
Close this window to return to IVIS http://www.ivis.org
Proceeding of the Belgian Equine Practitioners Society
28 November 2015 - Leuven, Belgium
Next Meeting:
Reprinted in the IVIS website with the permission of BEPS
Belgian Equine Practitioners Society Study Days Nov. 2016 - Leuven, Belgium

9
DIAGNOSTIC ANALGESIA OF THE FOOT: TECHNIQUES &
INTERPRETATIONS
PROF. DR. MICHAEL SCHRAMME, JOHN SCHUMACHER, JIM SCHUMACHER AND WILHITE
ECOLE NATIONALE VETERINAIRE DE LYON ( FRANCE) AUBURN UNIVERSITY, ALABAMA (USA)
UNIVERSITY OF TENNESSEE, KNOXVILLE, TENNESSEE (USA)
Summary
A palmar digital nerve block anaesthetises the entire foot, rather than just its palmar half. To
avoid partially anaesthetising the proximal interphalangeal joint, the palmar digital nerves
should be anaesthetised near or distal to the proximal margin of the collateral cartilages. A
basilar sesamoid nerve block may ameliorate pain within the metacarpo (metatarso)
phalangeal joint. Mepivacaine administered into the distal interphalangeal (DIP) joint
desensitises the DIP joint and the subsynovial palmar digital nerves thereby also anesthetising
the navicular apparatus, the toe region of the sole and the digital portion of the deep digital
flexor tendon (DDFT). Even though analgesia of the DIP joint results in analgesia of the
navicular bursa, analgesia of the navicular bursa does not result in analgesia of the DIP joint.
Analgesia of the DDFT sheath likely desensitises only structures within the sheath and the
DDFT distal to the sheath.
Anaesthesia of the palmar digital nerves (Palmar digital nerve block-PDNB)
The PDNB is sometimes referred to as the “heel block” because clinicians have long believed
that a positive response to anaesthesia of the palmar digital nerves localizes pain to the palmar
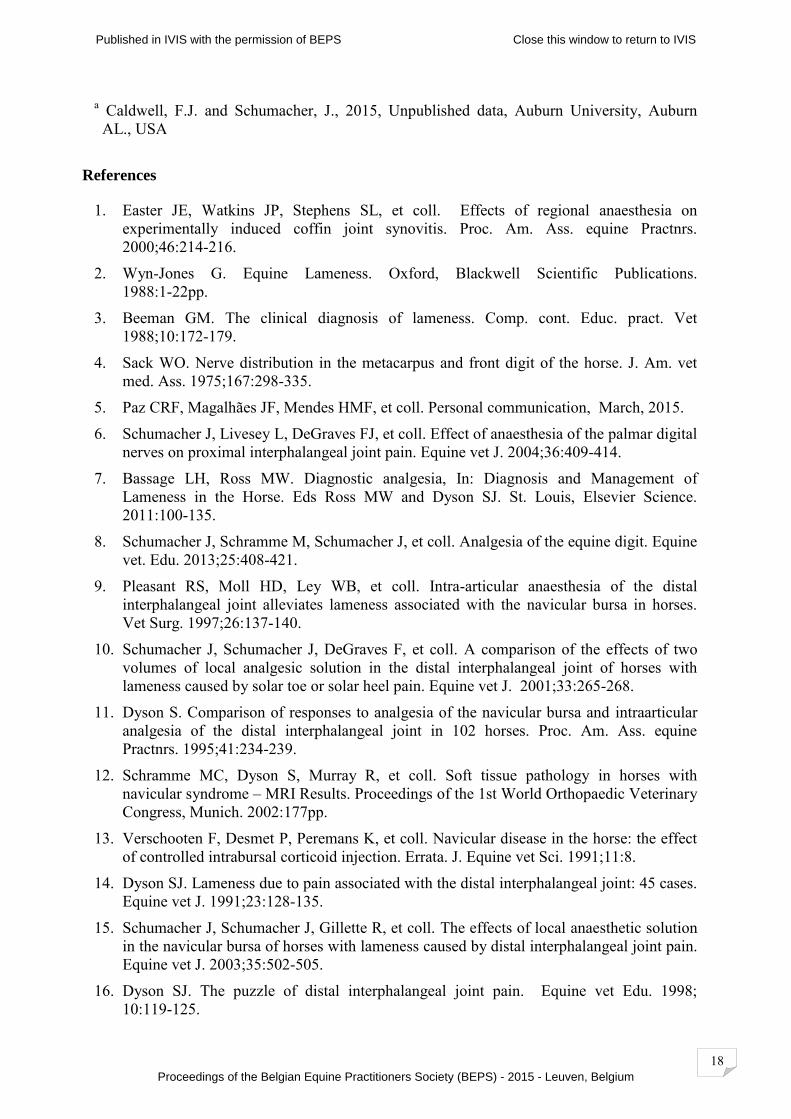
third or half of the foot, including the palmar portion of the DIP joint. Easter et al.1 found,
however, that anaesthesia of the palmar digital nerves just proximal to the bulbs of the heel
alleviated lameness caused pain in the DIP joint, indicating that the palmar digital nerves
innervate the entire DIP joint.
Published in IVIS with the permission of BEPS Close this window to return to IVIS
Proceedings of the Belgian Equine Practitioners Society (BEPS) - 2015 - Leuven, Belgium

10
The PD nerves should be anaesthetised near or distal to the proximal margin of the collateral
cartilage.2,3 One theoretical advantage of anaesthetizing the palmar digital nerves as far
distally as possible is that anaesthesia of the dorsal branches of the palmar digital nerve is
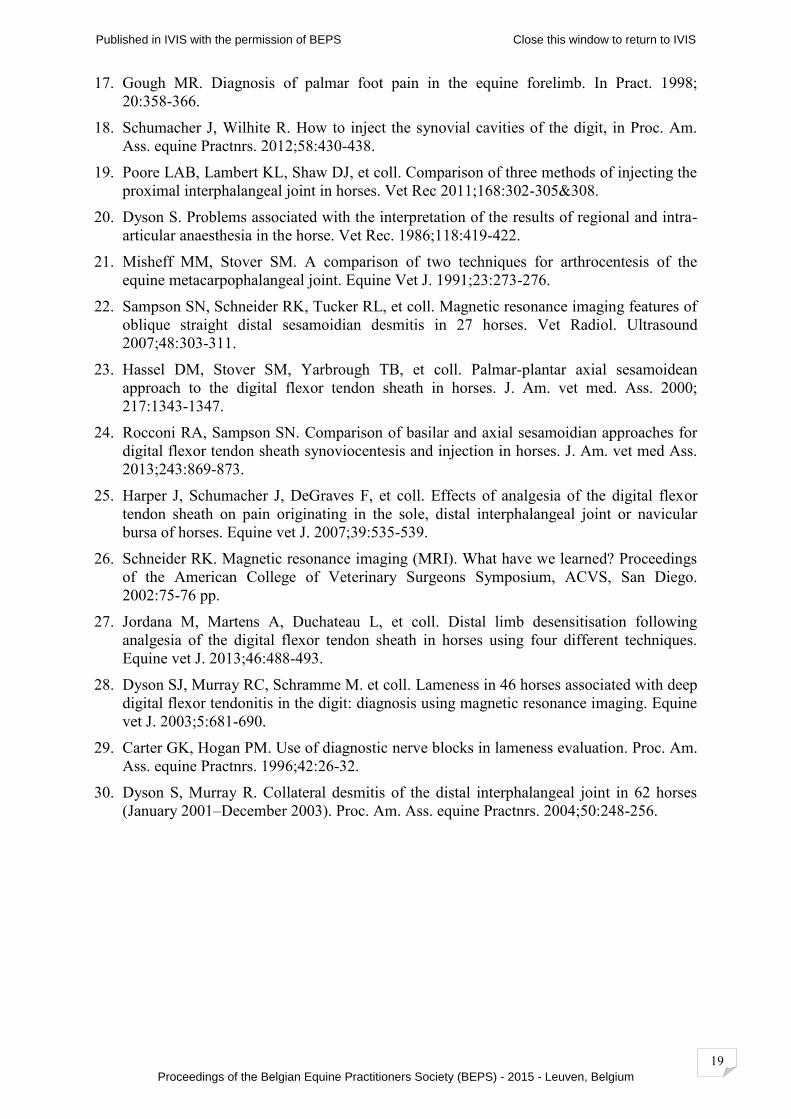
more likely to be avoided (Beeman 1988). According to results of the study by Sack4 and that
of Easter et al.,1 however, the dorsal branches are unlikely to contribute much more than
sensory innervation to the dorsal aspect of the coronary band and dorsal laminae of the foot.
Recent research suggests the even the dorsal laminae of the foot are desensitised by a PDNB.5
Research indicates, therefore, that a PDNB anaesthetises the entire foot.
A more important reason for depositing local anaesthetic solution as far distally in the pastern
as possible when performing a PDNB is that more proximal deposition of local anaesthetic
solution increases the likelihood of causing analgesia of the pastern joint.6
Ring block
A ring block, performed at the level of a PDNB is unlikely to result in a positive response
after a negative response to a PDNB because the dorsal branches of the palmar digital nerves
contribute little to sensation within the foot.1,4,5 The PDNB will already have anaesthetised the
entire foot. The use of a pastern ring block performed at mid pastern level, however, should
be considered as a better alternative to the basilar sesamoid (basisesamoid) nerve block
(BSNB) or abaxial sesamoid nerve block (ASNB) because these blocks may inadvertently,
partially or entirely desensitise the metacarpo/metatarso phalangeal (MC/MT-P) (fetlock)
joint in addition to the entire foot and pastern, which erroneously localise pain to the foot or
pastern in horses with fetlock pain. A positive response to a ring block performed at mid
pastern level, after a negative response to a PDNB, localizes lameness to the pastern region.
Basilar or Abaxial sesamoid nerve block (BSNB or ASNB)
Bassage and Ross6 distinguish between anaesthesia of the palmar or plantar digital nerves
where local anesthetic is deposited at the base of the proximal sesamoid bones (i.e., a BSNB)
and anaesthesia of the palmar or plantar digital nerves where local anaesthetic solution is
deposited more proximally alongside the proximal sesamoid bones (i.e. an ASNB).
Anaesthesia of the digital nerves and their dorsal branches, at either level, alongside or at the
base of the proximal sesamoid bones, desensitises the foot, the pastern joint, the middle
phalanx and associated soft tissues, and the distal and palmar aspects of the proximal phalanx.
Published in IVIS with the permission of BEPS Close this window to return to IVIS
Proceedings of the Belgian Equine Practitioners Society (BEPS) - 2015 - Leuven, Belgium
11
Clinicians should be aware that an ASNB or BSNB may ameliorate or abolish pain within the
MC/MT-P joint.2,6 Performing the nerve block at the base of the proximal sesamoid bones
(i.e., a BSNB) decreases the likelihood of partially desensitizing the MC/MT-P joint.2 Using a
small volume of local anaesthetic solution (i.e., <2 mL) may also decrease the likelihood of
partially anaesthetising the MC/MT-P joint.
Analgesia of the distal interphalangeal joint (DIP joint)
Local anaesthetic solution is most easily and accurately administered into the DIP joint using
a dorsal parallel or dorsal inclined approach, where a needle is placed into the dorsal pouch of
the DIP joint on or near midline, through or just proximal to the coronary band.
The effect of local anaesthetic solution in the DIP joint has been reviewed.8 Local anaesthetic
administered into the DIP joint desensitises the DIP joint, the navicular bursa, the navicular
bone, the toe region of the sole and the digital portion of the deep digital flexor tendon
(DDFT) of most horses. When a large volume of mepivacaine HCl (e.g. 10 mL) is
administered, the heel region of the sole may also be desensitised.
Possible explanations for analgesia of the navicular apparatus (i.e., the navicular bone and its
associated ligaments) after local anaesthetic solution is administered into the DIP joint is the
desensitization of the palmar digital nerves where they lie in close proximity to the palmar
pouch of the DIP joint.9 Occasionally, the palmar aspect of the coronary band is desensitised
after anaesthesia of the DIP joint;10 this finding, as well as desensitisation of the solar region
of the toe support the theory that analgesia of the DIP joint causes desensitisation of the
palmar digital nerves. A negative response to intra-articular analgesia of the DIP joint may not
eliminate the navicular bone and its related structures as the source of lameness. In a study of
102 horses with chronic foot pain, Dyson found that 21% of horses failed to respond to intra-
articular analgesia of the DIP joint but improved significantly after intrabursal analgesia of the
navicular bursa.11 A later study showed that some lesions of the DDFT at the level of the
tendon’ s insertion to the distal phalanx may be more effectively desensitised by
administering local anaesthetic solution into the navicular bursa than by analgesia of the DIP
joint.12 Some of the lame horses in Dyson’s study 11 that responded to analgesia of the
navicular bursa, but were unresponsive to analgesia of the DIP joint, may have had lesions of
the insertion of the DDFT rather than disease of the navicular bone and its related structures.
Published in IVIS with the permission of BEPS Close this window to return to IVIS
Proceedings of the Belgian Equine Practitioners Society (BEPS) - 2015 - Leuven, Belgium

12
Ten mL mepivacaine HCl administered into the DIP joint may desensitise the entire sole, but
a smaller volume of mepivacaine (i.e. <6 mL) is unlikely to desensitise the heel portion of the
sole.10
Analgesia of the navicular bursa
Of the various techniques for inserting a needle into the navicular bursa showed that a method
described by Verschooten et al.13 is the most accurate. The foot can be held or placed in a
Hickman block using this method. A 20-gauge, 8.9-cm (3.5-inch), disposable, spinal needle is
inserted between the bulbs of the heel just proximal to the coronary band, and the needle is
advanced along a sagittal plane aiming for a point Verschooten termed “the navicular
position”. No matter the shape of the foot the navicular position is always in the same
location, 1 cm distal to the coronary band, midway between the dorsal and palmar limits of
the coronary band. The spinal needle is advanced toward the navicular position until the tip of
the needle contacts bone. At this time, a digital lateromedial radiograph can be taken to check
the position of the needle prior to injecting 3 to 4 mL of local anaesthetic solution. Injecting
the bursa can be facilitated by flexing the foot. Another method of determining success of the
procedure is to examine the foot radiographically immediately after injecting the bursa,
provided that 0.5 to 1.0 mL of radiopaque contrast medium was added to the local anaesthetic
solution.
Successful centesis of the bursa can also be determined ultrasonographically. For an
ultrasonographic view of the navicular bone, the frog is trimmed to pliable tissue, and soaked
in warm water for 30 to 120 minutes. The needle is advanced into the navicular bursa by
using Verschooten’s method of centesis13 and the position of the needle tip is determined
using a 7.5 MHz linear probe placed on the frog in a sagittal orientation. The needle is
properly placed when the tip of the needle is seen contacting the flexor surface of the
navicular bone. In the absence of imaging equipment, successful centesis of the bursa can be
assumed if the first 2-3 mLs of local anaesthetic solution is easily administered and then, as
pressure within the bursa increases as one to two more millilitres are administered,
administration becomes more difficult, resulting in refilling of the syringe with local
anaesthetic solution when pressure on the plunger is released. Bursal volume varies from 5
mL to greater than 10 mL depending on the presence of fibrosis of the bursa; the bursa may
rupture when a volume of solution between 6 and 10 mL is administered.
Published in IVIS with the permission of BEPS Close this window to return to IVIS
Proceedings of the Belgian Equine Practitioners Society (BEPS) - 2015 - Leuven, Belgium
13
A positive response to administration of local anaesthetic solution into the navicular bursa
indicates disease of the navicular bursa, the navicular bone, and/or its supporting ligaments,
solar toe pain,15 or disease of the distal portion of the DDFT.16 Even though analgesia of the
DIP joint results in analgesia of the navicular bursa,9 analgesia of the navicular bursa does not
result in analgesia of the DIP joint.14,15 Analgesia of the navicular bursa may help
todifferentiate pain associated with disease of the DIP joint from pain associated with disease
of the navicular bone and associated structures. Pain arising from the DIP joint can likely be
excluded as a cause of lameness when lameness is attenuated within 10 minutes by analgesia
of the navicular bursa.15
One possible explanation for the observation that analgesia of the DIP joint causes analgesia
of the navicular bursa but analgesia of the navicular bursa does not cause analgesia of the DIP
joint is that the site of direct contact between the palmar pouch of the DIP joint and the
palmar digital nerves is located proximal to the origin of the deep branches that innervate the
DIP joint and the navicular bursa, whereas the site of direct contact between the navicular
bursa and the palmar digital nerves is located distal to these branches.
In addition to experimental findings concerning the effect of analgesia of the navicular bursa,
clinical observations indicate that a positive response to intra-articular analgesia of the DIP
joint and a negative response to intra-bursal analgesia of the navicular bursa indicate pain
within the DIP joint as the cause of lameness.16 This clinical observation is valid if solar toe
pain can be eliminated with hoof testers as a cause of lameness.
The effect of time on interpretation of analgesia of the DIP joint or navicular bursa
Some clinicians have assumed that improvement in lameness observed within 10 minutes
after injecting the DIP joint with local anaesthetic solution indicates that lameness is caused
by pain in the DIP joint alone and that improvement observed more than 10 minutes after
injection is caused by diffusion of local anaesthetic solution into the navicular bursa or around
the nerves providing sensory innervation to the navicular bone and its associated
structures.14,17 This assumption appears to be invalid because a positive response to intra-
articular analgesia of the DIP joint has been observed to occur within 5 to 8 minutes of
injection in a majority of horses with navicular disease or experimentally-induced navicular
bursal pain.9,16
Published in IVIS with the permission of BEPS Close this window to return to IVIS
Proceedings of the Belgian Equine Practitioners Society (BEPS) - 2015 - Leuven, Belgium
14
Intra- articular and perineural analgesia of the proximal interphalangeal (PIP)
(pastern) joint
Approaches to the PIP joint have been reviewed18 and include dorsal, dorsolateral,
palmaroproximal, and palmarolateral approaches. Synovial fluid is frequently observed with
the palmaroproximal and palmarolateral approaches but is observed rarely using the other
approaches. Three of these approaches for arthrocentesis of the PIP joint were evaluated for
accuracy by Poore, et al.19 who found that students inexperienced in arthrocentesis of the PIP
joint were usually unsuccessful when performing these approaches.
A positive response to intra-articular analgesia of the pastern joint localises pain causing
lameness to that joint. Some horse lame because of in the pastern joint, however, do not
respond positively to intra-articular analgesia of the pastern joint when joint disease involves
subchondral bone.20 Because subchondral bone is innervated by nerves that enter the bone
marrow via the nutrient foramen, anaesthesia of nerves proximal to branches that enter the
nutrient foramen may be necessary to resolve subchondral bone pain and lameness. Because
the pastern joint is innervated by branches of the palmar digital nerves and their dorsal
branches, 4 an ASNB or BSNB nerve block resolves lameness caused by pain in the pastern
joint. Perineural anaesthesia of the palmar digital nerves and their dorsal branches at this
location should also anaesthetize these nerves proximal to the origin of the branches that enter
the nutrient foramen of the proximal phalanx and resolve lameness caused by subchondral
bone pain. Marked improvement in lameness of a horse with disease of the proximal
interphalangeal joint was observed when mepivacaine was infused through holes drilled into
the medullary cavity of both the first and second phalanges of the affected digit (Caldwell and
Schumacher, unpublished dataa).
Intra-articular analgesia of the metacarpo/metatarso phalangeal (MC/MT-P) (fetlock)
joint
Several techniques are described for intra-articular analgesia of the MC/MT-P joint. The
authors prefer the technique described by Misheff and Stover21 during which the limb is
positioned in partial flexion by holding the foot with one hand, while the needle is introduced
through the collateral sesamoidean ligament into the space between the articular surface of the
lateral sesamoid bone and the palmar aspect of the lateral metacarpal condyle. A volume of 7-
10 mL mepivacaine is administered.
Published in IVIS with the permission of BEPS Close this window to return to IVIS
Proceedings of the Belgian Equine Practitioners Society (BEPS) - 2015 - Leuven, Belgium
15
Although a positive response to intra-articular analgesia of the MC/MT-P joint localises
disease to that joint in most horses, not all lameness associated with an injury of the fetlock
joint resolves with intra-articular analgesia, and not all horses with lameness that improves
with intra-articular analgesia of this joint have disease of this joint. Whereas lameness caused
by intra-articular fragmentation, synovitis, capsulitis, and osteoarthritis improves or resolves
after intra-articular analgesia, lameness caused by injury of the subchondral bone or peri-
articular ligaments does not. Lameness caused by desmitis of the proximal portion of the
straight or an oblique distal sesamoidean ligament can improve after intra-articular analgesia
of the MC/MT-P joint.22
Analgesia of the digital flexor tendon sheath (DFTS)
Synoviocentesis of the DFTS can be performed by placing a 20- to 22-gauge needle into one
of the sheath’s several pouches. Access to these pouches is not difficult when the sheath is
distended with synovial fluid but is often difficult when it is not. A palmar axial sesamoidian
approach through the palmar/plantar annular ligament of the MC/MT-P joint is consistently
reliable for accurate synoviocentesis of the DFTS.23 Using this approach, the MC/MT-P joint
is flexed to a dorsal angle of 225o, the needle is placed through the skin at the level of the
midbody of the lateral proximal sesamoid bone, and then through the palmar annular
ligament, 3 mm axial to the palpable palmar border of the lateral proximal sesamoid bone,
immediately palmar to the palmar digital neurovascular bundle. The needle is inserted in a
transverse plane and advanced at an angle of 45o to the sagittal plane, aiming toward the
central intersesamoidean region, to a depth of 1.5 to 2.0 cm.
A basilar sesamoidian approach to the DFTS24 is likely to result in retrieval of synovial fluid
to verify accuracy. To perform the basilar sesamoidian approach the fetlock joint is held in a
slightly flexed position and the needle is inserted distal to the lateral proximal sesamoid bone
into a palpable depression created by the base of this bone and the lateral border of the
superficial flexor tendon. The needle is advanced at an angle of approximately 45° to the
transverse plane (in a lateromedial direction) and 45° to the dorsal plane (in a distoproximal
direction), to a depth of ≤ 1 cm. Seven-10 mL of local anaesthetic solution provides adequate
desensitization of the DFTS.
Published in IVIS with the permission of BEPS Close this window to return to IVIS
Proceedings of the Belgian Equine Practitioners Society (BEPS) - 2015 - Leuven, Belgium

16
A study demonstrated that pain induced in the toe and heel regions of the sole, pain associated
with synovitis of the DIP joint, and pain associated with synovitis of the navicular bursa were
not significantly attenuated by intrathecal analgesia of the DFTS.25 It is logical, therefore, to
assume that analgesia of the DFTS desensitises only structures that are contained within or
border on the sheath itself (i.e., the superficial and deep digital flexor tendons, the straight and
oblique distal sesamoidean ligaments, and the annular ligaments of the MC/MT-P and PIP
joints). It has been speculated that analgesia of DFTS may desensitise the portion of the
DDFT that lies within the foot.26 Leakage of local anaesthetic solution at the site of injection
or its diffusion from the DFTS, however, may desensitise skin of the heel region of the foot
from anaesthesia of the PDNs in some horses receiving intrasynovial analgesia of the DFTS
which may result in inadvertent desensitisation of the distal portion of the limb.27 The axial
and basilar sesamoidian approaches are less likely to result in leakage than are other
approaches to the DFTS. Skin sensitivity at the heel bulbs should be tested after intrasynovial
anaesthesia of the DFTS to determine if leakage of local anaesthetic solution at the injection
site has inadvertently anaesthetised a PDN.27
Diagnostic analgesia of the digital portion of the DDFT
An ASNB abolished or improved lameness localized to the foot in all of 46 horses found to
have a substantial abnormality in the digital portion of the DDFT using MRI.28 A PDNB,
analgesia of the DIP joint, or analgesia of the navicular bursa, however, each ameliorated
lameness of only about two-thirds of these horses.
Because lameness caused by disease of the DDFT within the foot may fail to improve
substantially after analgesia of the palmar digital nerves, the DIP joint, or the navicular bursa,
we believe that a portion of the DDFT within the foot and distal to the DFTS receives its
sensory supply from more proximal deep branches of the medial and lateral palmar digital
nerves that enter the DFTS. Improvement of lameness in horses with similar lesions of the
DDFT after intrathecal analgesia of the DFTS has been described.26
Performing intrathecal analgesia of the DFTS on horses with lameness that is unchanged after
anaesthesia of the palmar digital nerves but resolves after an ASNB, may be useful.
Resolution of lameness after intrathecal analgesia of the DFTS justifies suspicion of a lesion
within the digital portion of the DDFT or within structures contained within the DFTS.
Published in IVIS with the permission of BEPS Close this window to return to IVIS
Proceedings of the Belgian Equine Practitioners Society (BEPS) - 2015 - Leuven, Belgium
17
Anaesthesia of the hind foot compared to the forefoot
Innervation of the distal portion of the pelvic limb differs slightly from that of the thoracic
limb because the medial and lateral dorsal metatarsal nerves, which are branches of the deep
peroneal nerve, provide additional innervation to the digit and third metatarsal bone. In
addition, the medial plantar metatarsal nerve may also continue distally into the coronary
dermis. Because of this additional nerve supply to the distal portion of the pelvic limb, some
clinicians recommend that the dorsal metatarsal nerves, in addition to the plantar metatarsal
nerves, be anaesthetised when performing nerve blocks of the lower portion of the pelvic
limb. The authors and others29 believe, however, that most lameness involving the distal
portion of the pelvic limb can usually be evaluated without anesthetising the dorsal metatarsal
nerves.
Diagnostic analgesia of the collateral ligaments of the DIP joint
Lameness caused by disease of the collateral ligaments of the DIP joint often fails to improve
significantly after analgesia of the DIP joint itself.30 Only 24% of 30 horses with MRI
evidence of collateral ligament disease showed a significant improvement in lameness after
intra-articular analgesia of the DIP joint, and none of the horses improved after intra-bursal
analgesia of the navicular bursa. A PDNB, however, improved lameness significantly in 72%
of these horses, and all became sound after an ASNB. Consequently, when lameness is
abolished by a PDNB but not by analgesia of the DIP joint or navicular bursa, and no
radiographic abnormalities of the foot can be detected, collateral desmitis of the DIP joint
must be considered as a possible cause of lameness, as long as the presence of solar pain can
be eliminated with hoof testers.
Clinical impressions suggest that the degree of improvement in lameness associated with
injury to a collateral ligament after PDNB is determined by the extent of the injury and the
level at which the palmar digital nerve is anaesthetised. The further proximal the level of the
injury within the collateral ligament, the less likely that lameness is affected by analgesia of
the DIP joint or anaesthesia of the palmar digital nerves. This observation suggests that the
branches innervating the proximal aspect and origin of the collateral ligaments arise from the
palmar digital nerves proximal to the site where the palmar digital nerves lie alongside the
palmar pouch of the DIP joint or from the dorsal branches of the palmar digital nerve. A
pastern ring block or ASNB may be required to abolish lameness when osseous remodelling
is present at the origin of the collateral ligament at the level of the middle phalanx.
Published in IVIS with the permission of BEPS Close this window to return to IVIS
Proceedings of the Belgian Equine Practitioners Society (BEPS) - 2015 - Leuven, Belgium
18
a Caldwell, F.J. and Schumacher, J., 2015, Unpublished data, Auburn University, Auburn AL., USA
References
1. Easter JE, Watkins JP, Stephens SL, et coll. Effects of regional anaesthesia on experimentally induced coffin joint synovitis. Proc. Am. Ass. equine Practnrs. 2000;46:214-216.
2. Wyn-Jones G. Equine Lameness. Oxford, Blackwell Scientific Publications. 1988:1-22pp.
3. Beeman GM. The clinical diagnosis of lameness. Comp. cont. Educ. pract. Vet 1988;10:172-179.
4. Sack WO. Nerve distribution in the metacarpus and front digit of the horse. J. Am. vet med. Ass. 1975;167:298-335.
5. Paz CRF, Magalhães JF, Mendes HMF, et coll. Personal communication, March, 2015. 6. Schumacher J, Livesey L, DeGraves FJ, et coll. Effect of anaesthesia of the palmar digital
nerves on proximal interphalangeal joint pain. Equine vet J. 2004;36:409-414. 7. Bassage LH, Ross MW. Diagnostic analgesia, In: Diagnosis and Management of
Lameness in the Horse. Eds Ross MW and Dyson SJ. St. Louis, Elsevier Science. 2011:100-135.
8. Schumacher J, Schramme M, Schumacher J, et coll. Analgesia of the equine digit. Equine vet. Edu. 2013;25:408-421.
9. Pleasant RS, Moll HD, Ley WB, et coll. Intra-articular anaesthesia of the distal interphalangeal joint alleviates lameness associated with the navicular bursa in horses. Vet Surg. 1997;26:137-140.
10. Schumacher J, Schumacher J, DeGraves F, et coll. A comparison of the effects of two volumes of local analgesic solution in the distal interphalangeal joint of horses with lameness caused by solar toe or solar heel pain. Equine vet J. 2001;33:265-268.
11. Dyson S. Comparison of responses to analgesia of the navicular bursa and intraarticular analgesia of the distal interphalangeal joint in 102 horses. Proc. Am. Ass. equine Practnrs. 1995;41:234-239.
12. Schramme MC, Dyson S, Murray R, et coll. Soft tissue pathology in horses with navicular syndrome – MRI Results. Proceedings of the 1st World Orthopaedic Veterinary Congress, Munich. 2002:177pp.
13. Verschooten F, Desmet P, Peremans K, et coll. Navicular disease in the horse: the effect of controlled intrabursal corticoid injection. Errata. J. Equine vet Sci. 1991;11:8.
14. Dyson SJ. Lameness due to pain associated with the distal interphalangeal joint: 45 cases. Equine vet J. 1991;23:128-135.
15. Schumacher J, Schumacher J, Gillette R, et coll. The effects of local anaesthetic solution in the navicular bursa of horses with lameness caused by distal interphalangeal joint pain. Equine vet J. 2003;35:502-505.
16. Dyson SJ. The puzzle of distal interphalangeal joint pain. Equine vet Edu. 1998; 10:119-125.
Published in IVIS with the permission of BEPS Close this window to return to IVIS
Proceedings of the Belgian Equine Practitioners Society (BEPS) - 2015 - Leuven, Belgium
19
17. Gough MR. Diagnosis of palmar foot pain in the equine forelimb. In Pract. 1998; 20:358-366.
18. Schumacher J, Wilhite R. How to inject the synovial cavities of the digit, in Proc. Am. Ass. equine Practnrs. 2012;58:430-438.
19. Poore LAB, Lambert KL, Shaw DJ, et coll. Comparison of three methods of injecting the proximal interphalangeal joint in horses. Vet Rec 2011;168:302-305&308.
20. Dyson S. Problems associated with the interpretation of the results of regional and intra-articular anaesthesia in the horse. Vet Rec. 1986;118:419-422.
21. Misheff MM, Stover SM. A comparison of two techniques for arthrocentesis of the equine metacarpophalangeal joint. Equine Vet J. 1991;23:273-276.
22. Sampson SN, Schneider RK, Tucker RL, et coll. Magnetic resonance imaging features of oblique straight distal sesamoidian desmitis in 27 horses. Vet Radiol. Ultrasound 2007;48:303-311.
23. Hassel DM, Stover SM, Yarbrough TB, et coll. Palmar-plantar axial sesamoidean approach to the digital flexor tendon sheath in horses. J. Am. vet med. Ass. 2000; 217:1343-1347.
24. Rocconi RA, Sampson SN. Comparison of basilar and axial sesamoidian approaches for digital flexor tendon sheath synoviocentesis and injection in horses. J. Am. vet med Ass. 2013;243:869-873.
25. Harper J, Schumacher J, DeGraves F, et coll. Effects of analgesia of the digital flexor tendon sheath on pain originating in the sole, distal interphalangeal joint or navicular bursa of horses. Equine vet J. 2007;39:535-539.
26. Schneider RK. Magnetic resonance imaging (MRI). What have we learned? Proceedings of the American College of Veterinary Surgeons Symposium, ACVS, San Diego. 2002:75-76 pp.
27. Jordana M, Martens A, Duchateau L, et coll. Distal limb desensitisation following analgesia of the digital flexor tendon sheath in horses using four different techniques. Equine vet J. 2013;46:488-493.
28. Dyson SJ, Murray RC, Schramme M. et coll. Lameness in 46 horses associated with deep digital flexor tendonitis in the digit: diagnosis using magnetic resonance imaging. Equine vet J. 2003;5:681-690.
29. Carter GK, Hogan PM. Use of diagnostic nerve blocks in lameness evaluation. Proc. Am. Ass. equine Practnrs. 1996;42:26-32.
30. Dyson S, Murray R. Collateral desmitis of the distal interphalangeal joint in 62 horses (January 2001–December 2003). Proc. Am. Ass. equine Practnrs. 2004;50:248-256.
Published in IVIS with the permission of BEPS Close this window to return to IVIS
Proceedings of the Belgian Equine Practitioners Society (BEPS) - 2015 - Leuven, Belgium

DISTAL LIMB BLOCKSWhat do they really tell me?
DISTAL LIMB BLOCKSWhat do they really tell me?
Michael SchrammeDrMedVet, certEO, Phd, DipECVS, DipACVS
Professor Equine Surgery
University of Lyon
Accurate diagnosis
Prognosis Treatment
Regional Analgesia
Physical Examination
Diagnostic Imaging
LAMENESS
THE PUZZLE OF DISTAL LIMB LAMENESS
The Best Answers still come from Local Analgesia
Navicular Pain or Palmar Heel Pain?
Published in IVIS with the permission of BEPS Close this window to return to IVIS
Proceedings of the Belgian Equine Practitioners Society (BEPS) - 2015 - Leuven, Belgium

DIAGNOSIS OF FOOT LAMENESS
DIAGNOSIS OF FOOT LAMENESS
by integrating the differential response to1. Abaxial sesamoid nerve block2. Palmar digital nerve block 3. Coffin joint anesthesia4. Navicular bursa anesthesia5. Digital sheath anesthesia
Is it possible to localise pain in the foot accurately?
Diagnosis of Foot Lameness
• What we have been told… and have believed– Palmar Dig Nerve Block (PDNB)
• Only palmar 1/3 of foot– Including dorsal branches
• Entire foot– DIP joint = DIP joint– Bursa = Bursa
• THE END
Palmar Digital Nerve Block
Published in IVIS with the permission of BEPS Close this window to return to IVIS
Proceedings of the Belgian Equine Practitioners Society (BEPS) - 2015 - Leuven, Belgium
Palmar Digital Nerve Block
Palmar Digital Nerve Block
• Desensitises coffin joint synovitis!
PDNB
Time Preinjection
Postinjection
15 min 30 min 60 min
Lameness 0/4 3/4 0/4 - -
Palmar Digital Nerve Block
• The dorsal digital nerves do not innervate the joint capsule of the coffin joint.
Sack 1975
Cutaneous only
Published in IVIS with the permission of BEPS Close this window to return to IVIS
Proceedings of the Belgian Equine Practitioners Society (BEPS) - 2015 - Leuven, Belgium

Palmar Digital Nerve Block
• May desensitize the pastern joint!
PDNB
Time Pre injection
Post injection
1 cm 2 cm 3 cm
Lameness
<0/10>
<7/10>
<5/10>
<4/10*>
<4/10*>
Palmar Digital Nerve Block
• Deep branches of the PD nerves (3 & 5) to the PIP joint, arise at the level of the joint (Sack 1975).
PDNB
Published in IVIS with the permission of BEPS Close this window to return to IVIS
Proceedings of the Belgian Equine Practitioners Society (BEPS) - 2015 - Leuven, Belgium
Palmar Digital Nerve BlockFALSE NEGATIVE RESULTS
“A negative palmar digitalnerve block does not ruleout foot pain!”
Parkes and Dyson 2013
Palmar Digital Nerve BlockMinimizing proximal migration
• Insert close to margin of cartilage of the foot
• Point needle distally
• Use small amount of solution : 1 to 1 ½ mL
• Evaluate in 5-6 minutes
ASNB
Published in IVIS with the permission of BEPS Close this window to return to IVIS
Proceedings of the Belgian Equine Practitioners Society (BEPS) - 2015 - Leuven, Belgium
• Delayed onset of analgesia possible due to injection outside the perineural fascia.
= FALSE NEGATIVE
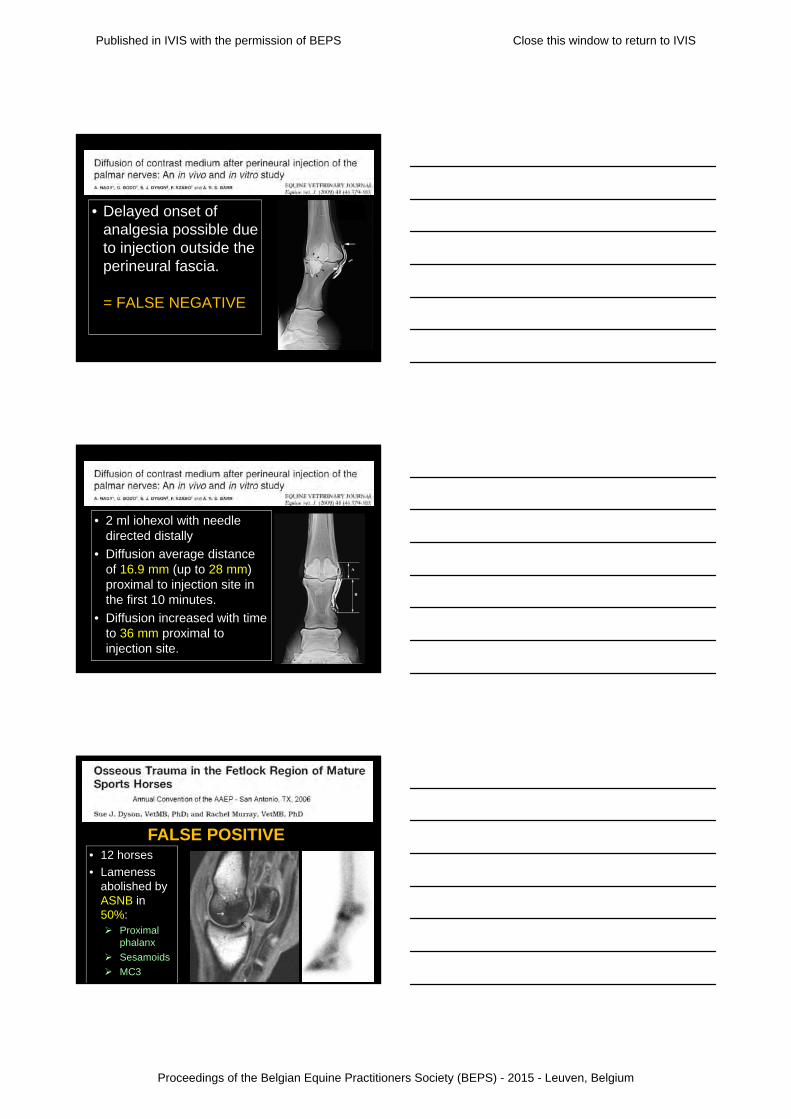
• 2 ml iohexol with needle directed distally
• Diffusion average distance of 16.9 mm (up to 28 mm) proximal to injection site in the first 10 minutes.
• Diffusion increased with time to 36 mm proximal to injection site.
• 12 horses
• Lameness abolished by ASNB in 50%: Proximal
phalanx
Sesamoids
MC3
FALSE POSITIVE
Published in IVIS with the permission of BEPS Close this window to return to IVIS
Proceedings of the Belgian Equine Practitioners Society (BEPS) - 2015 - Leuven, Belgium

• 8 horses
• Lameness abolished by ASNB in 86%
• None improved after PDNB.
FALSE POSITIVE
• Lameness improved > 80% or abolished by ASNB:
– 4 suspensory branch desmitis
– 1 sesamoiditis
– 1 metacarpophalangeal OA
– 1 osseous injury distal MC3
• 2/3 of branch injuries block to ASNB
– Dyson 2013
FALSE POSITIVE
PASTERN RING BLOCK (proximal palmar digital nerve block)
Published in IVIS with the permission of BEPS Close this window to return to IVIS
Proceedings of the Belgian Equine Practitioners Society (BEPS) - 2015 - Leuven, Belgium
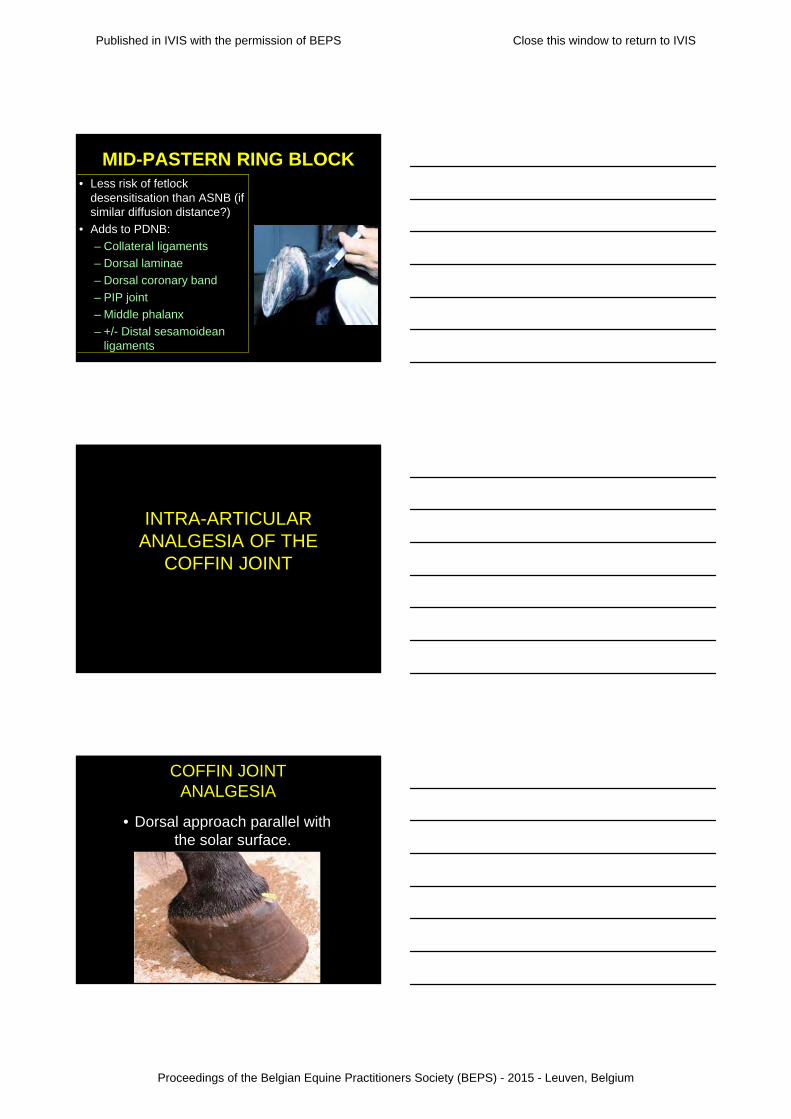
MID-PASTERN RING BLOCK• Less risk of fetlock
desensitisation than ASNB (if similar diffusion distance?)
• Adds to PDNB:
– Collateral ligaments
– Dorsal laminae
– Dorsal coronary band
– PIP joint
– Middle phalanx
– +/- Distal sesamoidean ligaments
INTRA-ARTICULAR ANALGESIA OF THE
COFFIN JOINT
COFFIN JOINT ANALGESIA
• Dorsal approach parallel with the solar surface.
Published in IVIS with the permission of BEPS Close this window to return to IVIS
Proceedings of the Belgian Equine Practitioners Society (BEPS) - 2015 - Leuven, Belgium
COFFIN JOINT ANALGESIA
5 cc results in desensitisation of:
• DIP joint (generally not collateral ligs)
• navicular bone
• navicular bursa
• toe region of the sole
• heel region of the sole, if 10 cc used
• distal DDF tendinitis
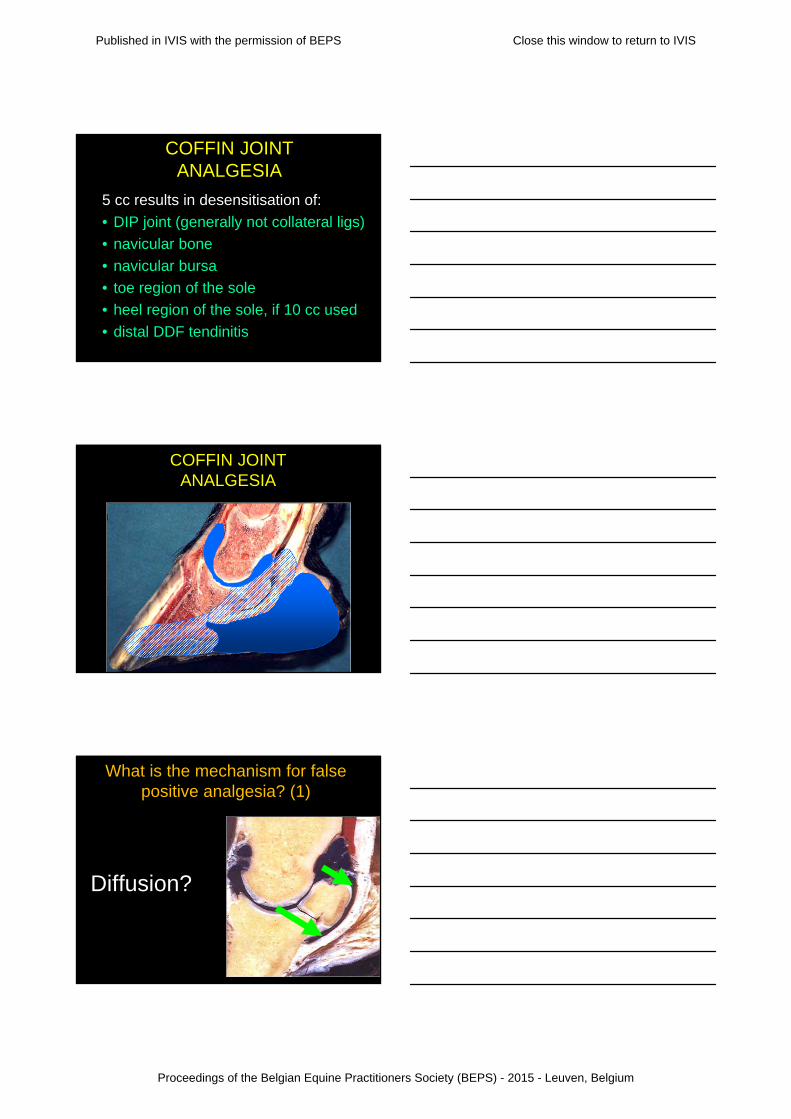
COFFIN JOINT ANALGESIA
What is the mechanism for false positive analgesia? (1)
Diffusion?
Published in IVIS with the permission of BEPS Close this window to return to IVIS
Proceedings of the Belgian Equine Practitioners Society (BEPS) - 2015 - Leuven, Belgium
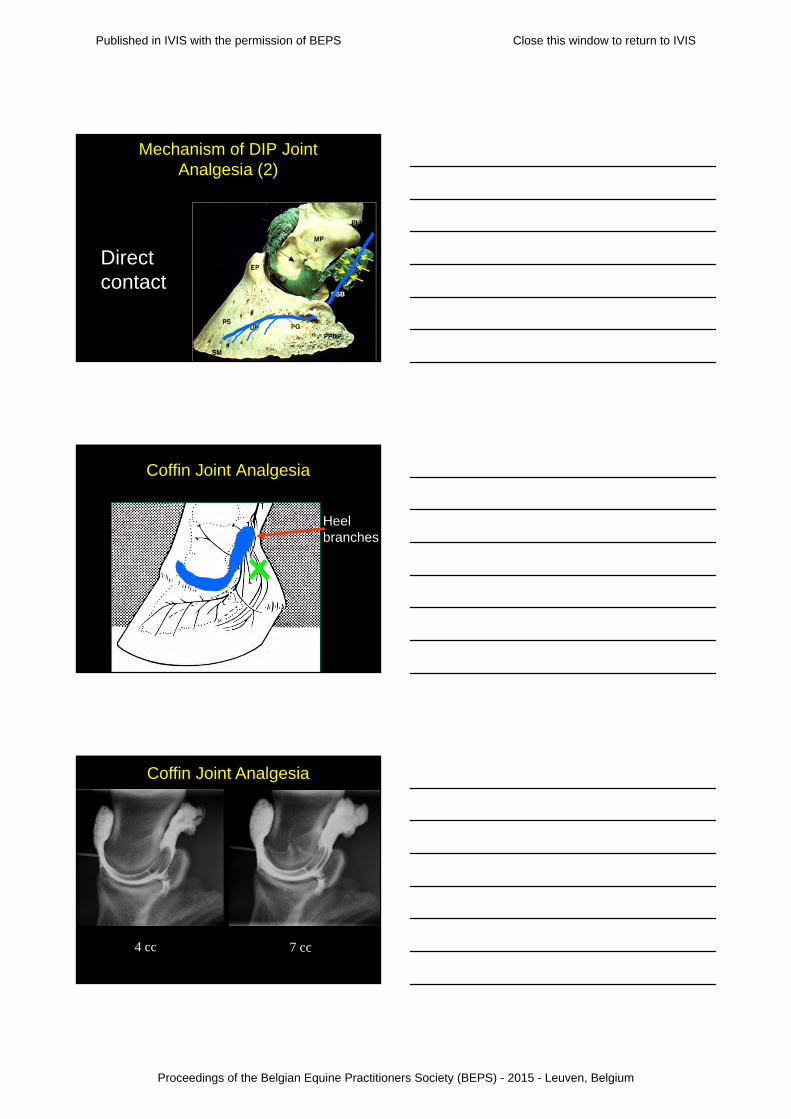
Mechanism of DIP Joint Analgesia (2)
Direct contact
Coffin Joint Analgesia
Heel branches
4 cc 7 cc
Coffin Joint Analgesia
Published in IVIS with the permission of BEPS Close this window to return to IVIS
Proceedings of the Belgian Equine Practitioners Society (BEPS) - 2015 - Leuven, Belgium
Coffin Joint Analgesia
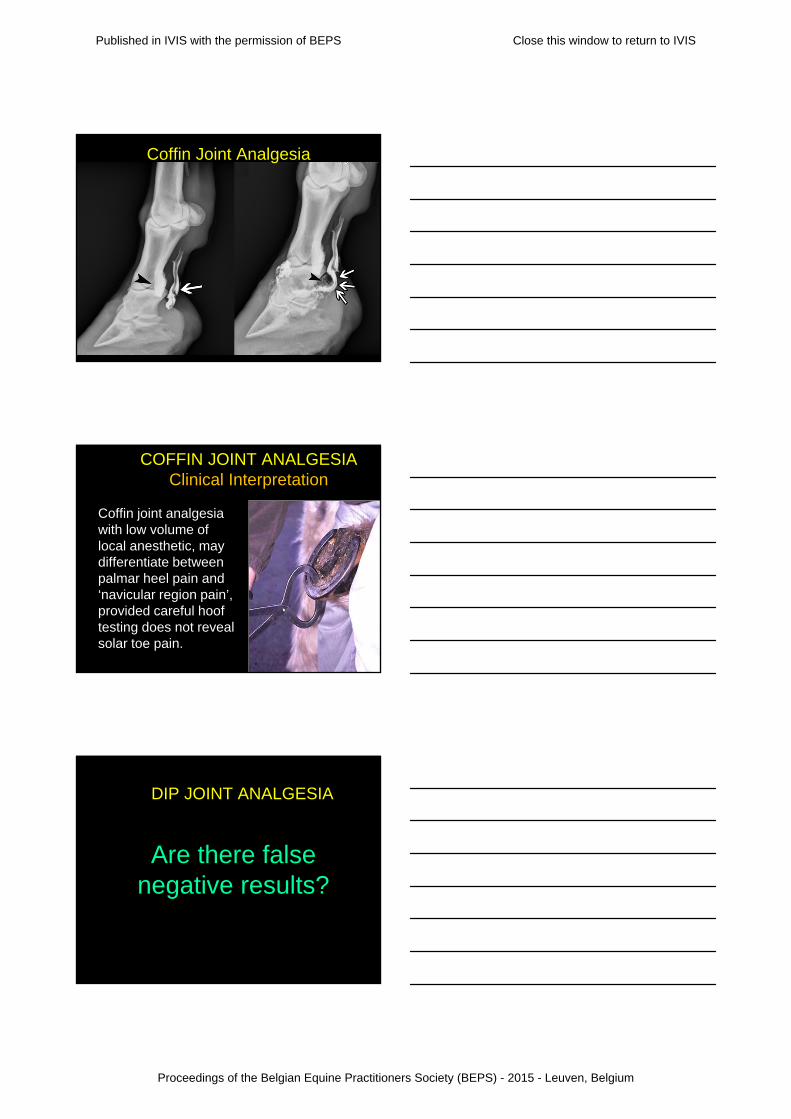
COFFIN JOINT ANALGESIAClinical Interpretation
Coffin joint analgesia with low volume of local anesthetic, may differentiate between palmar heel pain and ‘navicular region pain’,provided careful hoof testing does not reveal solar toe pain.
DIP JOINT ANALGESIA
Are there false negative results?
Published in IVIS with the permission of BEPS Close this window to return to IVIS
Proceedings of the Belgian Equine Practitioners Society (BEPS) - 2015 - Leuven, Belgium
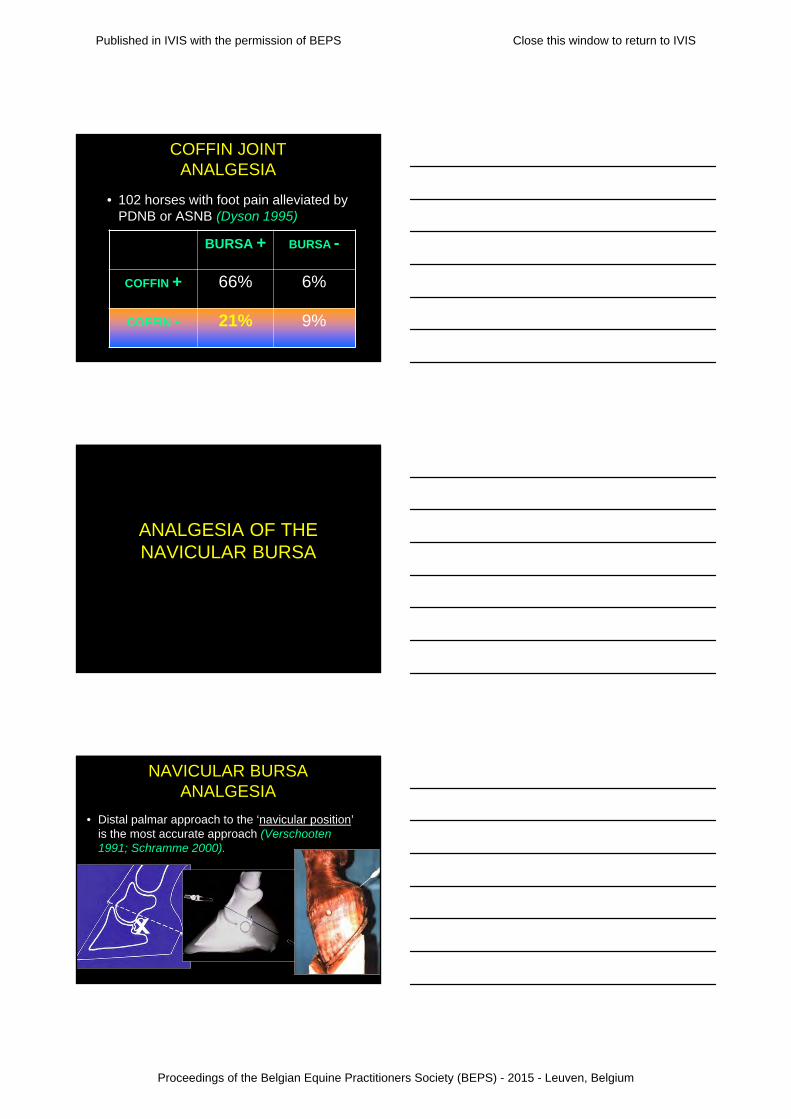
COFFIN JOINT ANALGESIA
• 102 horses with foot pain alleviated by PDNB or ASNB (Dyson 1995)
BURSA + BURSA -
COFFIN + 66% 6%
COFFIN - 21% 9%
ANALGESIA OF THE NAVICULAR BURSA
NAVICULAR BURSA ANALGESIA
• Distal palmar approach to the ‘navicular position’ is the most accurate approach (Verschooten 1991; Schramme 2000).
Published in IVIS with the permission of BEPS Close this window to return to IVIS
Proceedings of the Belgian Equine Practitioners Society (BEPS) - 2015 - Leuven, Belgium
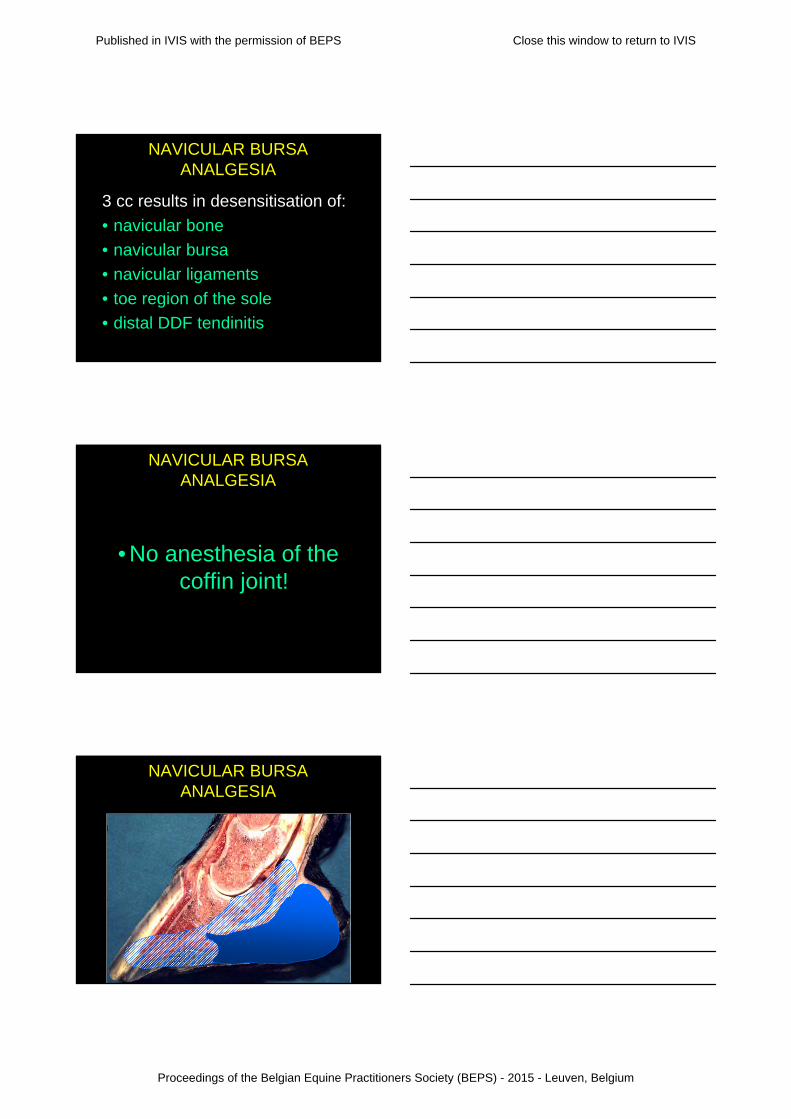
3 cc results in desensitisation of:
• navicular bone
• navicular bursa
• navicular ligaments
• toe region of the sole
• distal DDF tendinitis
NAVICULAR BURSA ANALGESIA
• No anesthesia of the coffin joint!
NAVICULAR BURSA ANALGESIA
NAVICULAR BURSA ANALGESIA
Published in IVIS with the permission of BEPS Close this window to return to IVIS
Proceedings of the Belgian Equine Practitioners Society (BEPS) - 2015 - Leuven, Belgium
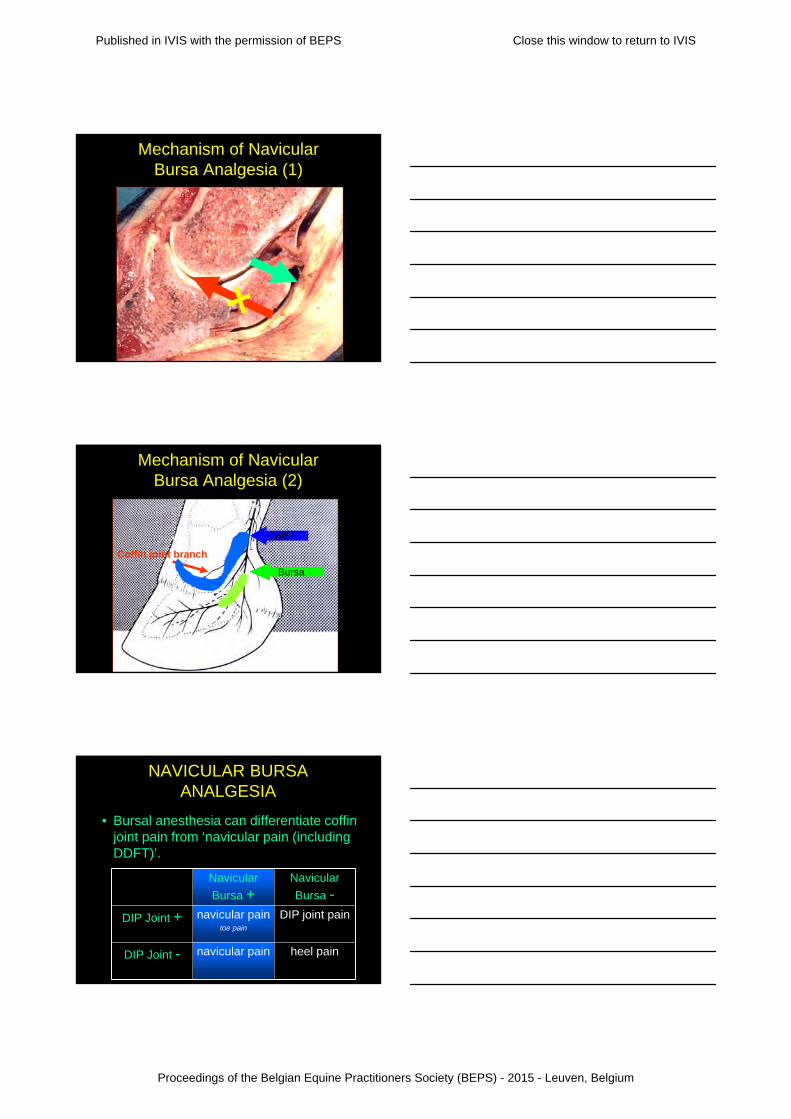
Mechanism of Navicular Bursa Analgesia (1)
Mechanism of Navicular Bursa Analgesia (2)
Coffin joint branch
Coffin
Bursa
NAVICULAR BURSA ANALGESIA
• Bursal anesthesia can differentiate coffin joint pain from ‘navicular pain (including DDFT)’.
Navicular
Bursa +Navicular
Bursa -
DIP Joint + navicular paintoe pain
DIP joint pain
DIP Joint - navicular pain heel pain
Published in IVIS with the permission of BEPS Close this window to return to IVIS
Proceedings of the Belgian Equine Practitioners Society (BEPS) - 2015 - Leuven, Belgium

NAVICULAR BURSA ANALGESIA
• Bursal anesthesia can differentiate coffin joint pain from ‘navicular pain (including DDF pain)’.
Dyson 1995105 horses
Navicular
Bursa +Navicular
Bursa -
DIP Joint + 66% 6%
DIP Joint - 21% 9%
REVIEW OF DIGITAL ANALGESIA
Low 4-point nerve block
Published in IVIS with the permission of BEPS Close this window to return to IVIS
Proceedings of the Belgian Equine Practitioners Society (BEPS) - 2015 - Leuven, Belgium
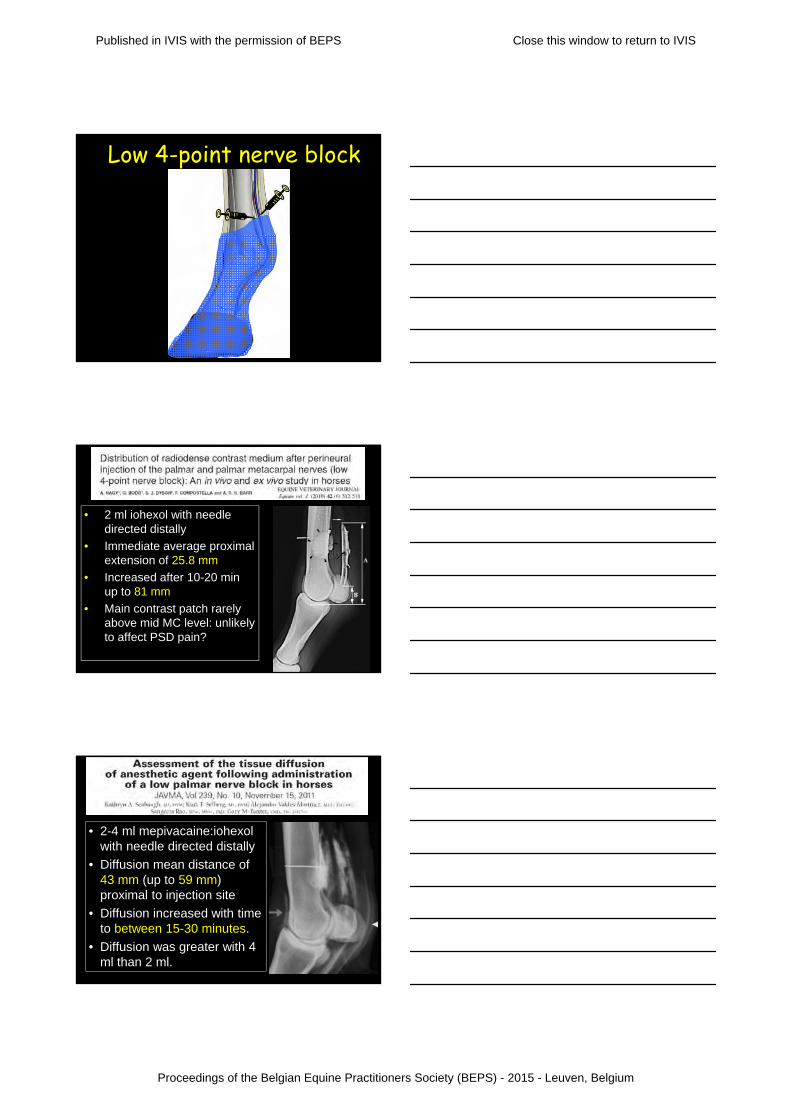
Low 4-point nerve block
• 2 ml iohexol with needle directed distally
• Immediate average proximal extension of 25.8 mm
• Increased after 10-20 min up to 81 mm
• Main contrast patch rarely above mid MC level: unlikely to affect PSD pain?
• 2-4 ml mepivacaine:iohexol with needle directed distally
• Diffusion mean distance of 43 mm (up to 59 mm) proximal to injection site
• Diffusion increased with time to between 15-30 minutes.
• Diffusion was greater with 4 ml than 2 ml.
Published in IVIS with the permission of BEPS Close this window to return to IVIS
Proceedings of the Belgian Equine Practitioners Society (BEPS) - 2015 - Leuven, Belgium
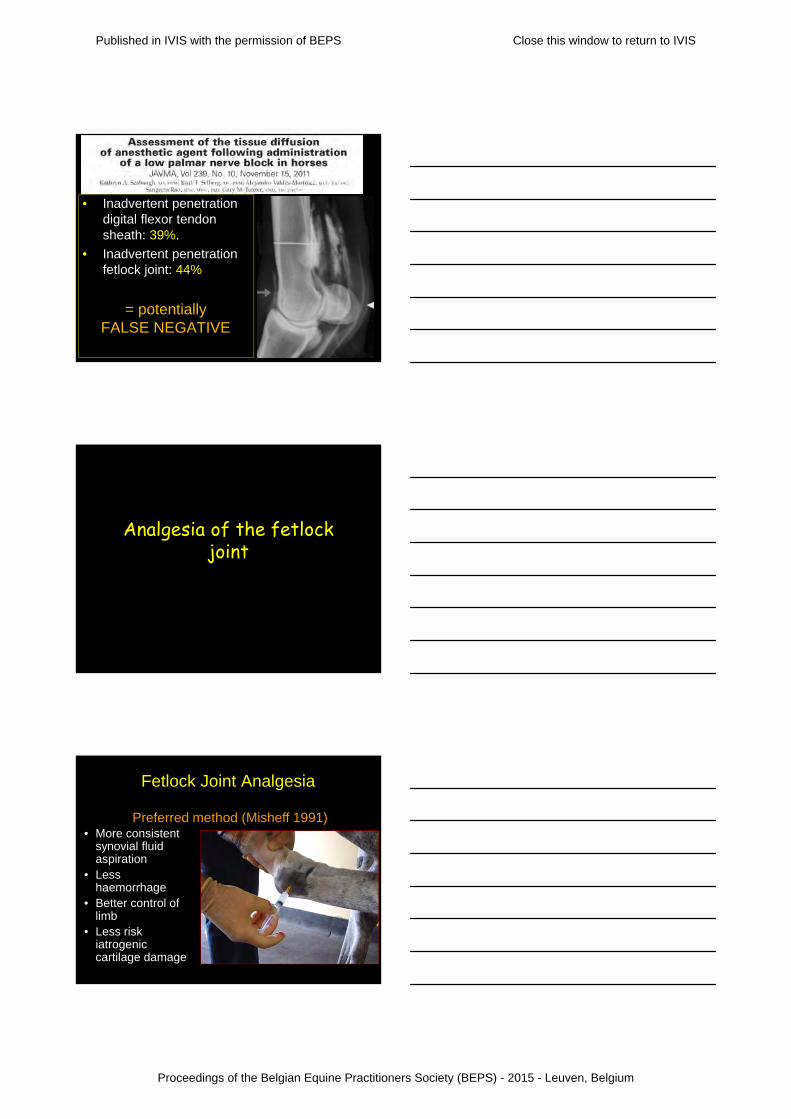
• Inadvertent penetration digital flexor tendon sheath: 39%.
• Inadvertent penetration fetlock joint: 44%
= potentially FALSE NEGATIVE
Analgesia of the fetlock joint
Fetlock Joint Analgesia
• More consistent synovial fluid aspiration
• Less haemorrhage
• Better control of limb
• Less risk iatrogenic cartilage damage
Preferred method (Misheff 1991)
Published in IVIS with the permission of BEPS Close this window to return to IVIS
Proceedings of the Belgian Equine Practitioners Society (BEPS) - 2015 - Leuven, Belgium
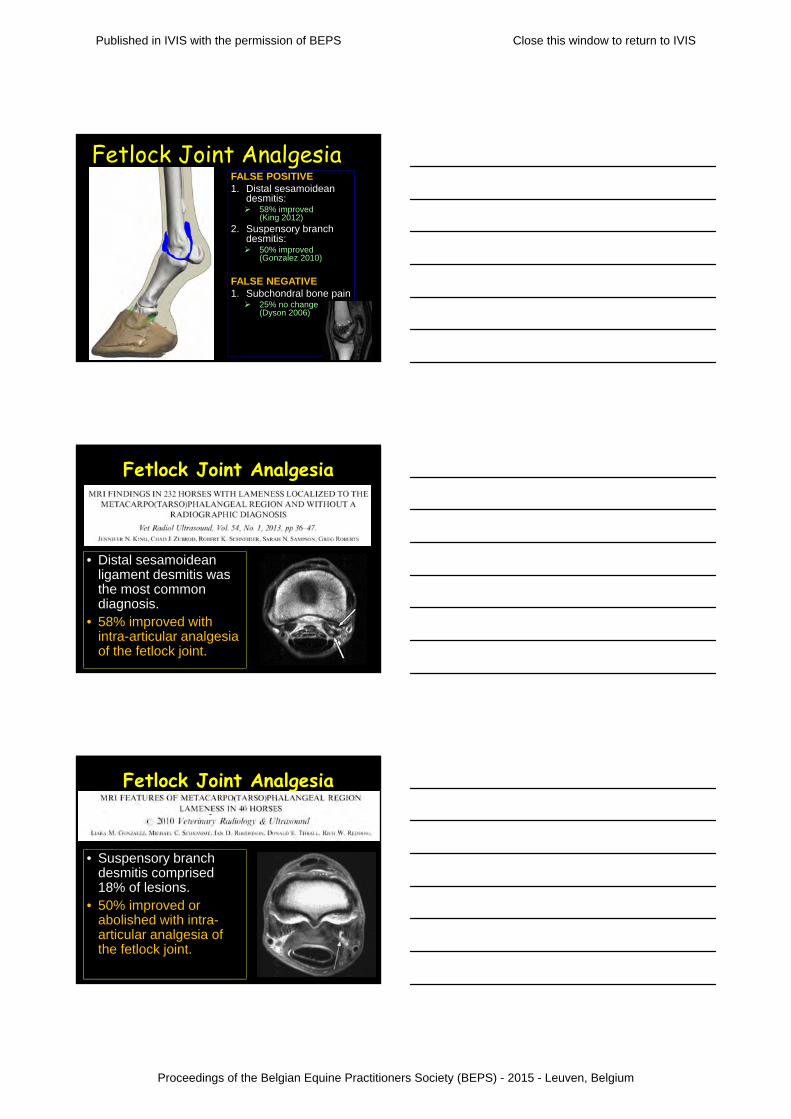
Fetlock Joint AnalgesiaFALSE POSITIVE1. Distal sesamoidean
desmitis: 58% improved
(King 2012)
2. Suspensory branch desmitis: 50% improved
(Gonzalez 2010)
FALSE NEGATIVE1. Subchondral bone pain 25% no change
(Dyson 2006)
Fetlock Joint Analgesia
• Distal sesamoidean ligament desmitis was the most common diagnosis.
• 58% improved with intra-articular analgesia of the fetlock joint.
Fetlock Joint Analgesia
• Suspensory branch desmitis comprised 18% of lesions.
• 50% improved or abolished with intra-articular analgesia of the fetlock joint.
Published in IVIS with the permission of BEPS Close this window to return to IVIS
Proceedings of the Belgian Equine Practitioners Society (BEPS) - 2015 - Leuven, Belgium
Fetlock Joint Analgesia
• 12 horses with subchondral bone injury of MC3 or P1.
• 25% did NOT improve with intra-articular analgesia of the fetlock joint.
Analgesia of the digital flexor tendon sheath
Published in IVIS with the permission of BEPS Close this window to return to IVIS
Proceedings of the Belgian Equine Practitioners Society (BEPS) - 2015 - Leuven, Belgium

ANALGESIA DIGITAL SHEATHPalmar/plantar Axial Sesamoidean Approach
• Needle is inserted through annular ligament of fetlock w/ limb flexed
• In transverse plane 3 mm axial to palmar/plantar border of proximal sesamoid bone
• Advanced ½ - ¾ in toward center of intersesamoidean region
• Synovial fluid can be aspirated consistently
Hassel et. al. JAVMA 217: 1343, 2000
• An 18-gauge, 3.8-cm needle was directed into the palpable depression at an angle of approximately 45° to the transverse plane and 45° to the dorsal plane, to a depth of 1 cm.
• Number of attempts at correct needle insertion were significantly lower than the axial technique.
• The basilar approach was 6 times more likely to result in synovial fluid aspiration
• An 18-20 gauge, 3.8-cm needle directed into the palpable depression at an angle of approximately 45°to the transverse plane and 45° to the dorsal
plane, to a depth of 1 cm.• The basilar approach was
6 times more likely to result in synovial fluid aspiration
Published in IVIS with the permission of BEPS Close this window to return to IVIS
Proceedings of the Belgian Equine Practitioners Society (BEPS) - 2015 - Leuven, Belgium

Analgesia of the Digital Sheath• Effects of analgesia of digital flexor
tendon sheath on pain in sole, coffin joint, or navicular bursa– No effect!– i.e., it does not block the palmar digital
nerve• Improvement of lameness in horses after
intrasynovial analgesia of the digital sheath is likely caused by attenuation of pain within the structures contained within the digital sheath.
Digital Flexor Tendon SheathANALGESIA DDFT?
Digital Flexor Tendon SheathFALSE POSITIVE1. Distal sesamoidean
desmitis: All horses
improved >70%(Sampson 2007)
2. DDF tendinopathy in the foot: Dyson 2013
FALSE NEGATIVE1. DDF tendinopathy
in the foot: Dyson 2013
Published in IVIS with the permission of BEPS Close this window to return to IVIS
Proceedings of the Belgian Equine Practitioners Society (BEPS) - 2015 - Leuven, Belgium

False positive Analgesia Digital Sheath through leakage of anesthetic?
Proximal Axial Basilar Distal
False positive Analgesia Digital Sheath?• At 30 minutes, 16% of limbs
had partial or complete desensitisation of the lateral heel bulb.
• Probability of loss of skin sensation was:– 4 x higher for proximal than
axial and base in forelimbs– 3 x higher for proximal than
axial and distal in hindlimbs
CONCLUSIONS
Published in IVIS with the permission of BEPS Close this window to return to IVIS
Proceedings of the Belgian Equine Practitioners Society (BEPS) - 2015 - Leuven, Belgium
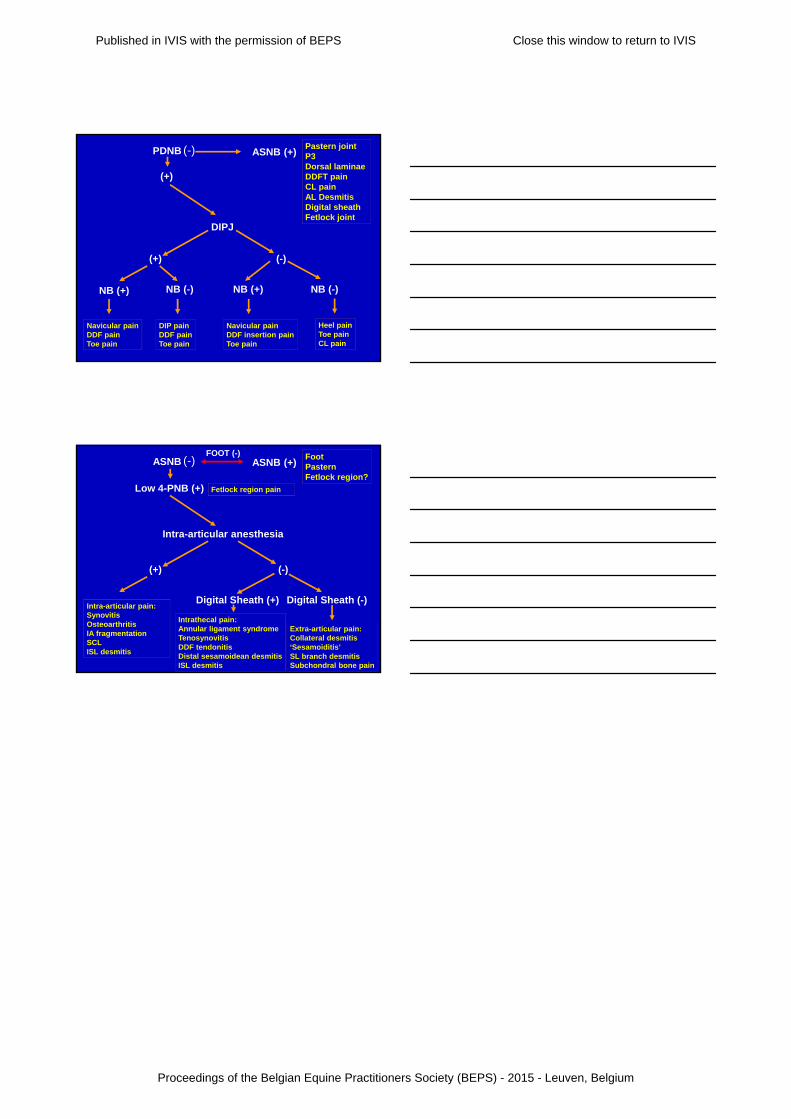
(+)
NB (+)
Navicular painDDF painToe pain
NB (-)
DIP painDDF painToe pain
(-)
Navicular painDDF insertion painToe pain
NB (+)
Heel painToe painCL pain
NB (-)
PDNB
DIPJ
(+)
ASNB (+)Pastern jointP3Dorsal laminae DDFT painCL painAL DesmitisDigital sheath Fetlock joint
(-)
(+)
Intra-articular pain:SynovitisOsteoarthritisIA fragmentationSCLISL desmitis
(-)
Intrathecal pain:Annular ligament syndromeTenosynovitisDDF tendonitisDistal sesamoidean desmitisISL desmitis
Extra-articular pain:Collateral desmitis‘Sesamoiditis’SL branch desmitisSubchondral bone pain
Digital Sheath (+) Digital Sheath (-)
Intra-articular anesthesia
Low 4-PNB (+)
ASNB (+)Foot PasternFetlock region?
(-)ASNB
Fetlock region pain
FOOT (-)
Published in IVIS with the permission of BEPS Close this window to return to IVIS
Proceedings of the Belgian Equine Practitioners Society (BEPS) - 2015 - Leuven, Belgium







