dr guadagno: ms senory symptoms
TRANSCRIPT
“Have I got MS?” - advice on sensory symptoms
Joe GuadagnoRoyal Victoria InfirmaryNewcastle upon Tyne

Outline
Brief reminder of MS: Incidence, dermographics Usual presenting features
Helpful basic tips? Temporal evolution of sensory symptoms
What are the typical sensory symptoms of MS? What is not typical for MS…… Other neurological conditions with sensory
symptoms New DMT’s – brief update!

Statistics
Commonest cause of acquired neurological disability in young people
Prevalence in UK (~1990s): NI 168/100 000
• (?230 2006) Tayside 184/100 000 NE England ?150/100 000
(1:650) F:M 3:1
What is MS?
Clinical diagnosis
Loosest definition:
1. At least 2 episodes of CNS dysfunction (relapses/attacks/exacerbations)
2. ‘disseminated in time and space’
3. not explained by something else
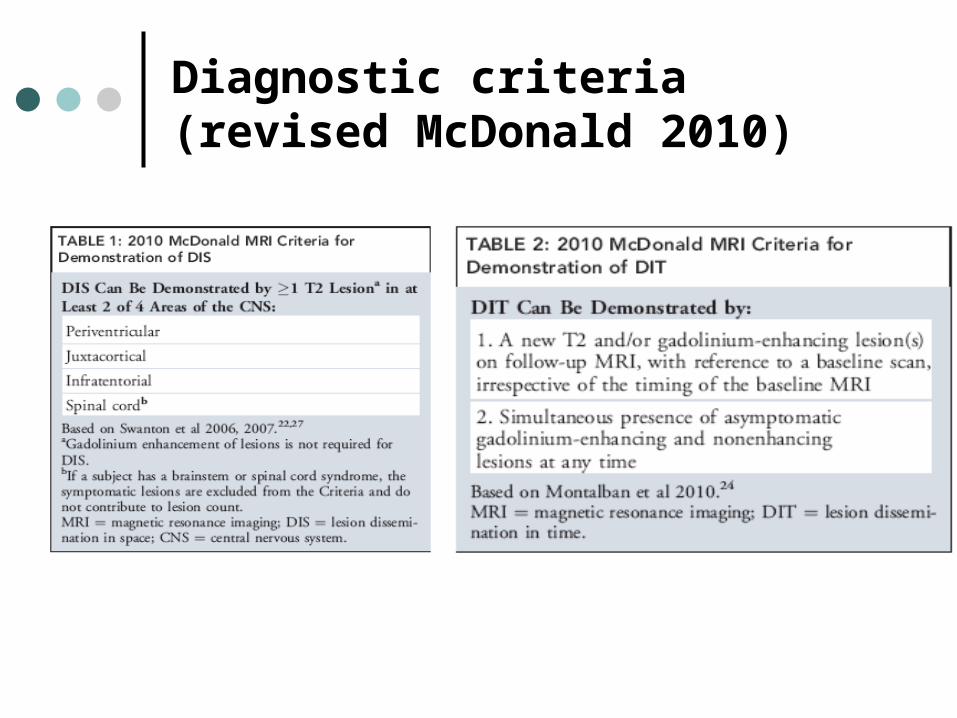
Diagnostic criteria (revised McDonald 2010)

MRI

relapsing/ remitting primary progressive
Patterns of MS
secondary progressive
85% 15%

relapsing/ remitting primary progressive
Patterns of MS
secondary progressive
85% 15%
( ‘benign’)
5%
Aetiology
genetic1 in 6 cases have affected relative
1 in 650 general population1 in 50 chance if one affected parentbut only 30% concordance in identical
twins
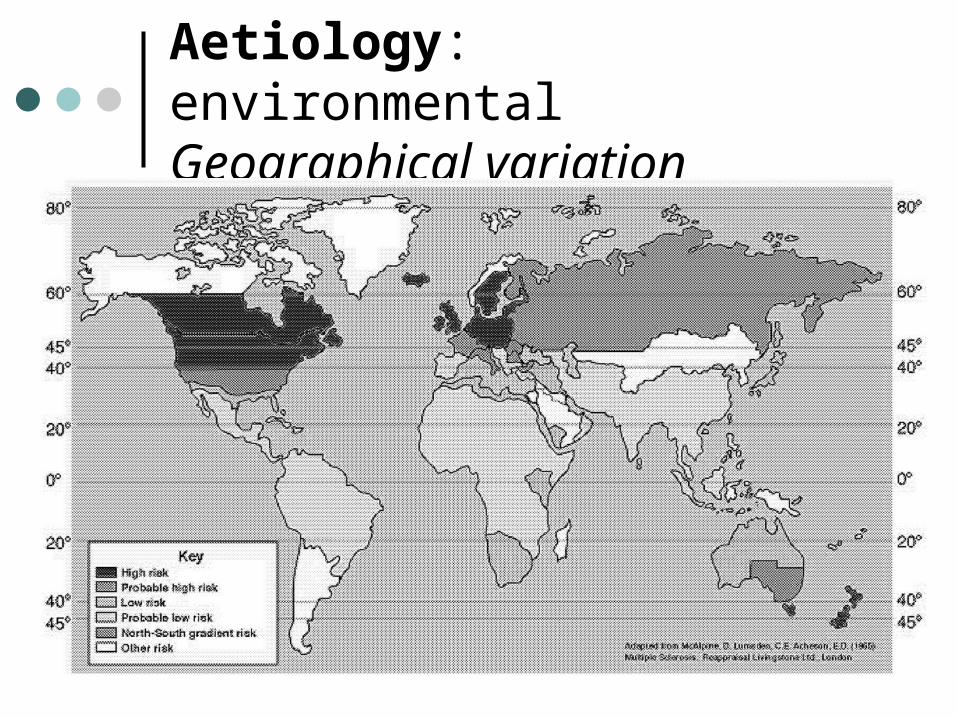
Aetiology: environmentalGeographical variation

UV exposure?
Genetic and environmental?
migration studies– environmental hit acquired in childhood (15yr)
– repeated or prolonged exposure
– latency
infections? EBV?
vitamin D/sunlight?
Hygiene Hypothesis – ‘idle immune system’
- acquired disease in a genetically susceptible individual: cumulative insults?
What is MS?
inflammation degeneration

What is MS?
inflammation degeneration

Common presentations (relapses)
transverse myelitis
brainstem syndromes
optic neuritis
paroxysmal symptoms

The duration of the attack should be longer than 24 hours!
And not in the context of an infection (pseudorelapse)

Helpful tip (when addressing sensory symptoms)
– remember the temporal evolution of relapses

Typical ON - RecoveryV
isua
l Fun
ctio
n
1 to 2/52 3 to 5/52

What are the typical sensory symptoms of MS?(Nb around 35% of presenting symptoms are
sensory (Olec 2005 and Paty et al 1994))
• ascending numbness starting in the feet;• bilateral hand numbness;• Hemiparesthesia (rare thalamic presentation);• dysesthesia in the whole of one limb (or non
dermatomal);• “sunburn” feeling or “itch” in a non-dermatomal
patch• MS ‘Hug’• Facial sensory disturbance and typical TN• Lhermittes phenomena
Whole body numbness or parasthesia Transient flitting sensory disturbances
(parasthesia or numbness) lasting minutes to hours
uncomplicated Bell’s palsy fatigue as isolated or predominant symptom chronic dizziness/ light-headedness “weakness” in setting of musculoskeletal
pain/tenderness atypical facial pain
What is not MS….

Sensory symptoms from other neurological disorders (and
should be referred……)

Keep in mind a little bit of neuroanatomy…………

Radiculopathies (pain!)

Entrapment neuropathies
CTS
Ulnar
Lateral Cutaneous Nerve
(meralgia parasthetica)
Common peroneal Nerve


Management of relapses
Nothing (especially sensory) Steroids
Oral 500mg methlypred for 5 days
IV 1000mg for 3 days
Disease modifying therapy - First line
Five licensed therapies Interferon-
• Avonex • Betaferon• Extavia• Rebif
Copaxone Prescribed under ABN
guidelines

† Measured as the total over 2 years‡ The Avonex trial required a sustained progression for 6 months; the Rebif trial, for 3 months; and the Copaxone trial, for 3 months
First line DMTs
Summary of results from pivotal phase 3 trials
Agent Dosage Reduction in relapses, % †
Relapse-free patients, % †
Interferon beta-1b (Betaferon)
8 mIU (250 µg)SC every other day
34 31
Interferon beta-1a (Avonex)
30 µgIM once weekly
32 38
Interferon beta-1a (Rebif)
22 µgSC 3 times weekly
29 27
44 µgSC 3 times weekly
32 32
Glatiramer acetate (Copaxone)
20 mgSC once daily 29 34
Adapted from Galetta S, et al. Arch Int Med 2002; 162; 2161-2169

Beyond one third relapse reduction…..
New Disease Modifying therapies.

Natalizumab (Tysabri)- A humanised monoclonal antibody

Leukocyte entry to the nervous system
blood
brain
firm adhesion
rolling slow rolling
capture diapedesis
chemokines (incl. MCP-1/CCR-
2)
inflammation
chemokines
selectins integrins (incl. VLA-
4)
migration

Natalizumab (Tysabri)
blood
brain
firm adhesion
rolling slow rolling
capture diapedesis
inflammation
selectins integrins (incl. VLA-
4)

Natalizumab: good things
AFFIRM Highly Active* 1 (n= 148 for TYSABRI, 61 for PBO)
81%
64%
reduction in annualised relapse rate vs. placebo over 2 years (p < 0.001)
reduction in the risk of disability progression, sustained for 24 weeks, as assessed over 2 years (p =0.008)
Patients With ≥2 Relapses in Prior Year and ≥1 Gd+ Lesion At Baseline

2010 2011

Progressive Multifocal Leukoencephalopathy (JC virus)

New Oral therapies!
Fingolimod (Gilenya)
“FDA Panel Unanimously Recommends Approval of First Oral MS Drug”A Food and Drug Administration advisory panel on Thursday unanimously
recommended approval of the first drug for multiple sclerosis (MS) that can be taken orally.

FREEDOMS: Annualised relapse rate (ARR) at 2 years (primary endpoint)
Kappos et al, N Engl J Med 2010; 362: 387–410; Cohen et al, Poster P901 presented at ENS 2011; Francis and Haering, April 2011; data on file Negative binomial regression model adjusted for treatment group, country, number of relapses in previous two years and baseline EDSS. Bars represent the 95% CI; ARR, annualised relapse rate; DMT, disease-modifying treatment. Based on efficacy and safety profile, fingolimod 0.5 mg/day is the only approved dose for the treatment of MS
0
0.18(0.15–0.22)
0.40(0.34–0.47)
0.1
0.2
0.3
0.4
ARR
Placebo (n=418)
Fingolimod 0.5 mg(n=425)
-54% p<0.001

Possibly not so good things about fingolimod
completely new class of drug (SIP1 inhibitor)
slows heart on first dose Macular oedema risk 2 deaths
herpes encephalitisDisseminated chicken poxno long term safety dataTeratogenicity?

31% reduction

inhibits dihydroorotate dehydrogenase (DHODH), - a mitochondrial enzyme involved in de novo pyrimidine synthesis (needed for the proliferation of activated lymphocytes).
LFT’s! – needs 2 weekly bloods for 6 months!
Hair thinning/alopecia Stays in system a long time (up to 2
years) so pregnancy effects?

Others dues soon….!
Tecfidera (dimethy fumarate - oral)
Lemtrada (Alemtuzemab – infusion)
