
plastin time, antithrombin III activity, factor VII activity andantigen, factor XII activity, protein C and protein S activity,heparin cofactor II, plasma homocysteine level, lupus antico-agulant (Exner, DRVVT), anticardiolipin antibodies (IgG,IgM), activated protein C-response, plasminogen activity,fibrinogen, tissue plasminogen activator antigen, and plas-minogen activator inhibitor activity and antigen. Plasmahistidine-rich glycoprotein levels were recurrently found to beelevated at 220%, however (reference range, 60%–148%,electroimmunodiffusion according to Laurell).
Since its first description in 1972, a few authors havereported an association between abnormal plasma levels ofhistidine-rich glycoprotein and systemic thromboembolicevents.4,5 We are unaware, however, of previous reports ofan association between increased plasma levels of histi-dine-rich glycoprotein and retinal vessel occlusion andcould find no reference to it in a computerized search usingMEDLINE.
Histidine-rich glycoprotein is a nonenzymatic proteinpresent in human plasma and platelets. It has beendemonstrated that histidine-rich glycoprotein interactswith the high-affinity lysine-binding site of plasminogen,which appears to play an important role in the regulationof fibrinolysis. Moreover, it has been found to interactstrongly with heparin, resulting in neutralization of theanticoagulant activity of heparin.6 Interestingly, both,increased4 and decreased levels5 of histidine-rich glyco-protein have been found in patients with deep veinthrombosis, lung embolism, or myocardial infarction.
In view of the absence of cardiovascular risk factors,we believe this case represents a coagulopathy secondaryto increased plasma levels of histidine-rich glycoprotein.It is plausible that increased plasma histidine-rich gly-coprotein levels are a risk factor for development ofocular vascular complications as they are for othervascular occlusions.
REFERENCES
1. Greiner K, Hafner G, Dick B, Dirk PE, Prellwitz W, Pfeiffer N.Retinal vascular occlusion and deficiency in the protein cpathway. Am J Ophthalmol 1999;128:69–74.
2. Incorvaia C, Lamberti G, Parmeggiani F, et al. Idiopathiccentral retinal vein occlusion in a thrombophilic patient withthe heterozygous 20210 G/A prothrombin genotype. Am JOphthalmol 1999;128:247–248.
3. Hattenbach LO, Klais C, Scharrer I. Heparin cofactor IIdeficiency in central retinal vein occlusion. Acta OphthalmolScand 1998;76:758–759.
4. Hennis BC, van Boheemen PA, Koeleman BPC, et al. Aspecific allele of the histidine-rich glycoprtein (HRG) locus islinked with elevated plasma levels of HRG in a Dutch familywith thrombosis. Br J Haematol 1995;89:845–852.
5. Souto JC, Gari M, Falkon L, Fontcuberta J. A new case ofhereditary histidine-rich glycoprotein defieciency with famil-ial thrombophilia. Thromb Haemost 1996;75:374–375.
6. Lijnen HR, Hoylaerts M, Collen D. Isolation and character-ization of human plasma protein with high affinity for lysinebinding sites in plasminogen. J Biol Chem 1980;225:10214–10222.
Trypan Blue Not Toxic for RetinalPigment Epithelium In VitroPeter Stalmans, MD, PhD,Elisabeth H. Van Aken, MD, PhD,Gerrit Melles, MD, PhD, Marc Veckeneer, MD,Eric J. Feron, MD, andIngeborg Stalmans, MD, PhD
PURPOSE: To investigate whether trypan blue has a toxiceffect on cultured retinal pigment epithelial (retinalpigment epithelium) cells.DESIGN: Experimental study with a direct live/dead cellstaining technique using fluorescent dyes.METHODS: Cultured human retinal pigment epitheliumcells were exposed for 5 minutes to various concentra-tions of trypan blue (0.06%, 0.15%, 0.30%), and cellviability was confocally measured.RESULTS: No increased cell death was found in culturesincubated in any of the trypan blue concentrations used.CONCLUSION: These findings indicate that a short expo-sure of trypan blue does not have a toxic effect oncultured retinal pigment epithelium cells. (Am J Oph-thalmol 2003;135:234–236. © 2003 by Elsevier Sci-ence Inc. All rights reserved.)
OVER THE PAST FEW YEARS, TRYPAN BLUE 0.06% HAS
been widely used for staining the anterior lenscapsule to facilitate the capsulorhexis during cataractsurgery in mature white cataract.1 Trypan blue is notapproved or available in the United States at this time,however.
More recently, clinical trials have been published stud-ies on trypan blue as an aid in vitreoretinal surgery forstaining epiretinal membranes in proliferative vitreoreti-nopathy2 or for macular pucker removal.3 After a contacttime of 1 to 3 minutes, trypan blue stains epiretinalmembranes at a concentration of 0.15% without stainingthe underlying neural retina.2,3
Accepted for publication Sept 4, 2002.From the Department of Ophthalmology (P.S., I.S.), UZLeuven,
Leuven, Belgium; Department of Ophthalmology (E.H.v.A.), GhentUniversity Hospital, Ghent, Belgium; Netherlands Institute for Innova-tive Ocular Surgery (G.M.) and Rotterdam Eye Hospital (M.V., E.J.F.),Rotterdam, The Netherlands; the Center for Transgene Technology andGene Therapy (I.S.), Flanders Interuniversity Institute for Biotechnol-ogy, KU Leuven, Belgium.
This study was supported by a grant from the Foundation for Researchin Ophthalmology, Belgium. Doctors Elisabeth H. Van Aken andIngeborg Stalmans are research assistants of the Fonds voor Wetenschap-pelijk Onderzoek—Flanders, Brussels, Belgium.
Dr. Melles has proprietary and financial interest in commerciallyavailable solutions of trypan blue for intraocular use (VisionBlueTM andMembraneBlueTM, D.O.R.C., Zuidland, The Netherlands).
Inquiries to Peter Stalmans, MD, PhD, Department of Ophthalmology,UZLeuven, Capucijnenvoer 33, B3000 Leuven, Belgium; e-mail: [email protected]
AMERICAN JOURNAL OF OPHTHALMOLOGY234 FEBRUARY 2003
Toxicity of trypan blue on the neural retina has beenevaluated in rabbit experiments,4 but toxicity on theretinal pigment epithelium remains to be determined.Because trypan blue may potentially contact the retinalpigment epithelium during vitreoretinal surgery, we inves-tigated the cytotoxicity on trypan blue on retinal pigmentepithelium cells in vitro.
In an experimental study, retinal pigment epitheliumcells were obtained from human cadaver eyes as describedearlier.5 Primary culture was obtained by explanting retinalpigment epithelium fragments in RPMI 1640 medium,supplemented with 20% fetal calf serum, 2 mmol/l L-glu-tamine, 100 IU/ml penicillin, 100 �g/ml streptomycin, and2.5 �g/ml fungizone. The retinal pigment epithelium cell linewas isolated by trypsin treatment from the primary culture.The epithelial origin of the cultured retinal pigmentepithelium cells was demonstrated by cytokeratin.
Cell viability was measured using a Zeiss confocalmicroscope with a 10� objective as described previously.5Briefly, the cells were loaded by a 30-minute incubationwith a live/dead fluorescent kit. They were excited at 488nm to stain viable cells with calcein-AM and at 540 nm tostain dead cells with ethidium homodimer-1 dye. The488-nm images obtained were processed using imagingsoftware. After thresholding the images, the fluorescentcells were automatically counted using the particle analyzefunction. The 540-nm images were manually analyzed to
avoid false measurements related to the autofluorescense ofthe trypan blue dye at its higher concentration.
For control experiments, a phosphate-buffered solutionwas used. A concentration of typan blue 0.3% was ob-tained by dissolving 60 mg in 2 ml phosphate bufferedsolution. The 0.06% concentration was obtained by dilut-ing the 0.3% concentration five times in buffered saltsolution. The concentration 0.15% (Membrane Blue,D.O.R.C., Zuidland, The Netherlands) was provided bythe manufacturer.
Osmolarity measurements were performed with a cryo-scopic osmometer. Statistical analysis was performed usinga Student t test with unpaired and two-tailed data and withunequal variance. A significance of P � .01 was predeter-mined.
A measurement of the osmolarity of the solutions wasperformed to exclude any cellular toxicity related to theosmolarity of the dyes.5 All solutions (phosphate bufferedsolution and trypan blue concentrations) were found to bein the iso-osmotic range (phosphate buffered solution: 289mOsm/kg, trypan blue 0.06%: 296 mOsm/kg, trypan blue0.15%: 298 mOsm/kg, trypan blue 0.30: 309 mOsm/kg).
To determine whether any of the solutions showedautofluorescence that could induce false-positive measure-ment, all conditions were measured without any live/deadsolution. No autofluorescense was found in either the488-nm or 540-nm spectrum after incubation in the
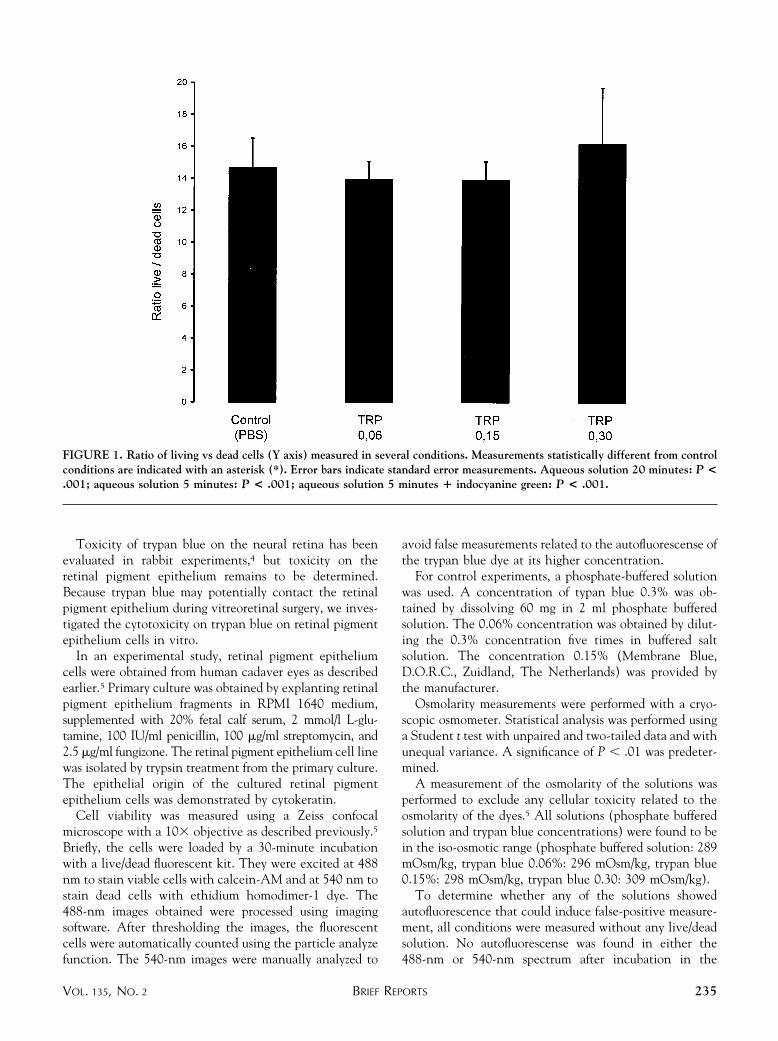
FIGURE 1. Ratio of living vs dead cells (Y axis) measured in several conditions. Measurements statistically different from controlconditions are indicated with an asterisk (*). Error bars indicate standard error measurements. Aqueous solution 20 minutes: P <.001; aqueous solution 5 minutes: P < .001; aqueous solution 5 minutes � indocyanine green: P < .001.
BRIEF REPORTSVOL. 135, NO. 2 235

control phosphate-buffered solution or in the presence ofthe lowest trypan blue concentration (0.06%). In thehigher concentration of 0.15% trypan blue, autofluores-cence spots with a granular appearance were visible; thesewere more appreciable in the 0.3% concentration. Thespots were easily distinguishable from nucleae of dead cells(visible after, for example, incubating the cells in ahypotonic medium), which are more oval in shape, have alower fluorescence, and contain a bright nucleolus. There-fore, the measurements in the 540-nm spectrum weremanually counted to avoid false measurements.
After incubating the cells for 5 minutes in phosphatebuffered solution, an average ratio of living vs dead cells of14.7 � 1.85 was found (n � 12, Figure 1). When the cellswere exposed for 5 minutes to the 0.06% trypan blueconcentration, a ratio of 14.0 � 1.12 was measured (n �12, Figure 1). This ratio was no different than the controlexperiments (P � .73).
Experiments with the 0.15% concentration resulted in aratio of 13.9 � 1.19 (n � 12) and with the 0.3%concentration in 16.2 � 3.52 (n � 10). Measurementsat both concentrations were not statistically significantcompared with control experiments (0.15%: P � .71;0.3%: P � .72, respectively).
Although trypan blue markedly facilitates the removalof epiretinal membranes,2,3 toxic effects resulting fromcontact with vital tissues in the posterior segment of theeye need to be excluded before determining whether thisdye can be used safely in vitreoretinal surgery. It has beendemonstrated in an animal model that at a concentrationof 0.15% or less trypan blue may exert little toxic effects atthe neuroretinal level following a contact time of 1month.4
When trypan blue is used to stain epiretinal membranes,it is generally applied for 1 to 3 minutes in an air-filled eyecavity to enhance its physical contact with the retina.When retinal breaks are present, the dye can potentiallydiffuse into the subretinal space. Therefore, the cytotoxiceffect of trypan blue on retinal pigment epithelium cellsneeds to be excluded.
In our study, cultured human retinal pigment epitheliumcells were grown to subconfluency and exposed for 5minutes to a trypan blue concentration of various concen-trations to mimic direct contact between trypan blue andthe retinal pigment epithelium layer. Such concentrationsof trypan blue are almost never reached during surgerybecause of dilution in the intraocular fluid remnant. Evenat a concentration twice as high (0.3%) as the commer-cially available preparation of trypan blue and at a contacttime longer than is generally required during surgery, wefound no direct toxic effect of trypan blue on the retinalpigment epithelium cells in vitro.
This study illustrates that trypan blue is not cytotoxicwhen applied to retinal pigment epithelium cells in vitro.
ACKNOWLEDGMENTS
The authors thank Professor W. Van Driessche and MagdaBressinck for completing the scientific experiments.
REFERENCES
1. Melles GR, De Waard PW, Pameyer JH, Beekhuis WH.Trypan blue capsule staining to visualize the capsulorhexis incataract surgery. J Cataract Refract Surg 1999;25:7–9.
2. Feron EJ, Veckeneer M, Parys-Van Ginderdeuren R, VanLommel A, Melles GRJ, Stalmans P. Trypan blue staining ofepiretinal membranes in proliferative vitreoretinopathy. ArchOphthalmol 2002;120:141–144.
3. Stalmans P, Feron E, Parys-Van Ginderdeuren R, Van Lom-mel A, Melles GRJ, Veckeneer M. Double vital-staining usingtrypan blue and infracyanine green in macular pucker surgery.Arch Ophthalmol 2003, forthcoming.
4. Veckeneer M, van Overdam K, Monzer J, et al. Oculartoxicity study of trypan blue injected into the vitreous cavityof rabbit eyes. Graefes Arch Clin Exp Ophthalmol 2001;239:698–704.
5. Stalmans P, Van Aken EH, Veckeneer M, Feron EJ,Stalmans I. Toxic effect of indocyanine green on retinalpigment epithelium related to osmotic effects of the solvent.Am J Ophthalmol 2002;134.
Small-size Pediatric VitrectomyWide-angle Contact LensGholam A. Peyman, MD, Christina Canakis, MD,Charalampos Livir-Rallatos, MD, andPaul Whalen, BSME
PURPOSE: We describe a new wide-field vitrectomy con-tact lens specifically designed to facilitate pediatric vit-reoretinal surgery.DESIGN: Experimental study, instrument description.METHODS: A wide-field contact two-piece glass vitrec-tomy lens was designed with the largest diameter of 13.6mm and a contact diameter of 7.00 mm, sacrificing onlythe more tilt-sensitive parts of the optics in order toreduce its physical size.RESULTS: Laboratory measurements in a model eye dem-onstrated a 61-degree binocular field of view, a 94-degreestatic field of view, and a maximum 129-degree field ofview. Image magnification was 0.50�. No complicationswere linked to the use of this instrument, and the need toexchange for another lens was never encountered in 10cases. The two-piece glass construction enabled this lens
Accepted for publication Aug 29, 2002.From the Department of Ophthalmology (G.A.P., C.C., C.L.-R.),
Tulane University Health Sciences Center, New Orleans, Louisiana andOcular Instruments Inc. (P.W.), Bellevue, WA.
Dr. Gholam A. Peyman and Paul Whalen have a proprietary interestin the instrument.
Inquiries to Gholam A. Peyman, MD, Department of Ophthalmology,Tulane University Health Sciences Center, 1430 Tulane Avenue SL-69,New Orleans, LA 70112-2699; fax: (504) 988-1390; e-mail:[email protected]
AMERICAN JOURNAL OF OPHTHALMOLOGY236 FEBRUARY 2003







