early pregnancy complications - montfort · uottawa.ca early pregnancy complications • journee...
TRANSCRIPT

uOttawa.ca
Early Pregnancy Complications
• Journee Montfort
Presented by: Vincent della Zazzera, April 8 2016
uOttawa.ca
Faculté des sciences sociales | Faculty of Social Sciences
uOttawa.ca
Early Pregnancy Complication
Nothing to disclose
uOttawa.ca
3

uOttawa.ca
Case 1
29yo presents with abdominal pain, light PV bleeding. She has been amenorrheic for the past 40 days and urine BhCG is +.
• Normal pregnancy
• Failed pregnancy
• Threatened abortion
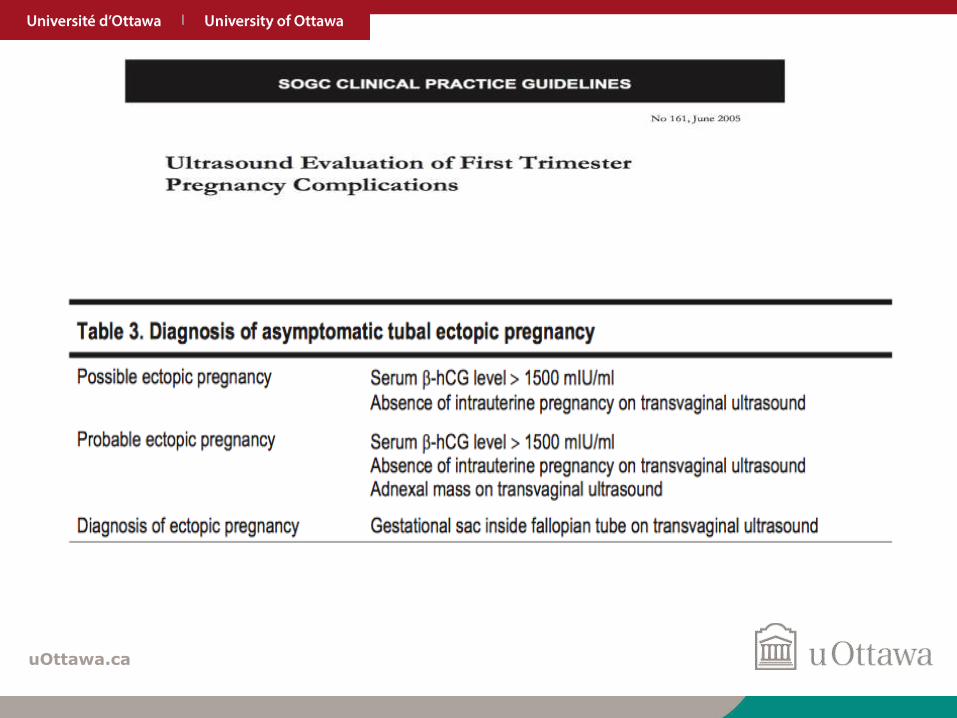
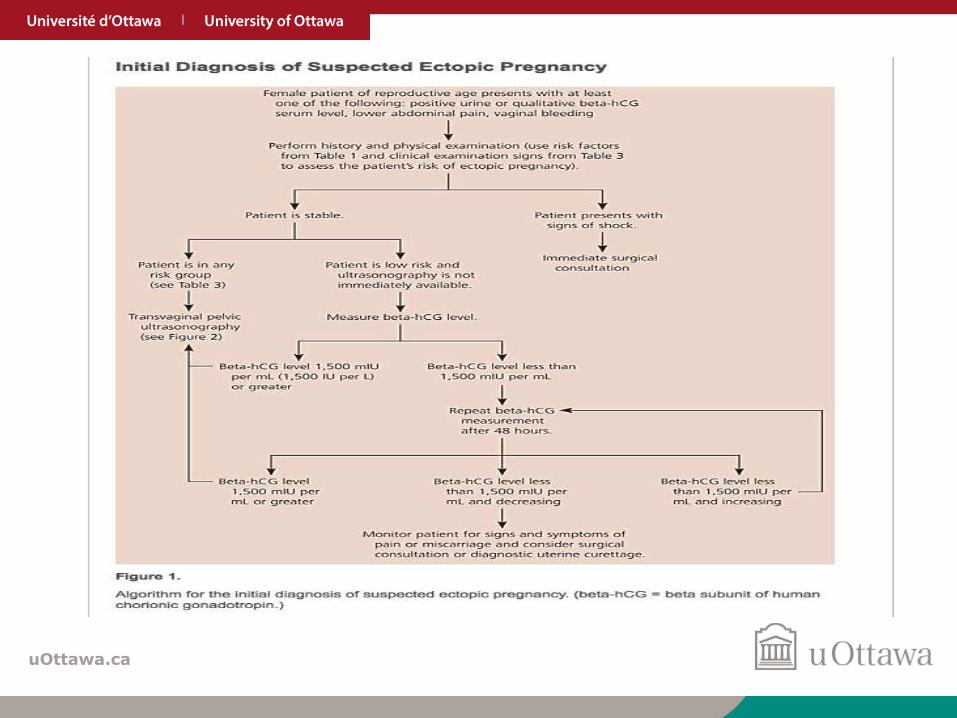
• PUL/Ectopic pregnancy

uOttawa.ca
Case 129yo presents with abdominal pain, light PV bleeding. She has been amenorrheic for the past 40 days and urine BhCGis +.
Investigations?
• B/W
– Complete CBC
– BhCG
– Progesterone
– Type, RH
– LFT’s, Renal function
• Ultrasound
– Gyne Ultrasound
• Early pregnancy scan, viability? r/o Ectopic

uOttawa.ca
Case 1Desired pregnancy
• Lab:
– BhCG; 1500, Progesterone 78
– A+
– CBC, LFT, Renal (N)
• Ultrasound:
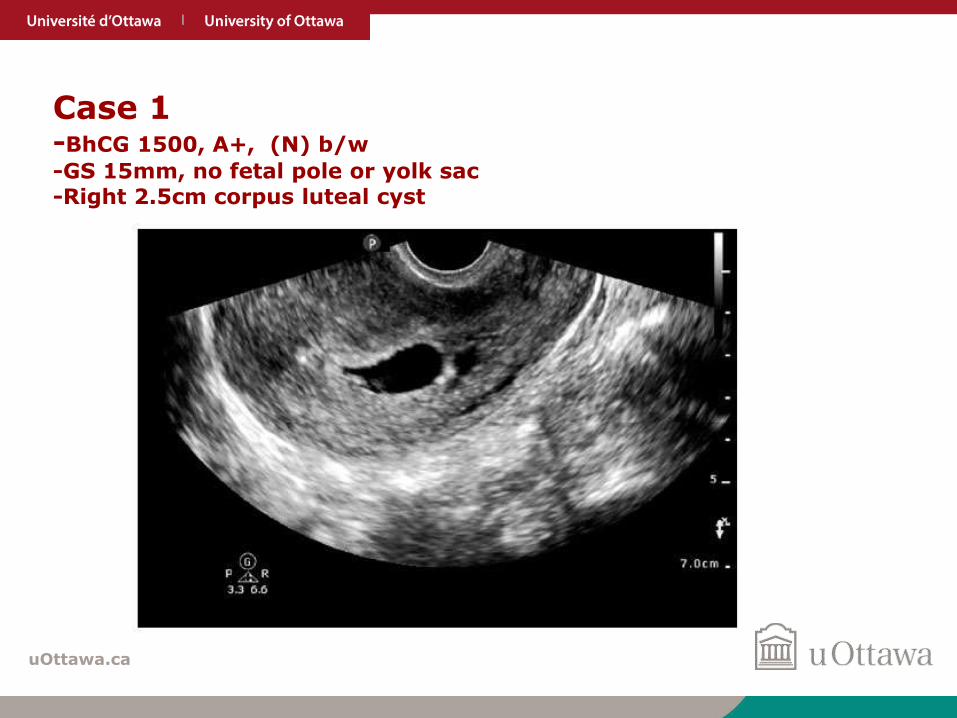
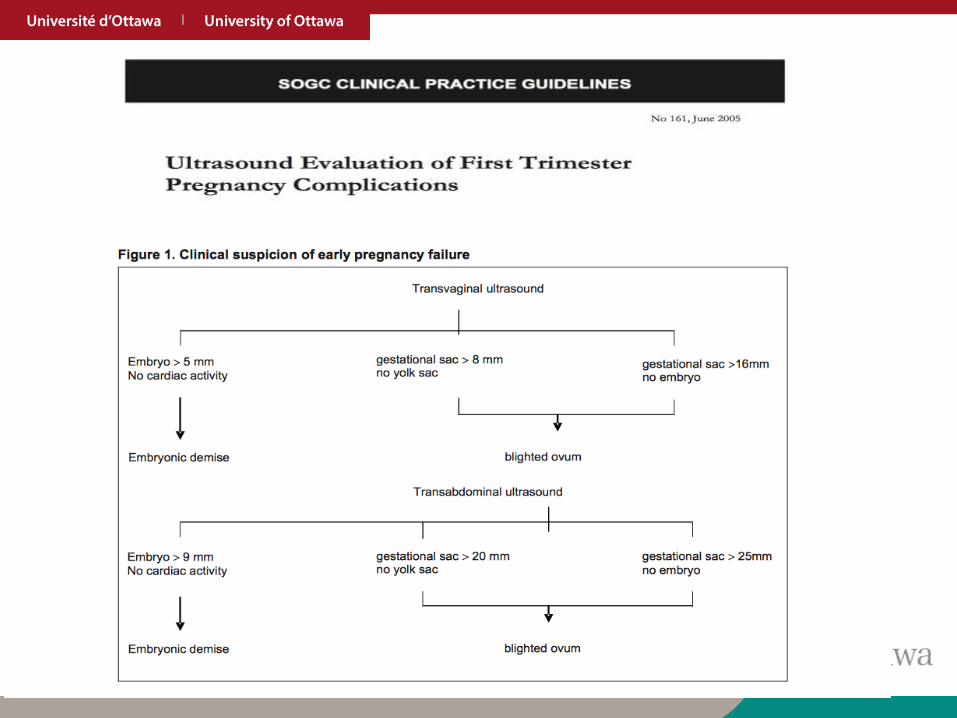
– Slight endometrial thickening with scan fluid, gestational sac measuring 15mm with no yolk sac or fetal pole is seen
– Bilateral adnexa and ovaries are unremarkable other than a small 2.5cm anechoic cyst on right ovary, likely corpus luteal cyst
uOttawa.ca
Case 1-BhCG 1500, A+, (N) b/w
-GS 15mm, no fetal pole or yolk sac -Right 2.5cm corpus luteal cyst
uOttawa.ca
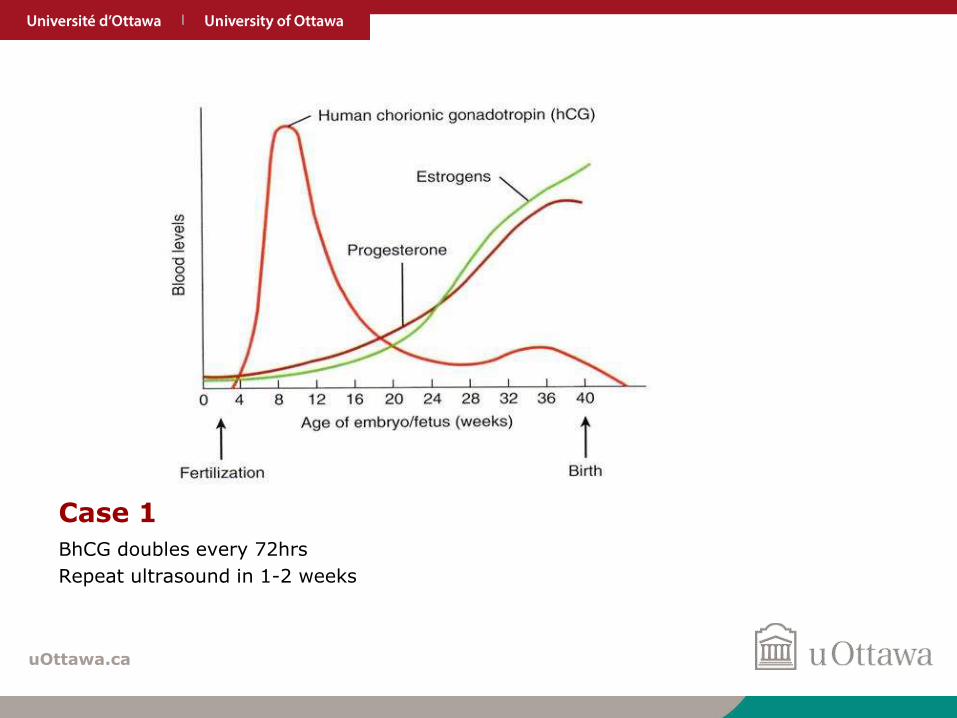
Case 1
BhCG doubles every 72hrs
Repeat ultrasound in 1-2 weeks

uOttawa.ca
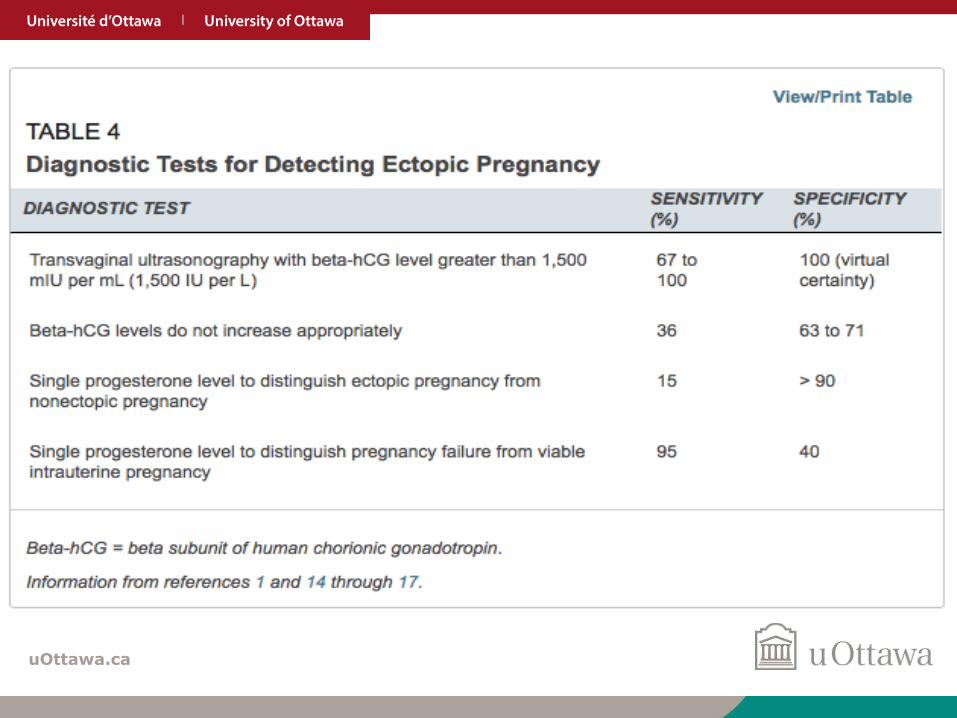
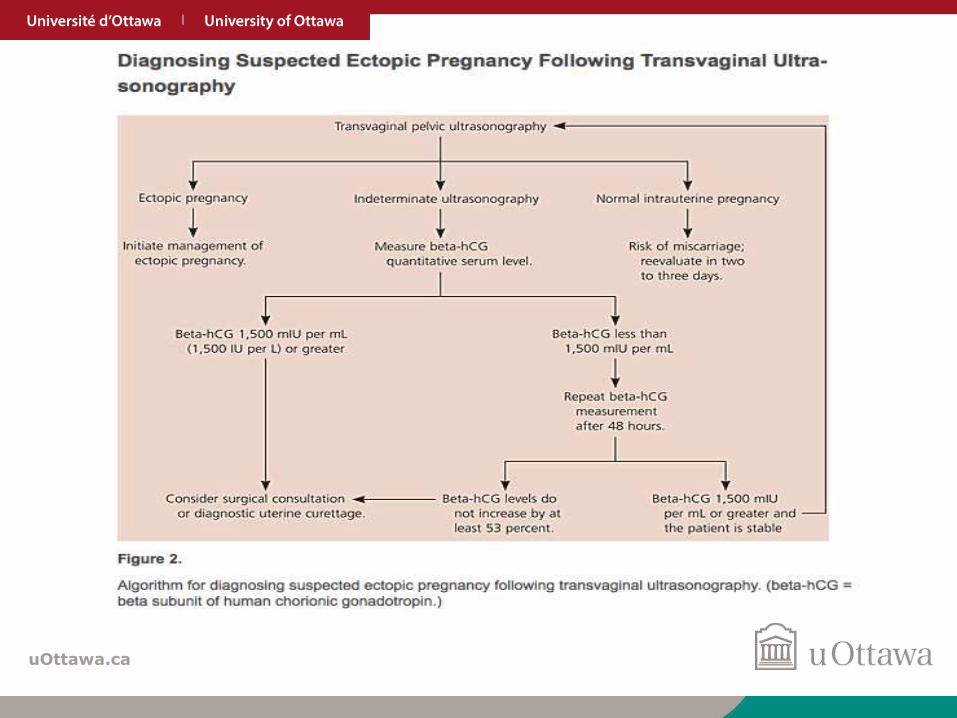
QUIZAt what BhCG level should we be able to confirm a
intra-uterine pregnancy?
• Endovaginal– 800
– 1200
– 2000
– 5000
– 7500
• Trans Abdominal – 800
– 1200
– 2000
– 5000
– 7500

uOttawa.ca
QUIZAt what BhCG level should we be able to confirm a
intra-uterine pregnancy?
• Endovaginal– 800
– 1200
– 2000
– 5000
– 7500
• Trans Abdominal – 800
– 1200
– 2000
– 5000
– 7500
uOttawa.ca
• First ultrasound performed after 7 to 13GA
• EDC assigned using ultrasound biometry
• Ultrasound is more accurate than a “certain” menstrual date
• Ideally all women should have a dating ultrasound

uOttawa.ca
Case 229yo presents with abdominal pain, light PV bleeding. She has been amenorrheic for the past 40 days and urine BhCGis +.
Investigations?
• B/W
– Complete CBC
– BhCG
– Progesterone
– Type, RH
– LFT’s, Renal function
• Ultrasound
– Gyne Ultrasound
• Early pregnancy scan, viability? r/o Ectopic
uOttawa.ca
Case 2Desired pregnancy
• Lab:
– BhCG; 900, Progesterone 30
– A-
– CBC, LFT, Renal (N)
• Ultrasound:
– Slight endometrial thickening with scan fluid, no gestational sac seen. NO IUPC seen
– Bilateral adnexa and ovaries are unremarkable other than a small 2.5cm anechoic cyst on right para-ovarian adnexal region, ectopic pregnancy can not be ruled out

uOttawa.ca
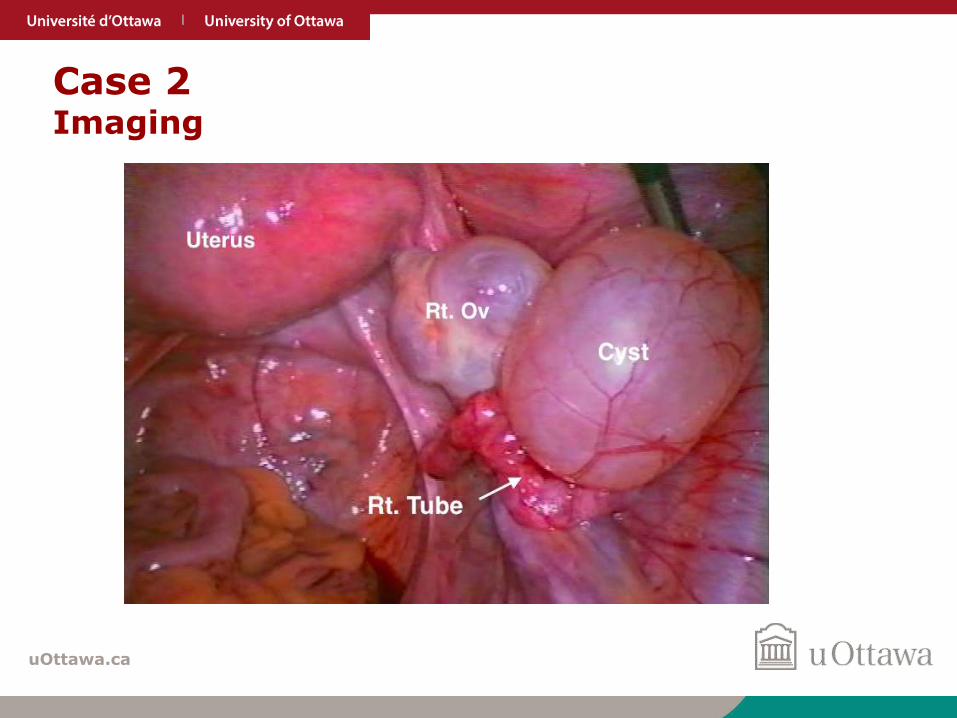
Case 2 Imaging
uOttawa.ca
Case 2 Imaging
uOttawa.ca
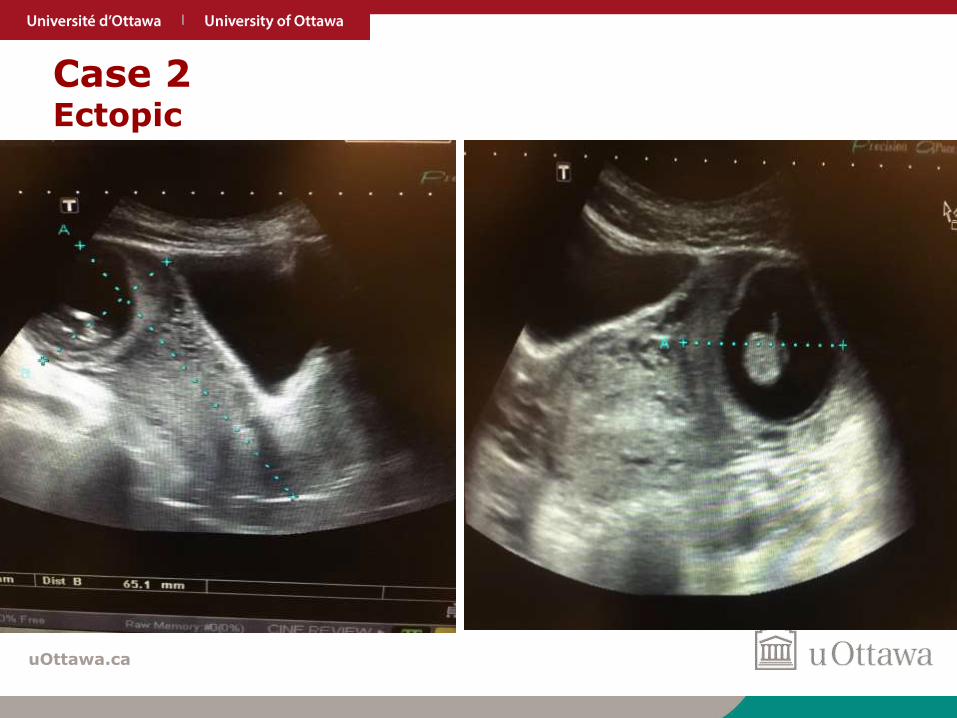
Case 2Ectopic
uOttawa.ca
uOttawa.ca
uOttawa.ca
uOttawa.ca
uOttawa.ca
uOttawa.ca
uOttawa.ca

uOttawa.ca
Case 3
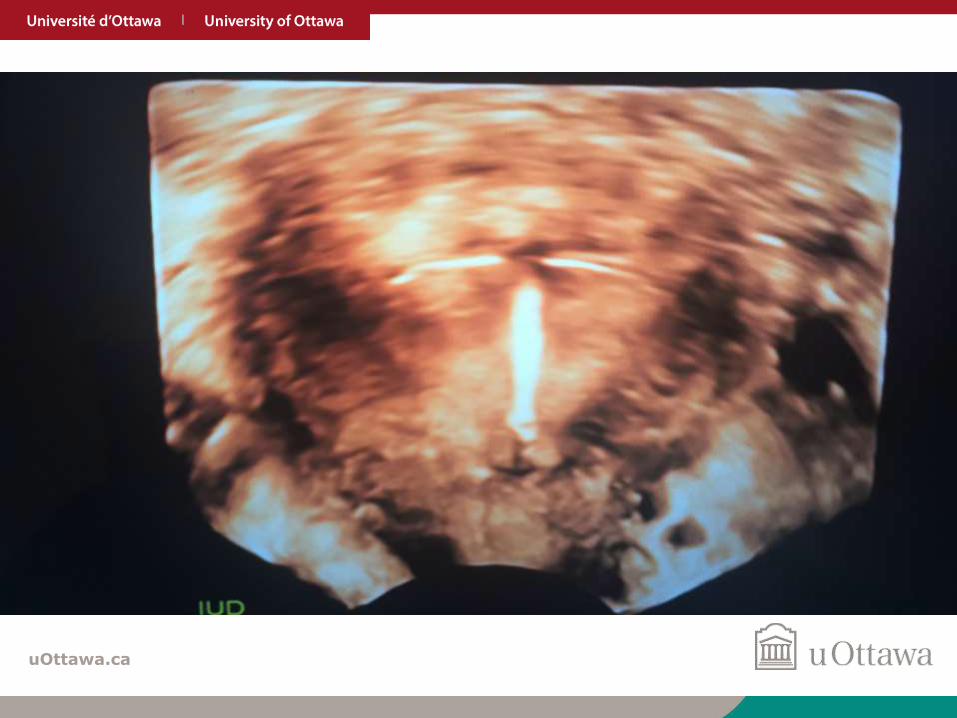
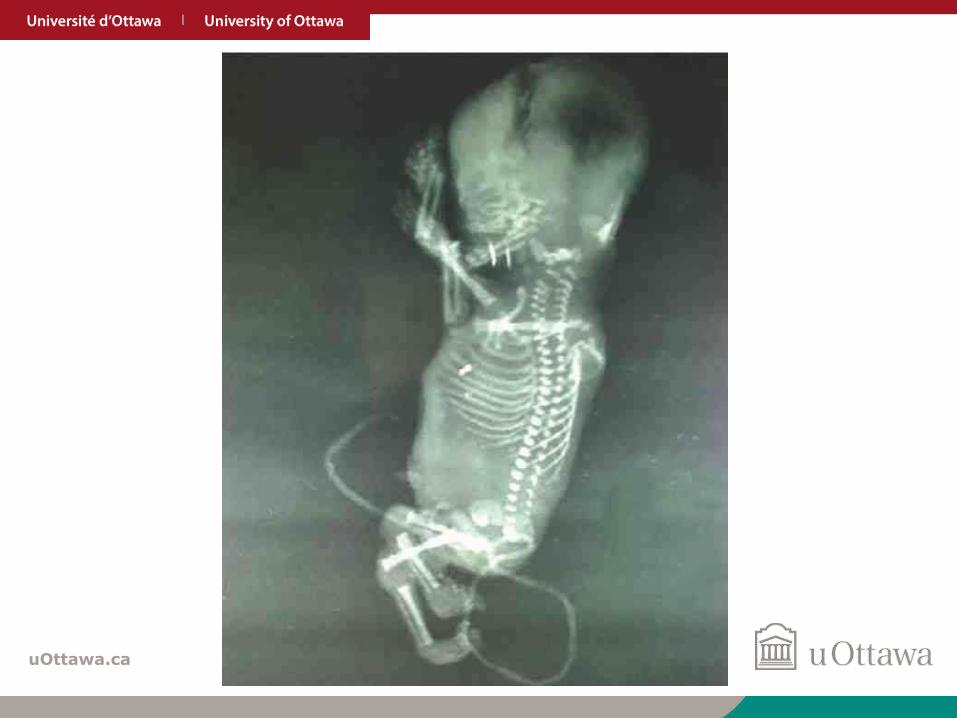
29yo presents with abdominal pain, light PV bleeding. She has been amenorrheic for the past 3 years due to Mirena IUD, urine BhCG is +.
• What to do if pregnant with IUD
• Confirm intra-uterine
• Rule out Ectopic
uOttawa.ca
uOttawa.ca
uOttawa.ca
Case 3
29yo presents with abdominal pain, light PV bleeding. She has been amenorrheic for the past 3 years due to Mirena IUD, urine BhCG is +.
Strings are present on exam, according to u/s IUP currently 6GA
• Remove IUD in office
• Leave IUD in situ
• Misoprostol 800mcg PV q24h x2
• Book for IUD removal and D&C
uOttawa.ca
Case 3
29yo presents with abdominal pain, light PV bleeding. She has been amenorrheic for the past 3 years due to Mirena IUD, urine BhCG is +.
Strings are NOT present on exam, according to u/s IUP currently 6GA
• Remove IUD in office
• Leave IUD in situ
• Misoprostol 800mcg PV q24h x2
• Book for IUD removal and D&C
uOttawa.ca
Case 3
29yo presents with abdominal pain, light PV bleeding. She has been amenorrheic for the past 3 years due to Mirena IUD, urine BhCG is +.
Strings are present on exam, according to u/s IUP currently 18GA
• Remove IUD in office
• Leave IUD in situ
• Misoprostol 800mcg PV q24h x2
• Book for IUD removal and D&C
uOttawa.ca
uOttawa.ca
IUD retained versus removed
• Tatum et al 275 women with cu-IUD
• 118 (43%) removed
– Live birth rate 79%
• 157 (57%) left in situ
– Live birth rate 44%
uOttawa.ca
uOttawa.ca
Case 3
29yo presents with abdominal pain, light PV bleeding. She has been amenorrheic for the past 3 years due to Mirena IUD, urine BhCG is +.
Strings are present on exam, according to u/s IUP currently 6GA
• Remove IUD in office
• Leave IUD in situ
• Misoprostol 800mcg PV q24h x2
• Book for IUD removal and D&C

uOttawa.ca
Case 3
29yo presents with abdominal pain, light PV bleeding. She has been amenorrheic for the past 3 years due to Mirena IUD, urine BhCG is +.
Strings are present on exam, according to u/s IUP currently 6GA
• Remove IUD in office
• Leave IUD in situ
• Misoprostol 800mcg PV q24h x2
• Book for IUD removal and D&C
uOttawa.ca
Case 3
29yo presents with abdominal pain, light PV bleeding. She has been amenorrheic for the past 3 years due to Mirena IUD, urine BhCG is +.
Strings are NOT present on exam, according to u/s IUP currently 6GA
• Remove IUD in office
• Leave IUD in situ
• Misoprostol 800mcg PV q24h x2
• Book for IUD removal and D&C
uOttawa.ca
Case 3
29yo presents with abdominal pain, light PV bleeding. She has been amenorrheic for the past 3 years due to Mirena IUD, urine BhCG is +.
Strings are NOT present on exam, according to u/s IUP currently 6GA
• Remove IUD in office
• Leave IUD in situ
• Misoprostol 800mcg PV q24h x2
• Book for IUD removal and D&C
uOttawa.ca
Case 3
29yo presents with abdominal pain, light PV bleeding. She has been amenorrheic for the past 3 years due to Mirena IUD, urine BhCG is +.
Strings are present on exam, according to u/s IUP currently 18GA
• Remove IUD
• Leave IUD in situ
• Misoprostol 800mcg PV q24h x2
• Book for IUD removal and D&C
uOttawa.ca
Case 3
29yo presents with abdominal pain, light PV bleeding. She has been amenorrheic for the past 3 years due to Mirena IUD, urine BhCG is +.
Strings are present on exam, according to u/s IUP currently 18GA
• Remove IUD
• Leave IUD in situ
• Misoprostol 800mcg PV q24h x2
• Book for IUD removal and D&C
uOttawa.ca
39