dr. kate chatters, clinical psychologist dr. rachel blundell, clinical psychologist aysem mehmet,...
TRANSCRIPT

Dr. Kate Chatters, Clinical PsychologistDr. Rachel Blundell, Clinical PsychologistAysem Mehmet, Psychological Well-Being PractitionerWendy O’Neill, Assistant Psychologist
19th November 2014
Learning Disabilities and IAPT-The Oxleas Model
“Despite their widespread experiences of disadvantage and social exclusion, and high risk of poor physical and
mental health, people with learning disabilities as a group are not well served by the NHS (Michael, 2008)
and are at risk of missing out on centrally funded initiatives such as the Improving Access to
Psychological Therapies (IAPT) programme.”
(Chinn, Abraham, Burke and Davies, 2014)

To date the evidence base regarding the effectiveness of CBT for people with learning disabilities and common mental health problems is still quite limited (Willner, 2005; Sturmey, 2006). There are a number of published case reports (Brown and Marshall, 2006; Willner, 2004), but few RCTs. (Chinn et al. 2014)
Outline for today
• What is IAPT• TLC Introduction • Who we see• Outcomes• Case discussion• Q & A’s
IAPT

Improving Access to Psychological Therapies (IAPT)
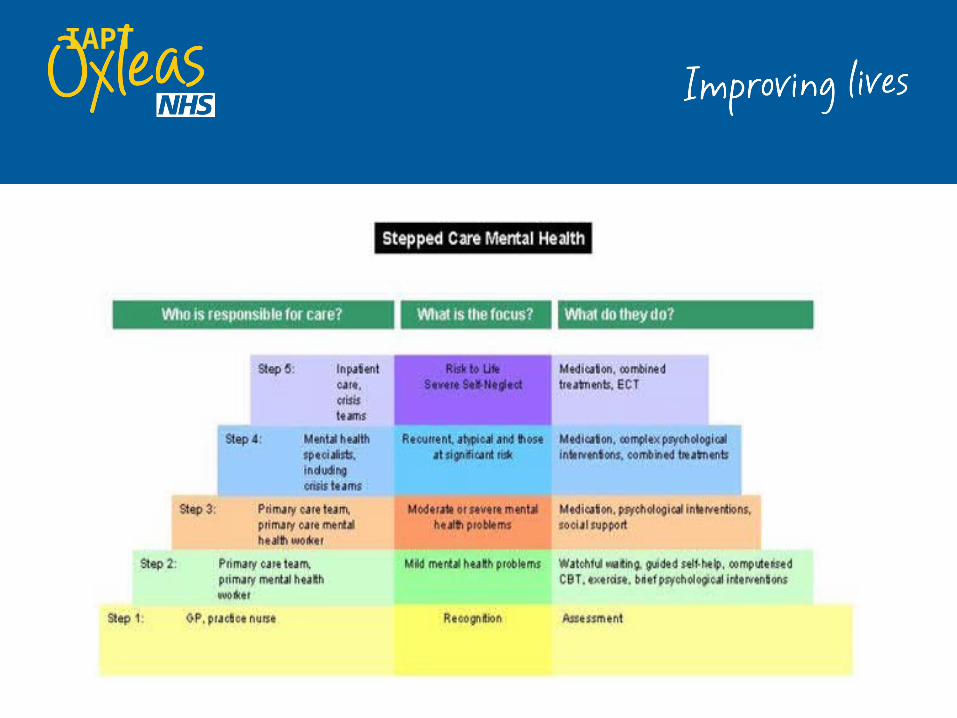
• Government led programme to train people to deliver step 2 and 3 CBT interventions in accordance with NICE recommendations.• Mild to moderate presentations = try step 2 and/or step 3
psychological interventions in preference to medication• Moderate to severe = try step 3 interventions before/in
conjunction with medication• Severe and complex = secondary care services
Our Service - TLC
• New Project – Official Launch July 2013• Tries to replicate mainstream IAPT - stepped care model for
People with Learning Disabilities• Set up with short term funding from commissioners• Recently became a permanent service• Started as IAPT-LD – now TLC • Separate service from CLDT and IAPT Greenwich Time To
Talk – good links
TLC Team
Aim of service:•To provide evidence based psychological interventions following the principles of the National IAPT programme to people with LD and their carers.•To provide primary care level – short term – focused – relatively low intensity interventions•To raise awareness of the mental health needs of people with LD (e.g GTTT/ MIND training).•To collect data on the effectiveness of these interventions.•To develop resources to support mainstream IAPT teams work•To path find!

Reasonable Adjustments
•Easy to read docs•Adapting interventions•Flexibility in appointments – same time/day/ accommodate carers•Longer sessions•Engagement with CLDT- collaborative work•Removing barriers to access
Eligibility – Inclusion
•Mild-moderate learning disability• 18 years or older• Lives in the Borough of Greenwich•Mild to Moderate Mental Health Problems • Can use psychological approach – adapted CBT
Inclusion
• Anxiety disorders • GAD• Obsessive compulsive
disorder (OCD)• Panic disorder• Agoraphobia• Social anxiety• Social phobia• Stress/work issues
• Depression• Adjustment disorders
(Coping with illness/chronic conditions)• Self image/self esteem• Sleep Management
Exclusion
• Acute psychotic symptoms• Bipolar disorder• Complex disorders• Eating disorders• Major drug or alcohol
problems• Complex MDT interventions
• Mania• Personality disorders• Sexual dysfunction• People with significant issues
of risk to self or others.
What we offer
• Individual therapy• Group therapy• Carers Workshops• Joint work/ consultation GTTT and MIND• Training

How similar to GTTT
• We offer Step 2 & Step 3 Interventions• Group Interventions• Use core outcome measure GAD/PHQ every session• Time limited 8-20 sessions• Self/GP referral

Differences between CLDT & IAPT-LD
CLDT•Assessments for eligibility & autism•Psychometric testing•Challenging Behaviour•Complex systemic work•Step 3-4 interventions•Wide range of MH difficulties
IAPT-LD•Step 2 & 3 interventions •Anxiety and depression•Short term – time limited•Clinic based model
1 year on…
• 53 referrals to TLC from July 2013 to present• 50% of these referrals were from CLDT 50% other sources inc.
GTTT• Small sample but reliable improvement* and reliable recovery
* rates broadly comparable to mainstream IAPT KPIs• Number of people showing reliable improvement at 6 sessions
stage is positive
Reflections
• Under Oxleas umbrella unlike other IAPT services that are not aligned• Promising preliminary outcome data evidencing that PWLD with
symptoms of depression and/or anxiety can demonstrate improved psychological wellbeing through a stepped care IAPT model.• Adds to very limited current evidence base• May help challenge current beliefs about candidacy* (FPLD research)• May help challenge beliefs that only long term work could improve mood
in LD • Staff all part-time but some members have a split post with CLDT – LD
clinicians• Stand alone status allows for greater flexibility in terms of adaptations
made – may not be achievable in current IAPT climate

Where next…
• GTTT – screening, joint projects, research• Resources – new interventions• FPLD • Research/Publications• Trust Quality Showcase

Break slide with title area hereSub heading area or space for another presenter’s nameAnd job title
Case PresentationSocial Anxiety
Demographics
21 year old male Lives at home with his parents and 2
younger brothers (18 years & 15 years). Unemployed & seeking employment. No risk reported
LD Diagnosis This client has a statement of SEN He attended specialist unit within a
mainstream school He has a global learning disability which
includes problems with reading, writing and fine motor skills
He was assessed by CLDT but was found not to be eligible for services due to FACS criteria
Presenting problem He was referred to our service for help
with social anxiety Trigger: Incident with a security guard He now has the belief that he looks
suspicious Previously assaulted: This has left him
feeling hyper-vigilant History of panic attacks
Impact of problem He avoids going out alone When he is out he will usually return
home sooner than he would like He will only go to places he is familiar
with and not too far from home For large parts of his week he is at home
without activity

Treatment Plan Psychoeducation on social anxiety &
panic Graded exposure Relaxation techniques Activity scheduling Signposting to Remploy employment
support
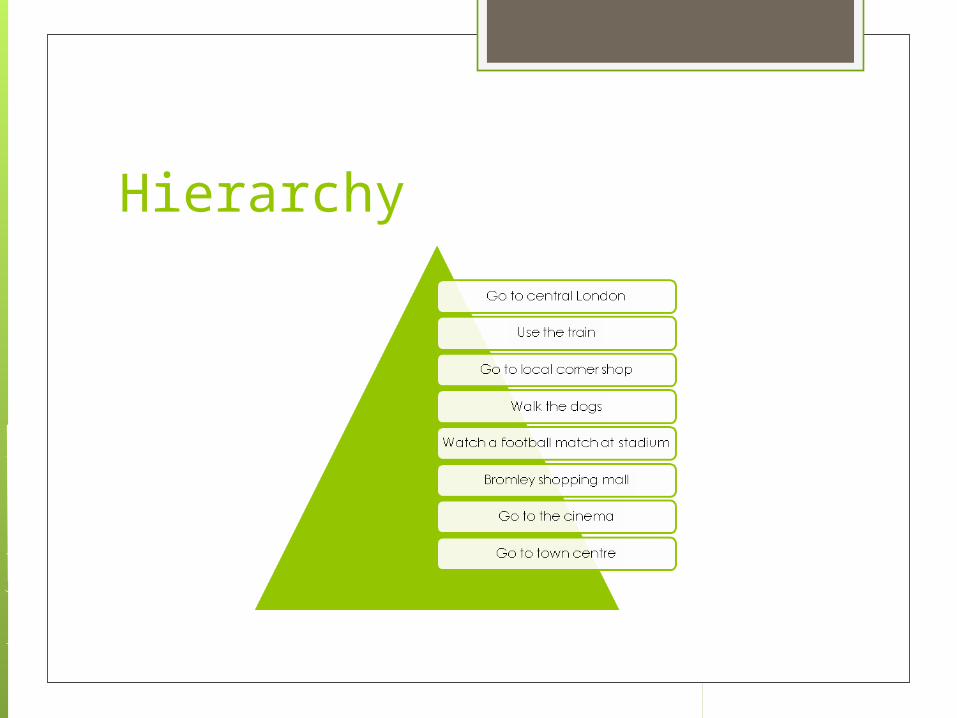
Hierarchy
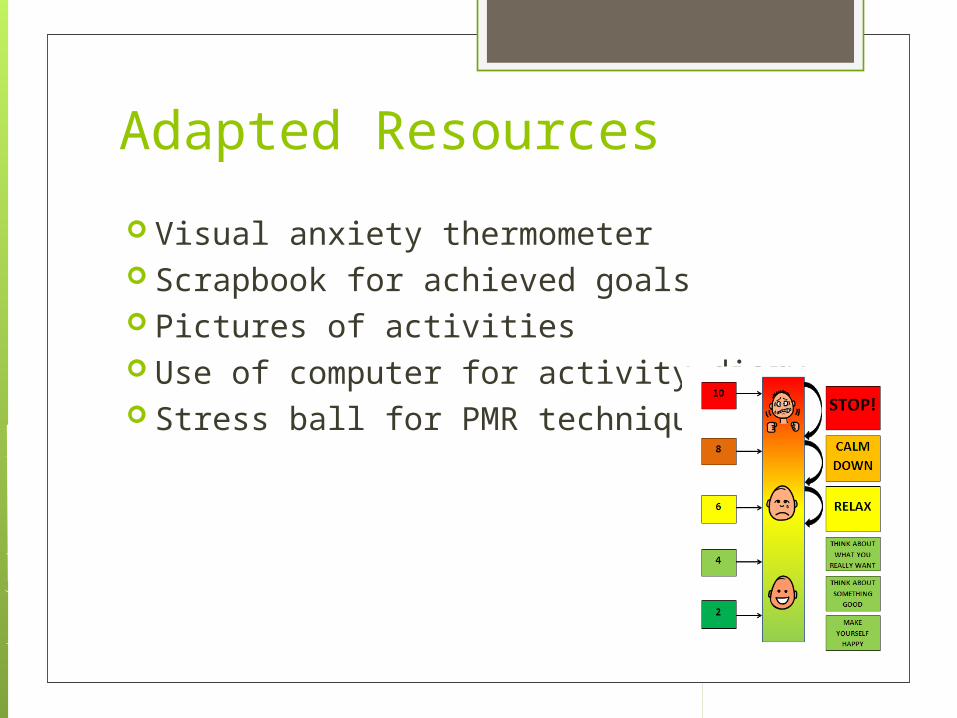
Adapted Resources
Visual anxiety thermometer Scrapbook for achieved goals Pictures of activities Use of computer for activity diary Stress ball for PMR techniques

Other adaptations His mum attended all sessions Phased sessions : Initially weekly
sessions however after session 10 we moved to fortnightly sessions.

Outcomes Client is no longer avoiding previously avoided
places/situations He does not leave a situation when he feels
anxious and instead using relaxation, breathing techniques and positive thinking
He goes out every day and his routine is more varied
He is spending more time with his family doing things like going to the cinema, taking his dogs for a walk, helping with household tasks, started going to the gym
This client has regularly been invited to several interviews and is due to start a work trial soon. He now feels more confident in public places
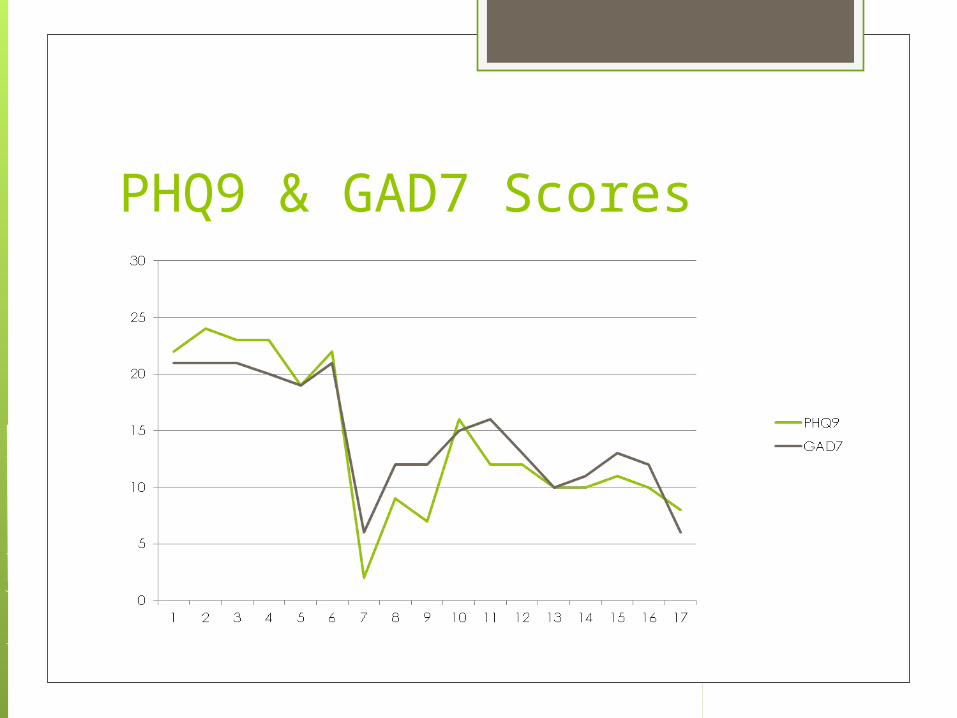
PHQ9 & GAD7 Scores

Thank you