Download - Optimal Clopidogrel Dosing
The antiplatelet effect of higher The antiplatelet effect of higher loading and maintenance dose loading and maintenance dose
regimens of clopidogrel: the Plavix regimens of clopidogrel: the Plavix Response in Coronary Intervention Response in Coronary Intervention
(PRINC) trial(PRINC) trial ACTRN12606000129583ACTRN12606000129583
11Gladding PA, Gladding PA, 11Webster MW, Webster MW, 11Zeng I, Zeng I, 11Farrell H, Farrell H, 11Stewart J, Stewart J, 11Ruygrok P, Ruygrok P, 11Ormiston J, Ormiston J, 22Gunes A, Gunes A, 33Perry J, Dahl M-L.Perry J, Dahl M-L.
11Green Lane Cardiovascular DepartmentGreen Lane Cardiovascular Department33Liggins Institute, Auckland, NZLiggins Institute, Auckland, NZ
22Uppsala University, SwedenUppsala University, Sweden
Funded by GLREF, NHFFunded by GLREF, NHFSupport from Sanofi NZSupport from Sanofi NZ
Optimal Clopidogrel DosingOptimal Clopidogrel Dosing
• Important for two reasons:Important for two reasons:1.1. Antiplatelet effect at PCI corresponds with Antiplatelet effect at PCI corresponds with
periprocedural infarction (ARMYDA-2)periprocedural infarction (ARMYDA-2)
2.2. Timing: Dosing <6-10hrs prior to PCI Timing: Dosing <6-10hrs prior to PCI ineffective (CREDO)ineffective (CREDO)
• Three recent studies have indicated that Three recent studies have indicated that doses >600mg are doses >600mg are notnot more effective more effective than 600mgthan 600mg
AimsAims
• To compare a higher split loading dose of To compare a higher split loading dose of clopidogrel (600mg + 600mg) with clopidogrel (600mg + 600mg) with standard 600mgstandard 600mg
• Compare 150mg with 75mg once dailyCompare 150mg with 75mg once daily
• Investigate the pharmacogenomics of Investigate the pharmacogenomics of clopidogrelclopidogrel
MethodsMethods
Time table
Percutaneous coronaryintervention
n=60600 mg
Clopidogrel
-10 minutes Baseline 2 hours 4 hours 7 hours 7 days
n=31intraarterial
5mg Verapamil
n=29intraarterial
Placebo
n=37600 mg
Clopidogrel
n=23Placebo
Randomization
SamplingSampling Sampling Sampling Sampling
Discharge
n=2275 mg/dayClopidogrel
n=3875 mg/dayClopidogrel
Randomization
N=36150mg/dayClopidogrel
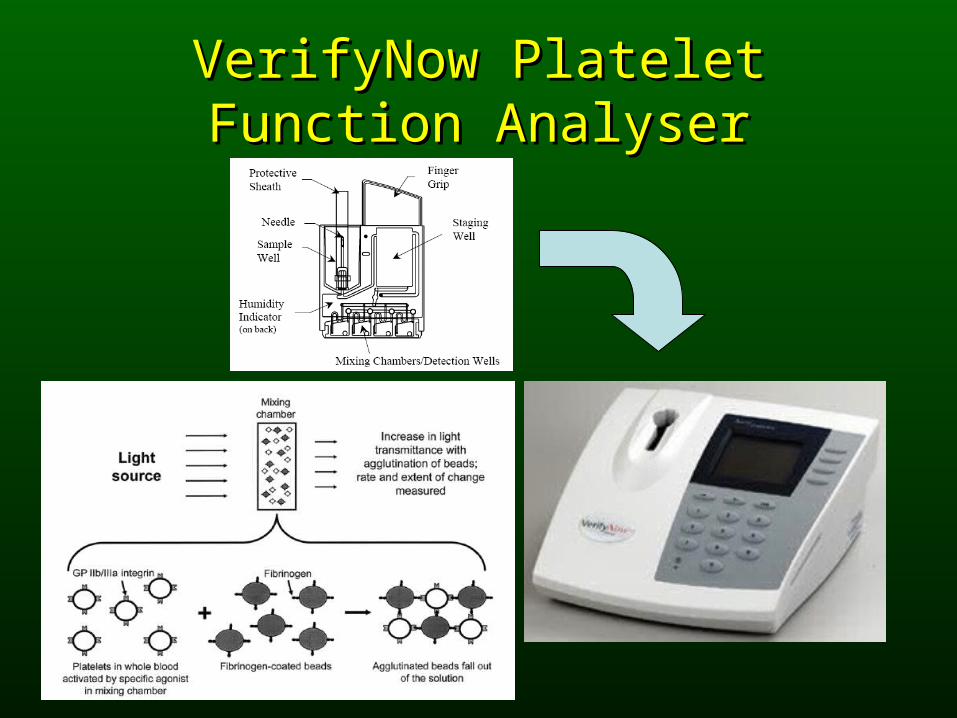
VerifyNow Platelet Function VerifyNow Platelet Function AnalyserAnalyser
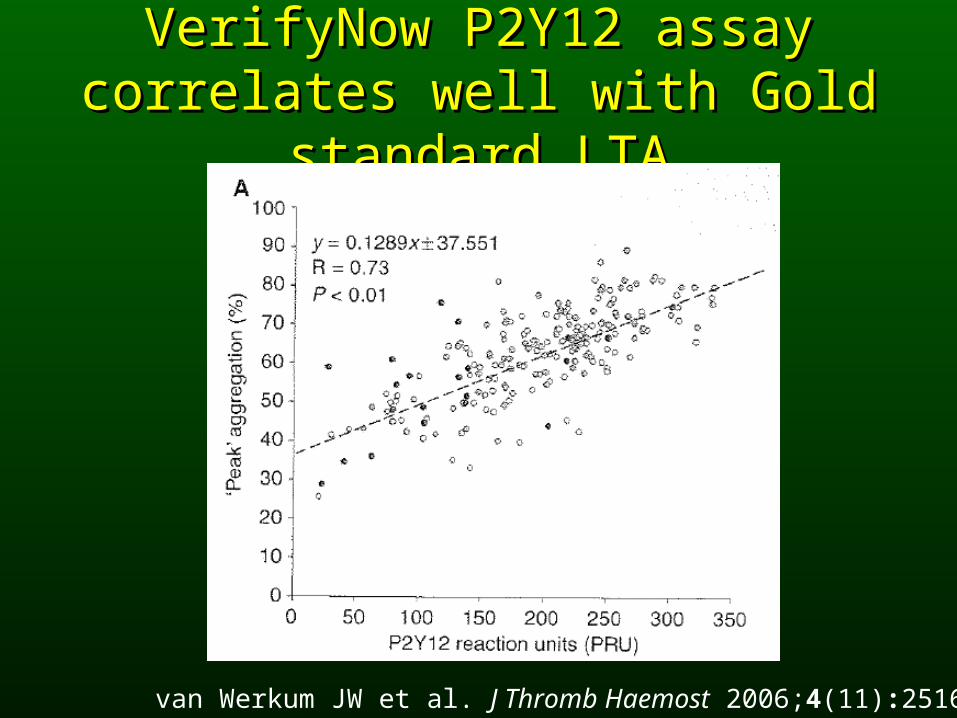
VerifyNow P2Y12 assay correlates VerifyNow P2Y12 assay correlates well with Gold standard LTAwell with Gold standard LTA
van Werkum JW et al. J Thromb Haemost 2006;4(11):2516-8.
Results of the PRINC (Results of the PRINC (PPlavix lavix RResponse esponse iin n CCoronary oronary
IntInteervention) trial.rvention) trial.
Placebo (n=29) Verapamil (n=31) P value Clopidogrel1200mg (n=37)
Clopidogrel 600mg (n=23)
P value Clopidogrel 75 (n=22)
Clopidogrel 150 (n=38)
P value
GenderMale 23(79%) 27(87%) 31(84%) 19(83%) 19(86%) 31(52%) 0.73
Age avg(SD) 64 (11) 71 (9.1) 0.02 70(10) 64(10) 0.06 68(9.4) 68(11) 0.99
EthnicityEuro 27(93%) 30(97%) 35(95%) 22(96%) 22(100%) 35(92%)
Maori 2(7%) 0(0%) 2(5%) 0(0%) 0(0%) 2(5%)
Other 0(0%) 1(3%) 0(0%) 1(4%) 0(0%) 1(3%) 0.7
ASA28(97%) 31(100%) 36(97%) 23(100%) 22(100%) 37(97%) >0.9
300mg 1(3%) 2(6%) 0(0%) 3(13%) 1(5%) 2(5%)
150mg 4(14%) 5(16%) 2(5%) 7(30%) 4(18%) 5(13%)
100mg 23(79%) 24(77%) 34(92%) 13(57%) 17(77%) 30(79%)
75mg 1(3%) 0(0%) 1(3%) 0(0%) 0(0%) 1(3%)
Statin Y 28(97%) 28(93%) >0.9 35(95%) 21(95%) >0.9 21(95%) 35(95%) >0.90
BB 23(79%) 24(80%) >0.9 31(84%) 16(73%) 0.33 17(77%) 30(81%) 0.75
ACE 14(48%) 19(63%) 0.24 20(54%) 13(59%) 0.71 14(64%) 19(58%) 0.36
DM 4(14%) 7(23%) 0.67 7(19%) 4(17%) >0.9 1(5%) 10(26%) 0.04
HTN 18(62%) 16(52%) 0.41 19(51%) 15(65%) 0.29 10(45%) 24(63%) 0.18
CHF 0(0%) 2(6%) 0.49 1(3%) 1(4%) >0.9 1(5%) 1(3%) >0.90
Current Smoker 5(17%) 1(3%) 0.098 3(8%) 3(13%) 0.672(9%) 4(11%) >0.90
Prior CABG 2(7%) 4(13%) 0.67 5(14%) 1(4%) 0.39 3(14%) 3(8%) 0.66
Recent NSTEMI 0(0%) 4(13%) 0.11 2(5%) 2(9%) 0.630(0%) 4(11%) 0.29
Recent STEMI 2(7%) 1(3%) 0.61 1(3%) 2(9%) 0.552(9%) 1(3%) 0.55
Prior PCI 6(21%) 6(19%) >0.9 7(19%) 5(22%) >0.93(14%) 9(24%) 0.51
PVD 5(17%) 8(26%) 0.54 8(22%) 5(22%) >0.9 2(9%) 11(29%) 0.11
FHx CAD 12(41%) 12(39%) 0.83 12(32%) 12(52%) 0.13 10(45%) 14(37%) 0.51
EF avg (SD) 72 (10) 65 (20) 0.29 71(11) 63(24) 0.34 66(23) 69(11) 0.82
LMS disease 0 1 1 0 1 0
1VD 19 21 22 18 13 27
2VD 6 5 9 2 4 7
3VD 1 0 1 0 0 1
Multi stents 4(14%) 5(16%) >0.9 7(19%) 2(9%) 0.46 2(9%) 7(18%) 0.46
DES 9(31%) 12(39%) 0.53 14(38%) 7(30%) 0.56 7(32%) 14(37%) 0.69
BMI avg (sd) 28.4 (4.9) 29.3 (3.9) 0.36 29(5) 28(4) 0.41 28.7(3.8) 28.9(4.8) 0.98
Base PRU 356.3 (44.8) 336.8 (67.3) 0.28 353(64) 335(45) 0.14348(56) 345(60) 0.67
0.50 >0.9
0.38 >0.9
0.23 0.29
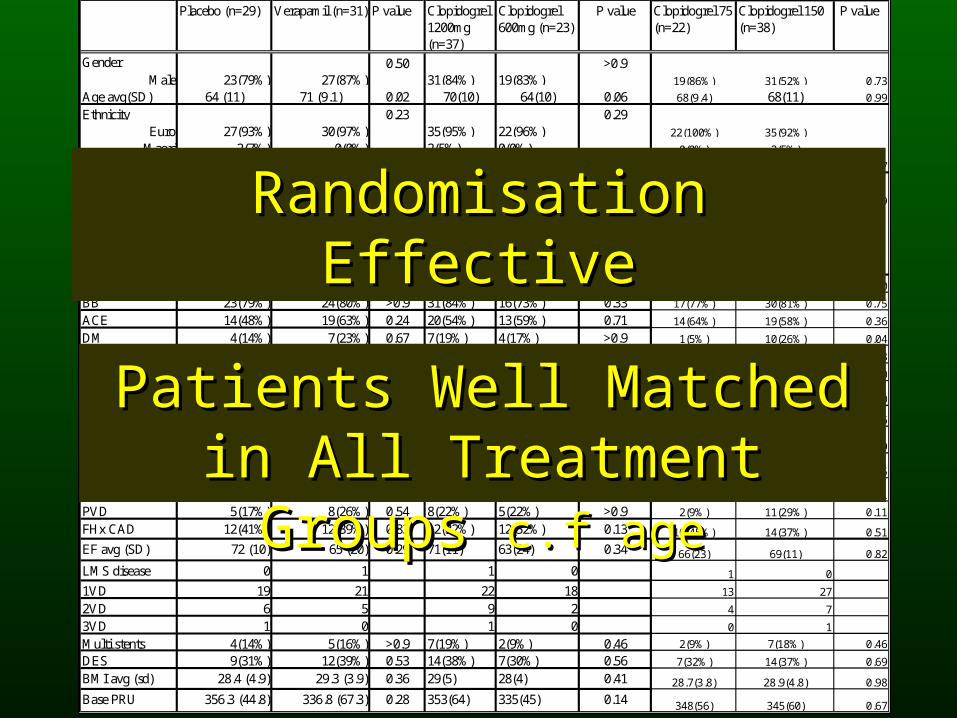
Randomisation EffectiveRandomisation Effective
Patients Well Matched in All Patients Well Matched in All Treatment Groups Treatment Groups c.f agec.f age
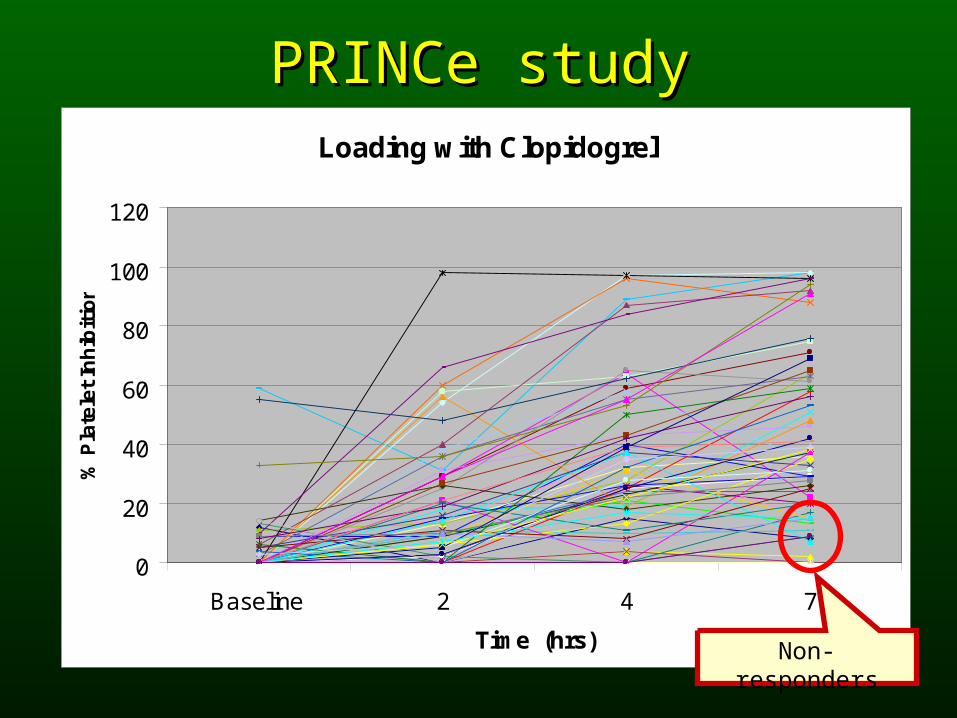
PRINCe studyPRINCe studyLoading with Clopidogrel
0
20
40
60
80
100
120
Baseline 2 4 7
Time (hrs)
% P
late
let
Inh
ibit
ion
Non-responders
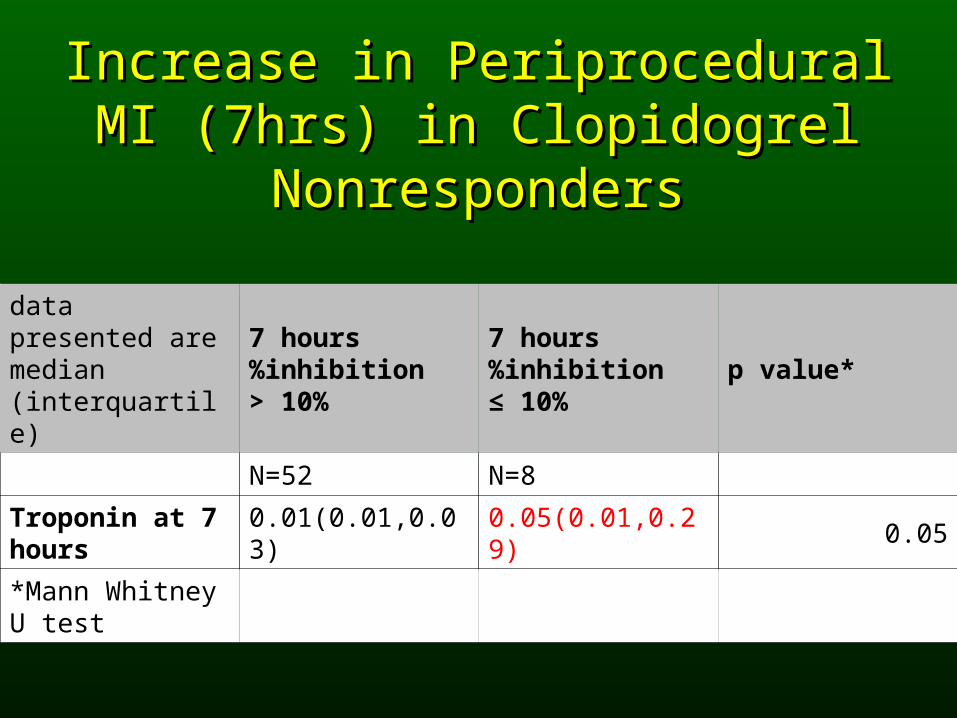
Increase in Periprocedural MI Increase in Periprocedural MI (7hrs) in Clopidogrel (7hrs) in Clopidogrel
NonrespondersNonresponders
data presented are median (interquartile)
7 hours %inhibition > 10%
7 hours %inhibition ≤ 10%
p value*
N=52 N=8
Troponin at 7 hours
0.01(0.01,0.03) 0.05(0.01,0.29) 0.05
*Mann Whitney U test
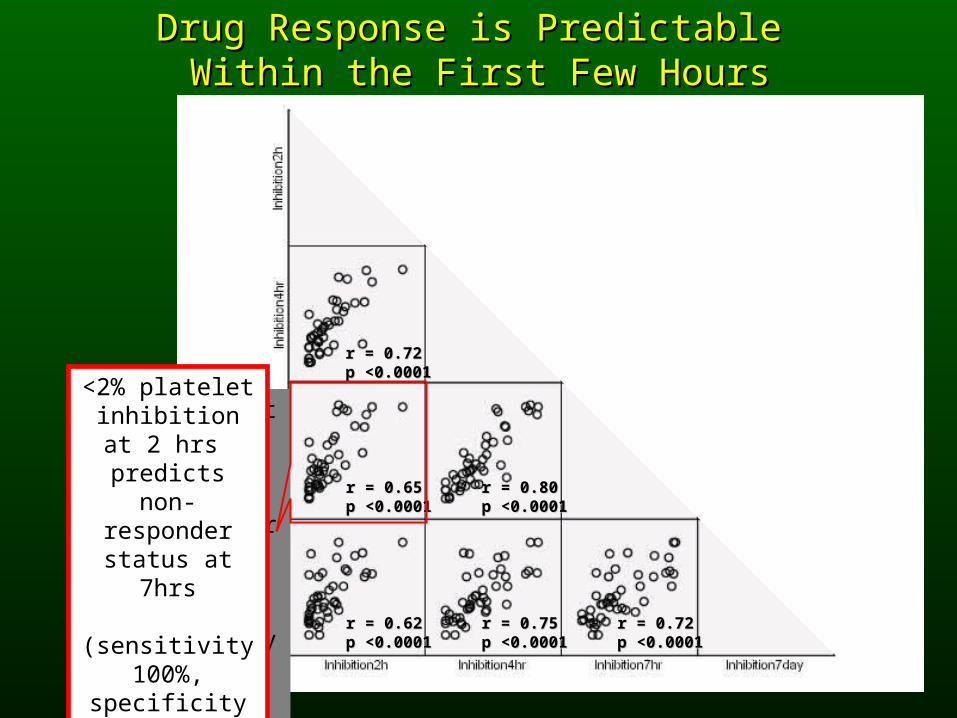
Drug Response is Predictable Drug Response is Predictable Within the First Few HoursWithin the First Few Hours
r = 0.72r = 0.72p <0.0001p <0.0001
r = 0.65r = 0.65p <0.0001p <0.0001
r = 0.62r = 0.62p <0.0001p <0.0001
r = 0.75r = 0.75p <0.0001p <0.0001
r = 0.80r = 0.80p <0.0001p <0.0001
r = 0.72r = 0.72p <0.0001p <0.0001
<2% platelet inhibition at 2 hrs
predicts nonresponder status at 7hrs
(sensitivity 100%, specificity
88%)
<2% platelet inhibition at 2 hrs
predicts non-responder status
at 7hrs
(sensitivity 100%, specificity
88%)
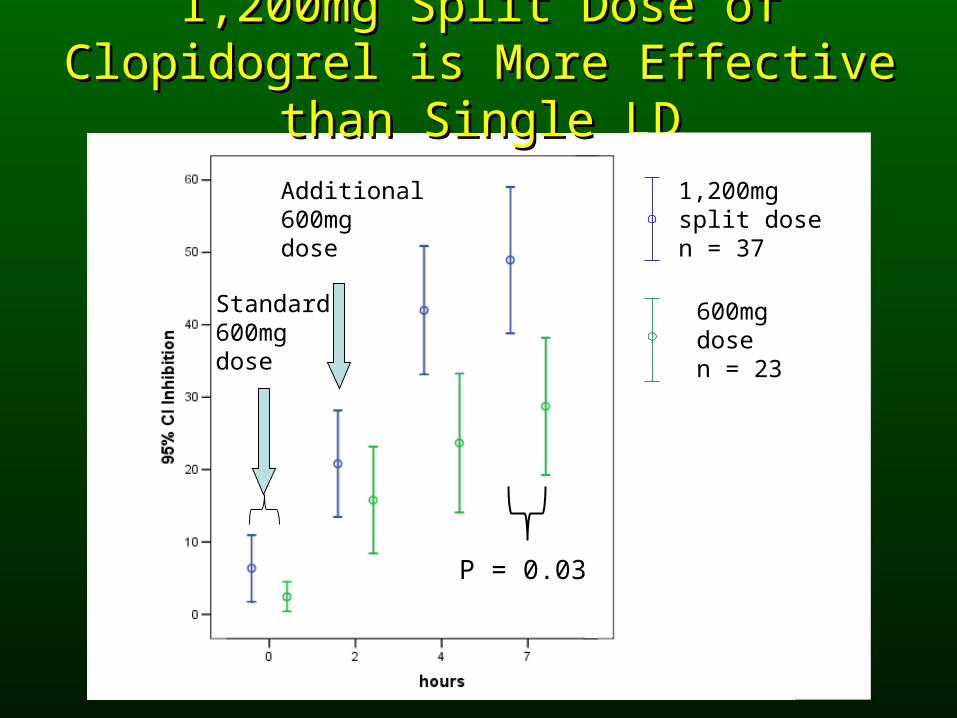
1,200mg Split Dose of Clopidogrel is 1,200mg Split Dose of Clopidogrel is More Effective than Single LDMore Effective than Single LD
P = 0.03
Standard600mg dose
Additional600mg dose
1,200mg split dosen = 37
600mg dosen = 23
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
clopidogrel 150mg clopidogrel 75mg
%in
hib
itio
n
Baseline
%inhibition at 7days
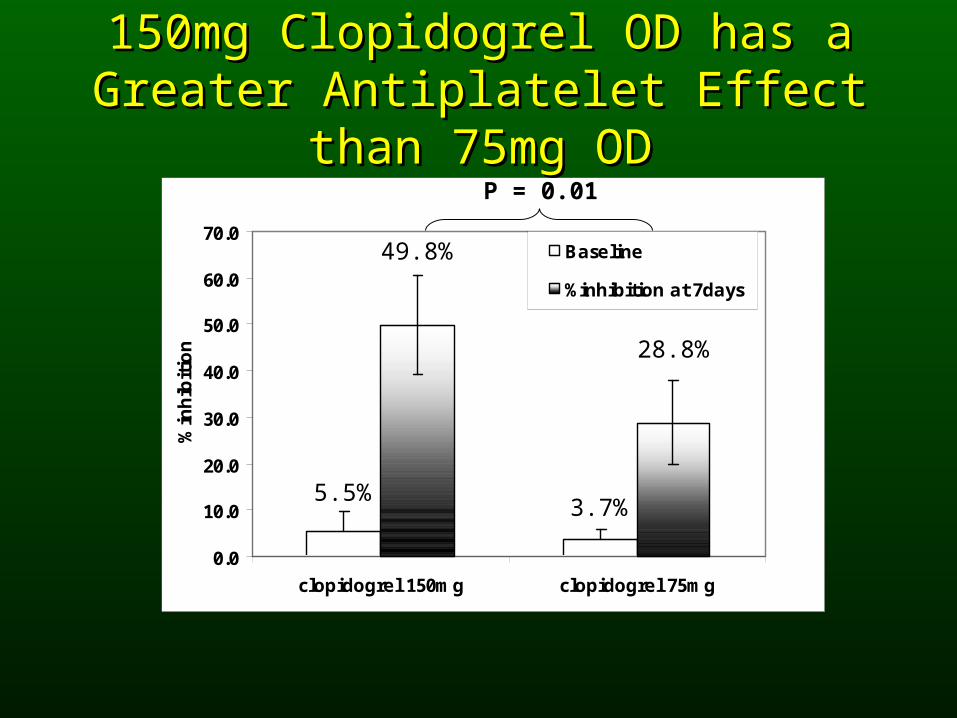
150mg Clopidogrel OD has a Greater 150mg Clopidogrel OD has a Greater Antiplatelet Effect than 75mg ODAntiplatelet Effect than 75mg OD
49.8%
5.5%3.7%
28.8%
P = 0.01
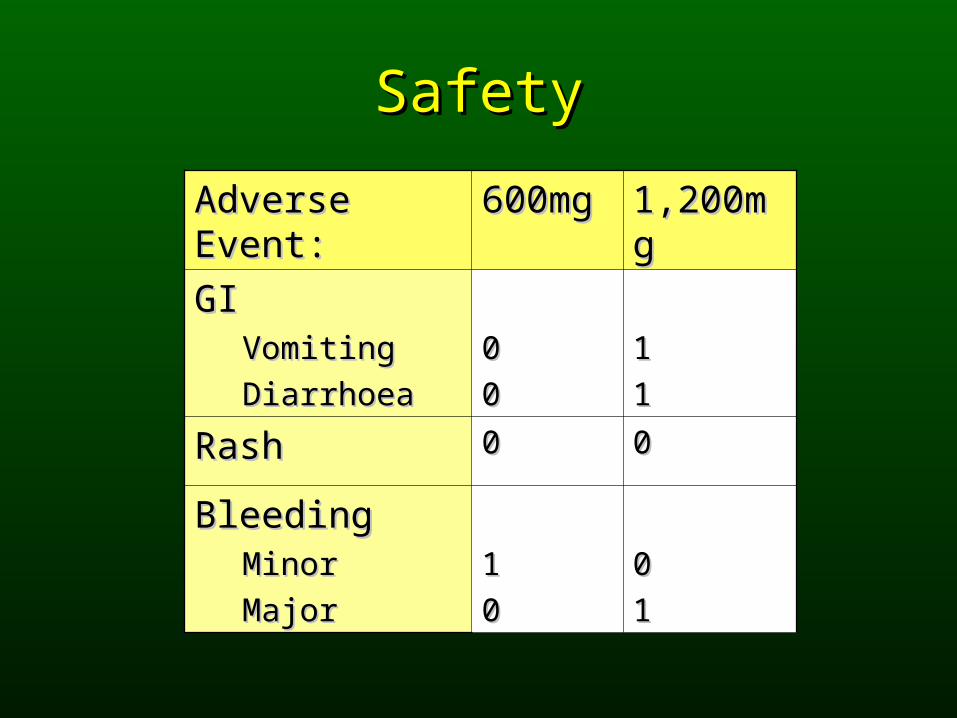
SafetySafety
Adverse Event:Adverse Event: 600mg600mg 1,200mg1,200mg
GIGIVomitingVomiting
DiarrhoeaDiarrhoea
00
00
11
11
RashRash 00 00
BleedingBleedingMinorMinor
MajorMajor
11
00
00
11
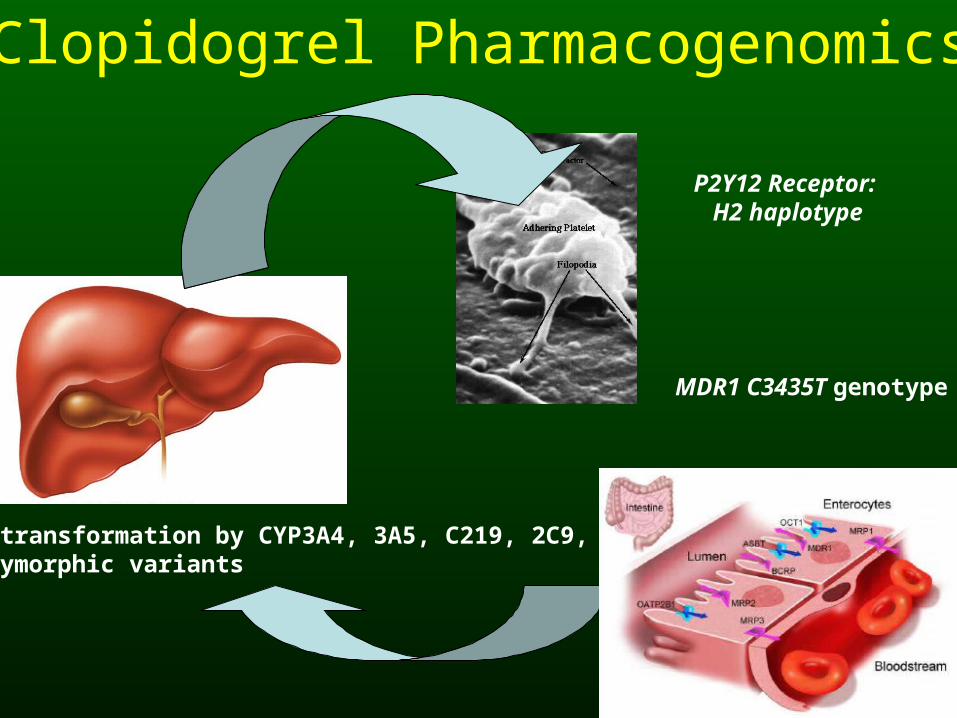
Biotransformation by CYP3A4, 3A5, C219, 2C9, 1A2Polymorphic variants
Clopidogrel Pharmacogenomics
MDR1 C3435T genotype
P2Y12 Receptor: H2 haplotype
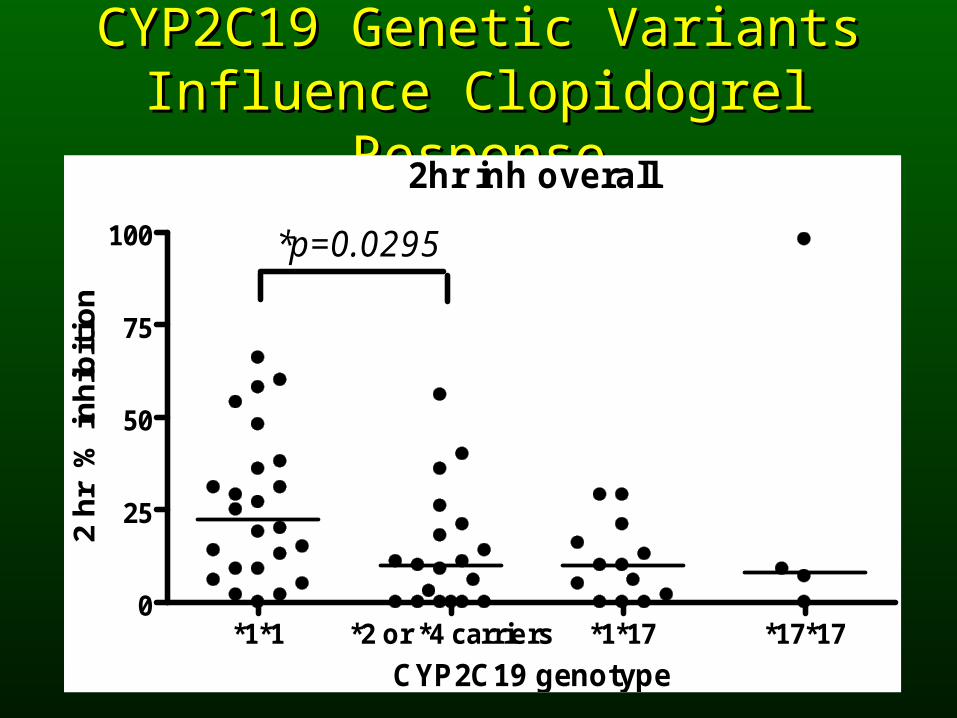
CYP2C19 Genetic Variants CYP2C19 Genetic Variants Influence Clopidogrel ResponseInfluence Clopidogrel Response
2hr inh overall
*1*1 *2 or *4 carriers *1*17 *17*170
25
50
75
100 *p=0.0295
CYP2C19 genotype
2 h
r %
in
hib
itio
n
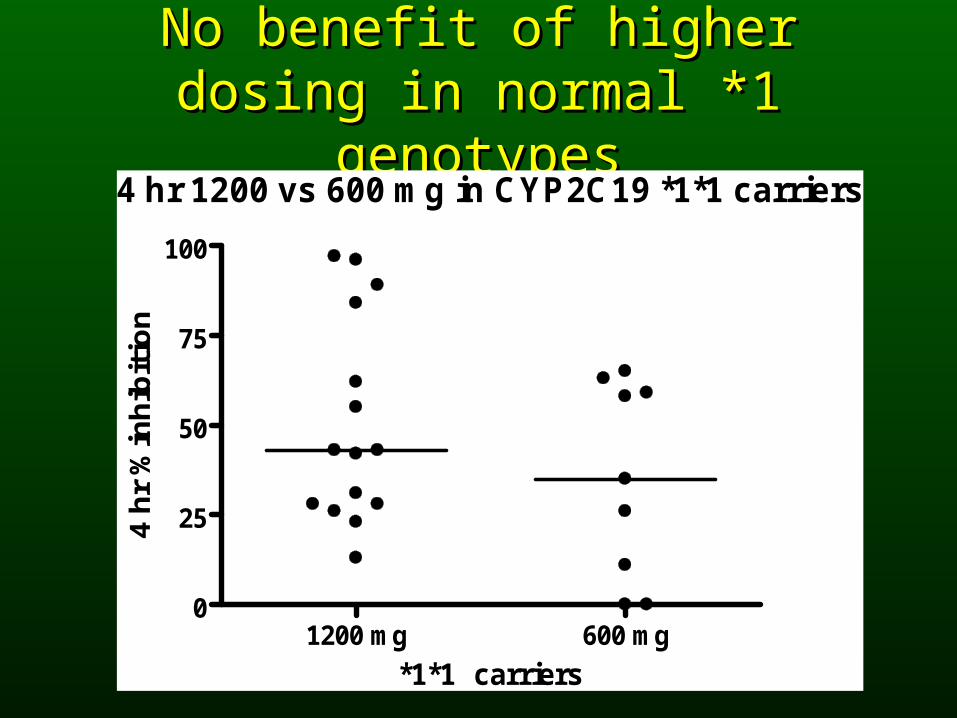
No benefit of higher dosing in No benefit of higher dosing in normal *1 genotypesnormal *1 genotypes
4 hr 1200 vs 600 mg in CYP2C19 *1*1 carriers
1200 mg 600 mg0
25
50
75
100
*1*1 carriers
4 h
r %
inh
ibit
ion
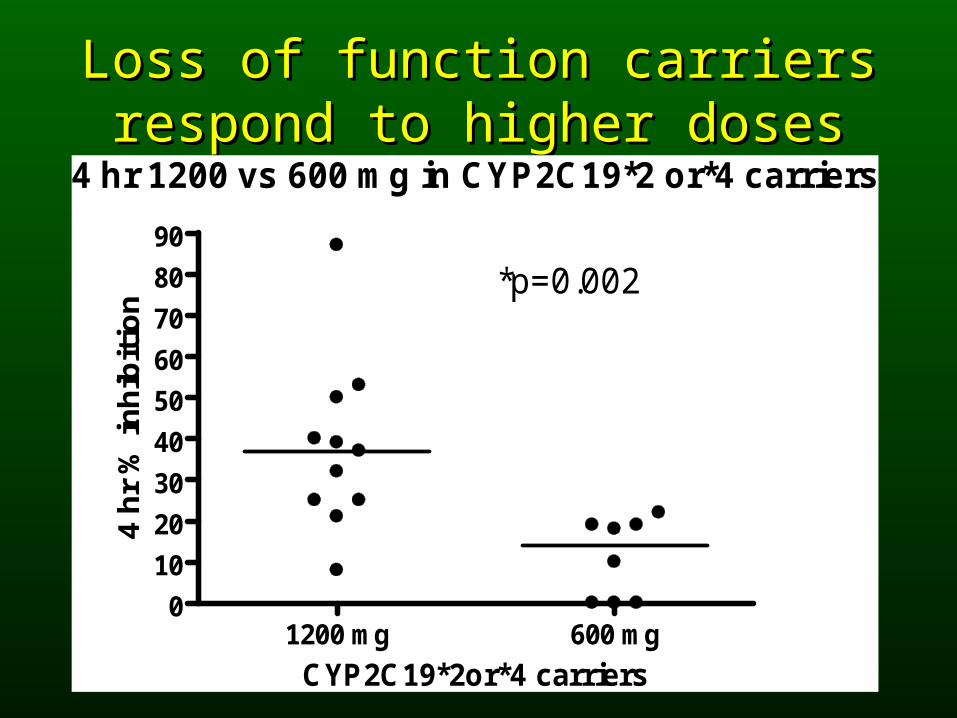
Loss of function carriers respond to Loss of function carriers respond to higher doseshigher doses
4 hr 1200 vs 600 mg in CYP2C19*2 or*4 carriers
1200 mg 600 mg0
10
20
30
40
50
60
70
80
90
*p=0.002
CYP2C19*2or*4 carriers
4 h
r %
in
hib
itio
n
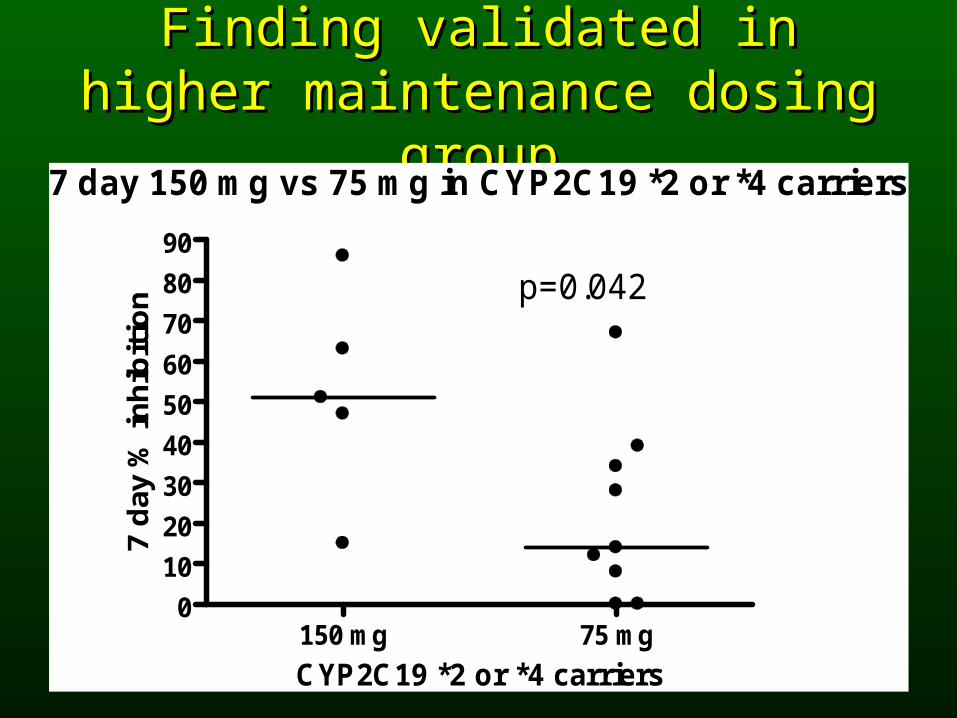
Finding validated in higher Finding validated in higher maintenance dosing groupmaintenance dosing group
7 day 150 mg vs 75 mg in CYP2C19 *2 or *4 carriers
150 mg 75 mg0
10
20
30
40
50
60
70
80
90
p=0.042
CYP2C19 *2 or *4 carriers
7 d
ay %
in
hib
itio
n
ConclusionConclusion
• Split loading with 600mg + 600mg (2hrs) Split loading with 600mg + 600mg (2hrs) clopidogrel increases the antiplatelet effectclopidogrel increases the antiplatelet effect
• 150mg OD > 75mg OD antiplatelet effect150mg OD > 75mg OD antiplatelet effect
• Response can be measured robustly with Response can be measured robustly with a POC analyser & predicted early (2hrs)a POC analyser & predicted early (2hrs)
• Pharmacogenetics might predict response Pharmacogenetics might predict response before Rx but phenotyping is still very before Rx but phenotyping is still very effectiveeffective
Jo PerryJo Perry
Mark WebsterMark Webster
Ralph StewartRalph Stewart
Irene ZengIrene Zeng
Helen FarrellHelen Farrell
Arzu GunesArzu GunesM-L DahlM-L Dahl
Auckland City Hospital Pharmacy Auckland City Hospital Pharmacy Clinical Trials UnitClinical Trials Unit







