
Spinal InfectionsHimanshu Sharma
Spinal InfectionsObjectives
• Epidemiology
• Pathology
• Clinical features
• Management
• Prognosis
Spinal InfectionsEpidemiology
• 2 - 4% all cases of “osteomyelitis”
• Rare: 1 in 250,000/yr but rising incidence
• Post-op discitis = 2-3%
• Pre-antibiotic mortality = 25-70%
• Delayed diagnosis common (50%+ > 3/12)

Spinal InfectionsLevels
Spondylodiscitis / facet disease
• Lumbar (59%)
• Thoracic (33%)
• Cervical (8%)
Epidural abscess (in 7%)
• Cervical (6-18%) anterior
• Thoracic
• Lumbar
Spinal InfectionsRisk Factors
• Peak incidence 7th decade
• Concurrent illness/infection
Diabetes Obesity
Immunosuppressed Malnutrition
Steroid therapy Irradiation
UTI
• Invasive procedures/ trauma
• Smoking
Spinal InfectionsPathology (1)
• Organisms
S aureus 30 -50% cases
Gram-negatives – UTI, Chest, Skin ulcers
Opportunistic in immune paresis
IVDA
• Route of spread
Haematogenous
Direct extension
Post-operative
Spinal InfectionsPathology (2)
• Vertebral metaphyses (end plate region)
= end-arteriole blood supply (filter)
Septic emboli
• Direct spread from implantation
Secondary spread to discs, paraspinal
tissues and spaces

Spinal InfectionsClinical Features
• Pain and focal tenderness 90%
• Fever 61%
• Root symptoms/signs 60%
• Abnormal neurology 20%
Also: deformity, muscle spasms, meningism, sinus,
and unexplained septicaemia

Investigations
• FBC• ESR• CRP• Blood & Urine cultures• Nutritional status • Biopsy
Spinal InfectionsDiagnosis
• Lab tests
White cell count 40-50%
ESR / CRP 80-90%
Positive Blood Culture 20-25%
• Imaging
• Biopsy
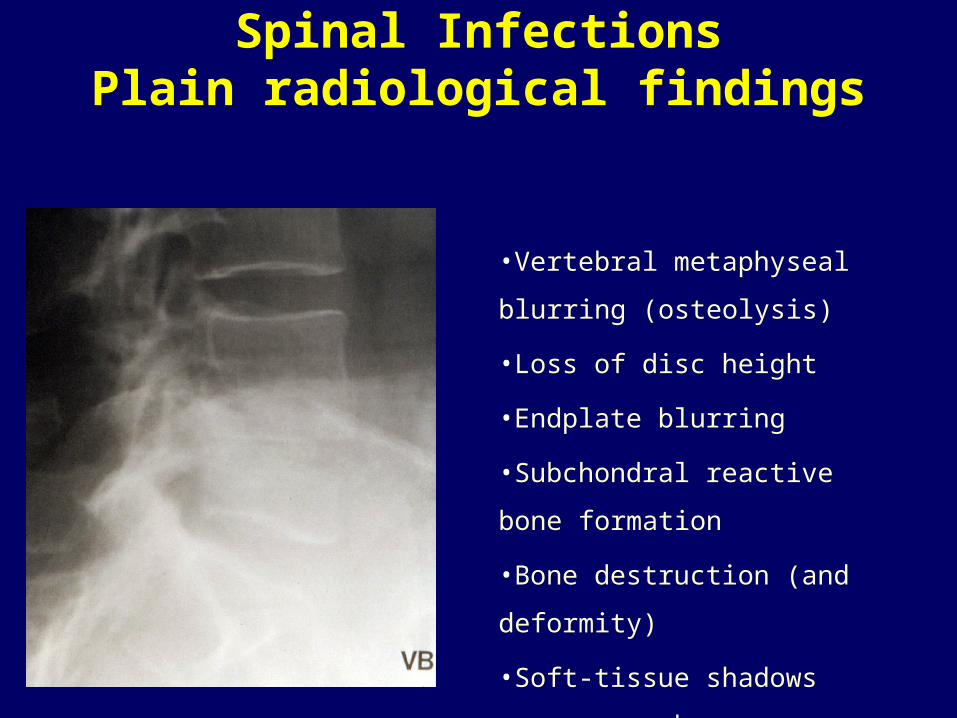
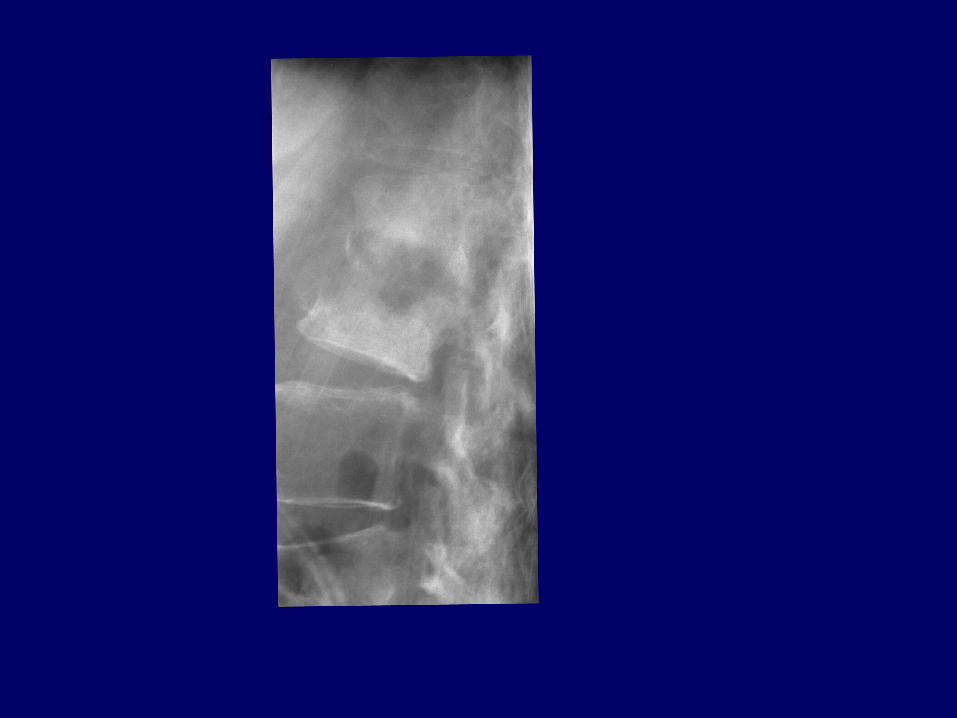
Spinal InfectionsPlain radiological findings
•Vertebral metaphyseal blurring
(osteolysis)
•Loss of disc height
•Endplate blurring
•Subchondral reactive bone
formation
•Bone destruction (and deformity)
•Soft-tissue shadows e.g.psoas
abscess

Pyogenicdiscitis/osteomyelitis
Bad disc = Good news
Spinal InfectionsImaging Studies - Isotopes
• Detect earlier than plain films
• High sensitivity / specificity
e.g. gallium + Tc = 95% accurate
• Little structural information
• False negatives in neutropenics
(gallium)
• False negatives in bone infarction (Tc)
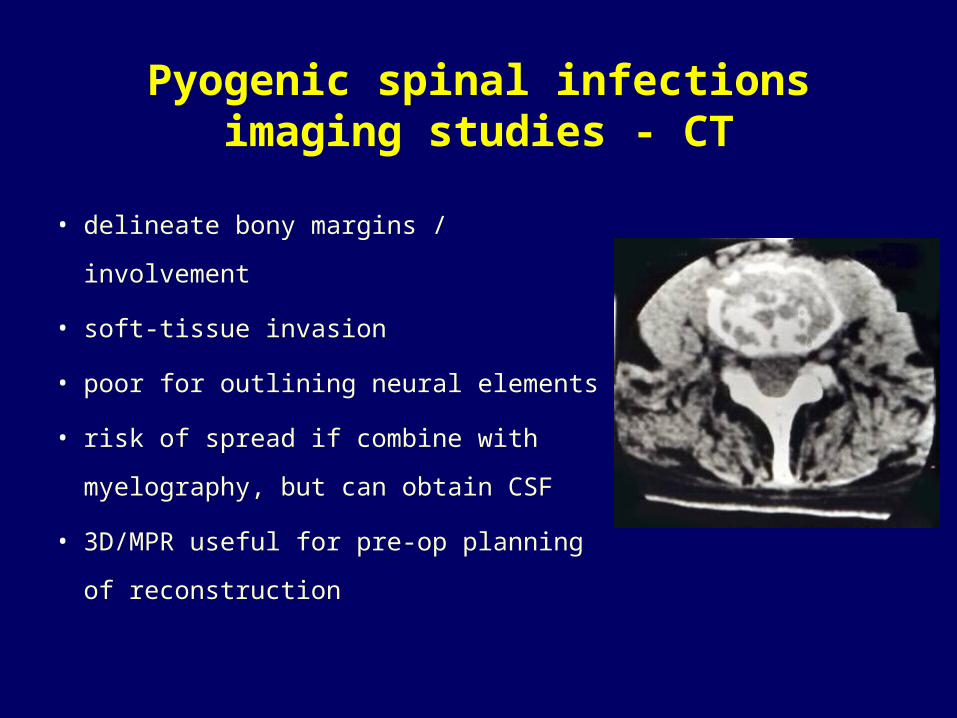
Pyogenic spinal infectionsimaging studies - CT
• delineate bony margins / involvement
• soft-tissue invasion
• poor for outlining neural elements
• risk of spread if combine with myelography,
but can obtain CSF
• 3D/MPR useful for pre-op planning of
reconstruction
Spinal InfectionsDifferential Diagnosis
• Granulomatous disease
• Metastases/Myeloma
• Degenerative disease
• Osteoporosis
• Local Scheuermann’s
• Spondyloarthropathies
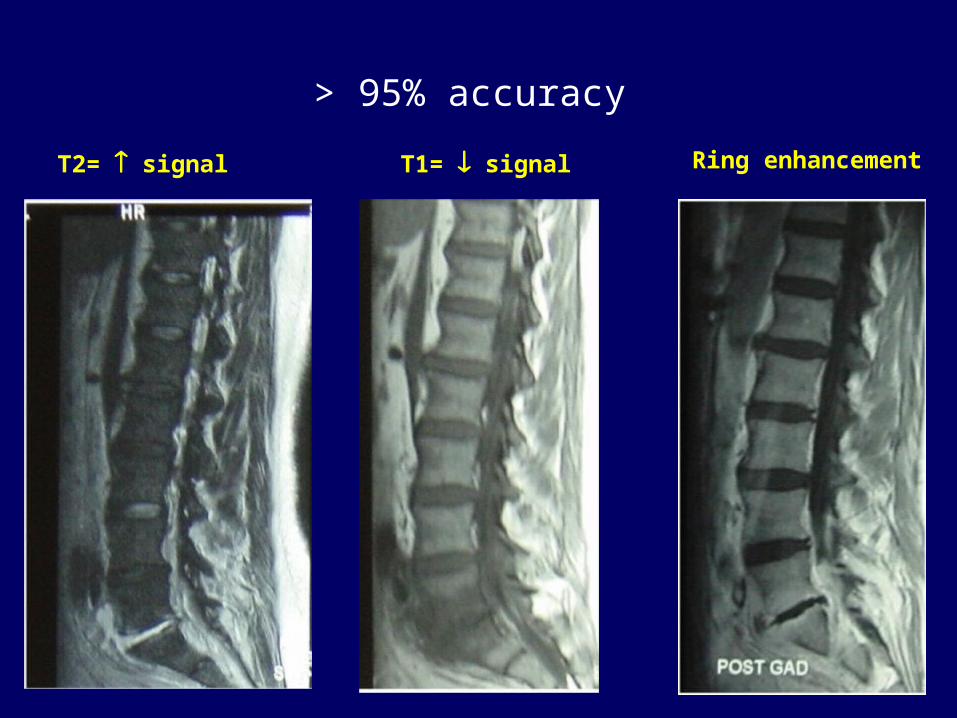
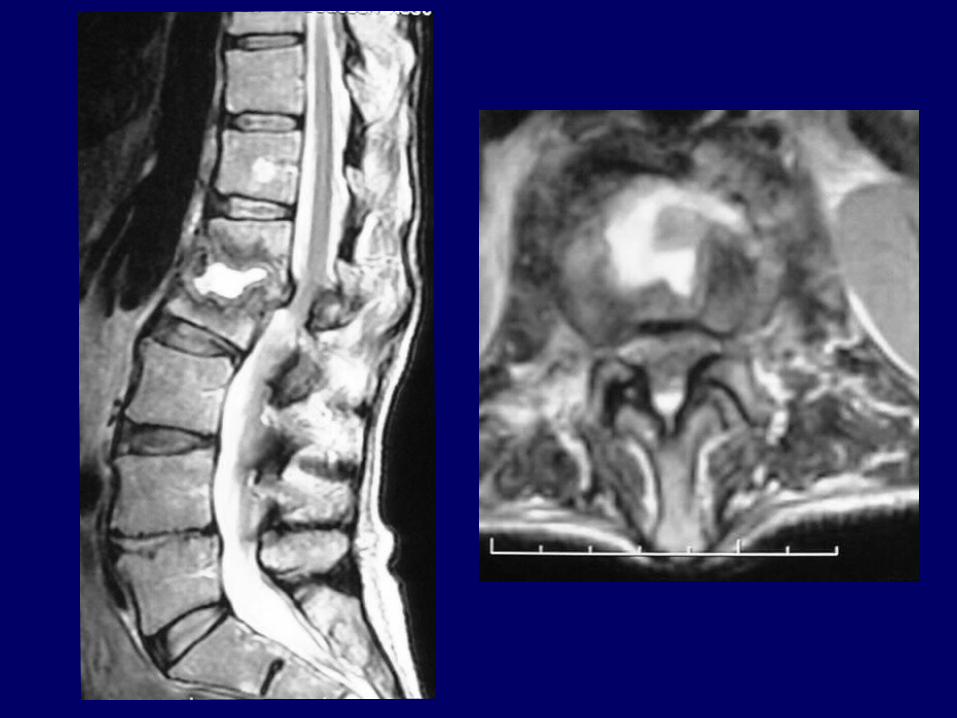
T1= signalT2= signal Ring enhancement
> 95% accuracy
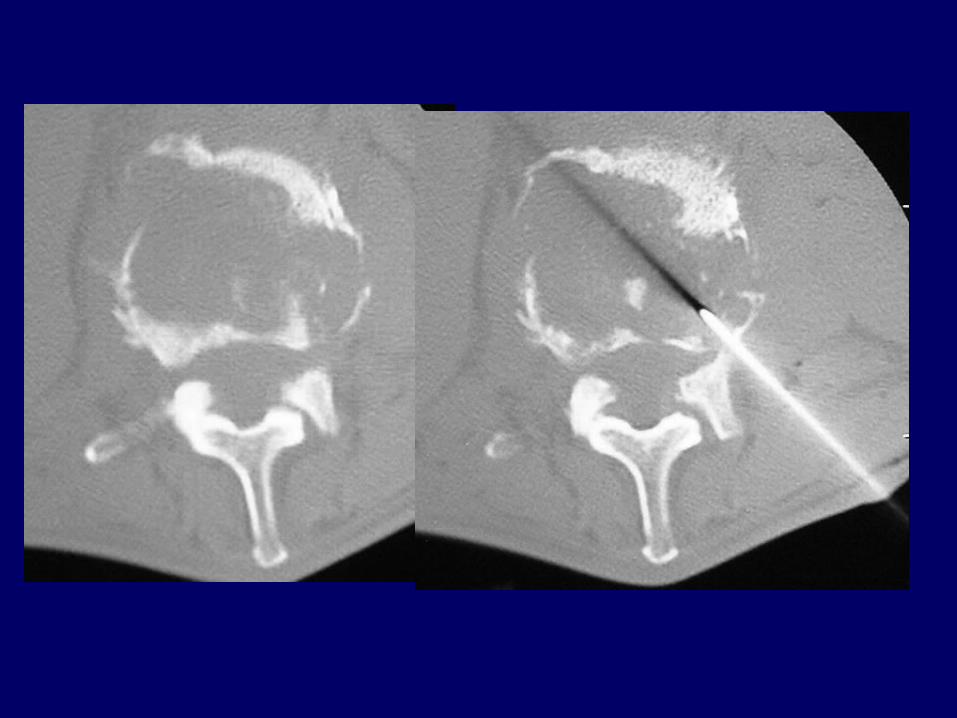
Spinal InfectionsBiopsy
Biopsy (for identification of the causative organism)
• Closed needle biopsy (guided)
– 68 - 86% accuracy (false negative 30%)
• Open biopsy
– > 80% accurate (false negative 14%)
• Special lab techniques (DNA PCR, etc)
Biopsy principles
• Biopsy material should be sent to microbiology for gram stain & acid-fast stain, aerobic, anaerobic, fungal and mycobacterial cultures and for histopathological examination.

Spinal InfectionsTreatment Goals
• Establish diagnosis
• Clear infection and prevent recurrence
• Pain relief
• Protect / restore neurological function
• Maintain / restore spine stability
Changed Battlefield
• Territory
– Patients
• Weapons
– Antibiotics
–Surgery
• Enemy
– Microbiology
Territory - changed
• Patient• Population Greying• Type 2 DM• Cancer• Steroids• HIV• Drug Abuse
• Iatrogenic Immunosuppression
Transplants
Dialysis
Enemy - changed
• More Resistant Strains of Bacteria• Hospital Acquired Infection• More previously unsuspected causes

Weapons -
• Antimicrobials
• Type and Scope of Surgery
Why is it important?
• Consequence of Inappropriate Management
• Multiple Surgery• Pain • Paralysis• Death• Financial Cost
• Causes of Inappropriate Management
• Lack of awareness• Empirical Antibiotics• Inappropriate /Inadequate
Surgery
Spinal InfectionsTreatment (1)
Antibiotics
– sensitivities
– adequate dose (iv then oral)
– ensure MBC reached
– adequate duration (> 6 weeks)
– monitor response (clinical/ indices/ imaging)
– toxicity profile and monitoring
Spinal InfectionsTreatment (2)
Immobilisation
– bed rest
– moulded orthoses (low thoracic / lumbar)
– halo-vest or orthosis (cervical / high thoracic)
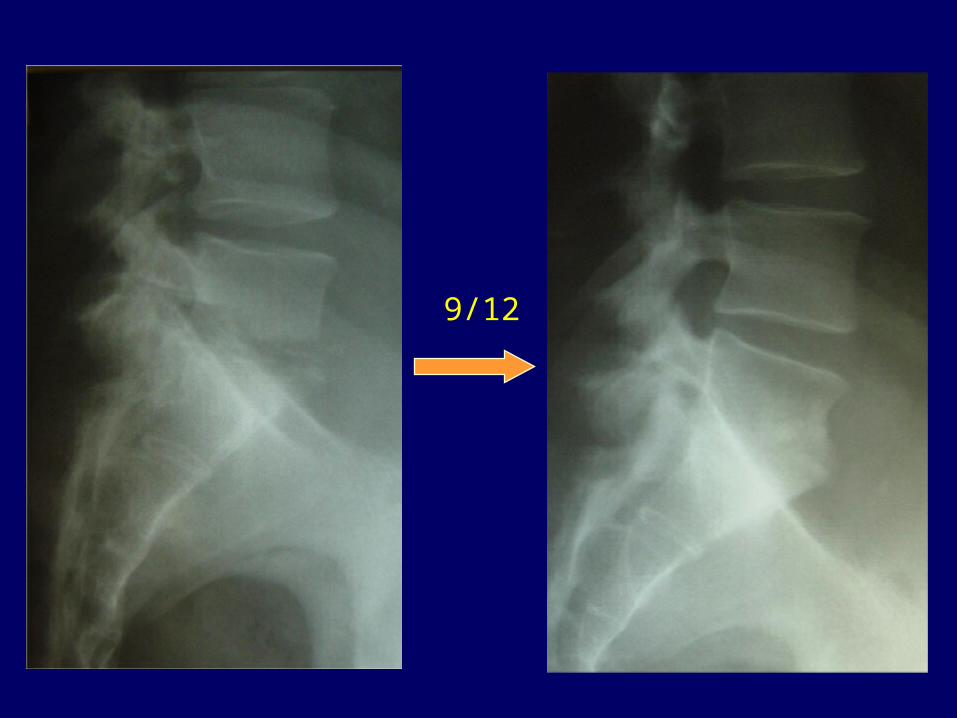
9/12

Pyogenic spinal infections







