
Jiraporn Sriprapaporn, M.D.
Nuclear Medicine
Siriraj Hospital
Mahidol University September 2015

Non-PET Oncologic Imaging_Jiraporn
Radiopharmaceuticals for Non-PET Oncologic Applications
Nonspecific
• Ga-67 citrate:
– Lymphoma
• Tl-201 chloride:
– Bone sarcomas
– Brain tumors
– Thyroid cancer
• Tc-99m sestamibi:
– Breast cancer
– Parathyroid adenomas
– Thyroid cancer
• Tc-99m tetrofosmin: Similar to sestamibi
Tumor-Type Specific
• I-131: Diff thyroid cancer (PTC, FTC)
• I-131 MIBG: Neural crest tumors (adrenal medullary imaging)
• Radiolabeled peptides: Somatostatin receptors (SSTR)
– In-111 pentetreotide (OctreoScan): Neuroendocrine tumors [NETs]
– Tc-99m HYNIC-TOC: NETs
– Tc-99m depreotide*: Lung cancer
• Radiolabeled monoclonal antibodies:
– Tc-99m arcitumomab (CEA-Scan)*: Colorectal cancer
– In-111 capromab pendetide (ProstaScint): Prostate cancer
– In-111 ibritumomab tiuxetan (Zevalin): Lymphoma
– I-131 tositumomab (Bexxar): Lymphoma
REF : modified from The Requisites
Non-PET Oncologic Imaging_Jiraporn
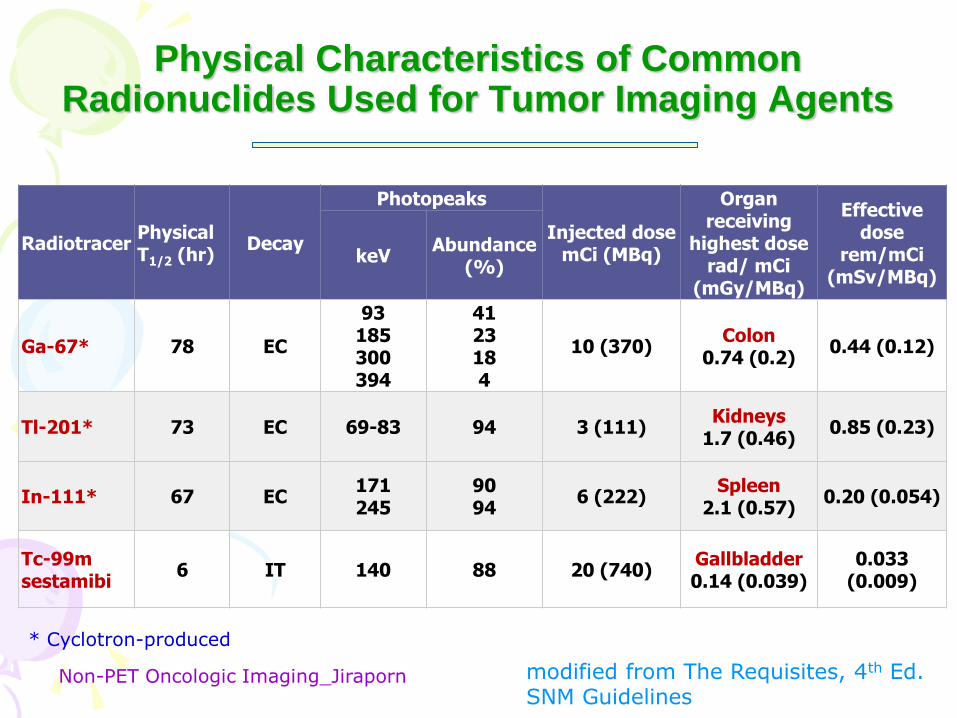
Physical Characteristics of Common Radionuclides Used for Tumor Imaging Agents
Radiotracer Physical T1/2 (hr)
Decay
Photopeaks
Injected dose mCi (MBq)
Organ receiving
highest dose rad/ mCi
(mGy/MBq)
Effective dose
rem/mCi (mSv/MBq)
keV Abundance
(%)
Ga-67* 78 EC
93 185 300 394
41 23 18 4
10 (370) Colon
0.74 (0.2) 0.44 (0.12)
Tl-201* 73 EC 69-83 94 3 (111) Kidneys
1.7 (0.46) 0.85 (0.23)
In-111* 67 EC 171 245
90 94
6 (222) Spleen
2.1 (0.57) 0.20 (0.054)
Tc-99m sestamibi
6 IT 140 88 20 (740) Gallbladder 0.14 (0.039)
0.033 (0.009)
modified from The Requisites, 4th Ed. SNM Guidelines
* Cyclotron-produced

Non-PET Oncologic Imaging_Jiraporn
• Lipophilic monovalent cation
• Mechanism: Passive diffusion across plasma
and mitochondrial membranes.
– Tc-99m MIBI accumulates within the mitochondria
and cytoplasm of cells
• Excretion:
– Hepatobiliary*
– Kidneys
• Dose: 10-20 mCi iv.
• Scan at 20 min pi.

Non-PET Oncologic Imaging_Jiraporn
• Choroid plexus • Salivary glands • Thyroid • Myocardium • Lung • Liver • Kidneys, and bladder • Skeletal muscles
• Excretion: via HB system GB bowel
Tc-99m MIBI
Early Delayed

Non-PET Oncologic Imaging_Jiraporn
• Thyroid carcinoma*
• Breast cancer**
• Parathyroid adenoma***
• Bone & soft tissue sarcoma
• Bronchogenic carcinoma
• Brain tumors
• Head & neck cancers

Non-PET Oncologic Imaging_Jiraporn
Tc-99m MIBI SPECT/CT Imaging in Lung Cancer
• Left lung cancer with left hilar
node metastasis
• Juliana Muniz Miziara, et al.
• Clinics vol.66 no.11 São
Paulo 2011 • http://www.scielo.br/scielo.php?script=
sci_arttext&pid=S1807-
59322011001100009

Tc-99m MIBI & Thyroid Cancer

Non-PET Oncologic Imaging_Jiraporn
• The overall sensitivity for the detection of thyroid cancer 36%-89%, and the specificity is 89-100% [37].
• Sestamibi is particularly sensitive for the detection of nodal metastases [37].
• The agent has poor sensitivity for the detection of lung metastases and residual neck bed thyroid tissue [37].
• The agent is particularly useful for F/U high risk patients with elevated Tg and negative I-131 TBS, and in patients with hurthle cell or MTC. [13,14,27,30]
37 Haugen BR, Lin EC. Isotope imaging for metastaic thyroid cancer. Endocr Metab Clin N Am 2001 30: 469-492
Non-PET Oncologic Imaging_Jiraporn
ABSTRACT OBJECTIVE: To evaluate the potential of technetium-99m methoxyisobutylisonitrile (Tc-99m MIBI) imaging as an alternative to I-131 total-body scan (I-131 TBS) for the follow-up of patients with differentiated thyroid carcinoma (DTC). PATIENTS AND METHODS: We performed 87 Tc-99m MIBI imaging studies in 76 DTC patients who had total or near-total thyroidectomy followed by a radioactive iodine ablation while receiving thyroxine therapy. The final diagnosis was correlated with I-131 TBS, serum thyroglobulin (Tg), other conventional imaging modalities, clinical outcome, and/or pathological report. RESULTS: Seventy-six recurrent tumours or metastatic conditions in 58 DTC patients were detected. The overall findings of Tc-99m MIBI showed 72% sensitivity, 100% specificity and 77% accuracy. The figures for I-131 scan were 57%, 100% and 66%, respectively. When classifying upon tumour locations, Tc-99m MIBI imaging had sensitivity of 79% for cervical, 50% for mediastinal, 65% for skeletal and 69% for pulmonary metastases and the corresponding values for I-131 TBS were 33%, 67%, 94% and 75%, respectively. Furthermore, Tc-99m MIBI could detect only 44% of thyroid remnants demonstrated by radioiodine scan. CONCLUSIONS: Tc-99m MIBI imaging is more sensitive than I-131 TBS in detecting tumours in the neck but less sensitive for metastasis elsewhere, as well as thyroid remnants. Therefore, Tc-99m MIBI imaging should not substitute but rather complement I-131 TBS for evaluation of DTC patients post-radioiodine ablation.
Technetium-99m methoxyisobutylisonitrile imaging in the follow-up of differentiated thyroid carcinoma. Sriprapaporn J1, Toopmongkol C, Satayaban B, Chantamoon N. Ann Acad Med Singapore 2002 Mar;31(2):195-8. Pubmed PMID: 11957557

Non-PET Oncologic Imaging_Jiraporn
• RESULTS: 76 recurrent tumors or metastatic conditions in 58
DTC patients
– Overall findings
• Tc-99m MIBI showed 72% sen, 100% spec and 77% acc
• I-131 scan showed 57%, 100% and 66%, respectively.
– When considering tumor location: Sens of MIBI : I131
• 79% : 33% for cervical LN metas.
• 50% : 67% for mediastinal metastasis.
• 65% : 94% for skeletal metastasis.
• 69% : 75% for pulmonary metastasis .
• 44% : 100% for thyroid remnants .
Tc-99m MIBI Imaging in the Follow-up of DTC
Sriprapaporn J et al. Ann Acad Med Singapore. 2002

Non-PET Oncologic Imaging_Jiraporn
Normal
Abnormal
A B

Non-PET Oncologic Imaging_Jiraporn
Tc-99m MIBI Imaging in DTC Conclusion
• Tc-99m MIBI imaging is more sensitive than
I-131 TBS in detecting tumors in the neck but less
sensitive for metastasis elsewhere, as well as thyroid
remnants.
• Therefore, Tc-99m MIBI imaging should not substitute
but rather complement I-131 TBS for evaluation of DTC
patients post-radioiodine ablation.
Sriprapaporn J et al. 2002
Non-PET Oncologic Imaging_Jiraporn
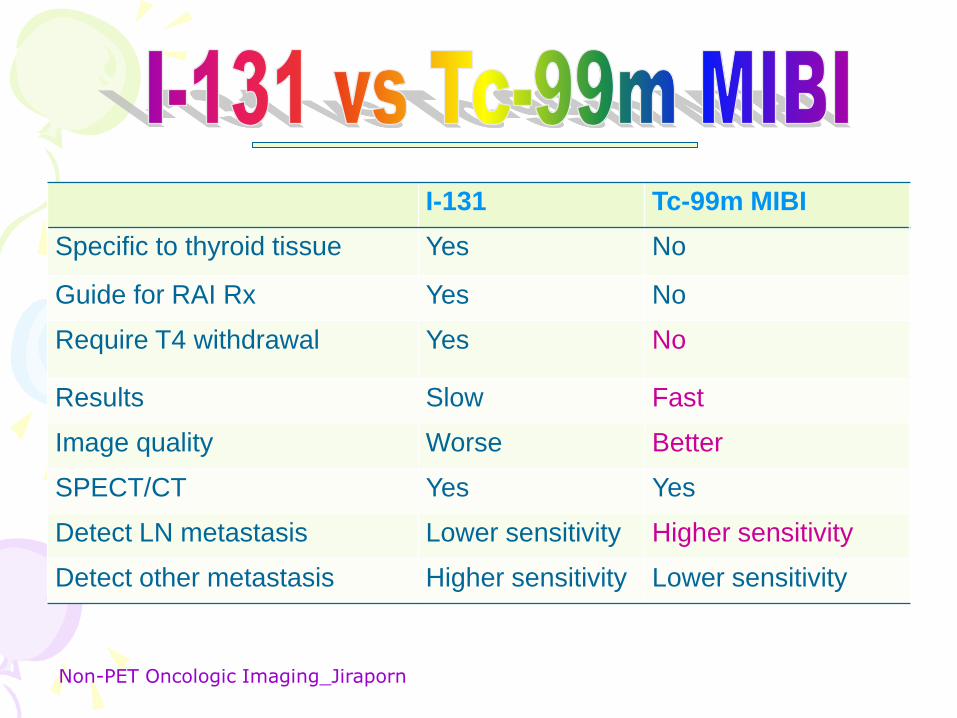
I-131 Tc-99m MIBI
Specific to thyroid tissue Yes No
Guide for RAI Rx Yes No
Require T4 withdrawal Yes No
Results Slow Fast
Image quality Worse Better
SPECT/CT Yes Yes
Detect LN metastasis Lower sensitivity Higher sensitivity
Detect other metastasis Higher sensitivity Lower sensitivity

Non-PET Oncologic Imaging_Jiraporn
Tc-99m MIBI
• More available (kit)
• Better image resolution
• Shorter physical T1/2
• Lower radiation exposure
• Higher dose can be used.
• Better SPECT image quality
• Lower cost
Tl-201
• Limited availability (cyclotron-produced)
• Poorer image resolution
• Longer physical T1/2
• Higher radiation exposure
• Higher dose is limited.
• Less impressive SPECT image quality
• Higher cost (imported)

Tc-99m MIBI & Breast Cancer

Non-PET Oncologic Imaging_Jiraporn
Breast Imaging
Mammography (MMG) screening test !
• Generally, sensitivity ~ 80-90%
• In dense breast: sensitivity ~ 50-85%
• Specificity ~ 35% high false-positive cases over Bx
/ surgery
• Interpretation:
BI-RADS: Breast
imaging-reporting
and data system
Surti S, SNM 2013

Non-PET Oncologic Imaging_Jiraporn
Breast Imaging Reporting and Data System (BI-RADS).
Category 1: Negative
• There’s no significant abnormality to report. In this case, negative means nothing bad was found.
Category 2: Benign (non-cancerous) finding
• This is also a negative MMG result (there’s no sign of cancer), such as benign calcifications, lor calcified
fibroadenomas.
Category 3: Probably benign finding – Follow-up in a short time frame is suggested
• The findings have a very high chance (> 98%) of being benign (not cancer). T
• Follow-up with repeat imaging is usually done in 6 months and regularly after that until the finding is
known to be stable (usually at least 2 years). This approach helps avoid unnecessary biopsies, but if the
area does change over time, it still allows for early diagnosis.
Category 4: Suspicious abnormality – Biopsy should be considered
• Findings do not definitely look like cancer but could be cancer, suggest Bx.
• 4A: finding with a low suspicion of being cancer
• 4B: finding with an intermediate suspicion of being cancer
• 4C: finding of moderate concern of being cancer, but not as high as Category 5
Category 5: Highly suggestive of malignancy – Appropriate action should be taken
• The findings look like cancer and have a high chance (at least 95%) of being cancer. Biopsy is very
strongly recommended.
Category 6: Known biopsy-proven malignancy – Appropriate action should be taken
• This category is only used for findings on a MMG that have already been shown to be cancer by a
previous biopsy. MMG may be used in this way to see how well the cancer is responding to treatment.
www.cancer.org

Non-PET Oncologic Imaging_Jiraporn
BI-RADS Reporting for Breast Density
2013 BI-RADS classifies breast density into 4 groups:
a) The breasts are almost entirely fatty
– The breasts contain little fibrous and glandular tissue, which means the
mammogram would likely detect anything abnormal.
b) There are scattered areas of fibroglandular density
– There are a few areas of fibrous and glandular tissue in the breast.
c) The breasts are heterogeneously dense, which may obscure small masses
– The breast has more areas of fibrous and glandular tissue that are found
throughout the breast. This can make it hard to see small masses.
d) The breasts are extremely dense, which lowers the sensitivity of MMG
– The breast has a lot of fibrous and glandular tissue. This may make it
harder to find a cancer that may be present, as it can blend in with normal
breast tissue.
– In some states, women whose mammograms show heterogeneously dense
or extremely dense breasts.

Non-PET Oncologic Imaging_Jiraporn
BI-RADS edition 2013
a- The breasts are almost
entirely fatty.
b- The breasts have scattered
areas of fibroglandular density.
c- The breasts are
heterogeneously dense
d - The breasts are extremely
dense.
Radionuclide Breast Imaging
Sensitivity of MMG is low in dense breasts !!!

Non-PET Oncologic Imaging_Jiraporn
Radionuclide Breast Imaging Techniques
• Scintimammography (SMM) or
mammoscintigraphy
– Gamma camera with supine position on the
ordinary imaging bed.
– Gamma camera with prone position on the
specially designed cushion.
– Good for lesions > 10 mm, sen 87%.
– Poor for lesions < 10 mm, sen. 59% [Xu HB,
2011]
• Molecular Breast Imaging (MBI)
– Small dual-head gamma camera, using
semiconductor materials, such as cadmium
zinc telluride (CZT)
– Overall sen ~ 90% [O’Connor, 2009]
Non-PET Oncologic Imaging_Jiraporn
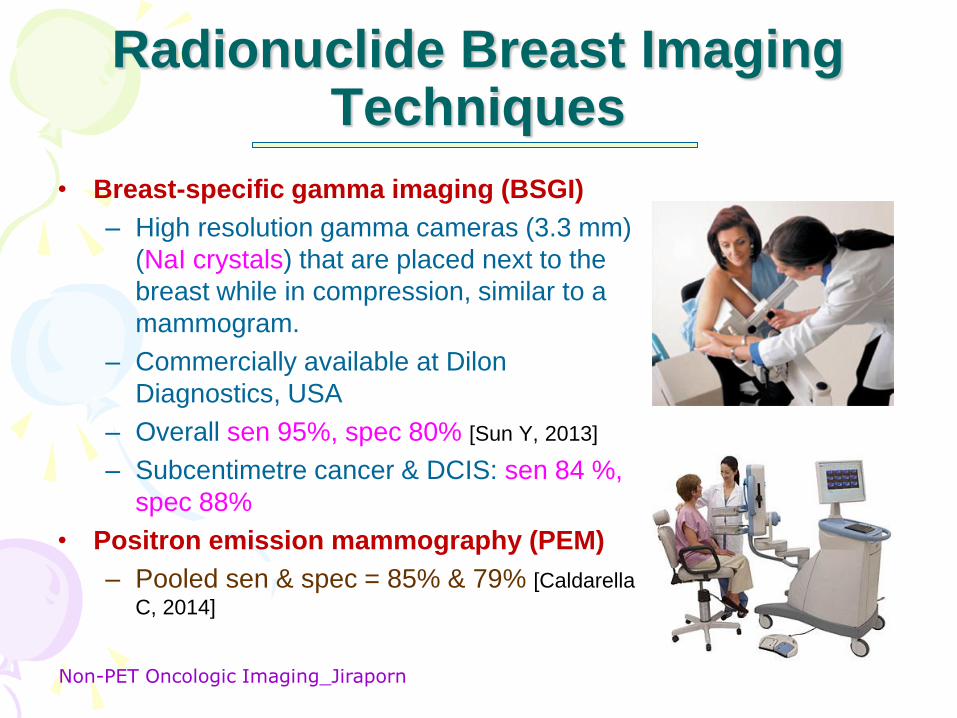
Radionuclide Breast Imaging Techniques
• Breast-specific gamma imaging (BSGI)
– High resolution gamma cameras (3.3 mm)
(NaI crystals) that are placed next to the
breast while in compression, similar to a
mammogram.
– Commercially available at Dilon
Diagnostics, USA
– Overall sen 95%, spec 80% [Sun Y, 2013]
– Subcentimetre cancer & DCIS: sen 84 %,
spec 88%
• Positron emission mammography (PEM)
– Pooled sen & spec = 85% & 79% [Caldarella
C, 2014]

Non-PET Oncologic Imaging_Jiraporn
2010
Non-PET Oncologic Imaging_Jiraporn
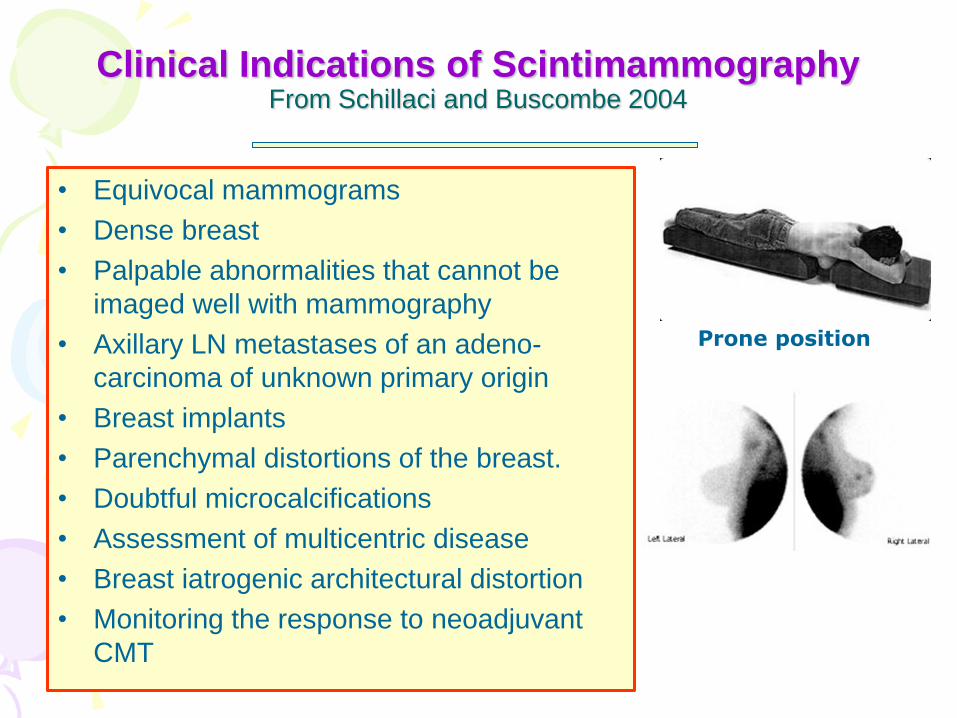
Clinical Indications of Scintimammography From Schillaci and Buscombe 2004
• Equivocal mammograms
• Dense breast
• Palpable abnormalities that cannot be
imaged well with mammography
• Axillary LN metastases of an adeno-
carcinoma of unknown primary origin
• Breast implants
• Parenchymal distortions of the breast.
• Doubtful microcalcifications
• Assessment of multicentric disease
• Breast iatrogenic architectural distortion
• Monitoring the response to neoadjuvant
CMT
Prone position

Non-PET Oncologic Imaging_Jiraporn
Radionuclide Breast Imaging
Author/Yr Sensitivity Specificity
MMG Surti S, 2013 • Overall: 80-90% • Dense breast:50-85%
• 35%
SMM Xu HB, 2011 • Palpable: 87% • Nonpalpable: 59%
• 86% • 89%
MBI O’Connor, 2009 • Overall: 90% • Lesions < 10 mm: 82%
BSGI Sun Y, 2013 • Overall: 95% • Subcentimetre cancer &
DCIS: 84%
• 80 • 88
Rechtman LR, 2014
• Nondense: 95.8% • Dense: 95.1%
PEM-FDG Caldarella C, 2014 • 85% • 79%
Non-PET Oncologic Imaging_Jiraporn
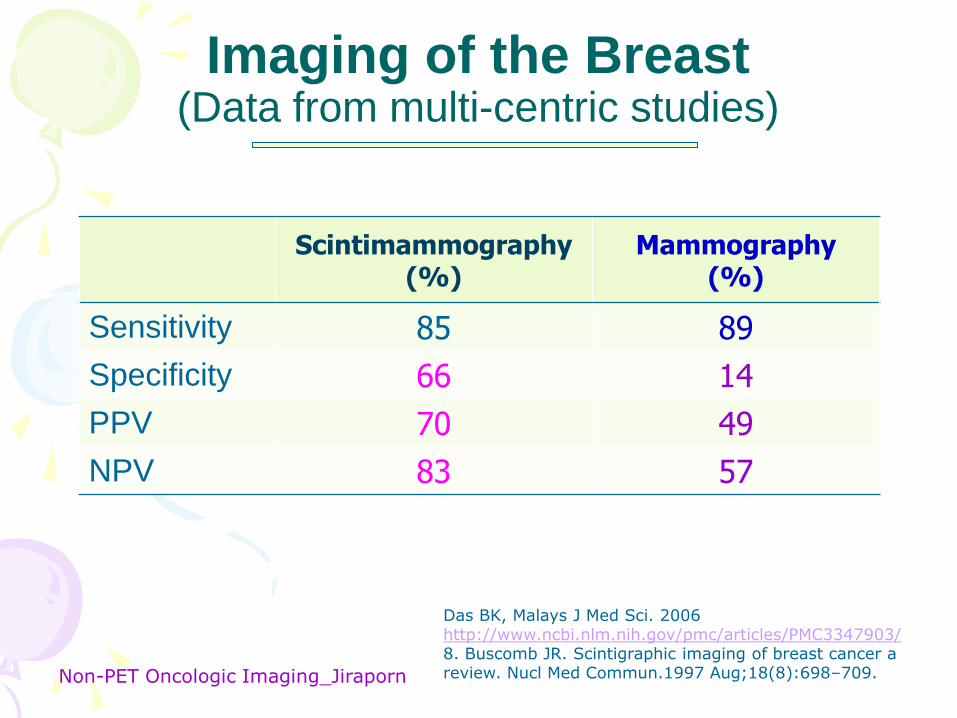
Imaging of the Breast (Data from multi-centric studies)
Scintimammography (%)
Mammography (%)
Sensitivity 85 89
Specificity 66 14
PPV 70 49
NPV 83 57
Das BK, Malays J Med Sci. 2006 http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3347903/ 8. Buscomb JR. Scintigraphic imaging of breast cancer a review. Nucl Med Commun.1997 Aug;18(8):698–709.

Non-PET Oncologic Imaging_Jiraporn
Tc-99m MIBI Scintimammography
• Right breast cancer • Left breast cancer with left axillary node metastastasis.

Non-PET Oncologic Imaging_Jiraporn
• Meta-analysis since January 1997.
• Each study had Pts > 100 cases.
• Total 2424 patients from single-center studies.
• The overall sensitivity & specificity was 85% & 84%
• Total 3049 patients from multicenter studies.
• The overall sensitivity & specificity was 85% & 83%
Non-PET Oncologic Imaging_Jiraporn
• 45 studies met our inclusion criteria.
• The summary estimates for Tc-99m MIBI in the diagnosis of breast
cancer in the studies included were as follows: sensitivity, 0.83 [95%
confidence interval (CI), 0.82-0.84]; specificity, 0.85 (95% CI, 0.83-
0.86); positive likelihood ratio, 5.06 (95% CI, 4.26-6.01); negative
likelihood ratio, 0.20 (95% CI, 0.17-0.24); and diagnostic odds ratio,
27.63 (95% CI, 21.63-36.10).
• For patients with a palpable mass, the sensitivity and specificity were
87 and 86%, respectively.
• For patients without a palpable mass, the sensitivity and specificity
were 59 and 89%, respectively.
• Tc-99m MIBI has a high level of overall accuracy for the diagnosis of
breast cancer.
Non-PET Oncologic Imaging_Jiraporn
Non-PET Oncologic Imaging_Jiraporn
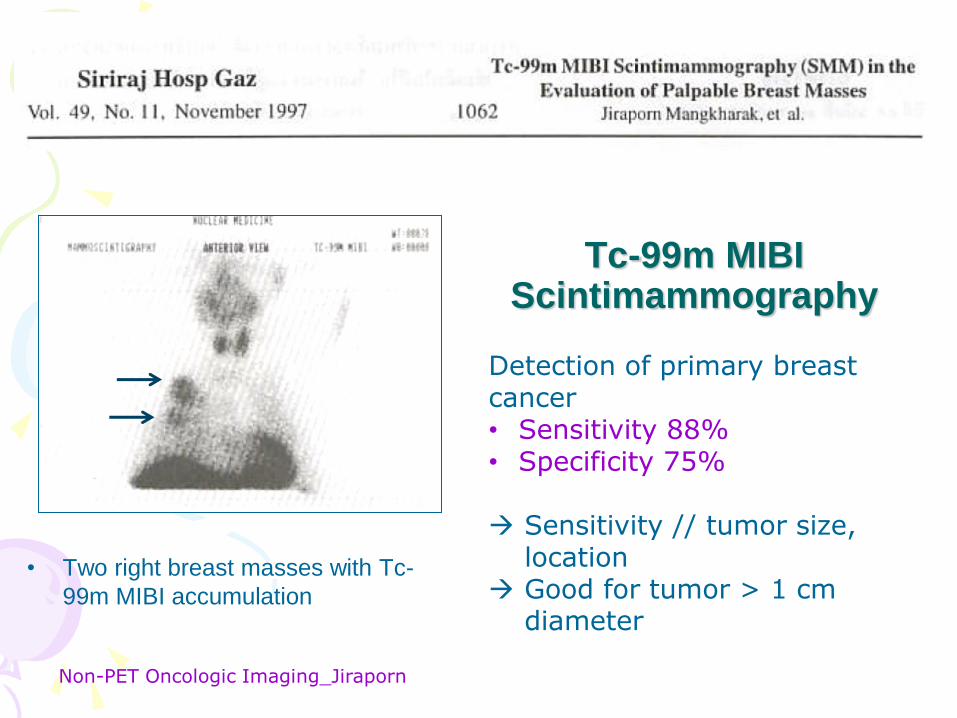
Tc-99m MIBI Scintimammography
• Two right breast masses with Tc-
99m MIBI accumulation
Detection of primary breast cancer • Sensitivity 88% • Specificity 75%
Sensitivity // tumor size,
location Good for tumor > 1 cm
diameter
Non-PET Oncologic Imaging_Jiraporn
Scintimammography (SMM) in Breast Cancer Patients.
Mangkharak J. J Med Assoc Thai. 1999 Mar;82(3):242-9. PubMed PMID: 10410478
• ABSTRACT
• The author retrospectively reviewed the scintimammography (SMM) using
201Tl and/or 99mTc-MIBI in 45 breast cancer patients.
• 36 cases with 37 intact breast masses and another 9 cases with previous
excision of the masses were studied.
• The sensitivity for the detection of the primary breast cancer was 92% and
that of ipsilateral axillary lymph node metastasis was only 48 %.
• SMM is helpful for the diagnosis of breast cancer and differentiating
malignant from benign masses, thus improving the accuracy of routine
mammography.
• In postoperative cases SMM is helpful to detect palpable local tumor
recurrence and axillary node metastasis but it is not accurate enough for
assessing the extent of microscopic tumor involvement locally and also
distant metastasis.
• Thus, it is not recommended to use SMM alone for staging of breast cancer.

Non-PET Oncologic Imaging_Jiraporn
The evaluation of combined scintimammography and tumor markers in breast cancer patients.
Mangkharak J, Patanachak C, Podhisuwan K, Pleehachinda R. Anticancer Res. 1997 May-Jun;17(3B):1611-4. PubMed PMID: 9179203
ABSTRACT:
• MATERIALS AND METHODS: 47 breast cancer patients (36 for preoperative evaluation,
others for postoperative investigation) were studied with SMM using 201Tl and/or 99mTc-
MIBI and serum CEA and CA15-3.
• RESULTS: SMM could pick up breast cancer in 91.7% of the patients with intact breast
masses and 2/2 cases of local recurrence. The uptake ratio tended to increased from stage
2A through 3B. Sensitivity of SMM to detect axillary node uptake was only 44.4%.
• No definite correlation between serum CEA and CA15-3 levels was observed.
• Elevated CA15-3 is a good indicator for recurrent and metastatic breast diseases and more
specific than CEA in clinical correlations.
• CONCLUSIONS: SMM may be helpful when mammographic results are questionable. SMM
can detect primary breast cancers and recurrent lesions that are palpable with high
sensitivity. Increased tumor-uptake ratio and rising serum tumor markers, more often seen
with elevated CA15-3 rather than CEA, could be useful for the prognosis of breast cancer
patients. CA15-3 is very helpful for monitoring therapeutic response since its level
correlates with the clinical state better than CEA.
Non-PET Oncologic Imaging_Jiraporn
Molecular Breast Imaging (MBI) O'Connor M, Rhodes D, Hruska C.
Expert Rev Anticancer Ther. 2009 Aug;9(8):1073-80. PubMed PMID: 19671027; PubMed Central PMCID: PMC2748346.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2748346/
• Molecular breast imaging (MBI) is a new NM technique that utilizes small semiconductor-based γ-
cameras in a mammographic configuration to provide high-resolution functional images of the
breast.
• Current MBI has used Tc-99m sestamibi, which is an approved agent for breast imaging.
• The procedure is relatively simple to perform. Imaging can be performed within 5 min post
injection, with the breast lightly compressed between the two detectors. Images of each breast are
acquired in the craniocaudal and mediolateral oblique projections facilitating comparison with
mammography. Key studies have confirmed that MBI has a high sensitivity for the detection of
small breast lesions.
• In patients with suspected breast cancer, MBI has an overall sensitivity of 90%, with a sensitivity
of 82% for lesions < 10 mm in size.
• Sensitivity was lowest for tumors < 5 mm in size.
• Tumor detection does not appear to be dependent on tumor type, but rather on tumor size.
Studies using MBI and BSGI have shown that these methods have comparable sensitivity to
breast MRI. A large clinical trial compared MBI with screening mammography in over 1000
women with mammographically dense breast tissue and increased risk of breast cancer and
showed that MBI detected 2-3 times more cancers than MMG. In addition, MBI appears to have
slightly better specificity than MMG in this trial.
• MBI provides high-resolution functional images of the breast and its potential applications range
from evaluation of the extent of disease to a role as an adjunct screening technique in certain
high-risk populations. MBI is highly complementary to existing anatomical techniques, such as
MMG, tomosynthesis and U/S.

Non-PET Oncologic Imaging_Jiraporn
MMG-ve, MBI & MRI +ve @ Rt lower quadrant Surgery found 9-mm ductal carcinoma in situ
O’Connor, 2009

Non-PET Oncologic Imaging_Jiraporn
Breast-specific Gamma Imaging (BSGI)

Non-PET Oncologic Imaging_Jiraporn
According to SNM Guideline
2010
Non-PET Oncologic Imaging_Jiraporn
Common Clinical Indications
I. In patients with recently detected breast malignancy
1. Evaluate the extent of disease (initial staging)
2. Detect multicentric, multifocal, or bilateral disease
3. Assess response to neoadjuvant chemotherapy
II. In patients at high risk for breast malignancy
1. Recurrence is suspected
2. Only a limited mammogram was obtained or previous
malignancy was occult on mammography
III. In patients with indeterminate breast abnormalities
(next slide)
SNM Guideline 2010

Non-PET Oncologic Imaging_Jiraporn
III. In Patients with Indeterminate Breast Abnormalities
1. Evaluate nipple discharge in patients with abnormal MMG or US findings, w or wo contrast ductography
2. Evaluate bloody nipple discharge in patients with normal MMG or ductography findings
3. Evaluate significant nipple discharge in patients who underwent ductography unsuccessfully
4. Evaluate lesions when patient reassurance is warranted [BIRADS 3]
5. Evaluate lesions—whether palpable or nonpalpable—identified by other breast imaging techniques
6. Evaluate palpable abnormalities not demonstrated MMG or US
7. Evaluate multiple breast masses demonstrated on breast imaging
8. Aid in biopsy targeting
9. Evaluate diffuse or multiple clusters of microcalcifications
10. Evaluate breasts for occult disease in cases of axillary LN metastases with an unknown primary
11. Evaluate unexplained architectural distortion
12. Evaluate a suggestive mammographic finding seen on 1 view only
13. Increase specificity by evaluating enhancing areas seen on MRI
SNM Guideline 2010

Non-PET Oncologic Imaging_Jiraporn
Common Clinical Indications
IV. In patients with technically difficult breast imaging
1. Radiodense breast tissue
2. Breast implants, free silicone, or paraffin injections compromising the mammogram
V. In patients for whom breast MRI would be indicated
1. MRI is diagnostically indicated but not possible:
a. Implanted pacemakers or pumps
b. Ferromagnetic surgical implants
c. Risk of a nephrogenic systemic fibrotic response to gadolinium
d. Body habitus exceeding the inside diameter of the
e. Patients with breasts too large to be evaluated within the breast coil MRI bore
f. Patients with acute claustrophobia
g. Other factors limiting compliance with a prescribed MRI study
2. An alternative is needed for patients who meet MRI screening criteria: breast cancer susceptibility gene 1 or 2; parent, sibling, or child with breast cancer; lifetime risk of 20%–25%; chest radiation performed between ages of 10 and 30 y
VI. In patients undergoing preoperative CMT who require monitoring of neoadjuvant tumor response
1. Determine the impact of therapy
2. Plan surgery for residual disease
SNM Guideline 2010

Non-PET Oncologic Imaging_Jiraporn
Interpretation Criteria
1. Homogeneous radiotracer uptake in the breast or axilla is consistent with a normal study (BIRADS 1).
2. Patchy or diffusely increased tracer uptake in the breasts is usually a normal variant, esp. when the distribution correlates with MMG (BIRADS 2).
3. Patchy uptake of mild to moderate intensity, eg. mastitis suggestive of benign disease of the breast (BIRADS 3).
4. Small focal increased uptake in the breast or axilla $ represent an equivocal result, consistent with malignancy, inflammation, atypia, or fat necrosis (BIRADS 4).
5. The intensity of focal uptake in malignant lesions is highly variable. Moderate to intense focal uptake with well-delineated contours is consistent with malignancy (BIRADS 5).
6. Focally increased uptake (1 or more foci) in the ipsilateral axilla, in the presence of a primary lesion, is strongly suggestive of axillary LN metastatsis. $
$ : in the absence of R’pharm infiltration
SNM Guideline 2010

Non-PET Oncologic Imaging_Jiraporn
Interpretation Pitfalls
1. Infiltration of the radiopharmaceutical administered in an
arm vein may cause false-positive uptake in the axillary LNs.
• Imaging of the injection site is helpful.
• Motion of the breast will decrease the accuracy of the test.
2. The sensitivity, specificity, and accuracy of this test depend
on several factors, including location & size of the breast
neoplasm being imaged.
• However, the sensitivity of this test for subcentimeter
tumors is high at around 95%.
SNM Guideline 2010
-- Inject radiotracer via the contralateral side !

Non-PET Oncologic Imaging_Jiraporn
False-positive Results
• Benign fibroadenomas,
• Fibrocystic change,
• Inflammation (including inflammatory fat necrosis)
False-negative results
• Small tumors (< 1 cm)
• Deep lesions
• Tumors with less avidity for sestamibi.

Non-PET Oncologic Imaging_Jiraporn
B S G I
• Fig. 1A Comparison of dense and nondense breast imaging with MMG and BSGI
• Images from mammography (A) and breast-specific gamma imaging (BSGI) (B) in 48-
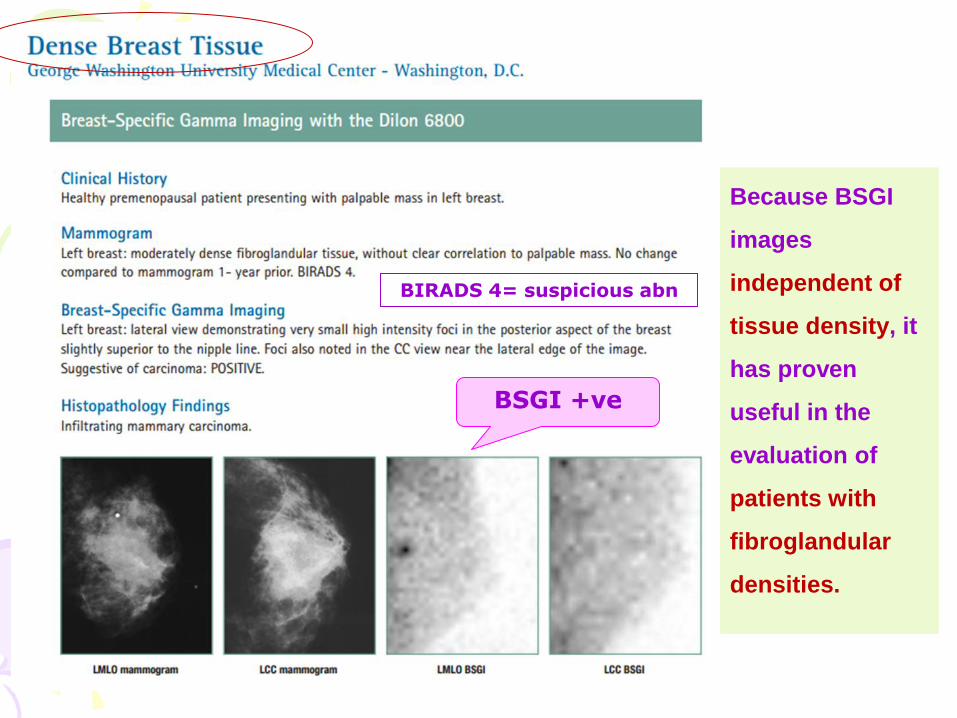
year-old woman with heterogeneously dense breast tissue show infiltrating ductal
carcinoma (IDC) in superior left breast.
• Images from mammography (C) and breast-specific gamma imaging (BSGI) (D) in 53-
year-old woman with predominantly fatty breast tissue show IDC in 2-o'clock position of
left breast.
Rechtman LR, et al. AJR 2014
Dense breasts Fatty breasts

Non-PET Oncologic Imaging_Jiraporn
• RESULTS. The overall sensitivity of BSGI for breast cancer
detection was 95.4%.
• Positive BSGI examinations 136 of 142 nondense breast
cancers and 195 of 205 dense breast cancers sensitivities
of 95.8% and 95.1%, respectively.
• There was no significant difference in BSGI breast cancer
detection and parenchymal breast density (p = 0.459).
• CONCLUSION. BSGI has high sensitivities for the detection
of breast cancer in women with dense and nondense breasts
and is an effective adjunct imaging modality in women with
both dense and nondense breasts.

Non-PET Oncologic Imaging_Jiraporn
Clinical usefulness of BSGI as an adjunct modality to MMG for diagnosis of breast cancer: a systemic review and meta-analysis.
Sun Y, Wei W, Yang HW, Liu JL. EJNMM 2013 Feb;40(3):450-63. PMID: 23151912
• PURPOSE: To assess the diagnostic performance of BSGI as an adjunct modality to MMG for
detecting breast cancer.
• METHODS:
• Comprehensive searches of MEDLINE (1984 to August 2012) and EMBASE (1994 to August 2012)
were performed. A summary receiver operating characteristic curve (SROC) was constructed to
summarize the overall test performance of BSGI. The sensitivities for detecting subcentimetre
cancer and ductal carcinoma in situ (DCIS) were pooled. The potential of BSGI to complement
MMG was also evaluated by identifying MMG-occult breast cancer.
• RESULTS:
• BSGI in detecting breast cancer : sensitivity 95 % (95 % CI 93-96 %), specificity 80 % (95 % CI 78-
82 %), positive likelihood ratio 4.63 (95 % CI 3.13-6.85), negative likelihood ratio 0.08 (95 % CI
0.05-0.14), and diagnostic odds ratio 56.67 (95 % CI 26.68-120.34).
• The area under the SROC was 0.9552 and the Q* point was 0.8977.
• The pooled sensitivities for detecting subcentimetre cancer and DCIS were 84 % (95 % CI 80-
88 %) and 88 % (95 % CI 81-92 %), respectively.
• Among patients with normal MMG, 4 % +ve BSGI, and among those with MMG suggestive of
malignancy, 6 % were diagnosed with additional cancers in the breast by BSGI.
• CONCLUSION: BSGI had a high diagnostic performance as an excellent adjunct modality to
mammography for detecting breast cancer. The ability to identify subcentimetre cancer and DCIS
was also high.

Non-PET Oncologic Imaging_Jiraporn
Breast-specific gamma imaging as an adjunct imaging modality for the diagnosis of breast cancer.
Brem RF et al. Radiology 2008 Jun;247(3):651-7. PMID: 18487533
• PURPOSE: To retrospectively determine the sensitivity and specificity of breast-specific gamma imaging (BSGI) for
the detection of breast cancer by using pathologic results as the reference standard.
• MATERIALS AND METHODS:
• This study was IRB approved and Health Insurance Portability and Accountability Act compliant. Informed consent
was obtained for participants who were not imaged as part of their clinical protocol but were participating in other
IRB-approved studies that used BSGI.
• A retrospective review of 146 women (aged 32-98 years) undergoing BSGI and breast biopsy was performed.
Patients underwent BSGI with intravenous injection of 30 mCi (1110 MBq) of Tc-99m sestamibi and were imaged in
craniocaudal and mediolateral oblique projections. Study images were assigned scores, and scores were classified
as positive (focal increased radiotracer uptake) or negative (no uptake or scattered heterogeneous physiologic
uptake) and compared with biopsy results. The sensitivity, specificity, PPV and NPV were determined.
• RESULTS:
• In 146 patients, 167 lesions underwent biopsy, of which 83 (16 ductal carcinoma in situ [DCIS] and 67 invasive
cancers) were malignant.
• Of 84 nonmalignant lesions, 82 were benign and 2 showed atypical histologic results (one atypical lobular
hyperplasia and one lobular carcinoma in situ).
• BSGI helped detect cancer in 80/83 malignant lesions with a sensitivity of 96.4% (95% CI: 92%, 99%) and correctly
identified 50 of 84 nonmalignant lesions as negative for cancer with a specificity of 59.5% (95% CI: 49%, 70%). The
PPV for 80/114 malignant lesions with a BSGI was 68.8% (95% CI: 60%, 78%) and the NPV for 50 /53 nonmalignant
lesions was 94.3% (95% CI: 88%, 99%).
• The smallest invasive cancer and DCIS detected were both 1 mm. BSGI helped detect occult cancer not visualized
at MMG or U/S in 6 patients.
• CONCLUSION: BSIG has high sensitivity (96.4%) and moderate specificity (59.5%) helping detect breast cancers.
• Erratum in Radiology. 2009 Apr;251(1):308.

Images from
Breast Specific Gamma Imaging
with Tc-99m MIBI
https://www.grandlakehealth.org/centers-of-excellence/womens-imaging-center/molecular-breast-imaging

Non-PET Oncologic Imaging_Jiraporn
• MMG -ve • BSGI -ve

Non-PET Oncologic Imaging_Jiraporn
• MMG +ve • BSGI +ve

Non-PET Oncologic Imaging_Jiraporn
• MMG - ? • BSGI -ve

Non-PET Oncologic Imaging_Jiraporn
“BSGI has been shown
to be a powerful and
important modality for
improving cancer
diagnosis in a high-risk
screening population
with normal MMG and
physical examination.”
Brem, Rachel M.D.
False-negative MMG
• MMG -ve • BSGI +ve

Non-PET Oncologic Imaging_Jiraporn
The functional
imaging of BSGI
complements the
anatomic
imaging of x-ray
MMG; providing
higher specificity
than other breast
imaging
modalities.
False-positive MMG
• MMG +ve • BSGI -ve
BIRADS 4
Non-PET Oncologic Imaging_Jiraporn
Because BSGI
images
independent of
tissue density, it
has proven
useful in the
evaluation of
patients with
fibroglandular
densities.
BIRADS 4= suspicious abn
BSGI +ve
Non-PET Oncologic Imaging_Jiraporn
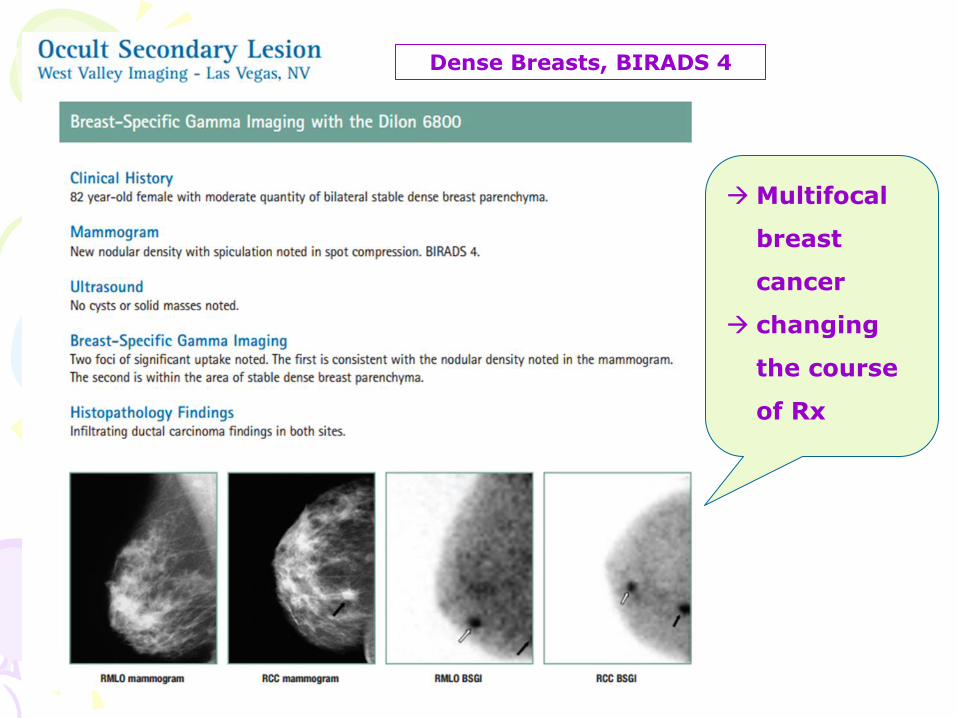
Multifocal
breast
cancer
changing
the course
of Rx
Dense Breasts, BIRADS 4

Non-PET Oncologic Imaging_Jiraporn
BSGI also has high sensitivity & specificity in DCIS.
Tc-99m MIBI for Parathyroid Imaging
To be continued in the next file.







