Download - Occupational health lect 4th year mbbs

D R A M B R E E N A N S A R
1

Aim
Students should be able to apply the basic principles of occupational medicine to their professional practice as doctors.
2

Objectives
At the end of the unit student should be able to:
Delineate occupational health, occupational hygiene, ergonomics, occupational diseases & Injuries.
Enlist occupational disease agents and factors (physical, chemical, biological, psychological, mental).
Identify factors or patterns in a patient’s history that may indicate a work related contribution to ill health.
Suggest preventive and/or corrective measures.
3

Layout of our study plan4
Introduction and physical hazards
Chemical hazards
Biological hazards
Occupational diseases
Occupational disorders
Occupational accidents
Ergonomics

Occupational Medicine/Health
a branch of medicine concerned with the interaction between health and work (“occupation”)
The joint international labor organization committee on Occupational health, 1950 defined occupational health as
“The highest degree of physical, mental and social well-being of workers in all occupations.”
5

Occupational/industrial hygiene
“The science and art devoted to the anticipation, recognition, evaluation and control of environmental factors/stresses that arise in a workplace and that may cause sickness, impaired health and well being or discomfort and inefficiency among workers or citizens of the community.”
6

ERGONOMICS7
Ergonomics is the study of men at work with a view to identify the stress factors operating in work environments and impairing the health of the workers and interfering with their work performance.

Why is occupational health and safety important?
8

Why is occupational health needed?
Is responsible for the promotion and maintenance of the highest degree of physical, mental and social well-being of workers in all occupations.
Prevents that workers have adverse effects on health caused by their working conditions.
9

Case scenario
Suppose you are an occupational physician.
A 31-year-old laboratory technician is referred to yourclinic by her manager, because of alleged latenessand poor performance at work. You are asked toassess whether there is an underlying medical causefor this.
10

History
She tells you that she has not been sleeping well lately, possibly due to nocturnal coughing. She says the lab is cold and damp and that by the end of the working day her right arm is aching. She says that when she told her manager, he was unsympathetic; telling her she should leave if she doesn’t like the job.
11

Scenario 212
A brick kiln laborer was brought unconscious to the emergency. He was hypotensive and sweating profusely.

Scenario 313
A person employed in the welding section of an automobile manufacturing plant reported
sick with redness of eyes and impaired vision. Examination confirmed the diagnosis of conjunctivitis.

QUESTIONS
1. What are the presenting medical problems?
2. What are the possible work-related causes of theirsymptoms?
3. How might you classify the potential hazards intheir workplace?
4. How will you respond to the manager’s questions?
5.What preventive measures will you suggest for thesepatients?
14

Aims of occupational health
1. To IDENTIFY & bring under control all the agents (physical, chemical, biological, mechanical & psychological) that are known or suspected to be hazardous.
2. To ENSURE that the physical & mental demands imposed on people match with their physiological & psychological capabilities, needs & limitation.
15

Aims of occupational health
3. To PROTECT the vulnerable and enhance their resistance to adverse working conditions.
4. To DISCOVER and IMPROVE work situation that contribute to the ill-health of workers.
5. To EDUCATE management and workers to fulfill their responsibilities relevant to health protection and promotion.
6. To CARRY OUT comprehensive in-plant health programmes which deal with man’s total health.
16

Main activity areas of occupational health
1. Identification & improvement
2. Matching & protection
3. Education & motivation
4. Holistic approach
17

Types of diseases among workers
Occupational diseases are restricted to predisposed occupational groups and are not seen in non-occupational settings. For example occupational skin disorders, occupational cancers etc.
There may be non-occupational diseases which are prevalent in the community outside the occupational settings. For example cholera, typhoid, malaria etc.
18

Types of diseases among workers
Partly occupational diseases or work related diseases are comparatively more frequent among industrial workers for example IHD, HTN, Peptic ulcer & psychosomatic illnesses.
19

FUNCTIONS OF OCCUPATIONAL HEALTH SERVICE
1. Pre-employment medical examination.
2. First Aid and emergency service.
3. Supervision of the work environment for the control of dangerous substances in the work environment.
4. Special periodic medical examination particularly for the workers in dangerous operations.
5. Health education for disseminating information on specific hazards and risks in the work environment.
20

6. Special examination and surveillance of health of women and children.
7. Advising the employer or management for improving working conditions, and placement of hazards.
8. Monitoring of working environment for assessment and control of hazards.
9. Supervision over sanitation, hygiene and canteen facilities.
FUNCTION OF HEALTH SERVICE - CONT..
21

FUNCTION OF HEALTH SERVICE - CONT..
10. Liaison and cooperation with the safety committees
11. Maintenance of medical records for medical check-up and follow-up for maintaining health standards and also for evaluation.
12. To carry out other parallel activities such as nutrition programme, family planning, social services recreation
etc. Concerning the health and welfare of the workers.
22

Types of occupational environment
Internal environment:
Industrial settings, offices, schools, hotels, hospitals, labs, & all government and private establishments.
External environment:
Extra industrial like environment for farmers, sailors, sheep herders, construction workers and other field workers.
23

Residential environment:
66% of time is spent at homes; if congenial & comfortable it will favourably effect industrial environment.
24

Occupational hazards
May be categorized in two ways:
According to target organ system
According to type of agent involved
25
a. According to type of agent involved
Physical hazards
Chemical hazards
Biological hazards
Psychosocial hazards
26

1. Physical hazards
1. High or low temperatures
2. Low pressures
3. Vibration
4. Noise
5. Ionizing radiation
6. Non-ionizing radiation
27

High temperature28

1. High temperatures
Decrease efficiency
Increased fatigue
Increased accident rates
Heat cramps
Heat exhaustion
Heat stroke
29

Comfort zone lie between:
69-80 ◦F or
20-27 ◦C
Occupations at risk:
Radiant heat in foundry, glass & steel industry
Heat stagnation in jute & cotton industry.
30
2. Low temperatures
Chilblains
Trench foot
Frost bite
Occupational exposures among:
Caisson workers, commercial fisherman, divers, dairy workers, refrigerator repairmen & outside workers in cold northern regions.
31

32

33

Prevention & control
2. Case management
3. Health education
34
1. Personal protection
1. Clothing
1. Warm/Light
2. Heat resistant
2. Metal heat refractors
3. Periodic salt & water
intake
4. Ear muffs
5. Goggles
6. Aprons and boots
7. Regulated exposure of
workers

3. Low pressures (at high altitude)
Manifestations of air expansion
Barodontalgia
Barosinusitis
Barotitis
Emphysema
Abdominal distention
35
3. Low pressures (at high altitude)
Manifestations of nitrogen effervescence
Bends
Chokes
Prickles
Paralysis
Aseptic bone necrosis
36

3. Low pressures (at high altitude)
Occupations at risk are:
Aviators, deep sea divers, balloonists, air passengers, tunellers etc.
37

4. Noise
Sound that is unwanted or disrupts one’s quality of life is called as noise. When there is lot of noise in the environment, it is termed as noise pollution
Auditory effects
Non- auditory effects
Factors affecting noise injury are intensity, frequency, range, duration of exposure & individual susceptibility.
38
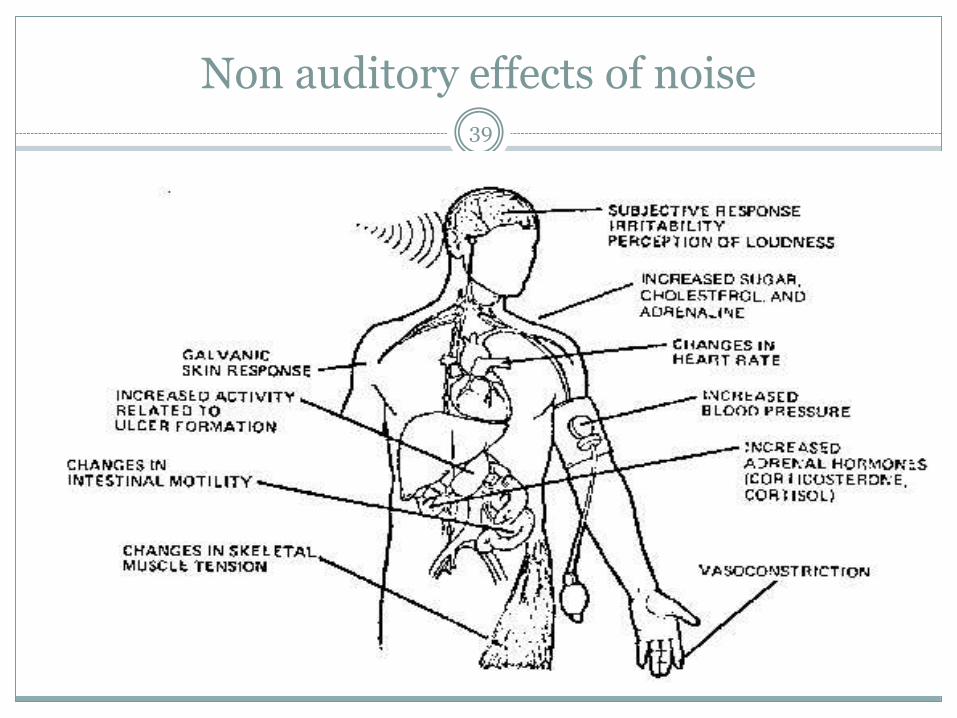
Non auditory effects of noise 39

40

Control measures41
Industrial measures Substitution:
For example riveting by welding, chipping by grinding, spur gears by spiral gears, blunt tools by sharp tools.
Reduction: By proper maintenance of machine and equipment, replacement of
worn out parts, lubrication of moving components etc.
Enclosure: Creating a sound proof barrier between machine and work area.
Soundproofing: To reduce the reverberation of noise Asbestos fibers, vegetable fibres, glass wool, mineral wool used as
blankets, blocks or panels.
Health education Legislation

5. Vibration
Long term exposure to 10-500hz may lead to: Vibration sickness
Whitening & numbness of fingers
Reactive hyperemia
Neurogenic damage
Osteoarthritic changes
Damaged tendons, ligaments & nerves
Occupational exposure among users of rotary discs, grinding wheels, drills, chisels & hammers etc.
42

6. Non-ionizing radiation
That do not cause ionization of tissues upon penetration. These include:
Infra red
Ultra violet
Microwave radiations
Laser beams
43

Thermal damage to eyes; injury to cornea, iris or lens
Acute skin burn with hyper pigmentation.
UV radiation is carcinogenic in addition to causing photokeratitis, conjunctivitis, erythema, sunburn, premature ageing of skin, pre-malignant and malignant conditions.
44

Microwave injuries include corneal injuries, lens opacities, frank cataract, retinal damage and testicular damage with decreased sperm count.
Laser injuries include corneal, retinal and cutaneous burns to field construction workers who se lasers to obtain alignment of dams, tunnels and pipes etc.
45

Sources of radiations46

7. Ionizing radiation
Exposure occur among workers of radiology department
Agents are Co 60, I 131, S 35, Krypton 85,K 42, Ce 137, Plutonium 139 & Ph 32
Maximum permissible range is 5 rem/yr/whole body
47

Health effects of acute exposure48

49

Protection from radiation50
Industrial measures:
Personal hygiene
Not to eat or smoke in restricted areas, no pipetting of radioactive solutions, no handling of isotopes with open wound, wash exposed parts before leaving the active area.
personal protection,
Use lab clothing and overalls, rubber gloves, canvas shoe covers, face sheilds, safety goggles, self contained breathing apparatus.
safety education,
51
radiation monitoring,
Use of Radiation monitoring devices such as film badges, pocket ionizing chambers, pocket dosimeters.
source shielding.
Gamma and x ray emitters in concrete chambers, neutron emitters in water. Paraffin or hydrogen containing substance, beta radiators in thin plastics, aluminium and thick rubber gloves.

Protection from physical hazards
1. Personal protection
1. Personal protective equipment
2. Regulated exposure to working environment
2. Case management
3. Health education
52

2. Chemical hazards
These hazards act in three ways:
Inhalation
Gases
Asphyxiant gases: CO, HCN, H2S
Irritant gases: chlorine, ammonia, SO2
Toxic gases: arsine & stibine
Inert gases: CO2, methane, nitrogen
Dusts
Organic: cotton fibre, sugar cane fibre, hay dust, tobacco
Inorganic: silica, asbestos, coal, iron
Ingestion & Local action
Metals
Type A intoxicants: with local action cadmium, beryllium, nickel
Type B intoxicants: lead, mercury, manganese
53

1. Gases which pose occupational threat
1. Asphyxiant gases:
Carbon monoxide:
Exposure to workers in electric, oil or blast furnaces, gas manufacturing plants, ovens, mines etc
It cause anaemic anoxia by forming carboxyhemoglobin.
Symptoms include: headache, dizziness, CNS manifestations.
Prevention:
public education on the safe operation of appliances, heaters, fireplaces, and internal-combustion engines,
emphasis on the installation of carbon monoxide detectors.
Equipment maintainence.
54

Symptoms of CO poisoning55

Hydrogen sulphide:
Exposure to sewers, miners breweries, tannaries.
It paralyses the respiratory center.
Symptoms include photophobia, lacrimation, salivation, chemosis, blurring.
HCN:
It interferes with respiratory enzymes which are necessary for tissue oxidation; leads to histolytic anaemia.
Exposure occurs among foundry workers, dye markers, petroleum refineries, smelters.
Symptoms include constriction of chest, hyper apnea, palpitations, convulsions and unconsciousness.
56

57
2. Irritant gases:
All three gases effect the mucous membrane of ENT & respiratory tract causing burning sensation, lacrimation, chemosis, conjunctivitis, rhinitis, coughing, sneezing, salivation & finally leading to pulmonary edema.
Ammonia
• skin
Sulpherdioxide
• GIT
Chlorine gas
• Nausea vomiting

58
Exposure to chlorine: in dye, textile, paper & chemical industries where chlorine is used as bleaching or disinfecting agent.
Exposure to ammonia: in workers engaged in refrigeration, cold storage & artificial ice-manufacturing plants.

59
3. Toxic gases: Arsine
Invade RBCs and lead to hemolysis, hemolytic anaemia, haemoglobinuria Garlic like odour. Arsine emits toxic fumes of arsenic when heated to decomposition
Stibine: It invades CNS and cause cerebral edema & depression of respiratory
symptoms.
Exposure occur among workers of semiconductor and metal refining industries.
In the event of a fire involving arsine or Stibine, use fine water spray and liquid and gas tight chemical protective clothing with breathing apparatus

60
4. Inert gases: Nitrogen, Methane & Carbon dioxide.
These gases lead to anoxic anoxia by diluting the concentration of oxygen in air. When O2 falls below 12% deep breathing starts At 10% markedly deep breathing occurs At 8% cyanosis of lips and face is seen At 5% consciousness is clouded leading to coma
Exposure to CO2 occur in mines, tunnels, vaults, cellars, tanks & from decomposition of sewage.
Exposure to nitrogen occur in wells, caves & mines. Exposure to methane occur in coal mines

2. Dusts causing occupational diseases61
Detrimental effects of dusts depend upon the following factors: Fineness i.e size of the particle:
Particles >10 µm -----settle down due to gravity
Particles < 10 µm-----remain suspended in air
Particles 5-10 µm-----arrested in upper respiratory tract
Particles 3-5 µm-------deposited in mid respiratory tract
Particles 1-3 µm-------enter and settle in alveoli
Particles <1 µm--------are constantly in Brownian movement and settle only when caught by alveoli and adhered to them
Concentration in air
Duration of exposure
Susceptibility of individual

Fate of dust particle62
The fate of dust particle is decided by their nature
Organic or inorganic
Soluble or insoluble
Inert or fibrogenic
Soluble dust particles are dissolved and absorbed into systemic circulation and eliminated by metabolic process.

63
Insoluble dust particles are handled by our physiological responses like coughing, sneezing, mucociliary activities and defense mechanisms of phagocytes.
When these mechanisms are overwhelmed the dust particles start accumulating in lungs. If these insoluble particles are fibrogenic they will initiate a reaction leading to “pneumoconiosis”

Pneumoconiosis 64
Is categorized in two ways:
1. Inorganic dusts Organic dusts
DUST DISEASE DUST DISEASE
1. Coal Anthracosis 1. Cane fiber Bagassosis
2. Silica Silicosis 2. Cotton dust Byssinosis
3. Asbestos Asbestosis 3. Tobacco Tobacosis
4. Iron Siderosis 4. Hay/ Grain dust
Farmer’s lung

Pneumoconiosis 65
2.
Classification Types of pneumoconiosis
1. Major pneumoconiosis Silicosis, Anthracosis, asbestosis
2. Minor pneumoconiosis Bagassosis, Byssinosis
3 . Benign pneumoconiosis Siderosis

Comparative features of different types66
Features Silicosis Asbestosis Anthracosis
1. Agent/ dust •Silica free or silicon dioxid or silicic acid
•Particles are 0.5 -3 µ are most dangerous.
•Asbestos fibres1. Serpentine or
chrysolite(safer)
2. Amphibolei. Crocidolite
(blue)ii. Amosite
(brown, safer)iii. Anthrophylite
(white)• 20-500µ in
length and 0.5-50 µ in diameter
• Coal dust

Silicosis
Silica free or silicon dioxid or silicic acid
Particles of size 0.5 -3 µ are most dangerous.
Occupational exposure Mining, pottery, ceramic, sand blasting, metal
grinding, building & construction work, rock mining, iron & steel industry.
67

Pathogenesis Fibrosis is initiated by silicic acid leading to nodular fibrosis,
emphysema, and right heart failure. Pulmonary tuberculosis may intervene in 50% of cases.
Dense nodular fibrosis 3-4 mm nodules and in upper part of lung.
Symptoms:
Irritant cough, dyspnea on exertion & pain in chest.
X-ray shows “snow-storm” appearence
68

Asbestosis
Causative agent: Asbestos fibres1. Serpentine or chrysolite (safer)2. Amphibole
Crocidolite (blue) Amosite (brown, safer) Anthrophylite (white)
20-500µ in length and 0.5-50 µ in diameter
69

Occupational exposure:
Manufacturers of Asbestos cement, fire proof textiles, roof tiling, brake lining & gaskets
Pathogenesis: Asbestos fibers initiate fibrosis of pulmonary tissue,
emphysema and its associated complications. Fibrosis is due to mechanical irritation, it is peri-bronchial,
diffuse and basal in location. Mesothelioma is commonly associated with asbestosis.
Symptoms: Dyspnea out of proportion, clubbing, cyanosis, cardiac
distress.
70

Sputum shows “asbestos bodies”.
X-ray shows ground glass appearance.
71

Comparative features of different types72
Features Silicosis Asbestosis Anthracosis
Occupational exposure
Mining, pottery, ceramic, sand blasting, metal grinding, building & construction work, rock mining, iron & steel industry.
Manufacturers of Asbestos cement, fire proof textiles, roof tiling, brake lining & gaskets.
Coal miners, coal processors & coal handlers and those manufacturing carbon electrodes.
Incubation period 6 months to 6 years
12 years

Comparative features of different types
73Features Silicosis Asbestosis Anthracosis
Pathogenesis Fibrosis is initiated by silicic acid leading to nodular fibrosis, emphysema, and right heart failure. Pulmonary tuberculosis may intervene in 50% of cases.Fibrosis is nodular and in upper part of lung.
Asbestos fibers initiate fibrosis of pulmonary tissue, emphysema and its associated complications.Fibrosis is due to mechanical irritation, it is peri-bronchial, diffuse and basal in location
•Coal dust initiates diffuse and massive fibrosisa. Simple
pneumoconiosis with ventilatory impairment.
b. Progressive massive fibrosis leading to emphysema and right heart failure.
Clinico-Pathologicfeatures
Irritant cough, dyspnea on exertion& pain in chest. Dense nodular fibrosis3-4 mm nodules.X-ray shows “snow-storm” appearence
Dyspnea out of proportion, clubbing, cyanosis, cardiac distress.Sputum shows “asbestos bodies”.X-ray shows ground glass appearance.
•From little ventilatory impairment to severe respiratory disability leading to pre-mature death.

Silicosis, Anthracosis & asbestosisX-ray findings
74
Byssinosis
Inhalation of cotton fiber dust
Symptoms: Chronic cough, progressive
dyspnea ending in chronic bronchitis and emphysema.
Occupational exposure: Textile industry
75

Bagassosis76
Inhalation of bagasse sugar cane dust containing thermophilic actinomycete, thermoactinomyces sacchari
Symptoms: Breathlessness, cough, haemoptysis, and
slight fever.
Occupational exposure: Manufacturing of paper, cardboard and
rayon.

Farmer’s lung
Inhalation of mouldy hay or grain dust containing thermophilic actinomycetes, Micropolyspora faeni
General & respiratory symptoms with physical signs.
77

Comparative features of different types
Features Byssinosis Bagassosis Farmer’s lung
Causative agent Inhalation of cotton fiber dust
Inhalation ofbagasse sugar cane dust containing thermophilicactinomycete, thermoactinomyces sacchari
Inhalation of mouldy hay or grain dust containing thermophilicactinomycetes, Micropolysporafaeni
Symptoms Chronic cough, progressive dyspnea ending in chronic bronchitis and emphysema.
Breathlessness, cough, haemoptysis, and slight fever.
General & respiratory symptoms with physical signs.
Occupational exposure
Textile industry Manufacturing of paper, cardboard and rayon.
78

Control of pneumoconiosis
Rigorous dust control measures Substitution, enclosure, isolation, hydroblasting, good house
keeping, personal protective measures
Regular physical examination of workers.
Periodic examination of workers, biological monitoring (X-ray & Lung function)
Personal protection Masks, respirators with mechanical filters
Regulated exposure
Health education
79

Bagassosis:
Bagasse control
Keep moisture content above 20%, spray bagasse with 2% propionic acid.
Asbestosis:
Use of safer types of asbestos (chrysolite & amosite)
Substitution with other insulants: glass fiber, mineral wool, calcium silicate. Plastic foams etc.
80

3. Aerosols
Aerosols of various type are released in metal-processing industries during smelting, mining & refining operations.
Inhalation of aerosols by workers result in metal intoxication manifested by metal-fume fever, pulmonary disease and systemic disease.
Accidental ingestion or their absorption through exposed skin leads to disturbances of alimentary tract & various dermatitis.
81

Group A intoxicants:
Aerosols interacting at local level, lesions restricted to skin and respiratory tract.
They include chromium, beryllium & nickel aerosols.
Group B intoxicants:
Aerosols interacting at distal levels invaribly affecting CNS besides other target organs.
They include lead, mercury and manganese.
82

Lead poisoning
Occupational exposure:
Production of batteries, welding & flame cutting of lead, moulding of lead containing alloys in foundries, lead soldering, spray painting with lead paints and grinding or sand blasting of lead alloys.
Sign & symptoms:
Lead encephalopathy:
delerium, coma, convulsions, mental dullness, transient paresis & toxic psychosis.
Chronic exposure result in poor memory, poor concentration, headache, transitory deafness and trembling.
83

84
Lead palsy:
Wrist drop, ankle drop
Lead ophthalmopathy
Diminution of visual fields, papilloedema, secondary atrophy and post neurotic atrophy of disc which may lead to permanent blindness.
Lead anemia:
Hypochromic ass with reticulocytosis and stipled cells.
Lead colic:
Peri-umblical or su-umblical area, preceeded by constipation characterized by severe pain and perspiration.
Lead line:
It is a dark blue stippled line on gums about 1mm from gingival margin.
Diagnosis of lead poisoning
History
Clinical features
Lab diagnosis
Coproporphyrin in urie (CPU)
Useful screening test. Levels in non-exposed persons are less than 150µg/l
Aminolevulinic acid in urine (ALAU)
If it exceeds 5mg/l, it indicates clearly lead absorption.
Lead in blood & urine:
Quantitative indicators of exposure
In urine >0.8mg/l indicates lead exposure (0.2-0.8 is normal)
In blood >70 µg/100ml is associated with clinical symptoms.
85

At levels above 80 µg/dL, serious, permanent health damage may occur (extremely dangerous).
Between 40 and 80 µg/dL, serious health damage may be occuring, even if there are no symptoms (seriously elevated).
Between 25 and 40 µg/dL, regular exposure is occuring. There is some evidence of potential physiologic problems (elevated).
Between 10 and 25 µg/dL, lead is building up in the body and some exposure is occuring.
• https://www.health.ny.gov/publications/2584/
86

Preventive measures
Substitution:
Isolation
Local exhaust ventilation
Personal protection
Good house keeping
Working atmosphere:
Lead concentration should be kept below 2mg/10m3.
Periodic examination of workers
Personal hygiene
Health education
87

Match the diseases related to the occupations shown in following pictures.
88

89

SILICOSIS
90

91

FARMER’S LUNGAND WHAT ELSE
92

93

MUSCULAR CRAMPSDUE TO DEHYDRATION & HEAT
94

95

W O O L S O R T E R ’ S D I S E A S E
A N T H R A X
96

Occupation related psychological and behavioural disorders
A healthy social climate (any industry or institution)
Increase the morale of workers
Increase their output
An unhealthy social climate
Psychological stress
Workers lose interest in their jobs
They are apprehensive, irritable and unsocial.
97

Behavioural changes
Minor changes like petty jealousies, fault finding & craving for undue attention
Leading to major psychological and behavioural disorders like absenteeism & occupational cramps
98

1. Absenteeism 99

Absenteeism
It is the practice of remaining absent from workfor one reason or the other.
Means staying absent from work on account of sickness or injury.
Only 10% of sickness is of occupational origin therefore, valid for compensation.
100
Sickness Absenteeism

History of the lab worker!!!
She tells you that she has not been sleeping well lately, possibly due to nocturnal coughing. She says the lab is cold and damp and that by the end of the working day her right arm is aching. She says that when she told her manager, he was unsympathetic; telling her she should leave if she doesn’t like the job.
101

QUESTIONS
1. What are the presenting medical problems?
2. What are the possible work-related causes of theirsymptoms?
3. How might you classify the potential hazards intheir workplace?
4. How will you respond to the manager’s questions?
5.What preventive measures will you suggest for thesepatients?
102

103

Side effects of absenteeism
Beyond acceptable levels it promotes:
among regular workers
Annoyance and frustration
Reduces their morale
Increases their workload
Interferes with production of goods in industries
Increases the cost of finished items
104

It is a multifactorial disorder
Personal reasons
Occupational reasons
Organizational reasons
Social reasons
105

a. Predisposing personal factors
Young age
Immaturity
Emotional instability
Short length of service
Lack of personal motivation
Destructive life style
Excessive smoking
Alcohol consumption
106

b. Predisposing occupational factors
Poor physical work environment
Unpleasant nature of work
Shift work system
High degree of motivation
No incentives for better work performance
107

c.Predisposing organizational factors
Hostile administrative climate
Hostile management attitude
Poor interpersonal relationship
Lack of worker participation in decision making
Authoritarian leadership style
Lack of economic incentive for better work
Irresistible sickness insurance
108

d. Societal or external factors
Availability of ample employment opportunities
Lack of social pressure that discourage staying at home
109

Prevention of absenteeism
Good industry management and practices (humanization)
Adequate pre-placement examination
Adequate inter-personal relations
Application of ergonomics
Health education
Of employers
Of management
Of workers
110

2. Occupational cramps
Seen in workers engaged in activities involving rapid repetitive movements of short range requiring precision and coordination.
For example those who have to type, write and operate keyboards.
111

3. Traumatic neurosis
It occur in workers who suffer an accident in an emotionally charged environment.
This usually does not occur after accidents outside the occupational settings.
These patients suffer from impaired memory, concentration & sleep, restlessness and irritability.
112

Occupational accidents and injuries
Agent, host and environmental factors are involved
Agent factors:
Physical
Chemical
Mechanical
Host factors:
Predisposing personality traits
Immaturity, inexperience, ignorance, inattentiveness, overconfidence
Predisposing age periods
Too young or too old
113

Predisposing habits
Excessive smoking or alcoholism
Predisposing diseases
Physical, mental or psychological origin.
Environmental factors
Poor illumination, poor communication, high temperatures, noise, high humidity levels,
Unsafe operations, unguarded machine parts
Hostile work environment, poor management, long working hours, frequent night shifts, non-availability of personal protective equipment.
114

Prevention
Safety education
Knowledge on causation of accidents
Safe operations of machines and mechanisms
Use of personal protective equipment
Engineering control
Safe designing of machineries, buildings & working areas
General measures like illumination, ventilation, noise control & temperature control.
Administrative control
Humanization of personal management, elimination of long working hours, interposition of rest periods, reduction in night shifts and improvement of comfort facilities.
115

Ergonomics- lecture objective
By the end of the lecture student should be able to:
Define ergonomics.
Name ergonomic related disorders/injuries.
Recognize and suggest control of occupational ergonomic hazards.
116

Ergonomics
It is the study of men at work with a view t identify the stress factors operating in a work environment and impairing physical, mental and psychological health of workers and interfering with their work performance.
117

“Ergonomics is an applied science concerned with the design of workplaces, tools, and tasks that match the physiological, anatomical, and psychological characteristics and capabilities of the worker.” Vern Putz-Anderson
“The Goal of ergonomics is to ‘fit the job to the person,’ rather than making the person fit the job.” Ergotech
“If it hurts when you are doing something, don’t do it.” Bill Black
What is Ergonomics?

Why do we care about
Ergonomics?

Types of Injuries
• Muscle pain
• Joint pain
• Swelling
• Numbness
• Restricted motion
• Repetitive stress injury
• Repetitive motion
injury
• Cumulative trauma
disorder
• Musculoskeletal
disorder

Target Regions
• Back
• Upper extremities
• Lower extremities

Multidisciplinary study
Anatomy and Physiology
Psychology
Anthropology
Epidemiology
Engineering
Engineering Psychology
Medicine
Biomechanics
122

Applied to..
Originated from defense sectors of US & UK.
From there it moved on to
Mining
Forestry
Agriculture
Now it has expanded to
Schools & colleges
Offices
Laboratories
Workshops
Business centers
Research centers
123

Occupational stress
Work stress
Monotonous work, shift work,
uneven work, static work, dynamic
work
Worker’s stress
Worker mismatch
Anthropometric mismatch: male/female, various age groups
Physical mismatch: muscular strength and work demand
Sensory mismatch: visual acuity and hearing
Cognitive mismatch: ability to process and interpret information
Awkward posturing
Poor work station layout
124

Role at work
Ambiguity or conflict in role at work
Environmental stress
Physical stressors
Poor ventilation, poor illumination,
high intensity noise, extremes of temperatures
Social stresses
Poor social relationships
Impersonal and inhumane management
Migration stress
Language barrier, culture barrier, change of climate, separation from families, discriminatory attitude of management.
125

Ergonomic solutions
Ergonomic designing
Application of human factor engineering in designing workstations, furniture items, machine components, and hand tools.
Ergonomic environment
Physical ergonomics
Temperature control
Noise control
Illumination sources
Adequate ventilation
Cognitive ergonmics
126

Organizational ergonomics;Worker friendly management policy
Appropriate worker placement
Appropriate work distribution
Appropriate worker rotation
Worker welfare
Canteen facility
Restrooms, change rooms
Drinking water points
Toilets
Crèches
First aid facility
127

• Decreased injury risk
• Increased productivity
• Decreased mistakes/rework
• Increased efficiency
• Decreased lost work days
• Decreased turnover
• Improved morale
Benefits of Ergonomics

1 . M E D I C A L M E A S U R E S
Health and welfare of industrial worker
129

1. Medical measures
Serial health check-ups
Pre employment
Pre placement
Periodical
Comprehensive health care
Medical care facility
First aid care boxes; duly equipped and regularly updated, rehabilitation of disabled workers,
Public health service
Immunization, disinfection, personal protection, environmental control and chemotherapy, MCH services, health education.
130

2. Engineering measures
Controlling the source
Substitution
Replacing harmful agent or process by a harmless agent or process.
Scope is limited to the availability of the alternative.
Examples include
Lead paint with zinc or iron paints
Mercury salts with silver salts
Safer asbestos varieties
Dry sweeping with wet sweeping
Dry drilling with wet drilling
131

Isolation
Segregation of a hazardous material or process by interposing barriers or increasing the intervening distance.
Examples include:
Enclosing a harmful material in a leakproof container.
Releasing of contaminants (dusts & fumes) in an enclosure and releasing them by exhaust ventilation.
Noise proof enclosures
Restriction of hazardous processes to night shifts only.
Local exhaust ventilation
It is an engineering mechanism for trapping the hazardous material or dust at its origin and disposing it off by negative pressure.
132

Controlling the environment
General ventilation
Thermal comfort
General illumination
Protecting the worker
Light and well fitting helmets
Goggles, eye shields or visors
Ear plugs or ear muffs
Mask or breathing apparatus
Liquid proof suits or gas proof suits, cold jackets, lead sheets and reflectors for radiation or temperature hazards.
Gloves and gumboots
133

3. Supportive measures
Administrative support
Worker friendly Management policy
To create congenial work environment, raise morale of the workers, increase their job satisfaction, improve their work performance & increase their work output.
Job rotation
For regulating worker exposure to hazardous agents
Housekeeping
Attention to cleanliness, illumination, ventilation, provision of eating, washing and waste disposal facilities, regular mopping and vacuum cleaning of all the passage ways, stair ways and working stations, continuous removal of dust and debri, egular coating of walls, windows and ceilings, dusting of furniture, machines, rafters, beams etc,
Keeping everything in its allotted place
134

Monitoring and surveillance
Periodic inspection and assessment of factory environment
Samples of blood, urine, exhaled air, saliva, hair and nails are collected from workers and analyzed.
Training and research
To familiarize the workers with working environment, agents which might be hazardous, personal protective equipment and their use.
Research to find out solutions to industrial problems, to determine permissible levels of various contaminants, to standardize various operations to render them safe and develop appropriate measures for better control of occupational hazards.
135

Legal provisions
The factories act
Employment provision; age, hrs of work, leave entitlement
Welfare provision; washing points, rest rooms, lunch rooms, sitting areas, Crèches, first aid boxes
Sanitary provisions; latrines, urinals, drinking water points, waste disposal arrangements
Safety provisions; Enclosure and fencing of dangerous machines, safety exits
The employees insurance
Medical benefit
Comprehensive medical care, including outpatient, inpatient, domiciliary investigational and MCH services
136

Sickness benefit
Periodic payment to workers disabled due to employment injury
Maternity benefit
Maternity leave, provision of Crèches,
Dependant benefit
Payable to widows and children under 18 years of age.
Funeral expenses
137

138







