drug-induced nephrotoxicity and its management...
TRANSCRIPT

International Bulletin of Drug Research., 2(3): 50-65
50
DRUG-INDUCED NEPHROTOXICITY AND ITS
MANAGEMENT -AN OVERVIEW
*M. LEENA1, SUBASH VIJAYAKUMAR
2, A.Y. RAO
3
______________________________________________________________________________
ABSTRACT
Drug-induced renal failure is common and responsible for a variety of pathological effects on the
kidney. Many medications can lead to renal dysfunction through various mechanisms, which can
cause significant morbidity. Our review article mainly focused on drugs associated with
nephrotoxicity and its prevention strategies. We developed a search strategy to find publications
on drug induced nephrotoxicity and its management so; we searched Science Direct, Medline
and PubMed bibliographic databases, and renal texts to identify relevant articles. Our review
suggested that proper understanding the mechanisms involved, and recognizing the clinical
presentations of renal dysfunction arising from use of commonly prescribed medications are
important if injury is to be detected early and prevented. As it is impossible to list all drugs
associated with nephrotoxicity, this article will summarize the mechanism of injury associated
with particular common medications, discuss clinical presentations, renal markers, and evaluate
strategies that prevent or minimize renal injury.
KEY WORDS
Nephrotoxicity, Renal biomarkers, Renal toxicity, Renal injury and Medications.
AFFILIATION
1. *M. Leena, Assistant Professor, MGM Hospital, Vaagdevi college of pharmacy Ram
Nagar, Hanamkonda, Warangal, Mob:9908114422, Email id: [email protected]
2. Subash vijayakumar, Department of Pharmacy Practice, Vaagdevi College of Pharmacy,
MGM Hospital, Warangal,A.P, India.
3. A.Y. Rao, Department of Oncology, KMC/MGM Hospital, Warangal, A.P, India.

International Bulletin of Drug Research., 2(3): 50-65
51
INTRODUCTION
Medication-induced nephrotoxicity has been cited, a major cause for acute renal failure in
humans, and antibiotics especially aminoglycoside antibiotics, have been among the most
common offending agents.1 Drugs causes approximately 20 percent of community and hospital
acquired episodes of acute renal failure. Among older adults, the incidence of drug-induced
nephrotoxicity may be as high as 66 percent.2 Most episodes of renal dysfunction are reversible,
with function returning to baseline when the medication is discontinued. Chronic renal injury can
however be induced by some medications, leading to chronic tubulo-interstitial inflammation,
papillary necrosis or prolonged proteinuria.3
Incidence of acute renal failure in the newborn
Acute renal failure in the new born may be caused by a failure of renal perfusion (pre-renal
failure), damage to the renal parenchyma (intrinsic renal failure) or obstruction of the urinary
tract (post-renal failure). Most cases of intrinsic renal failure in the newborn are due to asphyxia,
often in combination with sepsis and nephrotoxic drugs.4
Exposure to nephrotoxic drugs
separately, or in combination precede most episodes of ARF in the newborn. Antibacterial-
induced nephrotoxicity is an important parameter to be considered when treating the newborn
and this is particularly true when use of a combination of different antibacterials and/or drugs
with a nephrotoxic potential is being considered.5
Epidemic Nephrotoxicity
Nephrotoxicity can also induced by 'atypical' or 'unconventional' agents, such as environmental
agents (metals, minerals & animals), food agents (mushrooms, medicinal traditional herbals,
dietary supplement & melamine), drugs, and other products (ethylene glycol). Nephrotoxicity
varies according to local background, dependent on different food and cultural customs, as well
as to differences in local fauna and flora.6
Recent outbreaks of nephrolithiasis and acute kidney
injury among children in China have been linked to ingestion of milk-based infant formula
contaminated with melamine. The USFDA has twice amended its assessment of melamine
toxicity for infants, and concluded that only foods with less than 1 p.p.m. of melamine are safe
for infants.7
Mechanism of toxicity
Toxicity is a relative phenomenon that depends on the inherent structure and properties of a
chemical and on its dose. Exogenous chemicals are absorbed after ingestion, inhalation, or skin
contact and then distributed to various organs. Chemicals are frequently metabolized, often by
multiple enzymatic pathways; to produce that may be more toxic, les toxic than the parent
chemical. One or more of these products then interacts with the target macro molecules, resulting
in a toxic effect.8

International Bulletin of Drug Research., 2(3): 50-65
52
Figure 1: Absorption and distribution of toxicities.
Biotransformation of toxicants
Exposure
Absorption at portals of entry
Distribution to body
Metabolism
to more toxic
metabolites
Turnover
& repair
Metabolism
to more less
toxic
metabolites
Metabolism
to more
conjugate
products
Interaction with macromolecules
(Proteins, DNA, RNA, receptors)
Distribution
Toxic effects
(Genetic, carcinogenic, reproductive, immunotoxic)
Excretion
Toxicants
Phase I
reactions
Elimination in urine, bile, or feces
Secondary
metabolites
Phase II
reactions
Primary
metabolites
International Bulletin of Drug Research., 2(3): 50-65
53
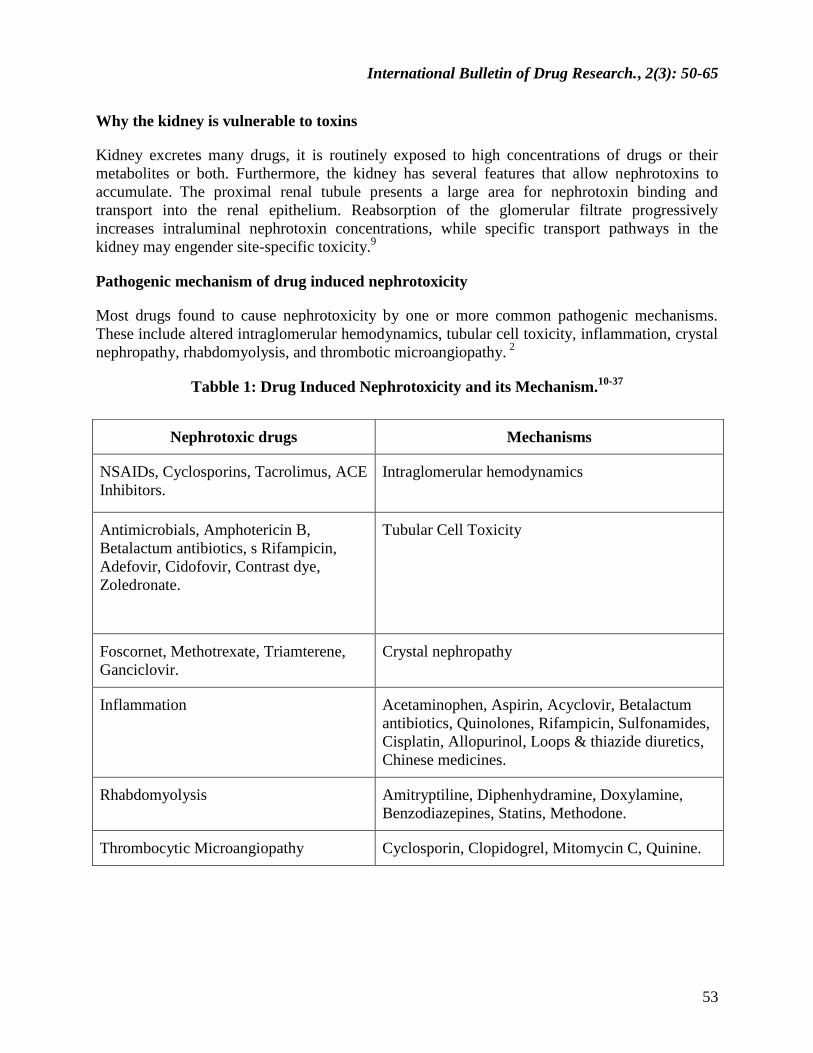
Why the kidney is vulnerable to toxins
Kidney excretes many drugs, it is routinely exposed to high concentrations of drugs or their
metabolites or both. Furthermore, the kidney has several features that allow nephrotoxins to
accumulate. The proximal renal tubule presents a large area for nephrotoxin binding and
transport into the renal epithelium. Reabsorption of the glomerular filtrate progressively
increases intraluminal nephrotoxin concentrations, while specific transport pathways in the
kidney may engender site-specific toxicity.9
Pathogenic mechanism of drug induced nephrotoxicity
Most drugs found to cause nephrotoxicity by one or more common pathogenic mechanisms.
These include altered intraglomerular hemodynamics, tubular cell toxicity, inflammation, crystal
nephropathy, rhabdomyolysis, and thrombotic microangiopathy. 2
Tabble 1: Drug Induced Nephrotoxicity and its Mechanism.10-37
Nephrotoxic drugs Mechanisms
NSAIDs, Cyclosporins, Tacrolimus, ACE
Inhibitors.
Intraglomerular hemodynamics
Antimicrobials, Amphotericin B,
Betalactum antibiotics, s Rifampicin,
Adefovir, Cidofovir, Contrast dye,
Zoledronate.
Tubular Cell Toxicity
Foscornet, Methotrexate, Triamterene,
Ganciclovir.
Crystal nephropathy
Inflammation Acetaminophen, Aspirin, Acyclovir, Betalactum
antibiotics, Quinolones, Rifampicin, Sulfonamides,
Cisplatin, Allopurinol, Loops & thiazide diuretics,
Chinese medicines.
Rhabdomyolysis Amitryptiline, Diphenhydramine, Doxylamine,
Benzodiazepines, Statins, Methodone.
Thrombocytic Microangiopathy Cyclosporin, Clopidogrel, Mitomycin C, Quinine.

International Bulletin of Drug Research., 2(3): 50-65
54
Figure 2: General Nephrotoxic factors.10
Figure 3: Clinical Features of Drug Induced Nephrotoxicity. 11
Acute tubular
necrosis
Magnesium
wasting
oliguria
Nephrolithiasis
Renal colic
hematuria
Glomerulo nephritis
Foamy urine
Marked facial and lower
extremity pitting edema
Oliguria
Protenuria
Skin rash
General
Costo –vertebral
angle edema
Elevated serum
creatinine fever
hypertension,
malaise
rapid weight gain
Acute interstitial
nephritis
Arthralgia
Eosinophilia
Eosinophiluria
Pyuria
Skin rash

International Bulletin of Drug Research., 2(3): 50-65
55
ASSESSMENT OF RENAL FUNCTION TESTS
According to the ICH S7A Harmomized tripartite Guideline (Safety Pharmacology Studies for
Human Pharmaceuticals), most of the parameters suggested to asses renal function includes
urinary volume, specific gravity, Osmolality, pH, fluid/electrolyte balance, proteins, cytology,
blood urea nitrogen, plasma creatinine and plasma proteins.12
Renal function test is given in the figure: 4.13
Table 2: Normal Ranges of blood and urine biochemistry.
Blood Chemistry Urine Biochemistry
Sodium 132–144 mmol/l
Potassium 3.5–5.5 mmol/l
Urea 3.5–7.4 mmol/l
Creatinine 44–80 μmol/l
Chloride 95–110 mmol/l
Plasma osmolality 275–295 m
osmol/kg
(HCO−3 + Cl−) 12–16 mmol/l
Sodium 100–200 mmol/24 h
Potassium 30–90 mmol/24 h
Protein < 0.15 g/24 h
Creatinine 9–17 mmol/24 h
Creatinine Clearance -120
ml/min
Urine Analysis
Urinalysis by definition refers only to the chemical analysis of urine. Routine urinalysis refers to
1. Macroscopic analysis which includes assessment of physical characteristics and chemical
analysis
2. Microscopic analysis for formed elements.15
Assessment of kidney function and identification of the site of injury within the nephron is the
best performed through the examination of urine. Injury can be assessed by examination of
cellular enzymes which are preferentially leaked into the urine.12
Renal function and glomerular filtration rate 14
Glomerular filtration rate (GFR) is the rate (volume per unit of time) at which ultrafiltrate is
formed by the glomerulus.16
and it is calculated by the clearance of specific substances.
Characteristics of an ideal marker for GFR Measurement17

International Bulletin of Drug Research., 2(3): 50-65
56
Constant rate of production (or for exogenous marker can be delivered intravenously at a
constant rate)
Freely filterable at the glomerulus (minimal protein binding)
No tubular reabsorption
No tubular secretion
No extra renal elimination or metabolism
Availability of an accurate and reliable assay
For exogenous marker: safe, convenient, readily available, inexpensive, and does not
influence GFR (physiologically inert)
Causes of interpatient variability include: 18
Body size: GFR conventionally factored by 1.73 m2
Sex: GFR approximately 8% higher in males
Race
Age: age-related decline in GFR, 0.75 to 1.0 mL/min/1.73 m2 (0.01 to 0.02 mL/s/ 1.73
m2) per year
Pregnancy: GFR elevated as much as 50% in first trimester and onward; returns
Toward normal by 4 to 8 weeks postpartum
Protein intake: GFR higher in patients on high-protein diet
Diurnal variation: values tend to be about 10% higher in afternoon than at night.
Normal range for GFR
The normal corrected GFR are
Male: 120±25 mL/min
Female: 95±20ml/min.19
Creatinine Clearance (C): creatinine concentration alone can be used to estimate GFR by a
number of mathematical models.
The commonly used are
Cockkroft-Gault equation,

International Bulletin of Drug Research., 2(3): 50-65
57
Modification of diet in renal disease (MDRD), and
Schwartz equation.14
Formulas to assess renal function.
and
Adjust Medication Dosages.
RENAL BIOMARKERS
Biochemical markers play an important role in accurate diagnosis and also for assessing risk and
adopting therapy that improves clinical outcome. According to the NIH working group, a
biomarker is a characteristic that is objectively measured as an indicator of normal biological
processes, pathogenic processes, or a pharmacological response to a therapeutic intervention
(Biomarkers Definitions Work Group, 2001).22
Ideal features of biomarkers used to detect drug-induced nephrotoxicity
Identifies kidney injury early (well before the renal reserve is dissipated and levels of
serum creatinine increase)
Reflects the degree of toxicity, in order to characterize dose dependencies
Displays similar reliability across multiple species, including humans
Localizes site of kidney injury
Tracks progression of injury and recovery from damage
Schwartz equation
eCrCl = (length [cm] × k) ÷ serum
creatinine (mg per dL)
k =0.55 (children one to 13 years of age)
0.70 (males 14 to 17 years of age)
0.55 (females 14 to 17 years of age). 20
MDRD equation
eGFR = 186 × serum creatinine (mg
per dL) −1.154
× age (years) −0.203
×
(0.742 if patient is female) × (1.210 if
patient is black).2
Cockcroft and Gault equation
Male: eCrCl = ([140 – age (years)]
× ideal body weight [kg]) ÷ (serum
creatinine [mg per dL] × 72).21

International Bulletin of Drug Research., 2(3): 50-65
58
Is well characterized with respect to limitations of its capacities
Is accessible in readily available body fluids or tissues.23
Existing biomarkers for detecting kidney injury
The current biomarkers, serum creatinine (SCr) and blood urea nitrogen (BUN), to monitor renal
safety are late and insensitive and show limited specificity with the serious consequences that
AKI can not be prevented or managed with appropriate tools. 24
Second-generation biomarkers for acute kidney injury
In the past decade, several efforts have been undertaken to identify better and earlier markers of
nephrotoxicity using genomics and proteomics approaches (Amin et al. 2004; Devarajan 2008;
Kramer et al. 2004; Thukral et al. 2005). Those new markers are more sensitive and can detect
damage earlier than BUN and creatinine levels.25
Table 3: List of biomarkers of nephrotoxicity. 26
Urinary protein with
enymatic activity
Filtered low- molecular
proteins
Heart -type fatty acid
binding protein
Liver type fatty acid
binding protein
Alanine amino peptidase
α-Glutathione-S-tranferase
γ-Glutamyl transpeptidase
п- Glutathione-S-tranferase
N-Acetyl-β-D-
glucosaminidase
α1
-Microglobulin
β2-
Microglobulin
Cystatin-C
Retinol binding protein
Interleukin-18
Kidney injury molecule-1
Microalbumin
Neutrophil gelatinase-
associated lipocalin
MANAGEMENT OF NEPHROTOXICITY.
Most patients with ARF recover with conservative management which includes
Fluid monitoring,
Protein restriction,
Drug adjustments,
Dietary or potassium control, and
Dialysis (usually temporary).27

International Bulletin of Drug Research., 2(3): 50-65
59
Main metabolic abnormalities in patients with renal failure.28
Anorexia – reduced oral nutrient intake
Gastrointestinal consequences of uraemia
Restrictive diets
Uremic toxicity – inadequate dialysis prescription
Metabolic acidosis
Endocrine factors (PTH, insulin resistance etc.)
Peripheral insulin resistance
Impairment of lipolysis
Low grade inflammatory state _activation of protein catabolism
Augmented catabolic response to intercurrent disease
Metabolic acidosis
Hyperparathyroidisms, uremic bone disease
Impairment of vitamin D3 activation
Conservative management
Fluid balance
Adequate hydration is important to maintain renal perfusion and avoid drug-induced renal
impairment. Whenever possible, volume status should be assessed and corrected, if necessary,
before initiation of nephrotoxic agents. This is particularly true when prescribing medications
such as angiotensin converting enzyme inhibitors, angiotensin receptor blockers, and NSAIDs,
which induce alterations in renal hemodynamics in patients who are significantly volume
depleted. 29
Nutrition
Nutrition is an important consideration in ARF Adequate energy must be provided in order to
promote anabolism and prevent catabolism, which potentiates hyperkalemia, hyperphosphatemia
and acidosis. The purpose of nutritional management is to prevent or treat malnutrition, to reduce
accumulation of waste products, potassium and phosphorus, and to prevent complications of
uremia 30

International Bulletin of Drug Research., 2(3): 50-65
60
Table 4: Vitamin supplementation in acute renal failure. 31
Vitamins Dose
Vitamin K 4mg/wk
Vitamin E 10iu/d
Thiamine Hcl (B1) 2mg/dl
Vitamin E 10iu/d
Riboflavin (B2) 2mg/d
Pantothenic acid 10mg/d
Ascorbic acid (C) 70-100mg/d
Biotin 200mg/d
Folic acid 1mg/d
Vitamin B12 4µg/d
Folic acid 1mg/d
Vitamin B12 4µg/d
Renal replacement therapy.
Renal replacement therapy is indicated in a patient with ARF when kidney function is so poor
that life is at risk.The common types of renal replacement therapy includes
Haemodialysis
Haemofiltration
Haemodiafiltration
Peritoneal dialysis.27
Common indications for dialysis in acute renal failure.30
Hyperkalemia
Severe metabolic acidosis
Hyperphosphatemia/hypocalcemia
To make space for nutrition and drug administration
Failure to improve with conservative management
Specific Prevention Strategies for Selected Agents

International Bulletin of Drug Research., 2(3): 50-65
61
Table 5: Drugs altering intraglomerular hemodynamics.
Medications Prevention strategies
Angiotensin converting enzyme
inhibitors
Angiotensin receptor blockers , NSAIDs
Tacrolimus
Use analgesic with less prostaglandin activity
Correct volume depletion before initiation of drug
especially if used on chronic basis.
Monitor renal function and vital signs, following
initiation or dose escalation especially if used in- at
risk patient
Use low effective dose.
Drugs associated with tubular cell toxicity
Medications Prevention strategies
Aminoglycosides
Amphotericin B
Contrast dye
Use extended-interval dosing ,administer during active period of day,
limit duration of therapy, monitor serum drug levels and renal function
2-3 times /week, maintain trough levels ≤1mcg/ml.
Saline hydration before and after dose administration, consider
administering as a continuous infusion over 24hours, use liposomal
formulation, limit duration of therapy.
Use low-osmolar contrast in the lowest dose possible and avoid
multiple procedures in 24 to 48 hours, 0.9% saline or sodium
bicarbonate (154mEq/L) infusion before and after procedure, with hold
NSAIDs and diuretics at least 24 hours before and after procedure,
monitor renal function 24 to 48 hours post-procedure, consider
acetylcysteine pre-procedure.
Drugs associated with chronic interstitial nephropathy
Medications Prevention strategies
Acetaminophen , aspirin,
NSAIDs
Lithium
Avoid long-term use, particularly of more than one analgesic, use
alternate agents in patients with chronic pain.
Maintain drug levels within the therapeutic range, avoid volume
depletion.
International Bulletin of Drug Research., 2(3): 50-65
62
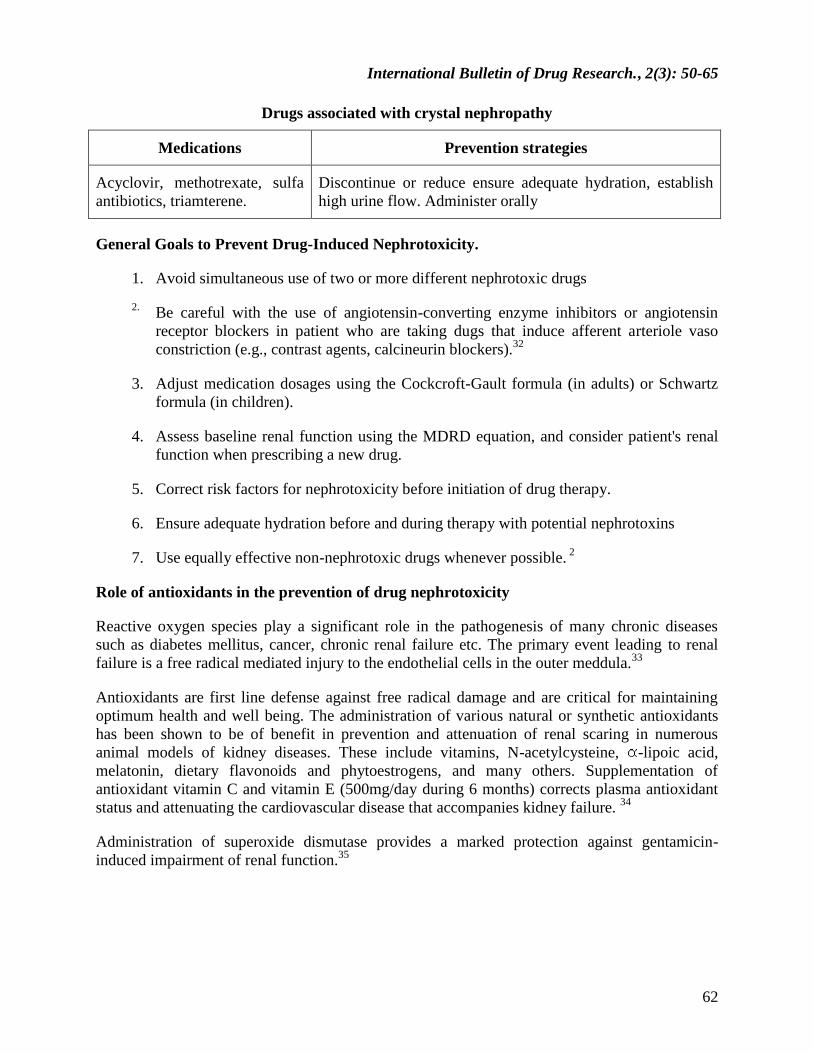
Drugs associated with crystal nephropathy
Medications Prevention strategies
Acyclovir, methotrexate, sulfa
antibiotics, triamterene.
Discontinue or reduce ensure adequate hydration, establish
high urine flow. Administer orally
General Goals to Prevent Drug-Induced Nephrotoxicity.
1. Avoid simultaneous use of two or more different nephrotoxic drugs
2. Be careful with the use of angiotensin-converting enzyme inhibitors or angiotensin
receptor blockers in patient who are taking dugs that induce afferent arteriole vaso
constriction (e.g., contrast agents, calcineurin blockers).32
3. Adjust medication dosages using the Cockcroft-Gault formula (in adults) or Schwartz
formula (in children).
4. Assess baseline renal function using the MDRD equation, and consider patient's renal
function when prescribing a new drug.
5. Correct risk factors for nephrotoxicity before initiation of drug therapy.
6. Ensure adequate hydration before and during therapy with potential nephrotoxins
7. Use equally effective non-nephrotoxic drugs whenever possible. 2
Role of antioxidants in the prevention of drug nephrotoxicity
Reactive oxygen species play a significant role in the pathogenesis of many chronic diseases
such as diabetes mellitus, cancer, chronic renal failure etc. The primary event leading to renal
failure is a free radical mediated injury to the endothelial cells in the outer meddula.33
Antioxidants are first line defense against free radical damage and are critical for maintaining
optimum health and well being. The administration of various natural or synthetic antioxidants
has been shown to be of benefit in prevention and attenuation of renal scaring in numerous
animal models of kidney diseases. These include vitamins, N-acetylcysteine, -lipoic acid,
melatonin, dietary flavonoids and phytoestrogens, and many others. Supplementation of
antioxidant vitamin C and vitamin E (500mg/day during 6 months) corrects plasma antioxidant
status and attenuating the cardiovascular disease that accompanies kidney failure. 34
Administration of superoxide dismutase provides a marked protection against gentamicin-
induced impairment of renal function.35

International Bulletin of Drug Research., 2(3): 50-65
63
Table 6: List of Antioxidants that ameliorate the nephrotoxicity of platinum compounds.36
Antioxidants Dose Route Duration Species Reference
Vitamin C or
E
100mg/kg Intraperitoneal Once Rats Kadikoylu et al.
(2004)
Xanthorrzhiol 200/kg Per oral 4 days Rats Kim et al. (2005)
Lycopene 4mg/kg Per oral 10 days Rats Atessahin et al.
(2005)
Tomato juice
+dried black
grapes
Supplement
to diet
– 6 days Rats Cetin et al.(2006)
Capsaicin 10mg/kg Per oral 6 days Rats Shimeda et al.
(2005)
Quercitin 50mg/kg Per oral 20 days Rats Francescato et
al.(2004)
Desferrioxami
ne
250mg/kg Intraperitoneal Once Rats Kadikoylu et al.
(2004)
Glutamine 300mg/kg Per oral Once Rats Mora et al. (2003)
CONCLUSION
Drug-induced kidney injury is a common condition associated with considerable morbidity and
mortality. Successful prevention requires assessing base line renal function before the initiation
of the therapy, followed by adjusting the dosage, monitoring renal function and vital signs during
therapy and avoiding nephrotoxic drug combinations. Additional characterization and validation
of individual biomarkers and biomarkers panels will ultimately result in earlier diagnosis of
kidney injury and improved prognosis of outcome.
REFERENCES
1. Gerald B, Appel M. Aminoglycoside nephrotoxicity. The American Journal of
Medicine 1990;88:16-0.
2. Cynthia N, Drug induced nephrotoxicity. Am Fam Physician 2008;78:743-0
3. Devasmitha C, Ziauddin A. Drug associated renal dysfunction and injury.
Nephrology 2006;2:2.
4. George B, Haycock. Management of acute and chronic renal failure in the new born.
Seminars in neonatalogy 2003:325-4.

International Bulletin of Drug Research., 2(3): 50-65
64
5. Fanos V, Cataldi L. Antibacterial-induced nephrotoxicity in the new born. Drug safe
1999;3:245-7.
6. Bacchetta J, Dubourg L, Juillard L et al. Non-drug-induced nephrotoxicity. Pediatr
nephrology 2009;12: 2291-0.
7. Vivek B, Paul C, Glenn M et al. Melamine nephrotoxicity: an emerging epidermic in
an era of globalization. Kidney international 2009;75:774-9.
8. Kumar, Abbas, Fausto, et al. Pathological basis of disease 2007;9: 417.
9. Xiaoging G,Chike N. How to prevent, recognize and treat drug induced
nephrotoxicity. Clinic journal of medicine 2002; 69:4.
10. Marc E. Renal injury due to environmental toxins, drugs and contrast agents. 11:11.2.
11. Roderick S, Annie P, Lisa P et al. Persistent nephrotoxicity during 10-year follow-up
after cisplatin or carboplatin treatment in childhood: Relevance of age and dose as
risk factors. European Journal of Cancer 2009;45:3213-9.
12. Susan G, Emeigh H. Assesment of renal injury in vivo. Journal of Pharmacolgical and
toxicological methods 2005;52: 30-5.
13. Muhammad S. Renal Function Tests. INV-05, Surgery investigations INV 05:30-1.
14. Andy McWilliam. Ross Macnab: Laboratory test of renal function. Anesthesia and
intensive care medicine 2009;10:296-9.
15. Abirami K, Tiwari S. Urinalysis in Clinical Practice , Journal Indian academy of
Clinical medicine 2001;2:1- 2.
16. Brian. Creatinine Clearance and Assesment of Renal Function. Australian Prescriber
2001;24:1.
17. Mitchell H, Rosner W. Renal Function Testing, American journal of Kidney
Diseases,2006; 47, No:174-183.
18. Mary W, Peter N. Contrast media-induced nephrotoxicity: identification of patients of
patients at risk and algorithms for prevention. J Vase interv Radiol 2001:12:3-9
19. Gowda S, Desai P, Kulkarni S et al. Markers of Renal function tests. North American
Journal of Medical Sciences 2010;2:4.
20. Claudio R, Rinaldo B, John A. Clinical care nephrology in pediatrics 2009;2:1606-7.
21. William J. Estimation of glomerular filtration with a new equation; Cock groft-gault
Vs MDRD4 equation. The Annals of pharmacotherapy 2007;41:475-0.
International Bulletin of Drug Research., 2(3): 50-65
65
22. Joseph V, Vishal S, Robert S et al. Next generation biomarkers for detecting Kidney
toxicity 2010;28:5.
23. Estelle M, Frank D. Impact of biomarker development on drug safety assessment.
Toxicology and Applied Pharmacology 2010; 243:167-9.
24. Kurt J, Laszlo N, lilla k et al. Discovery of metabolomic biomarkers for early
detection of nephrotoxicity. Toxicologic pathology 2009;37: 280-2.
25. Micheal A, Vishal S. Viadhya J. Biomarkers of nephrotoxic acute kidney injury,
Toxicology 2008; 245:182-3.
26. Roger Walker, Cate W. Acute Renal Failure. Clinical Pharmacy and Therapeutics.
Fourth edition chapter 18:250-3.
27. Wilfred D. Basics in Clinical Nutrition; Nutritional support in renal; disease. The
European Journal of Clinical Nutrition and metabolism2010;5:54-7.
28. Normal J, William E, Jhon J et al. Management of acute renal failure in the pediatric
patient. Hemofiltration versus hemodialysis, American Journal Kidney disease
1997;30:84-8.
29. George B. Management of acute and chronic renal failure in the new born seminars in
neonatology 2003;8:325-4.
30. Heather S, John D. Is parentral nutrition therapy of value in acute renal failure
patients? American Journal of kidney Disease 1995;25:96-2.
31. Emmanuel A. Clinical Features of Drug induced nephrotoxicity. Critical Care
Nephrology;58:317-8.
32. Shelgikar P, Deshpande K, Sardeshmukhi A et al. Role of oxidants and antioxidants
in ARF patients undergoing hemodialysis. Inadian J Nephrol 2005;15: 73-6.
33. Ratna P, Vasudha K. Antioxidant vitamins in chronic renal failure. Biomedical
research 2009;20:67-0.
34. Radhakrishna B, Norishi U, MD, Patric D et al. Oxidant Mechanism in Toxic Acute
renal failure, Physiology and cell biology update. American journal of kidney Disease
1997;29:465-7.
35. Badreldin H, Mansour S. Agents ameliorating or augmenting the nephrotoxicity of
cisplatin and other platinum compounds: A review of some recent research. Food and
chemical toxicology 2006;44:1173-3.