dr eric decloedt fccp (sa) mmed (clin pharm) division of ... · diabetic peripheral neuropathy...
TRANSCRIPT

Dr Eric Decloedt
FCCP (SA) MMed (Clin Pharm)
Division of Clinical Pharmacology

INCISION
Nociceptors
depolarise
Synaptic transmission:
Facilitate Inhibit
Substance P DA, NA, 5HT
Glutamate Opioids
Nerve growth factor GABA
Cannabinoids
Intensity &
Location Emotional

INCISION
Nociceptors
depolarise
Synaptic transmission:
Facilitate Inhibit
Substance P DA, NA, 5HT
Glutamate Opioids
Nerve growth factor GABA
Cannabinoids
Intensity &
Location Emotional

Cause of
symptoms
Time course Outcome Features
Acute pain Known Short-term Recovery
anticipated
Essential to
survival
Chronic pain Unknown Indeterminate Complete
remission often
not possible
Pathological


Site Psych
comorbidity
Examples
Peripheral Inflammation or
damage in
periphery
Minor Osteoarthritis
Rheumatoid arthritis
Cancer
Central Disturbance in
pain processing
Major Fibromyalgia
Spinal cord injury
Poststroke pain
Multiple sclerosis
Mixed Both Either Diabetic peripheral neuropathy
Postherpetic neuralgia
Trigeminal neuralgia
Phantom limb pain
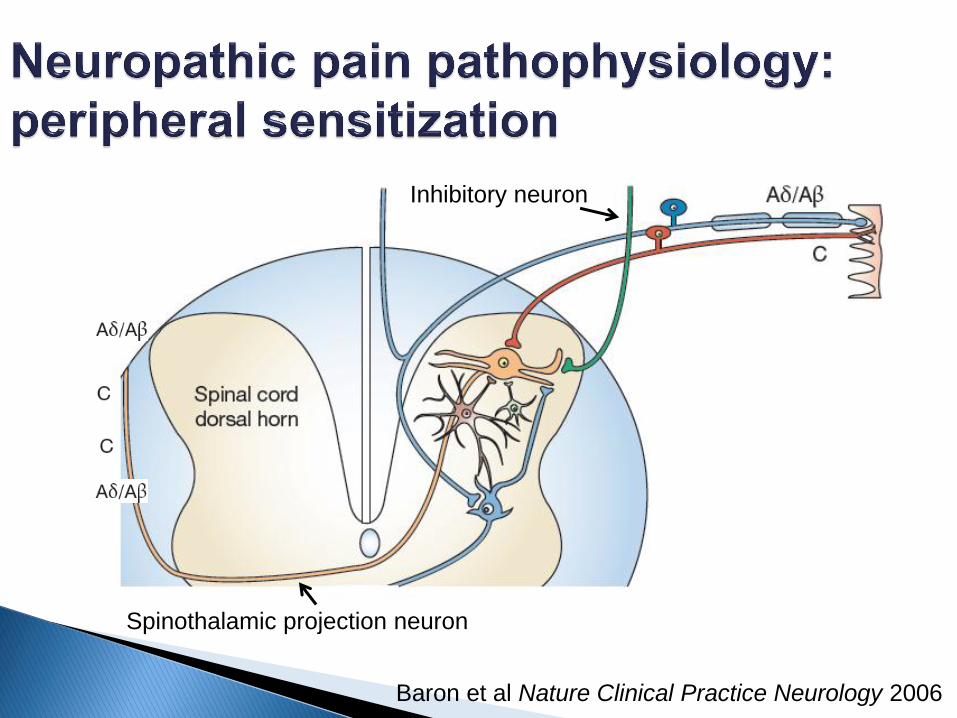
Baron et al Nature Clinical Practice Neurology 2006
Spinothalamic projection neuron
Inhibitory neuron

Baron et al Nature Clinical Practice Neurology 2006
Spinothalamic projection neuron
Inhibitory neuron

Baron et al Nature Clinical Practice Neurology 2006

Zeilhofer et al Annu Rev Pharmacol Toxicol 2012

Jaggi et al Brain Research 2011
Anterior cingulate
cortex
Rostral ventromedial
medulla
Periaqueductal gray

Moisset et al Neuroimage 2007
anterior
cingulate
cortex
prefrontal
cortex
primary
somatosensory
cortex
secondary
somatosensory
cortex

Borsook et al Curr Pain Headache Rep 2011

Gottschalk et al Am Fam Physician 2001

Challenging! ◦ Complex disease spectrum with heterogeneity
◦ Variability in studies
Outcome measures
Number of participants
Treatment duration
Quality of design
◦ Data manipulation & lack of transparency
◦ Expert panel of guidelines ?truly independent & no
conflict of interest
Landefeld et al NEJM 2009

TCAs
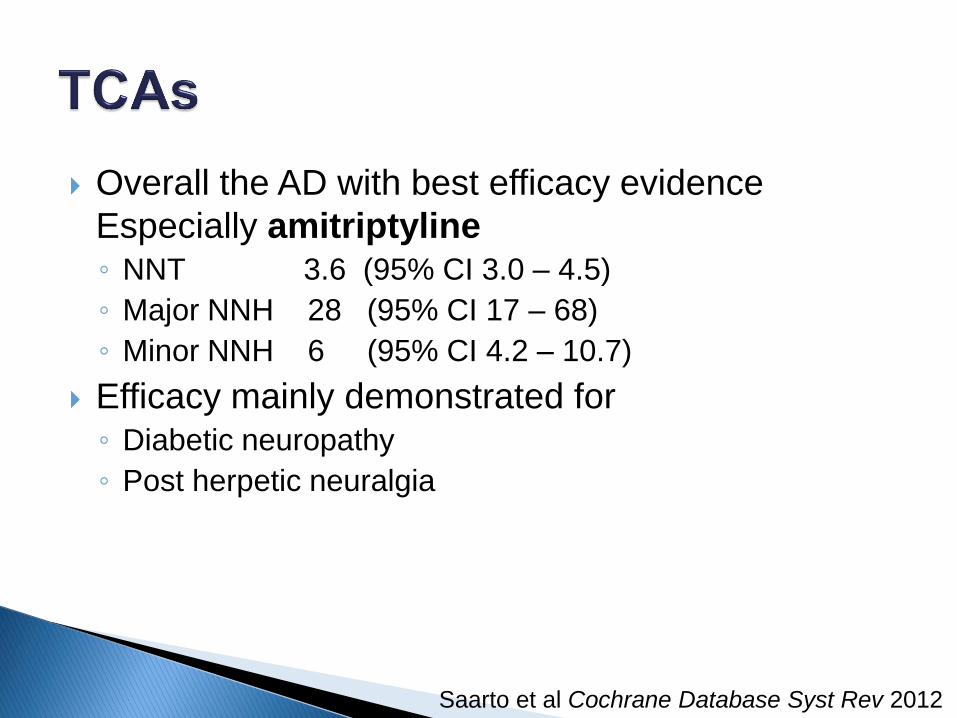
Overall the AD with best efficacy evidence
Especially amitriptyline ◦ NNT 3.6 (95% CI 3.0 – 4.5)
◦ Major NNH 28 (95% CI 17 – 68)
◦ Minor NNH 6 (95% CI 4.2 – 10.7)
Efficacy mainly demonstrated for ◦ Diabetic neuropathy
◦ Post herpetic neuralgia
Saarto et al Cochrane Database Syst Rev 2012

Inexpensive
Pain response expected ± 7 days – titrate weekly
Low dose analgesic vs higher dose AD ◦ ? Treatment of choice in comorbid depression
Cardiovascular (screening ECG)
Anticholinergic side effects
Sedation
CYP2D6 DDI
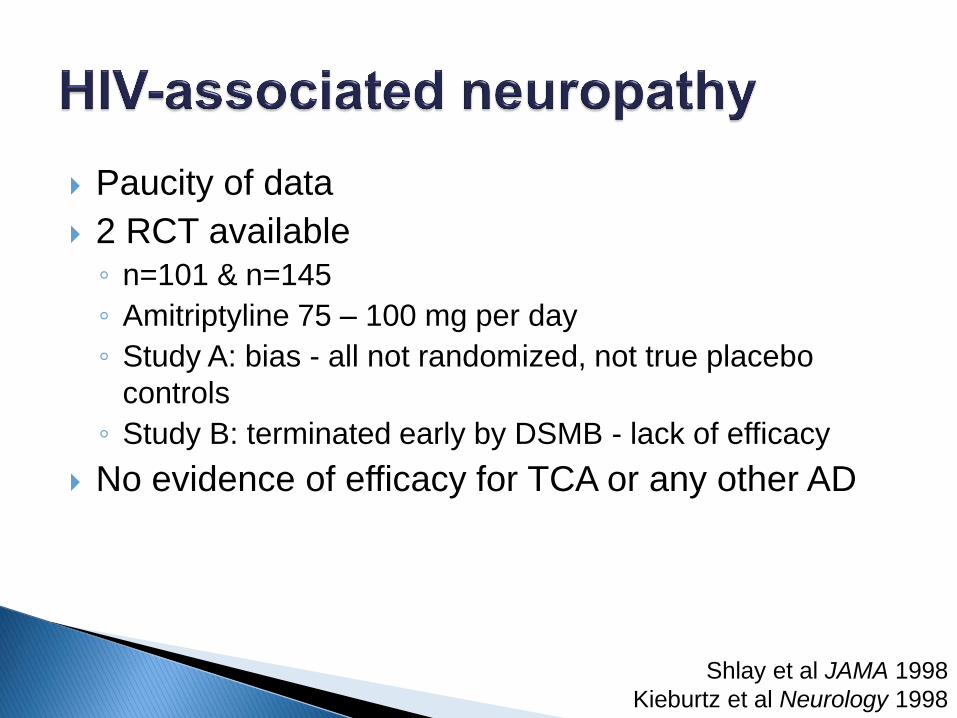
Paucity of data
2 RCT available ◦ n=101 & n=145
◦ Amitriptyline 75 – 100 mg per day
◦ Study A: bias - all not randomized, not true placebo
controls
◦ Study B: terminated early by DSMB - lack of efficacy
No evidence of efficacy for TCA or any other AD
Shlay et al JAMA 1998
Kieburtz et al Neurology 1998

SNRIs

Duloxetine ◦ Diabetic peripheral neuropathy
NNT 6 (5 – 10)
◦ Fibromyalgia
NNT 8 (5 – 17)
◦ Major NNH 17 (12 – 50)
Venlafaxine ◦ Diabetic peripheral neuropathy
◦ Mixed or negative study results:
post-mastectomy pain, postherpetic neuralgia, other
?lower doses used in some
Rowbotham et al Pain 2004
Sindrup et al Neurology 2003
Bair et al Postgrad Med 2011
Lynn et al Cochrane Database Syst Rev 2010

Depression and NP treatment doses similar
Duloxetine registered for diabetic NP
Cardiovascular side-effects (venlafaxine) ◦ Study setting: 5% developed ECG changes
CYP2D6 DDI
Dose adjust in renal and hepatic impairment
(duloxetine)
Response expected within 2 weeks
Rowbotham et al Pain 2004

SSRIs

Limited data for effectiveness
Diabetic neuropathy & somatoform disorder :
superior to placebo ◦ Fluoxetine, paroxetine, citalopram, escitalopram
Insufficient data reported to calculate NNT
Compared to TCAs: less pain relief ◦ Imipramine > paroxetine
◦ Desipramine > amitriptyline > fluoxetine
Maina et al J Clin Psych 2002
Sindrup et al Pain 1990
Rowbotham et al Pain 2004
Ciaramella et al Minverva Anestesiologica 2000

Diabetic
PN
HIV
PN
Post-
herpetic
PN
Central
pain
Fibro-
myalgia
NNT
NNH
(Major)
Antidepressants
TCAs
SNRIs
SSRIs
11+
5+
3+/1-
1+/1-
4+
1-
2+
1-
1+
3.6 (3.0 – 4.5)
6.0 (5 – 10)
insufficient
28 (17 – 68)
17 (12 – 50)
Insufficient
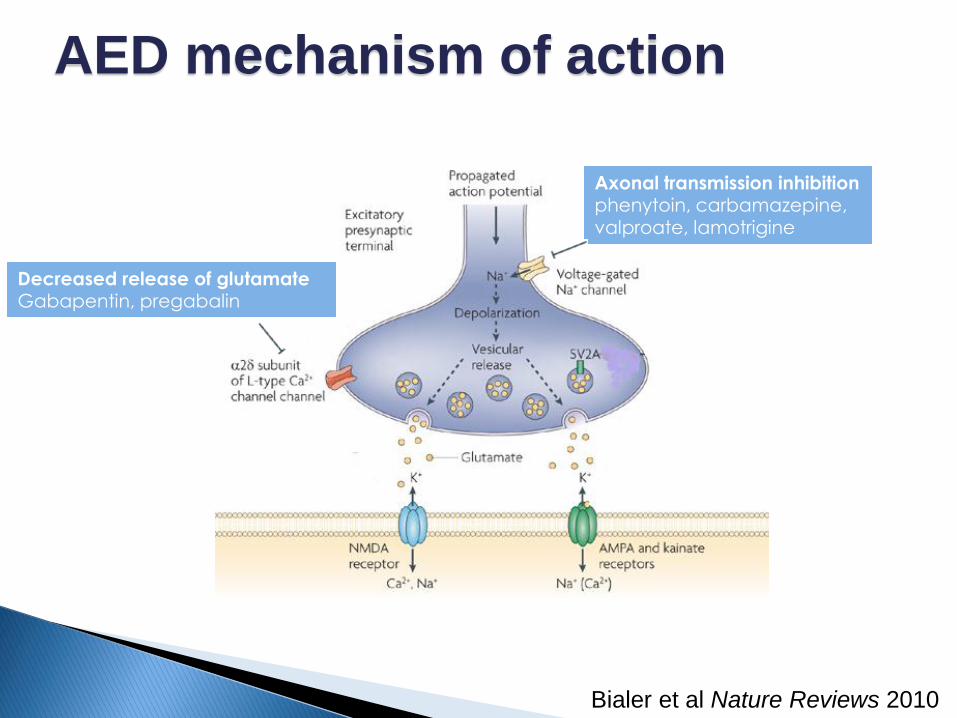
Axonal transmission inhibition phenytoin, carbamazepine, valproate, lamotrigine
Decreased release of glutamate Gabapentin, pregabalin
AED mechanism of action
Bialer et al Nature Reviews 2010
Phenytoin ◦ No evidence
Sodium valproate ◦ No convincing efficacy evidence
Lamotrigine ◦ No convincing efficacy evidence
Birse et al Cochrane Database Syst Rev 2012
Gill et al Cochrane Database Syst Rev 2011
Wiffen et al Cochrane Database Syst 2011

Carbamazepine ◦ 5 good quality RCTs, n=298
◦ Efficacy evidence
Trigeminal neuralgia, DPN, postherpetic neuralgia, central
stroke pain
NNT 2 (1.6 – 2.5)
Limited: short duration, limited size, poorly defined outcomes
NNH 2.6 (2.1 – 3.5)
Inconsistently reported
Wiffen et al Cochrane Database Syst Rev 2011

Carbamazepine ◦ Auto-induction – dose increase at 3 weeks
Omitted in most studies
◦ Cutaneous skin reactions
5-10% Asians: HLA-B*1502 → SJS

Gabapentin ◦ Efficacy evidence: diabetic neuropathy, post herpetic
neuralgia, mixed neuropathic pain
◦ > 30% improvement compared to placebo
NNT 5.8 (4.8 – 7.2)
◦ > 50% improvement compared to placebo
NNT 6.8 (5.6 – 8.7)
◦ Major NNH 32 (19 – 100) & minor NNH 6.6 (5.3 – 9)
Moore et al Cochrane Database Syst Rev 2011

Pregabalin ◦ Best NNT for 50% improvement at max dose (600 mg)
Postherpetic neuropathy 3.9 (3.1 – 5.1)
Peripheral diabetic neuropathy 5.0 (4.0 – 6.6)
Central neuropathic pain 5.6 (5.3 – 14)
Fibromyalgia 11 (7.1 – 21)
Usual dose 75 mg bd, increased to 150 mg bd
Adverse events dose related: Major NNH 5 - 10
Moore et al Cochrane Database Syst Rev 2011

Gabapentin ◦ Absorbed by an active and saturable transport system:
careful dose titration
◦ Not metabolized & no enzyme induction
Pregabalin ◦ Registered for neuropathic pain
◦ Linear pharmacokinetics – easier dosing
◦ Not metabolized & no enzyme induction

Diabetic
PN
HIV
PN
Post-
herpetic
PN
Central
pain
Fibro-
myalgia
NNT
NNH
(Major)
Antidepressants
TCAs
SNRIs
SSRIs
11+
5+
3+/1-
1+/1-
4+
1-
2+
1-
1+
3.6 (3.0 – 4.5)
6.0 (5 – 10)
insufficient
28 (17 – 68)
17 (12 – 50)
Insufficient
Anticonvulsants
Carbamazepine
Gabapentin
Pregabalin
3+/2-
3+/3-
5+
1-
1-
5+
5+
1-
1+/1-
2+
1+
4+
2.0 (1.6 – 2.5)
5.8 (4.8 – 7.2)
3.9 (3.1 – 5.1)
2.6 (2.1 – 3.5)
32 (19 – 100)
5 – 10

Efficacy evidence Diabetic peripheral neuropathy
Postherpetic neuropathy
Painful polyneuropathy
Tramadol ◦ 50% pain relief NNT 3.8 (2.8 – 6.3)
◦ Major NNH 8.3 (5.6 – 1.7)
Morphine, oxycodone, methadone ◦ 50% pain relief NNT 2.6 (28 to 70 day use)
◦ Minor NNH 4.2 & Major NNH 10
Duehmke et al Cochrane Database Syst Rev 2008
Eisenberg et al Cochrane Database Syst Rev 2009

Morphine ◦ Abuse potential
Tramadol ◦ Atypical : weak action at μ-receptor & inhibit 5HT & NA
re-uptake transporters
◦ No suppression of hypoxic drive
◦ Seizure risk
◦ Lower abuse potential
◦ DDI with other AD

Diabetic
PN
HIV
PN
Post-
herpetic
PN
Central
pain
Fibro-
myalgia
NNT
NNH
(Major)
Antidepressants
TCAs
SNRIs
SSRIs
11+
5+
3+/1-
1+/1-
4+
1-
2+
1-
1+
3.6 (3.0 – 4.5)
6.0 (5 – 10)
insufficient
28 (17 – 68)
17 (12 – 50)
Insufficient
Anticonvulsants
Carbamazepine
Gabapentin
Pregabalin
3+/2-
3+/3-
5+
1-
1-
5+
5+
1-
1+/1-
2+
1+
4+
2.0 (1.6 – 2.5)
5.8 (4.8 – 7.2)
3.9 (3.1 – 5.1)
2.6 (2.1 – 3.5)
32 (19 – 100)
5 – 10
Opioids
Opioids
Tramadol
2+
3+
2+
1+
2.6
3.8 (2.8 – 6.3)
10
8.3 (5.6 – 1.7)

No recipe! ◦ Co-morbid disease
◦ DDI
◦ Side effect profile
◦ Cost
◦ Patient response
Increase dose to maximum, add different class of drug

FIRST LINE - Good efficacy, lower cost ◦ TCAs & SNRIs
SECOND LINE ◦ Gapapentin (higher NNT)
◦ Pregabalin (response requires higher dose, registered)
◦ Carbamazepine (efficacy base on limited data)
◦ Tramadol (combination with AD problematic)
◦ Morpine (abuse potential)