
Prescribing Cultures and PharmaceuticalPolicy in the Asia-Pacific
Medicines Access, Affordability, and Use:The Role of Health Insurance Systems
Anita WagnerDepartment of Population Medicine
WHO Collaborating Center in Pharmaceutical Policy
Harvard Medical School & Harvard Pilgrim Health Care [email protected]
23 September 2009

Infant mortality: 37/1,000<5 mortality: 39/1,000Maternal mortality: 72/100,000Life expectancy: 13 years less
Infant mortality: 11/1,000<5 mortality: 14/1,000Maternal mortality: 54/100,000Life expectancy: 13 years more
Equity in Access?

World Health Survey 2002
WHS 2002: % Households with 4-week HealthExpenditures >40% of Non-Food Items
0
5
10
15
20
25
30
35
40
Bangladesh China India Lao People'sDemocratic
Republic
Malaysia Myanmar Pakistan Philippines Viet Nam
% H
ouse
hold
s w
ith H
igh
Fina
ncia
l Hea
lth C
are
Bur
den
Many families are at risk of catastrophic health expenditures

World Health Survey 2002
Many Households Use Savings,Borrow, Sell Assets to Pay for Care
0
10
20
30
40
50
60
Bangladesh China India Lao People'sDemocratic
Republic
Malaysia Myanmar Nepal Pakistan Philippines Viet Nam
% H
ouse
hold
s w
ith U
ndes
irabl
e C
opin
g St
rate
gies
A pig must be taken to the market everytime an ambulance siren wails.
A year’s work is ruined as soon as yousleep in a hospital bed.
And if you are struck with a seriousillness, 10 years of savings go up insmoke.
Chinese Saying


World Health Survey 2002
For Many Households, All HealthCare Spending is on Medicines
0
10
20
30
40
50
60
70
80
Bangladesh China India LaoPeople's
DemocraticRepublic
Malaysia Myanmar Nepal Pakistan Philippines Sri Lanka Viet Nam% H
ouse
hold
s Sp
endi
ng 1
00%
of H
ealth
Car
e on
Med
icin
es

Quality Use?• Overuse/misuse
– China: <2% of prescriptions c/w clinical practice• Penicillin injections for rheumatoid arthritis• 70% of village prescriptions antibiotics• 98% of common colds with antibiotics• 50% of antibiotics prescriptions unnecessary
• Underuse– Chronic disease treatment
• Product quality– >15% of drugs sold worldwide are fakes, in parts of
Africa & Asia >50%

Pharmaceutical Policy ObjectivesCompete
Improving EquitableAccess
Available to the poor
Keeping CostsAffordable
To patient and to thehealth system
EncouragingAppropriate Use
Necessary, safe, effective,properly taken

taxe
s
Consumers Providerspayment
treatment
Government(MOH)
infor
mat
ionstandards, paym
entsoversight
support
standards,education
ProfessionalOrganizations
lobbyingConsumerOrganizations
lobbying
information
A Complex Network of Key Actorsin the Pharmaceutical Sector
DrugIndustry
standards
$$
lobbying$$
marketi
ng promotioninformationinformation HealthInsurance
payment payment,controls
productpayment

- Leverage for Change
• Need for value– Most health for $
• Defined population targets– Members– Providers
• Information through data– Need– Services– Costs
• Policy tools– Cost– Quality– Value
HealthInsurance
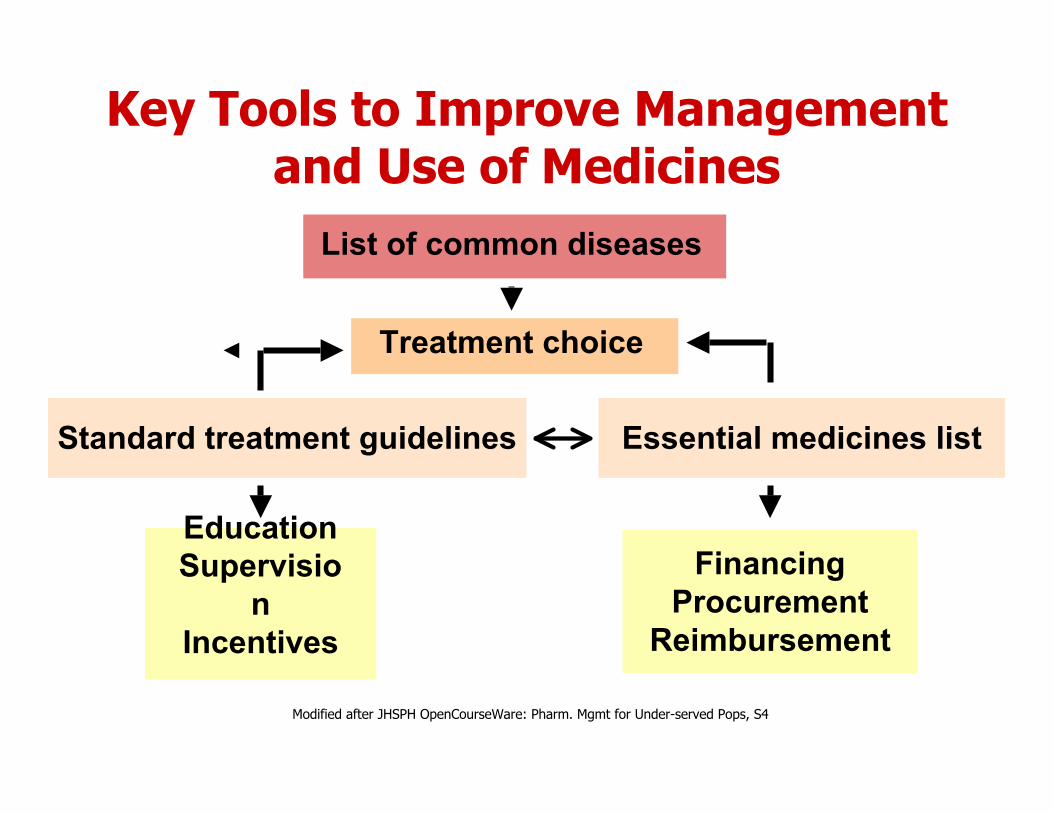
Modified after JHSPH OpenCourseWare: Pharm. Mgmt for Under-served Pops, S4
Key Tools to Improve Managementand Use of Medicines
List of common diseases
Standard treatment guidelines Essential medicines list
FinancingProcurement
Reimbursement
EducationSupervisio
nIncentives
Treatment choice

Pharmaceutical Policy Options
• Cost focused– “Active purchasing”
• Contracting with suppliers• Contracting with providers
– Formulary controls• Financial (cost-sharing) incentives to incentivize general or
specific drug use
• Quality focused– Utilization management
• Education via academic detailing, profiling, diseasemanagement, pay-for-performance
• Cost & Quality = Value focused– Low (no) cost-sharing for high value care
Kaiser Family Foundation 2008
ICIUM 2004
A Global Agenda forPolicy and Research inUse of Medicines
www.icium.org
History
• ICIUM 2004 (www.icium.org)– Improve access to and use of medicines– Need for sustainable system-level efforts
• Medicines and Insurance Coverage(MedIC) Initiative– Collaborative capacity building– Applied policy research & evaluation– Standard performance measures– Networking, experience, tools sharing
Capacity Building
Manila, 2007 Accra, 2008
Beijing, 2009

Collaborative Research

Health Insurance and Access to,Affordability, and Use of Medicines
• Huge need• Tremendous opportunities• Different approaches• Similar strategies
– Capacity building– Evidence generation– Policy implementation– Evaluation & monitoring

Additional Slides
Kaiser Family Foundation 2008
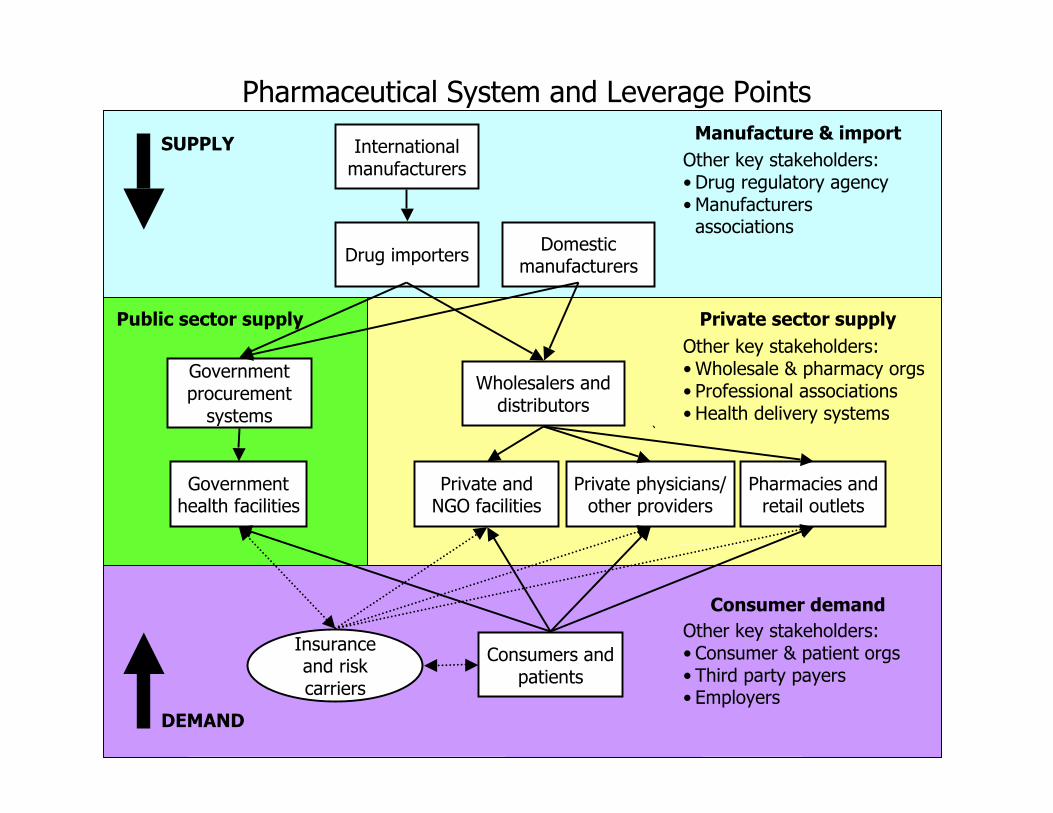
Internationalmanufacturers
Drug importers Domesticmanufacturers
SUPPLY Manufacture & importOther key stakeholders:• Drug regulatory agency• Manufacturers
associations
`
Wholesalers anddistributors
Private andNGO facilities
Private physicians/other providers
Pharmacies andretail outlets
Private sector supplyOther key stakeholders:• Wholesale & pharmacy orgs• Professional associations• Health delivery systems
Governmentprocurement
systems
Governmenthealth facilities
Public sector supply
Consumers andpatients
Insuranceand riskcarriers
Consumer demand
DEMAND
Other key stakeholders:• Consumer & patient orgs• Third party payers• Employers
Pharmaceutical System and Leverage Points

Kaiser Family Foundation 2008
Source: SSDS Inc for the World Bank
Complexity of Public SectorMedicines Supply in Kenya
Contra-ceptives and
RHequipment
STIDrugs
EssentialDrugs
Vaccinesand
Vitamin ATB/Leprosy
BloodSafety
Reagents(inc. HIV
tests)
DFI
D
KfW
UNICEF
JICA
GOK, WB/IDA
Source offunds for
commodities
CommodityType
(colour coded) MOHEquip-ment
Point of firstwarehousing KEMSA Central Warehouse
KEMSARegional
Depots
Organizationresponsible
for delivery todistrict levels
KEMSA and KEMSA Regional Depots (essential drugs, malaria drugs,
consumable supplies)
ProcurementAgent/Body
CrownAgents
Governmentof Kenya
GOK
GTZ(procurement
implementationunit)
JSI/DELIVER/KEMSA LogisticsManagement Unit (contraceptives,
condoms, STI kits, HIV test kits, TBdrugs, RH equipment etc)
EU
KfW
UNICEF
KEPI ColdStore
KEPI(vaccines
andvitamin A)
Malaria
USAID
USAID
UNFPA
EUROPA
Condomsfor STI/
HIV/AIDSprevention
CIDA
UNFPA
USGov
CDC
NPHLS store
MEDS(to Mission
facilities)
PrivateDrug
Source
GDF
Government
NGO/Private
Bilateral Donor
Multilateral Donor
World Bank Loan
Organization Key
JapanesePrivate
Company
WHO
GAVI
SIDA
NLTP(TB/
Leprosydrugs
Commodity Logistics System in Kenya (as of July 2006) Constructed and produced by Steve Kinzett, JSI/Kenya - please communicateany inaccuracies to [email protected] or telephone 2727210
Anti-RetroVirals
(ARVs)
Labor-atorysupp-
lies
GlobalFund forAIDS, TB
and Malaria
PSCMC(CrownAgents,GTZ, JSI
and KEMSA)
BTC
MEDS
DANIDA
Mainly District level staff: DPHO, DPHN, DTLP, DASCO, DPHO, etc or staff from the Health Centres,Dispensaries come up and collect from the District level
MEDS
Provincial andDistrictHospital
LaboratoryStaff
Organizationresponsible fordelivery to sub-district levels
KNCV
MSF
MSF
JSI/DELIVER
KEMSA
JSI
WHO
Increasing Need for Medicines:DM 2003 & 2025

Kaiser Family Foundation 2008
Source: WHO, World Health Survey, 2002
Average 4-week Medicine Expenditureswithin Household Expenditure Quintiles
$0
$10
$20
$30
$40
Ghana Coted'Ivoire
Senegal Morocco
Tunisia India
Pakistan Philippines
Med
icin
e E
xp
end
itu
res
in L
ast
4
Wee
ks b
y Q
uin
tile
s
Quintile 1 Quintile 2 Quintile 3 Quintile 4 Quintile 5
$88$153
Poor families cannot afford to pay for medicines

Source: National Health Accounts, 2004
OOP Expenditures Finance HealthCare in Low-Income Countries
852628721491High
8513169112Medium
910722823Low
Out-of-pocket (% of
private)
Socialsecurity
(% ofgovern-ment)
Private (%of total)
Govern-ment (%of total)
Per capita(US$)
Countryincome
level
Median Expenditures on Health in Asia Pacific Countries

Source: WHO World Health Survey, 2002
Most OOP Costs Spent onMedicines
15.65.218.225.948.475th percentile8.91.59.413.436.825th percentile
11.74.214.423.646.7Median8.95.021.927.237.0Vietnam
28.95.214.322.728.8Malaysia18.81.714.728.736.1Sri Lanka14.51.09.824.450.2Philippines
…
9.93.316.925.444.4India
8.71.025.943.121.3China13.65.08.16.367.1Bangladesh
OthersTraditionalOutpatientInpatientMedicines
Source: International Diabetes Federation
The Poor Pay Relatively More

Source: WHO-Health Action International Medicines Price Database
Medicines are Expensive in PrivateRetail Outlets in Many Countries
Median Low Price Generic = 3.4
Median Originator Brand = 12.2
35.8->
52.8->
42.6->
Source: WHO Country Pharmaceutical Indicators, 2006
Medicines Are Unaffordable toMany People in Poor Countries

Key Pharmaceutical Policy Questions
• How to select medicines for reimbursementfrom or in addition to an essentialmedicines list?
• How to manage a formulary process?• How to incentivize evidence-based
treatment according to standard treatmentguidelines?
• How to create basic information or combineinformation from multiple large scale datasources to track use and cost?

More targetedor tailored
More policy orsystems-oriented
Improved use of medicines
EconomicGive incentives, penalize, subsidize Differential generic/brand copayments Restrict reimbursement to essential drugs Pay for performance contracts
ManagerialGuide, systematize, facilitate
Treatment guidelines for providersConsumer price informationFeedback about generic prescribing
RegulatoryRegulate, prohibit, sanction
Provider standards and certification Mandatory generic substitution Fraud detection systems
EducationalInform, persuade, motivate
Educational outreach to practice groups Diabetes management groups for patients TV/radio educational spots
Improving Medicines Use







