drug use in pregnancy - prince of songkla...
TRANSCRIPT

Drug use in pregnancy
ผศ.พญ. ธารางรัตน หาญประเสริฐพงษหนวยเวชศาสตรมารดาและทารกในครรภ
ภาควิชาสูติศาสตรนรีเวชวิทยามหาวิทยาลัยสงขลานครินทร

Thalidomide
Anxiolytic and sedative drugMesoderm layers, such as limbs, ear,
cardiovascular system and bowel musculatureAbnormal shape or size to total absence of
a bone or limb segment (phocomelia)

Thalidomide
Upper limb phocomelia days 27-30Lower lime phocomeloa days 30-33Gallbladder aplasia days 42-43Duodenal atresia days 40-47
Thalidomide
Effective for cutaneuos lupus erythematosus, chronic graft versus-host disease, etcTwo highly effective forms of birth
control


Alcohol
Most frequent nongenetic causes of mental retardationLeading cause of preventable birth
defects

Fetal alcohol syndrome Diagnostic
criteria- all required
Dysmorphic facial features- Small palpebral fissure- Thin vermilion border- Smooth philtrum Prenatal and/or postnatal growth impairment Central nervous system abnormalities- Structural: head size<10th percentile, significant brain abnormality
on imaging- Neurological- Functional: global cognitive or intellectual deficits, functional
deficits in at least three domains
Alcohol-related birth defects
Cardiac: ASD, VSD, aberrant great vessels, conotruncal heart defectsSkeletal: radioulnar synostosis, vertebral
segmentation defect, joint contractures, scoliosisRenal: aplastic or hypoplastic kidneys,
dysplastic kidneys, horseshoe kidney, ureteralduplication

Alcohol-related birth defects
Eyes: strabismus, ptosis, retinal vascular abnormalities, optic nerve hypoplasiaEars: conductive or neurosensory hearing lossMinor: hypoplastic nails, clinodactyly, ‘hockey
stick’ palmar creases, refractive errors, ‘railroad track’ ears


Dose effect
No minimal amountBinge drinking: increased risk of
stillbirth


Tetracycline
May cause yellow-brown discoloration of deciduous teethDeposit in fetal long bonesUsed after 25 weeksNot increase risk of dental cariesAcceptable use: maternal syphilis in penicillin-
allergic women

Teratogens
Any agent- chemicals, viruses, environmental agents, physical factors, and drugsActs during embryonic or fetal development
to produce a permanent alteration of form or function

Criteria for proof of human teratogenicity
Careful delineation of clinical casesRare environmental exposure associated
with rare defect, with at least three reported cases-easiest if defect is severeProof that the agent acts on the embryo or
fetus, directly or indirectly

Criteria for proof of human teratogenicity
Proven exposure to agent at critical time (s) in prenatal developmentThe association must be biologically
plausibleTeratogenicity in experimental animals,
especially primates
Criteria for proof of human teratogenicity
Consistent finding by two or more epidemiological studies of high quality:
a) Control of confounding factorsb) Sufficient numbersc) Exclusion if positive and negative bias factorsd) Prospective studies, if possiblee) Relative risk of three or more


Critical developmental period
Pre-implantation: ALL OR NONEEmbryonic: 2nd-8th week‘most critical structural malformation’Fetal period: after 8th week

Counseling for teratogen exposure
Nature of exposure: length, dosage and timing of exposureOther exposure: alcohol, cigarette

Counseling for teratogen exposure
Background human baseline risk for major malformationsAnomaly associated with the agent in
questionRisk assessmentMethods of prenatal detection
Counseling for teratogen exposure
Limitations in our knowledgeLimitations of prenatal diagnostic capabilitiesPotential risk of medical condition for which a
drug is prescribesDisease state and the pregnancy and
preventive measures

Physiologic changes in pregnancy
Alteration in blood volumePlasma proteinsGastric emptying time that affect
dosing and distribution of drugsIncrease and some decrease in both
hepatic and renal elimination process

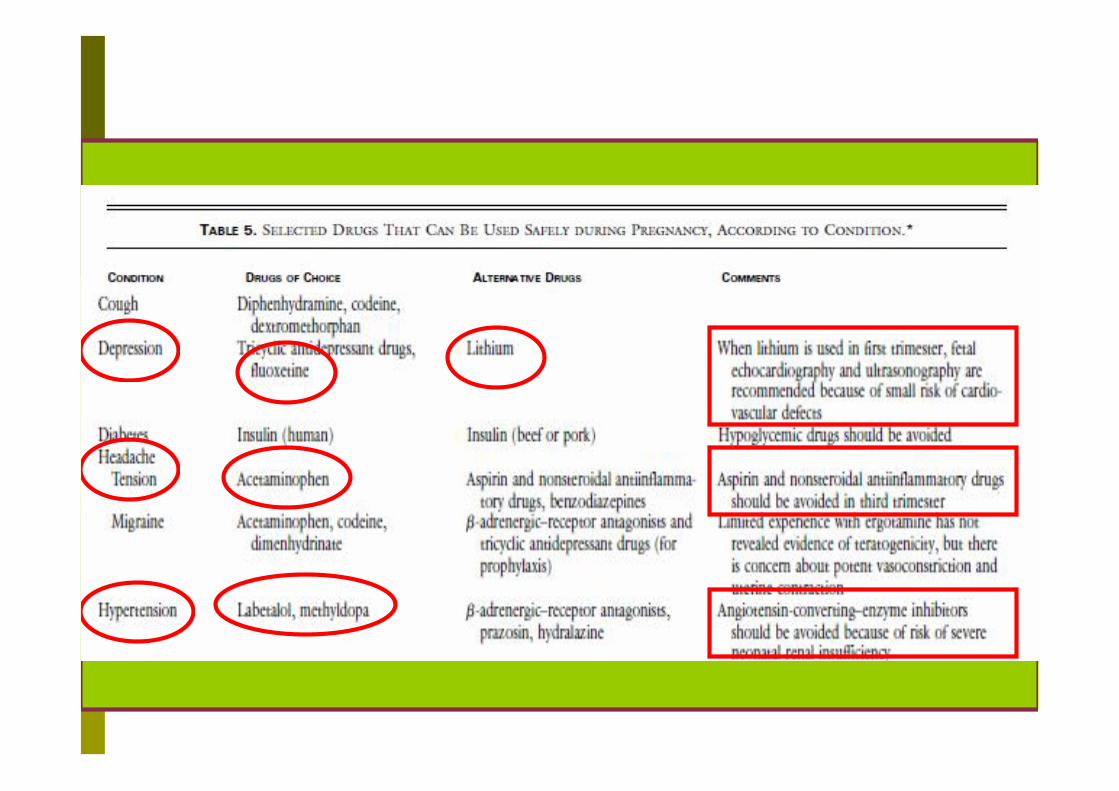
Decision of prescription
‘Does the benefit of the drug outweigh its risk’Consideration of factors:-gestational age-route of drug administration-drug crosses the placenta or excreted in breast milk-Molecular weight of the drugs-monotherapy or multiple drug

Common medication Antihypertensive Anticonvulsant Antifungal Anti-
inflammatory antimalaria
AntimicrobialAntineoplasticAntiviralVitamin Awarfarin


Angiotensin-converting enzyme inhibitors and angiotensin-receptor blocker
Disrupt the fetal renin-angiotensin systemFetal hypotension, hypoperfusionRenal ischemia, renal tubular dysgenesis and anuriaPrevent lung development and limb contracturesOccur after organogenesis
ACE INHIBITOR FETOPATHY

Anticonvulsant
epilepsy increases risk of fetal malformationMore prevalent with need for
multiple medication


Fetal hydantoin syndrome
upturned noseMid facial hypoplasiaLong upper lip with thin vermillion borderLower distal digital hypoplasiaPhenytoin (D) Carbamazepine (D)


Valproate (D)
neural tube defect, clefts, skeletal abnormalities, developmental delay1-2% with monotherapy9-12% with polytherapy



Antimicrobial
AmnioglycosidesChloramphenicolSulfonamideTetracycline

Amnioglycosides
using lower divided dosesNephrotoxicity and ototoxicityNot confirmed in prenatal exposure

Chloramphenicol
cross placentaNot increase congenital anomaliespretermCyanosis, vascular collapse,
hypotension and death

Sulfonamides
Cross placentaNot increase congenital anomaliesPreterm: hyperbilirubinemia if used
near delivery
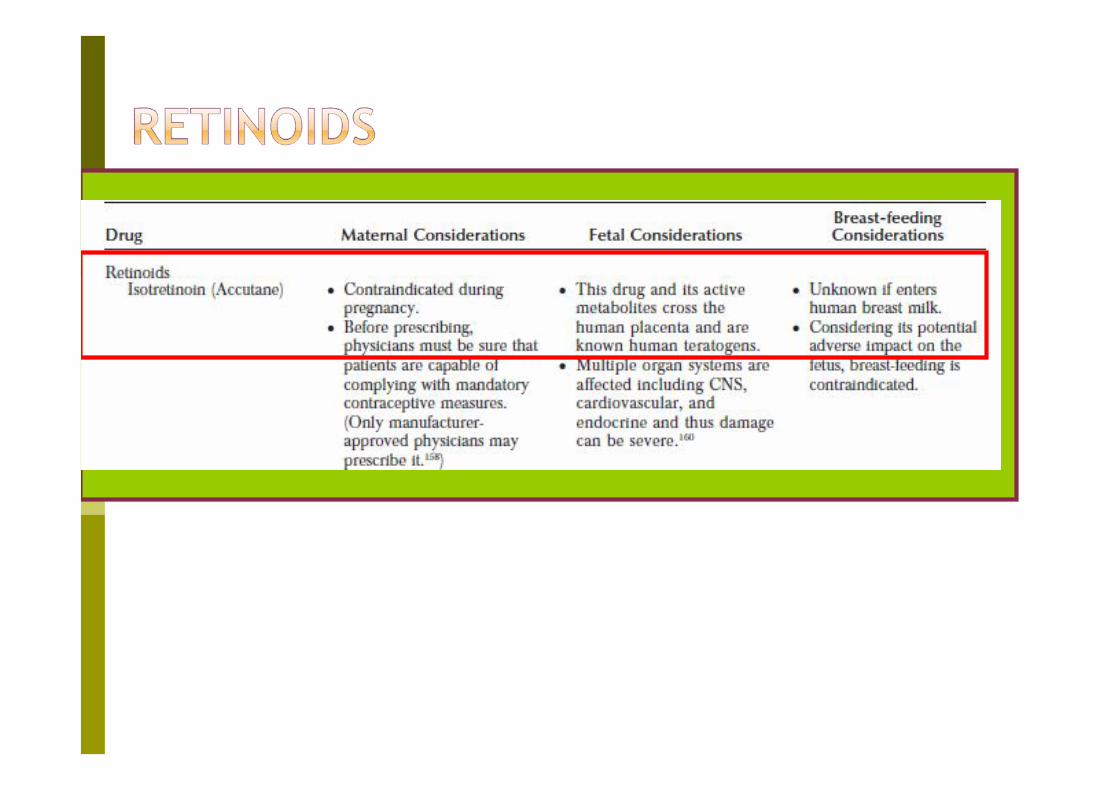

Isotretinoin (X)
Most potent teratogensMean serum half-life 12 hoursNot increase anomalies if discontinue
before conceptionCranium, face, heart, cardiovascular and
thymus




Hormone
androgenic progestins: Virilization of female fetuses and
feminization of male fetusesEstrogens: no association with congenital anomalies

หัวขอ: แมรองแพทยราชวิถีประมาทใหยากอนต้ังครรภ สงผลลูกพิการ เริ่มหัวขอโดย: Memory ท่ี มกราคม 20, 2010, 01:29:17 PM
เพ่ือนๆ นาจะไดยินขาวน้ีแลว อานแลวคิดยังงัย แลวเรานาจะมีบทบาทอะไรบางตอการเกิดลดอุบัติการณในเรื่องน้ี
น.ส.ภิญญามาศ โยธี นํา ด.ช.เชาวรินทร อองประเสริฐ หรือนองแชมป บุตรชายวัย 1 ขวบ 5 เดือน พรอมทนายความเครือขายผูเสียหายทางการแพทย เขาแจงความกับพนักงานสอบสวน สน.พญาไท ใหดําเนินคดีกับแพทยโรงพยาบาลราชวิถี 2 คน ฐานประมาทในการรักษาพยาบาล จนเปนเหตุใหบุตรชายพิการตลอดชีวิต
น.ส.ภิญญามาศ กลาววา ตนมีโรคประจําตัวลิ่มเลือดอุดตันท่ีขาขางซาย โดยใชสิทธิ์ประกันสังคมรักษาท่ีโรงพยาบาลมิชช่ัน ซึ่งแพทยรักษาดวยการใหกินยาวอรฟาริน กอนหนาตั้งครรภชวงป 2550 ประมาณ 8 เดือน แพทยไดสงตัวมารักษาตอท่ีโรงพยาบาลราชวิถ ีและใชสิทธิ์ 30 บาท พรอมแนะใหเปลี่ยนมาฉีดยาแทน เพราะยาชนิดน้ีอาจเปนอันตรายตอทารก แตแพทยโรงพยาบาลราชวิถีกลับรักษาโดยใหกินยาอยางเดิม โดยใหเหตุผลวา อายุครรภเกิน 5 เดือน เด็กสรางอวัยวะครบแลว จึงไมมีผลกระทบ แตเมื่อถึงกําหนดคลอดกลับพบวา เด็กหายใจเองไมได ตองใสเครื่องชวยหายใจ กะโหลกปดไมสนิท เลือดออกท่ีเน้ือสมอง และเน้ือสมองเหลือนอยมาก ปจจุบันตามองไมเห็น และหูไมไดยิน 1 ขาง รวมท้ังไมมีพัฒนาการใดๆ โดยกอนหนาน้ี ไดเขารองเรียนท่ีแพทยสภา และสํานักงานผูตรวจการแผนดินแลว แตยังไมคืบหนา
โดย ASTVผูจัดการออนไลน 16 ธันวาคม 2552 12:41 น.

Warfarin (D)
Embryopathy: nasal and midfacehypoplasia, stippled vertebral and femoral epiphyses (at least 5 mg/day)2nd and 3rd trimester: hemorrhage leading
to disharmonic growth and deformation from scarring in any of several organs


Warfarin (D)
9% permanent deformity or disability17% fetal death











prescribe a drug for a pregnant or breast-feeding woman?
Consideration of many factorsGestational ageRoute of drug administrationAbsorption rate of the drugcrosses the placenta or excreted in breast milk Dose of the drugMolecular weight of the drugMonotherapy or multiple drugs


Does the benefit of the Does the benefit of the drug outweigh its riskdrug outweigh its risk
????????????????

Reference
www.teratology.orgwww.safefetus.com


