTPI may be a useful compromise
East ESCALATE provides two modes:
1 Simulations for comparing and evaluating designs2 Interim Monitoring for executing designs and analyzing data
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 65 / 68

Work in Progress
Combination Designs
Enhancements
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 66 / 68

Outline
1 Phase 1 Dose Finding
2 References
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 67 / 68

References
Neuenschwander, Branson, Gsponer. Critical aspects of the Bayesian approach to phase I cancer trials.Statistics in Medicine 2008;27:2420 - 2439
Ji, Wang. Modified Toxicity Probability Interval Design: A Safer and More Reliable Method Than the 33 Design for Practical Phase I Trials. Journal of Clinical Oncology, 2013
Thall, Lee. Practical model-based dose-finding in phase I clinical trials: Methods based on toxicity. Int JGynecol Cancer 2003, 13, 251 - 261
He, Liu, Binkowitz, Quan. A model-based approach in the estimation of the maximum tolerated dose inphase I cancer clinical trials. Statistics in Medicine 2006; 25:2027 - 2042
Hrishikesh Kulkarni, Charles Liu East®Escalate Workshop Aug, 2015 68 / 68