
Plenary SessionFriday, October 17, 2014
8:30 to 10:00 AM
“Mental Health Promotion and Prevention in Primary Care:
An Idea Whose Time Has Come”Presentation by
William R. Beardslee, MDDepartment of Psychiatry
Boston Children’s Hospital and Harvard Medical School

Disclosure
William R. Beardslee, MD, has nothing to disclose. Dr. Beardslee receives NIMH funding, foundation
funding, and serves as a consultant to other research projects, governmental and
nongovernmental agencies.
“The child is the bearer of whatever the futureshall be … At this center … his incomparable tendernessto experience, his malleability, the almost unimaginable
nakedness and defenselessness of this wondrousfive-windowed nerve and core.”
James Agee, “Let Us Now Praise Famous Men”
“The pediatrician can regard the family as carrying the ‘chromosomes’ that perpetuate the culture and also form
the cornerstone of emotional development.”
Beardslee & Richmond. Mental Health of the Young: An Overview

“If you always do what you’ve always done, you’ll always get what you’ve always got.”
~ Albert Einstein
Health care reform must challenge existing paradigms and develop new
paradigms.
Envisioning the Future
What should a heath care system look like that fully meets the needs of families , incorporates prevention and treatment, and reflects cultural competence and cultural humility?
IOM 2009
7
Outline of Presentation 1. Institute of Medicine Prevention Report
2. Institute of Medicine Parental Depression Report
3. Preventive interventions focused on parental depression
4. Policy – Expansion of Medicaid and the ACA. An opportunity for treatment for depressed mothers
5. Practical and Policy Implications
Prevention of Mental Illness
Family-centered care Prevention of mental illness and problem
behavior Population level impact

The Triple Aims of the ACA
Improving the experience of care
Improving the health of populations
Reducing costs

The Committee
33

Preventive OpportunitiesEarly in Life
Early onset (¾ of adult disorders had onset by age 24; ½ by age 14)
First symptoms occur 2-4 years prior to diagnosable disorder
Common risk factors for multiple problems and disorders
12
Mental Health PromotionAims to:
Enhance individuals’– ability to achieve developmentally
appropriate tasks (developmental competence)
– positive sense of self-esteem, mastery, well-being, and social inclusion
Strengthen their ability to cope with adversity
13
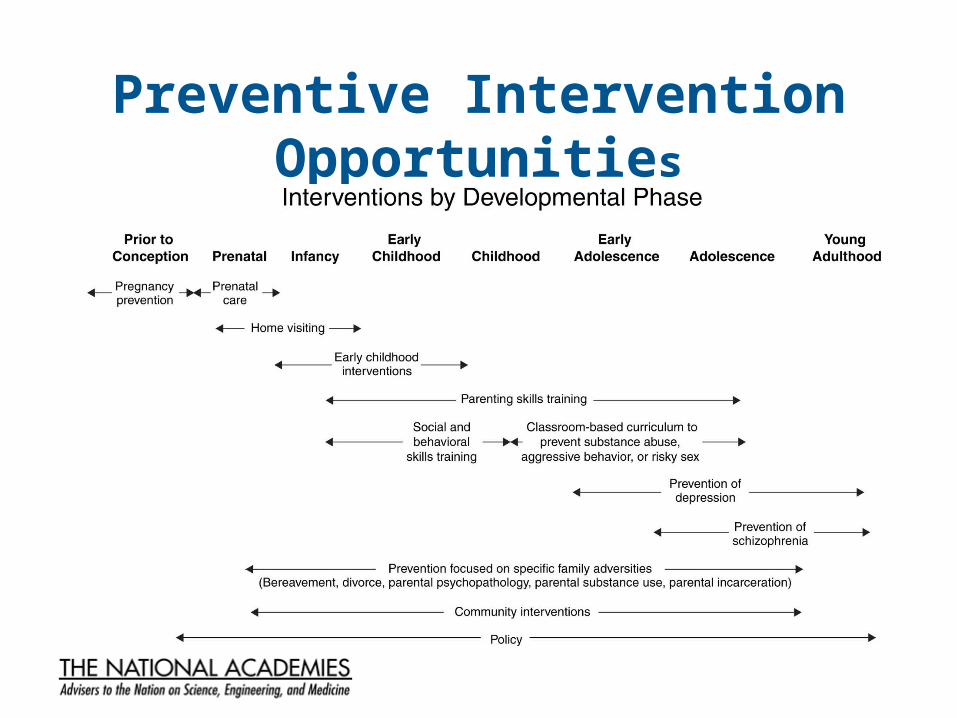
Preventive Intervention Opportunities
14
Implementation Strong across the board evidence for family-
based prevention strategies
Need to move from efficacy toward effectiveness trials
Implementation research has highlighted:– complexity– important role of community
Cultural humility and cultural and linguistic competence are essential for implementation

Recommendation Themes
Putting Knowledge into Practice
Continuing Course of Rigorous Research
16
A Central Theme
“The scientific foundation has been created for the nation to begin to create a society in which young people arrive at adulthood with the skills, interests, assets, and health habits needed to live healthy, happy, and productive lives in caring relationships with others.”

“One factor lurks in the background of every discussion of the risks for mental, emotional, and
behavioral disorders and antisocial behavior: poverty ... Although not the focus of this report,
there is evidence that changes in social policy that reduce exposure to these risks are at least as
important for preventing mental, emotional and behavioral disorders in young people as other
preventive interventions. We are persuaded that the future mental health of the nation depends
crucially on how, collectively, the costly legacy of poverty is dealt with.”

Risks for DepressionSpecific: Extensive family
history of depression, especially parents
Prior history of depression
Depressogenic cognitive style
Bereavement
General (Risks for many disorders)
Exposure to trauma Poverty Social isolation Job loss Unemployment Family breakup Loss of community Dislocation /
immigration Historical trauma

A series of recent meta-analyses demonstrate that in both adults and
children, a significant number of episodes of major depression
can be prevented.

Treatment: Current Evidence• A variety of safe and effective strategies exist for treating adults
with elevated symptoms or major depression, including:– cognitive behavioral– interpersonal therapy– medication
• A variety of strategies to deliver these treatments exist in a wide range of settings
• Almost no studies report whether the adults treated are parents or whether treatment affects children
Treatment: Current Evidence, continued.• Individuals should have informed choices in treatment “tools”
that are available to them
• Treatment tools and strategies to deliver these treatments should be – flexible, – efficient,– inexpensive, and above all – acceptable to the participants
in a wide variety of community and clinical settings
Preventive InterventionsPromising preventive intervention strategies exist. They include, for the most part:
• Treating the parents• Providing help with parenting• Using a two-generational approach
Some also directly involve children.
Depression Prevention Examples: IOM Report
1. Family Talk - Beardslee, et al., 20092. Prevention of depression - Garber, et al.,
2009 –moderated by acute parental depression
3. Parent/Child Coping Session - Compas et al., in press.
4. Mothers’ and babies’ program - Munoz
IOM 2009 24
Across both reports and in a variety of different risk situations, very strong
evidence exists for the valueof parenting programs.
25
Special Opportunities and Challenges
1. Developing systems that can give two-generational responses to parental depression
2. Responding to the needs of vulnerable populations, especially low income, culturally and ethnically diverse families
3. Responding to families experiencing depression along with other comorbidities in family adversities
4. Developing complex interventions that build on collaborative integrative and comprehensive service models

Core Challenges Lack of a home for prevention. It is not owned by any
one professional discipline.
Lack of a trained workforce
Lack of infrastructure to support the introduction of new programs
Lack of a payment system
Historically, a lack of attention to prevention as opposed to treatment

Family Talk Component Studies
1979 - 1985: Risk Assessment - Children of Parents with Mood Disorders
1983 - 1987: Resiliency Studies and Intervention Development
1989 - 1991: Pilot Comparison of Public Health Interventions
1991 - 2000: Randomized Trial Comparing Psychoeducational Family Interventions for Depression
1997 - 1999: Family CORE in Dorchester
1998: Narrative Reconstruction
2000: Efficacy to Effectiveness – Countrywide programs in Finland and at least five other places; Project
FOCUS with the Navy; Family Connections

Characteristics of Resilient Youth
Activities - Intense Involvement in Age Appropriate Developmental Challenges - in School, Work, Community, Religion, and Culture
Relationships - Deep Commitment to Interpersonal Relationships - Family, Peers, and Adults Outside the Family
Self-Understanding - Self-Reflection and Understanding in Action
Resilience in Parents Commitment to parenting
Openness to self-reflection
Commitment to family connections and growth of shared understanding
Seven modules1. Taking a history2. Psychoeducation and the family’s
story3. Seeing the children4. Planning the family meeting5. Holding the family meeting6. One week follow-up, check-in7. Long-term follow-up
Three Randomized Trials of Family Talk
High rankings - 3.5 out of a possible 4.0 in the National Registry of Evidence-based Programs and Practices for strength of evidence, SAMHSA.

Six Principles for a Successful Family Meeting
1. Pay attention to the timing of the meeting.
2. Gain commitment to the process from the entire family.
3. Begin by identifying specific major concerns and addressing them.
4. Bring together and reknit the family history.
5. Plan to talk more than once.
6. Draw on all the available resources to get through depression.
Narrative Project for FamiliesWho Sustained Changes – Self-Reflection Over
Time
1. The emergence of the healer within2. The need to understand depression
anew across development• Children’s growth• Vicissitudes of parental illness
Effective Family Programme I – Dr. Tytti Solantaus, Finland
Plan from the beginning to change child mental health system from a diagnosis and treatment system to a health promotive and prevention system.
A ten-year effort to locate services for parents struggling with adversity in all mental health and health clinics.
Effective Family Programme II – Dr. Tytti Solantaus, Finland
A family of interventions
A master trainer strategy
Adaptation of the approach to many different parental adversities
Latino Team
Latino Adaptation Familismo
Allocentric orientation
Kinds of separation in immigrant families
Differing involvement of parents and children in the mainstream culture
Immigration narrative
What helps parents cope with depression?
Focus on the children Visualizations. Envisioning a better future Prayer, songs, religion, church community, spiritual healing Support groups Helping others, sharing information Focusing in the present: “viviendo de dia a dia” (living day to day) Not giving up: “seguir la lucha” Alternative medicine Humor: “al mal tiempo buena cara” “yo no lloro, yo me rio”
Web-based training in Family Talk available at www.fampod.org.
The Family Connections program is available at www.childrenshospital.org/familyconnections.

FAMpod Home Page
http://fampod.org


FAMpod Collaborations

Olivia Golden, Amelia Hawkins, Tracy Vericker, Jennifer Macomber, Embry Howell, William Beardslee, and others.
three-year project best ways to help depressed low income women with young children
subsequent two-year project working with federal policymakers best possible entry points through which to help young children.
The focus on maternal depression was chosen because it is widespread among low income mothers, there is strong clinical evidence about effective treatment, and yet very few low income mothers, even those severely depressed, receive treatment.
Urban Institute Project

Expanded continuous coverage for low income women
Mandated coverage of preventative services including depression screening
Integrated care initiatives
ACA Opportunities
Reduced depression can increase employment
Early treatment can avoid more serious depressive episodes
Treating a mother’s depression can reduce child physical and mental health problems
Expanded Treatment under Medicaid Could be Cost-neutral or Cost-saving

Accountable Care Organizations
Patient-Centered Medical Homes
Health Homes
Medicaid Managed Care◦ Carve in◦ Carve out
Emerging Integrated Care Initiatives

Practical Implications Parental depression is prevalent in family
practice. Parental depression is treated when
recognized and can have a multiplier positive affect on the family when recognized and treated.
Available evidence confirms that we should both treat parents and ask them about how their kids are doing and support their parenting.

Practical Tips I Screening and referral are useful when
available referral sources have been identified.
PHQ-2 is a good initial screener when followed with the PHQ-9.
Attention to the system in which primary care occurs and its ability to deal effectively with depressed parents are as important as any particular intervention.

Practical Tips II Working with parents who are depressed
as parents first is essential. Elicit the parents’ concerns both about
himself/herself and about the children. Brief parenting interventions and referral
of children for evaluation are also helpful. Follow-up is essential.

Practical Tips III Attention to the family narrative and what
has been disrupted is important in helping the family get back on track in re-establishing rituals and having regular conversations.
A primary care physician is in the best position to provide family-centered preventive care for depression and to facilitate treatment.
Key Ongoing Themesfrom IOM Work
Major depression can be prevented
How to ameliorate the effects of poverty
Encouragement of nurturing environments
How to incorporate family prevention perspectives under the ACA
53
IOM Forum on Promoting Children’s Cognitive, Affective
and Behavioral HealthA focus on implementation and disseminationof health promotion and prevention strategies.
The first forum dealt with effectiveparenting interventions.
Co-chairs:
Dr. C. Hendricks BrownDr. William R. Beardslee
54

http://www.iom.edu/Reports/2014/Strategies-for-Scaling-Effective-Family-Focused-Preventive-Interventions.aspx
Key Research Issues for the Future
Poverty. What degree of interventions in what sectors is necessary to significantly change outcomes?
What are the best policy payment and clinical strategies for family-based mental health prevention in primary care?
How can systems both make enduring improvements and deal with the enormous pace of change and regulation?
Initiative fatigue?
56

Key Research Issues for the Future
(continued) International research - What characterizes
countries that invest heavily in young children and their parents. What can we learn that helps us make the same investments in this country.
How does one address and achieve scientific equity in the study of vulnerable populations?
57
Thank You … For more information, please contact:
Materials for Head Start parents and teachers about resilience and depression available at www.childrenshospital.org/familyconnections
Web-based training in Family Talk and other resources available at www.fampod.org
Perry DF, Miranda J, Ammerman RT, and Beardslee WR. Depression in mothers: More Than the Blues – A Toolkit for Family Service Providers. 2014, Washington, DC. Substance Abuse and Mental Health Services Administration. [On-line] http://store.samhsa.gov/product/SMA14-4878
References 1. Beardslee WR. When a parent is depressed: How to protect
your children from the effects of depression in the family. Originally published in hardcover under the title, Out of the darkened room: When a parent is depressed: Protecting the children and strengthening the family, by Little, Brown and Company, 2002. First paperback edition, 2003.
2. Beardslee WR. Commitment and Endurance: Common themes in the life histories of civil rights workers who stayed. Am J Orthopsychiatry, 1983, 53(1), 34-42.
References (continued)3. Beardslee WR, Ayoub C, Avery MW, Watts CI, and O’Carroll KL.
Family Connections: An approach for strengthening early care systems in facing depression and adversity. Am J Orthopsychiatry. 2010, 80(4), 482-95.
4. Beardslee WR, Brent DA, Weersing VR, Clarke GN, Porta G, Hollon SD, Gladstone TRG, Gallop R, Lynch FL, Iyengar S, DeBar L, and Garber J. Prevention of depression in at-risk adolescents: Longer-term effects. JAMA Psychiatry, 2013, 70(11), 1161-1170. doi: 10.1001/jamapsychiatry.2013.295. Available on-line in PubMed PMCID: PMC 3978119.

References (continued)5. Beardslee WR, Solantaus TS, Morgan BS, Gladstone TR, and
Kowalenko NM. Preventive interventions for children of parents with depression: International perspectives. MJA, 2012, Open 1 Suppl 1, 23-27.
6. Beardslee WR, Gladstone TRG, and O’Connor E. Transmission and prevention of mood disorders among children of affectively ill parents: A review. JAACAP, 2011, 50, 1098-1109. {On-line] www.jaacap.org.
7. Beardslee WR, Lester P, Klosinski L, Saltzman W, Woodward K, Nash W, Mogil C, Koffman R, and Leskin G. Family-centered preventive intervention for military families: Implications for implementation science. Prev Sci, 2011. DOI: 10.1007/s11121-011-0234-S. [On-line] Open source publication: http://www.springerlink.com/content/8265h1k18u4x77nr/fulltext.pdf

References (continued)8. Berwick DM, Nolan TW, and Whittington J. The triple aim:
Care, health, and cost. Health Affairs, 2008, 27(3), 759-769. doi: 10.1377/hlthaff.27.3.759. [on-line] http://content.healthaffairs.org/content/27/3/759.fuull.html.
9. Biglan A, Flay BR, Embry DD, and Sandler IN. The critical role of nurturing environments for promoting human well-being. Am Psychol. 2012. 257-271.
10. Cuijpers P, Beckman ATF and Reynolds III C. Preventing Depression: A Global Priority. JAMA, 2012, 1033-1034.
11. Cuijpers P, von Straten A, Smit F, Miahlopoulos C, and Beckman A. Preventing the onset of depressive disorders: a meta-analytic review of psychological interventions. Am J Psychiatry, 2008, 165(10), 1271-80.
References (continued)12. Garber J, Clarke GN, Weersing VR, Beardslee WR, Brent DA,
Gladstone TRG, DeBar LL, Lynch FL, D’Angelo E, Hollon SD, Shamseddeen W, and Iyengar S. Prevention of depression in at-risk adolescents: A randomized controlled trial. JAMA, 2009, 301(21), 2215-2224. [On-line] http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=2737625.
13. Golden O, Hawkins A, and Beardslee WR. Home visiting and maternal depression: Seizing the opportunities to help mothers and young children. Urban Institute. 2011.

References (continued)14. Howell E, Golden O, and Beardslee W. Emerging opportunities for
addressing maternal depression under Medicaid. Urban Institute. 2013 [On-line] http://www.urban.org.
15. Merry SN, Herrick SE, Cox GR, Brudevole-Iversen T, Bir JJ, McDowell H. Psychological and educational interventions for preventing depression in children and adolescents. Cochrane Database of Systematic Reviews 2011, Issue 12. Art. No.: CD003380. DOI: 10.1002/14651858.CD003380.pub3.
16. Munoz RF, Beardslee WR, and Leykin Y. Major depression can be prevented. Am Psychol. 2012. 67(4). 285-295.
17.
References (continued)17. National Research Council and Institute of Medicine. Preventing
Mental, Emotional, and Behavioral Disorders Among Young People: Progress and Possibilities. Committee on Prevention of Mental Disorders and Substance Abuse Among Children, Youth, and Young Adults: Research Advances and Promising Interventions. Mary Ellen O’Connell, Thomas Boat, and Kenneth E. Warner, Editors. Board on Children, Youth, and Families, Division of Behavioral and Social Sciences and Education. Washington, DC: The National Academies Press. 2009. [On line] http://www.nap.edu/catalog.php?record_id=12480.
18. National Research Council and Institute of Medicine. Depression in parents, parenting and children: Opportunities to improve identification, treatment, and prevention efforts. Washington, DC: The National Academies Press. 2009. [On line] http://www.nap.edu/catalog.php?record_id=12565.
References (continued)19. Perrino T, Beardslee W, Bernal G, Brincks A, Cruden G, Howe G,
Murry V, Pantin H, Prado G, Sandler I, and Hendricks Brown C. Towards scientific equity for the prevention of depression and internalizing symptoms in vulnerable youth. Prev Sci. In Press.
20. Perry DF, Miranda J, Ammerman RT, and Beardslee WR. Depression in Mothers: More Than the Blues—A Toolkit for Family Service Providers. 2014, Washington, DC: Substance Abuse and Mental Health Services Administration. [On-line] http://store.samhsa.gov/product/SMA14-4878 .







