drug prescribing for the elderly
TRANSCRIPT
GERIATRIC MEDICINE
Drug Prescribing for the ElderlyJOSEPH G. OUSLANDER, MD, Los Angeles
Age-related biologic and physiologic changes, the accumulation of multiplepathologic conditions with increasing age and several socioeconomic consid-erations combine to make drug prescribing for the elderly one of the mostchallenging tasks in clinical medicine. Numerous studies in older persons havedocumented alterations in the pharmacology of many drugs. Several generalrecommendations are presented which should make drug prescribing forelderly patients safer and more effective.
PRESCRIPTION MEDICATIONS represent a substan-tial portion of this country's ever-growing healthcare expenditures. They are not covered by manyinsurance plans for the elderly, and this can causeconsiderable out-of-pocket expense from what isoften a fixed and limited income.
It is not unusual that several different drugs areprescribed for an elderly patient, to be taken oncomplex dosage schedules. This is especially soin acute care hospitals, where Medicare patientsreceive an average of ten prescription drugs,' andin nursing homes, where many of the four to sevendrugs prescribed for each patient are inappropriateor ineffective.2
Drugs are a major cause of iatrogenic illnesses,conditions which are disturbingly common.3'4 Onerecent study found an iatrogenic illness in morethan a third of patients on the medical service ofa university hospital,4 and drugs were one of themost important factors in the development of thesecomplications. Older persons are particularly sus-ceptible to adverse drug reactions; the incidenceof adverse reactions in hospitals increases from
Refer to: Ouslander JG: Drug prescribing for the elderly, InGeriatric Medicine. West J Med 135:455-462, Dec 1981
Dr. Ouslander is Adjunct Assistant Professor of Medicine, De-partment of Medicine, a Fellow in Geriatric Medicine, UCLAMulticampos Division of Geriatric Medicine, Department ofMedicine, UCLA School of Medicine, and is affilated with theGeriatric Research, Education, and Clinical Center, SepulvedaVeterans Administration Medical Center, Sepulveda, California.
Reprint requests to: Joseph G. Ouslander, MD, GRECC 1 1E,Sepulveda VA Medical Center, Sepulveda, CA 91343.
3 percent in those aged 10 to 305 to close to 25percent in those older than age 80.X; Thesereactions contribute to more than 10 percent ofadmissions to geriatric departments in Great Brit-ain,7 and account for as many as 3 percent of alladmissions to US hospitals.8 As much as $3 billionper year may be spent in this country as a resultof adverse drug reactions.2
Given these costs, in both health and dollars,physicians should become aware of some of thecomplex considerations that attend prescribingfor the elderly. Age-related biologic and physio-logic changes, the accumulation of multiple patho-logic conditions with increasing age and severalsocioeconomic factors combine to make prescrib-ing drugs one of the most difficult, yet challenging,aspects of caring for these patients.
This article will briefly review age-relatedchanges that are relevant to drug prescribing, andmake several recommendations which are designedto make treatment of the elderly with drugs saferand more effective.
Age-Related Changes Relevant toDrug PrescribingAltered Reporting and Presentation of Illness
Altered reporting and presentation of illnesscan make accurate diagnosis, and therefore ap-propriate drug prescription, more difficult in
THE WESTERN JOURNAL OF MEDICINE 455

elderly patients. Impairments of hearing andvision, dementia and depression can all compro-mise a patient's ability to communicate symptoms.Vague and multiple somatic symptoms, extremelycommon in the elderly, often represent psychicdistress rather than physical illness.9 Interpreta-tion of these symptoms for physical illness, orexacerbation of an underlying medical condition,can result in inappropriate drug treatment.
Even when physical illnesses are present, theymay be difficult to diagnose. Confusion, falls andurinary incontinence may be the presenting mani-festations of a variety of treatable disorders; con-ditions such as hyperthyroidism and myocardialinfarction may present with vague or nonspecificsymptoms. As a result, treatable conditions cango unrecognized in this population.10"'1 Left un-recognized, these disorders will not only remainuntreated but may be exacerbated by drug treat-ment, or may alter the success of drug treatmentfor another illness.
Age-Related Biologic and Physiologic ChangesAge-related changes occur in many biologic
and physiologic functions." Table 1 lists severaltypes of changes that can affect the pharmacologyof many drugs.
It is crucial to keep in mind two characteristicsof changes that occur with age. First, the changesare gradual and occur over many years. Second,there is wide interindividual variation in the rateof these age-related changes. Thus, although ad-vancing age is associated with the decline in manyphysiologic functions, the extent of decline in anyindividual person is difficult to predict. This isimportant to remember when prescribing drugs;applying average age-related changes in physi-ologic functions to a particular older patient canbe misleading, and may result in overdosage, aswell as underdosage, of many drugs.
Absorption. As shown in Table 1, there areseveral age-related changes that could affect theabsorption of dr-ugs in the elderly."3 Althoughseveral studies of drug absorption in this popula-tion have been carried out,14 none have shownclinically meaningful changes. Altered absorptionof drugs, therefore, appears to be the least im-portant of age-related changes in pharmacology.
Distribution. Several changes related to age canaffect the distribution of drugs. Alterations inblood flow, especially to the major sites of drugelimination (liver, kidney) can have importantinfluences on drug kinetics and effects.'5 Changes
TABLE 1.-Age-Related Changes Relevant toPharmacology
Age-Related Change Phar n2acologic Function
Decreased absorptive surface AbsorptionDecreased splanchnic blood flowIncreased gastric pHAltered gastrointestinal motilityDecreased lean body mass DistributionDecreased total body waterDecreased serum albuminIncreased fatAltered protein bindingDecreased liver mass Hepatic metabolismDecreased liver blood flowDecreased enzyme activity and
inducibilityDecreased renal blood flow Renal excretionDecreased glomerular filtration rateDecreased tubular secretory functionAlterations in Receptor sensitivity
Receptor numberReceptor affinitySecond messenger functionCellular responses
in body composition, such as increased fat anddecreased extracellular fluid and lean body mass,10can alter the concentration and kinetics of drugsthat distribute in the various body compartments.Decline in serum albumin,'7 the major drug bind-ing protein, can make more free drug available forpharmacologic action. The combination of lowerserum albumin and polypharmacy may result inmany adverse drug interactions-especially in-volving those drugs that are highly protein bound,such as salicylates, anticoagulants and orally givenhypoglycemics.
Hepatic Melabolism. Although there are noage-related changes in routine liver function tests,the liver's capacity to metabolize drugs is alteredwith increasing age. Because blood flow to theliver declines,'1 first-pass hepatic extraction andmetabolism of orally administered drugs is dimin-ished. The ability of environmental factors, suchas cigarette smoking, to induce drug metabolizingenzymes decreases with age.18-20 Studies of age-related changes in specific hepatic drug metabolicpathways, such as oxidation, hydroxylation andacetylation, have shown variable results.'4"2".22The effects of aging on hepatic drug metabolismare therefore complex, dependent on several fac-tors and often difficult to predict.
Excretion. Several structural and functionalchanges occur in the kidney with increasing age23that have important influences on the excretion ofdrugs and their active metabolites (Table 1).
Because lean body mass declines with age, daily
456 DECEMBER 1981 * 135 * 6
GERIATRIC MEDICINE
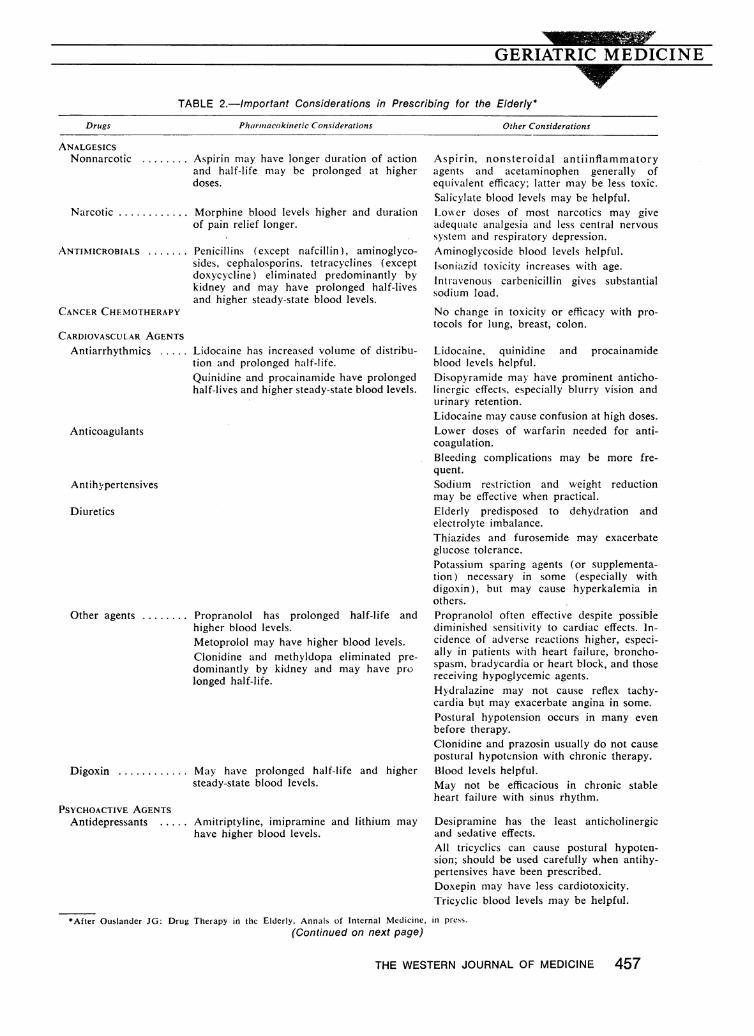
TABLE 2.-Important Considerations in Prescribing for the Elderly*
Pharmacokinetic Considerations
ANALGESICSNonnarcotic ........ Aspirin may have longer duration of action
and half-life may be prolonged at higherdoses.
Narcotic .......... Morphine blood levels higher and duration
ANTINlICROBIALS .....
CANCER CHEMOTHERAPY
CARDIOVASCULAR AGENTSAntiarrhythmics .....
Anticoagulants
Antihy,pertensives
Diuretics
Other agents ........
Digoxin ............
PSYCHOACTIVE AGENTSAntidepressants ....
Penicillins (except nafcillin), aminoglyco-sides, cephalosporins. tetracyclines (exceptdoxycycline) eliminated predominantly bykidney and may have prolonged half-livesand higher steady-state blood levels.
Lidocaine has increased volume of distribu-tion and prolonged half-life.Quinidine and procainamide have prolongedhalf-lives and higher steady-state blood levels.
Propranolol has prolonged half-life andhigher blood levels.Metoprolol may have higher blood levels.Clonidine and methyldopa eliminated pre-dominantly by kidney and may have prolonged half-life.
May have prolonged half-life and highersteady-state blood levels.
Amitriptyline, imipramine and lithium mayhave higher blood levels.
Other Considerations
Aspirin, nonsteroidal antiinflammatoryagents and acetaminophen generally ofequivalent efficacy; latter may be less toxic.Salicylate blood levels may be helpful.Lowxer doses of most narcotics may giveadequate anailgesia and less central nervous
system and respiratory depression.Aminoglycoside blood levels helpful.Isoniazid toxicity increases with age.
IntravenoUs carbenicillin gives substantialsodium load.
No change in toxicity or efficacy with pro-
tocols for lung, breast, colon.
Lidocaine, quinidine and procainamideblood levels helpful.Disopyramide may have prominent anticho-liinergic effects, especially blurry vision andurinary retention.Lidocaine may cause confusion at high doses.Lower doses of warfarin needed for anti-coagulation.Bleeding complications may be more fre-quent.Sodium restriction and weight reductionmay be effective when practical.Elderly predisposed to dehydration andelectrolyte imbalance.Thiazides and furosemide may exacerbateglucose tolerance.Potassium sparing agents (or supplementa-tion) necessary in some (especially withdigoxin), but may cause hyperkalemia inothers.Propranolol often effective despite possiblediminished sensitivity to cardiac effects. In-
cidence of adverse reactions higher, especi-ally in patients with heart failure, broncho-spasm, bradycardia or heart block, and thosereceiving hypoglycemic agents.Hydralazine may not cause reflex tachy-cardia but may exacerbate angina in some.
Postural hypotension occurs in many evenbefore therapy.Clonidine and prazosin usually do not causepostural hypotension with chronic therapy.Blood levels helpful.May not be efficacious in chronic stableheart failure with sinus rhythm.
Desipramine has the least anticholinergicand sedative effects.All tricyclics can cause postural hypoten-sion; should be used carefully when antihy-pertensives have been prescribed.Doxepin may have less cardiotoxicity.Tricyclic blood levels may be helpful.
*After Ouslander JG: Drug Therapy in the Elderly. Annals of Internal Medicine, in press.
(Continued on next page)
THE WESTERN JOURNAL OF MEDICINE 457
Drugs
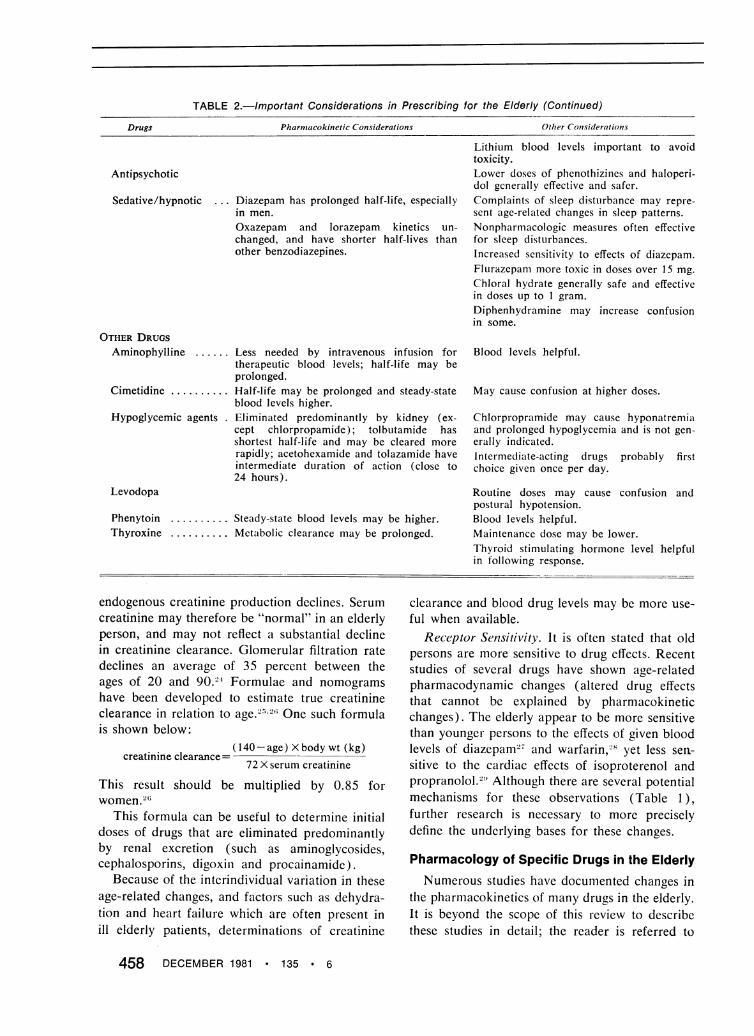
TABLE 2.-Important Considerations in Prescribing for the Elderly (Continued)Drugs Pharmacokinetic Considerations Other Considerations
Lithium blood levels important to avoidtoxicity.
Antipsychotic Lower doses of phenothizines and haloperi-dol generally effective and safer.
Sedative/hypnotic Diazepam has prolonged half-life, especially Complaints of sleep distturbance may repre-in men. sent age-related changes in sleep patterns.Oxazepam and lorazepam kinetics un- Nonpharmacologic measures often effectivechanged, and have shorter half-lives than for sleep disturbances.other benzodiazepines. Increased sensitivity to effects of diazepam.
Flurazepanm more toxic in doses over 15 mg.Chloral hydrate generally safe and effectivein doses up to 1 gram.Diphenhydramine may increase confusionin some.
OTHER DRUGSAminophylline ...... Less needed by intravenous infusion for Blood levels helpful.
therapeutic blood levels; half-life may beprolonged.
Cimetidine .......... Half-life may be prolonged and steady-state May cause confusion at higher doses.blood levels higher.
Hypoglycemic agents . Eliminated predominantly by kidney (ex- Chlorpropramide may cause hyponatremialcept chlorpropamide); tolbutamide has and prolonged hypoglycemia and is not gen-shortest half-life and may be cleared more erally indicated.rapidly; acetohexamide and tolazamide have Intermediate-acting drugs probably firstintermediate duration of action (close to choice given once per day.24 hours).
Levodopa Routine doses may cause confusion andpostulral hypotension.
Phenytoin ...... Steady-state blood levels may be higher. Blood levels helpful.Thyroxine ...... Metabolic clearance may be prolonged. Maintenance dose may be lower.
Thyroid stimulating hormone level helpfulin following response.
endogenous creatinine production declines. Serumcreatinine may therefore be "normal" in an elderlyperson, and may not reflect a substantial declinein creatinine clearance. Glomerular filtration ratedeclines an average of 35 percent between theages of 20 and 90.2- Formulae and nomogramshave been developed to estimate true creatinineclearance in relation to age.' One such formulais shown below:
( 140-age) X body wt (kg)72 X serum creatinine
This result should be multiplied by 0.85 forwomen.26
This formula can be useful to determine initialdoses of drugs that are eliminated predominantlyby renal excretion (such as aminoglycosides,cephalosporins, digoxiii and procainamide).
Because of the interindividual variation in theseage-related changes, and factors such as dehydra-tion and heart failure which are often present inill elderly patients, determinations of creatinine
clearance and blood drug levels may be more use-ful when available.
Receptor Sensitivity. It is often stated that oldpersons are more sensitive to drug effects. Recentstudies of several drugs have shown age-relatedpharmacodynamic changes (altered drug effectsthat cannot be explained by pharmacokineticchanges). The elderly appear to be more sensitivethan younger persons to the effects of given bloodlevels of diazepam27 and warfarin 28 yet less sen-sitive to the cardiac effects of isoproterenol andpropranolol.2!} Although there are several potentialmechanisms for these observations (Table 1),further research is necessary to more preciselydefine the underlying bases for these changes.
Pharmacology of Specific Drugs in the ElderlyNumerous studies have documented changes in
the pharmacokinetics of many drugs in the elderly.It is beyond the scope of this review to describethese studies in detail; the reader is referred to
458 DECEMBER 1981 * 135 * 6
crentinine. ripqrq
several recent reviews and texts that discuss thesestudies in depth.'4'30-34
Despite the large number of studies that havebeen done, it is difficult to make specific recom-mendations as to how to alter drug dosages forindividual elderly patients. .Several factors makethe development of guidelines, such as thoseavailable for altering drug dosages in renalfailure, very complex. These factors includethe wide interindividual variation of age-relatedchanges, the coexistence of multiple conditions,the variability of the clinical status of individualelderly patients and the technical difficulties in-volved in defining age-related pharmacokineticchanges.36
Table 2 and the discussion below briefly sum-marize pharmacologic information that is particu-larly relevant to the prescription of specific drugsfor the elderly.
A nalgesicsMany elderly persons frequently complain of
pain. It is important to attempt to differentiatepain from an inflammatory process from nonin-flammatory causes, because the former may re-spond more favorably to aspirin and nonsteroidalinflammatory drugs. These drugs are of generallyequivalent efficacy; the half-life of aspirin is in-creased in older persons, and may be greatlyincreased at higher doses. Determinations ofsalicylate blood levels may be helpful when highdoses are used. Acetominophen is safe in theelderly; it should be kept in mind that many pa-tients with minor pain may benefit by nonphar-macologic treatments.
Narcotic analgesics appear to give more painrelief, and may have prolonged duration of action,in older patients.37 These drugs can cause seda-tion, confusion and severe constipation (whichcan lead to fecal impaction and its attendantproblems) in the elderly; the need for these drugsshould be carefully assessed, therefore, and theiruse closely monitored.
A ntimicrobialsMost antimicrobial drugs are eliminated pre-
dominantly by renal excretion (Table 2).. Age-related changes in renal function should not in-fluence the standard dosages of most of thesedrugs; aminoglycosides, because of their potentialfor ototoxicity and nephrotoxicity, should be usedcarefully. Blood level determinations may be use-ful when using these agents.
GERIATRIC MEDICINE
Two antimicrobial agents may have special po-tential for adverse reactions in old persons. Intra-venously administered carbenicillin delivers a sub-stantial sodium load, and should be used carefullyin patients with symptomatic congestive heartfailure. Isoniazid hepatotoxicity increases with ageand its use should be carefully evaluated andmonitored.'8
Cancer ChemotherapyA recent analysis of data from the Eastern
Cooperative Oncology Group showed that toxicityfrom protocols for lung, breast and colon cancerdoes not increase in the elderly.39 This was truedespite the lack of any dosage reductions; theregimens also were equally effective in the olderage groups.
Cardiovascular AgentsAntiarrhythmics. Arrhythmias are common in
the elderly, but because of the potential toxicityof antiarrhythmic agents, the necessity for treat-ment should be carefully evaluated. Udocaine,quinidine and procainamide all have prolongedhalf-lives in the elderly; the latter two drugs alsohave higher steady-state blood levels.40 41 Bloodlevels of these agents can be helpful in monitoringtherapy. Disopyramide can cause prominent anti-cholinergic side effects in these patients, such as
urinary retention and blurry vision. Other newerantiarrhythmics have not been well studied inolder persons.
Antihypertenisives. The management of hyper-tension in the elderly remains controversial.42'43Although data are scarce in the very old (olderthan 75), recent studies involving persons between60 and 69 years of age indicate that hypertensionremains an important risk factor for cardiovascu-lar morbidity and mortality,"4 4 and that treat-ment may reduce this risk.46
Antihypertensives may, however, produce seri-ous adverse reactions in the elderly. Diuretics maypredispose to electrolyte imbalance and dehydra-tion, especially when an intercurrent illnessdecreases oral intake. They may also exacerbateurinary incontinence. Postural hypotension iscommon even without drugs, and may be exacer-bated by most antihypertensive agents. This maylead to falls and their sequelae; lethargy, depres-sion and confusion may also result from antihyper-tensive agents.
,3-Adrenergic blocking agents, although usefulfor hypertension as well as angina, must be used
THE WESTERN JOURNAL OF MEDICINE 459
carefully in the elderly. The incidence of adversereactions is higher,"7 especially with chronic ob-structive lung disease, congestive heart failure,bradycardia and concurrent hypoglycemic therapy.Although there is some evidence that old personsare less sensitive to the cardiac effects of pro-pranolol,29 its metabolism is diminished, half-lift prolonged and blood levels higher. 1948
The potential benefits of antihypertensive ther-apy must be carefully weighed against the possibleadverse effects on the quality of life. Restrictivediets, although helpful in some, may be unpalat-able and impractical for many elderly persons.The reader is referred to recent reviews for moredetailed suggestions on the management of hyper-tension in this population.4243
Digoxin. Digoxin is one of the most frequentlyprescribed yet potentially toxic drugs in theelderly.7": Recent studies have suggested thatpersons with chronic heart failure in sinus rhythmcan be safely withdrawn from therapy,4910 al-though this remains controversial."' Because ofits potential toxicity, the necessity for this agentshould be carefully evaluated (it should not begiven for nonspecific symptoms alone, such asfatigue, dyspnea or lower extremity edema).Blood levels may be helpful in determining com-pliance and toxicity. Toxicity may be especiallydifficult to diagnose because the manifestationsare often nonspecific (such as fatigue and weak-ness) .52
Psychoactive DrugsDespite considerable evidence that psychoactive
drugs have enhanced toxicity in older persons, 3-55they are commonly used in this population; 75percent of nursing home residents receive at leastone of these drugs and usually more.`';
Although the judicious use of these drugs canprovide dramatic relief of the anxiety, agitationand depression so common in the elderly, it shouldbe remembered that these symptoms may reflectunderlying physical illness.8 Excessive sedationmay result from many of these drugs, especiallyhypnotics such as flurazepam (when given in dosesof 30 mg or more). Many of these agents haveprominent anticholinergic effects (especially ami-triptyline, doxepin, thorazine and thioridazine)and can cause confusion, blurry vision, urinaryretention and constipation. Tricyclic antidepres-sants can cause postural hypotension (especiallywhen added to an antihypertensive agent) andfalls, as well as prolonged cardiac conduction.
They must be used very carefully in older patientswith underlying cardiovascular disease.;7 Manyof these drugs (especially antipsychotic drugs suchas haloperidol and thioridazine) can have promi-nent extrapyramidal side effects, and can exacer-bate underlying Parkinson's disease and other gaitdisturbances in these patients.
Although numerous drugs have been used toimprove cognitive function in the elderly, nonehave been shown in rigorously controlled studiesto have substantial impact on daily functionalcapabilities. Until further research yields betterdrugs, these agents (which are often very expen-sive) should not replace careful evaluation andfollow-up of cognitive impairment, and counselingof the patient and family.
The reader is referred to recent comprehensivereviews that deal in depth with psychoactive druguse in the elderly.32'58
Other DrugsImportant considerations for other commonly
used drugs in the elderly, such as aminophylline,cimetadine and oral hypoglycemic agents areshown in Table 2.
ComplianceCompliance is often a major obstacle to drug
treatment in any population. Most studies showbetween a third and a half of patients will fail tocomply with a medical regimen.59
Several factors make compliance an even morecomplex feature of drug prescribing in the elderly.Mild and chronic disorders that require prophy-lactic or suppressive therapy, and in which theconsequences of stopping therapy may be de-layed, lend themselves to noncompliance. Com-plex medical regimens, requiring several differentmedications and frequent doses, may also con-tribute to a higher incidence of noncompliance.All of these are common in the elderly population.
In addition to the prevalence of mutiple chronicillnesses and the attendant need for complex drugregimens, a variety of physical, psychologic, socialand economic barriers may impair an older pa-tient's ability to comply.
The average elderly person in this countryspends more than $100 a year on prescriptiondrugs,0 and these costs, usually not well coveredby reimbursement plans, come out of an alreadyfixed and limited income. Intellectual impairment,poor vision and diminished hearing may makepatient education difficult, and prevent a patient
460 DECEMBER 1981 * 135 * 6
GERIATRIC MEDICINEPI
from following instructions. Many older personshave cultural attitudes and beliefs that may makethe process even- harder. Weakened, arthritichands are often unable to open childproof con-tainers, and this may be a problem in as manyas 60 percent of elderly patients.61 Lack of trans-portation or fear of crime may prevent the elderlyfrom reaching a physician or pharmacist.Many studies emphasize the need for careful
supervision of elderly patients requiring long-termmedication.'63 One of these showed that teachinga patient an individual drug regimen in the hos-pital may help identify and overcome problemswith noncompliance.64 Instructional aids such astablet identification cards and tear-off calendarshave also been shown to improve compliance inthese patients.64
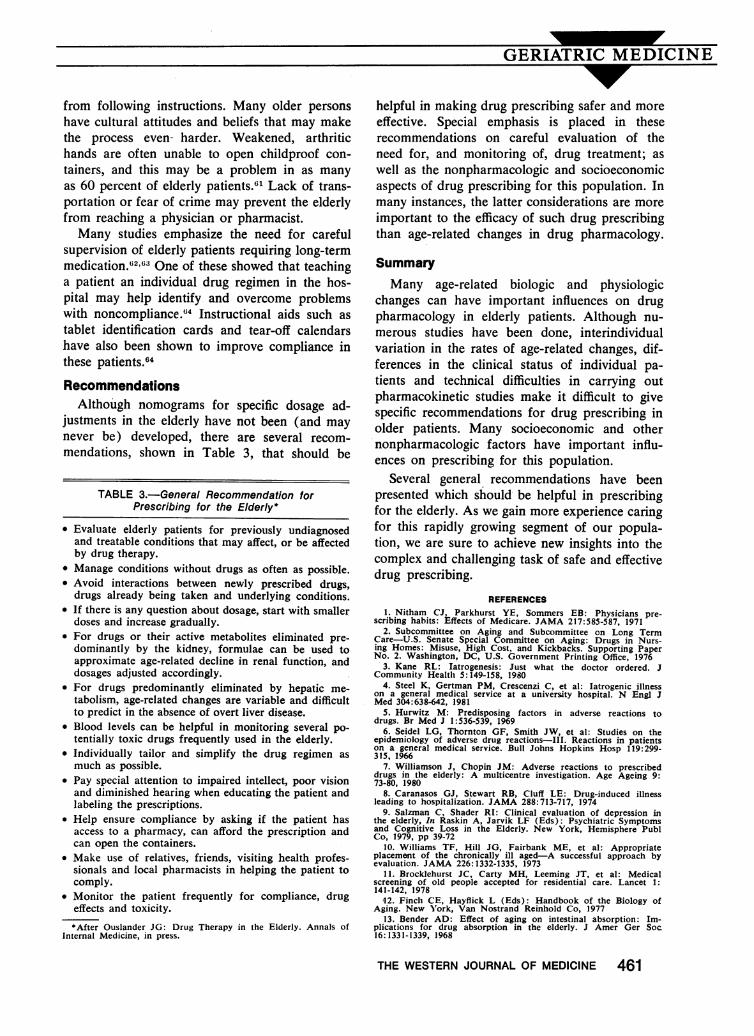
RecommendationsAlthough nomograms for specific dosage ad-
justments in the elderly have not been (and maynever be) developed, there are several recom-mendations, shown in Table 3, that should be
TABLE 3.-General Recommendation forPrescribing for the Elderly*
* Evaluate elderly patients for previously undiagnosedand treatable conditions that may affect, or be affectedby drug therapy.
* Manage conditions without drugs as often as possible.* Avoid interactions between newly prescribed drugs,
drugs already being taken and underlying conditions.* If there is any question about dosage, start with smaller
doses and increase gradually.* For drugs or their active metabolites eliminated pre-
dominantly by the kidney, formulae can be used toapproximate age-related decline in renal function, anddosages adjusted accordingly.
* For drugs predominantly eliminated by hepatic me-tabolism, age-related changes are variable and difficultto predict in the absence of overt liver disease.
* Blood levels can be helpful in monitoring several po-tentially toxic drugs frequently used in the elderly.
* Individually tailor and simplify the drug regimen asmuch as possible.
* Pay special attention to impaired intellect, poor visionand diminished hearing when educating the patient andlabeling the prescriptions.
* Help ensure compliance by asking if the patient hasaccess to a pharmacy, can afford the prescription andcan open the containers.
* Make use of relatives, friends, visiting health profes-sionals and local pharmacists in helping the patient tocomply.
* Monitor the patient frequently for compliance, drugeffects and toxicity.*After Ouslander JG: Drug Therapy in the Elderly. Annals of
Internal Medicine, in press.
helpful in making drug prescribing safer and moreeffective. Special emphasis is placed in theserecommendations on careful evaluation of theneed for, and monitoring of, drug treatment; aswell as the nonpharmacologic and socioeconomicaspects of drug prescribing for this population. Inmany instances, the latter considerations are moreimportant to the efficacy of such drug prescribingthan age-related changes in drug pharmacology.
SummaryMany age-related biologic and physiologic
changes can have important influences on drugpharmacology in elderly patients. Although nu-merous studies have been done, interindividualvariation in the rates of age-related changes, dif-ferences in the clinical status of individual pa-tients and technical difficulties in carrying outpharmacokinetic studies make it difficult to givespecific recommendations for drug prescribing inolder patients. Many socioeconomic and othernonpharmacologic factors have important influ-ences on prescribing for this population.
Several general recommendations have beenpresented which should be helpful in prescribingfor the elderly. As we gain more experience caringfor this rapidly growing segment of our popula-tion, we are sure to achieve new insights into thecomplex and challenging task of safe and effectivedrug prescribing.
REFERENCES1. Nitham CJ, Parkhurst YE, Sommers EB: Physicians pre-
scribing habits: Effects of Medicare. JAMA 217:585-587, 19712. Subcommittee on Aging and Subcommittee on Long Term
Care-U.S. Senate Special Committee on Aging: Drugs in Nurs-ing Homes: Misuse, High Cost, and Kickbacks. Supporting PaperNo. 2. Washington, DC, U.S. Government Printing Office, 1976
3. Kane RL: latrogenesis: Just what the doctor ordered. JCommunity Healtlh 5:149-158, 1980
4. Steel K, Gertman PM, Crescenzi C, et al: latrogenic illnesson a general medical service at a university hospital. N Engl JMed 304:638-642, 1981
5. Hurwitz M: Predisposing factors in adverse reactions todrugs. Br Med J 1:536-539, 1969
6. Seidel LG, Thornton GF, Smith JW, et al: Studies on theepidemiology of adverse drug reactions-I}I. Reactions in patientson a general medical service. Bull Johns Hopkins Hosp 119:299-315, 1966
7. Williamson J, Chopin JM: Adverse reactions to prescribeddrugs in the elderly: A multicentre investigation. Age Ageing 9:73-80, 1980
8. Caranasos GJ, Stewart RB, Cluff LE: Drug-induced illnessleading to hospitalization. JAMA 288:713-717, 1974
9. Salzman C, Shader RI: Clinical evaluation of depression inthe elderly, In Raskin A, Jarvik LF (Eds): Psychiatric Symptomsand Cognitive Loss in the Elderly. New York, Hemisphere PublCo, 1979, pp 39-72
10. Williams TF, Hill JG, Fairbank ME, et al: Appropriateplacement of the chronically ill aged-A successful approach byevaluation. JAMA 226:1332-1335, 1973
11. Brocklehurst JC, Carty MH, Leeming JT, et al: Medicalscreening of old people accepted for residential care. Lancet 1:141-142, 1978
12. Finch CE, Hayflick L (Eds): Handbook of the Biology ofAging. New Y'ork, Van Nostrand Reinhold Co, 1977
13. Bender AD: Effect of aging on intestinal absorption: Im-plications for drug absorption in the elderly. J Amer Ger Soc16:1331-1339, 1968
THE WESTERN JOURNAL OF MEDICINE 461
14. O'Malley K, Laher M, Cusack B, et al: Clinical pharma-cology a'nd the elderly patient, In Denham MJ (Ed): The Treat-ment of Medical Problems in the Elderly. Baltimore, UniversityPark Press, pp 7-9, 1980
15. Bender AD: The effect of increasing age on the distributionof peripheral blood flow in man. J. Amer Ger Soc 13:192-198, 1965
16. Norris AH, Lundy T, Shock NW: Trends in elected indicesof body composition in men between the ages of 30 and 80 years.Ann NY Acad Sci 110:623-639, 1963
17. Wallace S, Whiting B, Runcie J: Factors affecting drugbinding in plasma of elderly patients. Br J Clin Pharmac 3:327-330, 1976
18. Adelman RC: Age-dependent effects in enzyme induction-A biochemical expression of aging. Exp Gerontol 6:75-87, 1971
19. Vestal RE, Wood AJ, Branch RA, et al: Effects of age andcigarette smoking on propranolol disposition. Clin Phar Ther 26:8-15, 1979
20. Wood AJJ, Vestal RE, Wilkinson GR, et al: Effect ofaging and cigarette smoking on antip)rine and indocyaniine greenelimination. Clin Pharm Ther 26:16-20, 1979
21. Farrah F, Taylor W, Rawlins MD, et al: Hepatic drugacetylation and oxidation: Effect of aging in man. Br Med J 2:155-156, 1977
22. Ritschel WA: Age-dependent disposition of amobarbital:Analog computer evalutation. J Amer Ger Soc 12:540-543, 1978
23. Epstein M: Effects of aging on the kidney. Fed Proc 38:168-172, 1979
24. Rowe JW, Andres R, Tobin JD, et al: The effect of age oncreatinine clearance in man: A cross-sectional and longitudinalstudy. J Geront 31:155-163, 1976
25: Kampmann J, Siesback-Nielsen K, KristcnlsceI M, et al:Rapid evaluation of creatinine clearance. Acta Med Scani 196:517-520, 1974
26. Cockroft DW, Gault MH: Prediction of clreatinine clear-ance from serum creatinine. Nephron 16:31-41, 1976
27. Reidenberg MM, Levy M, Warner H, et al: Relationshipbetween diazepam dose, plasma level, age antid ceiial nelrvoLIssystem depression. Clin Pharm Ther 23:371-374, 1978
28. Shepherd AM, Hewick DS, Moreland TA, et al: Age as adeterminant of sensitivity to warfarin. Br J Clin Plharinii 4:315-320,1977
29. Vestal R, Wood AJJ, Shand DG: Reduced beta-adrenoceptorsensitivity in the elderly. Clin Pharin Ther 26:818-886, 1979
30. Jarvik LF, Greenblatt D, Harmani D (Eds): Pharnmacologyand the Aged Patient. New York, Raven Press, 1981
31. Lamy PP: Prescribing for the Elderly. Littleton, MA, PSGPublishing Co, 1980
32. Hicks R, Funkenstein HH, Dysken MW, et al: Geriatricpsychopharmacology, In Birren J, Sloane RB (Eds): Handbookof Mental Health and Aging. Englewood Cliffs, NJ, Prentice Hall,1980, pp 745-774
33. Richey DP, Bender AD: Pharmacokinetic consequences ofaging. Ann Rev Pharm Tox 17:49-65, 1977
34. Vestal RE: Drug use in the elderly. A review of problemsand special considerations. DruLgs 16:358-382, 1978
35. Bennett WM, Muther RS, Parker, RA, et al: DruLg therapyin renal failure: Dosing guidelines for adults. Ann Int Med 93:62-89, 286-325, 1980
36. Greenblatt DJ, Shader RI: Pharmacokinetics in old age:Principles and problems of assessment, In Jarvik LF, GreenblattDJ, Harman D (Eds): Pharmacology and the Aged Patient. NewYork, Raven Press, 1981, pp 27-46
37. BelIville JW, Forrest WH, Miller E, et al: Influence of ageon pain relief from analgesics-A study of postoperative patients.JAMA 217:1835-1841, 1971
38. Baily WC, Weill H, Derowen TA, et al: The effect ofisoniazid on transaminase levels. Ann Int Med 81:200-202, 1974
39. Begg CB, Cohen JL, Ellerton J: Are the elderly predisposedto toxicity from cancer chemotherapy?-An investigation usingdata from the Eastern Cooperative Oncology Group. Cancer ClinTrials 3:369-374, 1980
40. Reidenberg MM, Bamacho M, Kluger J, et al: Aging andrenal clearance of procainamide and acetylprocainamide. ClinPharm Ther 28:732-735, 1980
41. Ochs RH, Greenblatt DJ, Woo E, et al: Reduced quinidineclearance in elderly persons. Am J Cardiol 42:481-485, 1978
42. Kirkendall WM, Hammond JJ: Hypertension in the elderly.Arch Int Med 140:1155-1161, 1980
43. O'Malley K, O'Brien E: Management of hypertensicn in theelderly. N Engl J Med 302:1397-1401, 1980
44. Veterans Administration Cooperative Study Group on Anti-hypertensive Agents: Effects of treatment on morbidity in hyper-tension-III. Influence of age, diastolic pressure, and cardiovas-cular disease-A further analysis of side effects. Circulation 45:991-1004, 1972
45. Kannel WB, Gordon T: Evaluation of cardiovascular riskin the elderly-Tlhe Framingham Study. Bull NY Acad Mled 54:573-591, 1979
46. Hypertension Detection and Follow-tup Program CooperativeGroup: Five-year finidings of the hypertension detection and fol-low-up program-I. Reduction in mortality of persons witlh higiblood pressure, including mild hypertension. JAMA 242:2562-2576,1979
47. Greenblatt DJ, Kock-Weser J: Adverse reactions to pro-pranolol in hospitalized medical patients: A report fromii theBoston Collaborative Drug Surveillance Program. Am Heart J86:478-484, 1973
48. Castelden CM, George CF: The effect of age on the hepaticclearance of propranolol. Br J Clin Pharmacol 7:49-54, 1979
49. Johnston GD, McDevitt DG: Is maintenance digoxin neces-sary in patients with sinus rhythnm? Lancet 1:567-570), 1979
50. McHaflie D, Purcell H, Mitchell-Heggs P, et al: hlec cliniicalvalue of digoxin in patients with heart failure and sinuLs rhytlhm.Q J Med 47:401-419, 1978
51. Arnold SB, Byrd RC, Meister W, et al: Long-ternm digitalistlherapy improves left ventricular fuLnction in heart failuire. N EnglJ Med 303:1443-1448, 1980
52. Lely AH, Van Enter CHJ: Large-scale digitoxin intoxicatioll.Br Med J 1:737-740, 1970
53. Davies RK: Confusional episodes and antidepressant medi-cation. Am J Psychiatry 128:95-99, 1971
54. Boston Collaborative Drug Surveillance Program: Clinicaldepression of the central nervous system due to diazepam andchlordiazipoxide in relation to cigarette smoking and age. N EnglJ Med 288:277-280, 1973
55. Greenblatt DJ, Allen MD, Shader RI: Toxicity of high dosellurazepam in the elderly. Clin Pharm Ther 21:355-361, 1977
56. Special Committee on Aging, United States Senate: NuLrsingHome Care in the United States: Failure in Public Policy. Wash-ington, DC, Government Printing Office, 1974
57. Risch SC, Groom GP, Janowsky DS: Interfaces of psycho-pharmacology and cardiology-Parts One and Two. J Clin Psychiat42:23-34, 47-59, 1981
58. Jarvik LF, Kakkar PR: Aging and response to antidepres-sants, In Jarvik LF, Greenblatt DJ, Harman D (Eds): Pharma-cology and the Aged Patient. New York, Raven Press, 1981
59. Haynes RB, Taylor DW, Sackett DL (Eds): Compliance inHealth Care. Baltimore: The Johns Hopkins University Press,1979
60. National Center for Health Statistics: Health InterviewSurvey, U.S. 1975. DHEW Publication No. (HRA) 77-1543, Rock-ville, MD, 1977
61. Sherman FT, Warach JD, Libow LS: Child resistant con-tainers for the elderly? (Editorial). JAMA 241:1001-1002, 1979
62. Adkinson L, Gibson I, Andrews J: An investigation intothe ability of elderly patients to take prescribed drugs after dis-charge from hospital and recommendations concerning improvingthe situation. Gerontology 24:225-234, 1978
63. Libow LS, Mehl B: Self-administration of medications bypatients in hospitals or extended care facilities. J Amer Ger Soc18:81-95, 1970
64. Wandless I, Davie JW: Can drug compliance in the elderlybe improved? Br Med J 1:359-361, 1977
462 DECEMBER 1981 * 135 * 6