doxorubicin-induced chronic cardiotoxicity and - cancer research
TRANSCRIPT

[CANCER RESEARCH 42. 1817-1825, May 1982]0008-5472/82/0042-0000$02.00
Doxorubicin-induced Chronic Cardiotoxicity and Its Protection byLiposomal Administration1
Aquilur Rahman,2 Newton More, and Philip S. Schein
Department of Medicine. Division of Medical Oncology ¡A.P.. P. S.], and Department of Pathology [N. M.], Vincent T. Lombardi Cancer Research Center,Georgetown University, Washington, O. C 2000 7
ABSTRACT
The chronic cardiotoxicity of doxorubicin as a free drug orentrapped in positive and negative liposomes was morphologically evaluated in mice treated seven times i.v. at a dose of 4mg/kg. Liposomes were composed of phosphatidylcholine,cholesterol, and stearylamine (positive charge) or phosphati-
dylserine (negative charge). Administration of free doxorubicincaused a pattern of cardiac damage characterized by loss ofmyofiber elements, mitochondrial damage, nuclear abnormalities, swollen and distended sarcoplasmic reticulum leading tovacuolization, and increasing myeloid body accumulation. Cardiac tissues of mice treated with doxorubicin entrapped innegatively charged liposomes demonstrated pronounced lossof filaments, enlarged mitochondria, disruptive loss of crests,and expanded nuclear membrane. However, electron microscopic examination of the cardiac muscles of mice treated withpositive liposomes demonstrated a significant protection fromdrug-induced toxicity, with only minor loss of parallel fibrillar
arrangement and myofilaments in limited focal areas. The majority of the tissue demonstrated normal vasculature and intercalation of myocytes as compared to control groups. The meanqualitative and quantitative scores of toxic lesions for freedoxorubicin and entrapped in negative liposomes are 2.7 and2.23, respectively. However, the mean score for the group ofmice treated with positive liposomes is only 1.12, showing abetter than 2-fold scoring protection of both the extent and
severity of cardiac lesions.
INTRODUCTION
Doxorubicin is an important antitumor agent of the anthra-cycline group isolated from cultures of Streptomyces peucetius(6). Doxorubicin has demonstrated antitumor activity for a widerange of human cancers including lymphomas (3, 4, 24),leukemias (4, 10, 17, 24), and solid tumors including gastricand pancreatic cancer (4, 16, 18, 24). The mechanism ofaction is the formation of complex with nuclear DMA by intercalating between base pairs, thus causing steric obstruction toDMA-dependent RNA (7, 25). This drug also produces acute
toxicity in the form of bone marrow depression, alopecia, andoral ulcération (4, 18, 24). The principal treatment-limitingtoxicity of doxorubicin is a delayed cardiotoxicity, which ismanifested in the form of refractory congestive heart failure(14). This cumulative myocardial damage has been correlated
' This investigation was supported by the American Heart Association and by
National Cancer Institute Grant NO1 CM97310.2 To whom requests for reprints should be addressed, at Division of Medical
Oncology, Room 2230, Georgetown University Hospital, 3800 Reservoir Road,N. W.. Washington, D. C. 20007.
Received August 13, 1981; accepted February 8, 1982.
with doses in excess of 500 mg/sq m, or less in patients withprior mediastinal irradiation. Electron microscopic studies ofthe heart tissue in such cases have demonstrated a strikingdegeneration of myofibrils and mitochondrial distortion, as wellas a decrease in cardiac myocytes (22). As a correlate, phar-macokinetic studies have shown that Adriamycin is taken upavidly by heart muscle (26).
Recently, attempts have been made to control the pharma-cokinetics and disposition of drugs by the use of liposomes ascarriers of drugs (12, 13). We have demonstrated recently thatliposomal entrapment of doxorubicin significantly alters theplasma clearance and tissue disposition of the drug in mice(19, 21). Furthermore, it was shown that the acute cardiotoxicity induced by doxorubicin was significantly reduced by liposomal delivery of the drug encapsulated in a positivelycharged preparation. Electron microscopic studies demonstrated that the myocytes and myofibrillar structure of cardiacmuscle were markedly well preserved with doxorubicin entrapped in liposomes compared to free drug (20). In this paper,we describe the protection from drug-induced chronic cardi
otoxicity in mice when doxorubicin is administered entrappedin liposomes.
MATERIALS AND METHODS
The following lipids were purchased from Sigma Chemical Co. (St.Louis, Mo.); phosphatidylcholine, cholesterol, and phosphatidylserine.Stearylamine was purchased from K & K Laboratories (ICN, Plainview,N. Y.). All the lipids were used as received and were kept at -20°.
The lipids were checked for purity by thin-layer chromatography on
silica gel using the solvent system chloroform:methanol:water (70:30:5,v/v) and were found to be pure. Doxorubicin (NSC 123127) wassupplied by the Developmental Therapeutic Program, Division of Cancer Treatment, National Cancer Institute. All other chemicals werereagent grade.
For the chronic cardiotoxicity studies in mice, doxorubicin entrappedin positive liposomes was prepared by mixing 14.8 /¿molof the drugwith 50.6 ftmol of phosphatidylcholine, 20.7 iimol of cholesterol, and14.8 /¿molof stearylamine. Doxorubicin entrapped in negative liposomes was prepared by adding 50.6/¿mol of phosphatidylcholine, 20.7/¿molof cholesterol, 5.06 /¿molof phosphatidylserine, and 14.8 /¿molofthe drug. The organic solvents were then evaporated under a streamof nitrogen so that a thin film of lipid is formed on the sides of the flask.Ten ml of 0.01 M phosphate buffer with 0.85% NaCI solution (pH 7.4)were then added to the dried lipid and drug film, and the mixture wasdispersed with a magnetic stirring bar, yielding multilamellar liposomes.After a 0.5-hr swelling period, these multilamellar liposomes weresonicated for 20 min under a nitrogen atmosphere in a bath-typesonicator (Heat Systems Model 220F) at 35°.The nonentrapped dox
orubicin was separated from liposomal encapsulated drug by extensivedialysis against 0.01 M phosphate buffer with 0.85% NaCI, pH 7.4, at4°over a period of 30 hr with at least 3 changes of buffer solutions.
The amount of doxorubicin captured under these conditions was determined by fluorescence (1) after the completion of dialysis. The
MAY 1982 1817
Research. on January 1, 2019. © 1982 American Association for Cancercancerres.aacrjournals.org Downloaded from

A. Rahman et al.
average diameter of these liposomes as determined by electron microscopy was 700 ±200 (S.D.) A.
Male DBA/2 mice, weighing 22 to 25 g and obtained from CharlesRiver Breeding Laboratories, (Wilmington, Mass.), were randomly distributed into groups of 6, maintained in plastic cages in a standardizedenvironment, and fed on Lab-Blox laboratory chow pellets and water
ad libitum. Free and entrapped doxorubicin in either positive or negativeliposomes was administered via a tail vein at a dose of 4 mg/kg and at2% of body weight. Further controls included mice given injections of0.9% NaCI solution and other groups given injections of blank positiveliposomes with the same concentration of lipids used to entrap thedrug. All mice were given twice-a-week injections for a total of 7
treatments. After the fourth and sixth injections, treatment was discontinued for 2 weeks to allow for recovery of bone marrow function. Oneweek following the last injection, the mice were killed by cervicaldislocation, and the hearts were immediately removed and placed in0.9% NaCI solution. The apex of the left ventricle, with part of theseptum, was dissected out, minced into 1-cu mm blocks and fixed in
2.5% glutaraldehyde buffered with 0.1 M cacodylate, pH 7.2, for 2 hrat room temperature. The specimens were rinsed in buffer, osmicatedin Bennett and Luffs' collidine-buffered osmium tetroxide, dehydrated
in graded ethanols and acetone, and embedded in Epon. The remainderof each heart was placed in Trump fixative and embedded in methylmethacrylate (Polysciences) for light microscopic evaluation. For electron microscopy, preliminary 1-/im Epon sections were stained with
alkaline toluidine blue, and appropriate areas were chosen for sectioning. Random sections were taken on 200 mesh copper grids andstained with uranyl acetate and lead citrate. A JEOL 100 S electronmicroscope at an accelerating voltage of 80 keV was utilized forviewing the sections. For light microscopy, 1.5-/¿mmethyl methacrylatesections were cut, using glass knives on a Servali JB-4 microtome,and stained with Gill's hematoxylin and Lee's méthylèneblue-basic
fuchsin.Scoring System. The scoring system was similar to that used by
Jaenke (11), for light microscopy, which was adapted to electronmicroscopic analysis as follows. Evaluation was made at no less than2 levels per block of tissue, and scoring was tabulated individually foreach of 20 grid squares of tissue section per grid (200 mesh) using thecriteria presented in Table 1. The product of severity and extent of thedamage observed in each mouse was scored, and the total scoresrepresented the combined qualitative and quantitative values per average grid square area (Table 2).
RESULTS
Fig. 1D represents by light microscopy a typical area ofmyocardial damage following treatment with free doxorubicin;it is characterized by extensive vacuolation and loss and/ordisorganization of contractile elements. Mice treated with doxorubicin entrapped in negatively charged liposomes showeddegenerative alterations distributed in focal areas, some advanced in nature, usually surrounded by normal-appearingtissue (Fig. 1c). However, light microscopic sections of heartsfrom mice treated with doxorubicin entrapped in positivelycharged liposomes (Fig. IB) showed an overall appearancecomparable to that of control tissue (Fig. 1/\); there were onlyoccasional affected myofibers, which were difficult to discernand may represent preparatory artifacts.
Electron microscopic examination of the heart tissues correlated well with the light microscopic findings. Administrationof free doxorubicin caused a pattern of cardiac damage characterized by loss of myofiber elements, mitochondrial damage,nuclear abnormalities, swollen and distended sarcoplasmicreticulum leading to vacuolization, and increasing myeloid bodyaccumulation. All these lesions were commonly present and
Table 1
Qualitative scoring1+ Early degenerative alterations in some cells, i.e.. loss of parallel ori
entation, swelling of mitochondria, and cell vesiculation, etc.2+ Advanced degenerative changes, i.e., intracytoplasmic inclusions (e.g.,
myelin whorls), loss of myofilaments. separation of intercalateddiscs, nuclear modifications.
3+ Mvoti hi 111;u atrophy, loss of contractile elements.4+ Myofiber degeneration accompanied by myolysis.
Quantitative scoring1+ Involvement of single scattered myofibers.2+ Involvement of groups of myofibers.3+ Focal groups.4+ Confluent groups.
Table 2
Electron microscopic evaluation of doxorubicin cardiotoxicity
BlocksFA,"FA2FAsFA.—
ve/lipi-ve/lipz-ve/lips-ve/lip«-ve/lips+ve/lip,+
ve/lip2+ve/lip3+ve/lip.+ve/lips+ve/lip6T
a>Qualitativ«23311727212810231391116598'Quantitative3731282232391130181218207128'QuaJilalrv*
+
quantitativ«606245495367215329212936122116Mr'3.003.102.252.452.653.351.052.651.451.051.451.800.601.050.80Av.2.702.23119life
' T, total: Mr. mean of total qualitative and quantitative.6 FA, free doxorubicin group; —ve/lip, doxorubicin entrapped in negative
liposomes; -t-ve/lip, doxorubicin entrapped in positive liposomes.
are represented typically in Figs. 2 and 3. Large regions ofcardiac muscle demonstrated an early involvement (Fig. 2A)with loss of filaments, swelling of mitochondria with vacuolization, and distention of the sarcoplasmic reticulum. Of particularinterest in this micrograph is the abrupt division between affected and apparently nonaffected cells separated by a normalintercalated disc.
Fig. 26 shows the extensive loss of cellular elements typicalin the more advanced stages of damage. This would appear asvacuolization of myofibrils and/or myolysis by light microscopy. There is also the nuclear distortion and condensation ofheterochromatin at the periphery of the nucleus. Fig. 2C demonstrates a myocyte with large accumulations of myeloid bodies, autophagic vacuoles, and other inclusion bodies of electron-dense material. This corresponds to the most severe dam
age observed in these samples prior to absolute dissolutionand myolysis of the cells. Free and pleomorphic mitochondriaare present even at this apparent late stage of toxicity. Myofilaments can be seen in short segments, haphazardly dispersed throughout the damage cell, while some areas appearto be devoid of their remnants.
Fig. 3 presents higher magnifications of regions with theadvanced damage seen after the administration of doxorubicinas a free drug. In Fig. 3A, the nuclear envelope is distendedand separated from the main body of the nucleus, which hasan unusual contorted appearance. A thin band of condensedchromatin lies at the nuclear periphery, and the remainingchromatin pattern is irregular. Also present are slightly distortedmitochondria. Fig. 3B shows an advanced mitochondrial de-
1818 CANCER RESEARCH VOL. 42
Research. on January 1, 2019. © 1982 American Association for Cancercancerres.aacrjournals.org Downloaded from

generation, with swelling, loss of cristae, total disruption, andinclusion. Fig. 3C presents an example of the myeloid- ormyelin-type inclusion bodies observed with extensive toxicdamage. There are variations in size and density and thepresence of other dense inclusions with some myelin lamellaesurrounding mitochondria. The intercalated disc shown in Fig.3D is separated, and there are electron-lucent spaces betweenthese normally abutted membranes.
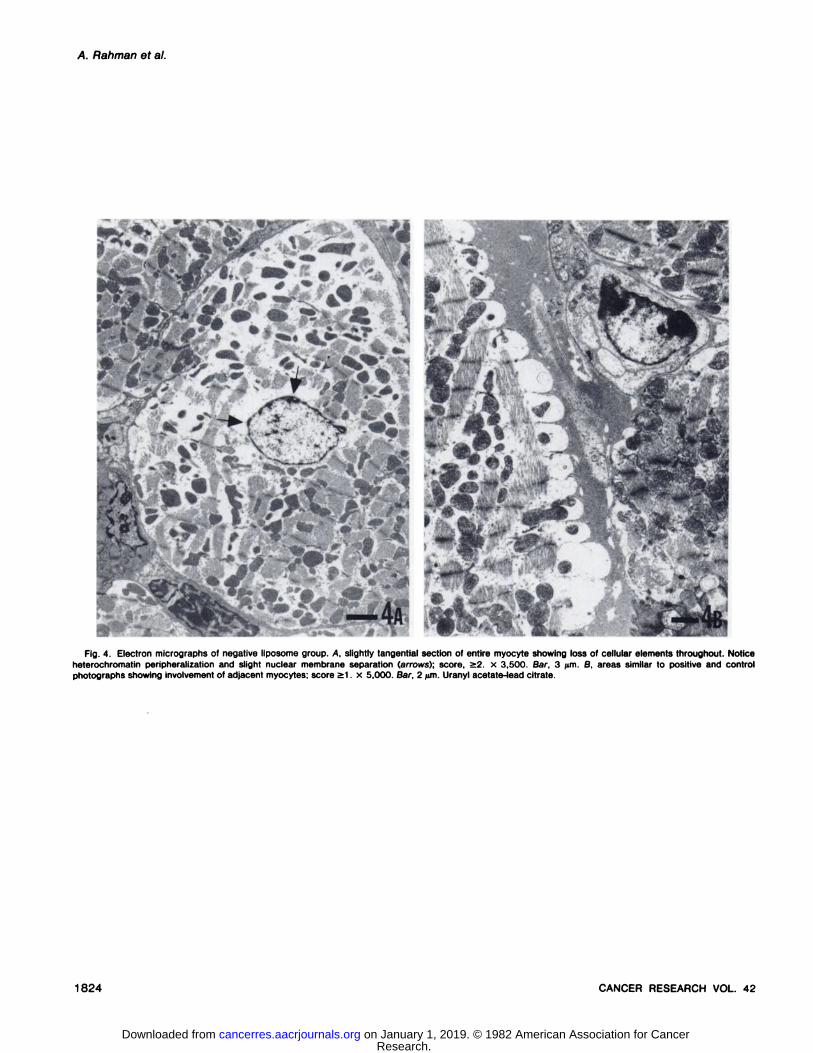
Fig. 4A presents the damage to cardiac tissue after administration of doxorubicin entrapped in negatively charged liposomes, as seen in a cross-section perpendicular to the length
of the myocytes. Loss of filaments is pronounced, enlargedmitochondria predominate the cleared spaces, and the nuclearmembrane is expanded. A point of interest is the early involvement of adjacent myocytes. Fig. 4ßis a similar area, but in thisexample the cut is longitudinal allowing visualization of thebanding pattern. Loss of myofilaments is evident in one my-ocyte, while a disorganized and disrupted Z-line pattern is seen
in the adjacent cell. The mitochondria in this cell appear to beswollen and losing their cristae, which is accompanied by atleast one early myelin inclusion body. This type of area wouldscore a 2 to 3 depending on the extent of the area covered.
Electron microscopic examination of the cardiac muscles ofmice treated with positive liposomes demonstrated a pictureconsistent with protection from drug-induced damage; there
was only minor loss of parallel fibrillar arrangement and myofilaments in limited focal areas (Fig. 5/\), while the majority ofthe tissue appeared normal when compared to controls. Asshown in Fig. 5A, normal vasculature and intercalation ofmyocytes were evident in mice treated with positive liposomes.Fig. 56 presents the limited nature of damage seen with thepositive liposomes. However, when compared to control tissue(Fig. 5, C and D), the overall morphology of this group of micewas regarded as normal and scored as Grade 1 (Table 1).
Table 2 represents statistical evaluation of the scoring oftoxic lesions recorded in the cardiac ultrastructure of differentgroups of mice treated either with free or liposomal entrappeddoxorubicin. The mean qualitative and quantitative scores forthe free doxorubicin group and the doxorubicin-entrapped-in-negative-liposomes group are 2.7 and 2.23, respectively. How
ever, the mean score for the group of mice treated with positiveliposomes is substantially reduced, with a value of 1.12 (p <0.05). There appears to be a better than 2-fold scoring protec
tion of both the extent and severity of cardiac lesions for themice treated with doxorubicin entrapped in positive liposomeswhen compared to the free drug.
DISCUSSION
The ultrastructural changes in the cardiac muscle of miceand rabbit after administration of doxorubicin observed in thisstudy have been well described previously (2, 11, 22). Distortion, fragmentation and loss of myofilaments, swelling, clearingand disruption of mitochondria, separation of the nuclear membrane, loss or depletion of ribosomal components, dilation ofthe sarcoplasmic reticulum, and myelin inclusion bodies arecharacteristic lesions. Each of these can be observed in varyingdegrees of severity and extent of involvement dependent upontotal dose and length of treatment and observation. In thecurrent study, the degree of damage could be correlated withthe particular regimen of doxorubicin administration; those
Liposomal Protection of Doxorubicin Chronic Cardiotoxicity
mice receiving free doxorubicin or doxorubicin entrapped innegatively charged liposomes showed more extensive damageultrastructurally than did mice receiving doxorubicin entrappedin positively charged liposomes.
Also evident in the samples examined was the focal natureof the lesions, as reported in other studies (5). In some areas,only one or 2 scattered myocytes were affected; whereas inother areas, there was evidence of confluent damage. There,light microscopy can be of assistance in determining topographic patterns of lesion distribution and severity. However,light microscopy could do little to determine the specific natureof the damage at the cellular level. Characteristics of the lesionswere varying degrees of vacuolization, apparent loss of myofilaments, myolysis, and atrophie degeneration.
The degree of protection of the cardiac muscle of micetreated with doxorubicin entrapped in positive liposomes hasbeen correlated with drug uptake in this organ. We havepreviously reported (20) that entrapment of doxorubicin inpositive liposomes results in a marked reduction in the in vivouptake of the drug in cardiac tissue when compared to freedrug and drug entrapped in negative liposomes. At 4 mg/kgi.V., the peak drug concentration in heart occurred in 30 minfollowing administration of free doxorubicin or doxorubicinentrapped in negative liposomes, the values being 8.3 and 9.1jug/g, respectively (Chart 1). In contrast, the peak cardiacuptake with doxorubicin encapsulated in positive liposomesoccurred at 5 min, and the drug equivalent was only 4.6 /ig/g.In addition, the cardiac concentration x time values for doxorubicin administered in positive liposomes were considerablyless than that of free drug or negative liposomes for the24-hr period of observation. Moreover, the antitumor activity of
doxorubicin was fully retained in P388 leukemia and Lewislung carcinoma in mice when administered in positive liposomes (20). In accordance with this pharmacological observation, the damage of cardiac tissue ultrastructurally for thegroup of mice treated with positive liposomes progresses onlyto the point of early toxic manifestations. No areas of extensivedegradation were observed in these mice, and damage waslimited to structural myofibrillar components, mitochondria, andsarcoplasmic reticulum. Absence of ribosomal material wasnoted in areas that were cleared of myofibers, and these werelimited in scope. Nuclear alterations were very slight, consisting
IO Free Doxorubicin
Doxorubicin Entrapped inNegatively Charged LiposomesDoxorubicin Entrapped inPositively Charged Liposomes
i j1234
Hours
Chart 1. Doxorubicin disposition in mice heart following i.v. administration offree and liposome-entrapped drug. oars. S.D. See Ref. 20 for experimentaldetails.
MAY 1982 1819
Research. on January 1, 2019. © 1982 American Association for Cancercancerres.aacrjournals.org Downloaded from

A. Rahman et al.
mainly of condensation of heterochromatin to the periphery ofthe nucleus.
Recently, Bertazzoli et al. (2) have demonstrated cardiacdegenerative lesions in mice similar to those described inhumans (14) after repeated i.v. administration of doxorubicin.A significant correlation between the lesion scores and thedoses of doxorubicin was demonstrated with a cumulativetoxicity dose of 36.4 mg/kg suggested. Our studies correlatewell with their observation with respect to morphological alteration in the cardiac tissue after repeated i.v. administration offree doxorubicin. However, entrapment of doxorubicin in positively charged liposomes affords a qualitative and quantitativeprotection of cardiac damage. As indicated in Table 2, there isa greater than 2-fold protection of both the extent and the
severity of cardiac lesions with the positive liposome regimen.In addition, other investigators (8, 9, 15) have shown thatdoxorubicin reduces cardiotoxicity in mice when administeredentrapped in aqueous phase of anionic liposomes. It appearsthat the method of preparation as well as the ratio of lipids usedto form the liposomes can possibly alter the disposition of theentrapped agent.
The major treatment-limiting toxicity of doxorubicin, asidefrom bone marrow depression, is cumulative and potentiallyirreversible cardiac damage. A drug delivery system whichselectively reduces the cardiac uptake of doxorubicin mayhave potential future applications if drug delivery to targettumor tissue is not diminished (23). In the present study, thereduced chronic cardiotoxicity of doxorubicin in the specificpositive liposomes suggests that this form of drug delivery mayhave potential for clinical use.
ACKNOWLEDGMENTS
The authors thank Karen O. Bivins for typing the manuscript.
REFERENCES
1. Bachur. N. R.. Moore. A. L.. Burnstein, J. G.. and Lio. A. A tissue distributionand disposition of daunomycin in mice. Fluorometric and isotopie methods.Cancer Chemother. Rep., 54 89-94, 1970.
2. Bertazzoli. C., Bellisin. 0., Magrini, U., and Tosaner, M. G. Quantitativeexperimental evaluation of Adriamycin cardiotoxicity in the mouse. CancerTreat. Rep.. 63. 1877-1883, 1979.
3. Bonadonna, G., DeLena, M. D., Monfardini, S., and Milani, F. Combinationchemotherapy with Adriamycin in malignant lymphoma. In: Adriamycin Review, pp. 200-215. Ghent. Belgium: European Press Medicon, 1975.
4. Bonadonna, G., Monfardini, S., DeLena, M. D., Fossati-Bellani, F.. andBereiter, G. Phase I and preliminary Phase II evaluation of Adriamycin (NSC-
123127). Cancer Res., 30. 2572-2582, 1970.5. Dantcher. D.. Slioussartchouk, V., Paintrand. M., Hayat, M., Bourut, C., and
Mathé,G. Electron microscopic studies of the heart and light microscopicstudies of the skin after treatment of golden hamsters with Adriamycin,detorubicin, AD-32 and aclacinomycin. Cancer Treat. Rep., 63 875-888.1979.
6. DiMarco. A.. Gaetani. M., and Scarpinato, B. Adriamycin (NSC-123127): anew antibiotic with antitumor activity. Cancer Chemother. Rep., 53. 33-37.1969.
7. DiMarco, A., Zunino, F.. Silvestrini, R., Gambarucci, C., and Gambetta, R.A. Interaction of some daunomycin derivatives with deoxyribonucleic acidand their biological activity. Biochem. Pharmacol., 20 1323-1328, 1971.
8. Forssen, E. A., and Tokes, Z. A. In vitro and in vivo studies with Adriamycinliposomes. Biochem. Biophys. Res. Commun., 97. 1295-1307, 1979.
9. Forssen. E. A., and Tokes, Z. A. Use of anionic liposomes for the reductionof chronic doxorubicin-induced cardiotoxicity. Proc. Nati. Acad. Sei. U. S.A., 78: 1873-1877. 1981.
10. Haanen, C., and Hillen, G. Combination chemotherapy with doxorubicin in"bad risk" leukemia patients. In: Adriamycin Review, pp. 193-199. Ghent,
Belgium: European Press Medicon, 1975.11. Jaenke, R. S. An anthracycline antibiotic induced cardiomyopathy in rabbits.
Lab. Invest., 30: 292-304, 1974.12. Juliano, R. L., and Stamp, D. Pharmacokinetics of liposome-encapsulated
antitumor drugs. Biochem. Pharmacol.. 27: 21-27, 1978.13. Kimelberg, H. K. Differential distribution of liposome-entrapped 3H-
methotrexate and labelled lipid after intravenous injection in a primate.Biochim. Biophys. Acta, 44: 531-550, 1976.
14. Lefrak, E. A.. Pitha, J., Rosenheim, S., and Gottlieb, J. A. A clinicopathologicanalysis of Adriamycin cardiotoxicity. Cancer (Phila.). 32. 302-314, 1973.
15. Maslow, D. E., Mayhew. E., Olson, F., and Rustum, Y Reduction of inhibitoryeffect of Adriamycin on myocardial contraction in vitro by entrapment inliposomes. Proc. Am. Assoc. Cancer Res., 21: 281, 1980.
16. Middleman. E., Luce. J., and Frei, E. Clinical trials with Adriamycin. Cancer(Phila.). 28. 844-850, 1971.
17. Oldham. R. K., and Pomeroy, T. C. Treatment of Ewing's sarcoma with
Adriamycin (NSC-123127). Cancer Chemother. Rep., 56 635-639, 1972.18. Philips, F. S.. Gilladoga, A., Marquardt, H., Sternberg, S. S., and Vidal, P.
M. Some observations on the toxicity of Adriamycin (NSC-123127). CancerChemother. Rep. Part III, 6. 177-181, 1975.
19. Rahman, A., Gutierrez. P.. Raschia, S.. Mhatre, R., and Schein, P. S.Pharmacokinetics of liposome-encapsulated doxorubicin. Fed. Proc., 40:685, 1981.
20. Rahman, A., Kessler, A., More, N., Sikic, B., Rowden, G., Woolley, P., andSchein, P. Liposomal protection of Adriamycin-induced cardiotoxicity inmice. Cancer Res.. 40: 1532-1537, 1980.
21. Rahman. A., Kessler, A., MacDonald, J.. Waravedkar. V., and Schein, P.Liposomal delivery of Adriamycin. Proc. Am. Assoc. Cancer Res., 20. 288,1979.
22. Rinehart, J. J.. Louis, R. P., and Balcerzak, S. P. Adriamycin cardiotoxicityin man. Ann. Intern. Med., 81: 475-478, 1974.
23. Trouet, A., Deprez-de Campeneere, D., and deDuve, C. Chemotherapythrough lysosomes with a DNA-daunorubicin complex. Nat. New Biol., 239.110-112, 1972.
24. Wang, J. J., Cortes, E., Sinks, L. F., and Holland, J. F. Therapeutic effectand toxicity of Adriamycin in patients with neoplastic disease. Cancer(Phila.), 28. 837-843, 1971.
25. Ward, D. C., Reich, E., and Goldberg. I. H. Base specificity in the interactionof polynucleotides with antibiotic drugs. Science (Wash. D. C.), 749: 1259,1965.
26. Yesair. D. W., Schwartzbach, E., Shuck. D., Denine, E. P., and Asbell, M. A.Comparative Pharmacokinetics of daunomycin and Adriamycin in severalanimal species. Cancer Res., 32. 1177-1183, 1972.
1820 CANCER RESEARCH VOL. 42
Research. on January 1, 2019. © 1982 American Association for Cancercancerres.aacrjournals.org Downloaded from
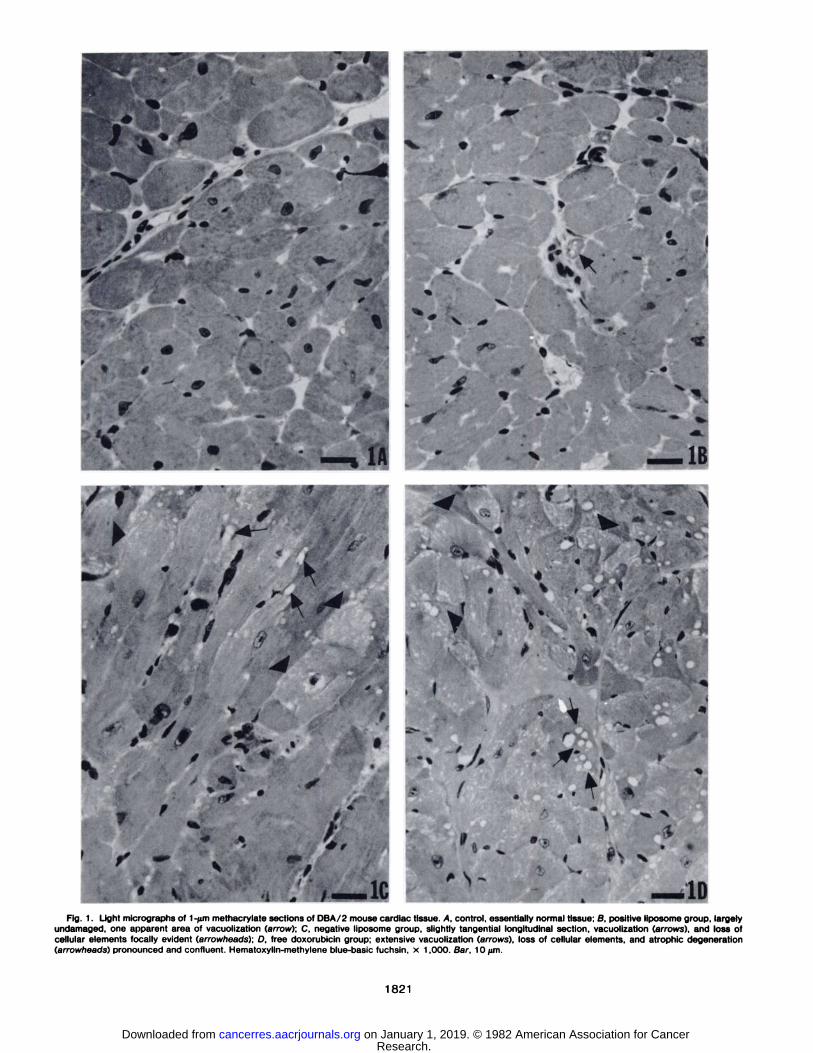
—10Fig. 1. Light micrographs of l -/im methacrylate sections of DBA/2 mouse cardiac tissue. A. control, essentially normal tissue; B. positive liposome group, largely
undamaged, one apparent area of vacuolization (arrow); C, negative liposome group, slightly tangential longitudinal section, vacuolization (arrows), and loss ofcellular elements focally evident (arrowheads); D, free doxorubicin group; extensive vacuolization (arrows), loss of cellular elements, and atrophie degeneration(arrowheads) pronounced and confluent. Hematoxylin-methylene blue-basic fuchsin, x 1,000. Bar, 10fim.
1821
Research. on January 1, 2019. © 1982 American Association for Cancercancerres.aacrjournals.org Downloaded from

Fig. 2. Electron micrographs of free doxorubicin group showing progression of cardiotoxic manifestations present simultaneously in any one sample. A. earlychanges; note swelling of sarcoplasmic compartments and reticulum (arrows), thinning of myofilaments, vacuolation separating vascular and myocyte cell membranes(sfar); apparently normal intercalated disc separates damaged and undamaged cells (arrowheads). X 3,500. Bar, 3 ¿im.ß,extensive loss of cellular elements seenas "clearing" of cell with concomitant disorganization of organelles. Note bizarrely distorted myocyte nucleus, fragments of myofilaments. and deposition of electron-
dense material (arrow); scores S3. x 3.500. Bar, 3 /im. C, severe atrophie degenerative state of myocyte showing replacement of elements with electron-densematerials, autophagic vacuoles, and myelin figures. Note bizarre and group mitochondria; score, «4. x 3,500. Bar, 3 ^m. Uranyl acetate-lead citrate.
1822
Research. on January 1, 2019. © 1982 American Association for Cancercancerres.aacrjournals.org Downloaded from

Fig. 3. Examples of specific damages in free doxorubicin cardiotoxicity group. A, distorted myocyte nucleus showing vacuolation and separation of nuclearmembrane, x 11.000. Bar, 1 /im. ß,mitochondria showing swelling and loss of cristae. Note total absence of internal structure, gaps, and fusion of adjacentmembranes, x 20.000. Bar, 4 /im. C, electron-dense materials and myelin bodies (arrows). Note enclosed former mitochondrion (star), x 20,000. Bar, 4 pm. D,separation of intercalated disc membranes and resultant "open" spaces. Note attached myofilaments. x 20.000. Bar, 4 /im. Uranyl acetate-lead citrate.
1823
Research. on January 1, 2019. © 1982 American Association for Cancercancerres.aacrjournals.org Downloaded from
A. Rahman et al.
<4?
"v •- •
Ai
..:% r̂Kw^Ãj»/*--^*^ '•£*NdS'Ãi*fe %Afefe5*«VJV* 'rlf SJWE^%A-»
*
%f*r«•»•"
Uk~
!•*^J
f ^
Fig. 4. Electron micrographs of negative liposome group. A, slightly tangential section of entire myocyte showing loss of cellular elements throughout. Noticeheterochromatin peripheralization and slight nuclear membrane separation (arrows); score. a2. x 3.500. Bar. 3 /im. B. areas similar to positive and controlphotographs showing involvement of adjacent myocytes: score ^1. x 5.000. Bar, 2 ¡on.Uranyl acetate-lead citrate.
1824 CANCER RESEARCH VOL. 42
Research. on January 1, 2019. © 1982 American Association for Cancercancerres.aacrjournals.org Downloaded from

Fig. 5. Electron micrographs of DBA/2 cardiac tissue. A, positive liposome group depicting normal endothelium and surrounding myocyte structure. Noteuniformities of myofilaments, banding patterns, arrangement of mitochondria, and intercalated discs (arrows), x 3,000. Bar, 3 um. B, positive liposome group:example of extent of limited focal nature of damage comparable to control (see D). Considered equivalent to early toxic damage rating -1 in scoring system.X 7,000. Bar, 1 /¿m.C, control group, nucleus of vascular endothelium with normal adjacent myocyte ultrastructure. X 7,000. Bar, 1 firn. D, control group,myofilament fragmentation presumed to be normal cellular processing occurring in minute areas although procedural artifact cannot be ruled out unequivocally;score. ~1. x 7.000. Bar, 1 /itn. Uranyl acetate-lead citrate.
1825
Research. on January 1, 2019. © 1982 American Association for Cancercancerres.aacrjournals.org Downloaded from

1982;42:1817-1825. Cancer Res Aquilur Rahman, Newton More and Philip S. Schein by Liposomal AdministrationDoxorubicin-induced Chronic Cardiotoxicity and Its Protection
Updated version
http://cancerres.aacrjournals.org/content/42/5/1817
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/42/5/1817To request permission to re-use all or part of this article, use this link
Research. on January 1, 2019. © 1982 American Association for Cancercancerres.aacrjournals.org Downloaded from