dr.shahnaz ahmadi iran university of medica science
TRANSCRIPT

Placenta previaPlacental abruption
Dr.shahnaz Ahmadi
Iran university of medica science

Antepartum Hemorrhage
• Third-trimester bleedingObstetric Placental Previa Placenta Abruption Uterine Rupture vasa previa : Fetal Vessel RuptureNo obstetric: Acute vaginitis/cervicitis,
Cervical polyp, Cervical cancer, Trauma

Placenta previa
Definition
• Placenta previa:The inferior edge of placenta load at
the lower uterine segment, or even reach the internal cervical os after 28 weeks gestation.

Risk factors
cesarean delivery ,this risk rises as theNumber of PC/S
ART Maternal smoking
RCOG

The mid pregnancy routin fetal anomali should include localization of placenta
The term placenta previa should be used when the placenta lies directly over internal os.
TVS for the diagnosis of P.P is superior to transabdominal and transperineal approaches.
Asymptomatic placenta previa
• Determine whether the previa resolves with increasing gestational age
• Determine whether placenta is also acreta
• Reduce the risk of bleeding
• Optimal time for cesarean
Monitoring placental position
If the placenta edge is over or <2 cm from the internal os in the second trimester : follow up at 32 weeks
At 32 weeks : placenta edge >=2 cm ……..normal
Over or <2 cm ……..follow up at 36 weeks
At the 36 week: if not over but <2 cm , risks and benefits of a trial of labor should be discussed with the patient
Color and pulsed doppler are useful to confirm the position of the placental edge and rule out vasa previa
The placenta accreta should be excluded

placenta previa
placenta previa

central placenta previa
Reducing risk of bleeding
Avoid any sexual activity
Avoid digital cervical examination
Avoid moderate and strenuous exercise, heavy lifting (20 pounds) , standing for prolonged periods of time(4h.)

Screening for growth restriction
• No or minimally incresed risk of iugr

Inpatient versus outpatient maternal monitoring
Women who have not experienced antepartum bleeding at low risk and can generally be managed on outpatient until vaginal bleeding occurs or scheduled for C/S
However patient specific risk factors ; short cervical length , rapid cervical shortening ,inability to get to the hospital promptly , lack of home support in case an emergency .
SMFM does not recommend routine CL screening in the late preterm period for PP
Antenatal corticosteroid :48 h. before C/S ( GA: <37 wk.)

Timing of delivery
• C/S at 36+0 to 37+6 : uncomplicated placenta previa

Acute care of bleeding placenta previa
• These women should be admitted to the labor and delivery
Goal: maintain maternal hemodynamic stability /determined if emergency C/S delivery is indicated

Maternal and fetal assessment
• BP,HR,RR,O2 satu. ,U/O ,closely monitoring of( tachypnea, tachycardia,hypotension,low oxygen saturation,and air hunger ……..hypovolemia)
• FHR • LAB test ; CBC,BGRH and antibody screen
,cross match 2-4 units of PRBC
• If suspected coexistent abruption or with heavy blood loss resulting in hemodynamic instability : check fibrinogen ,PT ,PTT

STABILIZATIONIntravenous access and crystalloid
(urine output :30ml/hour )
Transfusion (delivery is not imminet:Hb:10g/dl , delivery is imminet:Hb:8g/dl )
Do not administer tocolytic drugs to actively bleeding patients
Tranexamic acid is not administered before delivery

Indication for delivery C/S is indicated for :
• Active labor
• Nonreassuring fetal heart rate
• Severe and persistent vaginal bleeding
• Significant V.B after 34 weeks of gestation

• Suggest a course of MgSO4 therapy for neuroprotection in patients with preterm 24 to 32 weeks

Expectant management of stable patients after bleeding Symptomatic women less than 34 weeks of gestation who
are hemodynamically stable or quickly stabilized and have a normal FHR are candidates for expectant management
Antenatal corticosteoids ( administerd to symptomatic women 23+0 -33+6 and would give to women whose first bleeding at 34+0 to 36+6)
Correction of anemia ( oral or parenteral iron)
Anti-D immune globulin
Fetal assessment (there is no proven value of NST or BPP in asymptomatic PP.)
Tocolysis :do not use tocolytic drugs in PP. , may use tocolytic while administring a course bethametasone). INDOMETHACI is not used
Cerclage

Discharge criteria • Women with P.P whose bleeding has
stopped for a min. 24 h. and who have no other pregnancy
• To returne hospital 20 min
• Be reliable
• Maintain modified bed rest at home
• Have an adult companion available 24 h/day

Management of coexistent
• PPROM
• Timing of delivery :in patient with stable PP…….36+0 to 37+6)
emergency C/S:
• Labor
• Severe and persistent V.B
• Significant V.B after 34 weeks
Cesarian delivery :
• Preparation
• Management of the placenta


Differential diagnosis• Placental abruption
• Disruption of vasa previa
• Cervical polyp or erosion
• Cancer of cervix

Placental abruption

Clinical Features
Abruptly,persistent abdominal pain with vaginal bleeding
Maternal compromise/ shock(Volume of vaginal bleeding not correspond to patient condition)
Anomaly of fetal condition
The uterus touched hard with pain
The size of uterus is bigger than it should be in that gestation age

• Should be evaluated proptly on a labor

Sonography
Differential diagnosis
• Placental previa
• Uterus rupture
Following actions
• Continuous fetal heart rate monitoring
• Secure intravenous access
• Closely monitor the mother’s hemodynamic status (HR,BP,U/O,RR)
• Quantify blood loss
• CBC,BGRH,fibrinogen, PT,PTT ,Cr,liver function ,lee white test

• In women who continue to have signs of moderate or sever abruptin ,notify the blood bank.
• If bleeding continues and the estimated 500 to 1000 ml, we transfuse blood

Transfusion goals • HCT>25-30%
• PLT>=75000
• Fibrinogen>=100mg/dl
• PT , PTT <1.5 times control

• Notify the anesthesia team .
• Mgso4 for <32 weeks
• Antenatal corticosteroids <34 weeks
• Keep the patient warm
• oxygen

• The most important factor for delivery versus expectant management :
• Gestational age
• Fetal and maternal status

• Abruption severe is accompained by >=1 of the following:
• Maternal:DIC, hypovolomic shock, need for transfusion or hysterectomy,renal failure ,death
• Fetal: nonreassuring fetal status, IUGR, need for preterm birth, death

Approach • Dead fetus : minimizes the risk of
maternal morbidity or mortality ( placenta seperation is greater 50 percent )
• Unstable mother : C/S is best option
• Stable mother : vaginal delivery is preferable.

Live fetus • Category III
• Category II
• Reassuring fetal status

Less than 34 weeks • Fetus and mother are stable :
• Administer corticosteroids (23-34)
• Tocolysis (tachycardia ,hypotension)
• Antenatal fetal assessment(NST,BPP weekly)
• Hospitalization :48h without vaginal bleeding)
• Delivery

Delivery• Withouth any symptom : 37to38
weeks,because increased risk of stillbirth( do not amniocentesis to document fetal lung maturity)
• Delivery befor 37 : IUGR, preeclampsia, PROM,NST nonreactive)
• ABG
• Send placenta to pathology
34-36 weeks of gestation • Deliver ……..acute abruption
• Expectant …….. Light bleeding,normalV.S. , uterine quiescence, without tenderness ,normal FHR

36 WEEKS TO TERM GESTATION
• Vaginal delivery is preferable.
Oxytocin and amnitomy

Postpartum care • Oxytocin infusion
• Vital sign, blood loss ,urine output ,uterine size, Hb, coagulation studies,
Future pregnancies• Recurrence risk.
• There are no laboratory screening tests( antiphospholipid antibodies or inherited thrombophilia is not indicated )
• Routine fetal antepartum is not helpful
• Timing of deliver

• Abruption in prior pregnancy and who have no bleeding ,IUGR, preeclampsia…..spontaneous labor or 40-41 w
• Who had perinatal death or more than one prior abruption ..36-37 after documentation of fetal lung maturity ( lamellar body >50000/microliter

Uteroplacental apoplexy:
widespread extravasation of blood into the uterine musculature and beneath the uterine serosa

Complications
DIC,dysfunction of coagulation
Post partum hemorrhagic/shock
Amniotic fluid embolism
Acute renal failure
Fetal death

Vasa Previa Rarely reported condition in which
the fetal vessels from the placenta cross the entrance to the birth canal
Reported incidence varies, but most resources note occurrence in 1:2500 pregnancies
Associated with a high fetal mortality rate (50-95%) which can be attributed to rapid fetal exsanguination resulting from the vessels tearing during labor

Risk Factors for Vasa Previa
Bilobed and succenturiate placentas
Velamentous insertion of the cord
Low-lying placenta and/or placenta previa
Multiple gestation
• Pregnancies resulting from in vitro fertilization
• Palpable vessel on vaginal exam
• Maternal history of uterine surgery

Vasa Previa - Management When vasa previa is detected prior to labor, the
baby has a much greater chance of surviving
It can be detected during pregnancy with use of transvaginal sonography, preferably in combination with color Doppler
Some researchers have suggested screening color Doppler in the second trimesters of patients with risk factors present on routine 20 week ultrasound
Vasa Previa - Management• When vasa previa is diagnosed prior to labor,
elective caesarian delivery can save the baby’s life
• The International Vasa Previa Foundation recommends hospitalization in the third trimester, delivery by 35 weeks, and immediate blood transfusion of the infant in the event of a rupture
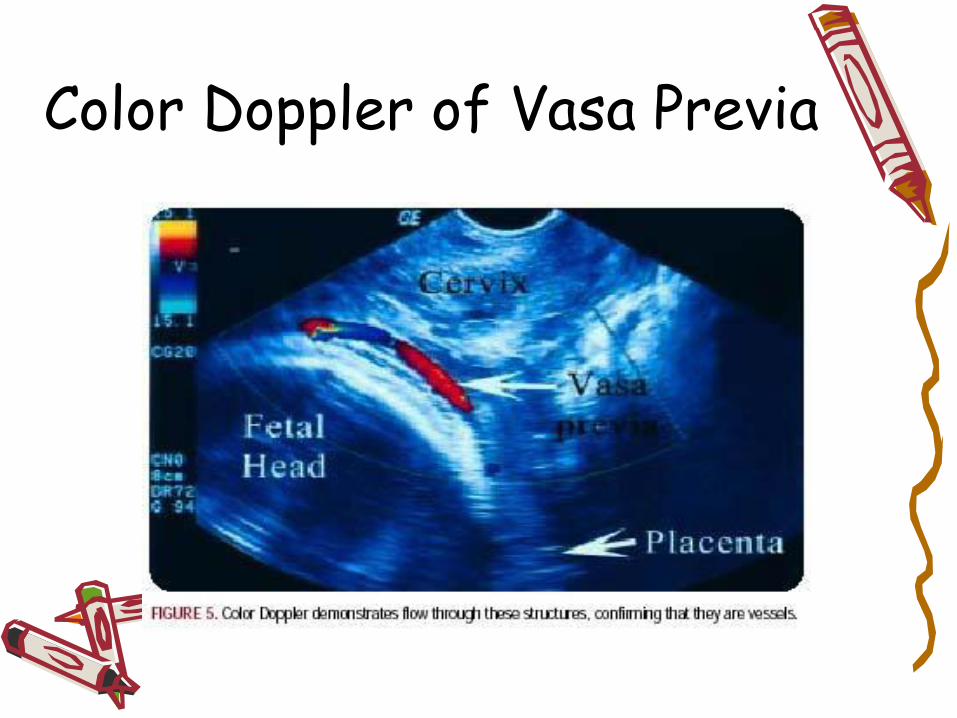
Color Doppler of Vasa Previa

Vasa Previa - Diagnosis in the Acute Setting
• Clinical scenarios suggesting vasa previa:
-significant bleeding at the time of membrane rupture
-fetal heart rate abnormalities associated with vaginal bleeding
-palpable vessels on vaginal examination
