dr. meissner's presentation
TRANSCRIPT

2013 Immunization Schedule & Pertussis Update
H. Cody Meissner, M.D.
Boston Floating Hospital for Children
Tufts University School of Medicine
June 6, 2013
Webinar
MCAAP & MA Dept of Health

Disclaimers/Disclosures
• I have no relevant financial relationships with the manufacturer(s) of any commercial product(s) and/or provider of commercial services discussed in this CME activity.
• I do not intend to discuss an unapproved/investigative use of a commercial product/device in my presentation.

Licensed Vaccines in United States
Routine childhood use:
• Diphtheria, tetanus, pertussis
• Haemophilus influenzae type b
• Hepatitis A
• Hepatitis B
• Human papillomavirus
• Influenza
• Measles, mumps, rubella
• Meningococcal
• Pneumococcal
• Poliomyelitis
• Rotavirus
• Varicella
Special settings:
• Adenovirus
• Anthrax
• Bacille Calmette-Guérin (BCG)
• Herpes zoster (shingles)
• Japanese encephalitis virus
• Rabies
• Typhoid
• Vaccinia (smallpox)
• Yellow fever


Bordetella pertussis Major Antigens and Virulence Factors
Pertussis toxin (PT), also known as lymphocytosis- promoting factor (LPF)
Filamentous hemagglutinin (FHA)
Pertactin (PRN), also known as 69 kilodalton protein
Fimbrial agglutinogens (FIM)

Illness due to B. pertussis is Unique
• Difficult to recognize and diagnose because of atypical symptoms
• Only major infectious disease not associated with fever
• Symptoms in adults & adolescents may be non-specific
• Between paroxysms of cough there are no abnormal physical findings
• Infants may present with respiratory distress & apnea
• Only respiratory infection in children that is more common in girls and more often fatal in girls
• Immunity after infection or immunization is short-lived
• People with pertussis can be contagious for up to 3 weeks
• Contagious for up to 5 days after starting treatment
• Diagnostic tests may not be readily available

0
50,000
100,000
150,000
200,000
250,000
300,000
1922 1930 1940 1950 1960 1970 1980 1990 2000 2010
Nu
mb
er
of
case
s
Year
Reported Pertussis Cases – 1922–2010
DTwP
0
10,000
20,000
30,000
1990 1995 2000 2005 2010
Tdap
DTaP
SOURCE: CDC, National Notifiable Diseases Surveillance System and Supplemental Pertussis Surveillance System and 1922-1949,
passive reports to the Public Health Service

Pertussis Deaths U.S., 2000-2009
Younger than 3 Months
3 Months and Older
Total
175 19 194
(90%) (10%)

Possible Explanations for Increase in Reported Pertussis
(Reasons why DTwP, DTaP, Tdap vaccines fail)
• Greater awareness & reporting of pertussis
– Increased surveillance
• Waning vaccine induced immunity
• Acellular vaccine less potent than whole cell vaccine
– DTwP efficacy > DTaP
• Availability of better diagnostic tests
– Culture, serology, PCR
• Genetic changes in B. pertussis
• True increase in disease burden

Initial DTaP series
• Routine vaccination:
– Minimum age 6 weeks
– Administer a 5 dose series at 2,4,6 and 15-18 mon and 4-6 yrs
– 4th dose may be administered as early as 12 mon if at least 6 mon after 3rd dose
– 5th (booster) dose not indicated if 4th dose administered at ≥4 yrs
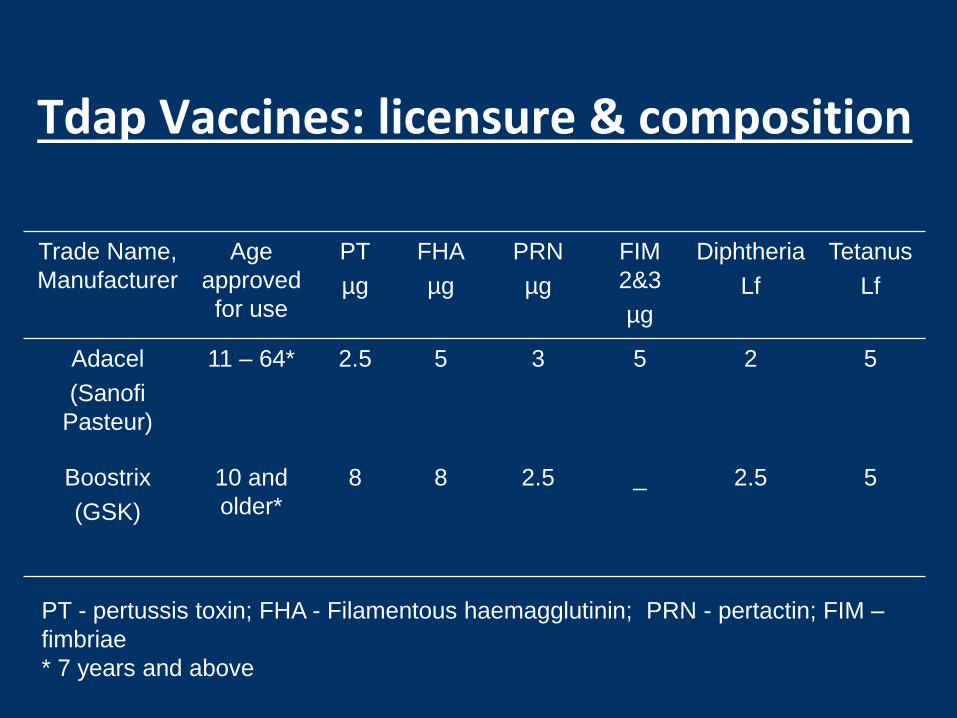
Tdap Vaccines: licensure & composition
Trade Name,
Manufacturer
Age
approved
for use
PT
µg
FHA
µg
PRN
µg
FIM
2&3
µg
Diphtheria
Lf
Tetanus
Lf
Adacel
(Sanofi
Pasteur)
11 – 64* 2.5 5 3 5 2 5
Boostrix
(GSK)
10 and
older*
8 8 2.5 _ 2.5 5
PT - pertussis toxin; FHA - Filamentous haemagglutinin; PRN - pertactin; FIM –
fimbriae
* 7 years and above

Use of Tdap Among Children 7 Through 10 Years of Age
• Children 7 through 10 years of age who are not fully vaccinated against pertussis and who do not have a contraindication to pertussis vaccine should receive a single dose of Tdap
• Either brand of Tdap may be used
• Fully vaccinated at 7 years if:
– 5 doses of DTaP or
– 4 doses of DTaP if the fourth dose was administered on or after the 4th birthday

Percent of Pertussis PCR Positive tests by Vaccine Type for 1st 4 doses (2010-11)
Pediatr 2013;131:e1716

Current Recommendations for Tdap
• A single Tdap dose
– Adolescents aged 11-18 years, preferred at 11 or 12 yrs
– Adults aged 19 and older with focus on: • Pregnant women are recommended Tdap with every pregnancy
• Health care professionals
• Parents & siblings
• Relatives ≥65 yrs
– Further guidance will be forthcoming on timing of revaccination in persons who have received Tdap previously
• No minimal interval from prior Td
• Decennial Td booster for those who received 1 Tdap
– 5 yrs for wound management

Use of Tdap Among Adults 65 Years of Age or Older
• Adults 65 years of age and older who previously have not received Tdap, should receive a single dose of Tdap
• When feasible, Boostrix should be used for adults 65 years of age and older
• Administer Adacel if Boostrix is not available

Tdap Recommendations for Pregnant Women
• Administer Tdap to pregnant adolescents and adults during each pregnancy
– preferably during 27-36 weeks’ gestation
– regardless of number of yrs since prior Td or Tdap
• If not administered during pregnancy, Tdap should be administered immediately postpartum

Precautions & Contraindications to Vaccination
• DTaP Contraindications
• Severe allergic reaction (anaphylaxis) • Encephalopathy within 7 days not due to other cause • Children <1 yr with evolving neurologic disorder
Precautions • Moderate or severe acute illness • Temperature ≥40.5ᴼC within 48 hr • Hypotonic, hyporesponsive episode within 48 hr • Persistent, inconsolable crying lasting ≥3 hr • Convulsions within 3 days
• Tdap Contraindications
• Severe allergic reaction • Encephalopathy within 7 days not due to other cause
Precautions • Moderate or severe acute illness • Guillain-Barré syndrome within 6 wks • Progressive neurologic disorder • Severe Arthus reaction