e-poster06 rusza aimradial20170921 coronary artery fistula
Upload: international-chair-on-interventional-cardiology-and-transradial-approach
Post on 21-Jan-2018
106 views
TRANSCRIPT
Transradial access fortranscatheter coil embolisations
Ruzsa Z., Bárczi Gy., Édes I. F., Molnár L., Becker D., Merkely B.
AimRadial 2017

Disclosures
I have no conflict of interest to declare
R. Vijayvergiya. International Journal of Cardiology, vol. 140, no. 2, pp. e30–e33, 2010

Coronary artery anomalies (CAAs)
• CAAs has a global incidence of 5.64%
- Split RCA: 1.23%
- Ectopic RCA (left sinus): 1.13%
- Fistulas: 0.87%
- Absent left main coronary artery: 0.67%
- Circumflex arising from right sinus: 0.67%
• Incidence of CAA related sudden death is 0.6%
Angelini P., Br Heart J 1992; 68: 601-607

Anomalies of coronary terminationCoronaro-pulmonary fistula
Clinical features & diagnosis
- Stress test: Treadmill, stress echo, scintigraphy
- Imaging: CT-angio, MR angio, angiography
Adult presentation
- Some patients remain asymptomatic
- Reported complications- Heart failure- Angina- Myocardial infarction- Coronary steal- Endocarditis- Dyspnoe
R. Vijayvergiya. International Journal of Cardiology, vol. 140, no. 2, pp. e30–e33, 2010

Coronary fistula Morphology
72% fistulas: large 5 – 20mm diameter 95% single feeding vessel, less tortuous
44% originated from RCA, 56% from LCA
61% drained into RA, 28% into RV, 11% to LV 28% fistulas: small <5mm
88% multiple feeders and more tortuous
88% originated from LCA, 12% from RCA 66% drained into RV, 34% into PA
Pathophysiology Acts like a L-R shunt
Coron-RA or veins (like ASD)
No shunt Coron- LA (like Mitral regurgitation)
Coron-RV (like Aortic regurgitation)
Steal- angina pectoris Proximal coronary ectasia
Endocarditis
Functional significance
Definite signs of fistulous flow-feeding vessel diameter >50% expected diameter
Angiographically prompt visualization of receiving structure with step up in concentration of injected substance
Evidence of volume overload in affected cardiac chambers
Evidence of steal involving myocardial nutrient blood flow

How to measure the functionalsignificance of the shunt in CPF and IMA sidebranch??Coronary Pulmonary shunt
• Ischemia• Treadmill test• Stress Echo• Scintigraphy• PET_CT• Stress MRI• iFR/ FFR /CFR ??• Stress MRI
• Shunt• MRI (Qp/Qs)• Haemodinamic investigation
IMA side branch
• Coronary ischemia• Stress test ???
• Hand grip test ??
• FFR ???

How should I treat coronarypulmonary fistulas??
• Medical treatment• ASA
• Endocarditis prophylaxis
• Surgical closure
• Invasive treatment• Stent graft placement
• Coil embolisation
• Vascular plug

Coil closure- Imaging
• Coronary CT angio helps in detection of the origin
• Coronarography technique– Use large hole guiding catheters with back up support
– Use a guide catheter kept in position by a 0.014-inch guidewire
– Mechanical injector
– Identify receiving chamber or vessel
– Complete visualization of nutrient myocardial branches

Coil closure- coils and microcatheters• Coils:
– Standard coils (0.035-0-052)• Giantuco
• Tornado
– Controlled release coils (0.035)• Jackson and flipper coils
– Micro coils (0.014-0.018)• GDC/ DC coils
• Cook DCS coils
• Microcatheters– 0.018 compatible
• Renegate microcatheter (Boston Sci)
• Progreat (Terumo)
– 0.014 compatible• Finecross
Coil closure- Technical aspects
• Aim for complete occlusion• Many coils may be needed
• Vascular plugs or similar devices in large vessels (>3-4 mm) better
• Vessel access• Plugs or other devices may require large sheaths
• Tortuous routes, acute angles• Soft tip catheters, wide range of curves
• Various wires both soft and stiff
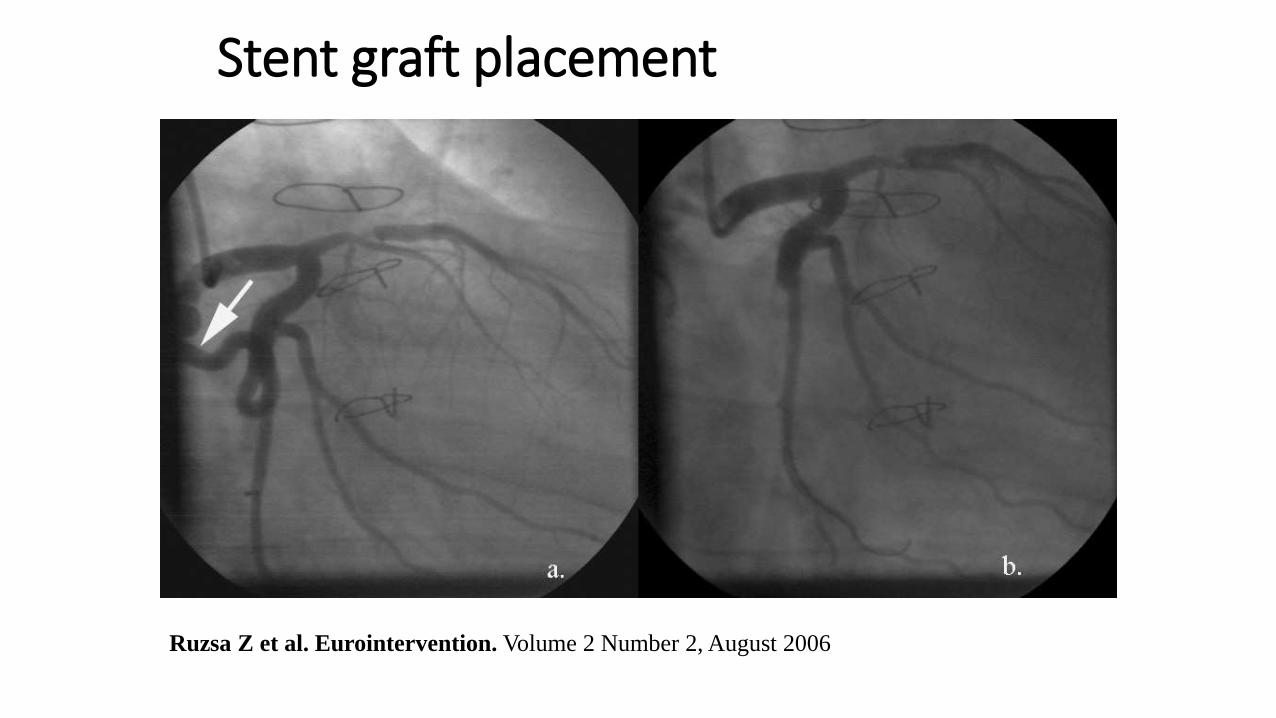
Stent graft placement
Ruzsa Z et al. Eurointervention. Volume 2 Number 2, August 2006

Amplatz vascular plug placement
Larry A. Latson. Catheterization and Cardiovascular Interventions 70:110–116 (2007)

Methods• Retrospective analysis of transcatheter coil embolisations performed
in 11 pts from TR access
• Included patients with angina pectoris, or dyspnoe at stress• and positive Treadmill test and angiographically detected CAF or patent side
branch on the IMA
• with significant shunt on MRI
• Excluded asymptomatic patients or patients with negative stresstest or no significant shunt
• Imaging• Coronary angiography (no ad hoc intervention)
• MRI for shunt detection and LV analysis
• CT angio for shunt anatomical detection

Coil closure- Technique• Access:
– Radial of femoral access 6-7 F sheath
• Guiding: – Appropriate coronary guiding catheter with good back up support– Appropriate projection of coronary anatomy
• Guidewire:– 300 cm long coronary extra support GW– Use buddy wire or 0.018 GW when the microcatheter don’t pass
• Microcatheter– Don’t use diagnostic catheter in coronary arteries only in very proximal fistulas !!!!– Microcatheter size like the coil !!!!
• Balloon: – „temporary ballon occlusion” might be important
• Coiling:– Firstly flush with water !!!– The pusher might have the same size like the microcatheter !!!– First coil placement is crutial– Fill the dilated vessel by using 30% larger coil than the dilated vessel– Other coils same size or smaller until the aneurysm or dilated vessel filled by a nest of
coils– Detachable coils when the distal part is very tortuous and stenosis is present

Angio guided LAD-pulmonary fistula
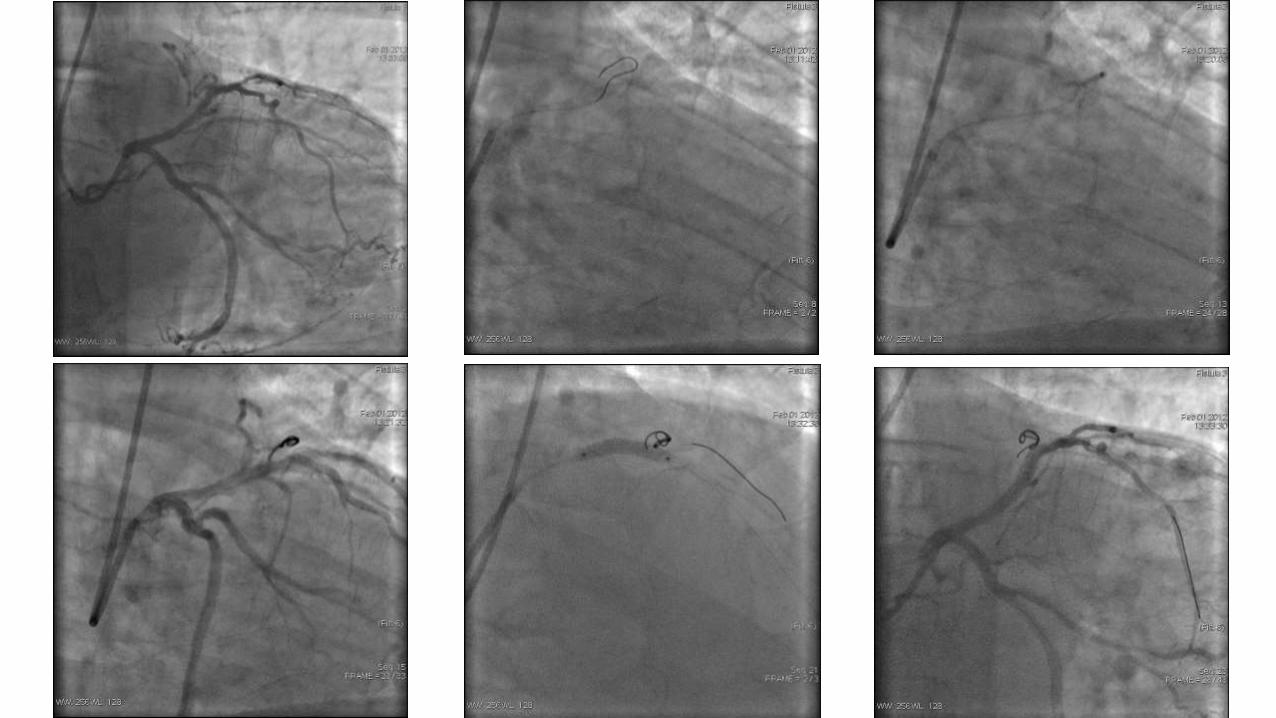


Angio guidedLM-Pulmonary fistula

1. 2. 3.
4. 5. 6.

CT guided CF closure- IM fistula
TCT 2014

Coronaro-pulmonary fistula (left)

Coronaro-pulmonary fistula (right)

Coronaro-pulmonary fistula

IM-Pulmonary fistula


Coronaro-pulmonary fistula (right)

FFR guided CPF closure
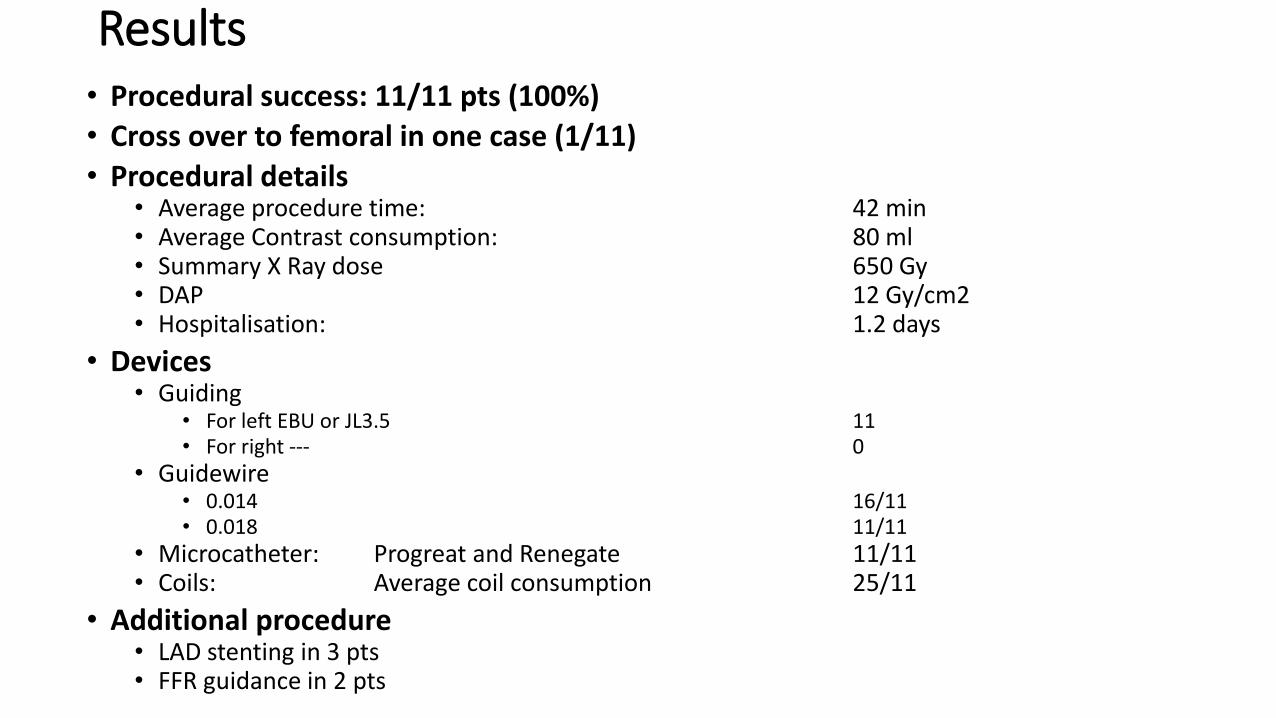
Results• Procedural success: 11/11 pts (100%)
• Cross over to femoral in one case (1/11)
• Procedural details• Average procedure time: 42 min• Average Contrast consumption: 80 ml• Summary X Ray dose 650 Gy• DAP 12 Gy/cm2• Hospitalisation: 1.2 days
• Devices• Guiding
• For left EBU or JL3.5 11• For right --- 0
• Guidewire• 0.014 16/11• 0.018 11/11
• Microcatheter: Progreat and Renegate 11/11• Coils: Average coil consumption 25/11
• Additional procedure• LAD stenting in 3 pts• FFR guidance in 2 pts

Follow up• Symptoms
• 11 asymptomatic patients at 2 months
• In 2 patiens angina and repeat embolisation due to partial recanalisation at 12 months
• Complications• No MACCE at 12 months
• Re-intervention• in 3 pts at 12 months (repeat embolisation)
• In 3 patients potential re-intervention due to multiple fistulas

Conclusion
• Radial access is effective and safe for CPF and IMA sidebranch embolisation
• All patients with angina become symptom free after successful CPF and IMA sidebranch closure
• The indication of the procedure is still not fully clarified
• Wide selection of equipment is needed
• Small fistulas can be closed very easily with coils
• Large fistulas might needs plugs, but it is very rare
• Try to close completly the fistula at first time
• In most cases the long term results are good, but recanalisation rate is 30% afterone year