dsrip meeting agenda - nyp.org · 2017-09-19 · dsrip meeting agenda page 1 date & time 8/18...
TRANSCRIPT
DSRIP Meeting Agenda
PAGE 1
Date & Time 8/18/17 @ 9:00 – 10:00AM Meeting Title IT – Clinical Operations Committee
Location NYP Milstein Heart Center Room 4
Facilitator Alvin Lin & Elaine Fleck
Go to Meeting https://global.gotomeeting.com/join/676507237
Conference Line Dial +1 (408) 650-3123 Access Code: 676-507-237
Invitees
Chair: Elaine Fleck (NYP) Chair: Alvin Lin (NYC DOHMH PCIP/REACH)
Gil Kuperman (NYP) Terri Udolf (St. Christopher’s Inn)
Alissa Wassung (God’s Love We Deliver) Sandy Merlino (VNSNY)
Susan Wiviott (The Bridge) Amy Shah (NYC DOHMH)
David Chan (City Drug & Surgical) Maria Lizardo (Northern Manhattan Improvement Corp.)
Jean Marie Bradford, MD (NYPSI) Catherine Thurston (SPOP)
Genevieve Castillo (Methodist) Stuart Myer (VillageCare)
Dan Johansson (ACMH, Inc.) Renato Leonel (Isabella)
Julissa Nunez (VNSNY) Mitze Amoroso (ArchCare)
Theo Figurasin (NYSNA) Todd Rogow (Healthix)
Steven Lam (CBWCHC) Priscilla Pena (1199 SEIU)
Andres Pereira, MD Patricia Hernandez (NYP)
Nelson Mesa (NYP) Andrew Missel (NYP)
Isaac Kastenbaum (NYP) Rachel Naiukow (NYP)
Meeting Objectives Facilitator Time Start End
Welcome & Roll Call Alvin Lin 5 min 9:00 9:05
Vision for the Committee & Review Updated Performance Data Formats
Elaine Fleck, Alvin Lin
10 min 9:05 9:15
Adult Medicine Quality Improvement Population Line Presentation
Elaine Fleck 30 min 9:15 9:45
Workforce Training & Development
Proposed Training Evaluation Plan Rachel Niaukow 10 min 9:45 9:55
Next Steps Andrew Missel 5 min 9:55 10:00
Action Items
Description Owner Start Date Due Date Status
Present draft integrated committee charter Co-Leads /
Andrew Missel 4/21/17 TBD Not Started

Committee Outlook & ApproachIT/Clinical Operations
Governance Committee
August 18, 2017
1

Agenda for 8/18/2017
Meeting Objectives Facilitator Time Start EndWelcome & Roll Call Alvin Lin 5 min 9:00 9:05
Vision for the Committee & Review Updated Performance Data Formats
Elaine Fleck, Alvin Lin
10 min 9:05 9:15
Adult Medicine Quality Improvement Population Line Presentation
Elaine Fleck 30 min 9:15 9:45
Workforce Training & Development• Proposed Training Evaluation Plan
Rachel Niaukow 10 min 9:45 9:55
Next Steps Andrew Missel 5 min 9:55 10:00
2

Vision: Shift to Pay for Performance (P4P)
Through DSRIP, NYS has prioritized restructuring a healthcare delivery
system to reduce avoidable hospital use by 25% over 5 years. By
increasing quality of care and collaboration, the system can transform to
decrease avoidable costs.
3
DSRIP goals have shifted from infrastructure to driving performance
Pay for Reporting (P4R)
PPS can earn incentive payment for successfully reporting measures
to NYS DOH within the timeframes for each measurement year.
Pay for Performance (P4P)
PPS will receive achievement values for results that meet or exceed
the annual improvement target.
DRAFT

Catalyst for Change: Shift to Pay-for-Performance
4
Note: As part of a December 2015 waiver amendment request to the federal Centers for Medicare and Medicaid Services, New York is seeking to slightly modify these percentages.
Source: New York State Department of Health, Attachment I—NY DSRIP Program Funding and Mechanics Protocol, April 2014.
15%
45%
65%
85%
20%
25%
15%
15%
15%
80%
60%
40%
20%
DSRIP Year 1 DSRIP Year 2 DSRIP Year 3 DSRIP Year 4 DSRIP Year 5
Project progress milestones Pay-for-reporting Pay-for-performance
We are here
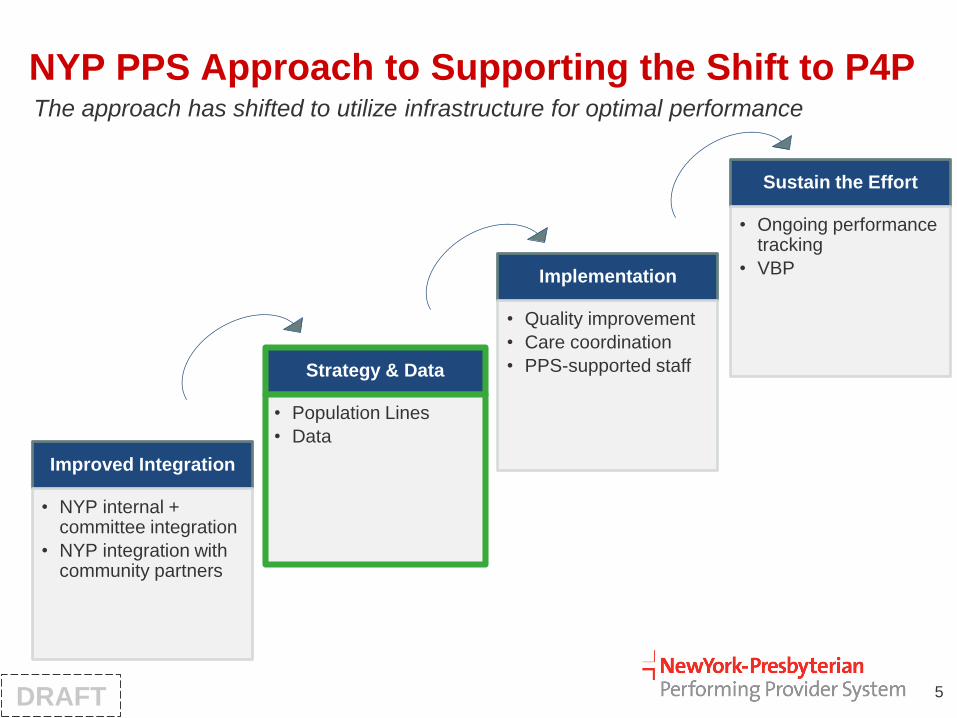
NYP PPS Approach to Supporting the Shift to P4P
Improved Integration
• NYP internal + committee integration
• NYP integration with community partners
Strategy & Data
• Population Lines
• Data
Implementation
• Quality improvement
• Care coordination
• PPS-supported staff
Sustain the Effort
• Ongoing performance tracking
• VBP
5
The approach has shifted to utilize infrastructure for optimal performance
DRAFT

Focusing on Data and Overview of Measures
6
Simplifying the data is key to reducing the noise and meeting performance goals
CategoryOn-Track to Meet
MY3 TargetMetric Name
Yes Adults w/ Preventive or Ambulatory Care Visit in Last Year - 65 and older
Yes Chlamydia Screening (16 - 24 Years)
No Adults w/ Preventive or Ambulatory Care Visit in Last Year - 20 to 44 years
No Adults w/ Preventive or Ambulatory Care Visit in Last Year - 45 to 64 years
No Cervical Cancer Screening
Yes Antidepressant Medication Management - Effective Acute Phase Treatment
Yes Antidepressant Medication Management - Effective Continuation Phase Treatment
Yes Diabetes Monitoring (Both LDL-C Test & HbA1c Test) for People with Diabetes and Schizophrenia
Yes Engagement of Alcohol and Other Drug Dependence Treatment (Initiation and 2 visits within 44 days)
Yes Follow-Up after Hospitalization for Mental Illness - Within 30 Days
Yes Follow-Up after Hospitalization for Mental Illness - Within 7 Days
Yes Follow-up care for Children Prescribed ADHD Medications - Continuation Phase*
Yes Follow-up care for Children Prescribed ADHD Medications - Initiation Phase
No Adherence to Antipsychotic Medications for People with Schizophrenia
No Cardiovascular Monitoring (LDL-C Test) for People with Cardiovascular Disease and Schizophrenia*
No Diabetes Screening for People with Schizophrenia or Bipolar Disease who are Using Antipsychotic Medication
No Initiation of Alcohol and Other Drug Dependence Treatment (1 visit within 14 days)
Yes Children w/ PCP Visit in the Last Year - 12 to 24 months
No Children w/ PCP Visit in the Last Year - 25 months to 6 years
No Children w/ PCP Visit in the Last Year (or Prior Year) - 12 to 19 years
No Children w/ PCP Visit in the Last Year (or Prior Year) - 7 to 11 years
Yes HIV/AIDS Comprehensive Care - Syphilis Screening
No HIV/AIDS Comprehensive Care - Engaged in Care
No HIV/AIDS Comprehensive Care - Viral Load Monitoring
Yes Potentially Avoidable Readmissions
Yes Potentially Preventable Admissions - Adults (PQI 90)
Yes Potentially Preventable Admissions - Children (PDI 90)
No Potentially Preventable Emergency Room Visits
No Potentially Preventable Emergency Room Visits (for Persons with BH Diagnosis)
Adult Preventive
Behavioral Health
Pediatric Preventive
Sexual Health
Utilization
DRAFT

Potentially Preventable ED Visits for Patients with Behavioral Health Diagnoses (All Ages)
7
MetricUnit of
MeasurementMY3 Goal
CurrentPerformance(Dec. 2016)
Gap to CloseOn-Track to Meet MY3
Target?
Potentially Preventable ED Visits (Pts w/ Behavioral Health Diagnoses)
Rate per 100 People
3,022 visits (rate = 74.77)
3,628 visits(rate = 89.76)
606 visits (rate = 14.99)
No
Data are current as of: 12/31/2016.
Source: NYS (MAPP), accessed 08/09/2017.
PPS Hub # Pts in Denom.# Preventable
ED VisitsMeasure Result
ED Not In Network 1,746 1,648 94.39No MC PCP Assigned 976 1,107 113.42NYP West Campus 876 657 75.00NYP East Campus 176 124 70.45Charles B Wang CHC 143 12 8.39
Key Take-Aways:
1. To meet its annual target, NYP PPS must have prevented 606 unnecessary ED visits for
people with behavioral health diagnoses.
2. 43% (1,746/4,402) of people in this metric use EDs not associated with the NYP PPS
network, and an additional 24% (976/4,042) do not have a managed care assigned PCP.
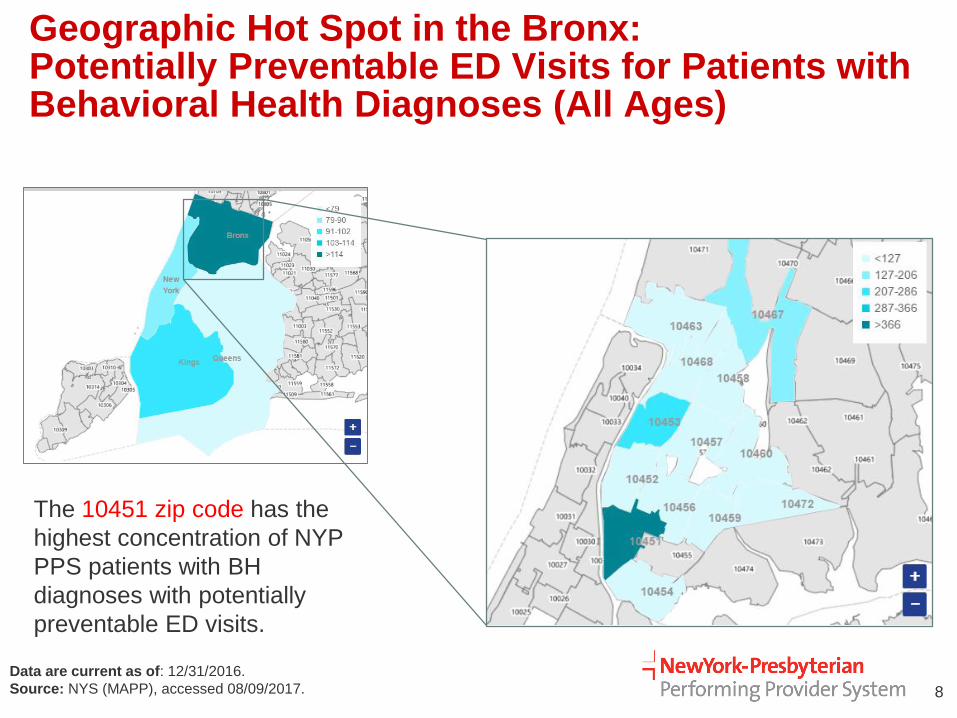
Geographic Hot Spot in the Bronx: Potentially Preventable ED Visits for Patients with Behavioral Health Diagnoses (All Ages)
8
Data are current as of: 12/31/2016.
Source: NYS (MAPP), accessed 08/09/2017.
The 10451 zip code has the
highest concentration of NYP
PPS patients with BH
diagnoses with potentially
preventable ED visits.

Example: Drill Down on Individual Measures
9
79.64
77.6 77.23 77.73 77.9579.16
80.72
77.6 77.98
82.12 81.81
89.76
74.77
70.00
75.00
80.00
85.00
90.00
Jan '16 Feb '16 Mar '16 Apr '16 May '16 Jun '16 Jul '16 Aug '16 Sep '16 Oct '16 Nov '16 Dec '16
Rat
e o
f P
PV
-BH
Month, YearMonthly Result Target
Performance on Potentially Preventable ED Visits for Patients with BH Diagnoses
Sources: NYS (MAPP), accessed 8/17/2017.
Adult Population Line to address why metric
performance has not improved and to guide strategy
to meet or exceed target.
Desired direction of change =
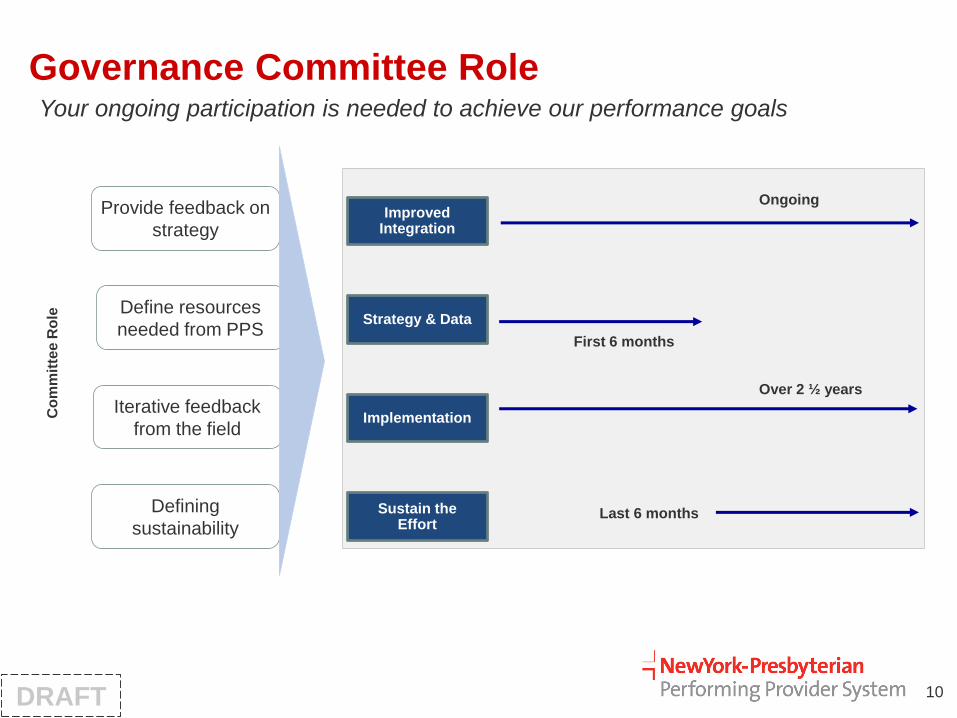
Governance Committee Role
10
Your ongoing participation is needed to achieve our performance goals
Improved Integration
Strategy & Data
Implementation
Sustain the Effort
Ongoing
First 6 months
Over 2 ½ years
Last 6 months
Co
mm
itte
e R
ole
Provide feedback on
strategy
Define resources
needed from PPS
Iterative feedback
from the field
Defining
sustainability
DRAFT

Discussion & Feedback
1. Any general feedback on shifting to the new phased approach?
2. How will data simplification enable you to drive success across
practices?
11
NYP PPS Workforce Development & Training Resources
Rachel Naiukow
Program Coordinator
Division of Community & Population Health
NewYork-Presbyterian Hospital

Objectives
• Introduce new Workforce webpage
• Overview of new training resources and existing training
• Review opportunities for engagement and new training evaluation strategy

Workforce Webpage
• http://www.nyp.org/pps/resources/workforce-development
• NYP PPS Training Center
• Other Training & Resources
• Job Board
• Workforce Strategy
• Training Request Form
Training Resources
• NYP PPS Training Center
• Course information on webpage
• Additional courses coming soon

Training Resources
• Other Training and Workforce Resources
• Center to Advance Palliative Care (CAPC) membership• FREE CMEs/CEUs!!!
• CAPC Designations
• And more…
• Quality Interactions Resource Center• Resource center
• Cross-Cultural Care course
• Training demos
Opportunities for engagement
• Training request form
• Open call for training and workforce resources to share
• Engaging collaborator leaders as trainers
• Training evaluations: 30-day post-training interviews

Training evaluations: 30-day post-training interviews
• Goals:• Meaningful, qualitative feedback
• Capturing impact on care delivery and/or operations
Previous Post-Training Survey Questions
• Did you find this webinar to be helpful and relevant to your current work?
• Did you gain or learn something that you could realistically utilize and implement in your current work?
• Please rate how likely you are to utilize the skills and techniques presented in the webinar in your daily work. (1-5)
• On a scale of 1 to 5, 5 being the being the highest and 1 being the lowest, how satisfied are you with this presentation?
• What topics would you like to see covered in future trainings?

Questions
• Does the timeframe make sense for follow up regarding “impact”?
• Are there any quantitative measures that can and should be collected in this engagement?
• Is this strategy reasonable to capture outcomes?
