Type 2 Diabetes MellitusType 2 Diabetes MellitusTreating to TargetTreating to Target
January 22, 2004.
Dr. William Harper
Endocrinology & Metabolism
Assisstant Professor of Medicine
McMaster University
www.drharper.ca
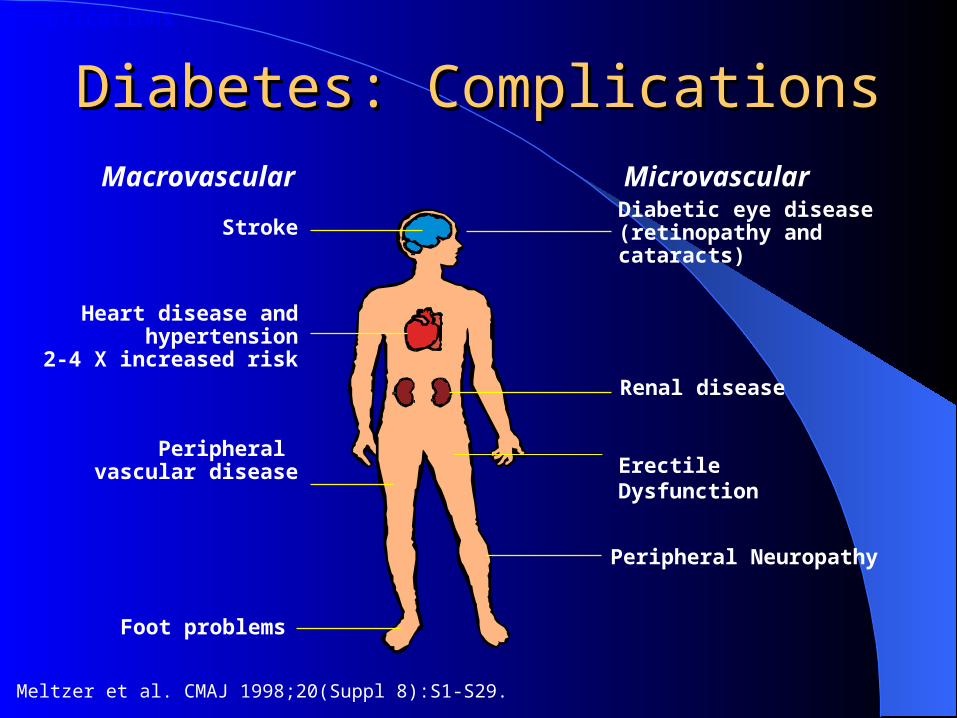
Macrovascular Microvascular
Stroke
Heart disease and hypertension
2-4 X increased risk
Foot problems
Diabetic eye disease(retinopathy and cataracts)
Renal disease
Peripheral Neuropathy
Peripheral vascular disease
Diabetes: ComplicationsDiabetes: Complications
Meltzer et al. CMAJ 1998;20(Suppl 8):S1-S29.
Complications
Erectile Dysfunction

Disease Burden of Diabetes MellitusDisease Burden of Diabetes Mellitus
• Leading cause of blindness (12.5% of cases)• Leading cause of ESRD (42% of cases)• 50% of all non-traumatic amputations• 2.5x increase risk of stroke• 2-4x increase in cardiovascular mortality• DM responsible for 25% of cardiac surgeries• Mortality in DM: 70% due to Cardiovascular
disease

Haffner et al, NEJM, 339(4):229-34, 1998.Haffner et al, NEJM, 339(4):229-34, 1998.

Evans et al.Evans et al.
BMJ 324: 939-942 April 2002 Cross-sectional study
DM 1155 patients MI 1347 patients
Cohort study DM 3477 patients MI 7414 patients

How is CAD Different in Diabetics ?How is CAD Different in Diabetics ?
> CAD extent Multi-vessel disease Distal disease – more difficult to revascularize
Silent ischemia/MIYoungerWomenWorse outcomes despite revascularization
Increased re-stenosis after PCI even with stents ACB: worse periop & long-term outcomes

T2DM: “Rx to Targets”T2DM: “Rx to Targets”What are the targets?

What are the targets?What are the targets?
Cardiovascular risk factor modification ASA, Smoking Cessation Lipids Blood Pressure
• Proteinuria/DM nephropathy• Angiotensin II attenuation benefits independent of BP
Glycemic control Microvascular benefit Macrovascular benefit ? Target insulin resistance > insulin deficiency ?

Canadian Lipid Working Group:Canadian Lipid Working Group:Target Levels in DiabetesTarget Levels in Diabetes
Canadian recommendations place patients with diabetes in “very high” risk group for CAD
LDL TC/HDL ratio TG
< 2.5 mmol/L < 4 < 2.0
mmol/L
Statins effective in lowering LDL1
Fibrates are useful for raising HDL, lowering TG1,2
Some OHA may improve lipids, but are not indicated for lipid management3
may need to use combo or Niacin cautiously

Heart Protection Study & DMHeart Protection Study & DM n = 20,530 (3982 with Diabetes Mellitus) hi-risk patients
age 40-80, prior CAD or PVD, DM, HTN (males age > 65) Non-fasting TC > 3.5 mM
5.5 year RCT: Simvastatin 40 mg od vs placebo Mortality ARR 1.8% (NNT 56) Vascular Event ARR 5.4% (NNT 19)
– Coronary event, Stroke, Revascularisation
Benefit obtained even in low cholesterol patients: LDL baseline 2.5 mM 1.7 mM with Rx Prior LDL targets for hi-risk patients too high?
– Canadian Lipid Work Group 2.5 mM– NCEP 2.6 mM– CARE 3.2 mM

Heart Protection StudyHeart Protection Study

Lipids & DMLipids & DM
What about HDL & TG?Fibrates > Statins at HDL and TGVA-HIT, a “low HDL Study”
2531 patients (620 DM), hi-risk with prior CAD HDL < 1.0 mM, TG < 3.4 mM, LDL < 3.6 mM RCT Gemfibrozil 600 mg po bid Coronary death or MI ARR 4.4% (NNT 23) LDL 2.3-3.6 mM at baseline Not on a statin despite LDL > 2.5 mM
Lipids & DMLipids & DM
In DM patients where LDL is already adequately controlled by a statin, will the addition of a fibrate provide further benefit?
ACCORD: 10,000 patients with ½ Lipid control arm RCT: simvastatin + fenofibrate v.s. placebo Results…

What are the targets?What are the targets?
Cardiovascular risk factor modification ASA, Smoking Cessation Lipids Blood Pressure
• Proteinuria/DM nephropathy• Angiotensin II attenuation benefits independent of BP
Glycemic control Microvascular benefit Macrovascular benefit ? Target insulin resistance > insulin deficiency ?
DM: BP cntrlDM: BP cntrl
Difficult to consider BP cntrl in DM without also taking into account:
Proteinuria/DM nephropathy Cardiovascular benefit of reducing angiotensin II
action independent of BP

Renin-Angiotensin-Aldosterone AxisRenin-Angiotensin-Aldosterone Axis
Angiotensinogen(Renin substrate)
Angiotensin I Angiotensin II
Renin+
ACE
BradykininCoughRash -
Aldosterone
Na retentionK+ & H+ loss
ARB (ex. Losartan/Cozaar)
ACE-IACE-I (ex. Ramipril/Altace)

BP Trials in DM patients (some)BP Trials in DM patients (some)
UKPDSHOTALLHATLIFEHOPE
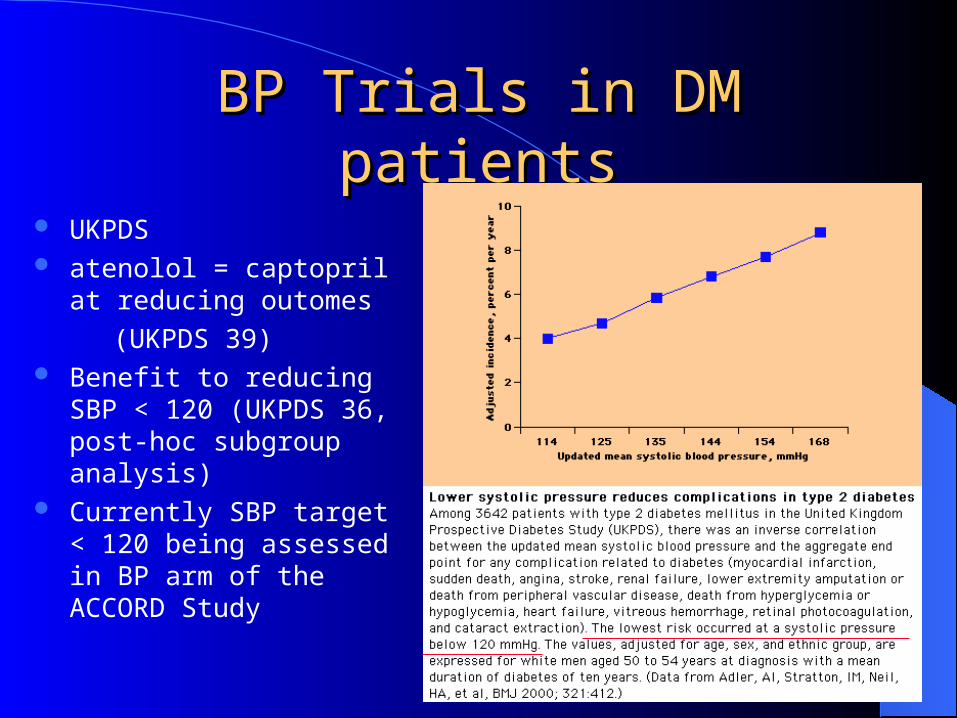
BP Trials in DM patientsBP Trials in DM patients
UKPDS atenolol = captopril at
reducing outomes
(UKPDS 39) Benefit to reducing SBP <
120 (UKPDS 36, post-hoc subgroup analysis)
Currently SBP target < 120 being assessed in BP arm of the ACCORD Study

BP Trials in DM patientsBP Trials in DM patients
UKPDS: atenolol = captopril in events HOT: felodipine, CV events with DBP < 80 ALLHAT
Chlorthalidone > lisinopril or amlodipine (less CHF) Chlorthalidone BS/diagnosis of DM
LIFE (DM substudy) 1195 patients with DM/HTN/LVH Losartan > atenolol in CV death/MI/CVA despite equivalent
BP lowering effects
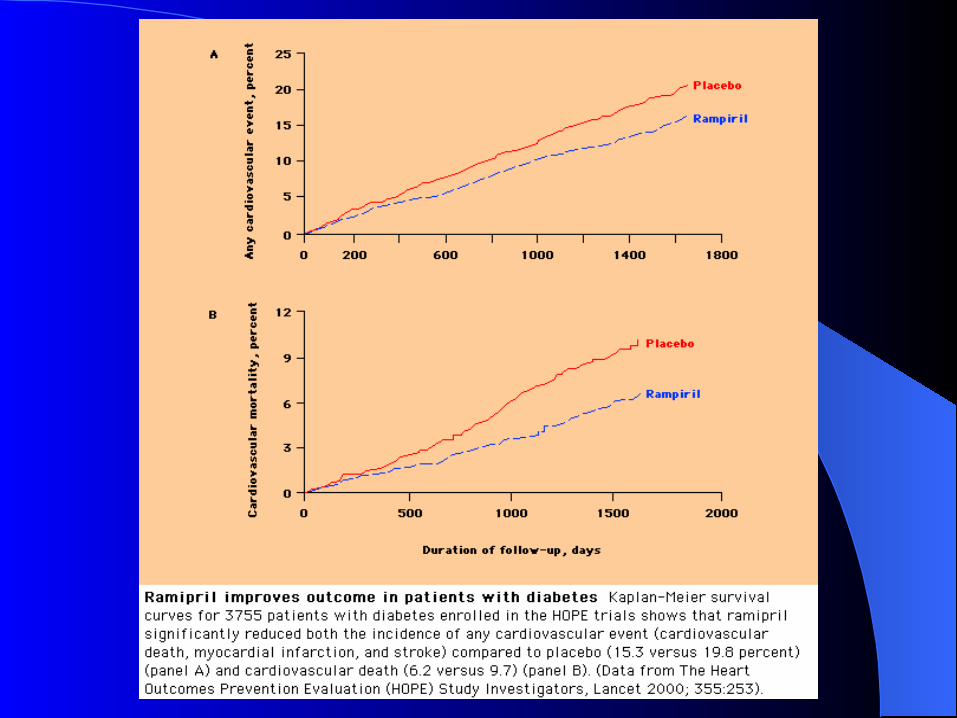
HOPE: not a BP trial per se

Effect of ACE InhibitionEffect of ACE Inhibitionin Diabetesin Diabetes
HOPE StudyHOPE StudyRelative Risk Reduction of Ramipril vs. Placebo in Subjects with Diabetes
22% Myocardial infarction p = 0.01
33% Stroke p = 0.0074
37% Cardiovascular death p = 0.0001
24% Overt nephropathy p = 0.027
17% Revascularization p = 0.031
20% Heart failure p = 0.019
HOPE investigators. Lancet 2000;355:253-259.
Complications
DM > 55 yo & 1 additional CV risk factor
(HTN, microalbuminuria, current smoker, TC > 5.2 mM, HDL < 0.9 mM)

DM NephropathyDM Nephropathy
Microalbuminuria: 30-300 mg/d (20-200 ug/min)Macroalbuminuria: > 300 mg/d (> 200 ug/min)

DM Nephropathy & BPDM Nephropathy & BP
T1DM: ACE-I albumin excretion and progression to overt
nephropathy (macroalbuminuria) in patients with microalbuminuria even if BP is normal
ACE-I progression to ESRD or death in patients with overt nephropathy and serum creat > 132 uM

DM Nephropathy & BPDM Nephropathy & BP
T2DM: ACE-I & ARB progression of micro to macro albuminuria In contrast to T1DM, no demonstrated benefit of ACE-I over
other anti-HTN (ex. UKPDS 39 captopril vs atenolol) in preventing ESRD in patients with overt nephropathy
ARBs have been shown to be renal protective in T2DM with overt nephropathy:
• IDNT: irbesartan (Avapro) ESRD/death/creat 2x• RENAAL: losartan (Cozaar) creat 2x and ESRD
• Note: in both IDNT and RENAAL all ACE-I were stopped during the study

ACE-I & ARB Combination?ACE-I & ARB Combination?
STENO-2: part of a multifactorial approach (only 28% patients)
CHF Studies: CHARM: candesartan (Atacand) mortality, CHF admits, and
onset of DM Val-HeFT: valsartan (Diovan) CHF admits
CALM Study: Mogensen et.al. BMJ 2000;321:1440-1444 T2DM, HTN, microalbuminuria candesartan & lisinopril (Zestril, Prinivil) 12 wk study outcomes: BP, proteinuria

CALM StudyCALM Study
Combo Rx with candesartan & lisinopril reduced BP
Lisinopril reduced proteinuria Candesartan reduction of
proteinuria was NS either alone or in combination with lisinopril

BP Cntrl in DM: BP Cntrl in DM: CHEPCHEP guidelines guidelines
Canadian Hypertension Education Program BP target:
< 130/80 (SBP 120? (ACCORD) / HOT target DBP 80) < 125/75 Proteinuria > 1 gm/d
Initial therapy 2nd line therapy
DM with nephropathy ACE-I or ARB Addition of 1 or more of thiazide, -blocker, CCB, or
an ACE-I/ARB combo
DM without nephropathy ACE-I, ARB, or thiazide Combo of 1st line drugs or addition of -blocker and/or
CCB

What are the targets?What are the targets?
Cardiovascular risk factor modification ASA, Smoking Cessation Lipids Blood Pressure
• Proteinuria/DM nephropathy• Angiotensin II attenuation benefits independent of BP
Glycemic control Microvascular benefit Macrovascular benefit ? Target insulin resistance > insulin deficiency ?

Glycemic ControlGlycemic Control
UKPDS 33, Lancet 352:837-53, 1998.RCT of a policy of intensive BS control
FPG < 6 mM v.s. FPG < 15 mM Achieved a number of ways:
– Sulfonylurea (chlorpropamide or glibenclamide/glyburide)
– Metformin (overweight subgroup, add-on)
– Insulin (bedtime basal +/- basal/bolus regimens)

UKPDS 33: Main studyAny DM related end point: 12% RRRMicrovascular complications: 25% RRR
Reduced eye disease: retinal laser Sx (19%), cataract Sx (24%), DM retinopathy (21%)
33% RRR microalbuminuria, 74% RRR in doubling of creatinine
MI: 16% RRR (P = 0.052 NS)No mortality benefit
Glycemic Control & ComplicationsGlycemic Control & Complications

UKPDS 34: overweight metformin substudy Unlike sulfonylurea & insulin: no weight gain Any DM related end point: 32% RRR DM related death: 42% RRR All cause mortality: 36% RRR MI: 39% RRR Metformin + SU: increased mortality?
DM related 96%, All-cause 60%
Glycemic Control & MetforminGlycemic Control & Metformin

T2DM & Macrovascular diseaseT2DM & Macrovascular disease
Why no clear benefit in UKPDS to glycemic cntrl? Low CV risk patients:
UKPDS cntrl death rate: 1.2 % per year HOPE cntrl death rate: per year 2.5% per year
Unable to maintain glycemic cntrl due to limited interventions: Available: glyburide, chlorpropamide, metformin, regular insulin No newer sulfonylureas: glimepiride (Amaryl), gliclazide (diamicron) No meglitinides: repaglinide (Gluconorm), nateglinide (Starlix) No TZD’s: rosiglitazone (Avandia), pioglitazone (Actos) No insulin analogues: (Humalog, Novorapid, Lantus)

Natural History of Type 2 DiabetesNatural History of Type 2 Diabetes
Normal Impaired glucosetolerance
Type 2 diabetes
Time
Insulinresistance
Insulinproduction
Glucoselevel
-celldysfunction
Henry. Am J Med 1998;105(1A):20S-6S.

DCCT, NEJM 329:977-86, 1993.
UKPDS 33, Lancet 352:837-53, 1998.

Traditional Therapies Do Not Traditional Therapies Do Not Influence Influence -Cell Failure-Cell Failure
cohort, median valuesoverweight patients
06
7
8
9
10
-1 0 2 4 6 8 10Years from randomisation
ChlorpropamideConventionalGlibenclamideInsulin
Metformin
HbA
1c (
%)
UKPDS 34. Lancet 1998; 352: 854-865
0
20
40
60
80
100
0 1 2 3 4 5 6 7ß
cel
l fun
ctio
n (%
)0
20
40
60
80
100
0 1 2 3 4 5 6 7
ß c
ell f
unct
ion
(%)
Years from randomisationConventional Sulphonylurea Metformin
Non obese � ObeseOverweightNon-Overweight
UKPDS 16: Diabetes 1995; 44: 1249-1258

Control Zucker Rats ROSIG Zucker Rats
12 weeks
16 weeks
Thiazolidinedione Thiazolidinedione ββ-cell preservation: -cell preservation: Animal studiesAnimal studies

GLUCOSE ABSORPTION
GLUCOSE PRODUCTION
Metformin Thiazolidinediones
MUSCLE
PERIPHERAL GLUCOSE UPTAKE Thiazolidinediones Metformin
PANCREAS
INSULIN SECRETION Sulfonylureas: Glyburide, Gliclazide, Glimepiride Non-SU Secretagogues: Repaglinide, Nateglinide
ADIPOSE TISSUELIVER
Alpha-glucosidase inhibitors
INTESTINE
Adapted from Sonnenberg, Kotchen Curr Opin Nephrol Hypertens 1998; 7:551-5.
Sites of Action of Currently Sites of Action of Currently Available Therapeutic OptionsAvailable Therapeutic Options

Drug Trade Dose Cost ODB
Glyburide Diabeta Start 1.25-5 mg od
Spit dose bid > 10mg/d
Max 10 mg bid
$14/mos Yes
Gliclazide Diamicron Start 80 mg bid
Max 160 mg bid$90/mos No
Gliclazide
MRDiamicron
MR
Start 30 mg od
Max 120 mg od$30/mos Exp Sect 8
Glimepiride Amaryl Start 1-2 mg od
Max 8 mg od$30/mos No
Repaglinide Gluconorm Start 0.5 mg tid-qid
Max 4 mg qid$45/mos Exp Sect 8
Nateglinide Starlix Start 60-120 mg tid
Max 180 mg tid$45/mos No
Metformin Glucophage Start 500 mg od-bid
Max 1000 mg bid$14/mos Yes
Pioglitazone Actos Start 15-30 mg od
Max 45 mg od$92/mos Exp Sect 8
Rosiglitazone Avandia Start 4 mg od
Max 4 mg bid$ 60/mos
$ 120/mos
Exp Sect 8

Gliclazide 2+ + 0 0 +
Glimepiride 2+ + 0 0 +
Repaglinide 1+ + 0 0 0 0 +
Nateglinide 1+ ? 0 0 0 0 +
Metformin 0 0 0 2+ + 0 -
Acarbose 0 0 0 3+ 0
Rosiglitazone 0 + + 0 0 * +
Pioglitazone 0 + + 0 0 * +
Hypoglycemia Wt. Gain Edema GI Lactic Liver Use in effects Acidosis Toxicity Renal Failure
Adapted from Lebovitz H: Endocrinol & Metab Clinics of NA; 30 (4)909-933
* Liver enzyme monitoring recommended in product monographs
Glyburide 4+ + 0 0 -

TZD adverse effectsTZD adverse effects Edema
4-5% of patients get mild-moderate edema 15% if TZD used in combo with insulin
Mild anemia (dilutional) Weight gain
Increase in subcutaneous not visceral fat
Myalgia (pioglitazone only) Myalgia 5.4% pioglitaz. versus 2.7% placebo Few patients with unexplained CK > 10x ULN
Contraindicated in class II, III and IV CHF
Contraindicated if ALT > 2.5x ULN or active liver disease

Metabolic Syndrome: Clinical DiagnosisMetabolic Syndrome: Clinical Diagnosis
Presence of any 3 of the following: Abdominal obesity (M > 102 cm, F > 88 cm) TG > 1.7 mM Low HDL (M < 1.0 mM, F < 1.3 mM) BP > 130/85 FPG > 6.1 mM


TZDs: effect on Metabolic SyndromeTZDs: effect on Metabolic Syndrome
Reduce insulin resistance/blood sugar Mild decrease in diastolic BP (2-4 mmHg) Decrease PAI-1 (reduces procoagulant state) Lipids:
– ↓TG ↑HDL (pioglitazone > rosiglitazone?)– ↓LDL (pioglitazone)– ↑LDL (rosiglitazone)
No change in ApoB so ↑ due to larger less atherogenic particle size
Decrease in carotid artery intimal-media thickness (IMT)

Targeting Insulin Resistance?Targeting Insulin Resistance?
Does targeting insulin resistance > insulin secretion reduce CV risk?
We don’t know yet! BARI-2D:
CV outomes Insulin sparing regimen (avandia, metformin)
versusInsulin providing regimen (sulfonylurea, insulin)
PPAR, RECORD, PROACTIVE TZD’s, CV outcomes

Targeting insulin Secretion?Targeting insulin Secretion?
Improve glycemic control in hi-risk patients to reduce CV risk Using novel agents to get there! ACCORD – glycemic cntrl arm HbA1c < 6 %
glimepiride, insulin glargine, (and rosiglitazone)
NAVIGATOR – nateglinide DIGAMI II - insulin ORIGIN, STREAM – insulin glargine

InsulinInsulin
Type Starts Peaks Duration
Humalog
NovoRapid
5-10 min 0.5-1hrs 3.5 hrs
Regular 30 min 2-4 hrs 6-8 hrs
NPH
Lente
1-2 hrs 6-10 hrs 16-24 hrs
Ultralente 4-6 hrs 8-24 hrs 24-36 hrs
Glargine 1.5h None Up to 24 hrs

Insulin Glargine (Lantus)Insulin Glargine (Lantus)
Substitution of glycine and arginine residues gives name “glargine” 2 arginine residues make glargine more soluble in acidic pH of injection medium
but less soluble in physilogic pH of subQ tissues Once injected, glargine precipitates leading to slower absorption Glycine substitution prevents degradation in subQ tissues

Insulin Glargine (Lantus)Insulin Glargine (Lantus)
Little to no peak effect Less hypoglycemia

Insulin Glargine (Lantus)Insulin Glargine (Lantus)

BIDS TherapyBIDS Therapy
T2DM: “Introduction to insulin”Keep on OHAsStart 0.2 U/kg SC qhs NPH or LantusIncrease by 2-4 U q4d until FBS 4-7

Putting it all togetherPutting it all together
Any evidence that a multifactorial approach (targeting glycemic cntrl, BP, lipids, proteinuria, etc.) works?

Multifactorial DM Rx: STENO-2Multifactorial DM Rx: STENO-2Jan 2003, NEJM 348:383-93RCT mimicking real life clinic160 T2DM patients with microalbuminuriaRandomized:
Conventional Rx as per National Guidelinesversus
Intensive Rx• Behaviour modification• Pharmacotherapy: targeting BS, BP, Lipids,
proteinuria, ASA (initially 2 prevention only, 1 prevention after 1999)

Multifactorial DM Rx: STENO-2Multifactorial DM Rx: STENO-2

Multifactorial DM Rx: STENO-2Multifactorial DM Rx: STENO-2

UKPDS 33, Lancet 352:837-53, 1998.
STENO-2, NEJM, 348:383-93, 2003.
DCCT, NEJM 329:977-86, 1993.

Multifactorial DM Rx: STENO-2Multifactorial DM Rx: STENO-2

Bottom Line: T2DM SurveillanceBottom Line: T2DM Surveillance
HbA1c, BP: q3mos UMALB/Creat ratio: q6mos - q1y Dilated eye exam q1-2y Feet exam at least q1y Cardiac GxT:
as indicated (symptoms, prior to new exercise regime)

Bottom Line: T2DM InterventionBottom Line: T2DM Intervention BP cntrl:
Target: < 130/80 (< 120/75 if proteinuria > 1g/d) 1st Line:
– HOPE criteria met: ACE-I, ARB if ACE-I intolerant
– No HOPE criteria: ARB 2nd Line: Thiazide 3rd Line: -blocker or DHP-CCB (Norvasc, Plendil) Combine ACE-I + ARB ? (watch K+!)
– CHF (as per CHARM or Val-HeFT)
– Overt nephropathy + HOPE criteria met
Angiotensin II blockade: Altace even if normal BP if HOPE criteria met
> 55 y & 1 CV risk factor: HTN, microalbuminuria, current smoker, TC > 5.2 mM, HDL < 0.9 mM

Bottom Line: T2DM InterventionBottom Line: T2DM Intervention Proteinuria
BP < 120/75, HbA1c < 7.0 % No HOPE: ARB HOPE Criteria met, microalbuminuria: ACE-I HOPE Criteria met, macroalbuminuria: ACE-I + ARB (watch K+!)
Lipids age > 40 or vascular disease, regardless of lipid profile Zocor 40 mg/d target LDL 2.5 mM Still hi TG, low HDL: consider gemfibrozil or niacin
• TG > 6.0-11.0 mM: risk of pancreatitis
ECASA 81 mg/d, Smoking cessation 2 prevention CAD: -blocker, ACE-I
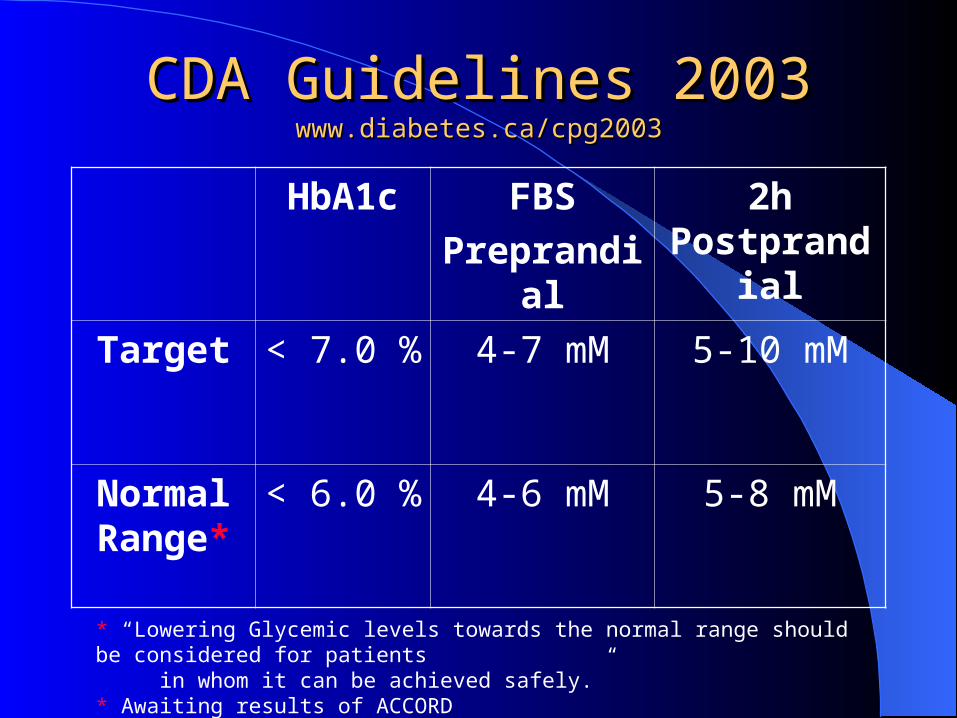
CDA Guidelines 2003CDA Guidelines 2003www.diabetes.ca/cpg2003www.diabetes.ca/cpg2003
HbA1c FBS
Preprandial
2h Postprandial
Target < 7.0 % 4-7 mM 5-10 mM
Normal Range*
< 6.0 % 4-6 mM 5-8 mM
* “Lowering Glycemic levels towards the normal range should be considered for patients in whom it can be achieved safely.”* Awaiting results of ACCORD

Clinical assessment and initiation of nutrition and physical activity
Mild to moderate hyperglycemia (A1C <9.0%)
Overweight(BMI 25 kg/m2)
Non-overweight(BMI 25 kg/m2)
Biguanide alone or incombination with 1 of:
• insulin sensitizer*• insulin secretagogue• insulin• alpha-glucosidase inhibitor
1 or 2† antihyperglycemicagents from differentclasses
• biguanide• insulin sensitizer*• insulin secretagogue• insulin• alpha-glucosidase inhibitor
Add a drug from a different class orUse insulin alone or in combination with:
• biguanide• insulin secretagogue• insulin sensitizer*• alpha-glucosidase inhibitor
Marked hyperglycemia (A1C 9.0%)
2 antihyperglycemic agentsfrom different classes †
• biguanide• insulin sensitizer*• insulin secretagogue• insulin• alpha-glucosidase inhibitor
Basal and/orpreprandial insulin
Add an oral
antihyperglycemic agentfrom a differentclass of insulin*
Intensify insulinregimen or add
• biguanide• insulin secretagogue**• insulin sensitizer*• alpha-glucosidase inhibitor
If not at targetIf not at targetIf not at targetIf not at target
L
I
F
E
S
T
Y
L
E
Timely adjustments to and/or additions of oral antihyperglycemic agentsand/or insulin should be made to attain target A1C within 6 to 12 months

Bottom Line: T2DM InterventionBottom Line: T2DM Intervention
Glycemic control: HbA1c < 7.0 % 1st line: insulin sensitizer (no hypoglycemia)
• Metformin (UKPDS sub-study, weight-sparing, $)• Thiazolidinedione (potential pleiotrophic benefits)• Metformin + Thiazolidinedione also possible
2nd line: insulin secretagogue• elderly, CrCl ?• Amaryl, Diamicron, Gluconorm, Starlix > Glyburide
3rd line: insulin (analogues > regular)• Lantus: lower FBS, less nocturnal hypo• Humalog, Novorapid: lower postprandial BS, less hypo
The EndThe End








