SVMPharma Ltd, Landmark House
Station Road,Hook,Hampshire, UK,
RG27 9HA
+44(0)1256962220www.svmpharma.com
RWE TRIALS
BIG DATA
CUSTOM DATA COLLECTION
THERWESERIESProvidingthebackground,theresearchandtheinsights.
PART II:
COLLECTING REAL WORLD
EVIDENCE
RWE Series Part II: Collecting Real World Evidence
© 2015 SVMPharma Ltd. All rights reserved. 2
To continue turn to Page 5
To continue turn to Page 6
To continue turn to Page 3
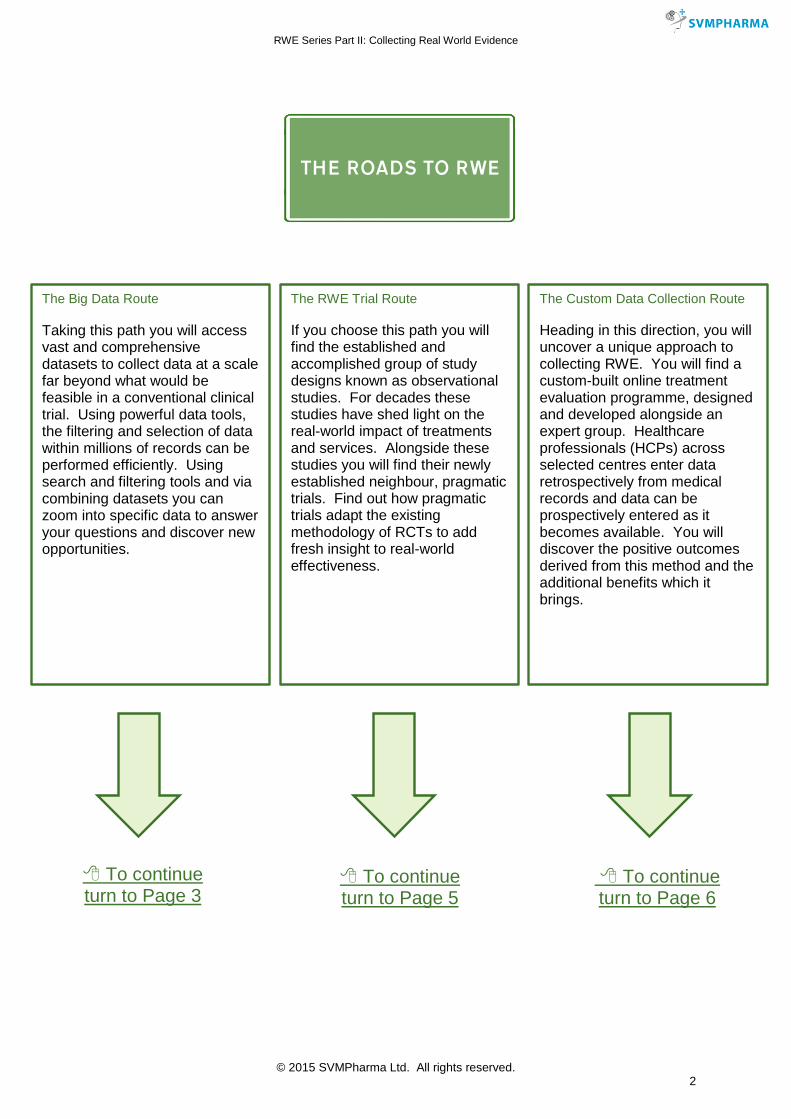
The Big Data Route
Taking this path you will access vast and comprehensive datasets to collect data at a scale far beyond what would be feasible in a conventional clinical trial. Using powerful data tools, the filtering and selection of data within millions of records can be performed efficiently. Using search and filtering tools and via combining datasets you can zoom into specific data to answer your questions and discover new opportunities.
The RWE Trial Route If you choose this path you will find the established and accomplished group of study designs known as observational studies. For decades these studies have shed light on the real-world impact of treatments and services. Alongside these studies you will find their newly established neighbour, pragmatic trials. Find out how pragmatic trials adapt the existing methodology of RCTs to add fresh insight to real-world effectiveness.
The Custom Data Collection Route Heading in this direction, you will uncover a unique approach to collecting RWE. You will find a custom-built online treatment evaluation programme, designed and developed alongside an expert group. Healthcare professionals (HCPs) across selected centres enter data retrospectively from medical records and data can be prospectively entered as it becomes available. You will discover the positive outcomes derived from this method and the additional benefits which it brings.
THE ROADS TO RWE
RWE Series Part II: Collecting Real World Evidence
© 2015 SVMPharma Ltd. All rights reserved. 3
1) The Big Data Route
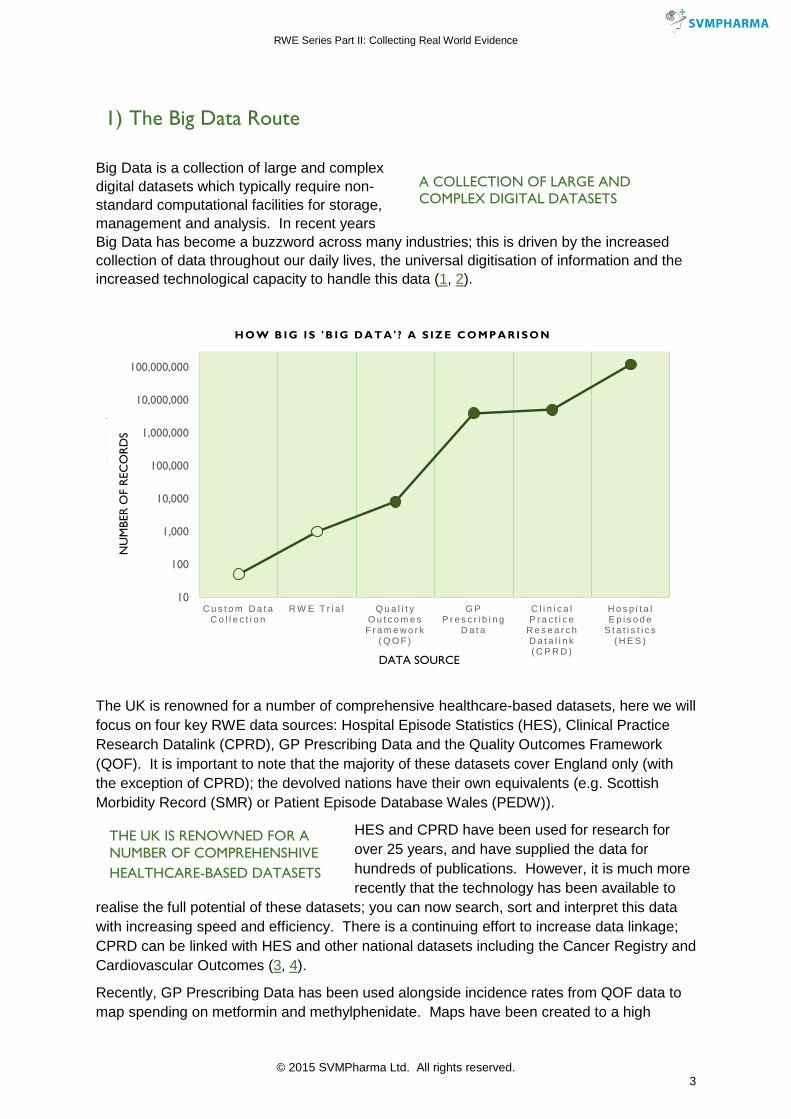
Big Data is a collection of large and complex digital datasets which typically require non-standard computational facilities for storage, management and analysis. In recent years Big Data has become a buzzword across many industries; this is driven by the increased collection of data throughout our daily lives, the universal digitisation of information and the increased technological capacity to handle this data (1, 2).
The UK is renowned for a number of comprehensive healthcare-based datasets, here we will focus on four key RWE data sources: Hospital Episode Statistics (HES), Clinical Practice Research Datalink (CPRD), GP Prescribing Data and the Quality Outcomes Framework (QOF). It is important to note that the majority of these datasets cover England only (with the exception of CPRD); the devolved nations have their own equivalents (e.g. Scottish Morbidity Record (SMR) or Patient Episode Database Wales (PEDW)).
HES and CPRD have been used for research for over 25 years, and have supplied the data for hundreds of publications. However, it is much more recently that the technology has been available to
realise the full potential of these datasets; you can now search, sort and interpret this data with increasing speed and efficiency. There is a continuing effort to increase data linkage; CPRD can be linked with HES and other national datasets including the Cancer Registry and Cardiovascular Outcomes (3, 4).
Recently, GP Prescribing Data has been used alongside incidence rates from QOF data to map spending on metformin and methylphenidate. Maps have been created to a high
THE UK IS RENOWNED FOR A
NUMBER OF COMPREHENSIVE
LARGE DATASETS
10
100
1,000
10,000
100,000
1,000,000
10,000,000
100,000,000
C u s t o m D a t a C o l l e c t i o n
R W E T r i a l Q u a l i t y O u t c o m e s
F r a m e w o r k ( Q O F )
G P P r e s c r i b i n g
D a t a
C l i n i c a l P r a c t i c e
R e s e a r c h D a t a l i n k ( C P R D )
H o s p i t a l E p i s o d e
S t a t i s t i c s ( H E S )
NU
MB
ER
OF R
EC
OR
DS
DATA SOURCE
H O W B I G I S ' B I G D A T A ' ? A S I Z E C O M P A R I S O N
A COLLECTION OF LARGE AND
COMPLEX DIGITAL DATASETS
THE UK IS RENOWNED FOR A
NUMBER OF COMPREHENSHIVE
HEALTHCARE-BASED DATASETS
RWE Series Part II: Collecting Real World Evidence
© 2015 SVMPharma Ltd. All rights reserved. 4
spatial resolution and combined with demographic and geographic data. This data can be analysed to distinguish between chance fluctuations and genuine differences in prescribing rates, and users can accurately identify where action is required (5).
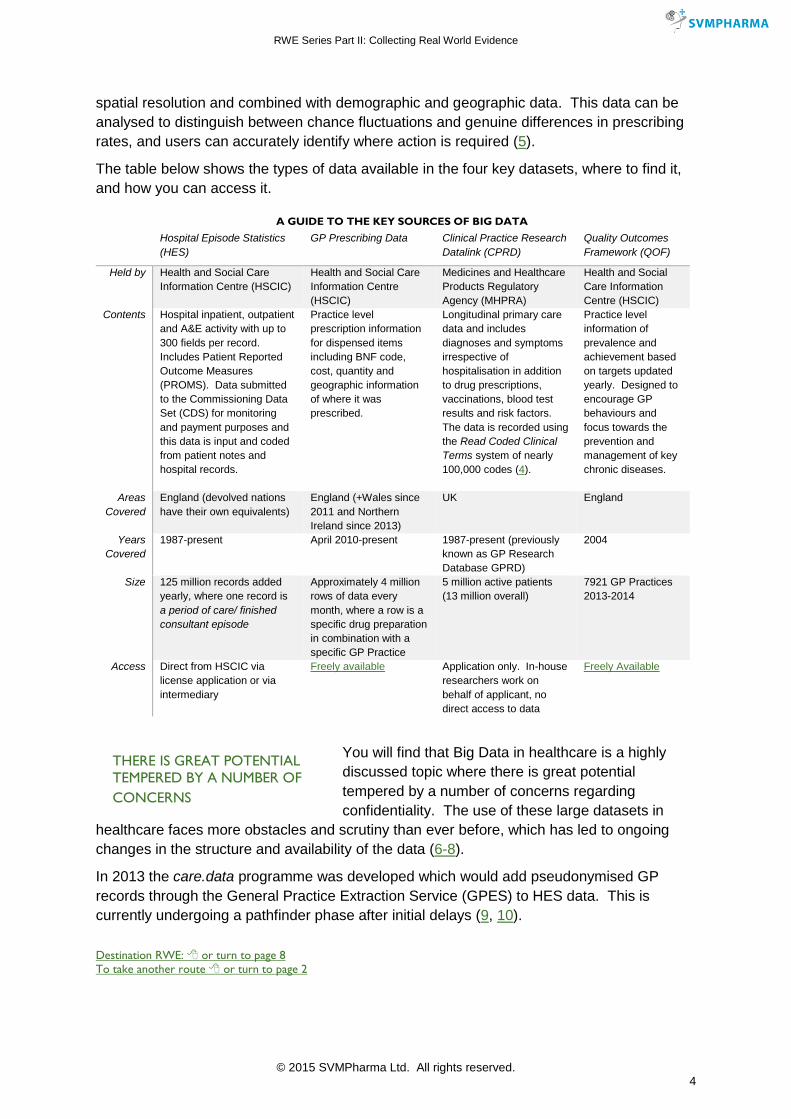
The table below shows the types of data available in the four key datasets, where to find it, and how you can access it.
Hospital Episode Statistics (HES)
GP Prescribing Data Clinical Practice Research Datalink (CPRD)
Quality Outcomes Framework (QOF)
Held by Health and Social Care Information Centre (HSCIC)
Health and Social Care Information Centre (HSCIC)
Medicines and Healthcare Products Regulatory Agency (MHPRA)
Health and Social Care Information Centre (HSCIC)
Contents Hospital inpatient, outpatient and A&E activity with up to 300 fields per record. Includes Patient Reported Outcome Measures (PROMS). Data submitted to the Commissioning Data Set (CDS) for monitoring and payment purposes and this data is input and coded from patient notes and hospital records.
Practice level prescription information for dispensed items including BNF code, cost, quantity and geographic information of where it was prescribed.
Longitudinal primary care data and includes diagnoses and symptoms irrespective of hospitalisation in addition to drug prescriptions, vaccinations, blood test results and risk factors. The data is recorded using the Read Coded Clinical Terms system of nearly 100,000 codes (4).
Practice level information of prevalence and achievement based on targets updated yearly. Designed to encourage GP behaviours and focus towards the prevention and management of key chronic diseases.
Areas Covered
England (devolved nations have their own equivalents)
England (+Wales since 2011 and Northern Ireland since 2013)
UK England
Years Covered
1987-present April 2010-present 1987-present (previously known as GP Research Database GPRD)
2004
Size 125 million records added yearly, where one record is a period of care/ finished consultant episode
Approximately 4 million rows of data every month, where a row is a specific drug preparation in combination with a specific GP Practice
5 million active patients (13 million overall)
7921 GP Practices 2013-2014
Access Direct from HSCIC via license application or via intermediary
Freely available Application only. In-house researchers work on behalf of applicant, no direct access to data
Freely Available
You will find that Big Data in healthcare is a highly discussed topic where there is great potential tempered by a number of concerns regarding confidentiality. The use of these large datasets in
healthcare faces more obstacles and scrutiny than ever before, which has led to ongoing changes in the structure and availability of the data (6-8).
In 2013 the care.data programme was developed which would add pseudonymised GP records through the General Practice Extraction Service (GPES) to HES data. This is currently undergoing a pathfinder phase after initial delays (9, 10).
Destination RWE: or turn to page 8
To take another route or turn to page 2
A GUIDE TO THE KEY SOURCES OF BIG DATA
THERE IS GREAT POTENTIAL
TEMPERED BY A NUMBER OF
CONCERNS
RWE Series Part II: Collecting Real World Evidence
© 2015 SVMPharma Ltd. All rights reserved. 5
2) The RWE Trial Route
Designing and conducting a trial is an important and robust way of collecting RWE with a significant amount of flexibility. RWE trials can be divided into two main groups, observational studies and pragmatic trials. Both types use existing or adapted study designs but shift the emphasis towards external validity in order to gain better understanding of real world practice.
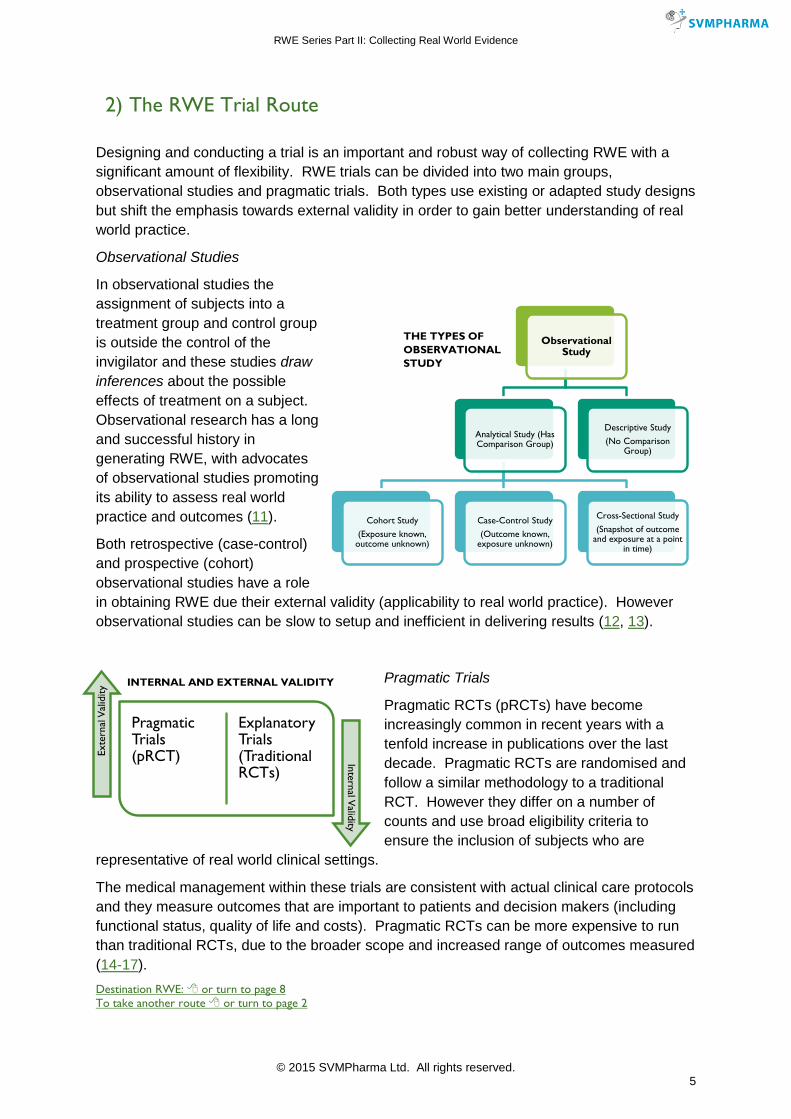
Observational Studies
In observational studies the assignment of subjects into a treatment group and control group is outside the control of the invigilator and these studies draw inferences about the possible effects of treatment on a subject. Observational research has a long and successful history in generating RWE, with advocates of observational studies promoting its ability to assess real world practice and outcomes (11).
Both retrospective (case-control) and prospective (cohort) observational studies have a role in obtaining RWE due their external validity (applicability to real world practice). However observational studies can be slow to setup and inefficient in delivering results (12, 13).
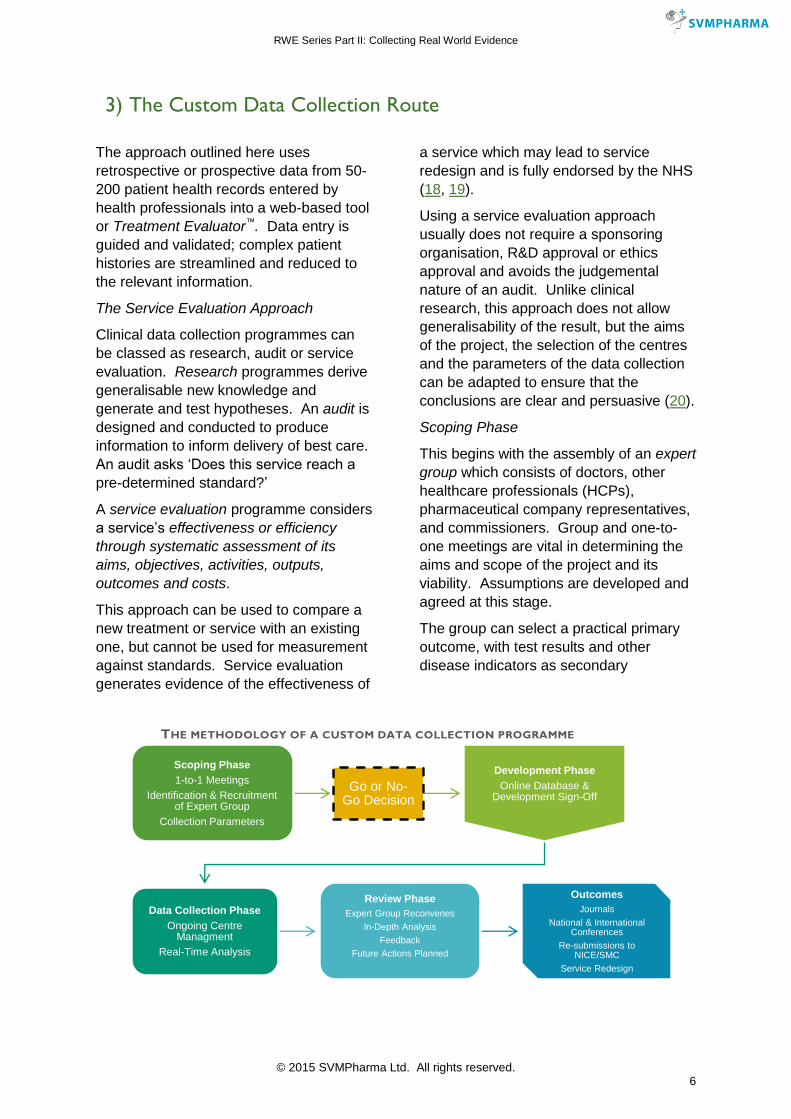
Pragmatic Trials
Pragmatic RCTs (pRCTs) have become increasingly common in recent years with a tenfold increase in publications over the last decade. Pragmatic RCTs are randomised and follow a similar methodology to a traditional RCT. However they differ on a number of counts and use broad eligibility criteria to ensure the inclusion of subjects who are
representative of real world clinical settings.
The medical management within these trials are consistent with actual clinical care protocols and they measure outcomes that are important to patients and decision makers (including functional status, quality of life and costs). Pragmatic RCTs can be more expensive to run than traditional RCTs, due to the broader scope and increased range of outcomes measured (14-17).
Destination RWE: or turn to page 8
To take another route or turn to page 2
Observational Study
Analytical Study (Has Comparison Group)
Cohort Study
(Exposure known, outcome unknown)
Case-Control Study
(Outcome known, exposure unknown)
Cross-Sectional Study
(Snapshot of outcome and exposure at a point
in time)
Descriptive Study
(No Comparison Group)
THE TYPES OF
OBSERVATIONAL
STUDY
Pragmatic Trials (pRCT)
Explanatory Trials (Traditional RCTs)
Exte
rnal
Val
idity
Inte
rnal V
alidity
INTERNAL AND EXTERNAL VALIDITY
RWE Series Part II: Collecting Real World Evidence
© 2015 SVMPharma Ltd. All rights reserved. 6
3) The Custom Data Collection Route
The approach outlined here uses retrospective or prospective data from 50-200 patient health records entered by health professionals into a web-based tool or Treatment Evaluator™. Data entry is guided and validated; complex patient histories are streamlined and reduced to the relevant information.
The Service Evaluation Approach
Clinical data collection programmes can be classed as research, audit or service evaluation. Research programmes derive generalisable new knowledge and generate and test hypotheses. An audit is designed and conducted to produce information to inform delivery of best care. An audit asks ‘Does this service reach a
pre-determined standard?’
A service evaluation programme considers a service’s effectiveness or efficiency through systematic assessment of its aims, objectives, activities, outputs, outcomes and costs.
This approach can be used to compare a new treatment or service with an existing one, but cannot be used for measurement against standards. Service evaluation generates evidence of the effectiveness of
a service which may lead to service redesign and is fully endorsed by the NHS (18, 19).
Using a service evaluation approach usually does not require a sponsoring organisation, R&D approval or ethics approval and avoids the judgemental nature of an audit. Unlike clinical research, this approach does not allow generalisability of the result, but the aims of the project, the selection of the centres and the parameters of the data collection can be adapted to ensure that the conclusions are clear and persuasive (20).
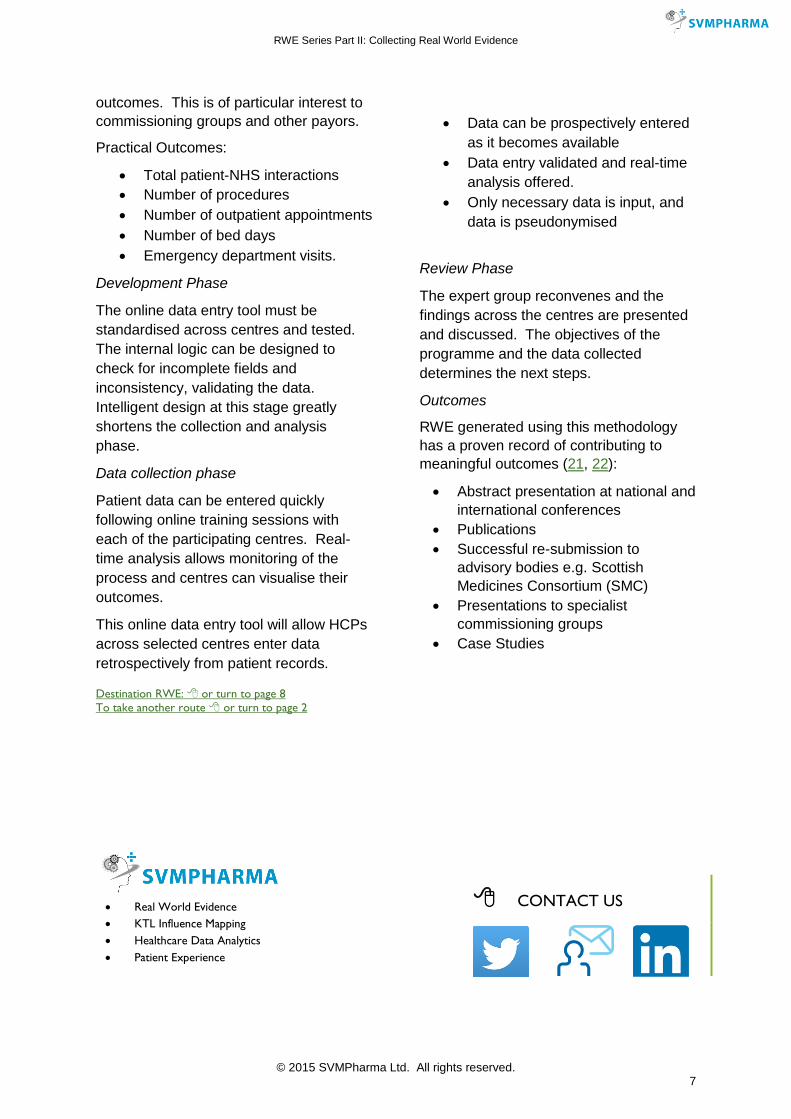
Scoping Phase
This begins with the assembly of an expert group which consists of doctors, other healthcare professionals (HCPs), pharmaceutical company representatives, and commissioners. Group and one-to-one meetings are vital in determining the aims and scope of the project and its viability. Assumptions are developed and agreed at this stage.
The group can select a practical primary outcome, with test results and other disease indicators as secondary
Scoping Phase
1-to-1 Meetings
Identification & Recruitment of Expert Group
Collection Parameters
Go or No-Go Decision
Development Phase
Online Database & Development Sign-Off
Data Collection Phase
Ongoing Centre Managment
Real-Time Analysis
Review PhaseExpert Group Reconvenes
In-Depth Analysis
Feedback
Future Actions Planned
OutcomesJournals
National & International Conferences
Re-submissions to NICE/SMC
Service Redesign
THE METHODOLOGY OF A CUSTOM DATA COLLECTION PROGRAMME
RWE Series Part II: Collecting Real World Evidence
© 2015 SVMPharma Ltd. All rights reserved. 7
outcomes. This is of particular interest to commissioning groups and other payors.
Practical Outcomes:
Total patient-NHS interactions Number of procedures Number of outpatient appointments Number of bed days Emergency department visits.
Development Phase
The online data entry tool must be standardised across centres and tested. The internal logic can be designed to check for incomplete fields and inconsistency, validating the data. Intelligent design at this stage greatly shortens the collection and analysis phase.
Data collection phase
Patient data can be entered quickly following online training sessions with each of the participating centres. Real-time analysis allows monitoring of the process and centres can visualise their outcomes.
This online data entry tool will allow HCPs across selected centres enter data retrospectively from patient records.
Data can be prospectively entered
as it becomes available Data entry validated and real-time
analysis offered. Only necessary data is input, and
data is pseudonymised
Review Phase
The expert group reconvenes and the findings across the centres are presented and discussed. The objectives of the programme and the data collected determines the next steps.
Outcomes
RWE generated using this methodology has a proven record of contributing to meaningful outcomes (21, 22):
Abstract presentation at national and international conferences
Publications Successful re-submission to
advisory bodies e.g. Scottish Medicines Consortium (SMC)
Presentations to specialist commissioning groups
Case Studies
Destination RWE: or turn to page 8
To take another route or turn to page 2
CONTACT US
Real World Evidence
KTL Influence Mapping
Healthcare Data Analytics
Patient Experience
RWE Series Part II: Collecting Real World Evidence
© 2015 SVMPharma Ltd. All rights reserved. 8
Destination: RWE
Each of the three routes leads to RWE, providing data which can drive clinical outcomes and enhance the value of a product. However you will see that each route has strengths and weaknesses, did you make the right choice?
Big Data is important in identifying trends and relationships and inspiring new directions for marketing and growth. The scope and volume of data can be persuasive and powerful, however
accessibility and completeness varies.
Pragmatic RCTs and prospective observational studies require a considerable investment in time and money but can produce robust and powerful RWE.
Custom data collection, via the approach outlined, allows data to be collected, analysed and presented within a period of several months. This is invaluable when faced with an approaching deadline, for instance, submissions or re-submissions to NICE, SMC or specialist commissioners. This data can differentiate a product in a competitive marketplace and the data collection process encourages engagement with the centres and key prescribers.
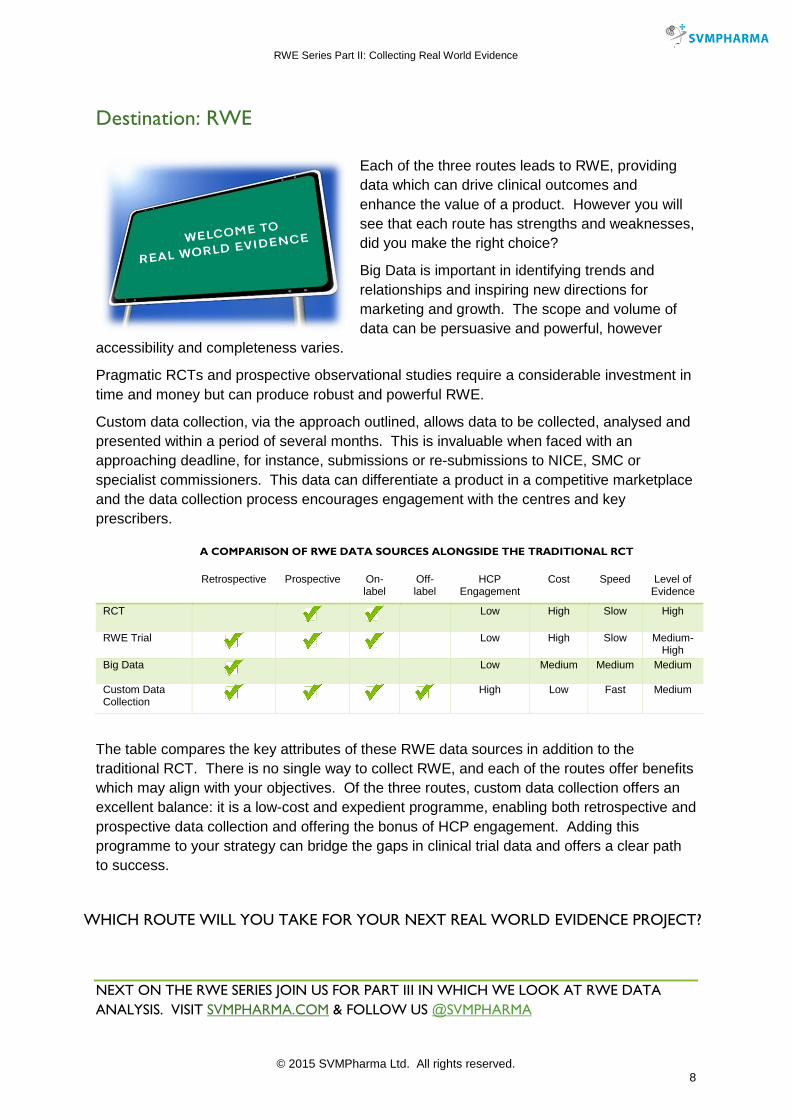
The table compares the key attributes of these RWE data sources in addition to the traditional RCT. There is no single way to collect RWE, and each of the routes offer benefits which may align with your objectives. Of the three routes, custom data collection offers an excellent balance: it is a low-cost and expedient programme, enabling both retrospective and prospective data collection and offering the bonus of HCP engagement. Adding this programme to your strategy can bridge the gaps in clinical trial data and offers a clear path to success.
NEXT ON THE RWE SERIES JOIN US FOR PART III IN WHICH WE LOOK AT RWE DATA
ANALYSIS. VISIT SVMPHARMA.COM & FOLLOW US @SVMPHARMA
Retrospective Prospective On-label
Off-label
HCP Engagement
Cost Speed Level of Evidence
RCT
Low High Slow High
RWE Trial
Low High Slow Medium-High
Big Data
Low Medium Medium Medium
Custom Data Collection
High Low Fast Medium
A COMPARISON OF RWE DATA SOURCES ALONGSIDE THE TRADITIONAL RCT
WHICH ROUTE WILL YOU TAKE FOR YOUR NEXT REAL WORLD EVIDENCE PROJECT?
RWE Series Part II: Collecting Real World Evidence
© 2015 SVMPharma Ltd. All rights reserved. 9
1. Murdoch TB, Detsky AS. THe inevitable application of big data to health care. JAMA. 2013;309(13):1351-2.
2. Bollier D, Firestone CM. The promise and peril of big data: Aspen Institute, Communications and Society Program Washington, DC, USA; 2010.
3. Williams T, van Staa T, Puri S, Eaton S. Recent advances in the utility and use of the General Practice Research Database as an example of a UK Primary Care Data resource. Therapeutic Advances in Drug Safety. 2012;3(2):89-99.
4. Denaxas SC, George J, Herrett E, Shah AD, Kalra D, Hingorani AD, et al. Data Resource Profile: Cardiovascular disease research using linked bespoke studies and electronic health records (CALIBER). International Journal of Epidemiology. 2012.
5. Rowlingson B, Lawson E, Taylor B, Diggle PJ. Mapping English GP prescribing data: a tool for monitoring health-service inequalities. BMJ Open. 2013;3(1).
6. Keen J, Calinescu R, Paige R, Rooksby J, editors. Big Health Data: Institutional and Technological Challenges. paper at IPP2012 conference ‘Big Data, Big Challenges’, Oxford, Sept; 2012.
7. Schultz T. Turning healthcare challenges into big data opportunities: A use-case review across the pharmaceutical development lifecycle. Bulletin of the American Society for Information Science and Technology. 2013;39(5):34-40.
8. Pope C, Halford S, Tinati R, Weal M. What's the big fuss about 'big data'? Journal of health services research & policy. 2014;19(2):67-8.
9. Square T, Lane B. Care. data. 2013.
10. Mitchell C, Moraia LB, Kaye J. Health database: Restore public trust in care. data project. Nature. 2014;508(7497):458-.
11. Benson K, Hartz AJ. A Comparison of Observational Studies and Randomized, Controlled Trials. New England Journal of Medicine. 2000;342(25):1878-86.
12. Black N. Why we need observational studies to evaluate the effectiveness of health care1996 1996-05-11 07:00:00. 1215-8 p.
13. Silverman SL. From Randomized Controlled Trials to Observational Studies. The American Journal of Medicine. 2009;122(2):114-20.
14. Brass E. The gap between clinical trials and clinical practice: the use of pragmatic clinical trials to inform regulatory decision making. Clinical pharmacology and therapeutics. 2010;87(3):351-5.
15. Patsopoulos NA. A pragmatic view on pragmatic trials. Dialogues in Clinical Neuroscience. 2011;13(2):217-24.
16. Roland M, Torgerson DJ. Understanding controlled trials: What are pragmatic trials? BMJ (Clinical research ed). 1998;316(7127):285.
17. New JP, Bakerly ND, Leather D, Woodcock A. Obtaining real-world evidence: the Salford Lung Study. Thorax. 2014.
18. University_Hospitals_Bristol. Operational Guidance 2007. Available from: http://www.uhbristol.nhs.uk/media/1689453/agreed_definitions_of_rd_ca_se_v4_oct_07_pdf.pdf.
19. National_Research_Ethics_Service. Defining Research 2010. Available from: http://www.uhbristol.nhs.uk/media/1572809/defining_research_leaflet_1_.pdf.
20. Gerrish K, Mawson S. Research, audit, practice development and service evaluation: Implications for research and clinical governance. Practice Development in Health Care. 2005;4(1):33-9.
21. Plant BJ, Downey D, Eustace JA, Gunaratnam C, Haworth C, Jones A, et al. WS7.4 Inhaled aztreonam lysine (Cayston) therapy significantly improves lung function, weight, hospitalisations and excerbation rates prospectively – an Irish and UK real world experience. Journal of Cystic Fibrosis.13:S15.
22. Scottish_Medicines_Consortium. Re-submission of aztreonam lysine (Cayston)2015 12 January 2015. Available from: http://www.scottishmedicines.org.uk/SMC_Advice/Advice/753_12_aztreonam_Cayston/aztreonam_lysine_Cayston_RESUBMISSION.








