east coast working group on diabetes in pregnancy
TRANSCRIPT

7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 1/59

7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 2/59
Screening & Diagnosis

7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 3/59

7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 4/59
ACHOIS (2005) : treating mild hyperglycemia(glucose intolerance) in pregnant women leadsto reduction in the composite endpoint of perinatal death, shoulder dystocia, bonefracture and nerve palsy

7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 5/59

7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 6/59
Landon et al (2009) : similarly demonstrated areduction in macrosomia, shoulder dystocia,cesarean delivery, and hypertensive disorderswith treatment.

7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 7/59
HAPO (2008) a prospective, blinded, multinationalobservational study
a continuous association between rising maternal glucose concentrations and large for gestational
age, pre-eclampsia, and primary cesarean section.positive association between maternal hyperglycemia and neonatal hypoglycemia, cordblood serum c-peptide, premature delivery,
intensive neonatal care, and hyperbilirubinemia

7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 8/59
1. Treatment of GDM will improve perinataloutcome (not perinatal mortality)
2. Glucose levels for diagnosis of GDM (after GTT)
are lower than previously thought.

7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 9/59
Screening methods: selective vs universalScreening protocol : timing
Classification of diagnosis
Diagnostic threshold

7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 10/59

7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 11/59
Organization Screening
ACOG (2001) American
College of Obstetricians
and Gynecologists
Risk assessment or perform universal screening at 24 –28
wks.
Low risk patients may be excluded from screening.
Screen with 50-g 1-h GCT.
Positive if 1-h > 7.2 mmol/l (130 mg/dl) or 7.8 mmol/l (140mg/dl)
Diagnose with 100-g OGTT.
SOGC (2002) Society of
Obstetricians and
Gynaecologists of Canada
Each of the following approaches is acceptable:
Routine screening at 24 –28 wks with 50-g GCT, using
threshold of 7.8 mmol/l (140 mg/dl) except in low risk
patients.Non-screening is also acceptable.
Consider the recommendations given by the Fourth
International Workshop-Conference for screening women
at high riskfor GDM early in pregnancy and again at 24 –28
wks if initial results are negative

7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 12/59
Organization Screening
5th International
Workshop-Conference
on Gestational
Diabetes Mellitus(2007)
Risk assessment should be performed at the first prenatal
visit.
Low risk women do not require any routine testing.
High risk women should undergo screening as soon aspossible (as below).
All other women should have screening at 24 –28 wks.
Screening can be done as 50-g GCT followed by diagnostic
OGTT if abnormal.
Abnormal if 1-h 7.8 mmol/l (140 mg/dl)
Or proceed directly to a diagnostic OGTT.

7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 13/59
Organization Screening
USPSTF (2008) U.S.
Preventive Services
Task Force
No recommendation made for routine screening due to
insufficient evidence.
Until there is better evidence, clinicians should discussion
screening with patients and make case-by-base decisions.
If a decision is made to screen for gestational diabetes, they
cite most screening is done between 24 and 28 wks and the50-g GCT is the most common test used in the United States
followed by the 100-g OGTT for confirmation.
NICE UK (2008) National
Institute for Health and
Clinical Excellence, UnitedKingdom
Perform risk assessment at the initial visit.
Women with any risk factors should be offered testing for
GDM.If a woman has had GDM in a prior pregnancy, she should be
offered SMBG at 16 –18 wks and repeat OGTT at 28 wks if
initial testing is normal.
Women without risk factors should be offered an OGTT at
24 –28 wks. Screen using the 75-g OGTT

7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 14/59
Organization Screening
ADA (2010) American
Diabetes Association
Risk assessment should take place at the first prenatal visit.
Do not screen low risk women.Screen high-risk women at the initial visit to identify pre-gestational
diabetes.
If negative at first visit, high risk women should be retested at
24 and 28 wks.Women of average risk should be universally screened
between 24 and 28 wks.Initial screening:
-hemoglobin A1c by NGSP-certified, standardized method, fasting
plasma glucose, 1 step 75-g OGTT with 2-h glucose level, or random
plasma glucose in a patient with classic symptoms of hyperglycemia2-step approach: Perform a 50-g glucose challenge test and if 1-h
plasma or serum glucose move on to either the 100-g OGTT or the 75-
g OGTT for diagnosis.
1-step approach: 75-g OGTT; this approach may be cost-effective in
high-risk>130 mg/dL or > 140 mg/dl, populations

7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 15/59

7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 16/59
Pregnant women should be screened if they have any of the following risk factors:
BMI >27kg/m
Previous macrosomic baby weighing 4kg or above
Previous gestational diabetes mellitus (GDM)
First-degree relative with diabetes
Bad obstetric history
Glycosuria at the first prenatal visitCurrent obstetric problems (essential hypertension,pregnancy induced hypertension, polyhydramnios andcurrent use of steroids)
Age above 25

7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 17/59
Screening is done using the 75g OGTT andperformed at least once at >24 weeks of gestation
Screening at an earlier stage of gestationdepends on the degree of suspicion and at thephysician’s/obstetrician’s request.

7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 18/59
Screen for risk
factor(s)
MGTT after 12-14 weeks or
as soon as risk identifiedRepeat test at 28-30 weeks
of gestation

7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 19/59
Screen for risk factor(s)
75 gm OGTT
At or after 28-30 weeks of
gestation
Normal
Gestational
Diabetes
mellitus
present
absent
positive
positive
negative
negative
75gm OGTT

7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 20/59
Selective vs Universal

7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 21/59
Organisation Selective Universal
ACOG (2001) American College of Obstetriciansand Gynecologists
SOGC (2002) Society of Obstetricians and
Gynaecologists of Canada
X X/
5th International Workshop-Conference
on Gestational Diabetes Mellitus (2007)
USPSTF (2008) U.S. Preventive Services
Task Force
X X
NICE UK (2008) National Institute for Health and
Clinical Excellence, United Kingdom
ADA (2010) American Diabetes Association *
CPG Management of Type 2 DM 2009
Perinatal Care Manual

7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 22/59

7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 23/59
> 7.0 mmol/l
Overt Diabetes inPregnancy
>5.1 mmol/l but
<7.0 mmol/l
75-g OGTT at 24 to28 weeks’ gestation
GestationalDiabetes
<5.1 mmol
At booking
Measure FPG, HbA1C, or random plasma glucoseon all or only women high-risk
7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 24/59
Selective screening: risk assessmentOGTT upon identification of risk factor

7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 25/59
• GDM complicates approx 7% of all pregnanciesin US (Nicholson W, 2009)
• NICE (2008) = average prevalence in Englandand Wales is approximately 3.5%

7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 26/59
Study Prevalance
Fuziah Paimin et al, 2011(unpub)
19.4%
Idris N et al, 2009 18.4%
Shamsuddin K, 2001 24.9%
Chan S, 1993 12.5%

7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 27/59
Idris N et al (2009), screening of GDM asrecommended by Malaysian CPG 2009/ADA willresult in 90% of patient being screened

7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 28/59
Screen for risk factor(s)
75 gm OGTT
At or after 24-28 weeks of
gestation
Normal
Gestational
Diabetes
mellitus
present
absent
positive
positive
negative
negative
75gm OGTT
7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 29/59
Timing

7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 30/59
OGTT should be prescribed once risk factorsidentified
If at risk
repeat GTT.

7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 31/59
Organization Screening design
ADIPS (1998) The Australasian Diabetes in
Pregnancy Society
Screen at 26 –30 wks.
WHO (1999) World Health
Organization
If high risk, screen in first trimester.
All others, screen at 24 –28 wks.
ACOG (2001) American College of
Obstetricians and Gynecologists
Risk assessment or perform universal
screening at 24 –28 wks.
SOGC (2002) Society of Obstetricians and
Gynaecologists
of Canada
Routine screening at 24 –28 wks with 50-g GCT
Japan (2002) The Committee of the Japan
Diabetes Society
Screen all at 24 –28 wks.

7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 32/59
Organization Screening design
Austrian (2004) Screen all at 24 –28 wks.
Joslin Diabetes Center (2005) Screen average-risk women at 24 –28 wks.
AACE (2007) American Association of Clinical
Endocrinologists
Screen low-risk women at 24 –28 wks.
NICE UK (2008) National Institute for Health
and Clinical Excellence,United Kingdom
Women without risk factors should be offered
an OGTT at 24 –28 wks.
ADA (2010) American Diabetes
Association
High risk women should be retested at 24 and
28 wks
Average risk should be universally screened
between 24 and 28 wks
7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 33/59

7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 34/59
Screen for risk factor(s)
75 gm OGTT
At or after 24-28 weeks of
gestation
Normal
Gestational
Diabetes
mellitus
present
absent
positive
positive
negative
negative
75gm OGTT
7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 35/59
7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 36/59
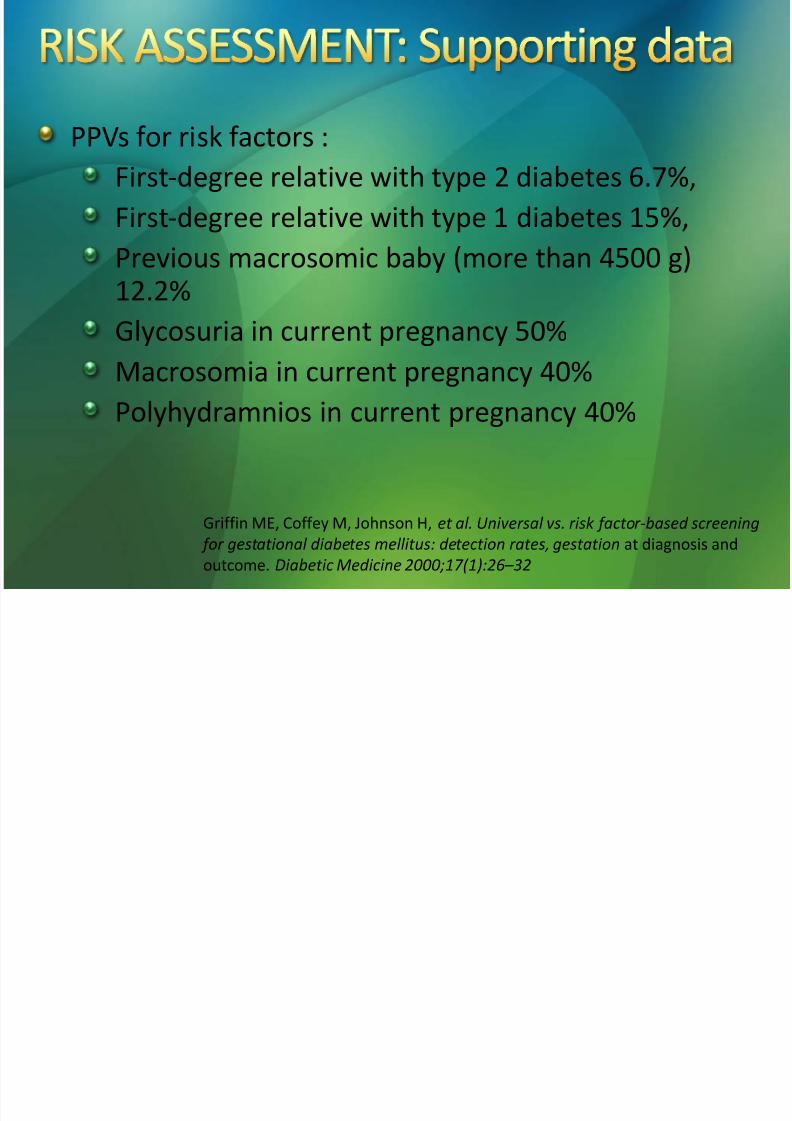
PPVs for risk factors :First-degree relative with type 2 diabetes 6.7%,
First-degree relative with type 1 diabetes 15%,
Previous macrosomic baby (more than 4500 g)
12.2%
Glycosuria in current pregnancy 50%
Macrosomia in current pregnancy 40%
Polyhydramnios in current pregnancy 40%
Griffin ME, Coffey M, Johnson H, et al. Universal vs. risk factor-based screening
for gestational diabetes mellitus: detection rates, gestation at diagnosis and
outcome. Diabetic Medicine 2000;17(1):26–
32
7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 37/59
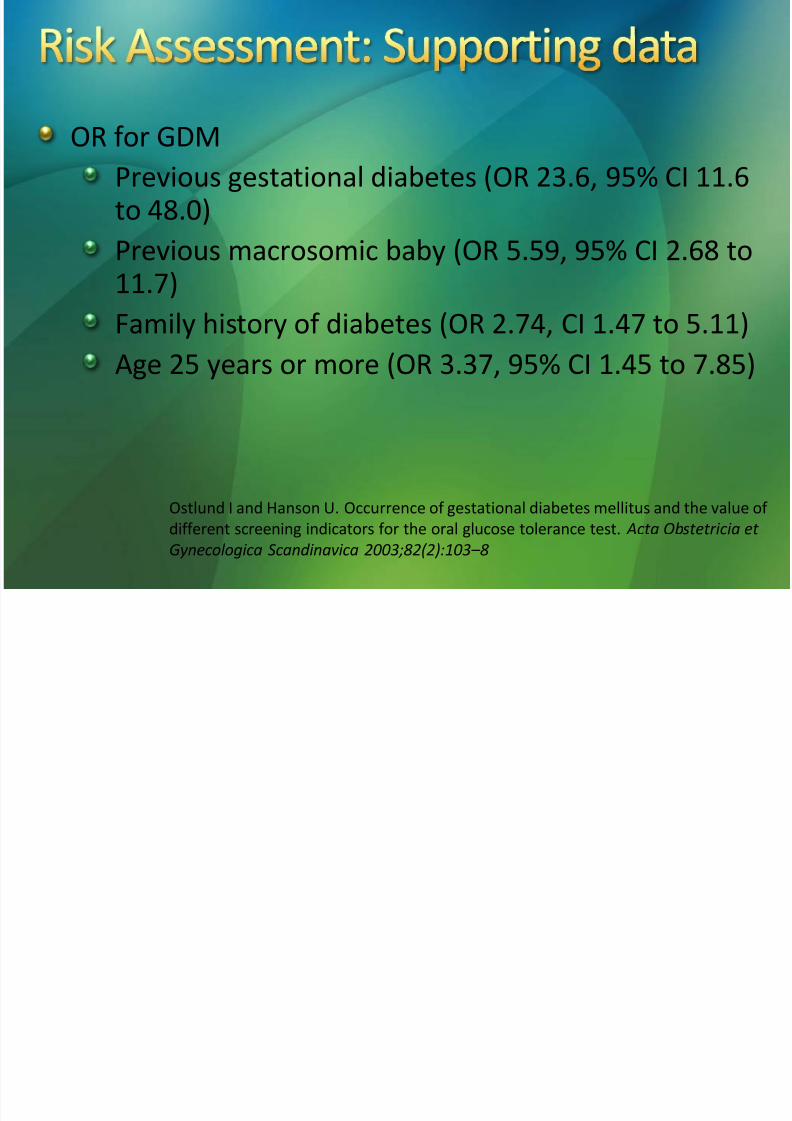
OR for GDMPrevious gestational diabetes (OR 23.6, 95% CI 11.6to 48.0)
Previous macrosomic baby (OR 5.59, 95% CI 2.68 to
11.7)Family history of diabetes (OR 2.74, CI 1.47 to 5.11)
Age 25 years or more (OR 3.37, 95% CI 1.45 to 7.85)
Ostlund I and Hanson U. Occurrence of gestational diabetes mellitus and the value of
different screening indicators for the oral glucose tolerance test. Acta Obstetricia et
Gynecologica Scandinavica 2003;82(2):103–
8
7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 38/59
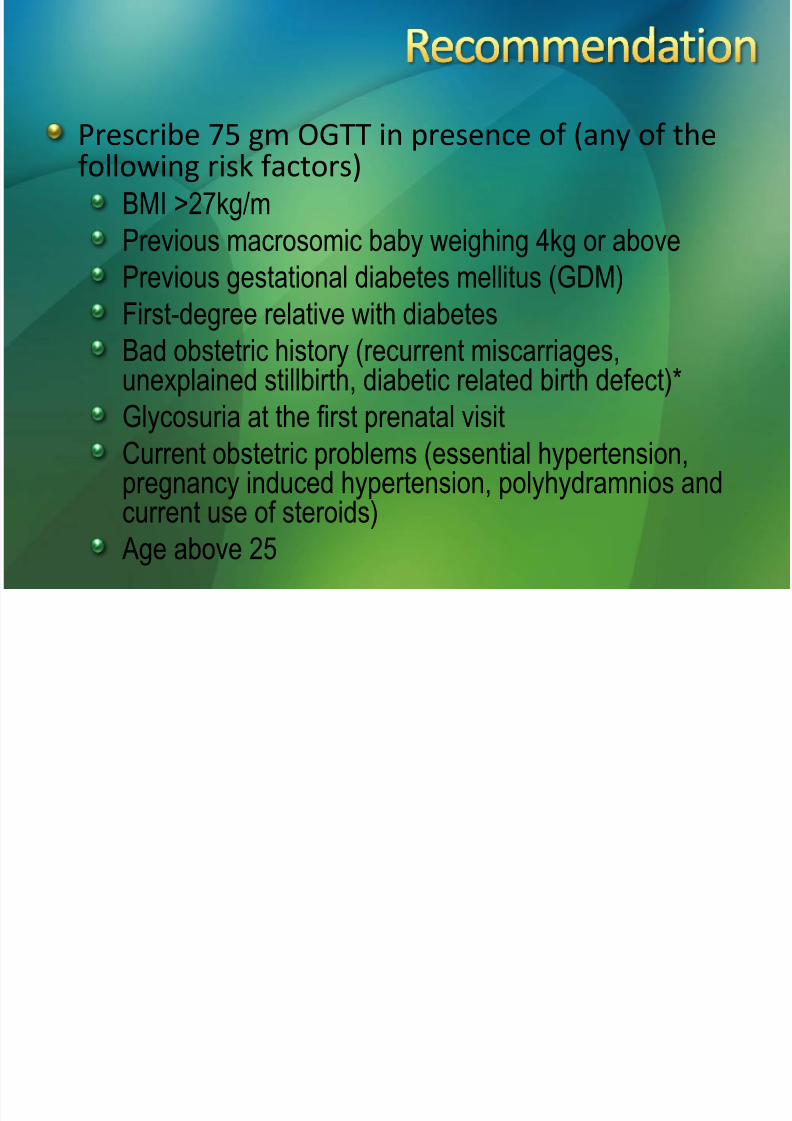
Prescribe 75 gm OGTT in presence of (any of thefollowing risk factors)
BMI >27kg/m
Previous macrosomic baby weighing 4kg or above
Previous gestational diabetes mellitus (GDM)First-degree relative with diabetes
Bad obstetric history (recurrent miscarriages,unexplained stillbirth, diabetic related birth defect)*
Glycosuria at the first prenatal visitCurrent obstetric problems (essential hypertension,pregnancy induced hypertension, polyhydramnios andcurrent use of steroids)
Age above 25
7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 39/59

7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 40/59
The International Workshop-Conferences on GDM(2007) have defined the condition as “any degreeof glucose intolerance with onset or firstrecognition during pregnancy”
While this facilites screening and diagnosis,management of undetected glucose intoleranceantedated the pregnancy might be misjudged.
7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 41/59
Current practice1. Gestational diabetes mellitus – diagnosed in
pregnancy
2. Established DM – diagnosed before pregnancy
*DM – diagnosed in pregnancy
*GDM – managed as established DM
7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 42/59
Increased risk of congenital anomalies inoffspring (Schaefer et al, 1997).
Risk of diabetes complications (nephropathyand retinopathy) requiring treatment during
pregnancy (Omori & Jovanovic, 2005).Need for rapid treatment and close follow-upduring pregnancy to ensure prompt restorationof normal glycemia (Bartha et al, 2000; Maegawa et al,
2003).Need to ensure confirmation and appropriatetreatment of diabetes after pregnancy.
7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 43/59
•Increasing prevalence of T2DM in Malaysiayounger female (in reproductive agegroup)higher risk of overt diabetes inpregnancy
• In Metabolic Study In Malaysia (May 2010) prevalence of T2DM in Malaysia (based on
OGTT) is 22.3%
7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 44/59
Classification of diabetes mellitus in pregnancy
1. Established diabetes mellitus
2. Overt diabetes in pregnancy (1st
diagnosed inpregnancy, but probably pre-pregnancy DM)
3. Gestational diabetes mellitus
7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 45/59

7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 46/59
7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 47/59
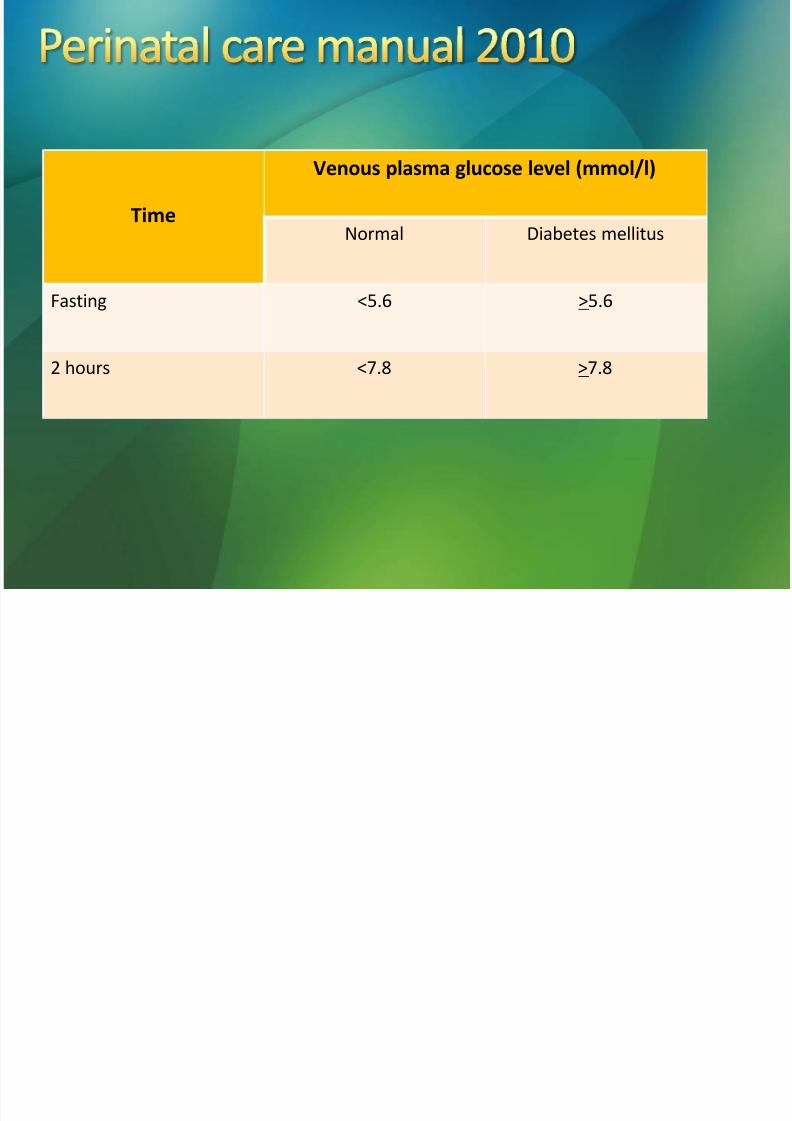
Time
Venous plasma glucose level (mmol/l)
Normal Diabetes mellitus
Fasting <5.6 >5.6
2 hours <7.8 >7.8
7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 48/59
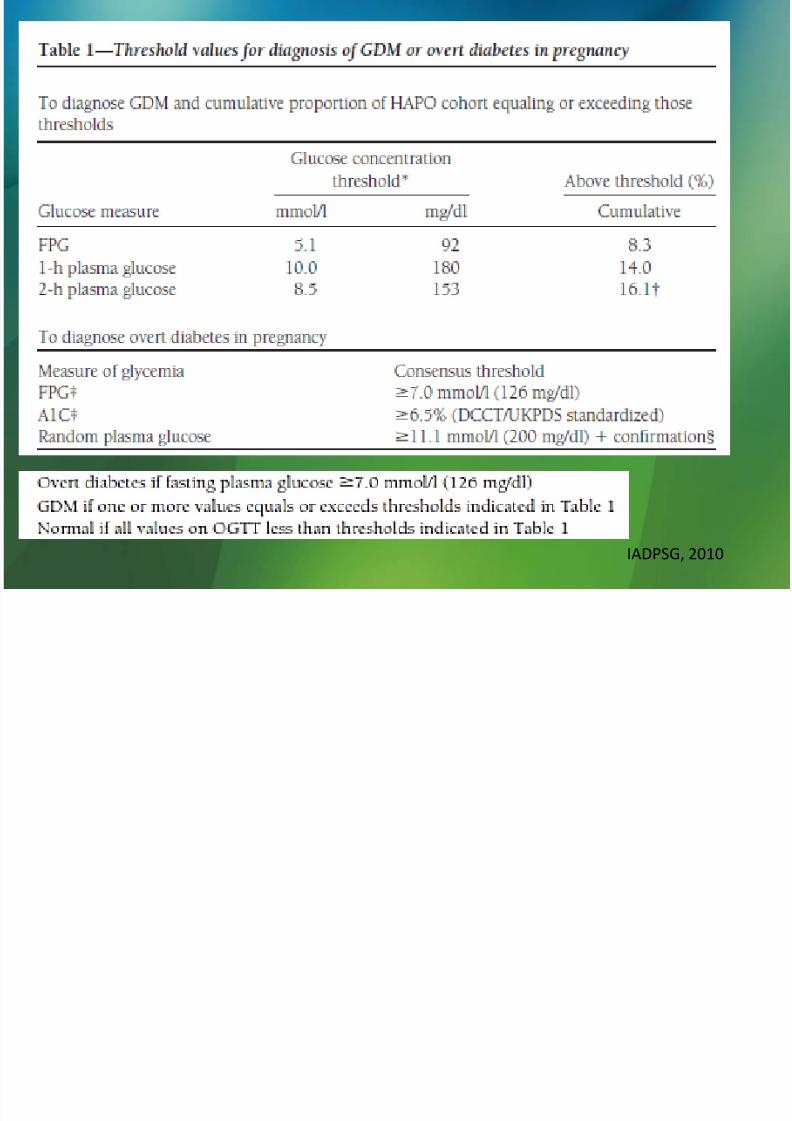
IADPSG, 2010
7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 49/59
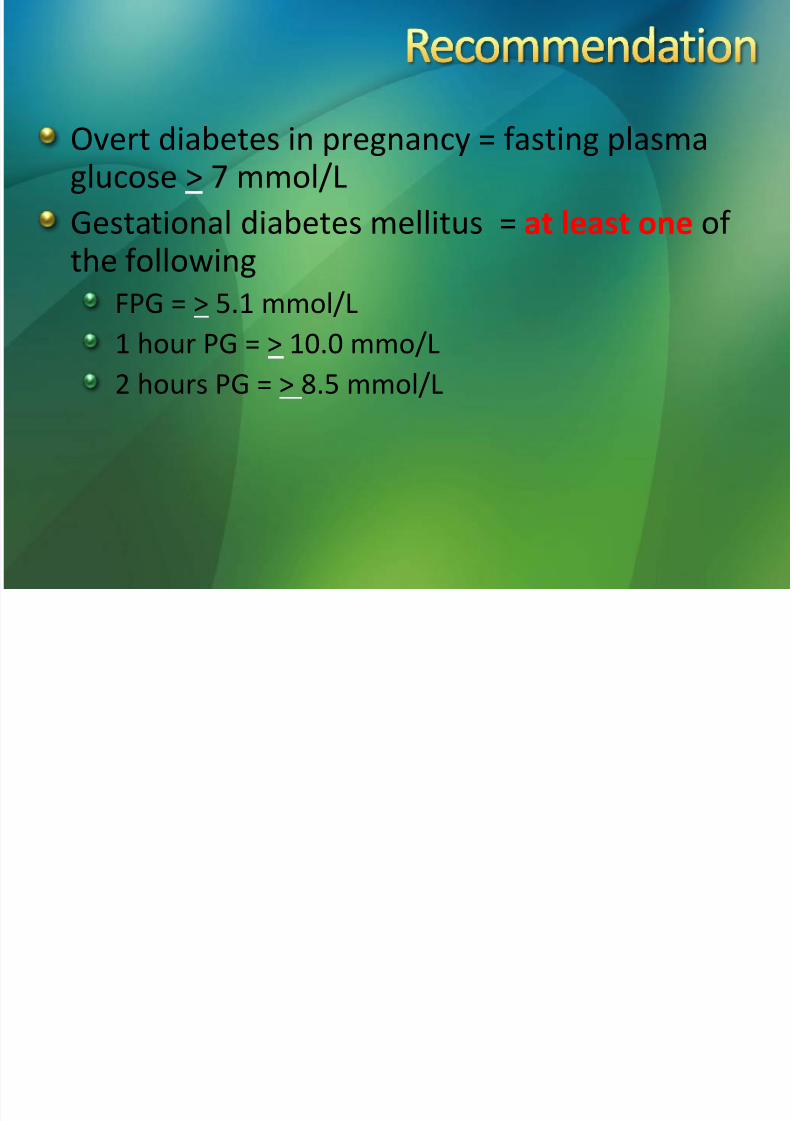
Overt diabetes in pregnancy = fasting plasmaglucose > 7 mmol/L
Gestational diabetes mellitus = at least one of the following
FPG = > 5.1 mmol/L
1 hour PG = > 10.0 mmo/L
2 hours PG = > 8.5 mmol/L

7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 50/59
75 gm oral glucose tolerance test3 days of normal diet
Fasting for at least 8 hours before the test
75gm glucose in 250 mls water to be finished in 10-15minutes
Rest during the 2 hours (of test procedure)

7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 51/59
75 gm OGTT Overt DM
GDM
Normal
75 gm OGTT Overt DM
GDM
Normal
……………………………………………………………………………………………………..
Antenatal
booking& all visits
24-28
weeks
gestation
7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 52/59
1. Screen the high risk women for diabetes in pregnancy atthe first and every antenatal encounters
2. Women at risk should undergo a 75 gm OGTT andplasma venous glucose testing at 0 (fasting state), 1 and2 hours post glucose load
3. Any one of the abnormal readings can be used in thediagnosis (of gestational diabetes mellitus)
4. Overt diabetes in pregnancy is diagnosed base on fastingplasma glucose
5. Those at risk and tested negative (for diabetes inpregnancy) on the initial encounter, should be re-testedat 24-28 weeks of gestation

7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 53/59
Dr Norhayati Yahaya
Dr Nurain Mohd Noor
Prof Mohd Shukri OthmanDr Iskandar Firzada Osman
Dr Khatijah Abd Rahman
AP Dr. Che Anuar Che Yaakob
Dr Zahar Azuar ZakariaDr Jusoh Senik
Dr Kamilah Mohamed
Dr Yazeed Zainal AbidinDr Nik Norashikin Nik AbdulRahman
Dr Jumizah Abd Kadir

7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 54/59
1. Detection rate2. Cost
3. Human resource
4. Training

7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 55/59
• Schaefer UM, Songster G, Xiang A, Berkowitz K, Buchanan TA,
Kjos SL. Congenital malformations in offspring of women withhyperglycemia first detected during pregnancy. Am J ObstetGynecol 1997;177:1165 –1171
• Omori Y, Jovanovic L. Proposal for the reconsideration of the
definition of gestational diabetes. Diabetes Care 2005; 28:2592 –2593
• Bartha JL, Martinez-Del-Fresno P, CominoDelgado R. Gestational
diabetes mellitus diagnosed during early pregnancy. Am JObstet Gynecol 2000;182:346 –350
• Maegawa Y, Sugiyama T, Kusaka H, Mitao M, Toyoda N.Screening tests for gestational diabetes in Japan in the 1st and2nd trimester of pregnancy. Diabetes Res Clin Pract 2003;62:47 –
7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 56/59
• Ostlund I and Hanson U. Occurrence of gestational diabetesmellitus and the value of different screening indicators forthe oral glucose tolerance test. Acta Obstetricia et Gynecologica Scandinavica 2003;82(2):103– 8
• Griffin ME, Coffey M, Johnson H, et al. Universal vs. risk
factor-based screening for gestational diabetes mellitus:detection rates, gestation at diagnosis and outcome.Diabetic Medicine 2000;17(1):26– 32
• Landon MB, Spong CY, Thom E, Carpenter MW, Ramin SM,
Casey B et al. A multicenter, randomized trial of treatmentfor mild gestational diabetes. N Engl J Med 2009; 361(14):1339 –1348.
7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 57/59
• Nicholson W, Bolen S, Witkop CT, Neale D, Wilson L, Bass E.
Benefits and risks of oral diabetes agent compared with insulin inwomen with gestational diabetes: a systematic review. ObstetGynaecol 2009; 113:193-205
•Crowther CA, Hiller JE, Moss JR, et al.; Australian CarbohydrateIntolerance Study in Pregnant Women (ACHOIS) Trial Group.Effect of treatment of gestational diabetes mellitus on pregnancyoutcomes. New England Journal of Medicine2005;352(24):2477 – 86.
• O'Sullivan JB & Mahan CM. Criteria for the oral glucose tolerancetest in pregnancy. Diabetes 1964; 13: 278 –285

7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 58/59
• HAPO Study Cooperative Research Group. Hyperglycemia andadverse pregnancy outcomes. N Engl J Med 1991-2002; 2008:358
• International Association of Diabetes and Pregnancy Study
Groups. International Association of Diabetes and PregnancyStudy Groups recommendations on the diagnosis andclassification of hyperglycemia in pregnancy. Diabetes Care 2010;33(3): 676 –682
• N Idris, CH Che Hatikah, MZ Murizah, MN Rushdan. UniversalVersus Selective Screening For Detection Of Gestational DiabetesMellitus In A Malaysian Population, Malaysian Family Physician2009; Volume 4, Number 2
7/27/2019 East Coast Working Group on Diabetes in Pregnancy
http://slidepdf.com/reader/full/east-coast-working-group-on-diabetes-in-pregnancy 59/59
• Shamsuddin K, Mahdy ZA, Rafiaah SI, Jamil MA. Risk Factorscreening for abnormal glucose tolerance in pregnancy.International Journal of Gynecology and Obstetric 2001;75:27-32
• Chan S. Prevalence of GDM in Malaysia. ASGODIP Report:
ASEAN, 7th Congress of ASEAN Federation of Endocrine Society,1993
• Landon MB, Spong CY, Thom E, Carpenter MW, Ramin SM, Casey
B et al. A multicenter, randomized trial of treatment for mildgestational diabetes. N Engl J Med 2009; 361(14): 1339 –1348