dr. richard e. pearl patient registration...
TRANSCRIPT

Dr. Richard E. Pearl
PATIENT REGISTRATION FORM
Please fill in completely Today's Date: Last Name: First Name: MI: Address: Apt. /Floor: City: State: Zip: Home Tel #: Cell Tel #: Work Tel #: Email address: Date of Birth: Sex: M F Social Seeurity#:
Marital Status (circle): Single Married Widowed Divorced Other Spouse's name: Home Tel #: Cell Tel #: Work Tel #:
Family Doctor: Address: City: Referring Physician: Address: City:
Tel #: State:
Zip: Tel #: State: Zip:
Emergency Contact Name: Relationship to Patient (circle): Spouse Parent/Guardian Other Home Tel #: Work #: Cell #:
Employer Information Occupation: Employer Address: Are you still working? (Circle): Yes or No Are you still working, part-time?
Employer Name: Employer Phone#: if no, what was your last date on the job? Full-time?
Insurance Information: Private Health Insurance Primary Insurance: Subscriber M #: Group #: insured Name: Relation to Patient: Social Security #: Date of Birth: Telephone # of Pol icy Holder: Insured address if different from above address: Secondary Insurance: Subscriber BD #: Group #: Insured Name: Relation to Patient: Social Security #: Date of Birth:
is this a Workman's Compensation accident? (Circle one) Yes No is this a No Fault Accident? (Circle one) Yes No If your problem is due w an accident, please note the accident date: Please provide insurance information on page 2.
Dr. Richard E. Pearl
Authorization, Assignment and Fee Agreerrrent
Richard E. Pearl, M.D., P.C., or any other medical doctors or companies associated with him, all referred
to as "Providers", are authorized to furnish information to providers of health services insurance or
benefits, or their representatives. In return for me and my dependents receiving medical services without
immediate payment, I assign now and forever, to Providers, any money due me from any source (except
Workers' Compensation payments and benefits) for these medical serVices, plus my right to sue those
responsible for payment if they do not pay what they owe. If I have and do not prosecute a Workers"
Compensation or No-Fault claim, or if payment under these types of claims is denied for any reason other
than Providers fees not meeting the applicable fee schedule, I agree to pay the usual and customary fees
for treatment as listed on the back of this paper, which I have read, to the extent permitted by law. I
understand that I am responsible for any amount not covered by insurance or benefits, and all reasonable
legal fees spent by Providers to collect the amount I owe. I understand that bills will be provided by
request only. I am responsible to provide insurance information to Providers. Providers, and Providers
only, can submit any dispute there may be under this Authorization, Assignment and Fee Agreement to
binding arbitration under the American Arbitration Association's New York, New York office.
Patient Signature I Date
FOR MEDICARE PATIENTS
I request that payment of authorized Medicare benefits be made on my behalf to Richard E. Pearl.
services furnished to me by the provider. I authorize any holder of medical information about me to releas Centers for Medicare and its agents any information needed to determine these benefits or the benef its
related services.
Patient Signature / Date

Dr. Richard E. Pearl
Notice of Privacy Practices Policies
Richard E. Pearl, M.D., P.C., is committed to protecting the privacy of their patients. It is the intent of the above named entities to comply with the Privacy Rule promulgated purSUant to the Health Insurance Portability and Accountability Act of 1996 ("HIPPA") and applicable New York State Law. The office of Richard E.Pearl, M.D, P.C.:
I. Makes its Notice of Privacy Practice's available upon request to any person. 2. Provides the Notice electronically or in person no later than the date of the first service delivery
after October 9, 2008 (including serviced delivered electronically). 3. Makes the Notice available at its offices for individuals to take with them upon request. 4. Posts the Notice in a clear and prominent location where it is reasonable to expect the individuals
receiving services to be able to read the Notice.
By signing below, I hereby acknowledge that the full privacy policy has been made available to me and will continue to me upon my request.
Patient Signature:
Date:

Authorization to Use or Disclose Health Information
Patient Name: Chart Number:
1. I authorize the use or disclosure of the above named individual's health information as described below. The following individual and organization are authorized to make the disclosure: Richard E. Pearl, M.D., P.C. As well as any health care provider Which I am referred to by the above. The type of information to be used or disclosed is as follows:
Problem list Medication list All histories and discharge summaries All lab results All x-ray and imaging reports All consultation reports and films The entire record relating to my treatment
4_ I understand that the information in my health record may include information relating to sexually transmitted disease, acquired immunodeficiency syndrome (AIDS), or human immunodeficiency virus (HIV). It may also include infoi illation about behavioral or mental health services, and treatment for alcohol and drug abuse.
5. The information identified above may be used by or disclosed to
This information for which I'm authorizing disclosure will be used for a liability claim.
7. I understand that I have a right to revoke this authorization at any time. I understand that if I revoke this authorization, I must do so in writing and present my written revocation to the health management department. I understand that the revocation will not apply to information that has been released in response to this authorization. I understand that the revocation will not apply to my insurance company when the law provides my insurer with the right to contest a claim under my policy.
S_ This authorization will expire five years from the date on which it was signed.
9. 1 understand that once the above information is disclosed, it May be redisclosed by the recipient and the information may not be protected by federal privacy laws or regulations .
10. I understand authorizing the use or disclosure of the information identified above is voluntary. I need not sign this form to ensure healthcare treatment.
Signature of patient or legal representative Date signed by legal representative, relationship to patient

Dr. Richard E. Pearl
PLEASE READ CAREFULLY AGREEMENT AS TO RESOLUTION OF CONCERNS
"I", "Patient/Guardian" shall be understood to mean . (Name of Patient or Guardian).
"Physician" shall be understood to mean Richard E. Pearl, M.D. I understand that I am entering into a contractual relationship with the physician for
professional care. I further understand that meritless and frivolons claims for medical malpractice have an adverse effect upon the cost and availability of medical care to patients and may result in irreparable harm to a medical provider. As additional consideration for professional care provided to me by the physician, I, the Patient/Guardian, agree not to initiate or advance, directly or indirectly, any meritless or frivolous claims of medical malpractice against the Physician.
Should I, initiate or pursue a meritorious medical malpraCtice claim against Physician, I agree to use as expert witnesses (with respect to issues concerning the standard of care), only physicians who are board certified by the American Board of Medical Specialties in the same specialty as the Physician.. Further, I agree that these physicians retained by me or on my behalf to be expert witnesses will be members in good standing of the American Academy of Orthopedic Surgeons_
I agree the expert will be obligated to adhere to the guidelines or code of conduct defined by the American Academy of Orthopedic Surgeons.
I agree to require any attorney I hire and any physician hired by me or on my behalf as an expert witness to agree to these provisions.
In further consideration, Physician also agrees to exactly the same above-referenced stipulations.
Each party agrees that his/her counsel shall have the right and be free to depose the other party's expert witness (es) at least 120 days before any scheduled trial date.
Each party agrees that a conclusion by a specialty society affording due process to an expert will be treated as supporting or refuting evidence of a frivolous or meritless claim. Patient/guardian and physician agree that this Agreement is binding upon them individually and their respective successors, assigns, representatives, personal representatives, spouses, and other dependents.
Physician and patient/guardian agree that these provisions apply to any claim for medical malpractice whether based on a theory of contract, negligence, battery, or any other theory of recovery. Patient/guardian acknowledges that he/she has been given ample opportunity to read this agreement and to ask questions about it.
Physician Patient/Guardian
Effective Date of Treatment Date of Signature

Dr. Richard E. Pearl
Medical Questionnaire Patient Name: Date: Date of Birth: Age: Sex NAME OF REFERRING PHYSICIAN ONLY: Would you like a copy of today's visit sent to your Family Doctor? (Circle) Yes or No
Past Medical History/Family History (Please check any of the following conditions that apply to yourself or your family
Family Self Family Self Diabetes Heart Problems High Cholesterol
Thyroid Disorder
Hypertension Asthma Strokes Seizures
If other please specify:
Allergies Please check any of the following allergies that may apply to you)
Aspirin Seasonal Dust Mites Sulfa Drugs Penicillin No Known Allergies
If other please specify:
Medications (Please list any medication you are currently taking including vitamins and all herbal
supplements)
Medication Dosage
Notes
Additional medications:

Social History (Please check if any of the following apply to you)
Alcohol use
Drug use Tobacco use
Other:
Surgical History (Please list any surgeries you underwent in the past)
Procedure
Year Notes
Review of Systems (Please check if any of the following apply to you)
Hypertension Neurological Disorders, i.e. strokes, seizures High Cholesterol Cancer Cardiac Disease Eye Disease
Respiratory Disease Arthritis or Gout Bowel Problems/Disease Diabetes Stomach Ulcers/Hernias Thyroid Disease
Liver Disease Kidney/Bladder/Prostate Disease Bleeding Disorders/Anemia Abnormal Vaginal Bleeding/GYN Disease
Anxiety, Depression or other condition Anesthesia Problems Dentures, Braces, Loose Teeth/Caps, Bridges Have you had a flu vaccine?
Have you had the Pneumococcal Vaccine? Have you had a Blood Transfusion? Date of Blood Transfusion Have you had a reaction to a Blood
Transfusion? Do you have a Healthcare Proxy? First date of Last Menstrual Period
HISTORY AND SYMPTOMS: I. Chief
Complaint: How long have you had this problem?
3. Was this the result of a fail or accident? Check one No Yes If yes, Date / / 4. Can you work or perform normal activities? Check one No Yes With restrictions
5. Circle symptoms associated with your chief complaint: Pain Numbness Tingling Weakness Muscle Spasm If other, please specify:
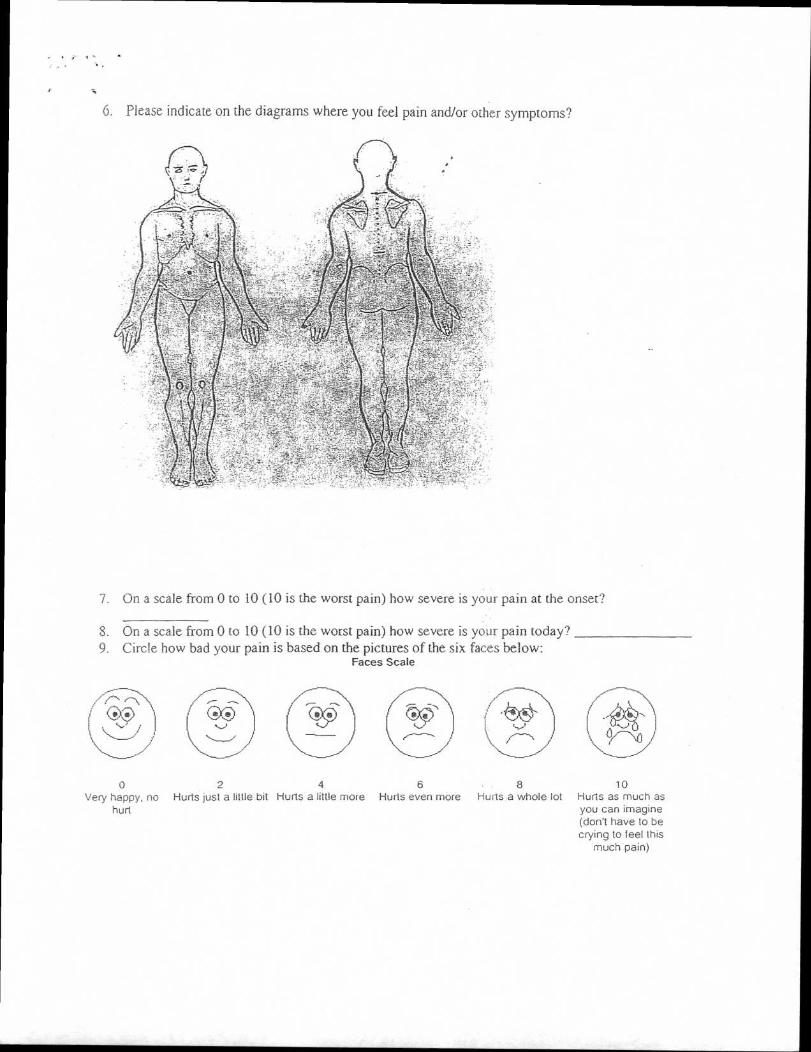
6. Please indicate on the diagrams where you feel pain and/or other symptoms?
7. On a scale from 0 to 10 (10 is the worst pain) how severe is your pain at the onset?
On a scale from 0 to 10 (10 is the worst pain) how severe is your pain today?
Circle how bad your pain is based on the pictures of the six faces below: Faces Scale
0 2 4 6 8 10 Very happy, no Hurts just a little bit Hurts a little more Hurts even more Hurls a whole lot Hurls as much as
hurt you can imagine (don't have to be crying to feel this
much pain)

Circle all that apply: 10. What is the quality of the pain? Sharp Shooting Stabbing Dull Aching
Intermittent Constant If other, please specify:
11. What makes your problem worse? Standing Sitting Walking Lifting Exercise Twisting Lying down Squatting Kneeling Bending Coughing Sneezing b If other, please specify:
12. What treatments have you had for this problem? Epidural injections Physical Therapy Massage Stimulation (TENS) Acupuncture
Trigger Point Injections Brace If other, please specify:
13. Do you have: MRI films X-ray films EMG (nerve conduction studies) CT scans Discogram Bone Scan If other, please specify:
14. What medications have you tried for your condition?
15. What medications are you currently on for your condition?
*****We must have the above information BEFORE you may see the doctor*****
I assign directly to Richard E. Pearl, M.D., all medical insurance and health benefits. I understand that in the event the charges are applied to my insurance deductible or charges are not covered, or if my insurance is invalid. I am responsible for all balances due.
I authorize any holder or medical information about me to release to the Health Care Financing Administration and its agents any information needed to determine these benefits payable for related
services.
Signature of Patient, Parent, Guardian, or Personal Representative
Please print name of Patient, Parent, Guardian, or Personal Representative