Download - OXFORD CONFERENCE ON INNOVATION AND TECHNOLOGY TRANSFER FOR GLOBAL HEALTH University of Oxford

OXFORD CONFERENCE ON INNOVATION AND TECHNOLOGY TRANSFER FOR GLOBAL HEALTH
University of Oxford

BRIDGING THE GAP IN GLOBAL HEALTH
INNOVATION:FROM NEEDS TO
ACCESS
9-13 September 2007

HEALTH INNOVATION:
THE NEGLECTED CAPACITY OF DEVELOPING
COUNTRIES TO ADDRESS NEGLECTED DISEASES
Carlos MorelOswaldo Cruz Foundation (FIOCRUZ), Rio de Janeiro, Brazil
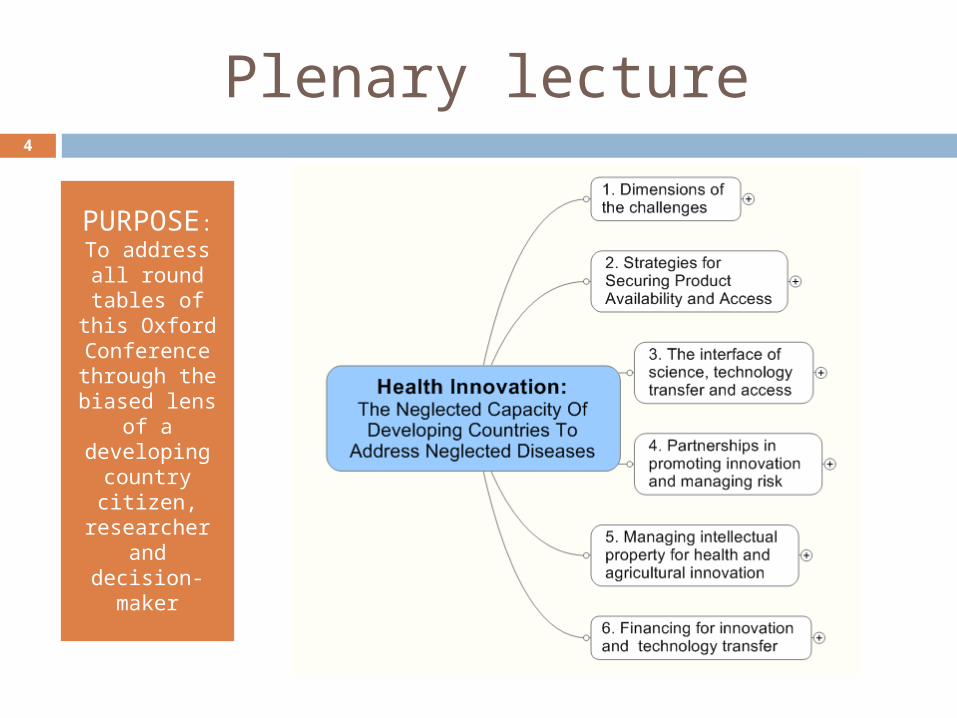
Plenary lecture4
PURPOSE:
To address all round
tables of this Oxford
Conference through the biased lens
of a developing
country citizen,
researcher and
decision-maker

1st Round Table5

Global, neglected and most neglected diseases (WHO &
MSF)6
World pharmaceutical market(>$600 bn in 2005)
Most neglected diseases(e.g. dengue, Chagas)
Neglected diseases(e.g. malaria, tuberculosis)
Global diseases(e.g. measles, diabetes)

Understanding global inequalities
Private health spending Malaria cases
Dorling D (2007) Worldmapper: The Human Anatomy of a Small Planet. PLoS Medicine 4(1)13-18
7

8
Public opinion sees illegal drugs
as a major problem all over
Africa

9
On the other hand the need to pay for medical and health care seems to vary among countries (e.g. Uganda x Mali)

Neglected tropical diseases
“The neglected tropical diseases are a group of
13 major disabling
conditions that are among the most common chronic infections in the world's poorest people”
10
Hotez et al, Control of Neglected Tropical Diseases. N Engl J Med 2007, 357:1018-1027
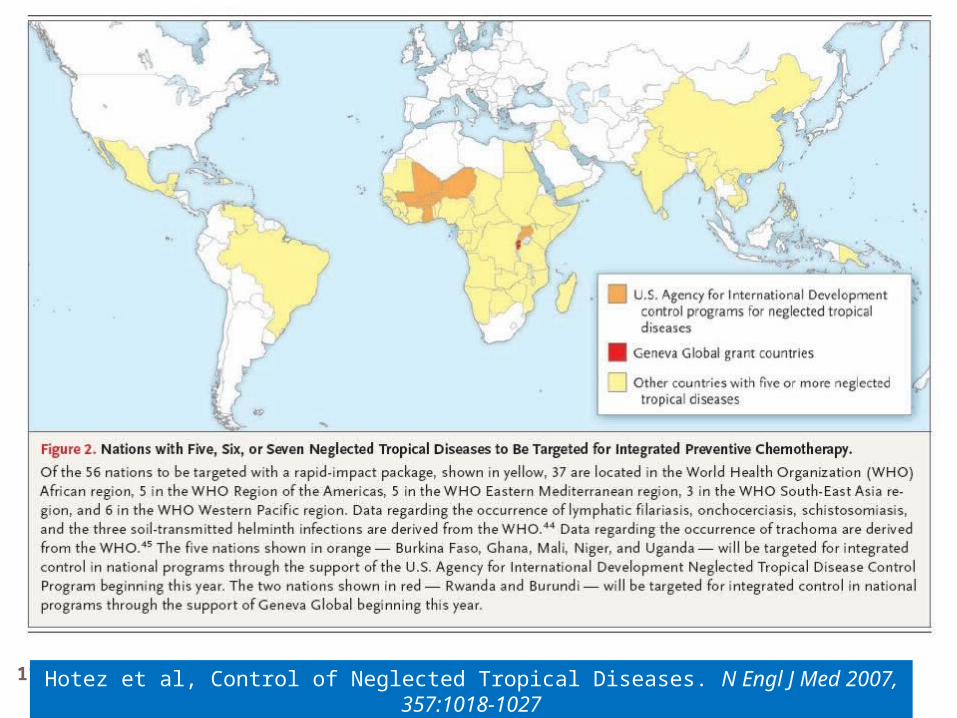
11 Hotez et al, Control of Neglected Tropical Diseases. N Engl J Med 2007, 357:1018-1027

Relationships between science, technology and
production12
Francisco Sagasti. Knowledge and innovation for development. The Sisyphus challenge of the 21st century, Cheltenham, UK; Northampton, USA:Edward Elgar, 2004. 151 pages

The Sisyphus challenge in Chile…
13
Scientometrics 72(1):93-103, 2007
The Sisyphus challenge in Chile…
14
“Developing countries share disbelief about the benefits of the
endogenous production of science as a tool for economical growth. Hence, public policies to strengthen science
and technology and promote the culture of innovation are, in general,
weak and sometimes incoherent”
Scientometrics 72(1):93-103, 2007

… and in Brazil15
Morel et al (2007) The road to recovery. Nature 449, in press

Entrepreneurship as ‘Conceptual Orphan’
“While the role of entrepreneurs and
entrepreneurship has never been denied, its most debilitating facet
is its limited, often cursory, coverage by the great thinkers on
economics and business”…
Hine and Kapeleris (2006) Edward Elgar Publishing Ltd, UK, 259 pp. ISBN-10 1 84376 584 4
16

Entrepreneurship as ‘Conceptual Orphan’
17
Hine and Kapeleris (2006) Edward Elgar Publishing Ltd, UK, 259 pp. ISBN-10 1 84376 584 4
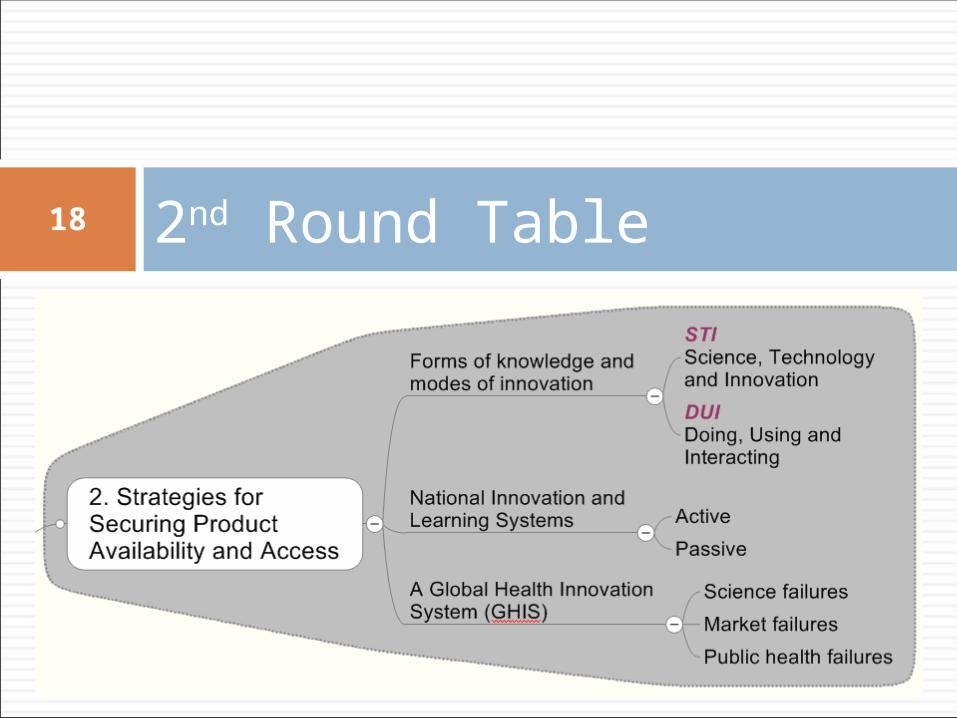
2nd Round Table18
Forms of knowledge and modes of innovation (Jensen et al, 2007)19
I. Science, Technology and Innovation - STI Based on the production and use of codified
scientific and technical knowledge (“explicit knowledge”)
High priority to the production of “know-why” Emphasis on the use of information and
communication technology as tools for codifying and sharing knowledge
“Global” knowledgeJensen MB, Johnson B, Lorenz E, Lundvall BA: Forms of
knowledge and modes of innovation. Research Policy 2007, 36:680-693.
Forms of knowledge and modes of innovation (Jensen et al, 2007)
II. Doing, Using and Interacting - DUI Relies on informal processes of learning
and experience-based know how High priority to the production of “know
how” and “know who” Strategies emphasizing the role played
by informal communication and communities of practice in mobilizing tacit knowledge for problem-solving and learning
“Local” knowledge
20
Jensen MB, Johnson B, Lorenz E, Lundvall BA: Forms of knowledge and modes of innovation. Research Policy 2007, 36:680-693.

Forms of knowledge and modes of innovation (Jensen et al, 2007)
Know-whatKnow-why
Know-howKnow-who
Emphasis on STI mode
Emphasis on DUI mode
21
Jensen MB, Johnson B, Lorenz E, Lundvall BA: Forms of knowledge and modes of innovation. Research Policy 2007, 36:680-693.

Forms of knowledge and modes of innovation (Jensen et al, 2007): Situations
Situation IOrganizations
are specialized in
one of the two modes
Situation II
Organizations try to
manage the two modes
STI DUI
STI DUI
22
Jensen MB, Johnson B, Lorenz E, Lundvall BA: Forms of knowledge and modes of innovation. Research Policy 2007, 36:680-693.
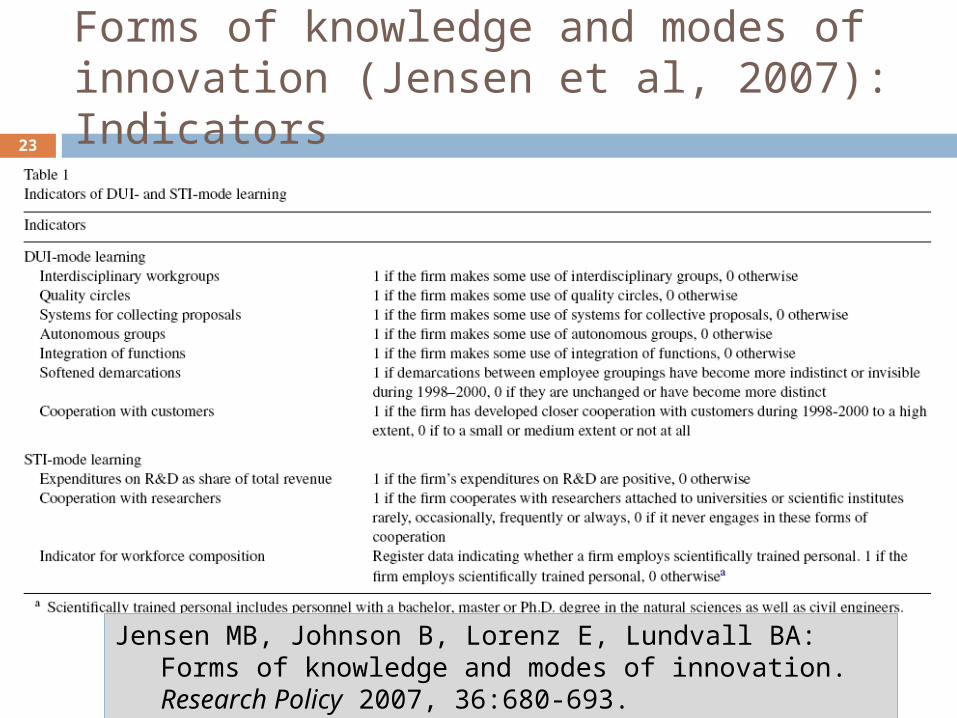
Forms of knowledge and modes of innovation (Jensen et al, 2007): Indicators23
Jensen MB, Johnson B, Lorenz E, Lundvall BA: Forms of knowledge and modes of innovation. Research Policy 2007, 36:680-693.
National Innovation & Learning Systems
24

ACTIVENIS
(Korea)
PASSIVE NLS
(Brazil)
25
National Innovation & Learning Systems

GDP per capitaKorea x Brazil, 1975-2004
26
1975Brazil: 5.502Korea: 3.722
2004Brazil: 7.531
Korea: 18.840

27

Science failures
Why: Insufficient knowledge Example: Unknown vaccines
Viral: Dengue, avian flu Bacterial: Leprosy, TB Parasitic: Malaria, leishmaniases, trypanosomiases
Need: Basic or “user-inspired” research; “Mode 2” of knowledge production (*)
Innovation modality New or improved products New R&D strategies: PDPs; PPPs (Brazil: Innovation
Law)(*) Gibbons M, Limoges C, Nowotny H, Schwartzman S, Scott P, Trow M: The new production
of knowledge: the dynamics of science and research in contemporary societies. London; Thousand Oaks; New Delhi: SAGE Publications; 1994
28

Market failures
Why: High costs prevent access to existing interventions or the development and production of cheaper ones
Example: antiretrovirals; combination therapies; new TB drugs
Need: Cheaper production processes; new funding strategies
Innovation modalities New methods/processes of production New funding policies (Push: PDPs; Pull: Global Funds)
New budgeting policies Increasing health budget (e.g. Brazilian taxation on financial
transactions) Decreasing health expenses (e.g. antiretrovirals IPR negotiations
between Governments and private sector)
29

Public health failures
Why: Lack of good governance or sound priorities; corruption; crises/war; cultural or religious factors; etc., prevent the access to cheap and readily available interventions
Examples Infectious diseases: polio vaccination (Religious or cultural factors);
leprosy chemotherapy (Brazil: wrong policy, lack of priority) Chronic diseases: obesity, tobacco (lobbying by multinational
companies) Needs: Education, civil society mobilization, human rights
approach Innovation modality: Process, strategy innovation
National Vaccination Days; WHO Tobacco Convention; educational TV campaigns (e.g. Brazilian soap operas with health messages); Tanzania’s experience in priority-setting in health systems (*)
(*) Savigny, Kasale, Mbuya, and Reid (2004) Fixing Health Systems
30

Science failure Market failure Public Health failure(knowledge/learning gap) (resources gap) (best practices gap)
New products, methods New processes New strategies or policies
Health Failures
Industrialized Countries
Innovative Developing Countries
Least Developed Countries
Ac
tio
ns
by
Na
tio
na
l In
no
va
tio
n S
ys
tem
s
Health Innovations needed
A “health failures / innovations needed / country actions” matrix 31

Science failure Market failure Public Health failure(knowledge/learning gap) (resources gap) (best practices gap)
Public funding of R&D (e.g. NIH genome projects of tropical pathogens)
Private sector participation at PDPs; Novartis/Singapore; Merck/Tres Cantos
North-South innovation networks; "Sister Institutions"/MIHR; CDTS/FIOCRUZ
"Bayh-Dole"-like laws to foster PDPs (e.g. Innovation Law/Brazil)
South-South networking with IDCs (e.g. FIOCRUZ/Brazil-ENSPA/Angola)
EDCTP-like clinical trials platforms
New products, methods New processes New strategies or policies
Health Failures
Industrialized Countries
Innovative Developing Countries
Least Developed Countries
Ac
tio
ns
by
Na
tio
na
l In
no
va
tio
n S
ys
tem
s
Health Innovations needed
A “health failures / innovations needed / country actions” matrix 32

33
Fighting science failures(knowledge gaps)
Fighting science failures(knowledge gaps)
34

Science failure Market failure Public Health failure(knowledge/learning gap) (resources gap) (best practices gap)
Drug-donation mechanisms (e.g. Mectizam)
Differential pricing; corporate image polishing
Increasing health budget (e.g. taxation on financial transactions/Brazil)
Negotiating price reductions (e.g. IP on antiretrovirals/Brazil)
Funding mechanisms e.g. Global Fund, GAVI
Fighting counterfeit drugs; improving regulatory situation
New products, methods New processes New strategies or policies
Health Failures
Industrialized Countries
Innovative Developing Countries
Least Developed Countries
Ac
tio
ns
by
Na
tio
na
l In
no
va
tio
n S
ys
tem
s
Health Innovations needed
A “health failures / innovations needed / country actions” matrix 35

Fighting market failures (resources gap)
36

Science failure Market failure Public Health failure(knowledge/learning gap) (resources gap) (best practices gap)
Donors (Rotary & polio; Sasakawa & leprosy; IDRC & priority setting)
Pressure through WHAs and Global Conventions (e.g. Tobacco; Kyoto)
Pressure from health sector and civil society (e.g. Brazil Constitution)
National vaccination days
Better priority setting (e.g. Tanzania's health budget/"for 80 cents more")
Educational campaigns; empowerment of women; fighting corruption
New products, methods New processes New strategies or policies
Health Failures
Industrialized Countries
Innovative Developing Countries
Least Developed Countries
Ac
tio
ns
by
Na
tio
na
l In
no
va
tio
n S
ys
tem
s
Health Innovations needed
A “health failures / innovations needed / country actions” matrix 37

Fighting public health failures(best practices gap)
38

Science failure Market failure Public Health failure(knowledge/learning gap) (resources gap) (best practices gap)
Public funding of R&D (e.g. NIH genome projects of tropical pathogens)
Drug-donation mechanisms (e.g. Mectizam)
Donors (Rotary & polio; Sasakawa & leprosy; IDRC & priority setting)
Private sector participation at PDPs; Novartis/Singapore; Merck/Tres Cantos
Differential pricing; corporate image polishing
Pressure through WHAs and Global Conventions (e.g. Tobacco; Kyoto)
North-South innovation networks; "Sister Institutions"/MIHR; CDTS/FIOCRUZ
Increasing health budget (e.g. taxation on financial transactions/Brazil)
Pressure from health sector and civil society (e.g. Brazil Constitution)
"Bayh-Dole"-like laws to foster PDPs (e.g. Innovation Law/Brazil)
Negotiating price reductions (e.g. IP on antiretrovirals/Brazil)
National vaccination days
South-South networking with IDCs (e.g. FIOCRUZ/Brazil-ENSPA/Angola)
Funding mechanisms e.g. Global Fund, GAVI
Better priority setting (e.g. Tanzania's health budget/"for 80 cents more")
EDCTP-like clinical trials platformsFighting counterfeit drugs; improving
regulatory situationEducational campaigns; empowerment
of women; fighting corruption
New products, methods New processes New strategies or policies
Health Failures
Industrialized Countries
Innovative Developing Countries
Least Developed Countries
Ac
tio
ns
by
Na
tio
na
l In
no
va
tio
n S
ys
tem
s
Health Innovations needed
A “health failures / innovations needed / country actions” matrix 39

3rd Round Table40

Components of health innovation
41

Components of health innovation
42

Innovative Developing Countries, IDCs
(*) Morel et al (2005) Innovation Strategy Today 1(1):1-15
http://www.biodevelopments.org/innovation/index.htm
43

44
Innovative Developing Countries, IDCs
(*) Morel et al (2005) Innovation Strategy Today 1(1):1-15
http://www.biodevelopments.org/innovation/index.htm

LDCs IDCs OECD and the six components of health innovation
45
(*) Morel et al (2005) Innovation Strategy Today 1(1):1-15
http://www.biodevelopments.org/innovation/index.htm
6 components or
determinantsLDC
s ID
Cs
O
EC
D
The power of the emerging... IDCs!
46

Health Innovation Networks47

Morel et al (2005) Science 309:401-404, 2005
Developing Country Vaccine Manufactures’ Network Brazil, Cuba, China, India, Indonesia, Mexico
WHO Developing Countries’ Vaccine Regulators Network Brazil, China, Cuba, India, Indonesia, Russia, South Africa, South
Korea, Thailand
48

50
National Health Innovation System
Morel et al (2005) Science 309:401-404, 2005

Collaborative research network on leprosy involving Brazilian
researchers51
Morel et al (2007) The road to recovery. Nature 449, in press
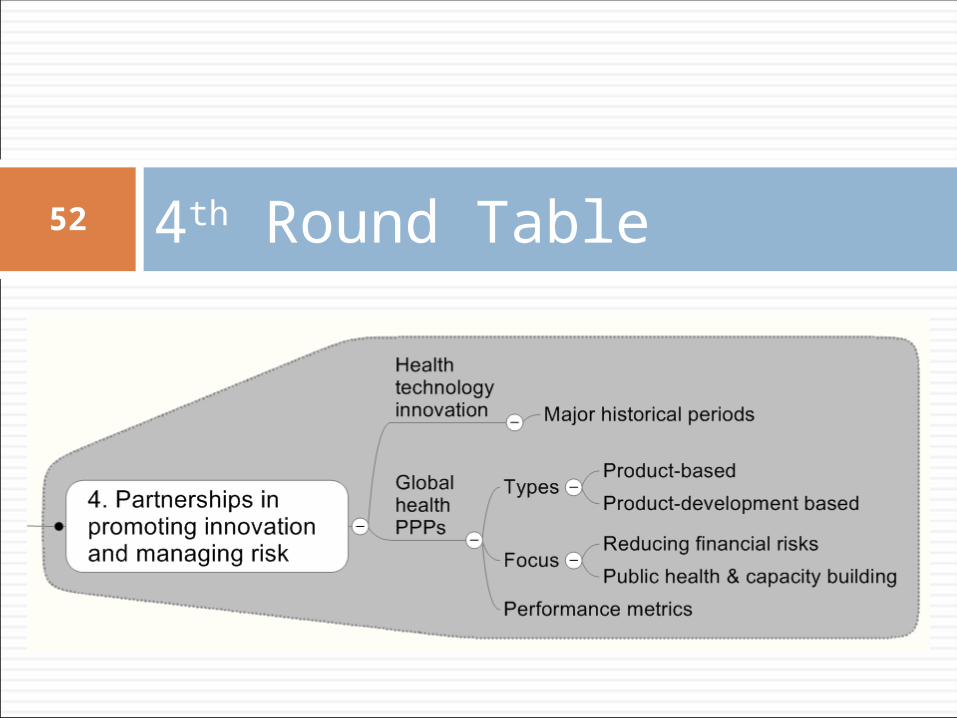
4th Round Table52

53
Health technology innovation: Major historical periods 1850-early 1900s’: Era of the public sectorEra of the public sector
Epitomized by the work of Pasteur 1900s’-1970s’: Era of the private sectorEra of the private sector
Emerged in Germany & chemical companies 1970s’-2000: Era of public sector Era of public sector
reawakeningreawakening United Nations: WHO Special Programmes (HRP,
TDR) USA: Bayh-Dole Act; NIH budget increase
2000- : Era of public-private partnerships Era of public-private partnerships (PPPs)(PPPs) Product Development Partnerships (PDPs) Innovative Developing Countries (IDCs) Health Innovation Networks
Mahoney, R & Morel, C. (2006) A Global Health Innovation System (GHIS). Innovation Strategy Today 2(1):1-12
54
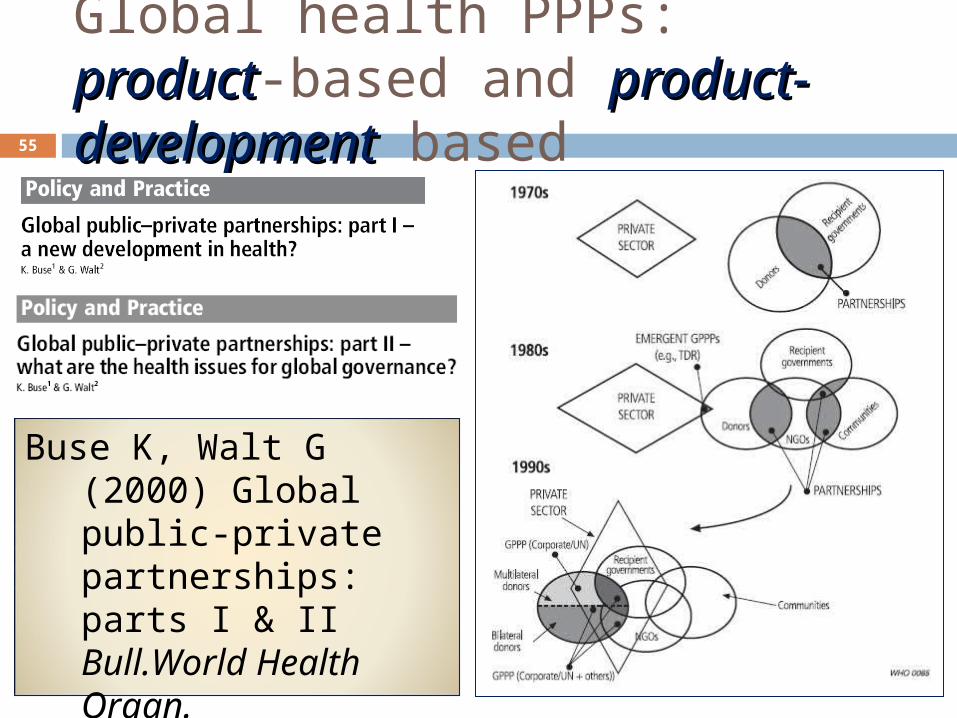
Global health PPPs: productproduct-based and product-product-developmentdevelopment based
Buse K, Walt G (2000) Global public-private partnerships: parts I & II Bull.World Health Organ. 78(4): 549-561 & 78(5): 699-709
55

56

57
Mary Moran’s Pharmaceutical R&D Policy Project
58

Mary Moran’s Pharmaceutical R&D Policy Project
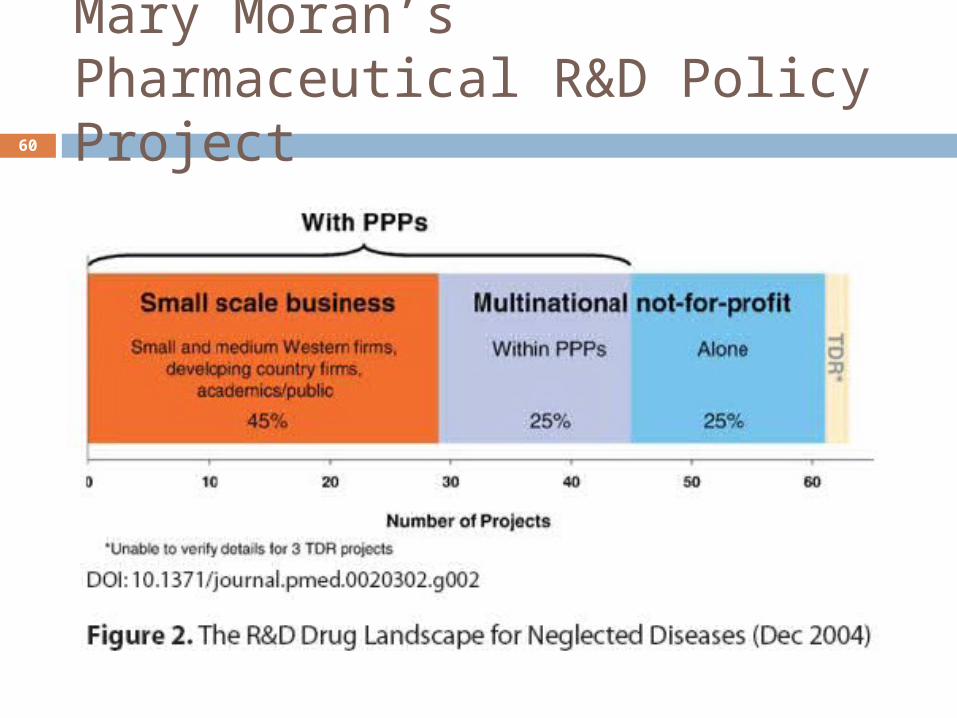
Mary Moran’s
team identified
three categories of major
players in drug
development for
neglected and most neglected diseases
Multinational drug companies 32 projects Working with PPPs or alone on a non-
commercial basis Smaller scale commercial firms
60-plus projects Working with PPPs on a commercial
basis Drug development PPPs
47 projects Working with large and small
companies
59
Mary Moran’s Pharmaceutical R&D Policy Project
60
Types of global health partnerships
61
There is today a large
number of global
health PPPs focusing on neglected and most neglected diseases. They are
quite different in
terms of vision and
goals.
Partnerships focusing at reducing financial risks of drug development MMV; TB Alliance
Partnerships focusing on public health and capacity building of endemic countries UN Special Programmes (HRP; TDR) Developing Country Vaccine
Manufactures’ Network WHO Developing Countries’ Vaccine
Regulators Network Partnerships addressing both goals
DNDi

Health PDPs: Broad range of mandates
Partnership focuses on product development and registration; minimal or no involvement of developing countries Most PDPs involving
multinational drug companies
Partnership’s mandate includes issues such as capacity building; training; involvement of endemic country institutions and public health WHO/country networks UN Special
Programmes
“Development as Growth” (*)
“Development as Freedom” (A. Sen)(*)
62
(*) Personal communication - Margaret Chon, Seattle University School of Law

A spectrum of global health PPPs
Nature of PPPs’visions and mandates
Focus on financial
risk reductio
n
Focus on increasin
g capacity
and public health
63

A spectrum of global health PPPs
Nature of PPPs’visions and mandates
Focus on financial
risk reductio
n
Focus on capacity building
and public health
64
DCVR (Developing Countries' Vaccine Regulators) Network
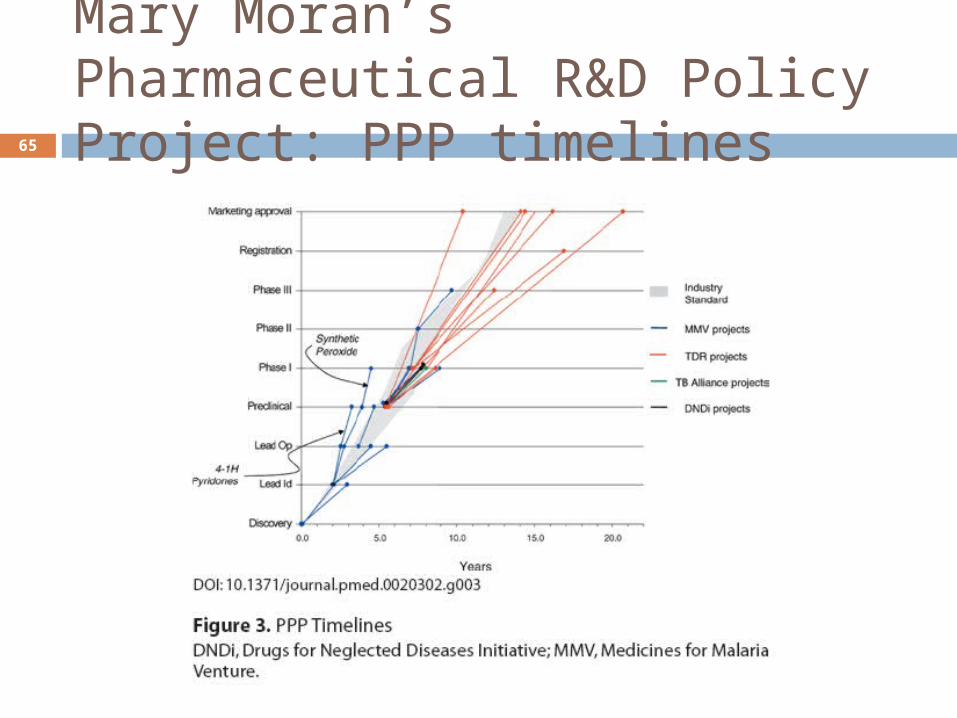
Mary Moran’s Pharmaceutical R&D Policy Project: PPP timelines65
66
Standard industry
metrics, as used by Moran’s project,
should be regarded as
just one component
of a broader set of metrics
when analyzing
Global PPPs of different
nature
Involvement of developing country partners National Innovation
Systems GLP, GCP, GMP Regulatory agencies
Strengthening local health systems & services
Mary Moran’s Pharmaceutical R&D Policy Project: Performance metrics

5th Round Table67
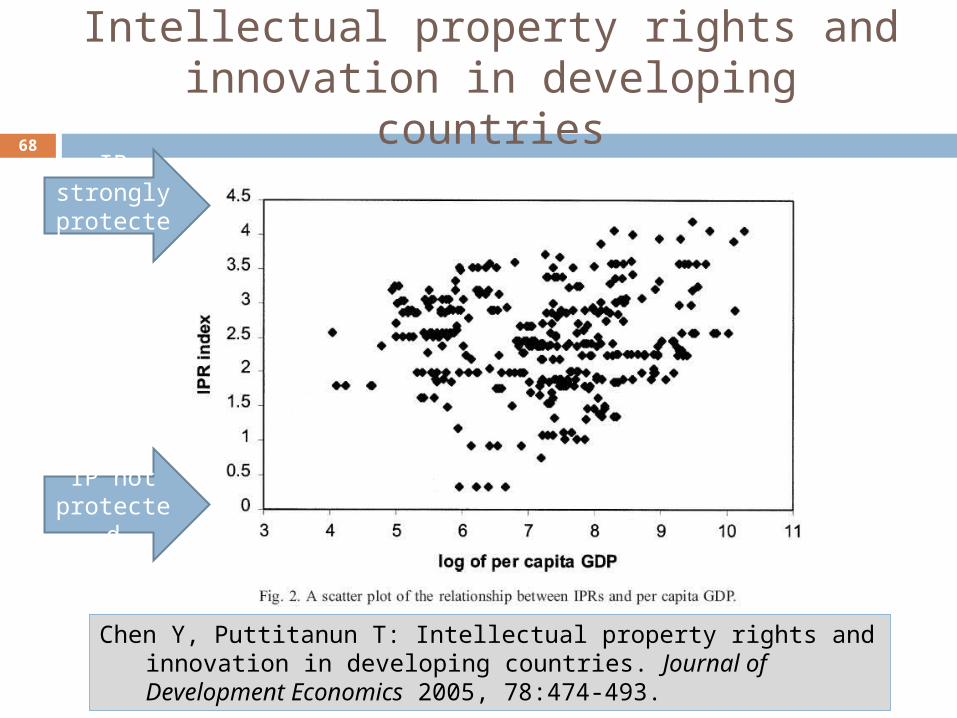
Intellectual property rights and innovation in developing countries
68
IP not protected
IP strongly
protected
Chen Y, Puttitanun T: Intellectual property rights and innovation in developing countries. Journal of Development Economics 2005, 78:474-493.

Chen Y, Puttitanun T: Intellectual property rights and innovation in developing countries. Journal of Development Economics 2005, 78:474-493.
Intellectual property rights and innovation in developing countries
69
IP protection due
to externa
l pressur
e
IP protection by
country decisio
nIP policy in
transition

IP and compulsory licences70

IP management in health
To address IP management
and licensing, one
of the six components of
health innovation, developing
countries need to train human resources and
strengthen their
institutions in this critical
area

Public Health, Innovation and IP
Resolution of the World Health
AssemblyIntergovernmental Working Group on
Public Health, Innovation and
Intellectual Property (IGWG)
http://www.who.int/phi/documents/en/
73
Public Health, Innovation and IP
74
Secretariat for Public Health, Innovation and Intellectual Property (PHI) Established in September 2006 Mandate
Facilitate implementation of Resolution WHA 59.24
Follow-up to the report of the Commission on Intellectual Property Rights, Innovation and Public Health

Resolution WHA 59.24 & IGWG
75
Intergovernmental Working Group (IGWG) Mandate
Global Strategy and Plan of Action “Securing an enhanced and sustainable basis for
needs-driven, essential health research and development relevant to diseases that disproportionately affect developing countries”
Submission to the Sixty-first World Health Assembly in May 2008
http://www.who.int/phi/en/ What next? May 2008 is approaching rapidly
Intergovernmental Working Group (IGWG)
76
Final product should go beyond a WHA resolution
The “Global Strategy and Plan of Action” will need to be institutionalized / hosted at a suitable home or platform Expertise in neglected diseases R&D Good interface with industry and PDPs Balanced governance involving developed
and developing countries Proven record of implementation capacity Long term vision and strategic thinking

6th Round Table77

Financing for what kind of innovation?
78
Hine and Kapeleris (2006) Edward Elgar Publishing Ltd, UK, 259 pp. ISBN-10 1 84376 584 4

The challenge of financing technological innovation: Vaccines79
Historical models of vaccine development Predominantly private sector development
Hepatitis B (HBV) vaccine: Merck Public (or nonprofit) sector vaccine design,
with handover to the private sector for trials and manufacturing Human papillomavirus (HPV) vaccine
Predominantly public-sector development Influenza vaccine: US Army
Coordination by a nonprofit entity Salk polio vaccine
IAVI Policy Research Working Paper #14 - R&D Models: Lesson from Vaccine History
The challenge of financing technological innovation: Vaccines80
Expanded Program for Immunization (EPI) vaccines $0.25 per dose; $1.50 total cost/child
New, non-EPI vaccines can cost 10x more $13.50 per fully immunized child The example of Dominican Republic
Budget of current national immunization program: $658,190
Addition of hepatitis b vaccine: additional $590,040
Addition of Hib vaccine: additional $2,880,000
Mahoney et al, Vaccine 18:2625-2635, 2000

Commercial trade of pharmaceuticals in Brazil
81
Morel et al (2007) The road to recovery. Nature 449, in press

82
Evolution of Latin America’s economies
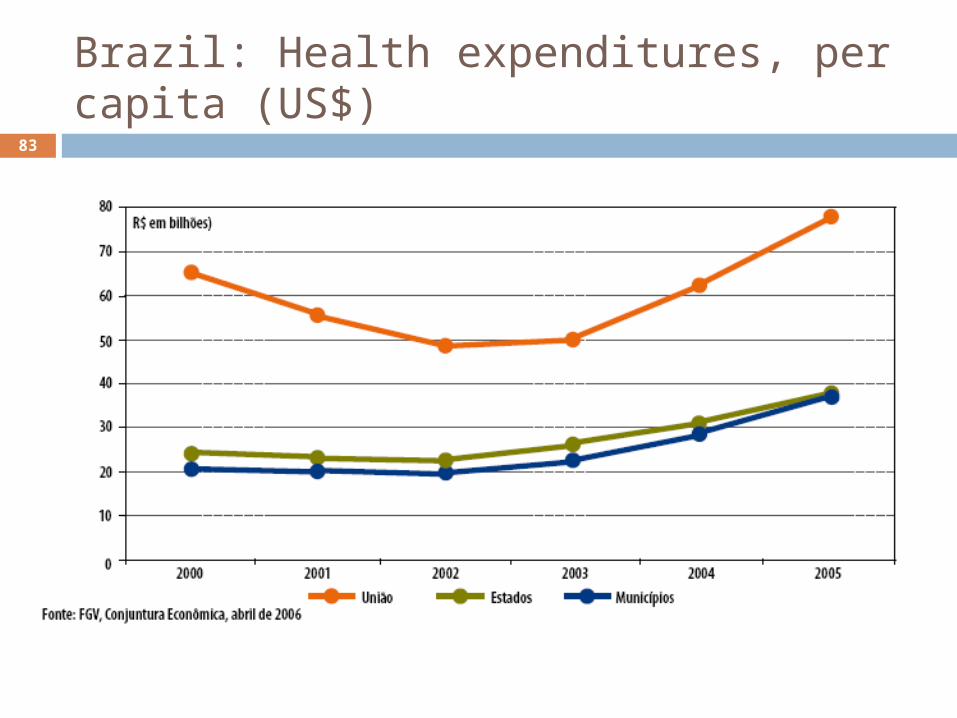
Brazil: Health expenditures, per capita (US$)
83

Brazil: Health expenditures, per capita (US$)
84
2002-05:
59.5% u
p
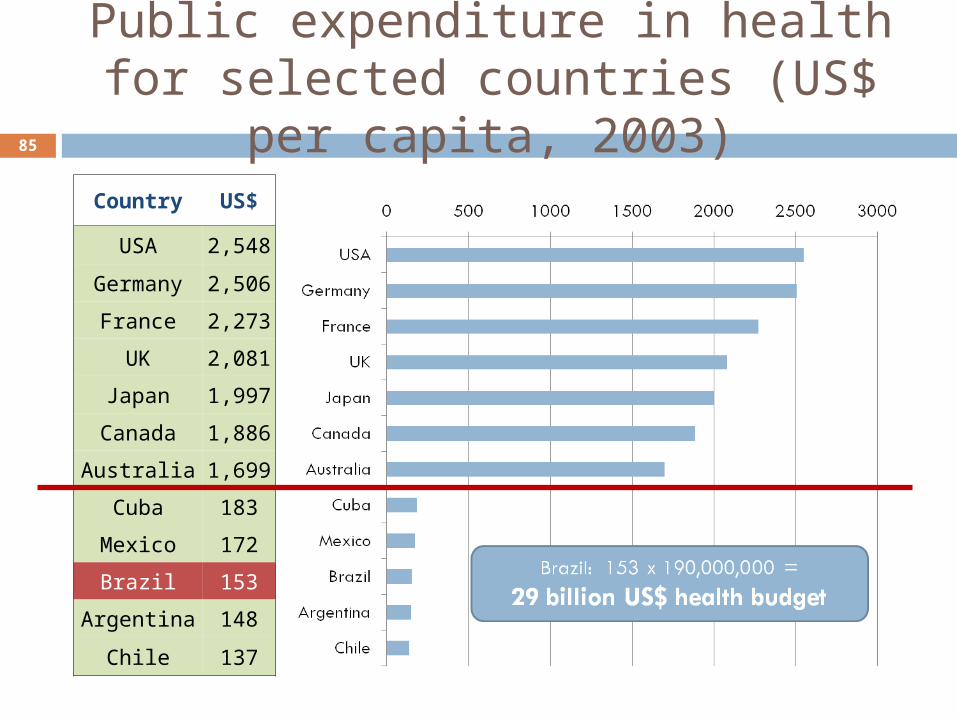
Public expenditure in health for selected countries (US$ per
capita, 2003)85
Country US$
USA 2,548
Germany 2,506
France 2,273
UK 2,081
Japan 1,997
Canada 1,886
Australia 1,699
Cuba 183
Mexico 172
Brazil 153
Argentina 148
Chile 137

Financing: It is not only money that counts
“Brazil’s approach to the HIV/AIDS epidemic has been characterized by an early public sector response, strong civil society participation, multisectoral mobilization of efforts and resources, a balanced and comprehensive
approach to prevention and treatment and the inclusion of a human rights perspective in all strategies”
86

Financing for what kind of innovation?
87
Gardner et al, Health Affairs 2007, 26(4):1052-1061.

88

89
Science 317:482-487, 27/July/2007








