4/7/2011
1
1
Future Technologies for PAD: Drug-Eluting
Stents and Balloons, Bioabsorbable Stents
Michael D. Dake, M.D.
Thelma and Henry Doelger Professor
Department of Cardiothoracic Surgery
Stanford University School of Medicine
Falk Cardiovascular Research Center
PAD: From the Office to the Angiosuite and Back Again SIR Annual Scientific Meeting
Saturday, March 26, 2011
2Michael Dake, MD
• Research/Research Grants, Clinical Trial Support– W. L. Gore– Cook Medical
• Consulting Fees/Honoraria– W. L. Gore– Abbott Vascular
• Equity Interests/Stock Options– NovoStent– Vatrix– Amaranth– CVRx– Endoluminl Sciences– REVA Medical– TriVascular– Cytograft Tissue Engineering
• Officer, Director, Board Member or other Fiduciary Role– VIVA Physicians Group
• Speaker’s Bureau– None
Within the past 12 months, the presenter or
their spouse/partner have had a financial interest/arrangement or affiliation with the organization listed below.
3
New Endovascular Options for PAD?
1. SFA and Popliteal
– Drug-Eluting Stents
– Drug-Delivery Balloons
– Bioresorbable Stents
4
New Endovascular Options for PAD?
1. SFA and Popliteal
– Drug-Eluting Stents
– Drug-Delivery Balloons
– Bioresorbable Stents

4/7/2011
2
5
#2 DES over BMSThe lesion characteristics that maybe associated
with incremental benefits: DES relative to BMS
• Re-stenotic lesions post-PTA
• In-stent re-stenosis
• Lesions in diabetic patients
• Long lesions >14 cm (c/w short or moderate lesions)
• Higher TASC rated lesions (DES “punching above rank”)
• …but in reality, possibly all lesions
6
Sirocco Trial Design
• Double-blind, randomized, balanced, prospective, feasibility trial in the SFA
• Primary endpoints: Safety & in-stent percent mean diameter stenosis via quantitative angiography determined within six months after stent placement.
7
Drug-Eluting Stents: SIROCCO II
Presented 2004 Annual Meeting of the Cardiovascular and Interventional Radiology Society of Europe
P = NS
18 month Duplex US follow-up.
Not approved for use in the US.
8
Everolimus
Triaxial Stent Delivery System
DYNALINK Self-expanding Nitinol Stent
EVAL polymer
Everolimus-eluting Peripheral Stent System
4/7/2011
3
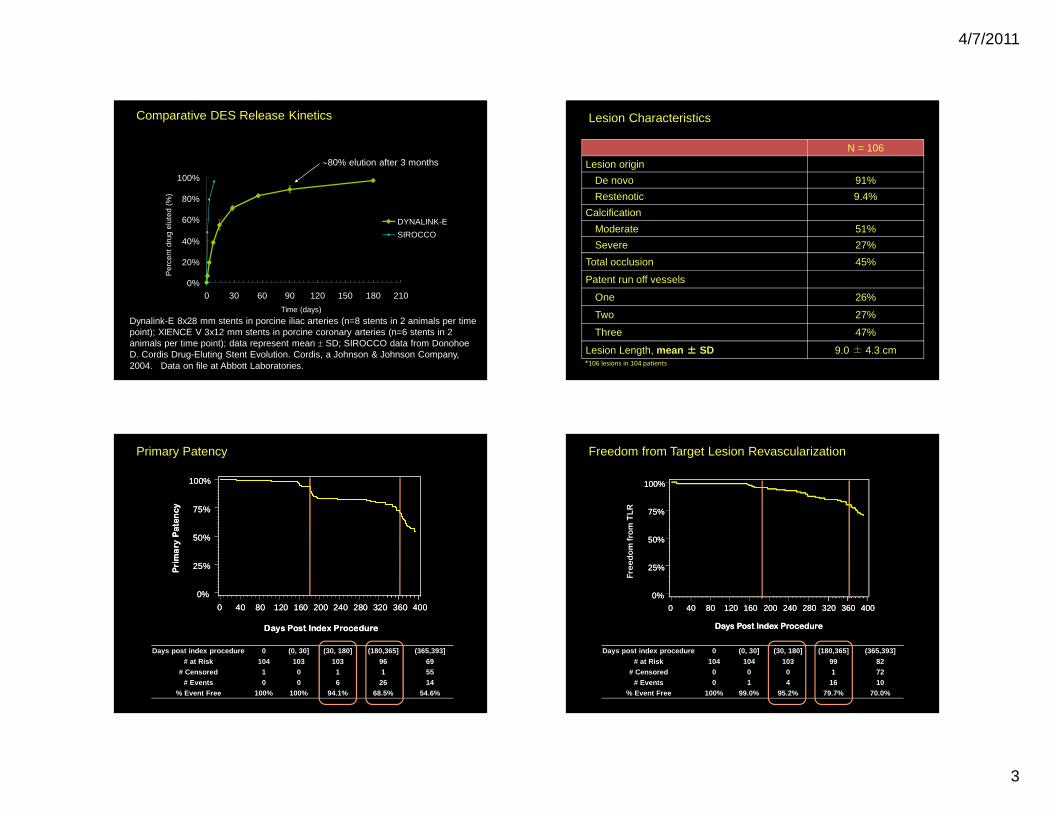
9Comparative DES Release Kinetics
Dynalink-E 8x28 mm stents in porcine iliac arteries (n=8 stents in 2 animals per time point); XIENCE V 3x12 mm stents in porcine coronary arteries (n=6 stents in 2 animals per time point); data represent mean ± SD; SIROCCO data from Donohoe D. Cordis Drug-Eluting Stent Evolution. Cordis, a Johnson & Johnson Company, 2004. Data on file at Abbott Laboratories.
∼80% elution after 3 months
0%
20%
40%
60%
80%
100%
0 30 60 90 120 150 180 210
Time (days)
Per
cent
dru
g el
uted
(%
)
DYNALINK-E
SIROCCO
10
N = 106
Lesion origin
De novo 91%
Restenotic 9.4%
Calcification
Moderate 51%
Severe 27%
Total occlusion 45%
Patent run off vessels
One 26%
Two 27%
Three 47%
Lesion Length, mean ±±±± SD 9.0 ± 4.3 cm
Lesion Characteristics
*106 lesions in 104 patients
11
Primary Patency
Days post index procedure 0 (0, 30] (30, 180] (180,365] (365,393]
# at Risk 104 103 103 96 69# Censored 1 0 1 1 55
# Events 0 0 6 26 14% Event Free 100% 100% 94.1% 68.5% 54.6%
Primary Patency
0%
25%
50%
75%
100%
Days Post Index Procedure
0 40 80 120 160 200 240 280 320 360 400
Primary Patency
0%
25%
50%
75%
100%
Days Post Index Procedure
0 40 80 120 160 200 240 280 320 360 400
12
Freedom from Target Lesion Revascularization
Days post index procedure 0 (0, 30] (30, 180] (180,365] (365,393]
# at Risk 104 104 103 99 82# Censored 0 0 0 1 72
# Events 0 1 4 16 10% Event Free 100% 99.0% 95.2% 79.7% 70.0%
0%
25%
50%
75%
100%
Days Post Index Procedure
0 40 80 120 160 200 240 280 320 360 400
Fre
edom fro
m TLR
0%
25%
50%
75%
100%
Days Post Index Procedure
0 40 80 120 160 200 240 280 320 360 400
4/7/2011
4
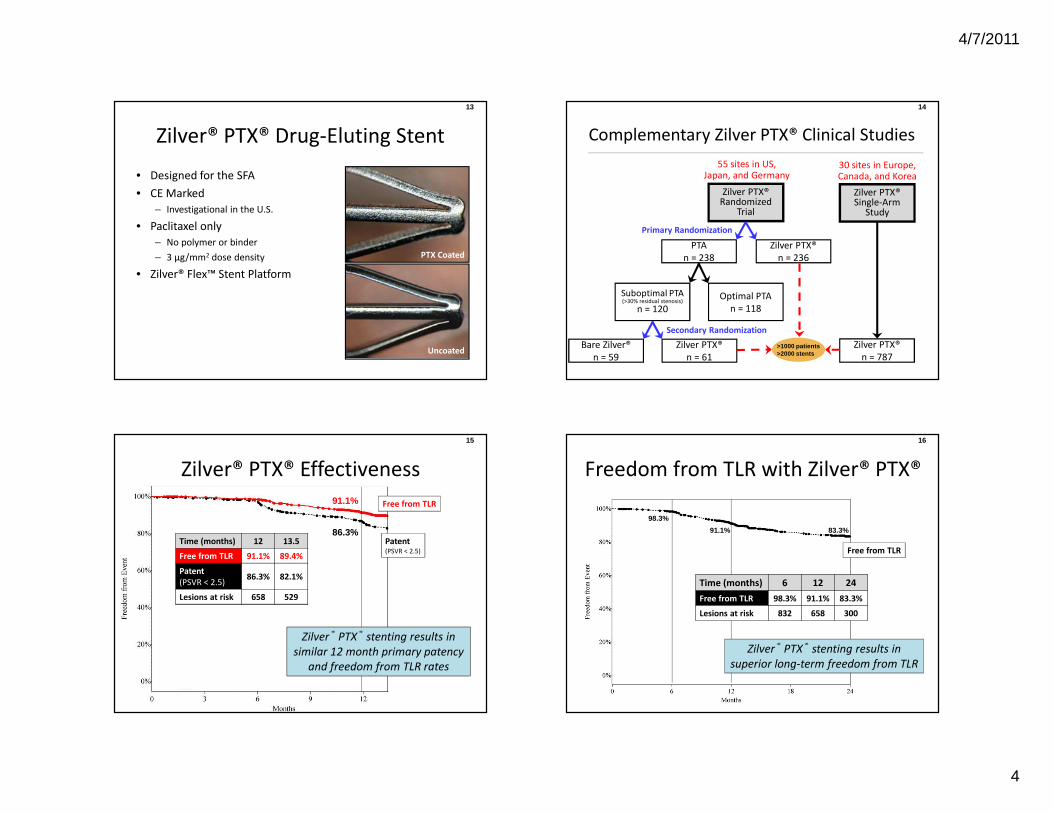
13
Zilver® PTX® Drug-Eluting Stent
• Designed for the SFA
• CE Marked
– Investigational in the U.S.
• Paclitaxel only
– No polymer or binder
– 3 µg/mm2 dose density
• Zilver® Flex™ Stent Platform
Uncoated
PTX Coated
14
55 sites in US, Japan, and Germany
Bare Zilver®
n = 59
PTA
n = 238
Optimal PTA
n = 118
Zilver PTX® Randomized
Trial
Suboptimal PTA(>30% residual stenosis)
n = 120
Zilver PTX®
n = 236
Zilver PTX®
n = 61
Primary Randomization
Secondary Randomization
Zilver PTX® Single-Arm
Study
Zilver PTX®
n = 787
30 sites in Europe, Canada, and Korea
>1000 patients>2000 stents
Complementary Zilver PTX® Clinical Studies
15
Zilver® PTX® Effectiveness
Free from TLR
Patent(PSVR < 2.5)
91.1%
86.3%Time (months) 12 13.5
Free from TLR 91.1% 89.4%
Patent
(PSVR < 2.5)86.3% 82.1%
Lesions at risk 658 529
Zilver® PTX® stenting results in
similar 12 month primary patency
and freedom from TLR rates
16
Freedom from TLR with Zilver® PTX®
Time (months) 6 12 24
Free from TLR 98.3% 91.1% 83.3%
Lesions at risk 832 658 300
98.3%
91.1% 83.3%
Free from TLR
Zilver® PTX® stenting results in
superior long-term freedom from TLR

4/7/2011
5
17 18
19 20
Zilver PTX Single-Arm Update
Performance in Long Lesions: > 15cm
4/7/2011
6
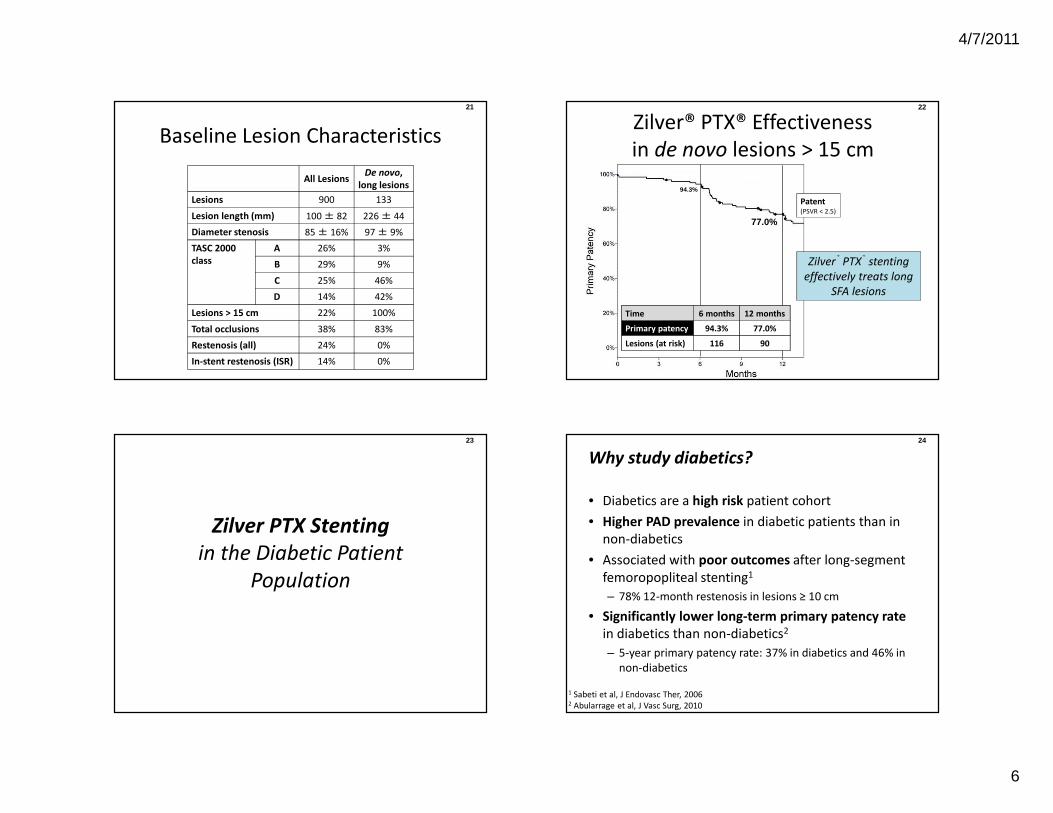
21
Baseline Lesion Characteristics
All LesionsDe novo,
long lesions
Lesions 900 133
Lesion length (mm) 100 ± 82 226 ± 44
Diameter stenosis 85 ± 16% 97 ± 9%
TASC 2000
class
A 26% 3%
B 29% 9%
C 25% 46%
D 14% 42%
Lesions > 15 cm 22% 100%
Total occlusions 38% 83%
Restenosis (all) 24% 0%
In-stent restenosis (ISR) 14% 0%
22
Zilver® PTX® Effectiveness
in de novo lesions > 15 cm
Patent(PSVR < 2.5)
77.0%
Time 6 months 12 months
Primary patency 94.3% 77.0%
Lesions (at risk) 116 90
94.3%
Zilver® PTX® stenting
effectively treats long
SFA lesions
23
Zilver PTX Stenting
in the Diabetic Patient
Population
24
• Diabetics are a high risk patient cohort
• Higher PAD prevalence in diabetic patients than in
non-diabetics
• Associated with poor outcomes after long-segment
femoropopliteal stenting1
– 78% 12-month restenosis in lesions ≥ 10 cm
• Significantly lower long-term primary patency rate
in diabetics than non-diabetics2
– 5-year primary patency rate: 37% in diabetics and 46% in
non-diabetics
Why study diabetics?
1 Sabeti et al, J Endovasc Ther, 20062 Abularrage et al, J Vasc Surg, 2010
4/7/2011
7
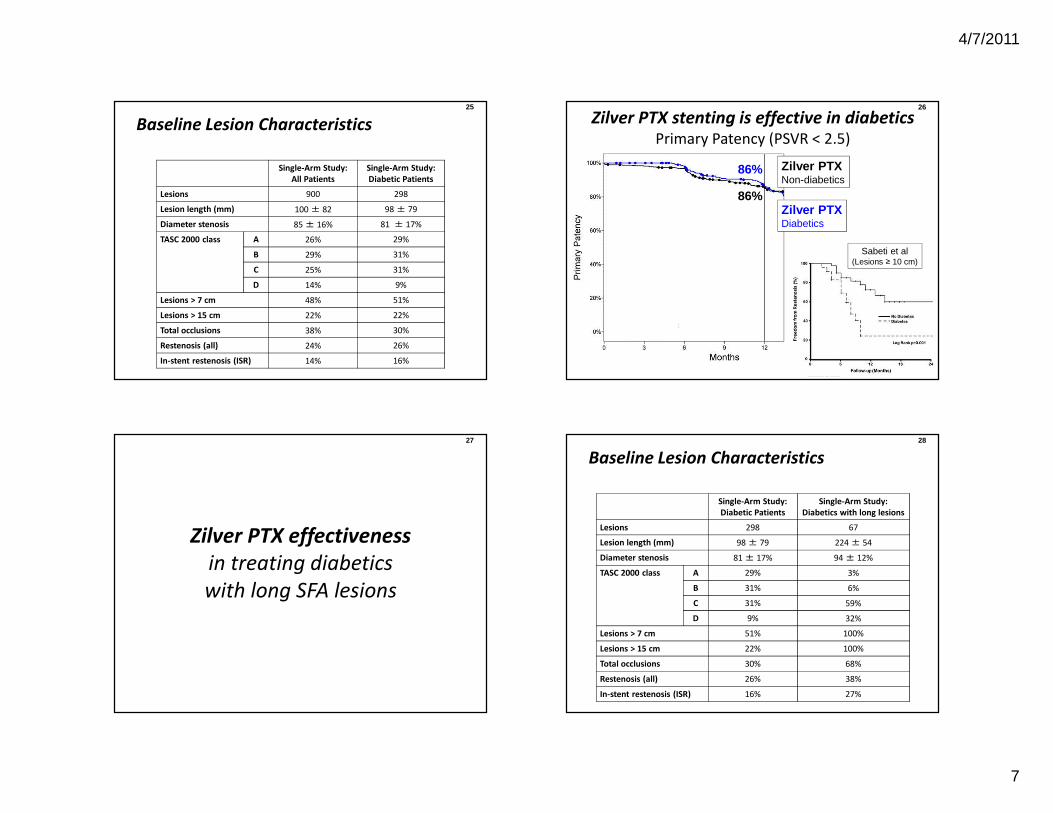
25
Baseline Lesion Characteristics
Single-Arm Study:
All Patients
Single-Arm Study:
Diabetic Patients
Lesions 900 298
Lesion length (mm) 100 ± 82 98 ± 79
Diameter stenosis 85 ± 16% 81 ± 17%
TASC 2000 class A 26% 29%
B 29% 31%
C 25% 31%
D 14% 9%
Lesions > 7 cm 48% 51%
Lesions > 15 cm 22% 22%
Total occlusions 38% 30%
Restenosis (all) 24% 26%
In-stent restenosis (ISR) 14% 16%
26
Zilver PTX stenting is effective in diabetics
Primary Patency (PSVR < 2.5)
Zilver PTXDiabetics
Zilver PTXNon-diabetics
86%
86%
Sabeti et al(Lesions ≥ 10 cm)
27
Zilver PTX effectiveness
in treating diabetics
with long SFA lesions
28
Baseline Lesion Characteristics
Single-Arm Study:
Diabetic Patients
Single-Arm Study:
Diabetics with long lesions
Lesions 298 67
Lesion length (mm) 98 ± 79 224 ± 54
Diameter stenosis 81 ± 17% 94 ± 12%
TASC 2000 class A 29% 3%
B 31% 6%
C 31% 59%
D 9% 32%
Lesions > 7 cm 51% 100%
Lesions > 15 cm 22% 100%
Total occlusions 30% 68%
Restenosis (all) 26% 38%
In-stent restenosis (ISR) 16% 27%
4/7/2011
8
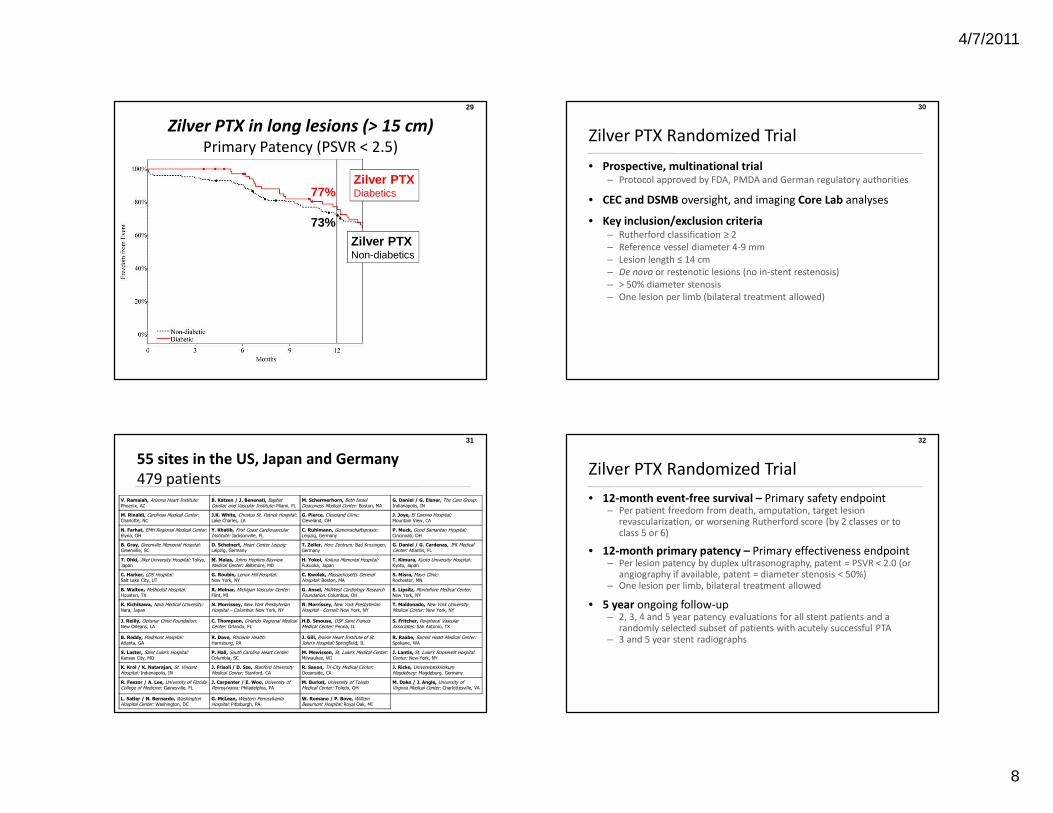
29
Zilver PTX in long lesions (> 15 cm)
Primary Patency (PSVR < 2.5)
77%
73%
Zilver PTXNon-diabetics
Zilver PTXDiabetics
30
• Prospective, multinational trial– Protocol approved by FDA, PMDA and German regulatory authorities
• CEC and DSMB oversight, and imaging Core Lab analyses
• Key inclusion/exclusion criteria– Rutherford classification ≥ 2
– Reference vessel diameter 4-9 mm
– Lesion length ≤ 14 cm
– De novo or restenotic lesions (no in-stent restenosis)
– > 50% diameter stenosis
– One lesion per limb (bilateral treatment allowed)
Zilver PTX Randomized Trial
31
V. Ramaiah, Arizona Heart Institute: Phoenix, AZ
B. Katzen / J. Benenati, Baptist Cardiac and Vascular Institute: Miami, FL
M. Schermerhorn, Beth Israel Deaconess Medical Center: Boston, MA
G. Daniel / G. Elsner, The Care Group: Indianapolis, IN
M. Rinaldi, Carolinas Medical Center: Charlotte, NC
J.K. White, Christus St. Patrick Hospital: Lake Charles, LA
G. Pierce, Cleveland Clinic: Cleveland, OH
J. Joye, El Camino Hospital: Mountain View, CA
N. Farhat, EMH Regional Medical Center: Elyria, OH
Y. Khatib, First Coast Cardiovascular Institute: Jacksonville, FL
C. Ruhlmann, Gemeinschaftspraxis: Leipzig, Germany
P. Muck, Good Samaritan Hospital: Cincinnati, OH
B. Gray, Greenville Memorial Hospital: Greenville, SC
D. Scheinert, Heart Center Leipzig: Leipzig, Germany
T. Zeller, Herz Zentrum: Bad Krozingen, Germany
G. Daniel / G. Cardenas, JFK Medical Center: Atlantis, FL
T. Ohki, Jikei University Hospital: Tokyo, Japan
M. Malas, Johns Hopkins Bayview Medical Center: Baltimore, MD
H. Yokoi, Kokura Memorial Hospital: Fukuoka, Japan
T. Kimura, Kyoto University Hospital: Kyoto, Japan
C. Harker, LDS Hospital: Salt Lake City, UT
G. Roubin, Lenox Hill Hospital: New York, NY
C. Kwolek, Massachusetts General Hospital: Boston, MA
S. Misra, Mayo Clinic: Rochester, MN
B. Walton, Methodist Hospital: Houston, TX
R. Molnar, Michigan Vascular Center: Flint, MI
G. Ansel, MidWest Cardiology Research Foundation: Columbus, OH
E. Lipsitz, Montefiore Medical Center: New York, NY
K. Kichikawa, Nara Medical University: Nara, Japan
N. Morrissey, New York Presbyterian Hospital – Columbia: New York, NY
N. Morrissey, New York Presbyterian Hospital - Cornell: New York, NY
T. Maldonado, New York University Medical Center: New York, NY
J. Reilly, Ochsner Clinic Foundation: New Orleans, LA
C. Thompson, Orlando Regional Medical Center: Orlando, FL
H.B. Smouse, OSF Saint Francis Medical Center: Peoria, IL
S. Fritcher, Peripheral Vascular Associates: San Antonio, TX
B. Reddy, Piedmont Hospital: Atlanta, GA
R. Dave, Pinnacle Health: Harrisburg, PA
J. Gill, Prairie Heart Institute of St. John’s Hospital: Springfield, IL
R. Raabe, Sacred Heart Medical Center: Spokane, WA
S. Laster, Saint Luke’s Hospital: Kansas City, MO
P. Hall, South Carolina Heart Center: Columbia, SC
M. Mewissen, St. Luke’s Medical Center: Milwaukee, WI
J. Lantis, St. Luke’s Roosevelt Hospital Center: New York, NY
K. Krol / K. Natarajan, St. Vincent Hospital: Indianapolis, IN
J. Frisoli / D. Sze, Stanford University Medical Center: Stanford, CA
R. Saxon, Tri-City Medical Center: Oceanside, CA
J. Ricke, Universitatsklinikum Magdeburg: Magdeburg, Germany
R. Feezor / A. Lee, University of Florida College of Medicine: Gainesville, FL
J. Carpenter / E. Woo, University of Pennsylvania: Philadelphia, PA
M. Burket, University of Toledo Medical Center: Toledo, OH
M. Dake / J. Angle, University of Virginia Medical Center: Charlottesville, VA
L. Satler / N. Bernardo, Washington Hospital Center: Washington, DC
G. McLean, Western Pennsylvania Hospital: Pittsburgh, PA
W. Romano / P. Bove, William Beaumont Hospital: Royal Oak, MI
55 sites in the US, Japan and Germany
479 patients
32
• 12-month event-free survival – Primary safety endpoint– Per patient freedom from death, amputation, target lesion
revascularization, or worsening Rutherford score (by 2 classes or to class 5 or 6)
• 12-month primary patency – Primary effectiveness endpoint– Per lesion patency by duplex ultrasonography, patent = PSVR < 2.0 (or
angiography if available, patent = diameter stenosis < 50%)– One lesion per limb, bilateral treatment allowed
• 5 year ongoing follow-up– 2, 3, 4 and 5 year patency evaluations for all stent patients and a
randomly selected subset of patients with acutely successful PTA– 3 and 5 year stent radiographs
Zilver PTX Randomized Trial
4/7/2011
9
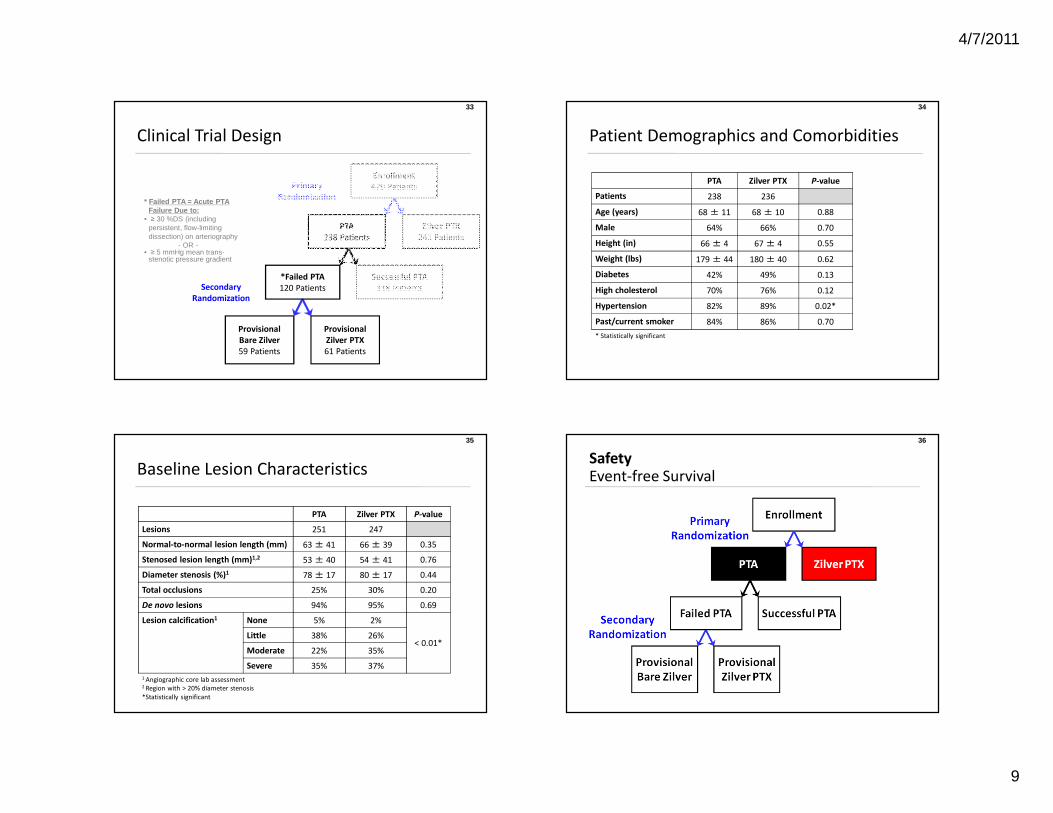
33
Clinical Trial Design
* Failed PTA = Acute PTA Failure Due to:
• ≥ 30 %DS (including persistent, flow-limiting dissection) on arteriography
- OR -• ≥ 5 mmHg mean trans-
stenotic pressure gradient
Enrollment
479 Patients
PTA
238 Patients
Successful PTA
118 Patients
Provisional
Bare Zilver
59 Patients
*Failed PTA
120 Patients
Zilver PTX
241 Patients
Provisional
Zilver PTX
61 Patients
Primary
Randomization
Secondary
Randomization
34
Patient Demographics and Comorbidities
PTA Zilver PTX P-value
Patients 238 236
Age (years) 68 ± 11 68 ± 10 0.88
Male 64% 66% 0.70
Height (in) 66 ± 4 67 ± 4 0.55
Weight (lbs) 179 ± 44 180 ± 40 0.62
Diabetes 42% 49% 0.13
High cholesterol 70% 76% 0.12
Hypertension 82% 89% 0.02*
Past/current smoker 84% 86% 0.70
* Statistically significant
35
Baseline Lesion Characteristics
PTA Zilver PTX P-value
Lesions 251 247
Normal-to-normal lesion length (mm) 63 ± 41 66 ± 39 0.35
Stenosed lesion length (mm)1,2 53 ± 40 54 ± 41 0.76
Diameter stenosis (%)1 78 ± 17 80 ± 17 0.44
Total occlusions 25% 30% 0.20
De novo lesions 94% 95% 0.69
Lesion calcification1 None 5% 2%
< 0.01*Little 38% 26%
Moderate 22% 35%
Severe 35% 37%
1 Angiographic core lab assessment 2 Region with > 20% diameter stenosis
*Statistically significant
36
SafetyEvent-free Survival
4/7/2011
10
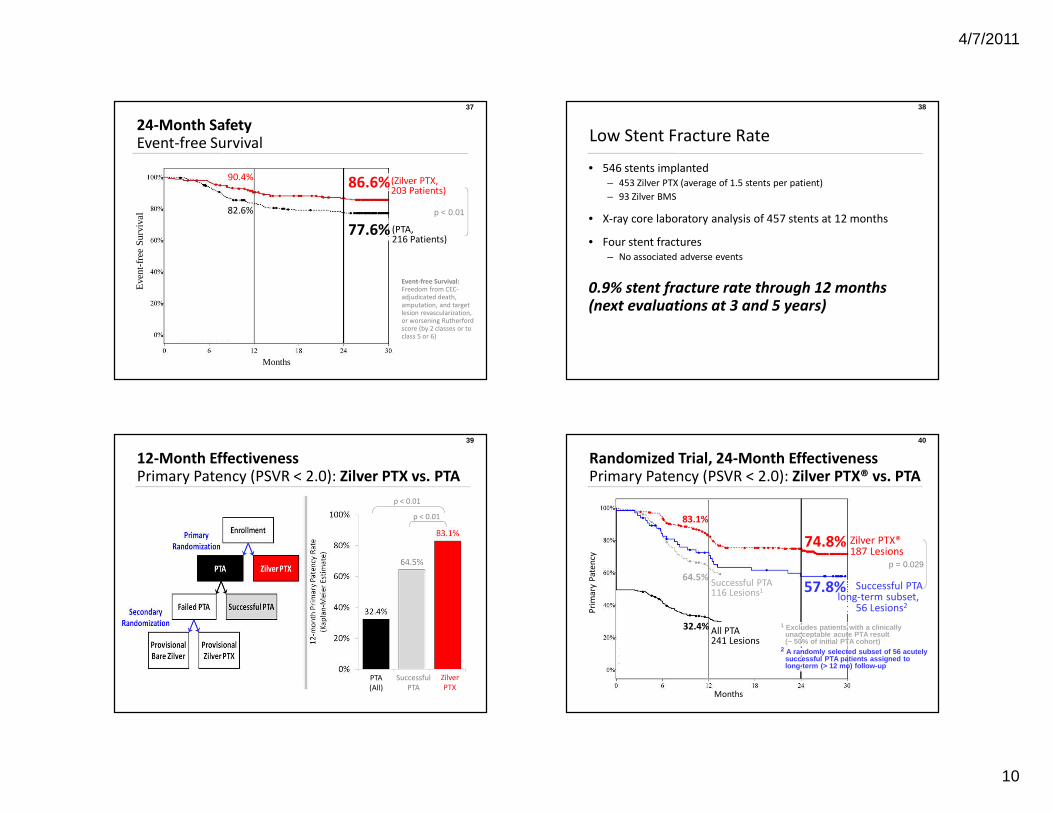
37
24-Month SafetyEvent-free Survival
77.6%(n = 216 patients)
90.4%
82.6%82.6%
86.6%
Eve
nt-f
ree
Surv
ival
Event-free Survival: Freedom from CEC-adjudicated death, amputation, and target lesion revascularization, or worsening Rutherford score (by 2 classes or to class 5 or 6)
77.6%
p < 0.01
(Zilver PTX,203 Patients)
(PTA,216 Patients)
Months
38
Low Stent Fracture Rate
• 546 stents implanted
– 453 Zilver PTX (average of 1.5 stents per patient)
– 93 Zilver BMS
• X-ray core laboratory analysis of 457 stents at 12 months
• Four stent fractures
– No associated adverse events
0.9% stent fracture rate through 12 months(next evaluations at 3 and 5 years)
39
12-Month EffectivenessPrimary Patency (PSVR < 2.0): Zilver PTX vs. PTA
Zilver
PTXPTA
(All)
p < 0.01
Zilver
PTX
Successful
PTA
p < 0.01
40
Pri
ma
ry P
ate
ncy
Months
Randomized Trial, 24-Month EffectivenessPrimary Patency (PSVR < 2.0): Zilver PTX® vs. PTA
83.1%
64.5%57.8%
32.4%
Successful PTA116 Lesions1
All PTA241 Lesions
Successful PTA long-term subset,
56 Lesions2
Zilver PTX®187 Lesions
p = 0.029
1 Excludes patients with a clinically unacceptable acute PTA result (~ 50% of initial PTA cohort)
2 A randomly selected subset of 56 acutely successful PTA patients assigned to long-term (> 12 mo) follow-up
74.8%
4/7/2011
11
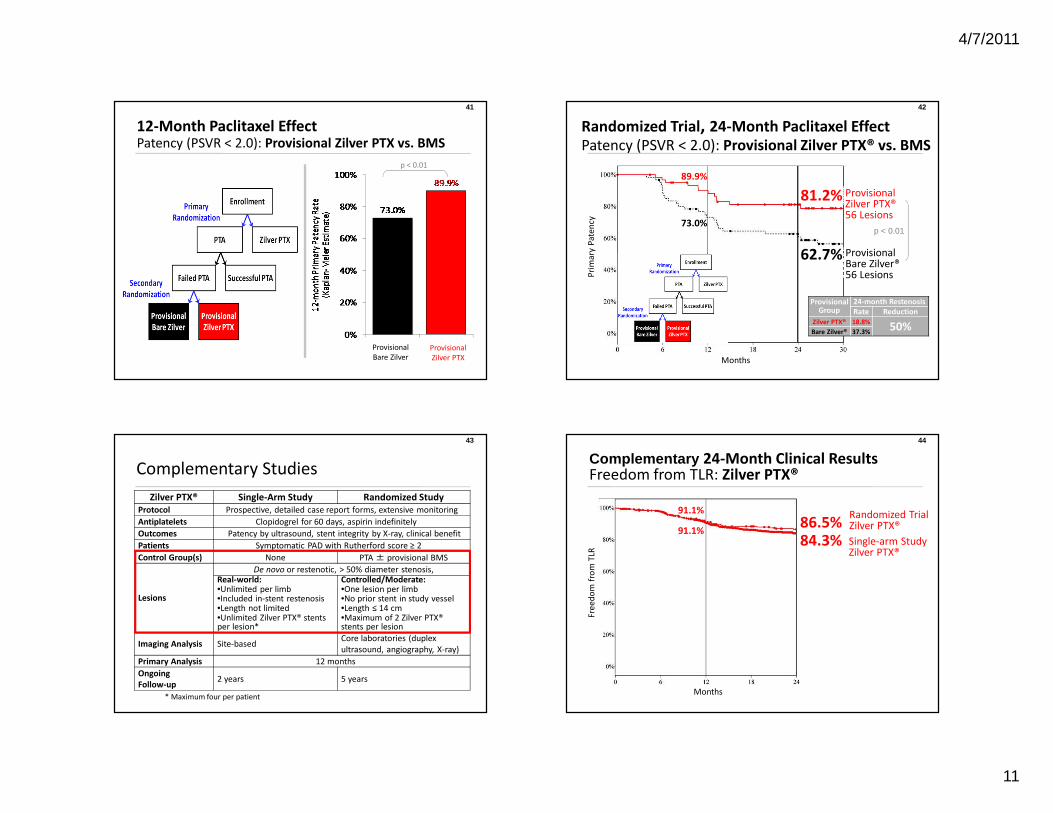
41
12-Month Paclitaxel EffectPatency (PSVR < 2.0): Provisional Zilver PTX vs. BMS
Zilver PTXProvisional
Bare Zilver
Provisional
Zilver PTX
p < 0.01
42
Pri
ma
ry P
ate
ncy
Months
Randomized Trial, 24-Month Paclitaxel EffectPatency (PSVR < 2.0): Provisional Zilver PTX® vs. BMS
89.9%
ProvisionalBare Zilver®56 Lesions
Provisional Zilver PTX® 56 Lesions
73.0%
ProvisionalGroup
24-month Restenosis
Rate Reduction
Zilver PTX® 18.8%50%
Bare Zilver® 37.3%
p < 0.01
81.2%
62.7%
43
Complementary Studies
Zilver PTX® Single-Arm Study Randomized Study
Protocol Prospective, detailed case report forms, extensive monitoring
Antiplatelets Clopidogrel for 60 days, aspirin indefinitely
Outcomes Patency by ultrasound, stent integrity by X-ray, clinical benefit
Patients Symptomatic PAD with Rutherford score ≥ 2
Control Group(s) None PTA ± provisional BMS
Lesions
De novo or restenotic, > 50% diameter stenosis, Real-world:•Unlimited per limb•Included in-stent restenosis•Length not limited•Unlimited Zilver PTX® stents per lesion*
Controlled/Moderate:•One lesion per limb•No prior stent in study vessel•Length ≤ 14 cm•Maximum of 2 Zilver PTX® stents per lesion
Imaging Analysis Site-basedCore laboratories (duplex
ultrasound, angiography, X-ray)
Primary Analysis 12 months
Ongoing
Follow-up2 years 5 years
* Maximum four per patient
44
Complementary 24-Month Clinical ResultsFreedom from TLR: Zilver PTX®
Randomized Trial Zilver PTX®
Fre
ed
om
fro
m T
LR
Months
91.1%
Single-arm Study Zilver PTX®
84.3%86.5%
91.1%
4/7/2011
12
45
Summary
• Drug and device combination opportunities will
continue to grow with technological advances
that promise to impact clinical practice and
transform medicine. High quality data is critical
to our understanding of what role these
therapies will legitimately play. Political,
regulatory and economic forces will have key
roles in creating these changes. Without a doubt,
we all need to prepare for these inevitable
developments.







