Quel impact de l’hépatopathie sous-jacente
sur l’insuffisance hépatique post-operatoire
Andrea Laurenzi - Daniel Cherqui
Hépatopathie
• Cirrhose
• Chimiothérapie
• Cholestase
Hépatopathie
• Cirrhose
• Chimiothérapie
• Cholestase

Operative risk and underlying liver1023 liver resections (1990-2008)
22
7,9
3,71,5
27
8,8 8,5
3,7
0
5
10
15
20
25
30
Transfusions <2000 Transfusions >2000 Mortality <2000 Mortality >2000
%Cirrhosis
No Liver Disease
Cherqui unpublished data

0 Cx Gr 1 Gr 2 Gr 3A Gr 3B Gr 4 Gr 5
MAJOR Rx 6 1 8 4 2 2 0
MINOR Rx 22 3 8 1 3 0 0
Liver Resection for HCC Paul Brousse Hospital 2013 - 2015
95 Patients 28 Laparoscopic
Cirrhosis 57 Fibrosis 15
NASH 14 Normal 9
Mortality 2Morbidity 40%
• Preoperative: patient selection– Liver functional reserve– Planning by imaging– Portal vein embolization
• Intraoperative– Reduction of hemorrhage– Parenchymal preservation– Coelioscopie
• Postoperative– Postop care– Follow up
Progress in Surgery for HCC
Cirrhose
• Sélection
• Management

Cirrhose
• Sélection
• Traitement
Sélection
• CHILD score• MELD score• Vert d’Indocyanine• HTP (gradient P-S, plaquettes….)• Fibrose (biopsie, fibroscan)• Volumetrie
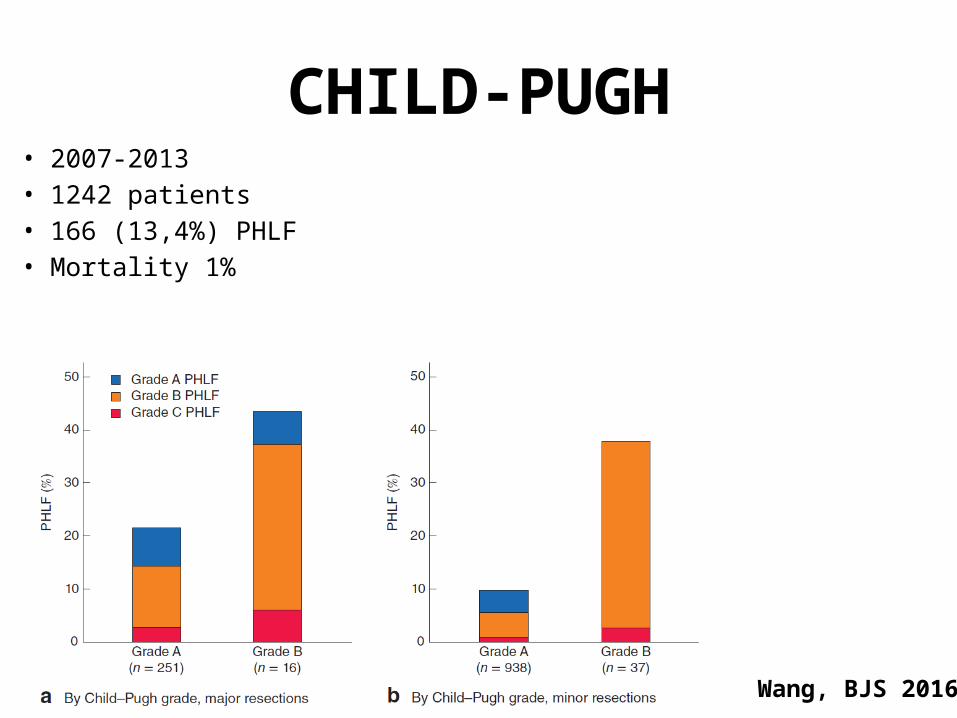
CHILD-PUGH• 2007-2013• 1242 patients• 166 (13,4%) PHLF• Mortality 1%
Wang, BJS 2016
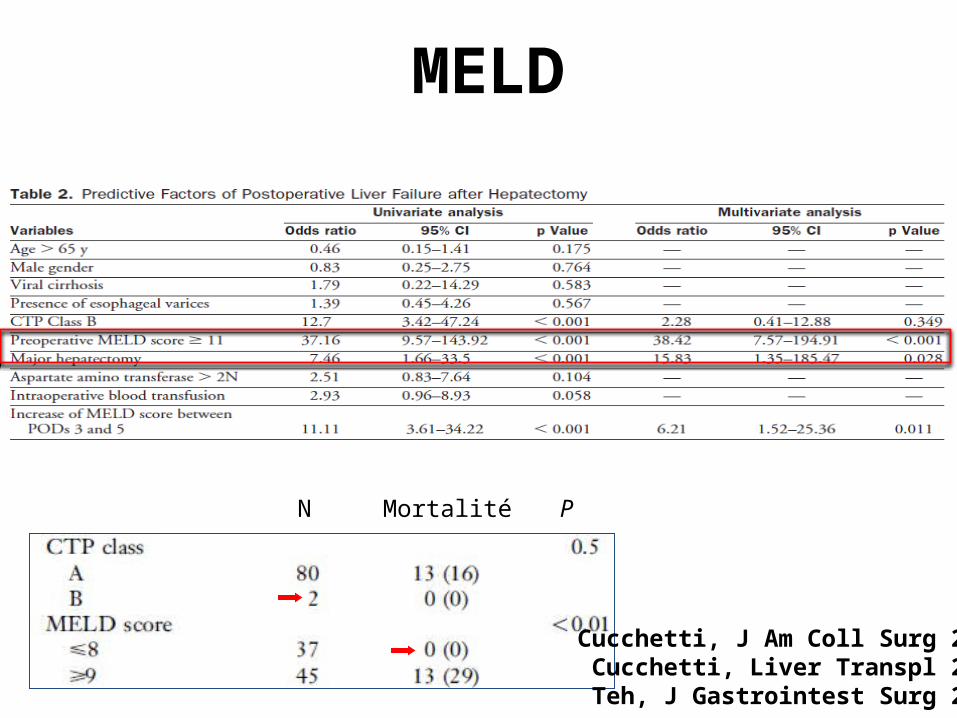
MELD
N Mortalité P
Cucchetti, J Am Coll Surg 2006Cucchetti, Liver Transpl 2006Teh, J Gastrointest Surg 2005

MELD
Cucchetti, Liver Transpl 2006
IHC postop
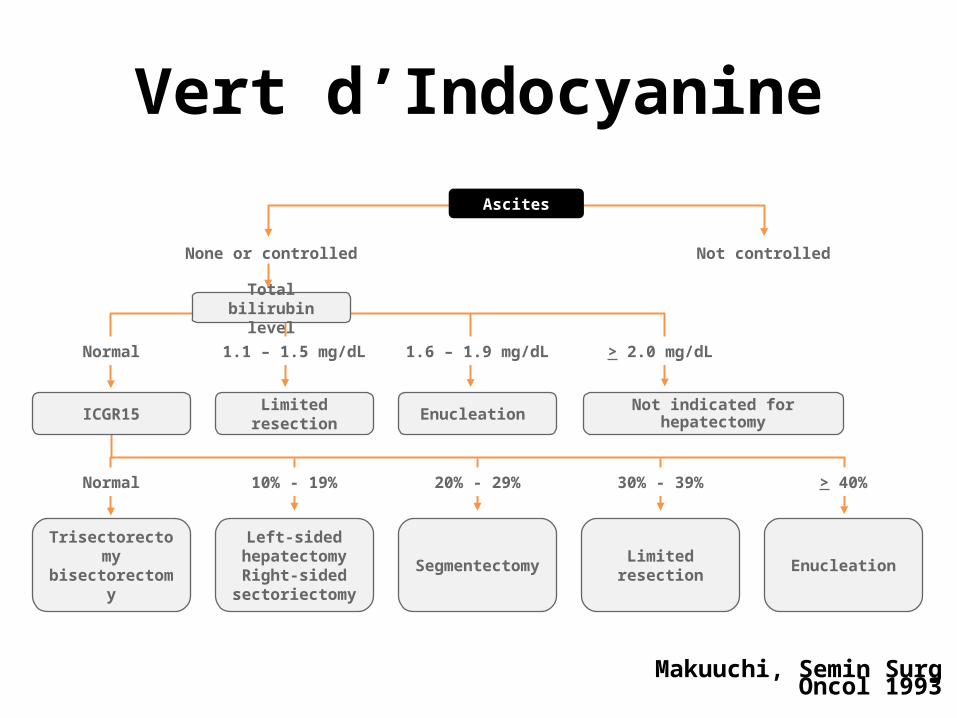
Makuuchi, Semin Surg Oncol 1993
Ascites
None or controlled Not controlled
ICGR15 Limited resection Enucleation Not indicated for hepatectomy
Trisectorectomy bisectorectomy
Left-sided hepatectomyRight-sided
sectoriectomy
Segmentectomy Limited resection Enucleation
Normal 1.1 – 1.5 mg/dL 1.6 – 1.9 mg/dL > 2.0 mg/dL
Total bilirubin level
Normal 10% - 19% 30% - 39% > 40%20% - 29%
Vert d’Indocyanine
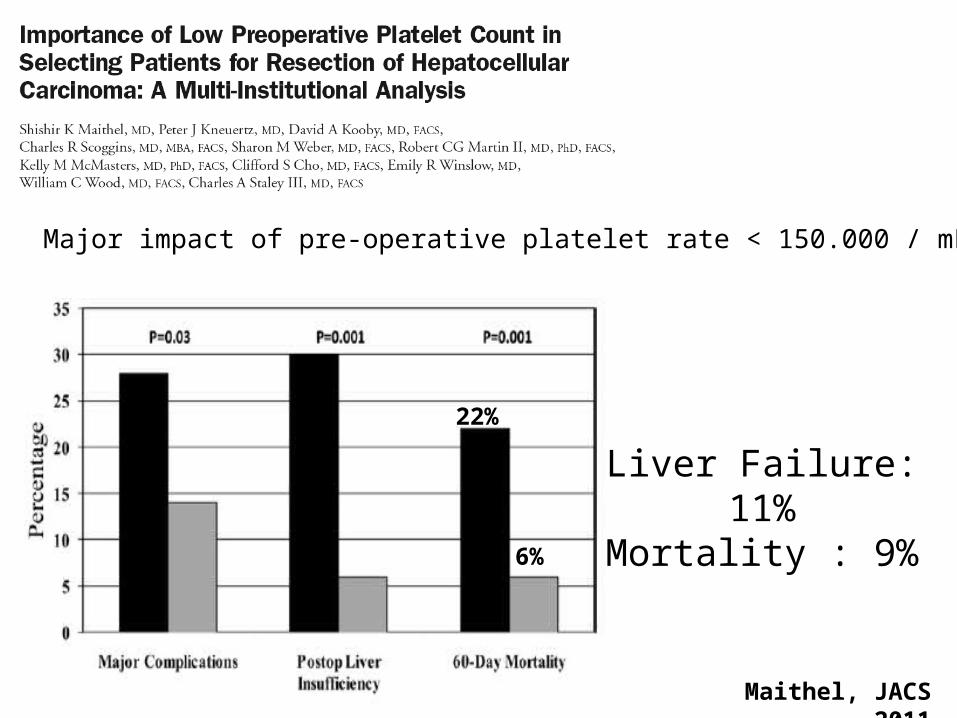
Major impact of pre-operative platelet rate < 150.000 / mL
22%
6%
Liver Failure: 11%Mortality : 9%
2011
Maithel, JACS 2011
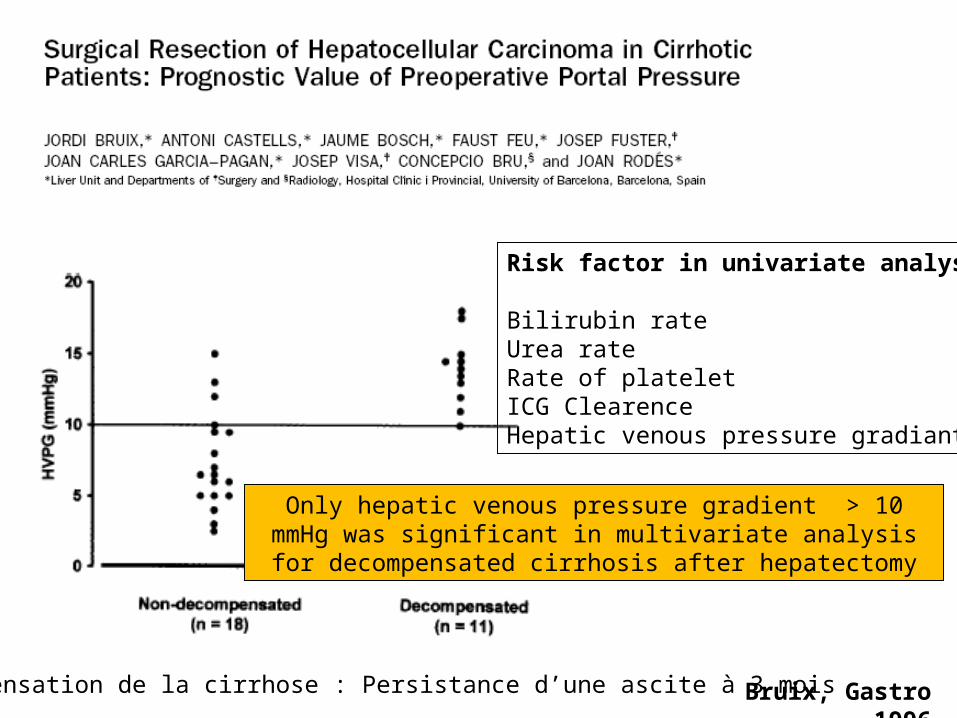
Only hepatic venous pressure gradient > 10 mmHg was significant in multivariate analysis for decompensated cirrhosis after hepatectomy
Risk factor in univariate analysis
Bilirubin rateUrea rateRate of plateletICG ClearenceHepatic venous pressure gradiant,
Décompensation de la cirrhose : Persistance d’une ascite à 3 mois Bruix, Gastro 1996
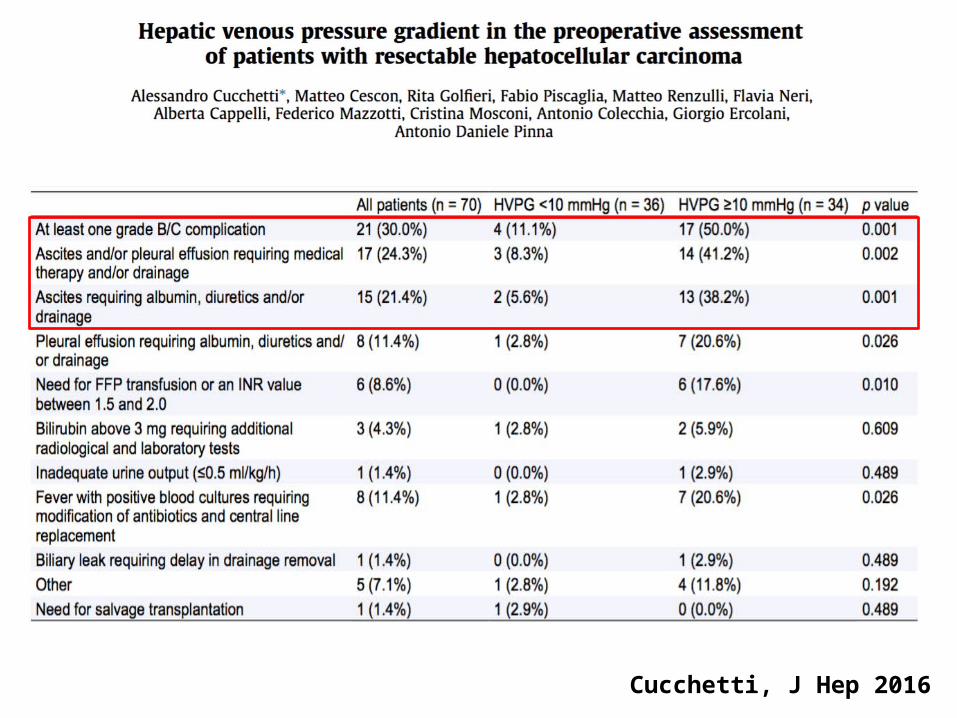
Cucchetti, J Hep 2016

Cucchetti, J Hep 2016
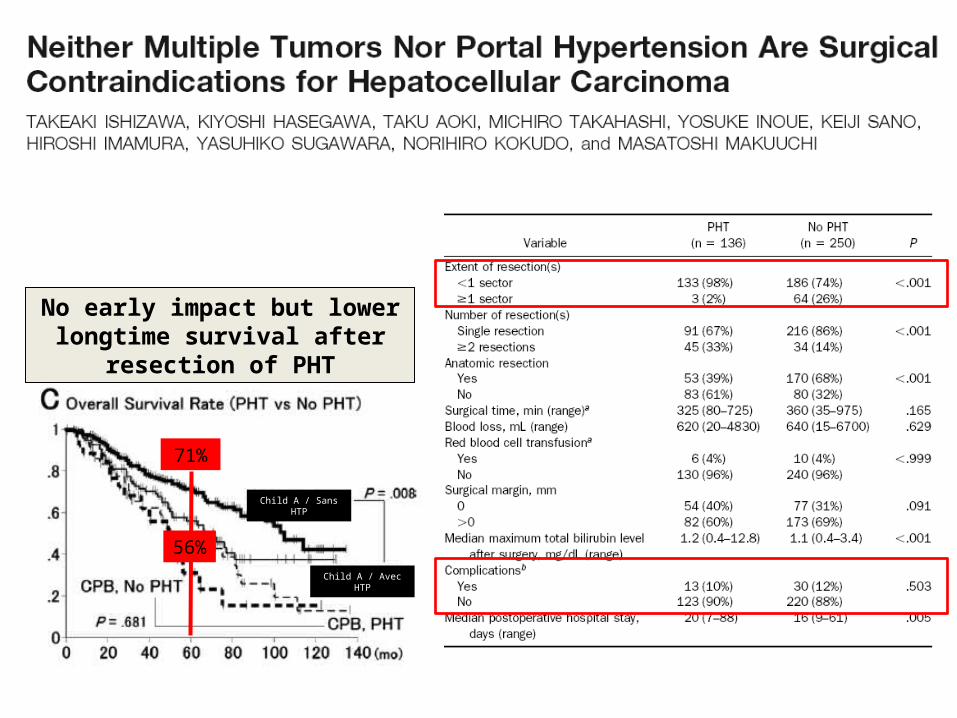
Child A / Sans HTP
56%
71%
Child A / Avec HTP
No early impact but lower longtime survival after resection of PHT
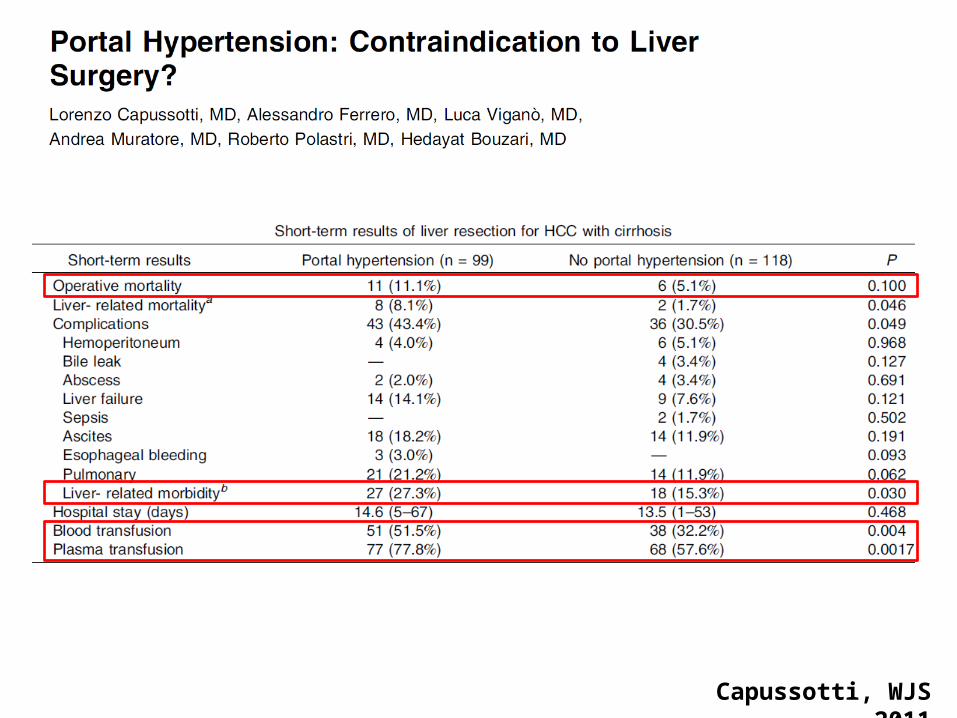
Capussotti, WJS 2011
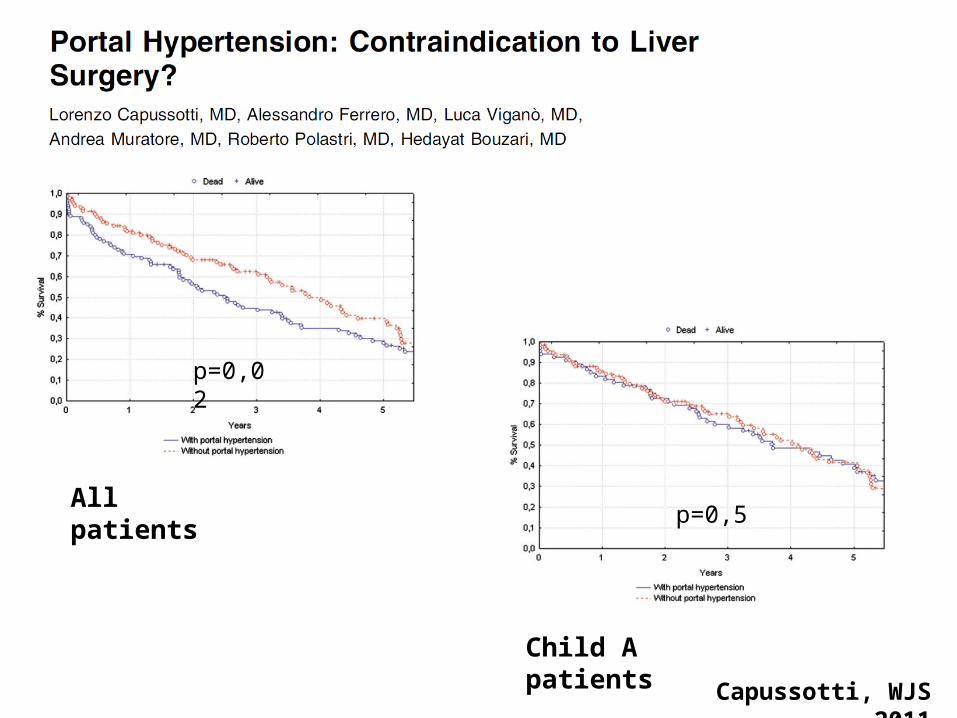
Capussotti, WJS 2011
p=0,02
All patients
Child A patients
p=0,5
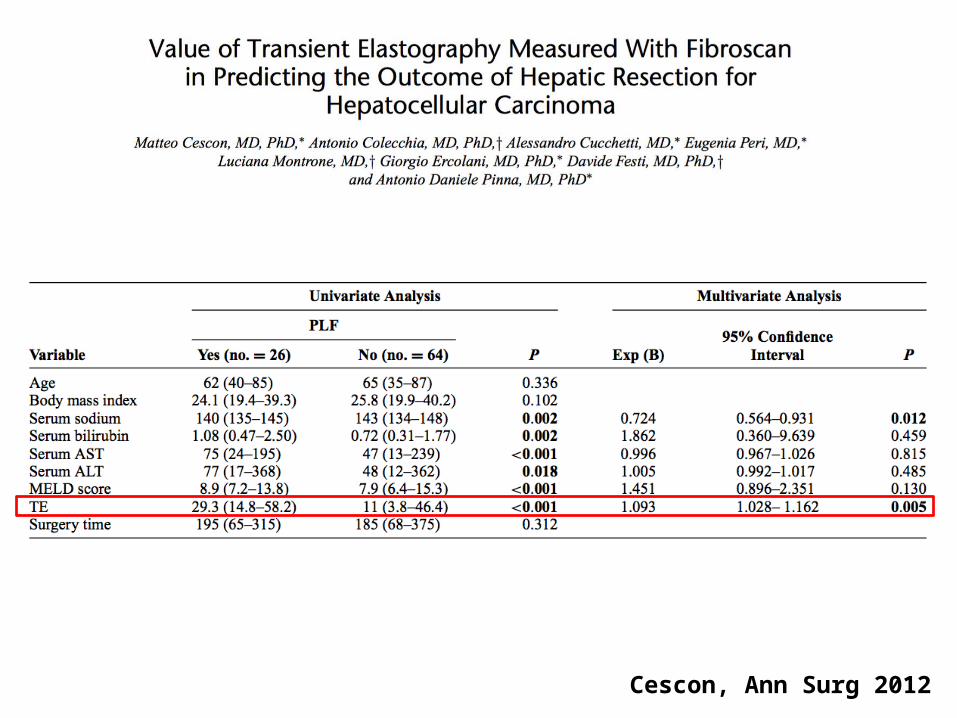
Cescon, Ann Surg 2012
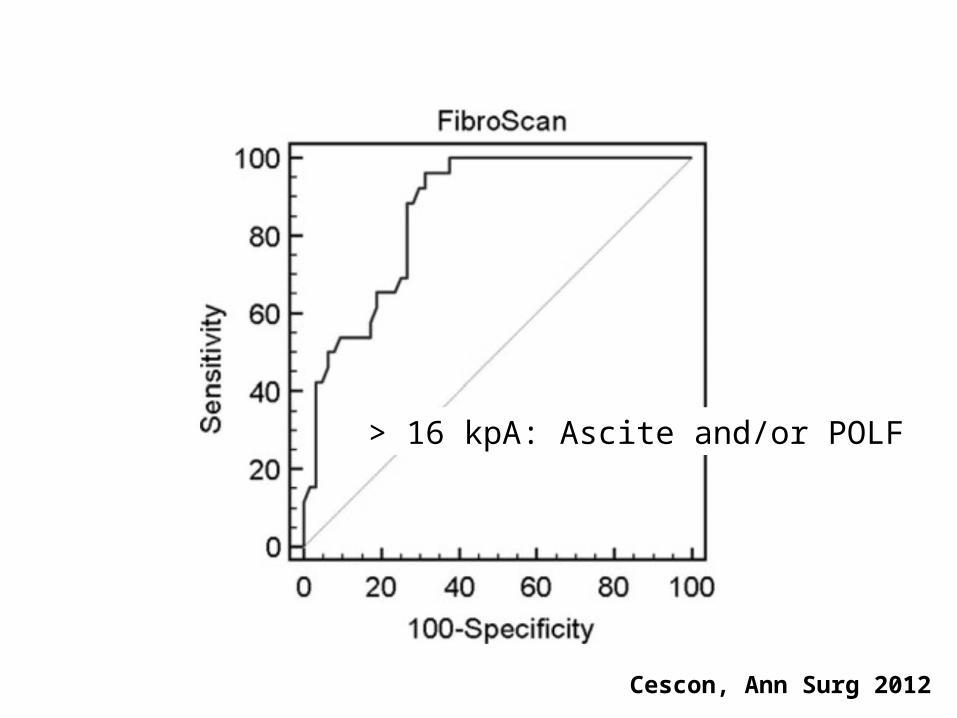
> 16 kpA: Ascite and/or POLF
Cescon, Ann Surg 2012
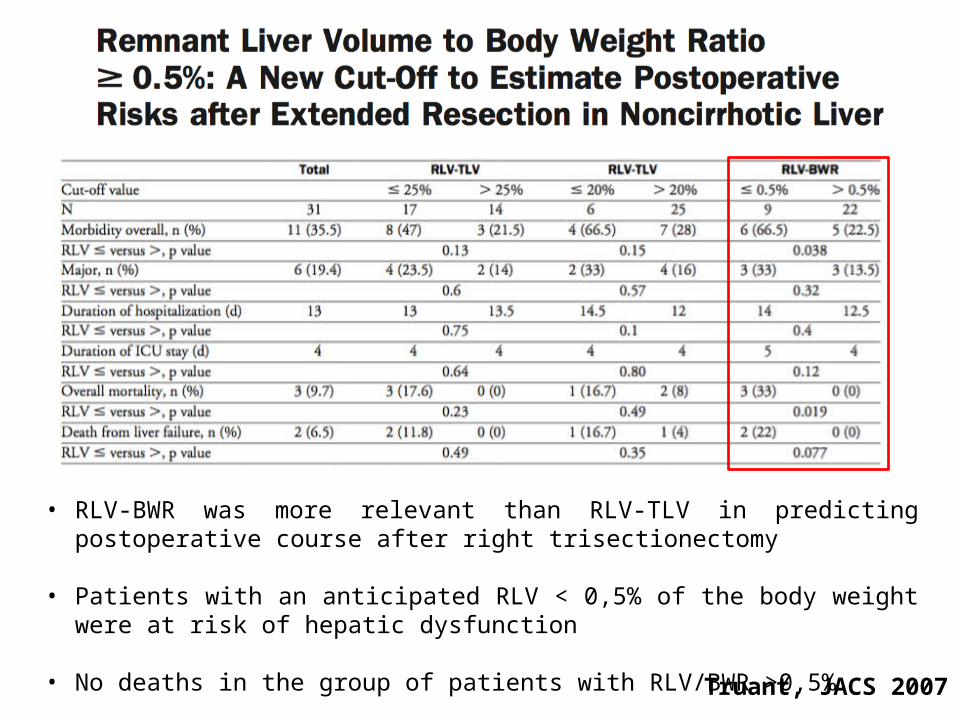
Truant, JACS 2007
• RLV-BWR was more relevant than RLV-TLV in predicting postoperative course after right trisectionectomy
• Patients with an anticipated RLV < 0,5% of the body weight were at risk of hepatic dysfunction
• No deaths in the group of patients with RLV/BWR >0,5%
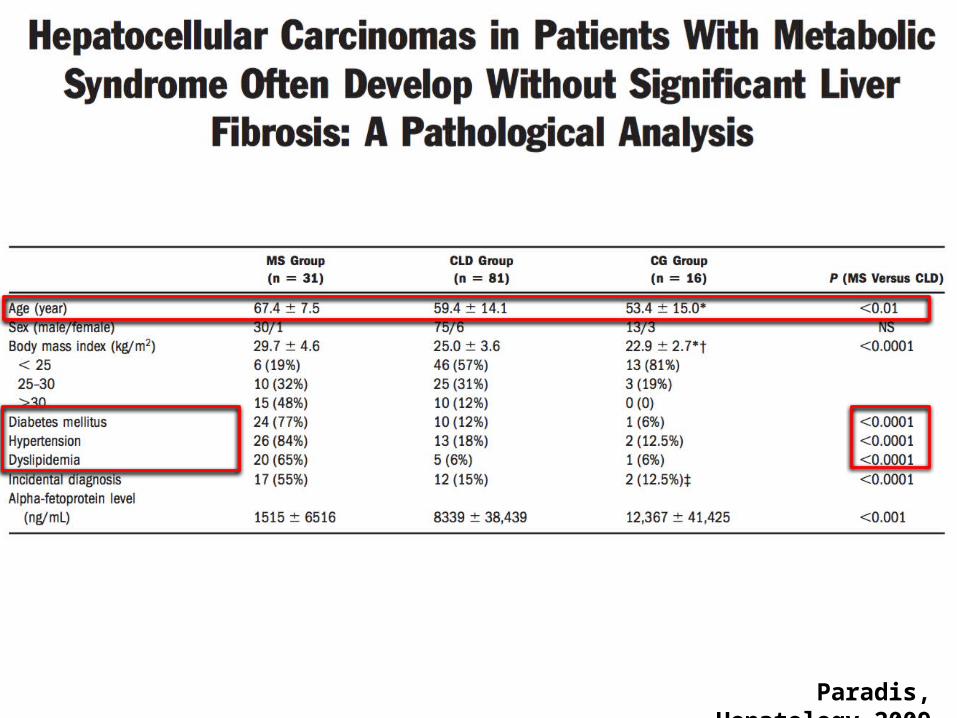
Paradis, Hepatology 2009
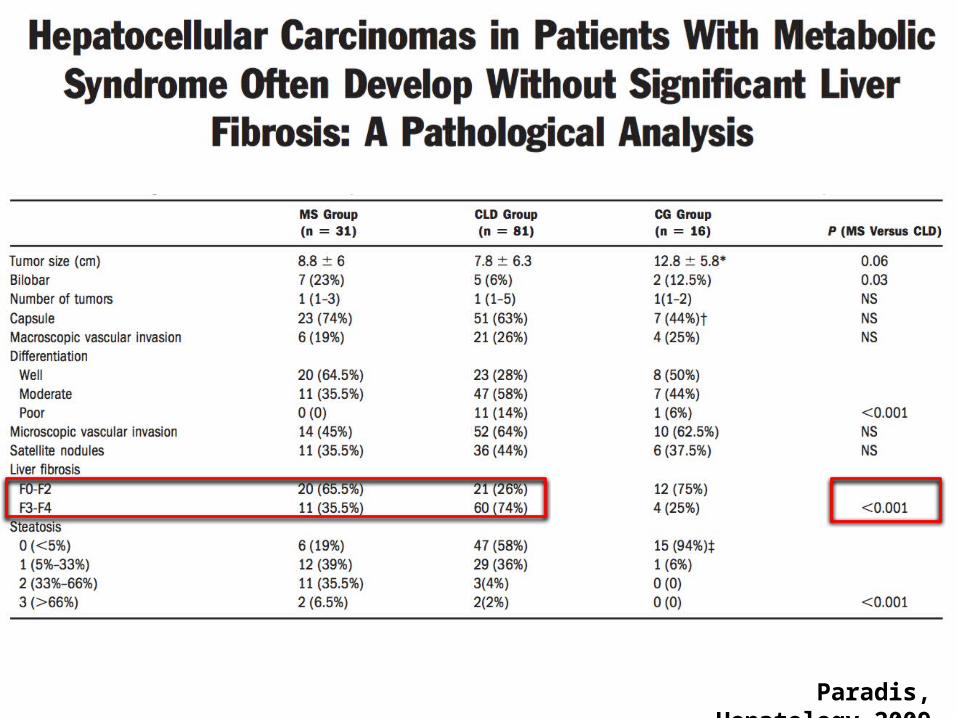
Paradis, Hepatology 2009
Agrawal, HPB 2011
Pre-operative liver biopsy to detect NASH in order to:
• Limit the extent of hepatic resection
• Use the PVE to optimize the post-operative outcome
• Aggressively treat the cardiovascular associated
disease
Wakai, JGIS 2011
• 225 patients
• 3 groups NAFLD – HCV – HBV
• Morbidity 59% vs 31/28% p= 0,043
• Mortality 12% vs 0,7%/3,3% p= 0,016
Cirrhose
• Sélection
• Management

Farges, Ann Surg 2003
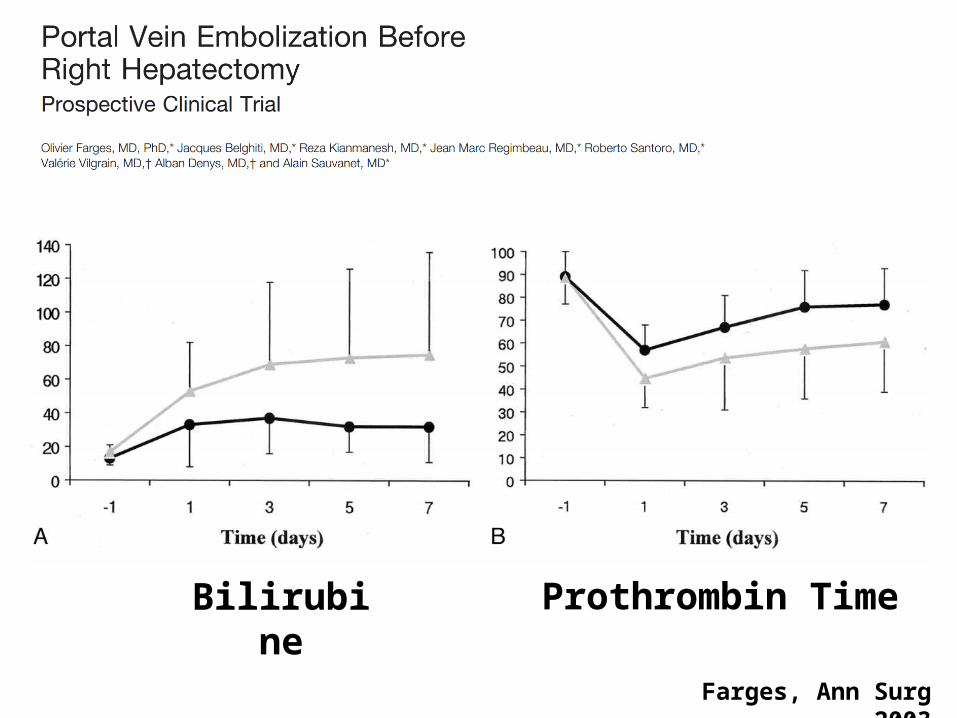
Farges, Ann Surg 2003
Bilirubine Prothrombin Time
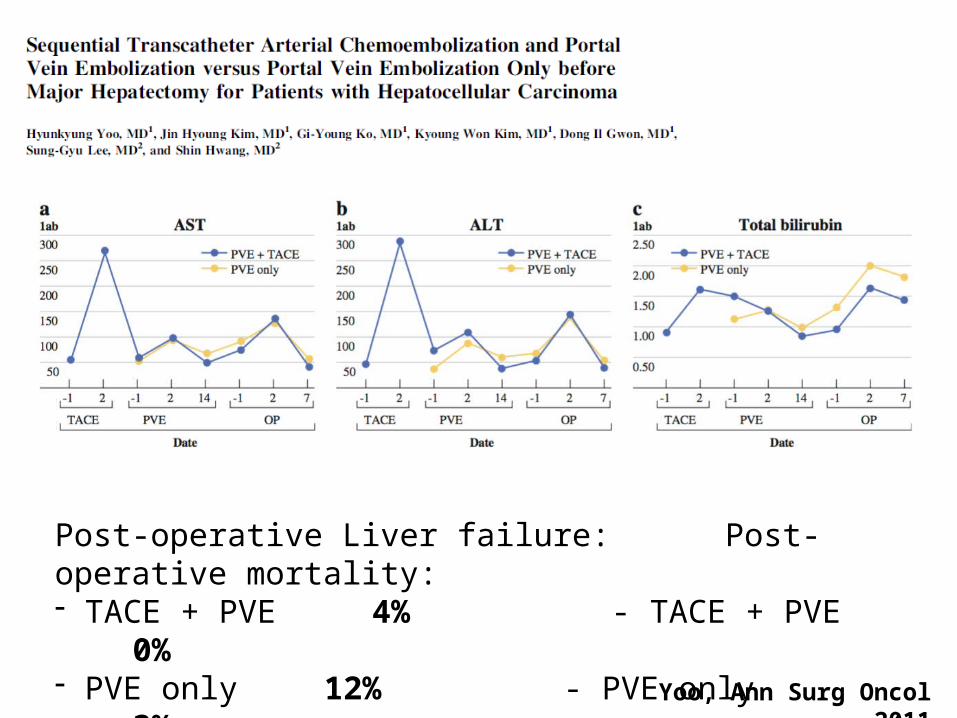
Post-operative Liver failure: Post-operative mortality:- TACE + PVE 4% -
TACE + PVE 0%- PVE only 12% - PVE only
3%Yoo, Ann Surg Oncol 2011
Optimal Technique
• Reduce blood loss
• Fluid restriction anesthesia
• Precise technique
• Intermittent Pringle Maneuver
T T
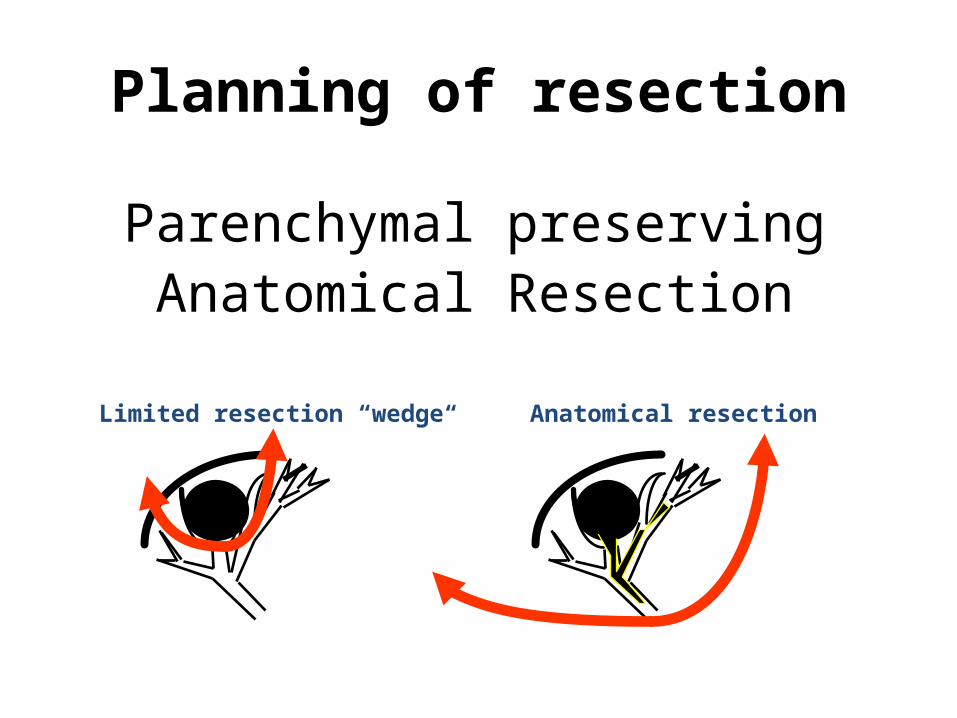
Limited resection “wedge“ Anatomical resection
Parenchymal preservingAnatomical Resection
Planning of resection
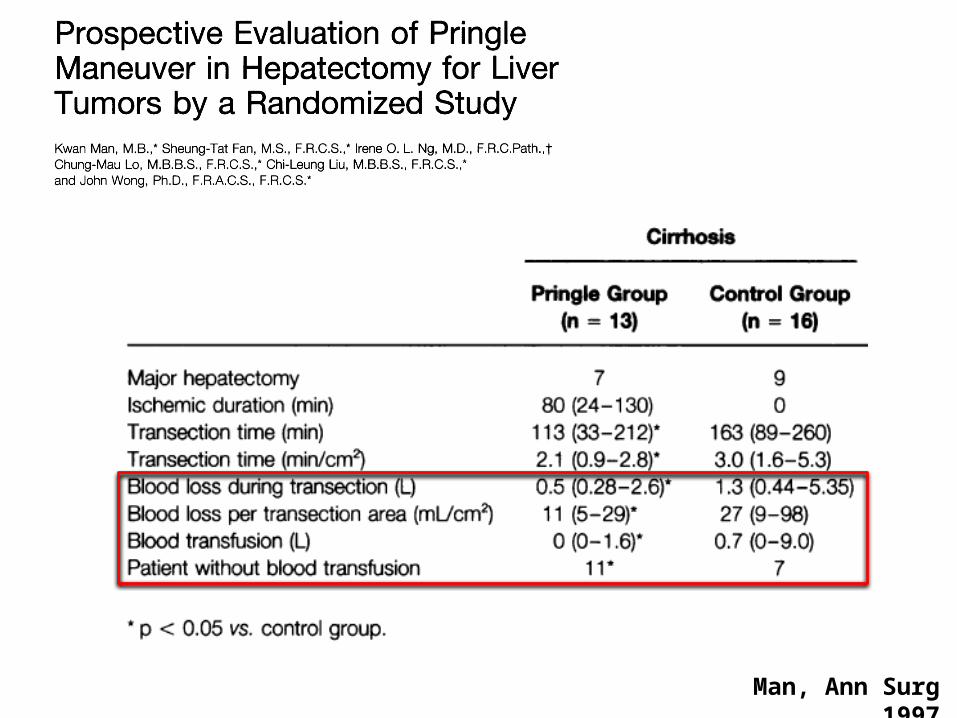
Man, Ann Surg 1997
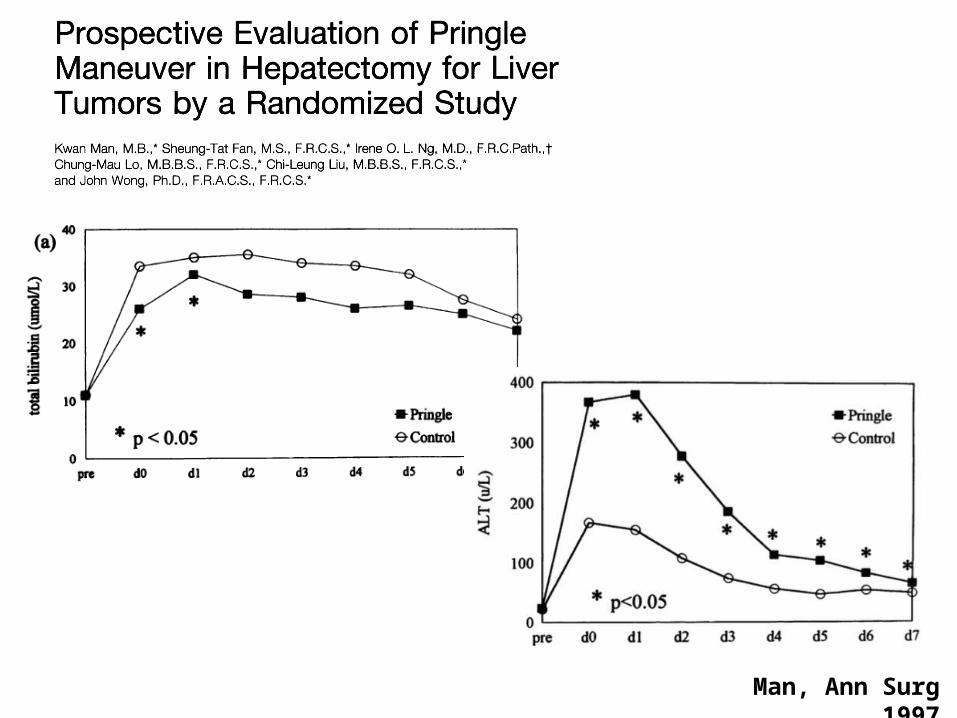
Man, Ann Surg 1997
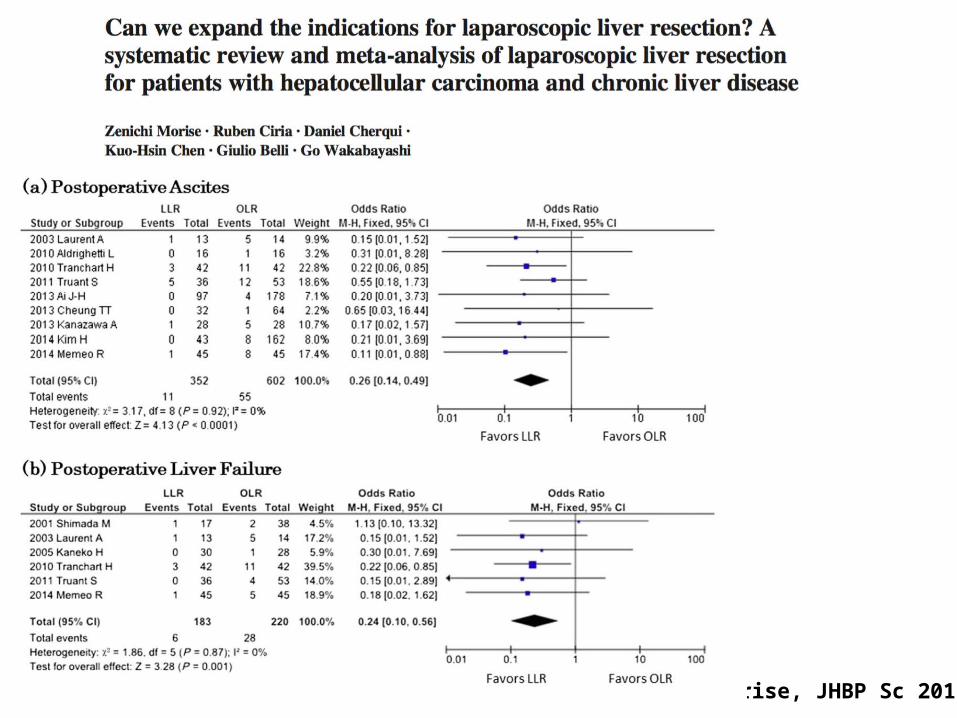
Morise, JHBP Sc 2015
Cirrhose - Conclusions• Major hepatectomy (≥ 3 segments)
– Child A – MELD <9
– No varices, platelets > 100 000, gradient <10 mmHg
– Response to portal vein embolization for Right Hepatectomy
– FLR ≥ 30-40%

Cirrhose - Conclusions• Major hepatectomy (≥ 3 segments)
– Child A– No varices, platelets > 100 000, gradient <10 mmHg– Response to portal vein embolization– FLR ≥ 30-40%
• Minor hepatectomy – Child A (B for tumorectomy)– grade 1-2 varices (laparoscopic)

Hépatopathie
• Cirrhose
• Chimiothérapie
• Cholestase
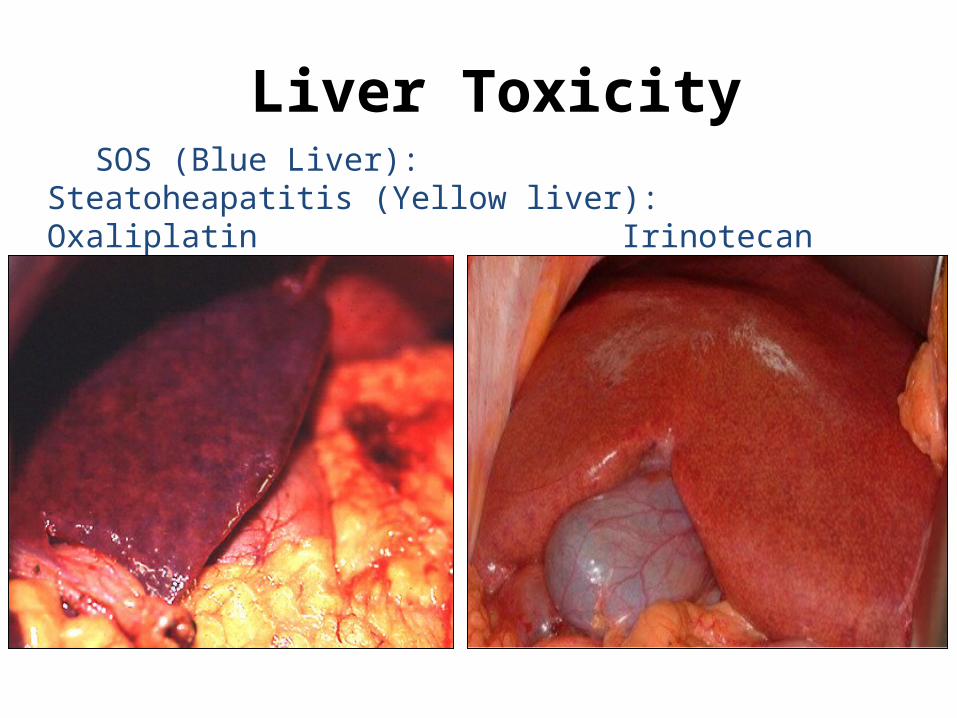
SOS (Blue Liver): Steatoheapatitis (Yellow liver): Oxaliplatin
Irinotecan
Liver Toxicity
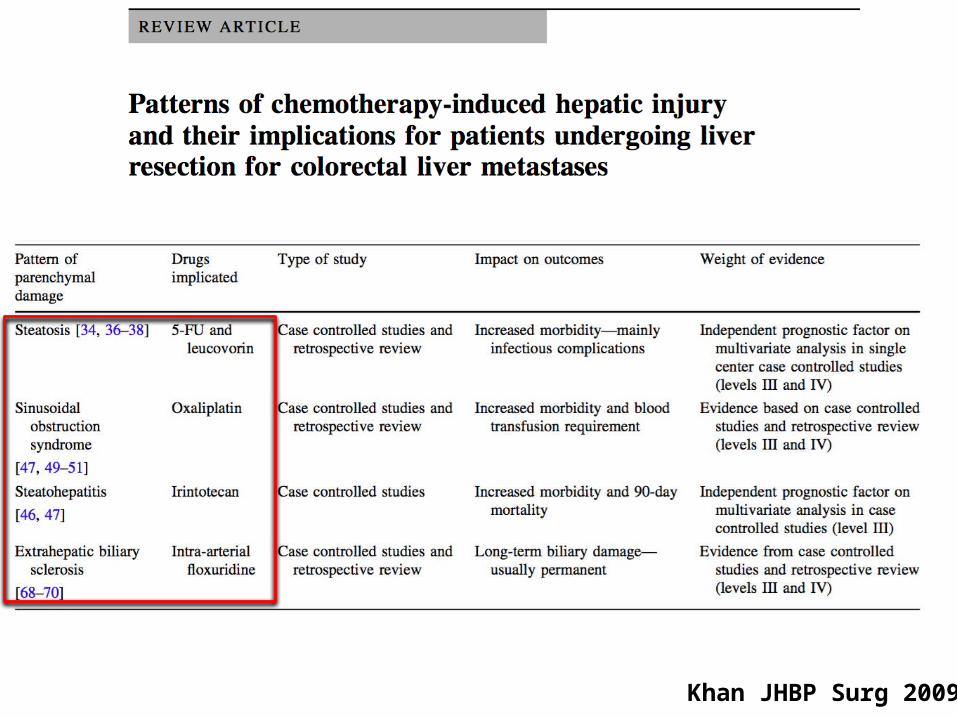
Khan JHBP Surg 2009
Rubbia-Brandt, Ann Oncol 2004
• 51% of patients who received pre-operative chemotherapy had sinusoidal dilatation
• 25% perisinusoidal and venocclusive fibrosis
• Developement correlated to the use of Oxaliplatine
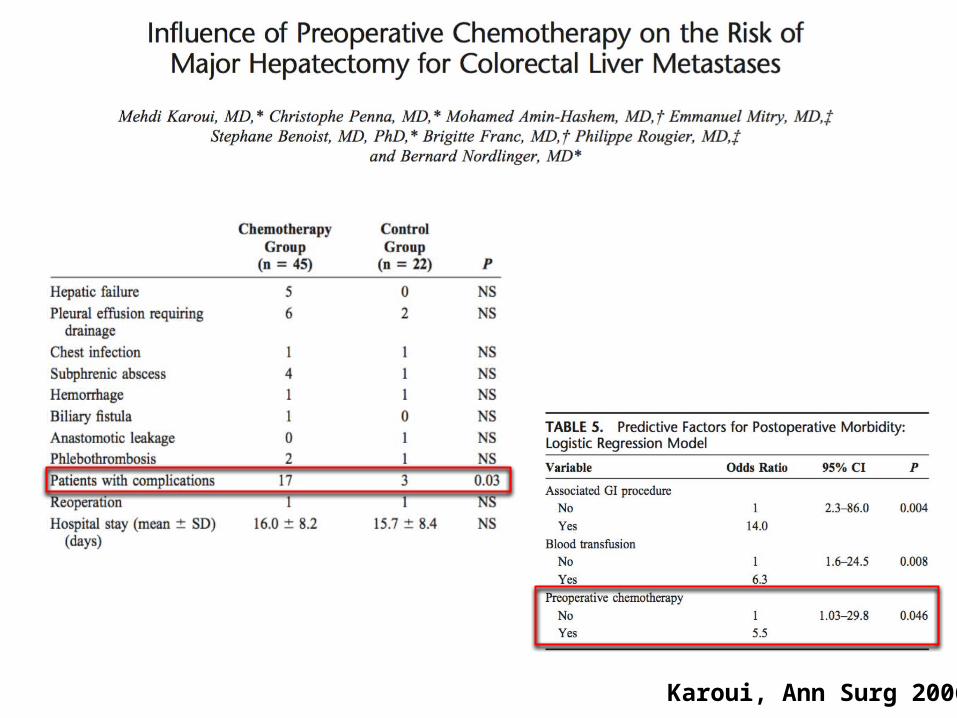
Karoui, Ann Surg 2006

Karoui, Ann Surg 2006
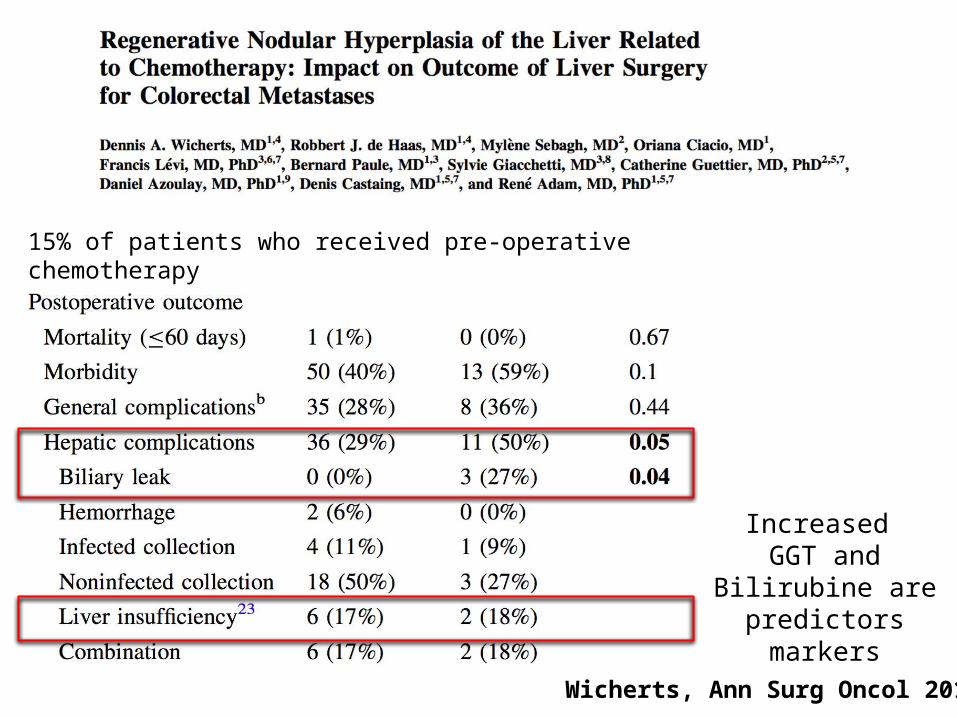
Wicherts, Ann Surg Oncol 2011
15% of patients who received pre-operative chemotherapy
Increased GGT and Bilirubine
are predictors markers
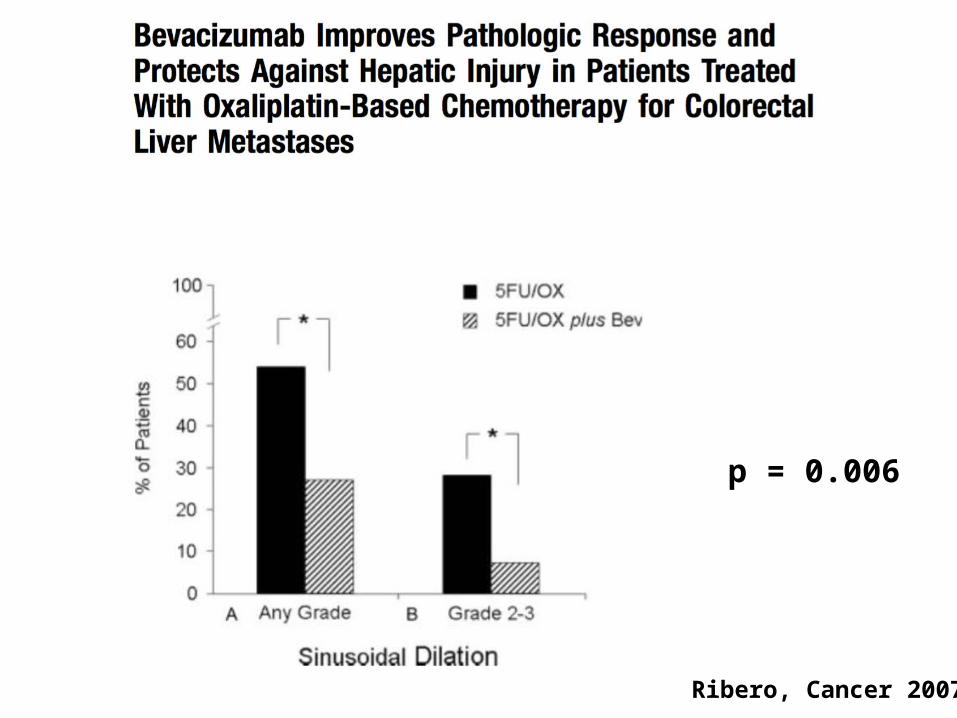
Ribero, Cancer 2007
p = 0.006
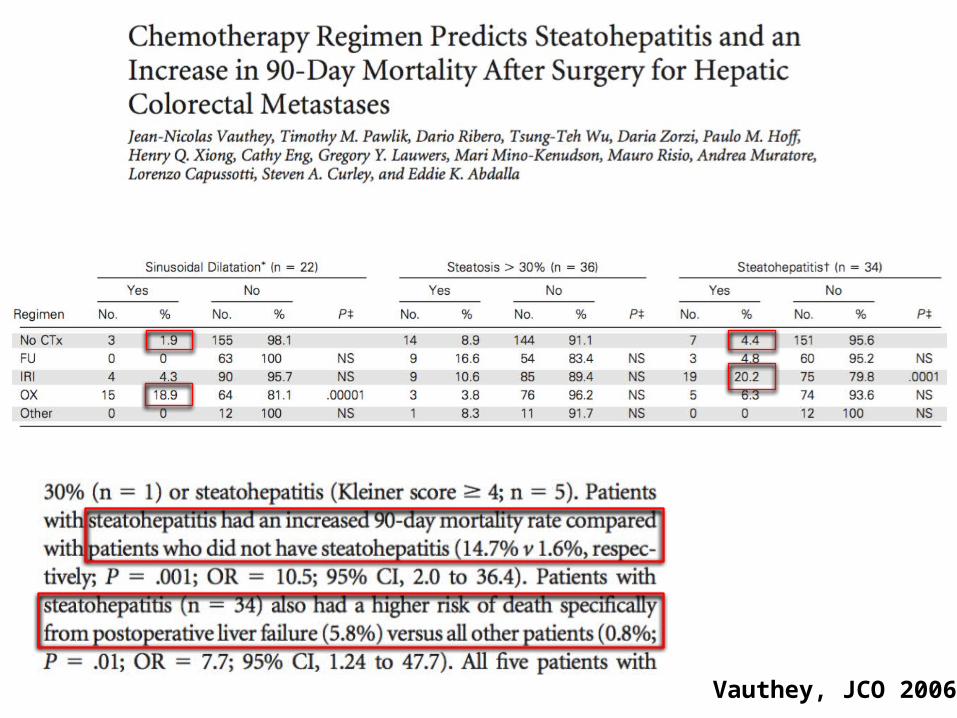
Vauthey, JCO 2006

Kishi, Ann Surg Oncol 2010
Extended chemotherapy increases liver toxicity without improving the pathological response

YesNoPost
hepa
tect
omy
PVP
(mm
Hg)
22.5 mmHg
15 mmHg
Liver failure « 50-50 » criteria
Allard, Ann Surg 2013
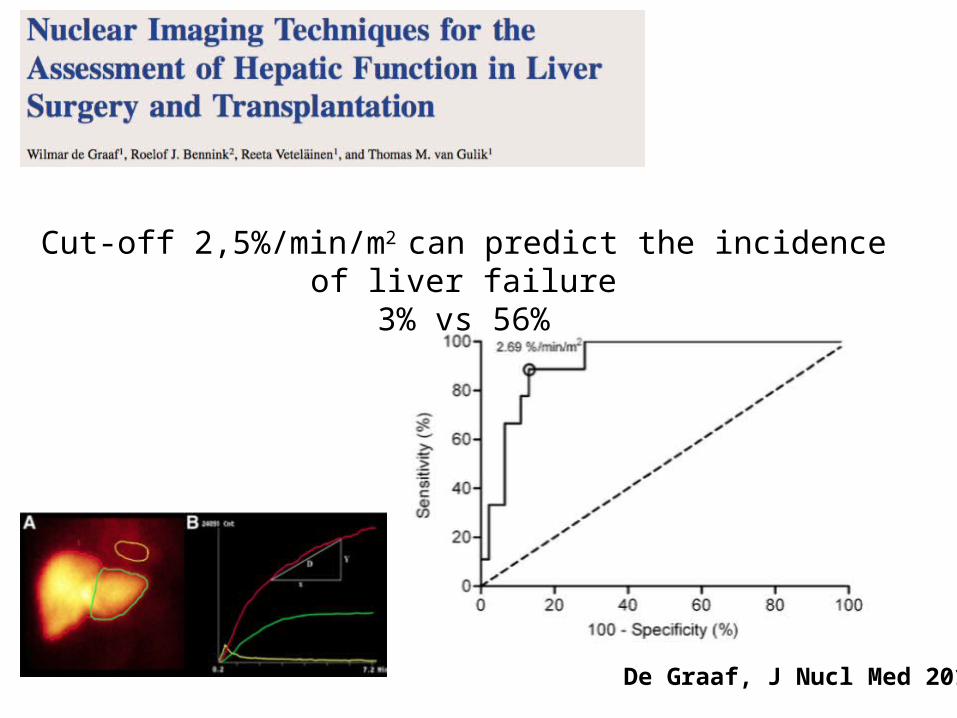
De Graaf, J Nucl Med 2010
Cut-off 2,5%/min/m2 can predict the incidence of liver failure3% vs 56%
Chimiothérapie - Conclusions• Attention aux lésions induites par la chimiothérapie
(> 6 cycles)• Augmentation de la morbidité post-opératoire• Une augmentation des cycles n’augmente pas la
réponse pathologique• Bevacizumab a un effet protecteur sur le
développent de SOS

Hépatopathie
• Cirrhose
• Chimiothérapie
• Cholestase

Cescon, Ann Surg 2009

Kawasaki, Ann Surg 2003
Morbidity related to biliary drainage 2,5%
No post-operative liver failure

Seyama, Ann Surg 2003
Cholangitis 30% (initial period)
1 Tumor seeding (percuteneous)
No post-operative liver failure
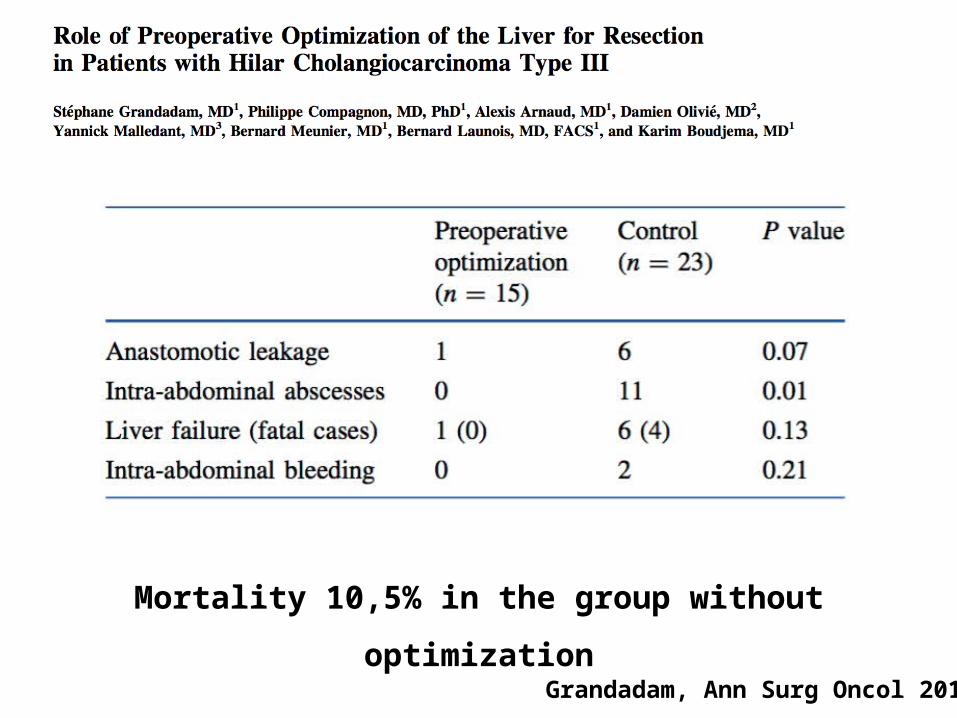
Grandadam, Ann Surg Oncol 2010
Mortality 10,5% in the group without optimization
Sugawara Surgery 2013
• 21% of cholangitis in patients with biliary drainage
• 75% of positive bile cultures at the operation• No difference in postoperative morbidity and
mortality in patients with and without biliary drainage

Takahashi, BJS 2010
• PTBD recurrence 5,9%• Survival in patients with PTBD poorer
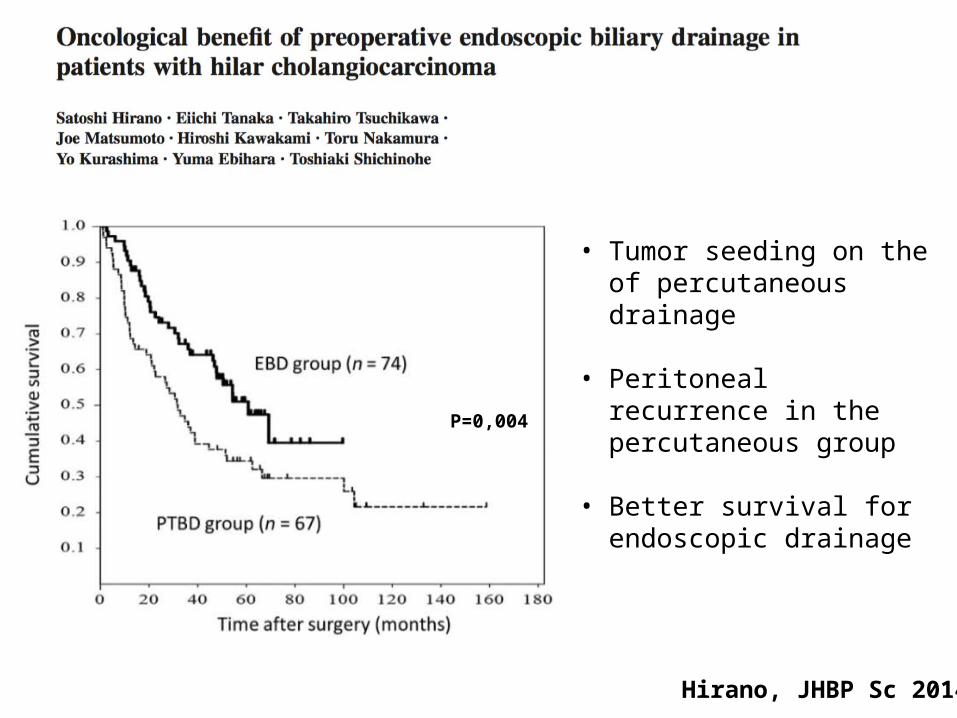
Hirano, JHBP Sc 2014
P=0,004
• Tumor seeding on the of percutaneous drainage
• Peritoneal recurrence in the percutaneous group
• Better survival for endoscopic drainage
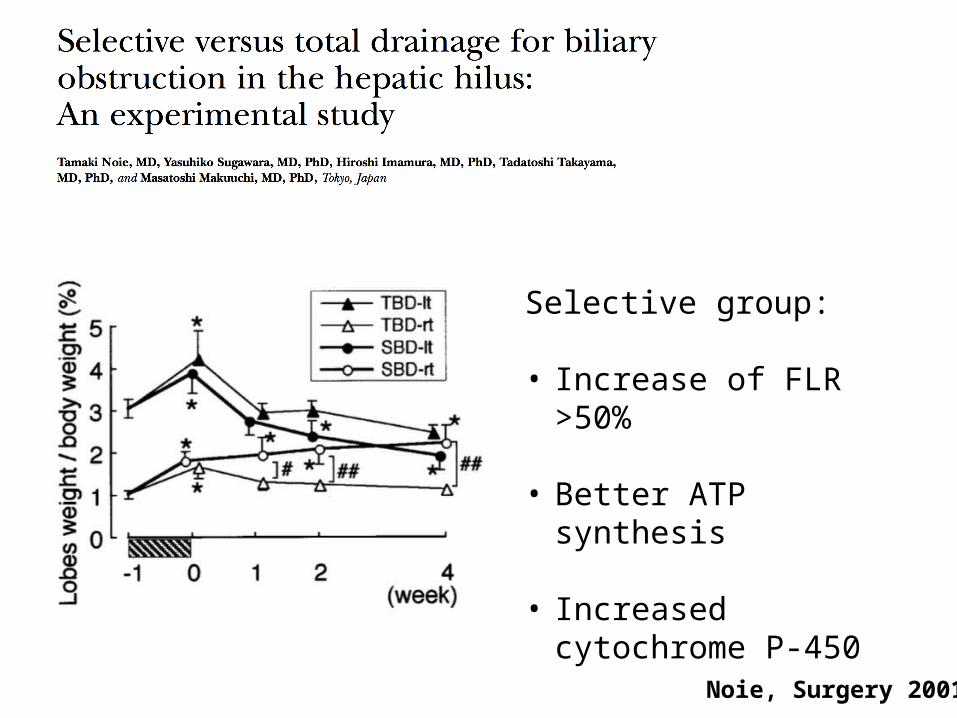
Noie, Surgery 2001
Selective group:
• Increase of FLR >50%
• Better ATP synthesis
• Increased cytochrome P-450
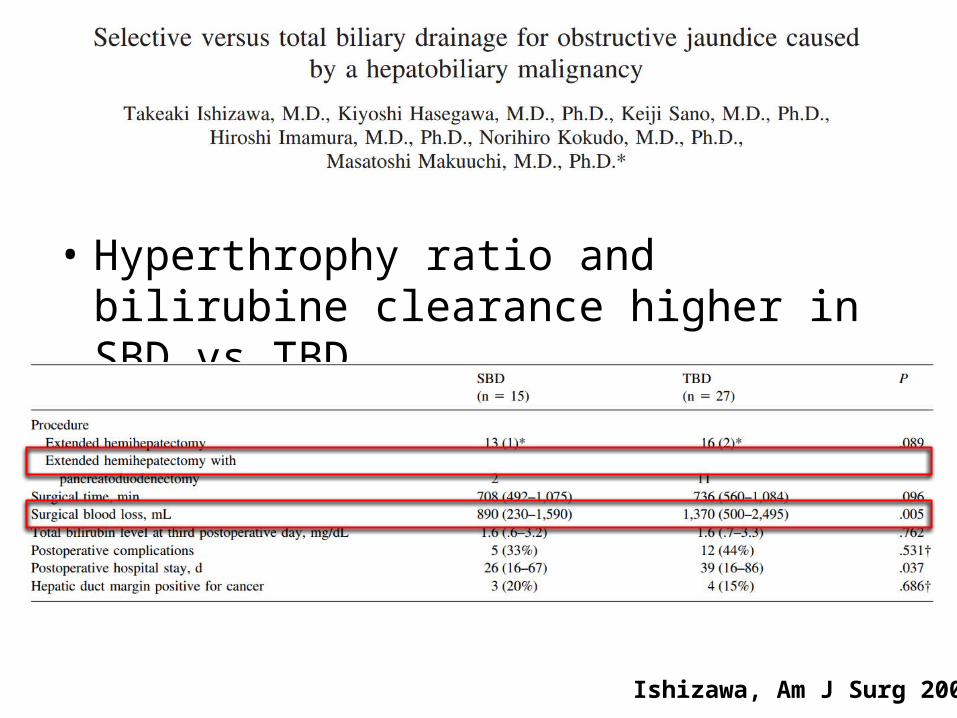
• Hyperthrophy ratio and bilirubine clearance higher in SBD vs TBD
Ishizawa, Am J Surg 2007

Iacono, Ann Surg 2013
Farges BJS 2013
• Biliary drainage does not affect mortality• Decrease the mortality rate after right sided
hepatectomy• Increase mortality after left sided
hepatectomy• Preoperative bilirubine > 50 mmol increases
mortality

Farges BJS 2013

Cholestase - Conclusions
• Optimisation du patient avant chirurgie
• Drainage biliaire du foie restant par voie endoscopique
• Traiter de façon systématique les patients avec prothèses biliaires avec antibiotiques à large spectre







