LogoLogo
PET and PET and SPECT in SPECT in EpilepsyEpilepsyRodolfo Ferrando, MD, MSc
Assistant Professor of Nuclear Medicine Hospital de Clínicas, Facultad de Medicina.
Universidad de la República.Montevideo, Uruguay.

�� 1% of the population1% of the population�� 2525--30% are not controlled with medication30% are not controlled with medication�� Up to 80% of refractory epilepsy patients rendered Up to 80% of refractory epilepsy patients rendered seizure free with epilepsy surgeryseizure free with epilepsy surgery�� Precise localization of epileptogenic zone is needed Precise localization of epileptogenic zone is needed before surgerybefore surgery
Epidemiology and Impact
�� Clinical neurology, neurophysiology, neuropsychology, Clinical neurology, neurophysiology, neuropsychology, radiology, nuclear medicine, psychology, neurosurgery, pathologyradiology, nuclear medicine, psychology, neurosurgery, pathology..�� Close interaction between all members of the teamClose interaction between all members of the team�� Interactive multidisciplinary review of all clinical casesInteractive multidisciplinary review of all clinical cases�� Nuclear medicine physician must be an active member of the Nuclear medicine physician must be an active member of the epilepsy surgery programepilepsy surgery program
Epilepsy Surgery ProgramA multidisciplinary approach
�� Seizure history and neurological examinationSeizure history and neurological examination�� Previous scalp EEG recordingsPrevious scalp EEG recordings�� VideoVideo--EEG monitoringEEG monitoring�� MRIMRI�� IctalIctal--interictal SPECTinterictal SPECT�� PETPET�� Neuropsychological testingNeuropsychological testing
Epilepsy Surgery ProgramPre-surgical evaluation
Epilepsy Surgery ProgramVideo-EEG monitoring
LogoLogo
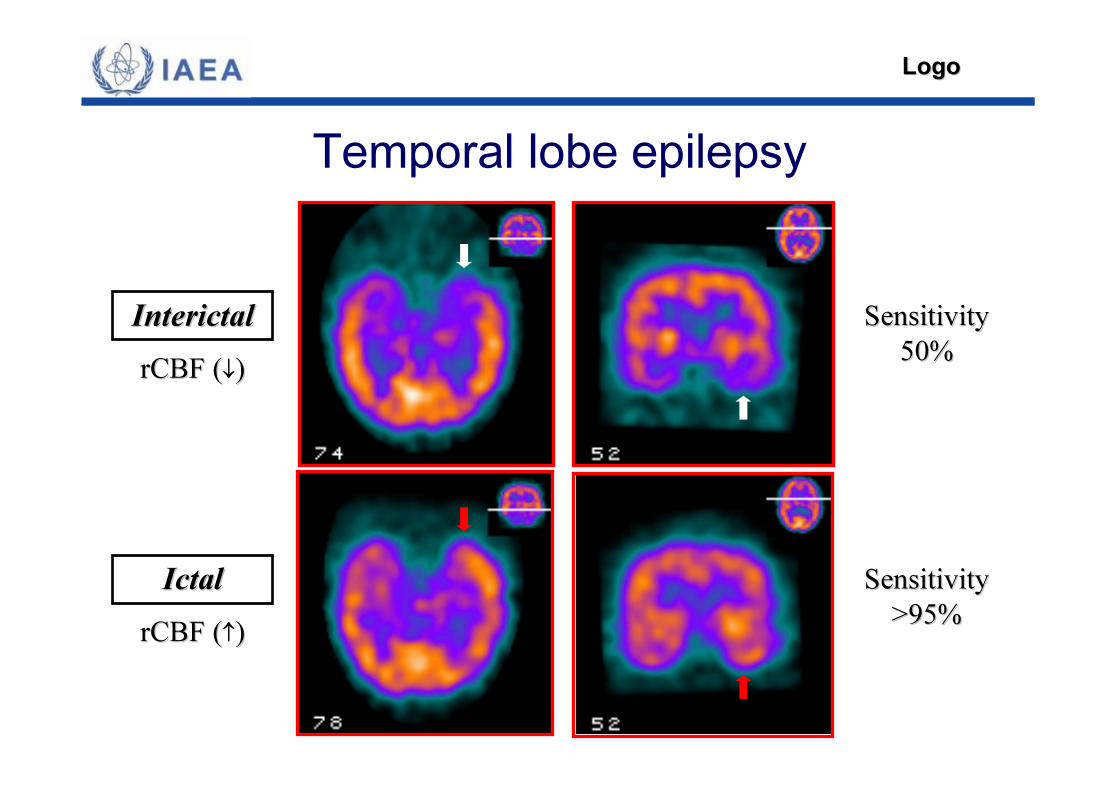
Temporal lobe epilepsy
InterictalInterictal SensitivitySensitivity50%50%rCBF (rCBF (↓))
IctalIctalrCBF (rCBF (↑))
SensitivitySensitivity>95%>95%
LogoLogo
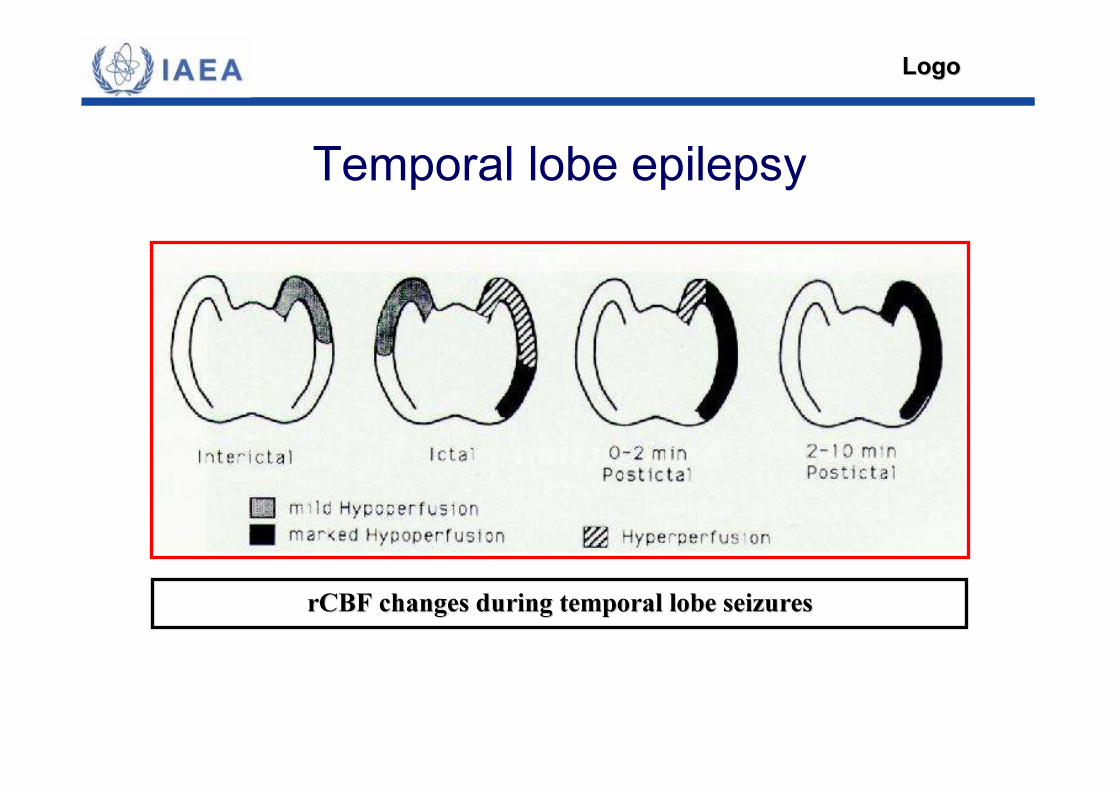
Temporal lobe epilepsy
rCBF changes during temporal lobe seizuresrCBF changes during temporal lobe seizures
LogoLogo
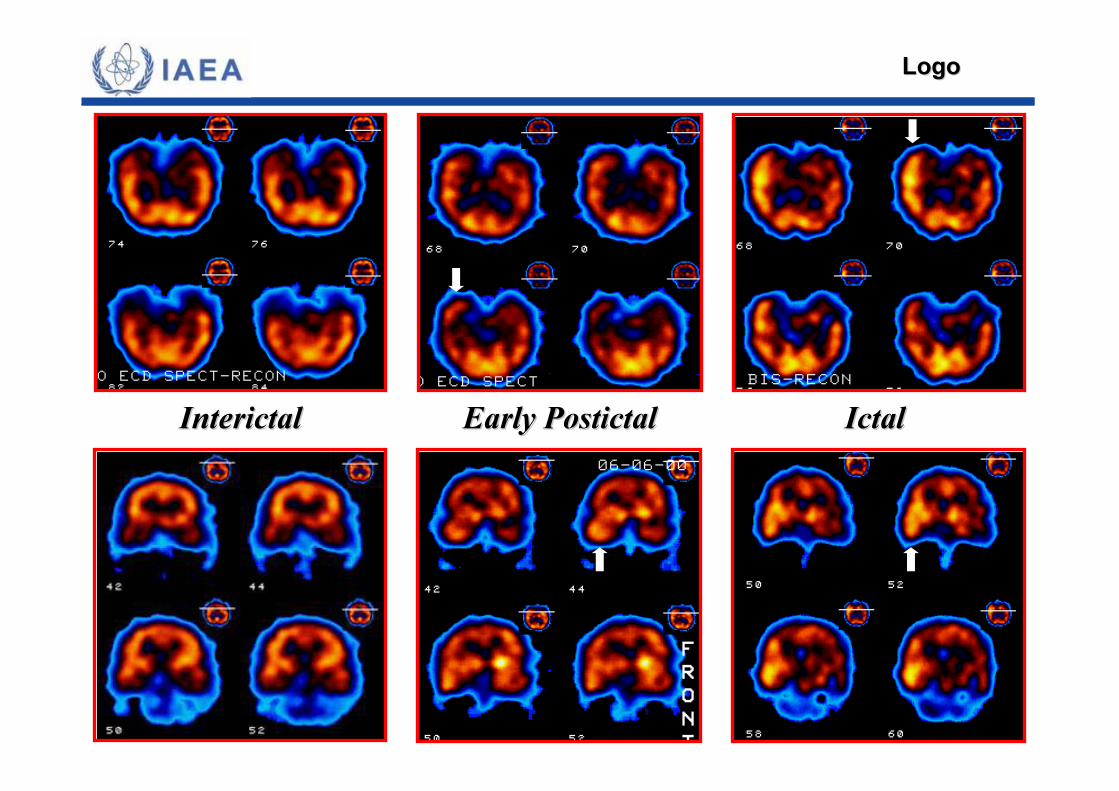
InterictalInterictal Early PostictalEarly Postictal IctalIctal
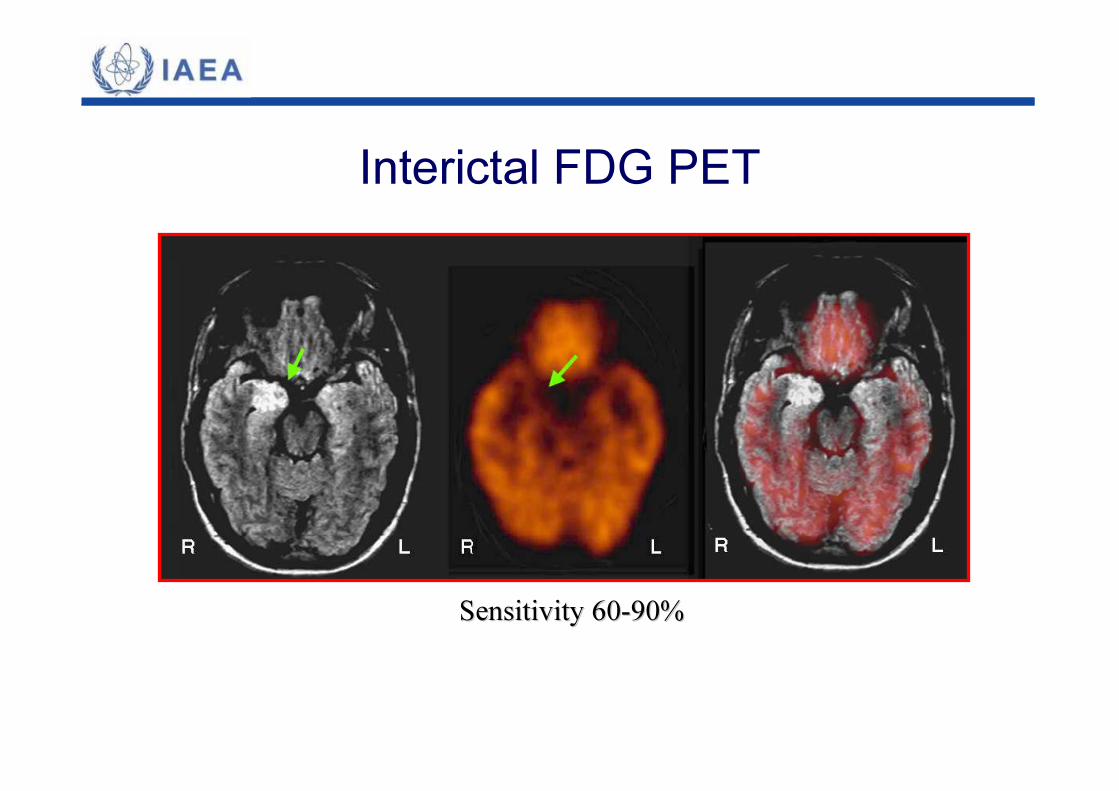
Interictal FDG PET
Sensitivity 60Sensitivity 60--90%90%
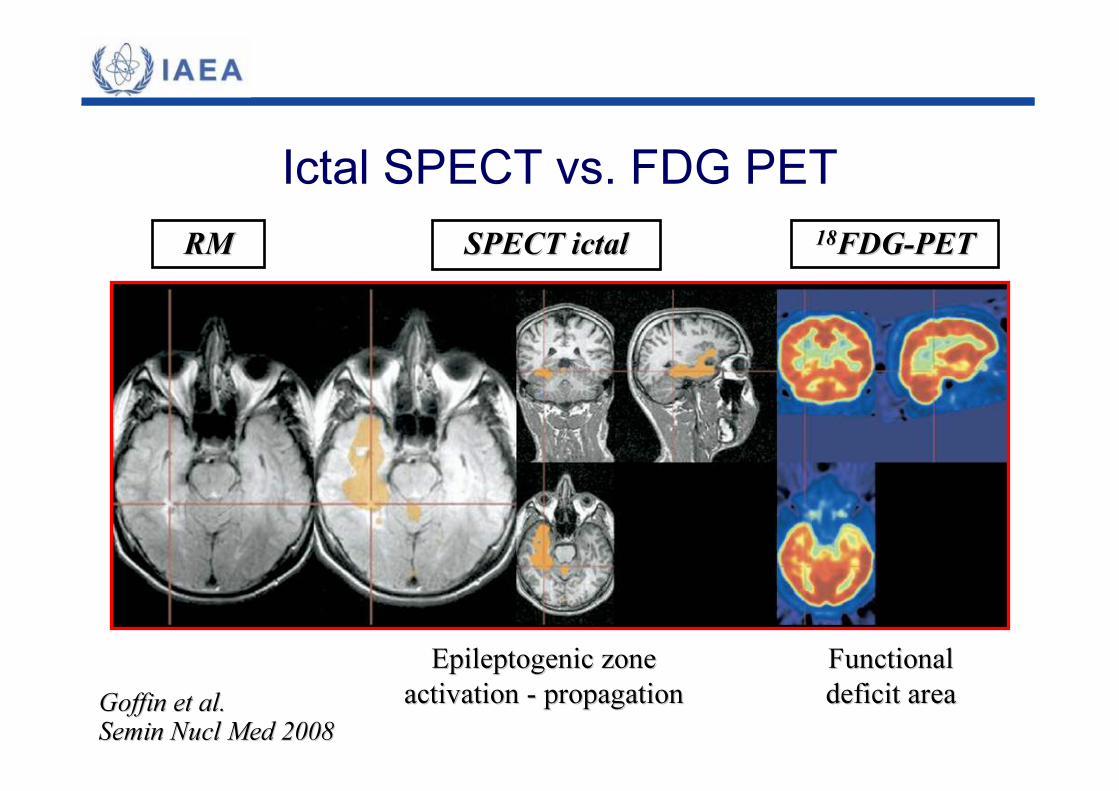
Ictal SPECT vs. FDG PETRMRM 1818FDGFDG--PETPETSPECT ictalSPECT ictal
Epileptogenic zoneEpileptogenic zoneactivation activation -- propagationpropagation
FunctionalFunctionaldeficit areadeficit areaGoffin et al. Goffin et al.
Semin Nucl Med 2008Semin Nucl Med 2008
�� Normal or inconclusive MRI is not unusual. Normal or inconclusive MRI is not unusual. �� Rapid rCBF changes. Short seizures are common.Rapid rCBF changes. Short seizures are common.�� Need for very early injectionNeed for very early injection�� Interictal SPECT has low sensitivity (30%)Interictal SPECT has low sensitivity (30%)�� Ictal SPECT remains highly sensitiveIctal SPECT remains highly sensitive�� Guide for invasive EEG recordingGuide for invasive EEG recording�� Subtraction images or SISCOM are requiredSubtraction images or SISCOM are required
Extratemporal epilepsy
SISCOM
SISCOM�� Improved localization, mostly in extratemporal epilepsy. Improved localization, mostly in extratemporal epilepsy. �� Epileptogenic zone detected in 50% of patients with no Epileptogenic zone detected in 50% of patients with no localizing EEG and 76% with normal MRIlocalizing EEG and 76% with normal MRI�� Localizing SISCOM concordant with surgical site predicts Localizing SISCOM concordant with surgical site predicts successful surgery outcome (58% vs. 18% with nonsuccessful surgery outcome (58% vs. 18% with non--localizing localizing or nonor non--concordant SISCOM).concordant SISCOM).
O’ Brien et al. Neurology 1998 and 2000
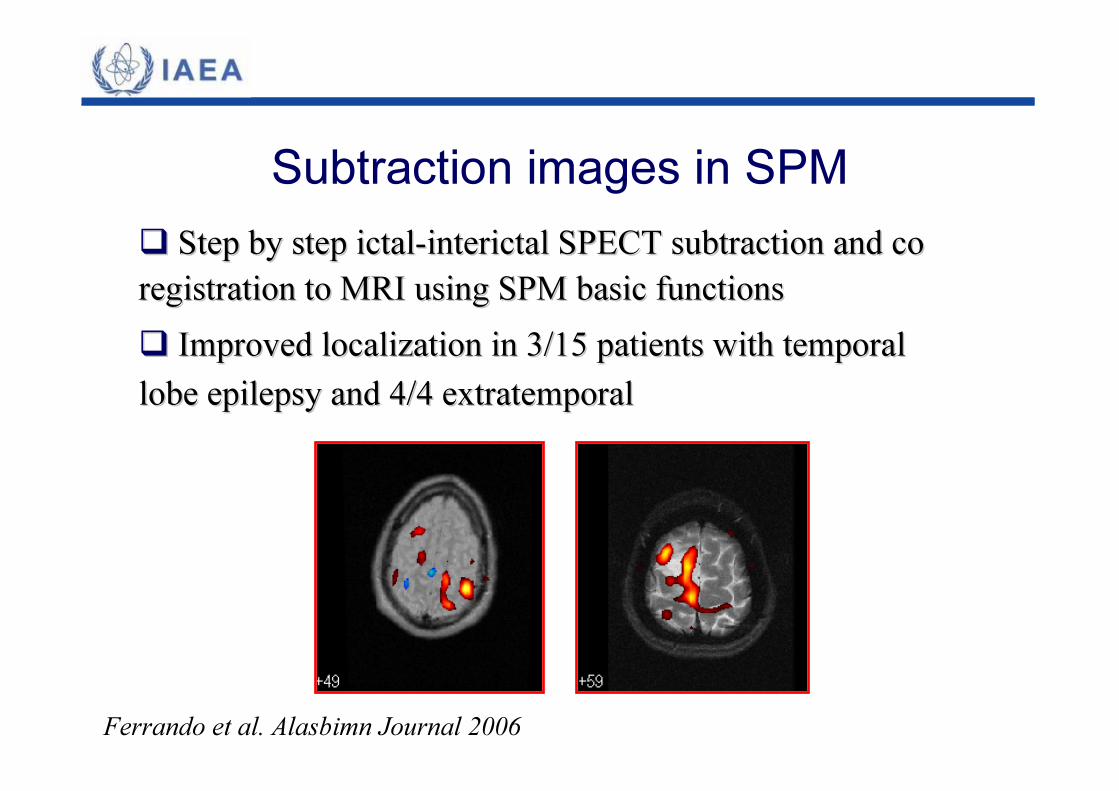
Subtraction images in SPM
Ferrando et al. Alasbimn Journal 2006
�� Step by step ictalStep by step ictal--interictal SPECT subtraction and co interictal SPECT subtraction and co registration to MRI using SPM basic functionsregistration to MRI using SPM basic functions�� Improved localization in 3/15 patients with temporal Improved localization in 3/15 patients with temporal lobe epilepsy and 4/4 extratemporallobe epilepsy and 4/4 extratemporal
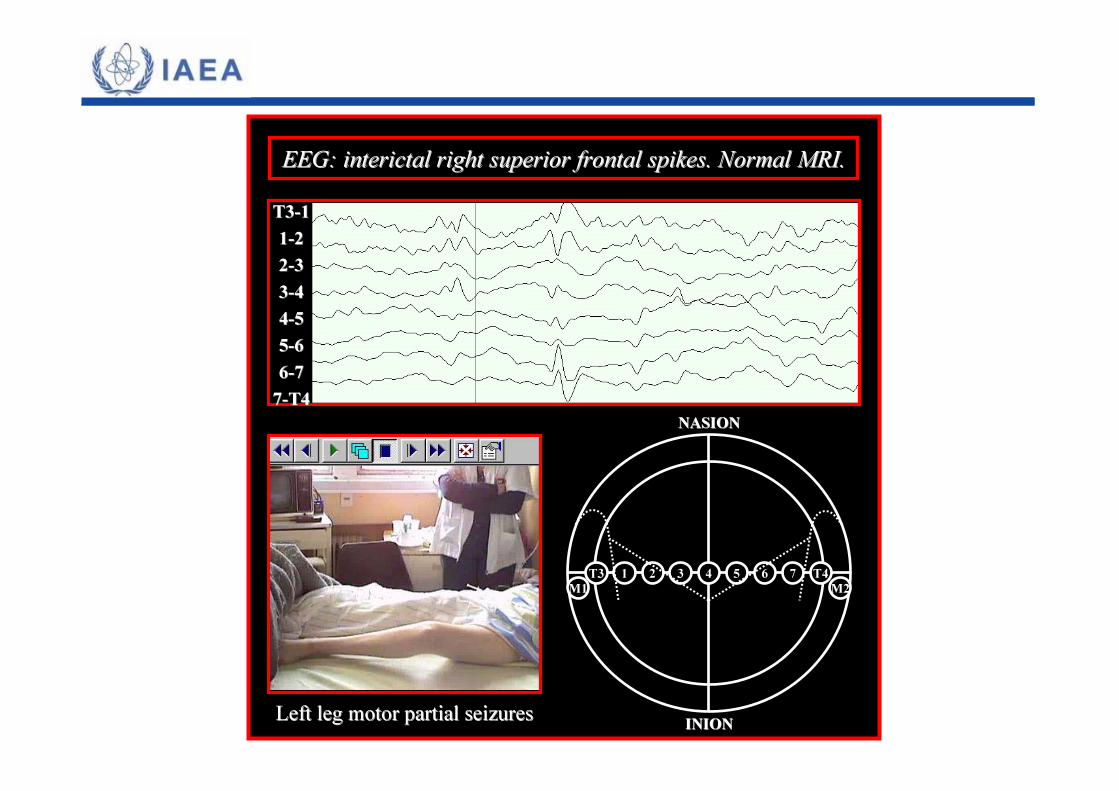
EEG: interictal right superior frontal spikes. Normal MRI.EEG: interictal right superior frontal spikes. Normal MRI.
NASIONNASION
INIONINION
T3 T4M1 M2
1 2 3 7654
Left leg motor partial seizuresLeft leg motor partial seizures
T3T3--1111--2222--3333--4444--5555--6666--7777--T4T4

Continuous partial epilepsy. Clonus of the right face.Normal MRIVideo-EEG: Left frontal rolandic and left temporal continuous activitySurgery: No
6 y/o female

Interictal
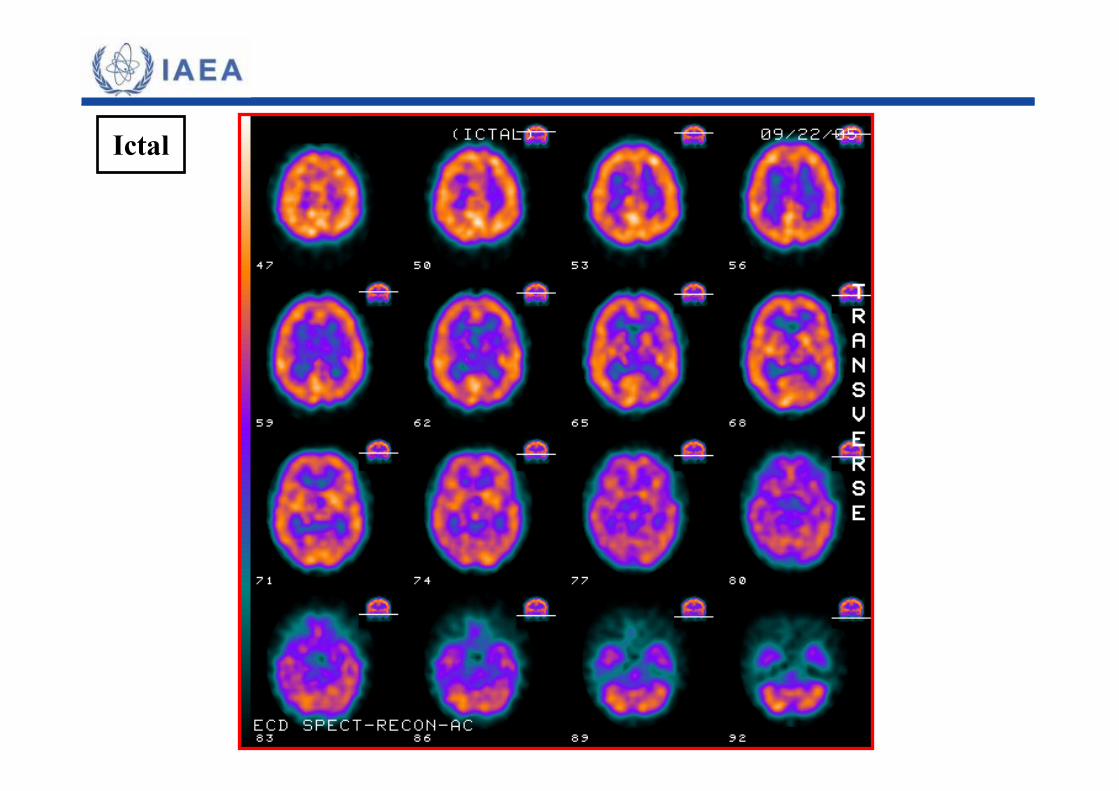
Ictal
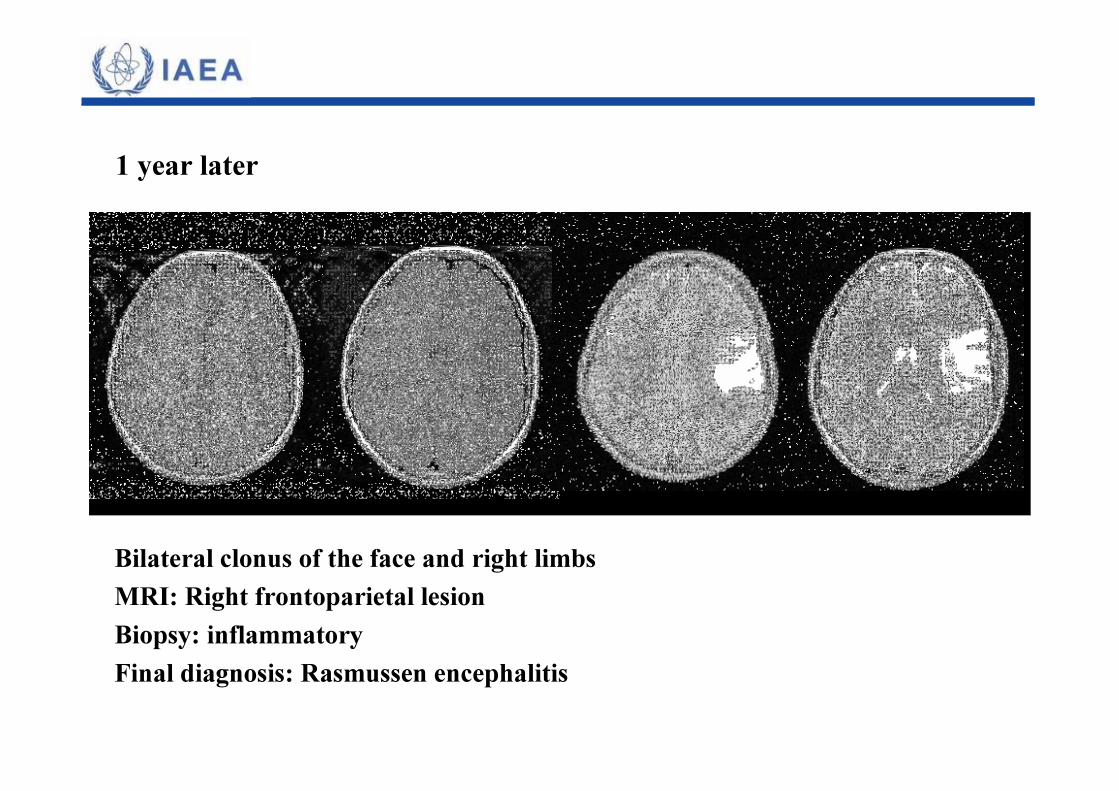
Bilateral clonus of the face and right limbsMRI: Right frontoparietal lesion Biopsy: inflammatoryFinal diagnosis: Rasmussen encephalitis
1 year later
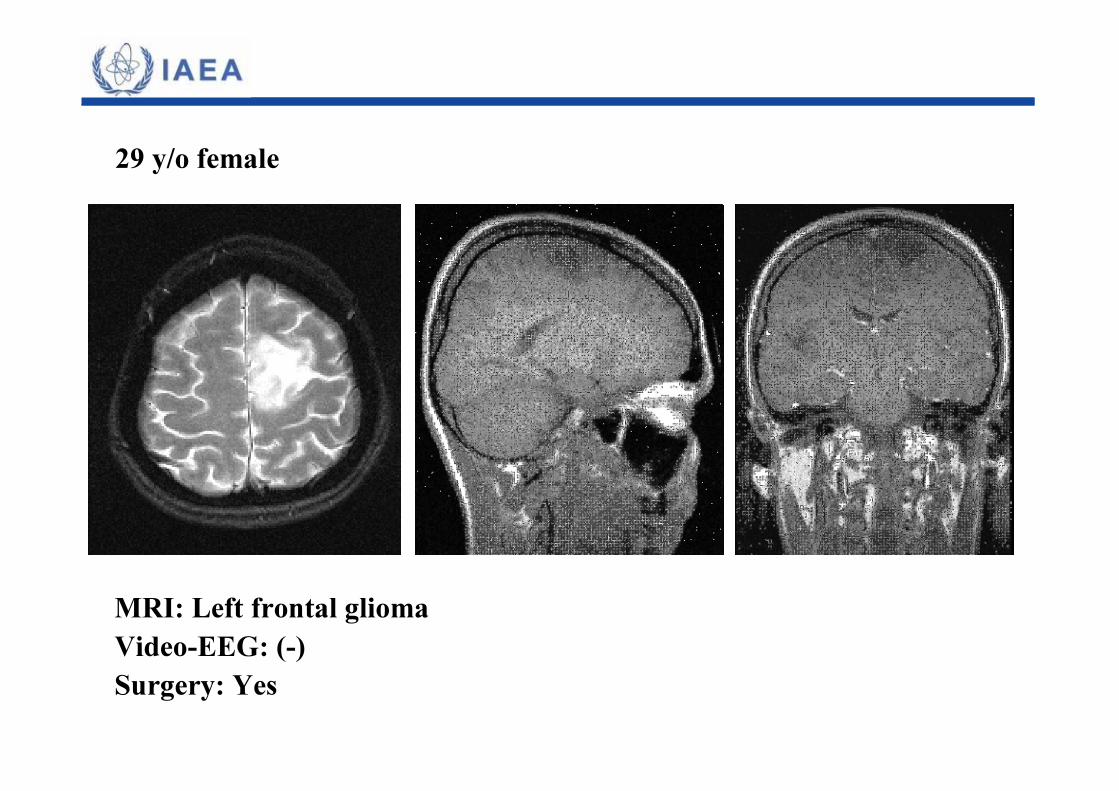
MRI: Left frontal gliomaVideo-EEG: (-)Surgery: Yes
29 y/o female
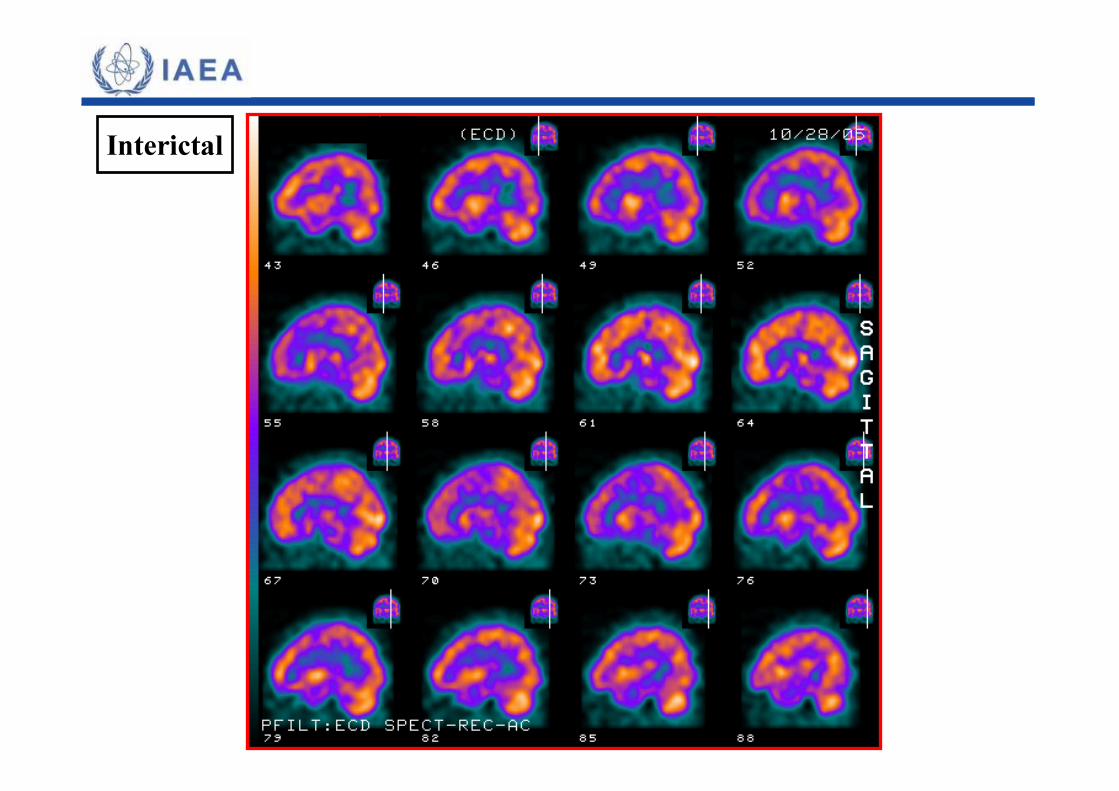
Interictal
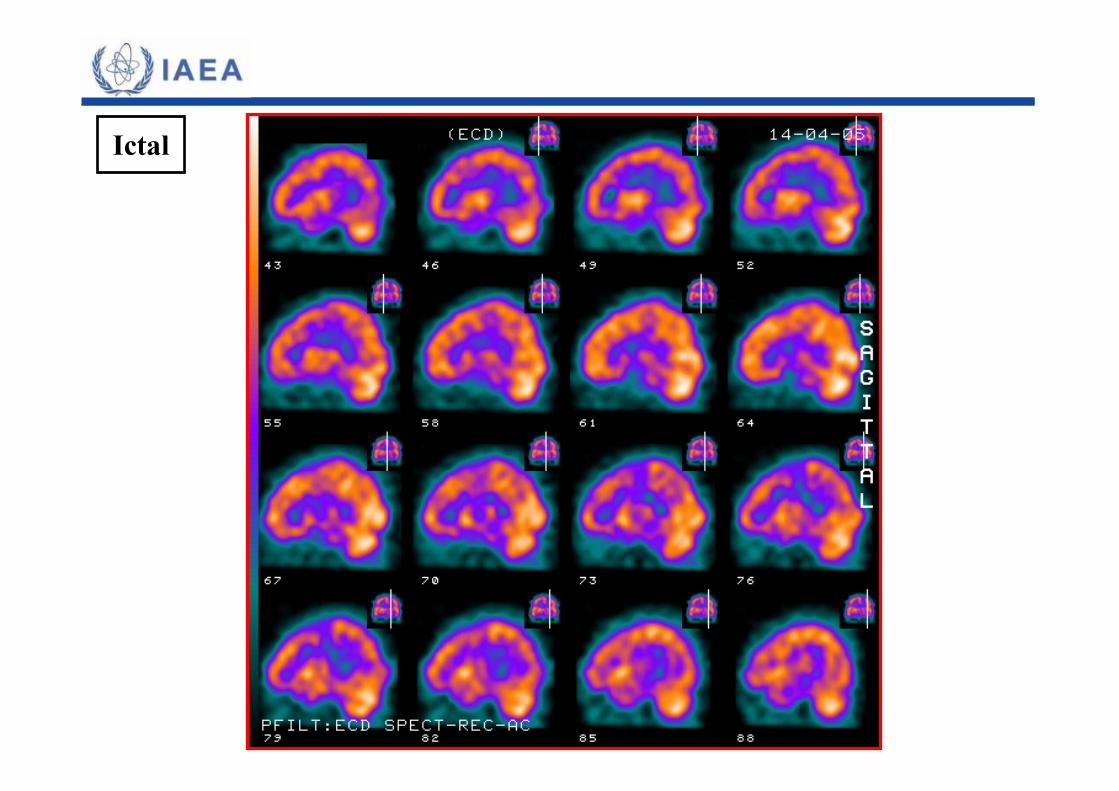
Ictal
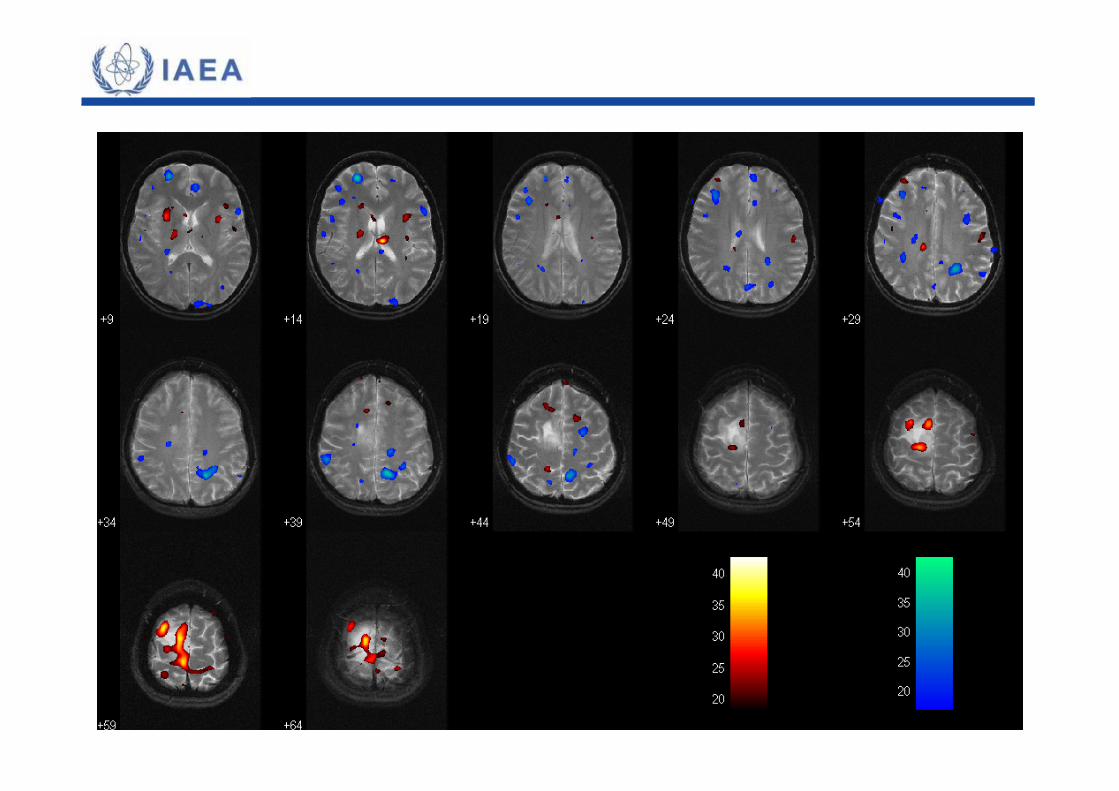
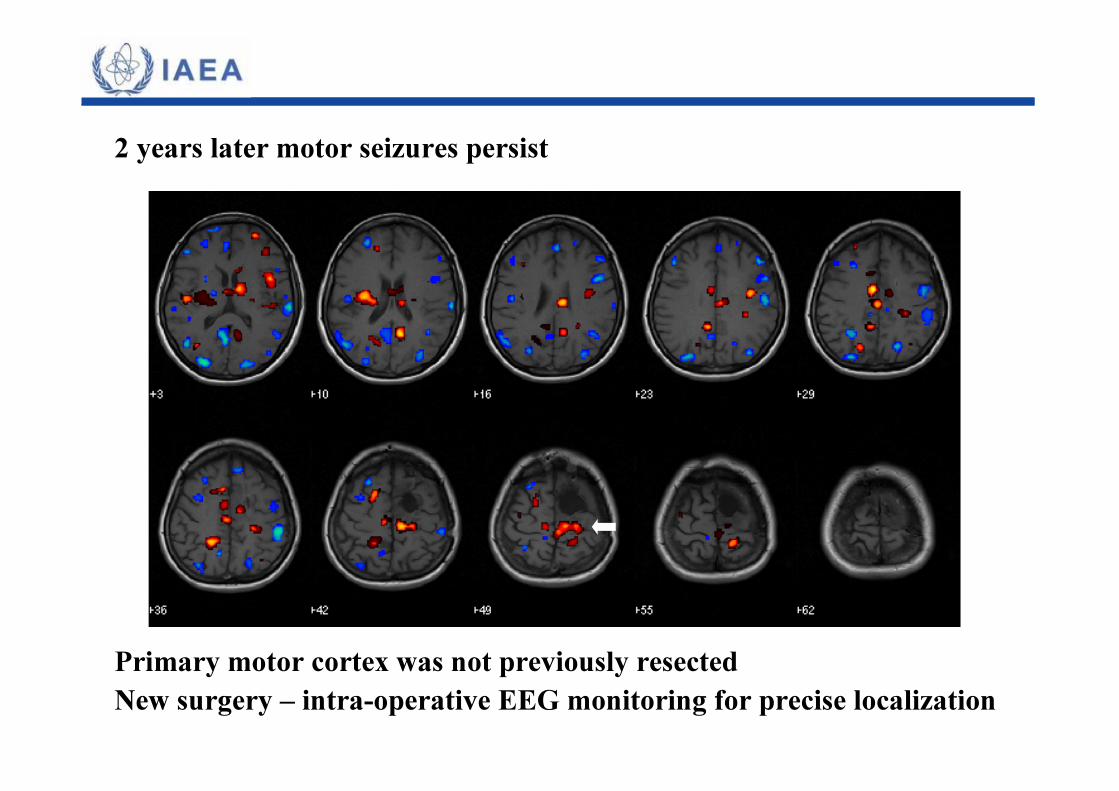
Primary motor cortex was not previously resectedNew surgery – intra-operative EEG monitoring for precise localization
2 years later motor seizures persist
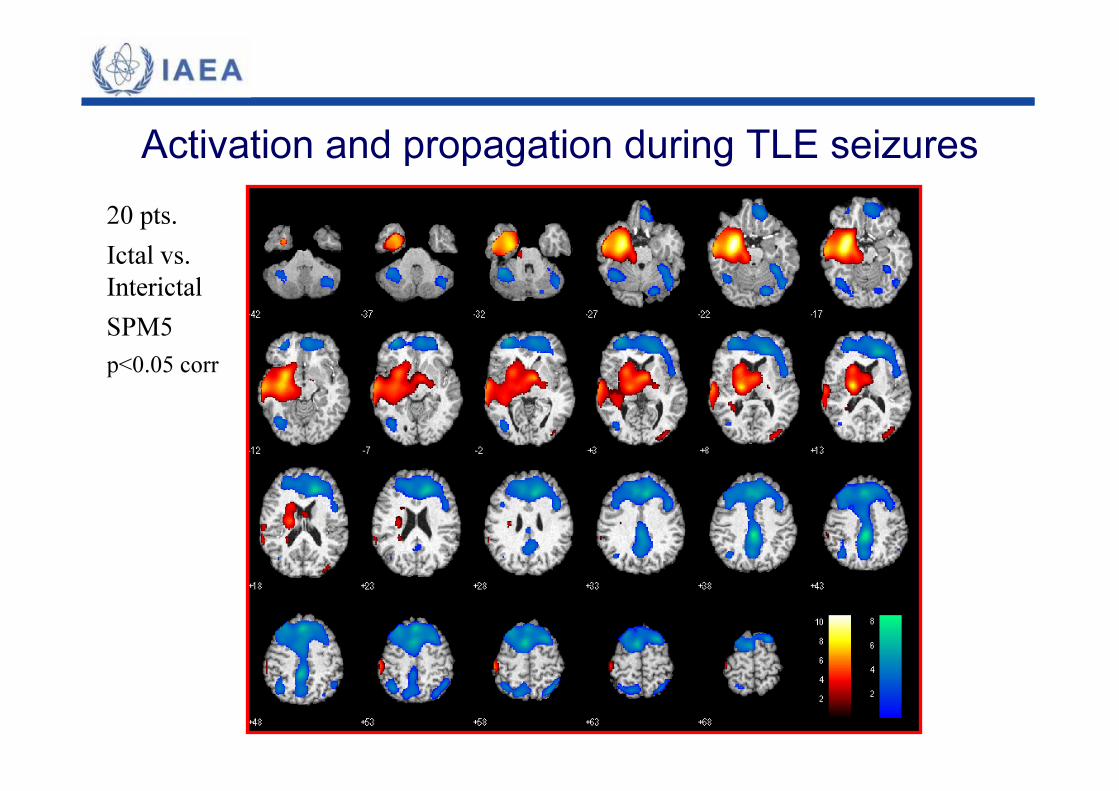
Activation and propagation during TLE seizures20 pts.Ictal vs. InterictalSPM5p<0.05 corr
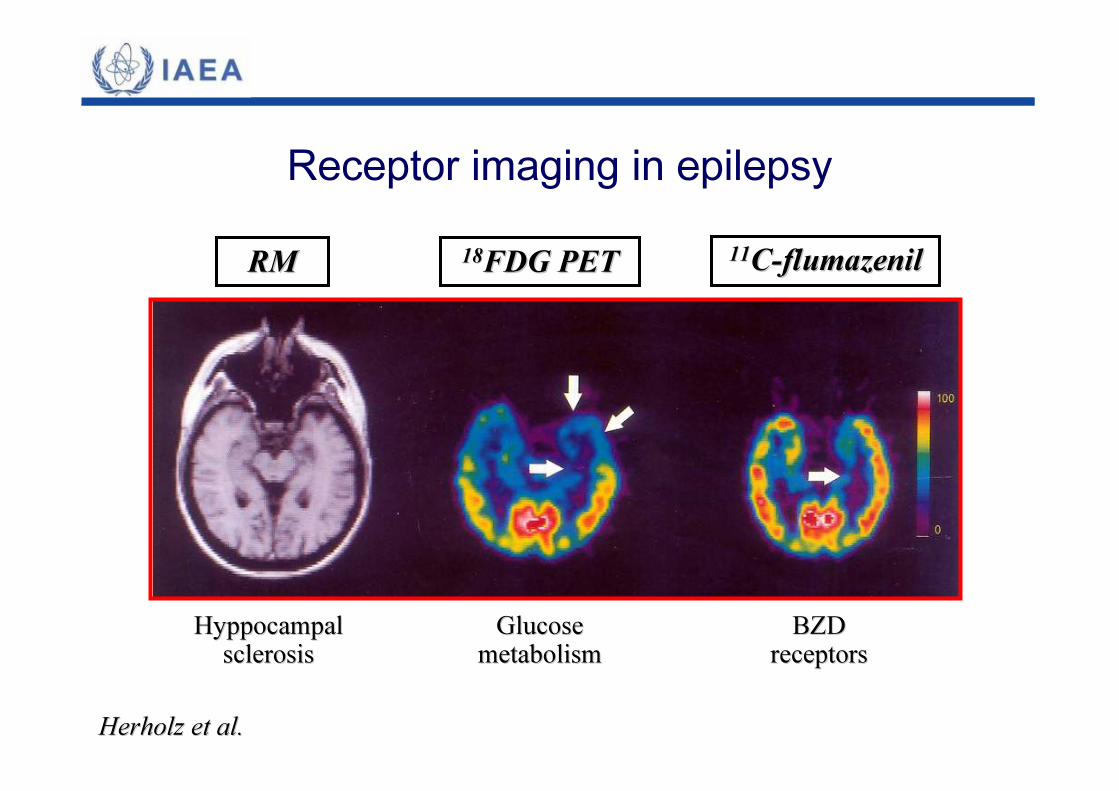
Receptor imaging in epilepsy
Herholz et al. Herholz et al.
RMRM 1818FDG PETFDG PET 1111CC--flumazenilflumazenil
HyppocampalHyppocampalsclerosissclerosis
GlucoseGlucosemetabolismmetabolism
BZDBZDreceptorsreceptors
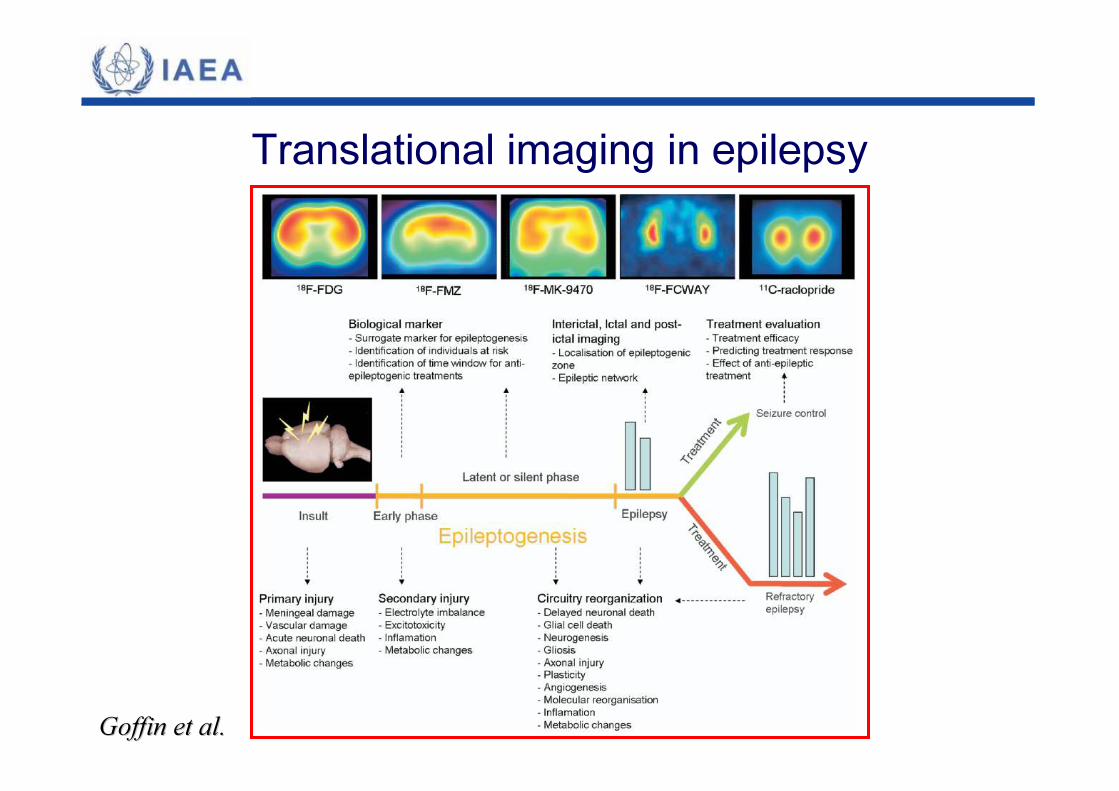
Translational imaging in epilepsy
Goffin et al. Goffin et al.







