dr. robert a. branch, md frcp
DESCRIPTION
“Guiding Community-Based Participatory Research in health for disadvantaged and minority high school students, focusing on science, math, health, and technology .”. Dr. Robert A. Branch, MD FRCP. Objectives. The Problem H ealth Education inadequate Literate W orkforce The solution - PowerPoint PPT PresentationTRANSCRIPT

“Guiding Community-Based Participatory Research in health for disadvantaged and minority high school students, focusing on
science, math, health, and technology.”
Dr. Robert A. Branch, MD FRCP

ObjectivesObjectives
• Uniquenesso Tiered Diffusion
Communication o Application Psychologyo Adolescents
• Vehicles for Changeo Knowledge Brokerso Continuous Self-Monitoring
• Feasibilityo Rural West Virginia
• Career Development• Adolescent Health• Community Health
• The Problemo Healtho Educationo inadequate Literate Workforce
• The solutiono Pitt-Bridgeo Salutogenesis (origin of
health)o Micro-Community-Based
Participatory Research (CBPR)
Can We Apply These Concepts to Pittsburgh?

Who is Robert A. Branch?Who is Robert A. Branch?
Call me ‘Bob’
• Born in Nairobi , Kenya in 2nd world war
• Father is a physiciano from St. Lucia
• Mother is a nurseo from England
• Raised in Nigeria• Schooled in England
• Bristol Medical School o 17 years oldo qualified by 22 years
• Internal Medicine in UK
• Emigrated 1975 • Vanderbilt for 17 years
o Clinical Pharmacologist
• Pittsburgh for 22 yearso Clinical Translational Scientist
*An Educator for over 50 years*

The US Health: The US Health: An International An International
PerspectivePerspective•Shorter Lives, Poorer Health
o US National Research Councilo Congress Requested Institute of Medicineo January 2013
• US Health Disadvantages
“Knowing is not enough; we must apply. Willing is not enough; we must do.”
-Johann Wolfgang von Goethe
The CauseThe Cause
“Even if health care plays some role, decades of research have documented health is determined by more than health care.” -2006 Report on Comparison of UK and US
Social Gradient ---------------------------- Income Inequality
United States•“My right to choose.”•Individualism
United Kingdom•“We are all in this together.” •Collectivism
At every social level UK>US

The Problem: Mal-The Problem: Mal-Adaptive Behavior Adaptive Behavior Related DiseasesRelated Diseases
Worse outcomes than 17 other countriesSpends greater than 2x per capita than other countries
Acute Events•Adverse Births•Vehicular Accidents•Violence•STDs
Chronic Events•Obesity•Type II Diabetes•Cardiovascular Disease•Chronic Pulmonary Disease•AIDS•Lung Cancer

Creating Change in Creating Change in HealthHealth
Who is to create change?•Government
o Incapable of Action
•Philanthropyo Inadequate Funding
•Advocacyo Inadequate Federal and State Funding
We need to find a new way!
Public health. Confronting the Sorry State of U.S. Health.Bayer R, Fairchild AL, Hopper K, Nathanson CA.
Science. 2013 Aug 30;341(6149):962-3. doi: 10.1126/science.1241249.PMID: 23990546

Bridging the GapBridging the Gap
Individual
Community
Institutional
Interpersonal
Federal
-
Im
pact
+- T
ime
+

Creating Change in Creating Change in HealthHealth
Identify the Causeo Misdistribution
• Money• Knowledge of Community• Behavior of Family
Involve Everyoneo Communityo Educatorso Health Care Providerso Policy Makers
Target the Most Vulnerableo Povertyo Minoritieso Ruralo Urban Communities
Use Adolescents•Most Flexible•Technologically Advanced•Already Established in the Community•Responsible

Seismic Changes in STEM Education
• Need for changeo National decrease in competitivenesso Concern of future high-tech work forceo Disgrace over differential State Standards
• Questions raised o What do we teach? What is learned?o When do we teach it? When is it learned?o How do we teach? How is it learned?
• Mathematicso The Common Core State Standards
• http://www.corestandards.org/resources/key-points-in-mathematics
• Scienceso The New Generation State Standards
• http://www.nextgenscience.org/next-generation-science-standards
Pennsylvania conservative resistance to change

Pitt-Bridge Vision and Pitt-Bridge Vision and GoalsGoals
• Visiono Provide a “Bridge" Between Health Sciences and STEM Disciplineso Learn How to Learno Learn How to Change Behavior
• Goalso Motivate minority and low-income high school students to enter higher
education o Pursue careers in STEM fields, particularly in health sciences-related
occupations.o Family improvement of healtho Self-improvement of health

CBPR Learning Program CBPR Learning Program Health Science ClubsHealth Science ClubsA Transformative Education Health Science
Program: Requires Integration of Essential Core Concepts
•Salutogenesis (origin of health- for community)•Adaptive Adolescent Hypothesis •Micro and macro CBPR•Application of cognitive psychology in scientific method •Community Research Knowledge Broker (CRKB)•Tiered Diffusion model of communication •Adolescents as family health care coaches

SalutogenesisSalutogenesis
*Origin of Health & Wellness for All*
Time
Vaccination
Prevention
Actionable Knowledge Concepts
Prophylaxis of Chronic Disease

Adaptive Adolescent Adaptive Adolescent Hypothesis Hypothesis
Brain Maturation•Burst of brain growth and change in structure
o Pruning of dendriteso Development fast track neuronal connections.
Wave of Brain Maturation •1st Step: 12 years
o Dexterity
•2nd Step:15-19 yearso Concept Integration
•Final Step: 21yearso Executive Decision Making
Source: J. Giedd, Nature 442, 865-867 (24 August 2006)

Adaptive Adolescent Adaptive Adolescent Hypothesis Hypothesis
Implication confers evolutionary benefit •Risk taking may be an advantage in times of peril
Ability to use reasoned choice to not conform to culturally acquired mal-adaptive behavior’s may be our best option for survival.

Community-Based Community-Based Participatory ResearchParticipatory Research
Community-Based Participatory Research: A
Capacity-Building Approach for Policy Advocacy Aimed at Eliminating Health
Disparities
Israel BA, Coombe CM, Cheezum RR, Schulz AJ, McGranaghan RJ, Lichtenstein R, Reyes AG, Clement J, Burris A. Am J Public Health. 2010 Nov;100(11):2094-102. doi: 10.2105/AJPH.2009.170506. Epub 2010 Sep 23. PMID: 20864728 PMCID: PMC2951933
Core Values
•Mutualityo Sharing by Members
•Equityo Governanceo Accountability
•Trusto Good Faith From All Partners

Core Principles of CBPRCore Principles of CBPR
• Long-Term Commitment
• Equitable Partnership in All Phases
• Emphasizes Local Relevance
• Builds on community strengths and resources
• Promotes Co-Learning and Capacity-Building

Micro-CBPR for Student Micro-CBPR for Student InvestigatorsInvestigators
Micro-CBPR Scientific Projecta)Subject Areab)Backgroundc)Questiond)Design & Approvale)Implementationf)Analysis & Inferenceg)Presentation
My ‘FIRST’ Health ProjectFunInnovative•Individual•IterativeRelevant•Respect•RelationshipsScientificTransformative
If a common data collection tool is used, the sum of multiple Micro-CBPR generates bonefide CBPR

Can ‘WE’ do better? All Questions Require, Comparisons, Quantitation, Analysis
Who are ‘WE’?•Who is the We?•Where do We live?•What is our environment?•What are our health problems?
Why do ‘WE’ do what we do?•How do We learn?•How do We make decisions?•How do We change?

Adverse, Culturally-Based,
Behavior
Adolescent-LedMicro-CBPR
Projects
AdaptionBehaviors
Ausubel’s Theory of Meaningful
Learning
Prochaska’s Trans-Theoretical Model of
Behavior Change
Learning to LearnCommunity Science
Project Change in Behavior
The potential for the CBPR Learning Paradigm to enhance health
A Communi
ty in Trouble
ImproveCommuni
tyAwarenes
s
Potential to Enhance Potential to Enhance HealthHealth

Clinical Research Clinical Research Knowledge BrokerKnowledge Broker
A New Community-Based Career Track
Who are they?•Recruited from senior STEM teachers with higher pay•Live in and know the local community•Receive special training in
o Ethicso principles of CBPRo study designo domains of health sciences interest
What do they do?•Organize integration of club activities•Mentor club teachers•Organize club group symposia•Maintain and evaluate quality

Tiered Diffusion Bi-Tiered Diffusion Bi-Directional Directional
CommunicationCommunication
Pitt-Bridge
Academic Medical Centers
Knowledge Brokers
STEMTeachers
Science Club
Students
Science Club
Families
*Science Club= 1 Teacher / 10 Students
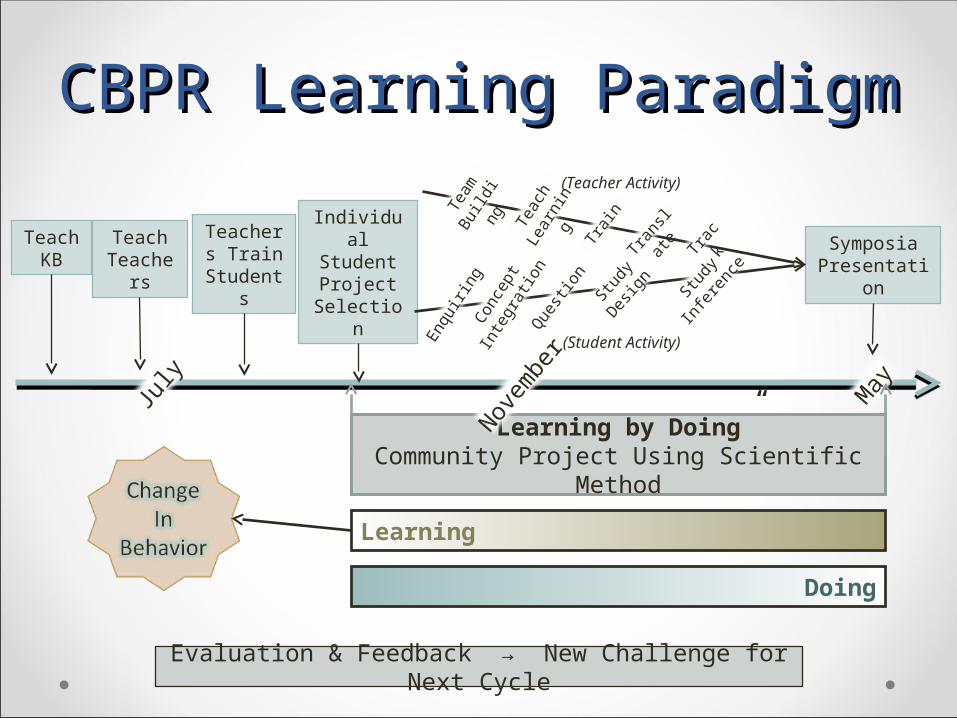
CBPR Learning ParadigmCBPR Learning Paradigm
“Learning by Doing”Community Project Using Scientific Method
July
November
May
TeachKB
TeachTeachers
Teachers Train
Students
Individual Student Project
Selection
Symposia Presentation
Enqu
iring
Conc
ept
Inte
grati
onQue
stion Stu
dyDes
ign Study
Inferen
ce
Doing
Learning
Evaluation & Feedback → New Challenge for Next Cycle
(Student Activity)
Team
Bu
ildin
g
Teac
h Le
arni
ng
Train
Trac
k
Tran
slate
(Teacher Activity)

Concept Map Networking Concept Map Networking ApproachApproach
Study HypothesisStudy Hypothesis
Study Rationale
TrainingTraining Design & ConductDesign & Conduct
HomeEconomics
HomeEconomics
ObesityEpidemicObesity
Epidemic
Sociology ofFamily
Sociology ofFamily
EthicsEthics CBPRCBPR
ResearchRegulationResearch
Regulation
InterventionIntervention StructureStructure ConductConduct
Metabolic SyndromeMetabolic Syndrome EnergyEnergy
DiabetesDiabetes
ComplicationsComplications
CardiovascularDisease
CardiovascularDisease
HeartAttackHeartAttack
StrokeStroke
EnergyBalanceEnergyBalance
ExerciseExercise DietDiet
FatFat
CarbohydrateCarbohydrateProteinProtein
NutritionNutrition
FoodLabelsFood
Labels
EducationProgram
EducationProgram
PortionSize
PortionSize
Pre/PostCohort
OfMothers
Pre/PostCohort
OfMothers
EndpointMeasuresEndpointMeasures
LogisticsLogistics
DataCollection
DataCollection
DataOrganization
DataOrganization
DataAnalysis
DataAnalysis

CBPR Learning Paradigm CBPR Learning Paradigm
• Educational Perspectiveo Integrate Common Core State Standards (CCSS) and the Next
Generation Science Standards (NGSS) by expanding into health sciences
• Student Perspectiveo Involve hands-on experiences in ethics, science-based problem-solving,
leadership, team-building, decision-making, and concept presentation in health sciences
• Community Perspectiveo These students will gain the knowledge, skills, and ability to become
family health care educators to promote wellness.

Feasibility ModelFeasibility Model• Encourage
o Entrepreneurshipo Self-Relianceo Team Worko Learn How To Learno Self Expectation
• Missiono Go To Collegeo Succeed in Career Developmento Improve Community Health
Health Science & Technology Academy (HSTA)
o Community organizations in 26 counties
o 76 Science clubs for high schoolo 4 Community Research Associateso Links to WVU and Pitt

HSTA Club EnrollmentHSTA Club Enrollment
2011 Enrollment Statistics
1st Generation College 53%
Food Voucher Aid 40%
Rural 73%
African American 30% (3% Statewide)
Total 786 Students
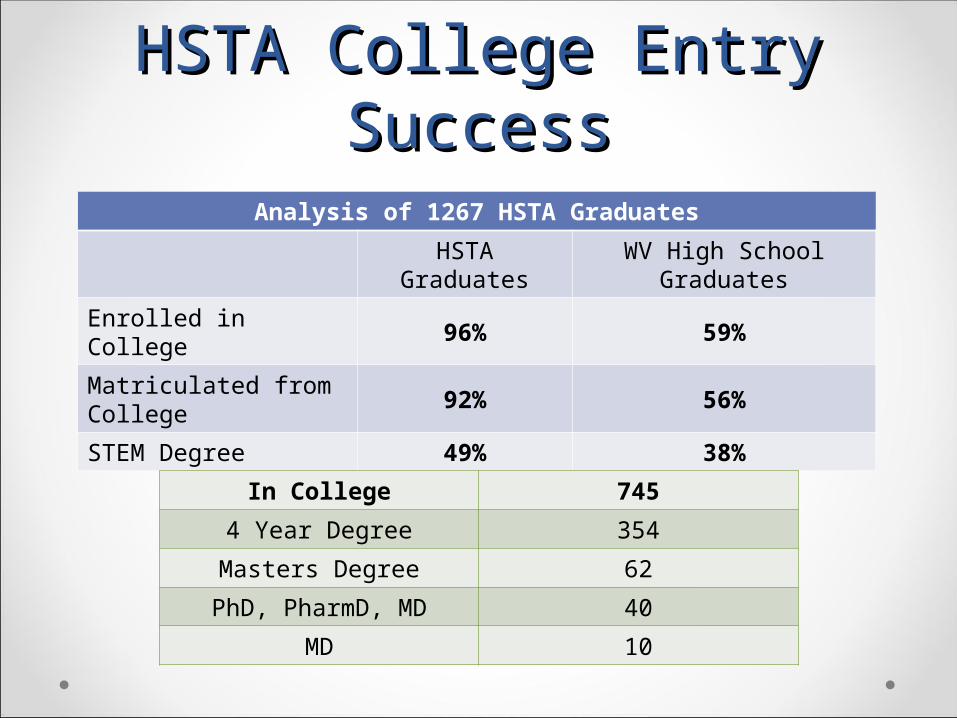
HSTA College Entry HSTA College Entry SuccessSuccess
Analysis of 1267 HSTA Graduates
HSTA Graduates
WV High School Graduates
Enrolled in College 96% 59%
Matriculated from College
92% 56%
STEM Degree 49% 38%
In College 745
4 Year Degree 354
Masters Degree 62
PhD, PharmD, MD 40
MD 10

Obesity in West VirginiaObesity in West Virginia
Subjects enrolled in 2007

Projected Mean BMI for Adolescent Cohort
BMI in HSTA family sample populations of West Virginia in subjects as they age from the present time. The slope of projections is estimated assuming the linear increase observed from the BRFFS study results from WV between 1985-2007 remains unchanged
Prevalence of Obesity Prevalence of Obesity and Diabetes (2007)and Diabetes (2007)

Community-Based Community-Based Participatory ResearchParticipatory Research
2007 2008 2009 2010 2011 2012 2013
Adults 648 56 356 40 125 103 100
% Obese (BMI>30)
40 35 41 42 42 39 40
BMI
29 +/- 6 29 +/- 7 29 +/- 7 32 +/- 12 29 +/- 7 29 +/- 7 31 +/- 9(mean +/- SD)
Adolescents 300 253 132 53 57 40 52
Age
15 +/- 2.7 14 +/- 3.4 14 +/- 3.2 16 +/- 2.2 14 +/- 3.2 14 +/- 3.2 14 +/- 3.3(mean +/- SD)
BMI
23 +/- 6 23 +/- 6 24 +/- 6 24 +/- 6 23 +/- 5 23 +/-6 24 +/- 7(mean +/- SD)
CDC Reported 6% increase in adult BMI 2007-2012

Lessons Learned in Lessons Learned in Community HealthCommunity Health
• Transition of HSTA coordinator to Community Research Knowledge Broker
• Adolescents can conduct Micro-CBPR
• Integration of related Micro-CBPR permits Community CPBR
• Multiple Micro-CBPR projects influences community behavior for health care condition

Proposed Plan of ActionProposed Plan of Action
The Pittsburgh BridgePhased Introduction
•Phase 1: Initiate and Learn
•Phase 2: Refine and Consolidate
•Phase 3: Expansion

PublicationsPublications• Branch RA, Paulsen S, Hanks S, Obesity Management Organized by Adolescents in Rural
Appalachia, JHUP Fall 2014 (in press)
• Branch, R., Chester, A., Morton-McSwain, C., Hanks, S. Udin Al Ayubi, S., Bhat Shelbert, K., Brimson, P., Buch, S., et al. A Novel Approach to Adolescent Obesity in Rural Appalachia of West Virginia: Educating Adolescents as Family Health Coaches and Research Investigators. Topics in the Prevention, Treatment and Complications of Type 2 Diabetes." Mark B. Zimering (ED) (2011). ISBN:9780953-307-590-7, InTech.
• Bardwell, G., Branch, R.A.,Buch, S., Cecchetti, A.,Chester, A., Groark, S.,Morton, C., Pancoska, P., Paulsen, S.,Vecchio, M." (2009, October).Feasability of Adolescents to Conduct Community Based Participatory Research on Obesity and Diabetes in Rural Appalachia." Clinical Translation Science.2(5)
• Chester, A, and R.A. Branch. Community Based Participatory Clinical Research in Obesity by Adolescents; Pipeline for Researchers of the Future. Clinical Translation Science. (2009).
• Pancoska P, Branch RA, Buch S, Cecchetti A, Parmanto B, Vecchio M et al. (2009) Family Networks of Obesity and Type 2 Diabetes in Rural Appalachia. Clinical and Translational Science 2(6):413-421. http://www.wiley.com/bw/journal.asp?ref=1752-8054