early arthritis clinic jack cush, md. what do i have to do to get this patient seen? 53 yowm under...
TRANSCRIPT

Early Arthritis Clinic
Jack Cush, MDJack Cush, MD

What do I have to do to get this patient seen?
• 53 yoWM under evaluation for eosinophilia53 yoWM under evaluation for eosinophilia• No Meds; PMHx prostatitis; ROS negativeNo Meds; PMHx prostatitis; ROS negative• Only c/o R knee effusion/warmth x 12 weeksOnly c/o R knee effusion/warmth x 12 weeks• Negative: CBC, BM Bx, Stool O/P, ANA, DNA, ESR, Negative: CBC, BM Bx, Stool O/P, ANA, DNA, ESR,
UA, CXR (pending RF, CRP)UA, CXR (pending RF, CRP)• Hematology W/U exhaustedHematology W/U exhausted
– How to w/u the swollen R knee (maybe L too)?How to w/u the swollen R knee (maybe L too)?• Next availalable rheumatology appt?Next availalable rheumatology appt?• Who you gonna call?Who you gonna call?
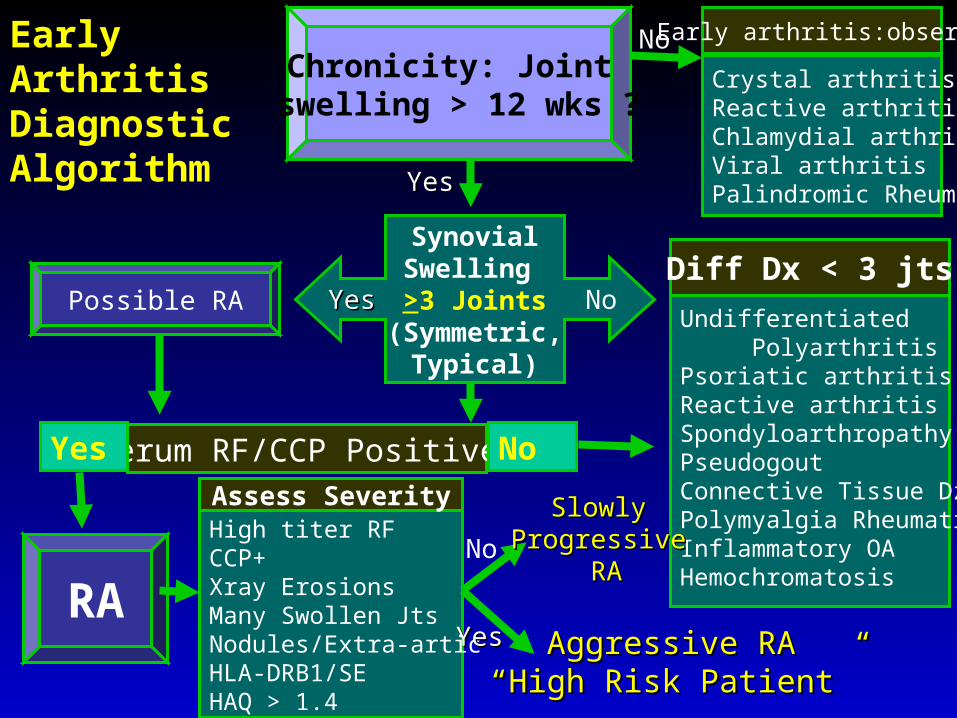
Early Arthritis Diagnostic Algorithm
Chronicity: Joint swelling > 12 wks ?
Serum RF/CCP Positive?Yes
Possible RA
RA
Crystal arthritisReactive arthritisChlamydial arthritisViral arthritisPalindromic Rheum.
Early arthritis:observe
SynovialSwelling >3 Joints
(Symmetric,Typical)
Undifferentiated PolyarthritisPsoriatic arthritisReactive arthritisSpondyloarthropathyPseudogoutConnective Tissue DzPolymyalgia RheumaticaInflammatory OAHemochromatosis
Diff Dx < 3 jts
No
High titer RFCCP+Xray ErosionsMany Swollen JtsNodules/Extra-articHLA-DRB1/SEHAQ > 1.4
Assess Severity
Aggressive RAAggressive RA““High Risk Patient”High Risk Patient”
SlowlySlowlyProgressiveProgressive
RARA
No
No
No
YesYes
YesYes
YesYes

CityCity PopulationPopulation RheumsRheums Pts/RheumPts/Rheum New RA/yrNew RA/yr
Ft. Smith, ARFt. Smith, AR 81,51881,518 22 83668366 1616
Ft Collins, COFt Collins, CO 124,665124,665 22 62,32262,322 2424
Little Rock, ARLittle Rock, AR 184,055184,055 2222 83668366 3737
Huntsville, ALHuntsville, AL 162,536162,536 55 32,50732,507 3232
Birmingham, ALBirmingham, AL 239,416239,416 45(30)45(30) 53205320 4747
Toledo, OHToledo, OH 309,106309,106 77 44,15844,158 6262
Omaha, NEOmaha, NE 399,106399,106 1212 33,27933,279 8080
Denver, CODenver, CO 560,415560,415 40(29)40(29) 14,01014,010 112112
Charlotte, NCCharlotte, NC 580,597580,597 1414 36,32836,328 116116
Nashville, TNNashville, TN 648,882648,882 2525 29,95529,955 138138
Louisville, KYLouisville, KY 698,080698,080 1818 38,78238,782 140140
SanAntonio, TXSanAntonio, TX 1,194,2221,194,222 30(24)30(24) 39,80739,807 238238
Dallas, TXDallas, TX 1,211,4671,211,467 46 (29)46 (29) 26,33626,336 242242
US City Populatoins and Expected NEW RA Cases every Year (28-56,000)

10.3 Million w/ Chronic Joint Symptoms Have Never Seen an MD
• 2001 CDC, BRFSS adult 2001 CDC, BRFSS adult telephone survey (>18yrs)telephone survey (>18yrs)
• 2001 estimated 47.5 million 2001 estimated 47.5 million with CJSwith CJS
• 10.3 million have not seen 10.3 million have not seen MD (~2.0 million w/ activity MD (~2.0 million w/ activity limitations). Risk Factors:limitations). Risk Factors:– < HS education, excellent-< HS education, excellent-
good health, no insurance, no good health, no insurance, no PCP, no activity limitation and PCP, no activity limitation and engaged in regular physical engaged in regular physical activity activity
876,000

Early RA: Window of Opportunity
MD?MD? PCPPCP RheumsRheums
#’s?#’s? 800,000800,000 725,000725,000
Sxs?Sxs? Wks-MosWks-Mos Mos-YrsMos-Yrs
RA/Inflammatory Arthritis Continuom
FewFew JointsJoints ManyMany
NormalNormal XRayXRay ErosiveErosive
PossiblePossible RemissionRemission Rare?Rare?
Full TimeFull Time Employed?Employed? DisabilityDisability

Early RA: A problematic diagnosis
• Most patients will not meet ACR criteriaMost patients will not meet ACR criteria• Most patients will not be RF+ ( 19- 45%)Most patients will not be RF+ ( 19- 45%)• Most patients will not seek medical careMost patients will not seek medical care• Most PCPs prefer to evaluate, rather than referMost PCPs prefer to evaluate, rather than refer• Many patients will remit with symptomatic RxMany patients will remit with symptomatic Rx• Histopathology similar: RA, ERA, UPAHistopathology similar: RA, ERA, UPA• Few features to distinguish RA vs UPAFew features to distinguish RA vs UPA
• Duration, #Jts, RF+, CCP+, ESR/CRPDuration, #Jts, RF+, CCP+, ESR/CRP• Cost of diagnositic evaluation is higher in UPACost of diagnositic evaluation is higher in UPA

• Early RA defined as < 12 weeks; the earlier the betterEarly RA defined as < 12 weeks; the earlier the better• Articular erosions/damage evident earlyArticular erosions/damage evident early Delay in Rx is Disastrous!Delay in Rx is Disastrous!• 11st st DMARD Choice is CRITICAL! DMARD Choice is CRITICAL!
– Use Best DMARD First!Use Best DMARD First!– Multiple Trials show signif. downstream effectsMultiple Trials show signif. downstream effects
• High Risk Early RA patients Can Be definedHigh Risk Early RA patients Can Be defined• RF and CCP are Predictive and OMINOUS togetherRF and CCP are Predictive and OMINOUS together• DMARDs work, COMBOs and Biologics are Better!DMARDs work, COMBOs and Biologics are Better!• Referral Rules: Referral Rules: >>3 jts, squeeze test, Sx 6-12 wks, RF+3 jts, squeeze test, Sx 6-12 wks, RF+• Challenge: how to facillitate early referralChallenge: how to facillitate early referral
Early RA: Take Home PointsEarly RA: Take Home Points

Short Delay of Therapy Affected Radiographic Outcome
Lard LR, et al.Lard LR, et al. Am J Med. Am J Med. 2001;111:446-451. 2001;111:446-451.
Time (months)Time (months)
00
22
44
66
88
1010
1212
1414
00 66 1212 1818 2424
Early Treatment = median 15 daysEarly Treatment = median 15 days
Delayed Treatment = median 123 daysDelayed Treatment = median 123 days
Sharp ScoreSharp Score

• Case-controlled, parallel studyCase-controlled, parallel study• Very early RA (VERA): dz duration 3 mosVery early RA (VERA): dz duration 3 mos• Late early RA (LERA): Late early RA (LERA): <<12 mos to DMARD12 mos to DMARD• DMARDS: SSZ, MTX, CQ, CYA, LEF, ComboDMARDS: SSZ, MTX, CQ, CYA, LEF, Combo• Evaluated at 36 mos: DAS28, Larsen scoreEvaluated at 36 mos: DAS28, Larsen score
– At study end DAS28 improved 2.8At study end DAS28 improved 2.8±±1.5 in the VERA vs. 1.5 in the VERA vs.
1.71.7±±1.2 in the LERA group (P<0.05)1.2 in the LERA group (P<0.05)
– Larsen scores showed a statistically significant Larsen scores showed a statistically significant
retardation of progression in VERA vs. LERAretardation of progression in VERA vs. LERA
Early Referral, Early DMARD in VERANell VP, Machold KP, Eberl G, et al. Rheumatology 2004

Percent of Patients Fulfilling ACR Response Criteria After 36 Months of Follow-Up
0
10
20
30
40
50
60
70
80
90
100
20% response 50% response 70% response
% P
atie
nts
Wit
h F
ulf
ille
d C
rite
ria
* P<0.05 Nell V. et al., Rheumatology 2004; 43:906-14.
**
LERAVERA1

Radiographic Changes in LERA and VERA1 Patients, Indicated by the Larsen Score
0
10
20
30
40
0 12 24 36
La
rse
n S
core
Months after DMARD initiation
* P<0.05 Nell V. et al., Rheumatology 2004; 43:906-14.
**
LERA
VERA1*
*
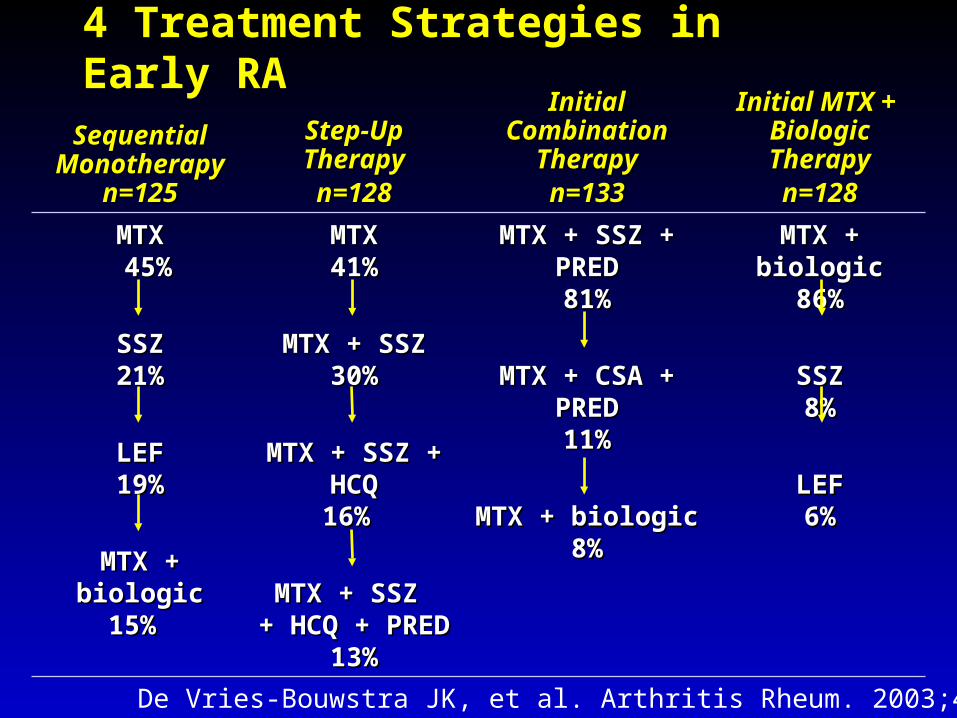
Sequential Sequential MonotherapyMonotherapy
n=125n=125
Step-Up Step-Up TherapyTherapyn=128n=128
Initial Initial Combination Combination
TherapyTherapyn=133n=133
Initial MTX + Initial MTX + Biologic Biologic TherapyTherapyn=128n=128
MTXMTX 45% 45%
SSZSSZ21%21%
LEFLEF19%19%
MTX + biologicMTX + biologic15% 15%
MTXMTX41%41%
MTX + SSZMTX + SSZ30%30%
MTX + SSZ + MTX + SSZ + HCQHCQ16% 16%
MTX + SSZ MTX + SSZ + HCQ + PRED+ HCQ + PRED
13%13%
MTX + SSZ + MTX + SSZ + PREDPRED81%81%
MTX + CSA + MTX + CSA + PREDPRED11%11%
MTX + biologicMTX + biologic8%8%
MTX + biologicMTX + biologic86%86%
SSZSSZ8%8%
LEFLEF6%6%
De Vries-Bouwstra JK, et al. Arthritis Rheum. 2003;48:3649.
4 Treatment Strategies in Early RA

0
10
20
30
40
50
60
70
80
0 3 6 9 12
Time (months)
Per
cent
age
I Monotherapy
II Step-up
III Combination
IV Biologic
Percentage of Patients in Remission: DAS44 < 1.6
Discontinuation of Biologic
De Vries-Bouwstra JK, et al. Arthritis Rheum. 2003;48:3649.

Aggressive Therapy Example: COBRA 1997
Study Study designdesign
Double-blind, randomized studyDouble-blind, randomized study
PopulationPopulation 155 early active RA patients 155 early active RA patients (no more than 2 years from ACR diagnosis)(no more than 2 years from ACR diagnosis)
Treatment Treatment groupsgroups
• Prednisolone (60Prednisolone (607.5 mg/day step-down), 7.5 mg/day step-down), MTX (7.5 mg/week), SSZ (2 g/day) vs MTX (7.5 mg/week), SSZ (2 g/day) vs SSZ (2 g/day)SSZ (2 g/day)
• Prednisolone and MTX tapered and stopped Prednisolone and MTX tapered and stopped after 28 weeks and 40 weeks, respectively after 28 weeks and 40 weeks, respectively
Follow-upFollow-up 56 weeks56 weeks
Boers M, et al. Boers M, et al. Lancet.Lancet. 1997;350:309-318. 1997;350:309-318. Landewe R, et al. Landewe R, et al. Arthritis Rheum.Arthritis Rheum. 2002:46:347-356. 2002:46:347-356.
ACR = American College of Rheumatology; COBRA = Combinatietherapie Bij Reumatoide ACR = American College of Rheumatology; COBRA = Combinatietherapie Bij Reumatoide Artritis; MTX = methotrexate; SSZ = sulfasalazine.Artritis; MTX = methotrexate; SSZ = sulfasalazine.

Step-Down TherapyStep-Down TherapyCOBRA Trial
Adapted from: Boers M, et al. Adapted from: Boers M, et al. Lancet.Lancet. 1997;350:309-318. 1997;350:309-318.
Clinical OutcomeClinical Outcome
0.0
0.4
0.8
1.2
1.6
Pooled Index
weeks
16 28 40 560
MTX
Pred
COBRA Treatment protocol
SSZ
Time (Weeks)
Po
ole
d In
de
x S
co
re
Prednisolone
MethotrexateSulfasalazine
Combined TreatmentCombined Treatment
SulphasalazineSulphasalazine

Early Aggressive Therapy Provides for Long-term Results
P=0.008
0
10
20
30
40
0 1 2 3 4 5
Damage Progression (Sharp/van der Heijde)
Years
COBRA:5.4 points/y
SSZ:8.6 points/y
Landewe RB, et al. Arthritis Rheum. 2002;46:347-356.
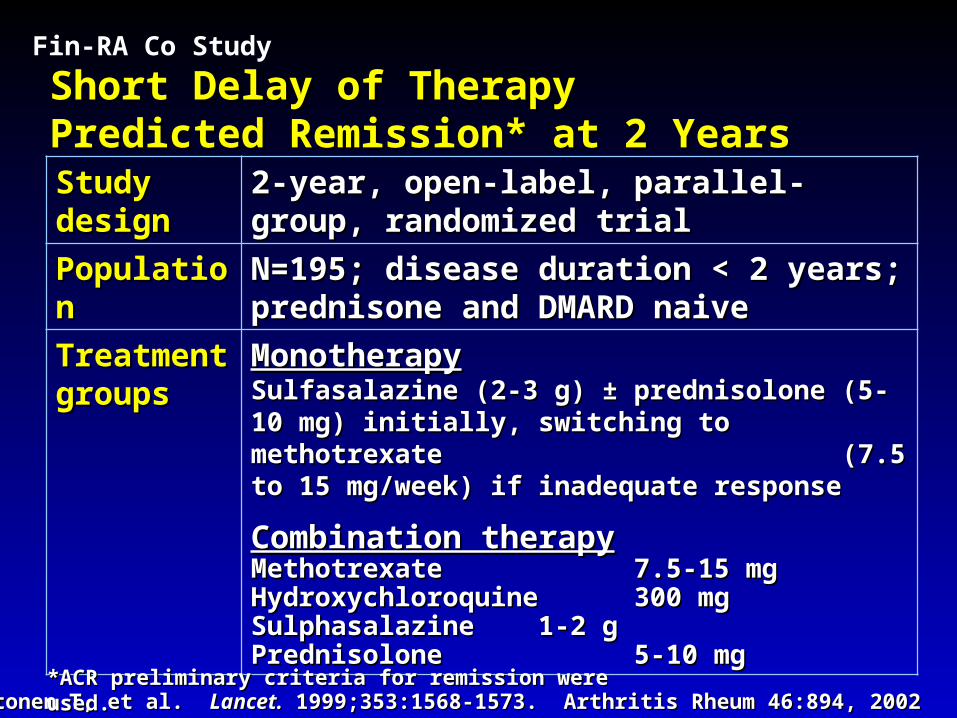
Short Delay of Therapy Short Delay of Therapy Predicted Remission* at 2 YearsPredicted Remission* at 2 YearsStudy Study designdesign
2-year, open-label, parallel-group, 2-year, open-label, parallel-group, randomized trialrandomized trial
PopulationPopulation N=195; disease duration < 2 years; N=195; disease duration < 2 years; prednisone and DMARD naiveprednisone and DMARD naive
Treatment Treatment groupsgroups
MonotherapyMonotherapy Sulfasalazine (2-3 g) Sulfasalazine (2-3 g) ±± prednisolone (5-10 mg) prednisolone (5-10 mg) initially, switching to methotrexate initially, switching to methotrexate (7.5 to 15 mg/week) if inadequate response(7.5 to 15 mg/week) if inadequate response
Combination therapyCombination therapyMethotrexateMethotrexate 7.5-15 mg7.5-15 mgHydroxychloroquineHydroxychloroquine 300 mg300 mgSulphasalazineSulphasalazine 1-2 g1-2 gPrednisolonePrednisolone 5-10 mg5-10 mg
Fin-RA Co Study
Mottonen T, et al. Mottonen T, et al. Lancet.Lancet. 1999;353:1568-1573. Arthritis Rheum 46:894, 2002 1999;353:1568-1573. Arthritis Rheum 46:894, 2002*ACR preliminary criteria for remission were used.*ACR preliminary criteria for remission were used.

050
100150200250300350400450500550600
0 1 2 3 4 5
Cumulative follow-up time (years)
Cu
mu
lati
ve w
ork
dis
abili
ty d
ays Combination Therapy
Single Therapy
Fin-Co-RA Work Disability Early RAFin-Co-RA Work Disability Early RA5 Yr Followup of Single vs Triple DMARD5 Yr Followup of Single vs Triple DMARD
Puolakka, K. et al., Arthritis Rheum 2004;50:55-62.
ß=119
ß=79
ß=annual regression coefficient
GREATERSick LeaveWork DisabilityRetirement

Genovese MC, et al. Arthritis Rheum. 2002;46:1443–1450.
% o
f P
atie
nts
0
20
40
60
80
59
72
4249
2429
100
ACR-20 ACR-50 ACR-70
MTX 20 mg
Etanercept 25 mgP = 0.005
P = NS
P = NS
Etanercept in Early RA: ACR Response Rates at Year 2
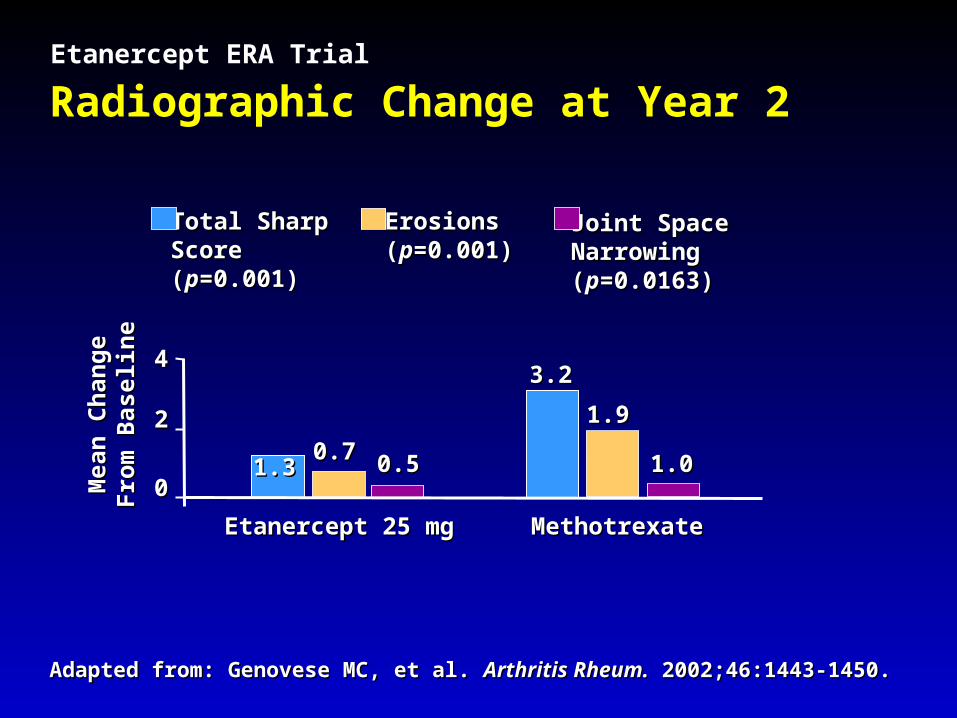
1.91.9
1.01.0
Mea
n C
han
ge
Mea
n C
han
ge
Fro
m B
asel
ine
Fro
m B
asel
ine
3.23.2
1.31.3
00
22
44
Etanercept 25 mgEtanercept 25 mg
Total Sharp Total Sharp Score Score ((pp=0.001)=0.001)
0.70.70.50.5
MethotrexateMethotrexate
Joint Space Joint Space Narrowing Narrowing ((pp=0.0163)=0.0163)
ErosionsErosions((pp=0.001)=0.001)
Radiographic Change at Year 2
Adapted from: Genovese MC, et al. Adapted from: Genovese MC, et al. Arthritis Rheum.Arthritis Rheum. 2002;46:1443-1450. 2002;46:1443-1450.
Etanercept ERA Trial

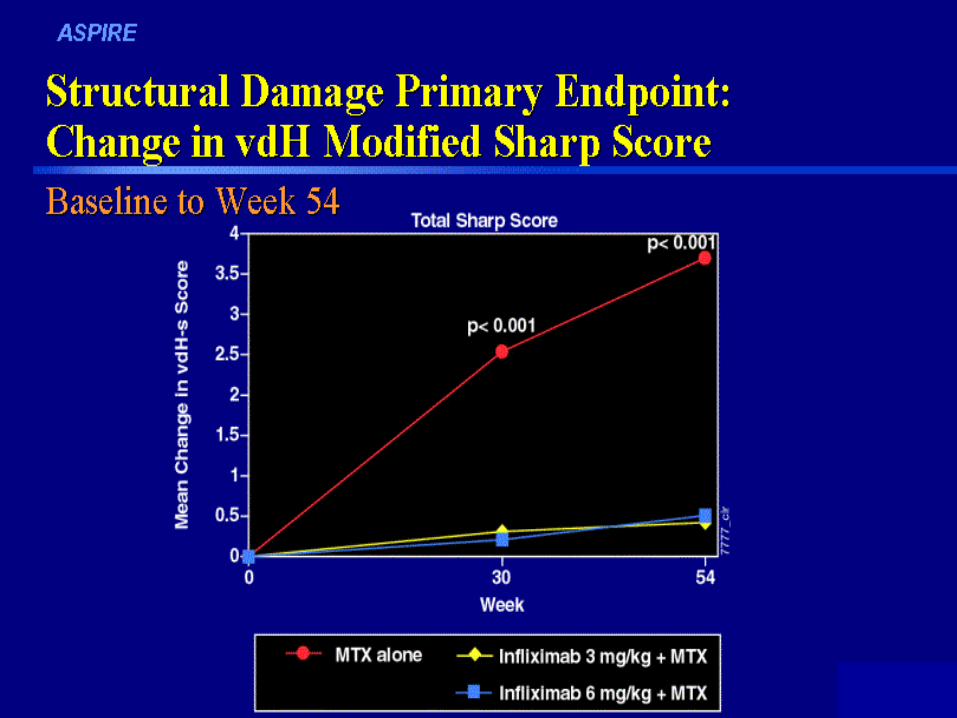
ASPIRE: MTX & INFLIXIMAB IN EARLY RA
• 54 wk phase IV DBRPCT– MTX vs MTX + Infliximab (3 or 6 mg/kg)
• Early RA < 3 yrs duration ( mean ~ 7 mos)• N=1050; 125 centers worldwide; 4:5:5 random• Inclusion
– 12 Tender & 10 Swollen (30 Tend & 19 Swoll)– RF+ or CRP^ or XRAY erosion ( > 80%)

Presbyterian Hospital of DallasEarly Arthritis Clinic
Tuesday AfternoonsTuesday AfternoonsJack Cush, MDJack Cush, MD
Andres Quiceno, MDAndres Quiceno, MDKathyrn Dao, MDKathyrn Dao, MD

EARLY ARTHRITIS CLINIC REFERRAL(Patients must have “arthrititis” for < 12 months)
Patient Name : Age :___________________Referring Physician Phone # Fax #Previously Seen a Rheumatologist? NO YES Whom: __________ Symptoms Began: Diagnosis Date: _________Reason for Referral (Choose any that apply) ?Acute PainAcute SwellingChronic PainChronic SwellingWidespread PainAffected Joints: Hand Feet Shoulder Knee Hip Back Neck+ANA (Result: Pattern: )+RF (Result: ) High ESR or CRP (Result: )OsteoarthritisLupusRheumatoid arthritisGoutFibromyalgiaLow back painSjogrens syndromeSclerodermaPolymyositis/dermatomyositisVasculitisPlease attach copies of recent labs, xrays, H&P or discharge summary

Results: Diagnoses 53 pts
• 10 wrongfully referred > 12 mos• 5 SLE (5 malar, 2dsDNA, 1 Sm, 3 pred)• 1 ANA(+) arthralgia• 5 RA/inflammatory polyarthritis (1 resolved)• 3 SpA & 1 PsA • 3 PSS and CREST (2 pred, 1 CTX)• 3 Myositis and Myopathy NOS• 3 Osteoarthritis• 5 Fibromyalgia/myofascial pain syndrome• 4 No known dx (dx pending)• 1 each: Urticaria, sialadenitis, drug-induced lupus,
bursitis

Diagnosing Early Arthritis in the CommunityPHD Early Arthritis Campaign (PEAK)
• Why Bother?Why Bother?• Who will benefit?Who will benefit?• Are PCPs and Specialists interested?Are PCPs and Specialists interested?• What do PCPs want?What do PCPs want?• How will it work?How will it work?• Goal: to identify > 90% of new onset RA patients Goal: to identify > 90% of new onset RA patients
in the next year?in the next year?• Cooperating Clinics: Internal medicine, Family Cooperating Clinics: Internal medicine, Family
practice, Emergency Departments, Orthopedics, practice, Emergency Departments, Orthopedics, IM subspecialties, OBGYNIM subspecialties, OBGYN

Multidisciplinary Awareness Campaign
• Goal: increase awareness, facillitate early referral Goal: increase awareness, facillitate early referral diagnosis of serious rheumatic diseasesdiagnosis of serious rheumatic diseases
• Cachement: PHD Community 1 millionCachement: PHD Community 1 million• Outcome: diagnosis of Early RA (N= 40Outcome: diagnosis of Early RA (N= 40 240) 240)• Role Players: Rheums, PR, Marketing, Phone, Role Players: Rheums, PR, Marketing, Phone,
Administration, Managed Care, Study CoordinatorsAdministration, Managed Care, Study Coordinators• Tools: Mailings, Signage, Publications, Local Ad Tools: Mailings, Signage, Publications, Local Ad
Campaign, DTC mailingsCampaign, DTC mailings• Success depends on PCP communitySuccess depends on PCP community

PHD Rheumatologists are Alligned
• Convinced that early diagnosis and early Convinced that early diagnosis and early aggressive Rx will positively impact outcomesaggressive Rx will positively impact outcomes
• Can be accomplished without effecting patient Can be accomplished without effecting patient load/flow. (work smarter, not harder)load/flow. (work smarter, not harder)
• Agree to study this Cooperative Effort Agree to study this Cooperative Effort – Protocol for intake, testing, DMARDs, Data.Protocol for intake, testing, DMARDs, Data.
• Create access to Consultation for PCPs, PatientsCreate access to Consultation for PCPs, Patients– Secondarily educate: facillitate referralsSecondarily educate: facillitate referrals

PCP Misconceptions
• Referrals are easy (how many? How prompt?)Referrals are easy (how many? How prompt?)• Diagnosis can be made by lab tests, xraysDiagnosis can be made by lab tests, xrays• Response to therapy confirms diagnosisResponse to therapy confirms diagnosis• Everyone responds to Steroids or NSAIDsEveryone responds to Steroids or NSAIDs
– Those that don’t cant be helpedThose that don’t cant be helped

Physician Education
• 3 Main Messages3 Main Messages– Rapid easy access to the Rheum of choiceRapid easy access to the Rheum of choice– Prompt appointments with rapid diagnosis Prompt appointments with rapid diagnosis
and treatmentand treatment– Rapid notice of outcome and return of Rapid notice of outcome and return of
patientpatient

• LOVE (Patient Satisfaction)LOVE (Patient Satisfaction)
• MONEY (Arthritis Patients are not time efficient)MONEY (Arthritis Patients are not time efficient)– Time = MoneyTime = Money– Rheumatology = voodoo medicine (ANA1000)Rheumatology = voodoo medicine (ANA1000)
• Access to RheumatologistsAccess to Rheumatologists
Whats the Motivation for PCPs

Physician Education Programs
• PCPs don’t want Rheum EducationPCPs don’t want Rheum Education– They Want Access to RheumatologistsThey Want Access to Rheumatologists
• Dear Dr. Letter: informs of program, remindsDear Dr. Letter: informs of program, reminds• RheumaKNOWLEDGY Cards (Pocket info)RheumaKNOWLEDGY Cards (Pocket info)• Referral Rules CardReferral Rules Card• Broadcast Fax/Frequent NewslettersBroadcast Fax/Frequent Newsletters• Group lunches/breakfasts with RheumsGroup lunches/breakfasts with Rheums
– Invite PCPs, Orthos, NP/PAInvite PCPs, Orthos, NP/PA• CME ForumsCME Forums• BEST: Immediate Feedback on patients referredBEST: Immediate Feedback on patients referred

EAC Models
• EAC Clinic (@PHD Tuesday is Early Arthritis day)EAC Clinic (@PHD Tuesday is Early Arthritis day)• Physician Extender (NP/PA) intake/screening Physician Extender (NP/PA) intake/screening • Prescreen: Chart review, FAX requests, MD to MD Prescreen: Chart review, FAX requests, MD to MD
referralreferral• Flexible Scheduling (promote, hold, fill spots)Flexible Scheduling (promote, hold, fill spots)• Meet and Greet Rapid SlotsMeet and Greet Rapid Slots• Free Arthritis Screening ClinicsFree Arthritis Screening Clinics
• Model Depends on the objective/settingModel Depends on the objective/setting– Private solo, group, multispecialty groupPrivate solo, group, multispecialty group– University, Academic, Clinical TrialsUniversity, Academic, Clinical Trials– Government/MunicipalGovernment/Municipal

Must There be A Patient Focused Effort?
• Most patients don’t seek medical careMost patients don’t seek medical care• Most newly afflicted patients don’t know who to see Most newly afflicted patients don’t know who to see
– PCP, Ortho, GYN, Chiropracter?– PCP, Ortho, GYN, Chiropracter?• Whats a Rheumatologist?Whats a Rheumatologist?
– Purveyor of RumorsPurveyor of Rumors– Specializes in Interior DesignSpecializes in Interior Design
• How will PCP sector perceive a public advertising How will PCP sector perceive a public advertising campaign encouraging new onset joint complaints campaign encouraging new onset joint complaints to see PCP?to see PCP?– To self refer to Early arthritis screening clinics?To self refer to Early arthritis screening clinics?
• Currently: EAC plans to only accept referred ptsCurrently: EAC plans to only accept referred pts

• Goal: increase awareness, facillitate early referral Goal: increase awareness, facillitate early referral diagnosis of serious rheumatic diseasesdiagnosis of serious rheumatic diseases
• Target: Rheums, PCPs, Orthos, OBGYNs, NP, PA, Target: Rheums, PCPs, Orthos, OBGYNs, NP, PA, Chiropractors, Patients, Media, Managed CareChiropractors, Patients, Media, Managed Care
• Cachement: Your Community N = ?Cachement: Your Community N = ?• Outcome: diagnosis & earlier RxOutcome: diagnosis & earlier Rx• Role Players: Rheums, PR, Marketing, Phone, Role Players: Rheums, PR, Marketing, Phone,
Administration, Managed Care, Study CoordinatorsAdministration, Managed Care, Study Coordinators• Tools: Mailings, Signage, Publications, Ad Tools: Mailings, Signage, Publications, Ad
Campaign, DTC mailingsCampaign, DTC mailings• PCP: Dear Dr., Rheum Education, NewlettersPCP: Dear Dr., Rheum Education, Newletters
“If you build it….they will come”

Guidelines for Referral to the Early Arthritis ClinicEmery P, et al. Ann Rheum Dis 2002 61:290-297
Refer when there is clinical suspicion!Refer when there is clinical suspicion!• >> 3 swollen Joints 3 swollen Joints• + MTP/MCP “squeeze test”+ MTP/MCP “squeeze test”• AM stiffness AM stiffness >> 30 minutes 30 minutes• + Rheumatoid factor+ Rheumatoid factor• Elevated ESR or C-Reactive ProteinElevated ESR or C-Reactive Protein
(NSAIDs/Prednisone may obscure findings)
Differential DiagnosisInflammatoryInflammatory• RARA• UPA/USPUPA/USP• Viral arthritisViral arthritis• SpASpA• Crystal arthritisCrystal arthritisAutoimmuneAutoimmune• SLE/UCTDSLE/UCTD• BehcetsBehcets• VasculitisVasculitis• CryoglobulinemiaCryoglobulinemiaNoninflammatoryNoninflammatory• OsteoarthritisOsteoarthritis• HemochromatosisHemochromatosisOthersOthers• Infectious arthritisInfectious arthritis• PMRPMR• SBESBE• Serum sicknessSerum sickness