durability and long-term clinical outcomes of fecal microbiota ...€¦ · preference for fmt as...
TRANSCRIPT
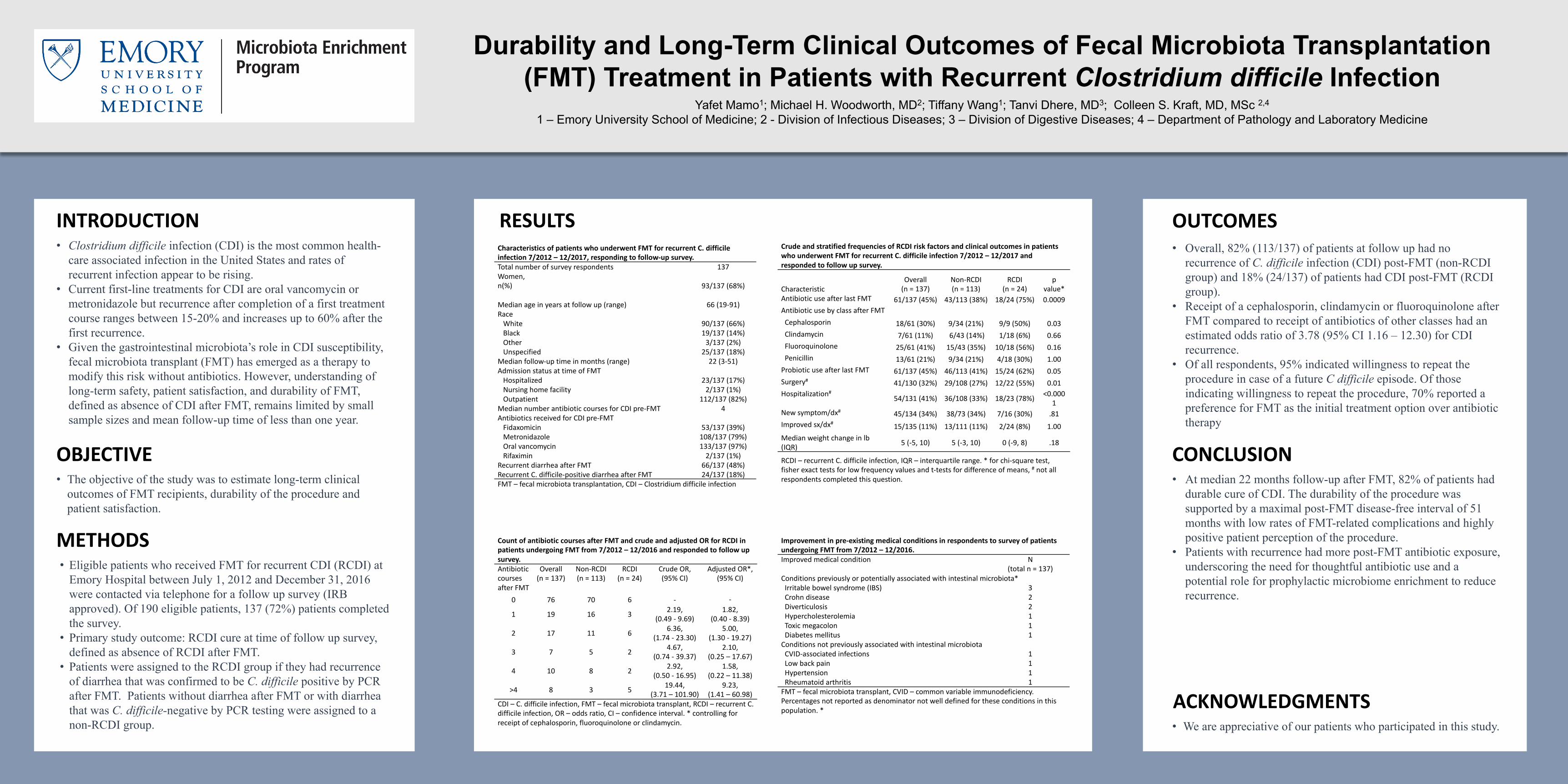
Durability and Long-Term Clinical Outcomes of Fecal Microbiota Transplantation(FMT) Treatment in Patients with Recurrent Clostridium difficile Infection
Yafet Mamo1; Michael H. Woodworth, MD2; Tiffany Wang1; Tanvi Dhere, MD3; Colleen S. Kraft, MD, MSc 2,4
1 – Emory University School of Medicine; 2 - Division of Infectious Diseases; 3 – Division of Digestive Diseases; 4 – Department of Pathology and Laboratory Medicine
• Clostridium difficile infection (CDI) is the most common health-care associated infection in the United States and rates of recurrent infection appear to be rising.
• Current first-line treatments for CDI are oral vancomycin or metronidazole but recurrence after completion of a first treatment course ranges between 15-20% and increases up to 60% after the first recurrence.
• Given the gastrointestinal microbiota’s role in CDI susceptibility, fecal microbiota transplant (FMT) has emerged as a therapy to modify this risk without antibiotics. However, understanding of long-term safety, patient satisfaction, and durability of FMT, defined as absence of CDI after FMT, remains limited by small sample sizes and mean follow-up time of less than one year.
INTRODUCTION
OBJECTIVE• The objective of the study was to estimate long-term clinical
outcomes of FMT recipients, durability of the procedure and patient satisfaction.
METHODS• Eligible patients who received FMT for recurrent CDI (RCDI) at
Emory Hospital between July 1, 2012 and December 31, 2016 were contacted via telephone for a follow up survey (IRB approved). Of 190 eligible patients, 137 (72%) patients completed the survey.
• Primary study outcome: RCDI cure at time of follow up survey, defined as absence of RCDI after FMT.
• Patients were assigned to the RCDI group if they had recurrence of diarrhea that was confirmed to be C. difficile positive by PCR after FMT. Patients without diarrhea after FMT or with diarrhea that was C. difficile-negative by PCR testing were assigned to a non-RCDI group.
• Overall, 82% (113/137) of patients at follow up had no recurrence of C. difficile infection (CDI) post-FMT (non-RCDI group) and 18% (24/137) of patients had CDI post-FMT (RCDI group).
• Receipt of a cephalosporin, clindamycin or fluoroquinolone after FMT compared to receipt of antibiotics of other classes had an estimated odds ratio of 3.78 (95% CI 1.16 – 12.30) for CDI recurrence.
• Of all respondents, 95% indicated willingness to repeat the procedure in case of a future C difficile episode. Of those indicating willingness to repeat the procedure, 70% reported a preference for FMT as the initial treatment option over antibiotic therapy
OUTCOMES
CONCLUSION• At median 22 months follow-up after FMT, 82% of patients had
durable cure of CDI. The durability of the procedure was supported by a maximal post-FMT disease-free interval of 51 months with low rates of FMT-related complications and highly positive patient perception of the procedure.
• Patients with recurrence had more post-FMT antibiotic exposure, underscoring the need for thoughtful antibiotic use and a potential role for prophylactic microbiome enrichment to reduce recurrence.
ACKNOWLEDGMENTS• We are appreciative of our patients who participated in this study.
CharacteristicsofpatientswhounderwentFMTforrecurrentC.difficileinfection7/2012– 12/2017,respondingtofollow-upsurvey.Totalnumberofsurveyrespondents 137Women,n(%) 93/137(68%)
Medianageinyearsatfollowup (range) 66(19-91)RaceWhite 90/137(66%)Black 19/137(14%)Other 3/137(2%)Unspecified 25/137(18%)
Medianfollow-uptimeinmonths(range) 22(3-51)AdmissionstatusattimeofFMTHospitalized 23/137(17%)Nursinghomefacility 2/137(1%)Outpatient 112/137(82%)
MediannumberantibioticcoursesforCDIpre-FMT 4AntibioticsreceivedforCDIpre-FMTFidaxomicin 53/137(39%)Metronidazole 108/137(79%)Oralvancomycin 133/137(97%)Rifaximin 2/137(1%)
RecurrentdiarrheaafterFMT 66/137(48%)RecurrentC.difficile-positivediarrheaafterFMT 24/137(18%)FMT– fecalmicrobiotatransplantation,CDI– Clostridiumdifficileinfection
RESULTSCrudeandstratifiedfrequenciesofRCDIriskfactorsandclinicaloutcomesinpatientswhounderwentFMTforrecurrentC.difficileinfection7/2012– 12/2017andrespondedtofollowupsurvey.
CharacteristicOverall(n=137)
Non-RCDI(n=113)
RCDI(n=24)
pvalue*
AntibioticuseafterlastFMT 61/137(45%) 43/113(38%) 18/24(75%) 0.0009AntibioticusebyclassafterFMTCephalosporin 18/61(30%) 9/34(21%) 9/9(50%) 0.03Clindamycin 7/61(11%) 6/43(14%) 1/18(6%) 0.66Fluoroquinolone 25/61(41%) 15/43(35%) 10/18(56%) 0.16Penicillin 13/61(21%) 9/34(21%) 4/18(30%) 1.00ProbioticuseafterlastFMT 61/137(45%) 46/113(41%) 15/24(62%) 0.05Surgery# 41/130(32%) 29/108(27%) 12/22(55%) 0.01Hospitalization# 54/131(41%) 36/108(33%) 18/23(78%) <0.000
1Newsymptom/dx# 45/134(34%) 38/73(34%) 7/16(30%) .81Improvedsx/dx# 15/135(11%) 13/111(11%) 2/24(8%) 1.00Medianweightchangeinlb(IQR) 5(-5,10) 5(-3,10) 0(-9,8) .18
RCDI– recurrentC.difficileinfection,IQR– interquartilerange.*forchi-squaretest,fisherexacttestsforlowfrequencyvaluesandt-testsfordifferenceofmeans,# notallrespondentscompletedthisquestion.
CountofantibioticcoursesafterFMTandcrudeandadjustedORforRCDIinpatientsundergoingFMTfrom7/2012– 12/2016andrespondedtofollowupsurvey.AntibioticcoursesafterFMT
Overall(n=137)
Non-RCDI(n=113)
RCDI(n=24)
CrudeOR,(95%CI)
AdjustedOR*,(95%CI)
0 76 70 6 - -
1 19 16 3 2.19,(0.49- 9.69)
1.82,(0.40- 8.39)
2 17 11 6 6.36,(1.74- 23.30)
5.00,(1.30- 19.27)
3 7 5 2 4.67,(0.74- 39.37)
2.10,(0.25– 17.67)
4 10 8 2 2.92,(0.50- 16.95)
1.58,(0.22– 11.38)
>4 8 3 5 19.44,(3.71– 101.90)
9.23,(1.41– 60.98)
CDI– C.difficileinfection,FMT– fecalmicrobiotatransplant,RCDI– recurrentC.difficileinfection,OR– oddsratio,CI– confidenceinterval.*controllingforreceiptofcephalosporin,fluoroquinoloneorclindamycin.
Improvementinpre-existingmedicalconditionsinrespondentstosurveyofpatientsundergoingFMTfrom7/2012– 12/2016.Improvedmedicalcondition N
(totaln=137)Conditionspreviouslyorpotentiallyassociatedwithintestinalmicrobiota*Irritablebowelsyndrome(IBS) 3Crohndisease 2Diverticulosis 2Hypercholesterolemia 1Toxicmegacolon 1Diabetesmellitus 1ConditionsnotpreviouslyassociatedwithintestinalmicrobiotaCVID-associatedinfections 1Lowbackpain 1Hypertension 1Rheumatoidarthritis 1FMT– fecalmicrobiotatransplant,CVID– commonvariableimmunodeficiency.Percentagesnotreportedasdenominatornotwelldefinedfortheseconditionsinthispopulation.*