Pulmonary hypertensionGoal directed therapy
Pulmonary Hypertension ProgrammePulmonary Hypertension ProgrammeUniversity of TorontoUniversity of Toronto
FMD
Disclaimer (1999)
• Support from– No one in particular

Disclaimer (2011)
• Support from– Actelion– Glaxo– Pfizer– United Therapeutics / Northern Therapeutics– Gilead– Lilly– Bayer


Goals
• Identify modifiable and non-modifiableprognostic factors in patients with pulmonaryarterial hypertension
• Interpret changes in hemodynamics andother indicators of disease severity
• Recognize how therapy is targeted inpatients with pulmonary hypertension

Dana Point Classification of PH
Galiè N et al. Eur Heart J 2009; 30:2493-537Galiè N et al. Eur Resp J 2009; 34:1219-63

Caregiver burden
• Emergent themes were – stresses on physical and mental well-being, – Stress on social and personal lives, – Threats to financial security and career paths. – The interviewees reported a sense of isolation as
related to dealing with a disease that is relatively unknown to the majority of friends and family.

“The unwillingness to admit to their loved-ones, or indeed to themselves, that the caregiver role was taxing, augmented the sense of isolation”
Vasoconstrictors
Vasodilators
An imbalance...

What is it?


Echo measures of RV function
TAPSE
Tei Index = (a – b) / b
Eccentricity index

Goals of treatment
• Improve quality of life• Restore exercise capacity• Improve survival


Treatment paradigm
• Add therapy for disease progression

2005; 25: 244–249
% o
f pati
ents
(n=1
69)
12 months 24 months
DeadOff bosentanOn dual agents
On bosentan alone

Treatment paradigm
• Add therapy for disease progression
• Add therapy for failure to reach goals


Respiratory Medicine (2010) 104, 1588e1607

Respiratory Medicine (2010) 104, 1588e1607

McLaughlin VV, et al. Circulation. 2002;106:1477-1482.
0
20
40
60
80
100
Surv
ival
(%)
0 12 24 36 48 60 72 84No. at risk 162 33 95 70 48 30 20 10
Months
FC=3
FC=4p=0.0001 by log-rank test
847260483624120
100
80
60
40
20
0
FC=1
No. at risk:
FC=2
FC=3
FC=4Su
rviv
al (%
)
Months
Impact of Functional Class on Survival
Functional Class at Baseline
Functional Class at 17±15 mos
102030466386112115

JACC Vol. 40, No. 4, 2002

Circulation. 2006;114:1482-1489

Circulation. 122(2):164-72, 2010 Jul 13. 2
Multivariate predictors of 1 year outcome in REVEAL
Predicting survival in pulmonary arterial hypertension: insights from the Registry to Evaluate Early and Long-Term Pulmonary Arterial Hypertension Disease Management (REVEAL).Benza RL; Miller DP; Gomberg-Maitland M; Frantz RP; Foreman AJ; Coffey CS; Frost A; Barst RJ; Badesch DB; Elliott CG; Liou TG; McGoon MD
Figure 2. Cox proportional-hazards estimates for multivariable model of survival, limited to terms included in the final stepwise model. Parameters significantly associated with 1-year survival only in univariable analyses included the Borg dyspnea scale, right ventricular dysfunction, pulmonary vascular resistance (PVR) index, pulmonary capillary wedge pressure, cardiac index, mean pulmonary artery pressure, and total serum bilirubin. Candidate predictor variables that were not significant at the univariable level included Tei index, vasoreactivity, race, newly diagnosed PAH, and income. Missing Borg scale and missing PVR index were both associated with lower-than-average observed survival and were therefore considered candidate predictor variables. APAH indicates associated I PAH; ECHO, echocardiogram; FPAH, familial PAH; mRAP, mean right atrial pressure; PoPH, portopulmonary hypertension; and RHC, right heart catheterization. *Reference category: NYHA/WHO functional class (Fn) II or missing. +If N-terminal proBNP is available and BNP is not, listed cut points are replaced with 1500 pg/mL. ++Restricted to tests performed within 1 year of enrollment; otherwise, the indicator is set to 0.
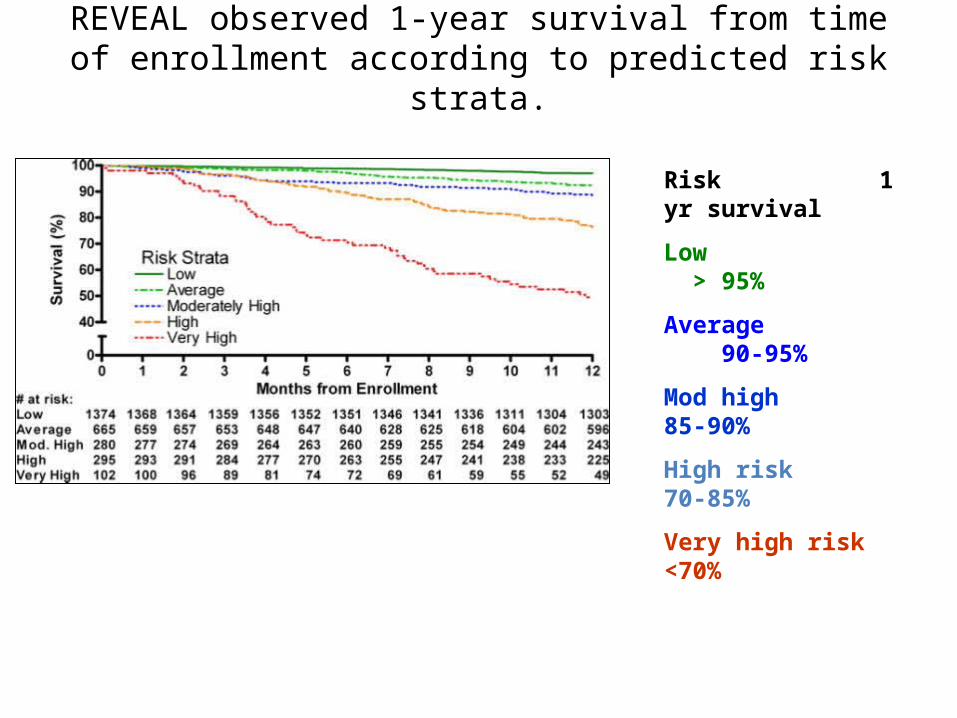
REVEAL observed 1-year survival from time of enrollment according to predicted risk strata.
Risk 1 yr survival
Low > 95%
Average 90-95%
Mod high 85-90%
High risk 70-85%
Very high risk <70%

15 possible risk factors
4 possible protective factors
0 - 22
Actual scores ranged from 1 – 15
With a mean of 7.4

Prevalent cases
Incident cases
Combination therapy• 26 observational studies and 5 randomized trials were identified.
• PDE-5 inhibitor and prostanoids, 6/7 studies reported improvement in 6MWD, 6/8 studies reported improvement in functional class, 6/6 studies reported improvement in hemodynamics and 1/2 trials demonstrated improvement in quality of life and time-to-clinical worsening.
• ERA and prostanoids, 4/6 studies and 1 trial reported improvement in 6MWD, 3/3 studies and 1/4 trials reported improvement in functional class, 4/5 studies and 1/4 trials reported improvement in PAP.
• ERA and PDE-5 inhibitor, 4/7 studies reported an improvement in 6MWD, and 2/6 studies report improvement in functional class.



Galiè N et al. Eur Heart J 2009; 30:2493-537Galiè N et al. Eur Resp J 2009; 34:1219-63

Galiè N et al. Eur Heart J 2009; 30:2493-537Galiè N et al. Eur Resp J 2009; 34:1219-63

Prognostically important variablesand treatment goals
CHEST 2006; 130:214–217


IIt’s best to avoid standing directly between a competitive jerk and his goals







