dr ismaiel abu mahfouz
TRANSCRIPT

Diseases of the uterus
Dr Ismaiel Abu Mahfouz
Benign and pre-malignant diseases of the uterus
•Fibroids
•Endometrial hyperplasia

Fibroids • Smooth muscle tumours of the uterus
• Prevalence: variable (4.5% - 68%)
•Benign
• 0.2% : malignant transformations (leiomyosarcoma)
• Variable size from mm to many cm
• Increased risk: o African-Caribbean race (2X)
o Advancing age
o Premenopause
o HTN
o Family history (? Genetics)
•Reduced risk o Parity, smoking, COCP


Classification • Subserosal
• Intramural
• Submucous

Presentation
• Incidental finding
o In significant number of women
• Gynaecological
o AUB / HMB: due to increase surface area and vascularity
o Pelvic pain, dyspareunia, pelvic mass
• Anaemia due to HMB
• Obstetrics
o Sub-fertility / Miscarriage: ? Interference with implantation
o Abdominal pain, preterm labour, malpresentation and CS, PPH
• Compression of organ systems:
o Pressure effects on GIT and UT

Complications Hyaline degeneration
• Common
• Presents as painful enlarged fibroids due to hyaline/cystic degeneration
Red degeneration (necrobiosis)
• Typically during pregnancy at mid-term due to infarction
Calcification
• Usually in postmenopausal women
Sarcomatous change
• 0.2% risk
• Suspect if rapidly growing fibroids at advanced age
Infection
• Rare
Torsion
• Pedunculated fibroids

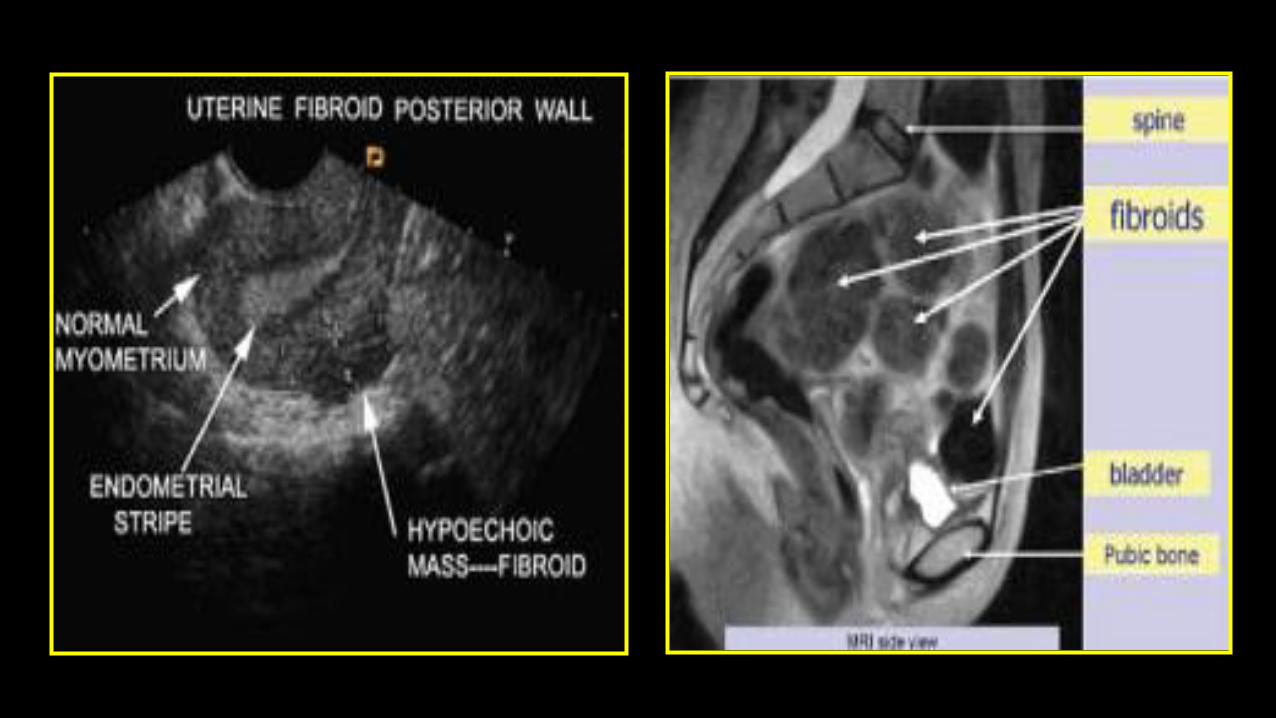
Investigations
Pelvic ultrasound
• First-line investigation
• TV or TA
MRI
• Useful when planning surgery
• Baseline prior to uterine artery embolisation (UAE)
Treatment
Individualised
Factors affecting choice of Rx
• Size
• location
• Number
• General medical health, age, BMI, previous surgery, previous fibroid Rx
• Desire for fertility preservation
• Women’s preference
Fibroid treatment Conservative :
Unlikely to be successful if large (>20w size) and multiple (if >5cm in size)
Options include
• Medical
• Myomectomy (Open, laparoscopic, hysteroscopic)
• Uterine artery embolisation
• MRI guided focused ultrasound
• Laparoscopic uterine artery occlusion
Radical
• Hysterectomy

Medical treatment COCP
• Reduce menstrual blood loss
• No change in fibroid size
LNG IUS system (Mirena IUS)
• Reduce menstrual blood loss > COCP
Ulipristal acetate (UPA)
• SPRM (selective progesterone receptor modulator)
• Reversibly blocks P receptor in endometrium and myometrium
• Orally active steroid
• Majority of women: reduction in size or prevention of further growth
• Used to treat HMB associated with uterine fibroids
Progestogens
• Cyclic P not recommended
Medical treatment
Preoperative GnRH agonist
3 – 4 month Rx prior to myomectomy / hysterectomy
• Reduces fibroid size and uterine volume
• Facilitates surgery through a low transverse abdominal incision in
women with large >24w sized multi-fibroids
• Improves preoperative haemoglobin levels
• Reduces perioperative blood loss and transfusion requirements
• Reduces hospital stay

Surgery for fibroid
Myomectomy and fertility Submucosal and intramural fibroids are associated with adverse fertility and
pregnancy outcomes
Therefore
• Removal of intracavitary part of submucous fibroid improves fertility
• Subserosal fibroids do not affect fertility outcome

Abdominal myomectomy
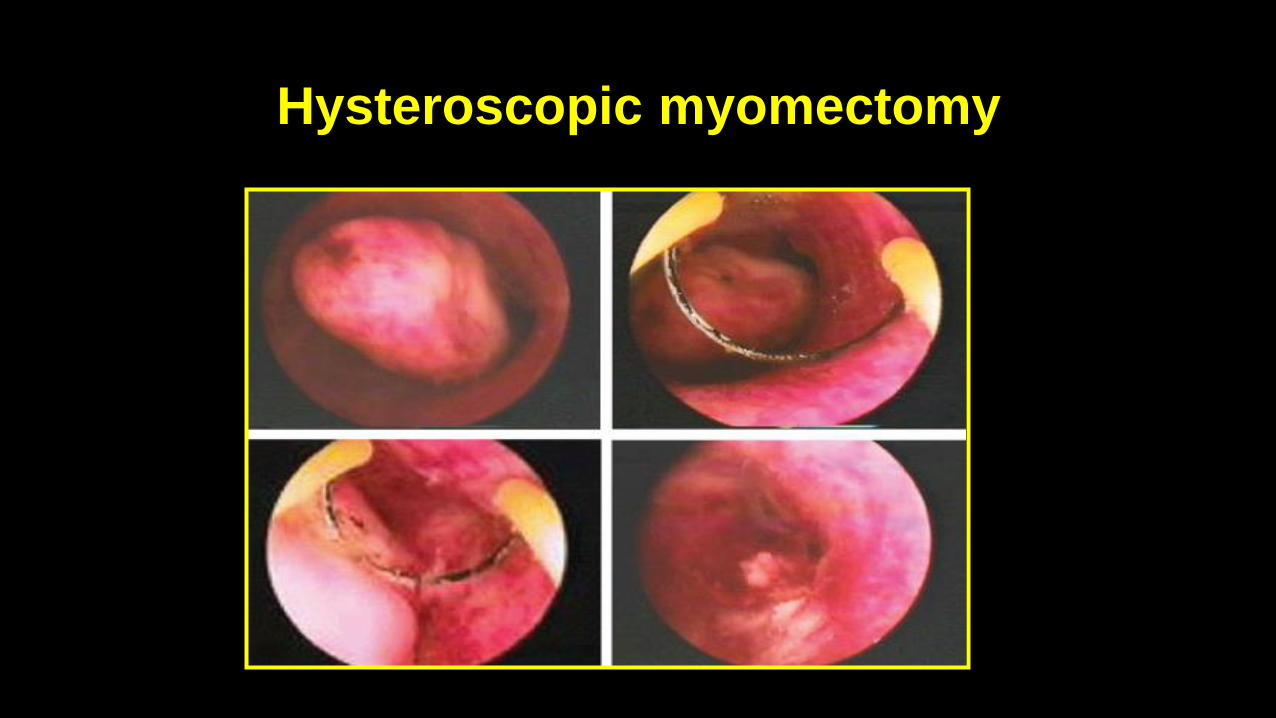
Hysteroscopic myomectomy

Uterine artery embolisation (UAE)

UAE Symptomatic fibroid
• Pt selection: multidisciplinary team ( Gynae, Interventional Radiology)
• Good outcome at short and medium term follow up
• Similar satisfaction rate to hysterectomy
Contraindication
• Active PID
• Pregnancy
• Women who may not accept a small risk of hysterectomy

MRI-guided focused ultrasound ablation

MRI-guided focused ultrasound ablation
• New innovation
• Effective and safe
• ? Fibroids less than 7-8 cm
• Improves QoL
• Adverse effects
• Low rate
• Abdominal pain, lumbar pain, first-degree burns, light vaginal bleeding

Surgery for fibroid
Hysterectomy can be considered as a first-step
• Severe symptoms (HMB, pressure effects, pain)
• Significant pathology (>20 week sized uterus) that is unlikely to respond to other Rx
• Women’s preference for definitive Rx
• No desire for future fertility

Endometrial hyperplasia

Endometrial hyperplasia Definition • Proliferation of glands of irregular size and shape with an increase in the
glands/stroma ratio Classification • Simple endometrial hyperplasia with or without atypia • Complex endometrial hyperplasia with or without atypia
Atypia • Most important prognostic factor for progression to ca • Hyperplasia without atypia: < 2% progress to ca in “ mean duration of 10 years” • Hyperplasia with atypia : 23% progress to ca in “mean duration of 4 years” • Endometrial ca may co-exist with atypical hyperplasia in 25% of patient
Treatment
Without atypia
• Progesterone (including Mirena IUS)
• Follow up endometrial sampling
• ? TAH
With atypia
• TAH +/- BSO

Malignant diseases of the uterus
• Endometrial ca
• Sarcoma

Endometrial ca

Endometrial ca
• Increasing in incidence
• 25% increase in last decade
• Most common gynae ca in developed countries
• Strongly related to obesity

Endometrial ca; Risk factors
Advancing age
• Peak incidence: 65 - 75 years
• 2–5% < 40 years
Prolonged exposure to E2
• Late menopause
• Exogenous E2
Low parity
• 21– 34% are nulliparous
• Reduced by 30% after first birth & by 25% with each subsequent birth
• Why higher parity is protective?
o Sloughing off of the endometrium during delivery
o Breaks in exposure to unopposed E2 during pregnancy

Endometrial ca Risk factors
Obesity
• 3-10 fold increase
Hypertension and Type 2 DM
Cigarette smoking
• Decreases ca endometrium by 20–40% (anti-estrogenic effects of nicotine)
Unopposed estrogen therapy
• Increases by 6-8 times
• COCPs protective
Family history
• HNPCC (Lynch syndrome)
Others
• Previous pelvic irradiation
• Tamoxifen
Diagnostic assessments Trans-vaginal ultrasound
• ET: cut-off 5 mm in postmenopausal women: suggestive of ca
Endometrial biopsy
• Office based (Pipelle)
• GA
Hysteroscopy and endometrial biopsy
• The standard investigation for Dx
• Outpatient or inpatient

Screening
•No accepted technique for endometrial ca screening
• Identification of high-risk factors: early detection

Pathology of endometrial cancer
Adenocarcinoma
•Arises commonly from the fundus
• ? Difficult to distinguish between well-differentiated ca and atypical hyperplasia
• 25% of atypias have co-existing carcinomas

Pathology of endometrial cancer
Papillary serous carcinoma and clear cell carcinoma
• Similar to cell type in ovary and fallopian tube ca
• Spread in a similar fashion to ovarian ca
o Full-staging laparotomy and omentectomy is required
•Aggressive course and poor prognosis
• 50% of treatment failures

Pathology of endometrial cancer
Others types
•Mucinous adenocarcinoma: uncommon
• Squamous carcinoma : uncommon
•Undifferentiated carcinoma: very rare

Grading and spread for endometrial cancer Grading
Mode of spread in endometrial cancer
Differentiation Grade Spread Description
Well 1 Limit to endometrium, <10% involve
outer third of myometrium
98% glandular or papillary
formations
Moderate 2 2–50% solid areas
Poor 3 <10% limit to endometrium, cervical
extension 15%
>50% solid areas
Mode Description
Direct spread Through fallopian tubes to ovaries and peritoneal cavity
Most common route . Myometrial and eventually serosal involvement
Lymphatic To parametrial, vaginal, pelvic and para-aortic nodes (via infundibulopelvic ligament)
Haematogenous To liver, lung, central nervous system and bone is rare (late-stage disease)

Patient evaluation History
• Abnormal uterine bleeding (PMB, HMB) 90% of women
• Vaginal discharge
• LUTS
• Weight loss, general weakness, abdominal swelling
Physical examination • Frequently normal
• Inspection and palpation of the vulva and vagina
• Suburethral area is common for metastatic deposits
• Exclude other causes for vaginal bleeding
• Bimanual rectal and vaginal examination to assess pouch of Douglas, parametria

Preoperative workup
• Full blood count
•Blood Glucose
• Liver and renal functions
•Consider Cystoscopy
•Consider Sigmoidoscopy
•CT scans: pelvis, abdomen
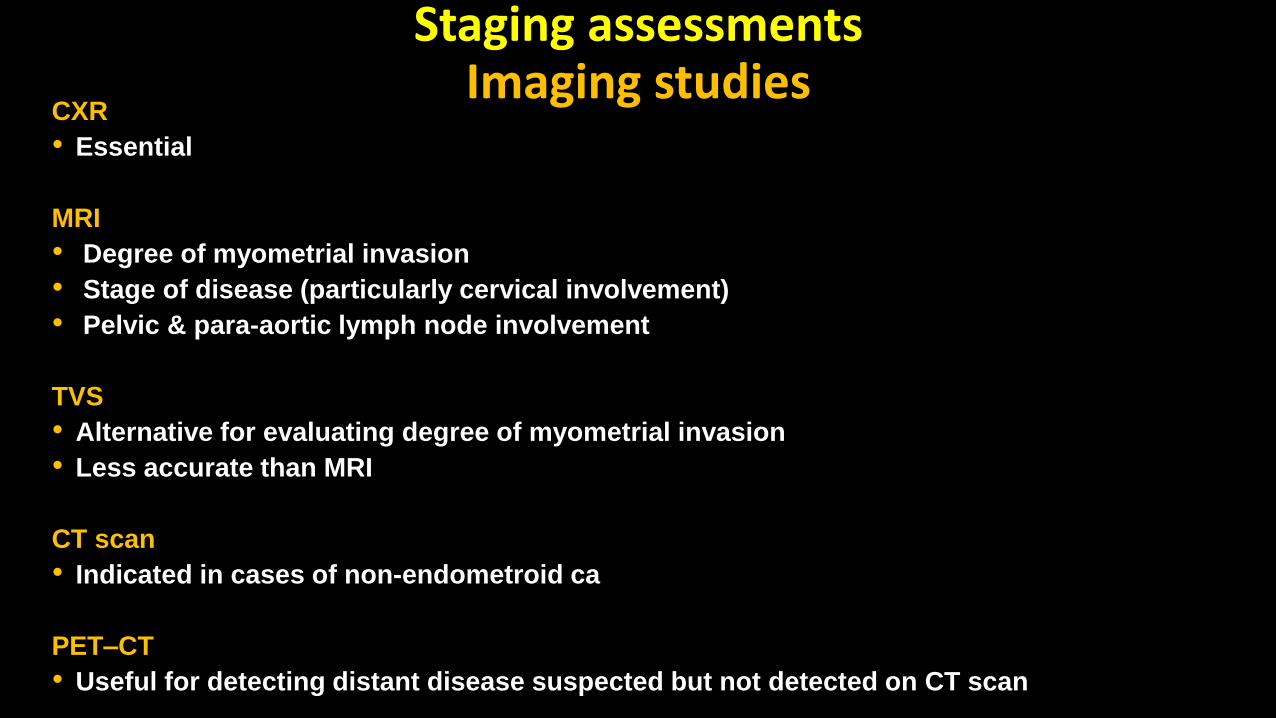
Staging assessments Imaging studies
CXR
• Essential
MRI
• Degree of myometrial invasion
• Stage of disease (particularly cervical involvement)
• Pelvic & para-aortic lymph node involvement
TVS
• Alternative for evaluating degree of myometrial invasion
• Less accurate than MRI
CT scan
• Indicated in cases of non-endometroid ca
PET–CT
• Useful for detecting distant disease suspected but not detected on CT scan

FIGO staging 2014 update
Stage I Tumour confined to the corpus uteri
IA: Tumour confined to the uterus. No or less than half myometrial invasion
IB: Tumour confined to the uterus. More than half myometrial invasion
Stage II Cervical stromal invasion but not beyond the uterus
Stage III Local and/or regional spread of the tumour
IIIA: Tumour invades serosa or adnexa
IIIB: Vaginal and/or parametrial involvement
IIIC1: Pelvic node involvement
IIIC2: Para-aortic involvement
Stage IV Tumour invades bladder and/or bowel mucosa and/or distant metastases
IVA: Tumour invasion of the bladder and/or bowel mucosa
IVB: Distant metastases: abdominal metastases and/or inguinal lymph nodes.

Treatment of ca endometrium
Surgery
• The main treatment
Radiotherapy
• If patient is unfit for surgery
•Adjuvant
Hormonal treatment
•High dose progesterone
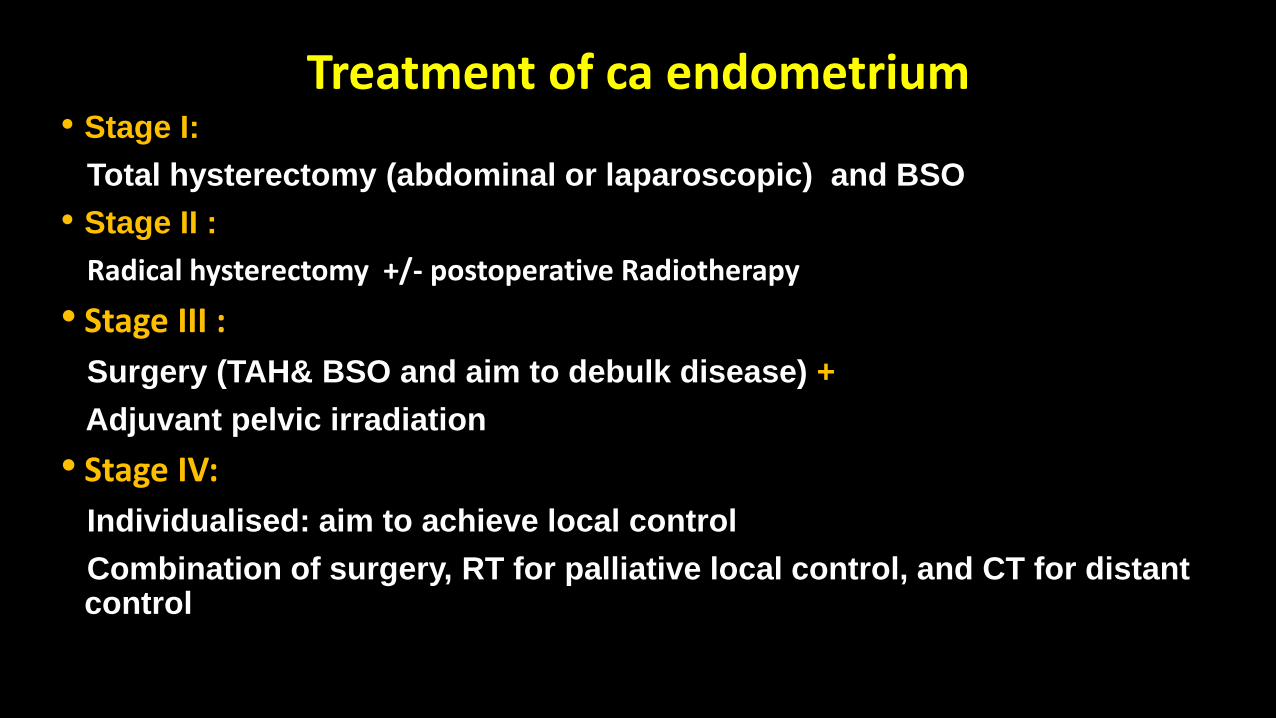
Treatment of ca endometrium • Stage I:
Total hysterectomy (abdominal or laparoscopic) and BSO
• Stage II :
Radical hysterectomy +/- postoperative Radiotherapy
• Stage III :
Surgery (TAH& BSO and aim to debulk disease) +
Adjuvant pelvic irradiation
• Stage IV:
Individualised: aim to achieve local control
Combination of surgery, RT for palliative local control, and CT for distant control

Prognostic factors
•Cell type
•Grade
•Depth of myometrial invasion
• Endocervical involvement

Recurrent disease
• Majority: within the first 36 months
• 75% of local recurrences present with vaginal bleeding or pelvic pain
• Always check for systemic spread
Treatment for recurrence
• Pelvic RT: appropriate If no previous RT
• Pelvic Exenteration: Prior radiation with isolated central pelvic recurrences with no evidence of LN involvement
• Progestogens & Tamoxifen: clinical response in 20%
• Doxorubicin, platinum-based & placitaxel: response rates: 30–40%

Sarcoma

Uterine sarcomas
•A rare group of heterogeneous neoplasms arising from the uterine corpus
•Mainly of carcinosarcomas, leiomyosarcomas, endometrial stromal sarcomas
•Aggressive clinical behaviour & poor prognosis
•High risk of local recurrence and distant spread

Epidemiology and prognostic factors Epidemiology
• 4–9% of all invasive uterine ca
• Black women had twice the risk
• Median age at diagnosis o Leiomyosarcoma: 48–54 years o Endometrial stromal sarcoma: 41–63 years o carcinosarcoma: 62–67 years
Prognostic factors
• Stage is the most important prognostic factor
• Poor prognostic factors: o High grade o Adnexal spread o Lymph node metastasis
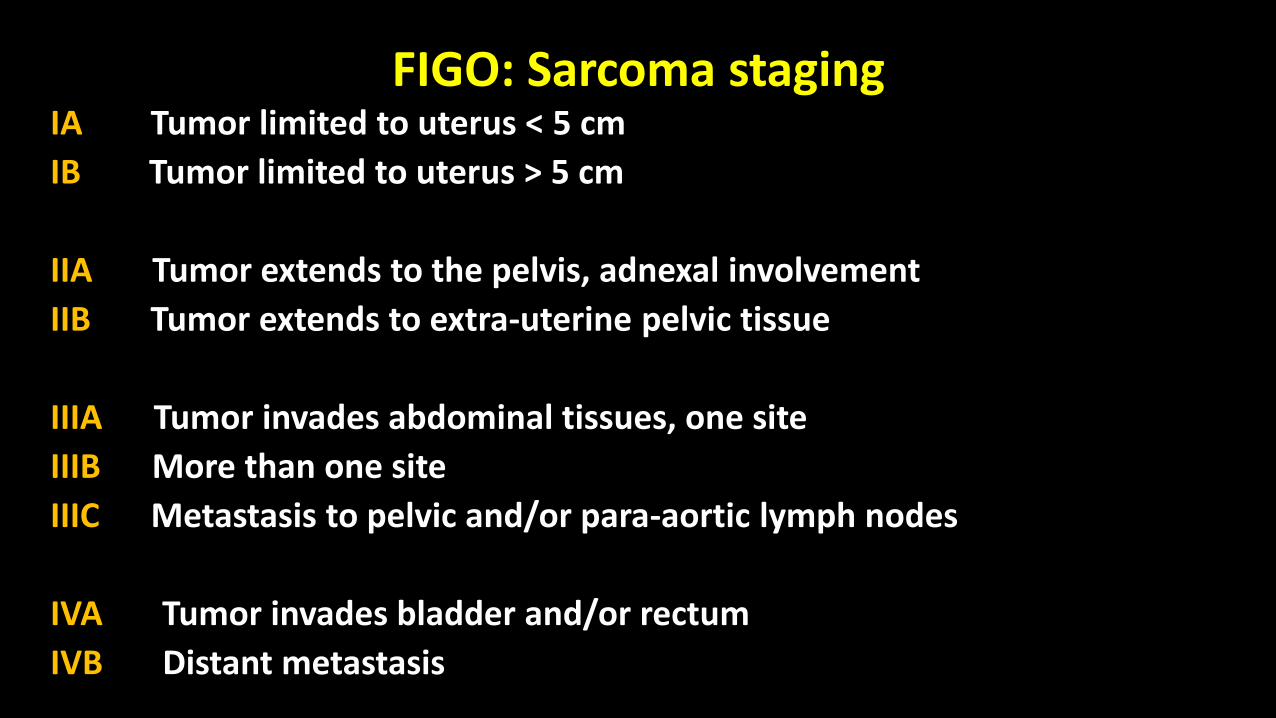
FIGO: Sarcoma staging IA Tumor limited to uterus < 5 cm
IB Tumor limited to uterus > 5 cm
IIA Tumor extends to the pelvis, adnexal involvement
IIB Tumor extends to extra-uterine pelvic tissue
IIIA Tumor invades abdominal tissues, one site
IIIB More than one site
IIIC Metastasis to pelvic and/or para-aortic lymph nodes
IVA Tumor invades bladder and/or rectum
IVB Distant metastasis
Treatment
Surgical resection
• The mainstay of Rx
• TAH & BSO is the standard surgical Rx
• Pelvic and/or para-aortic lymphadenectomy
• There is a limited role for adjuvant radiotherapy / chemotherapy