Download - Mark Horton MD MSPH April 28, 2011 The Economy, Health Care Reform and TB Control in California

Mark Horton MD MSPH April 28, 2011
The Economy, Health Care Reform
and TB Control in California

• The TB Landscape
• Economic and Budgetary Pressures on TB Control Activities
• Health Care Reform: Challenges and Opportunities for TB Control
• The Role of Local Public Health in TB Control
2

The TB Landscape
3

Tuberculosis in California
– New active cases at a historic low, BUT– California reports the largest number of TB
cases in the U.S.– Reservoir of latent TB infection (LTBI)
exceeds three million persons– LTBI pool is major source for California’s
future TB cases– Reactivation in 1 of 10 LTBI patients– Local transmission indicated by TB in children
and new outbreaks
4

TB Disease Burden in CA
2,329 New Cases (’10)
Over 10,000 Suspect Cases
20,000 – 30,000 Contacts
3 million Californians infected
35 million Californians at risk
5
6
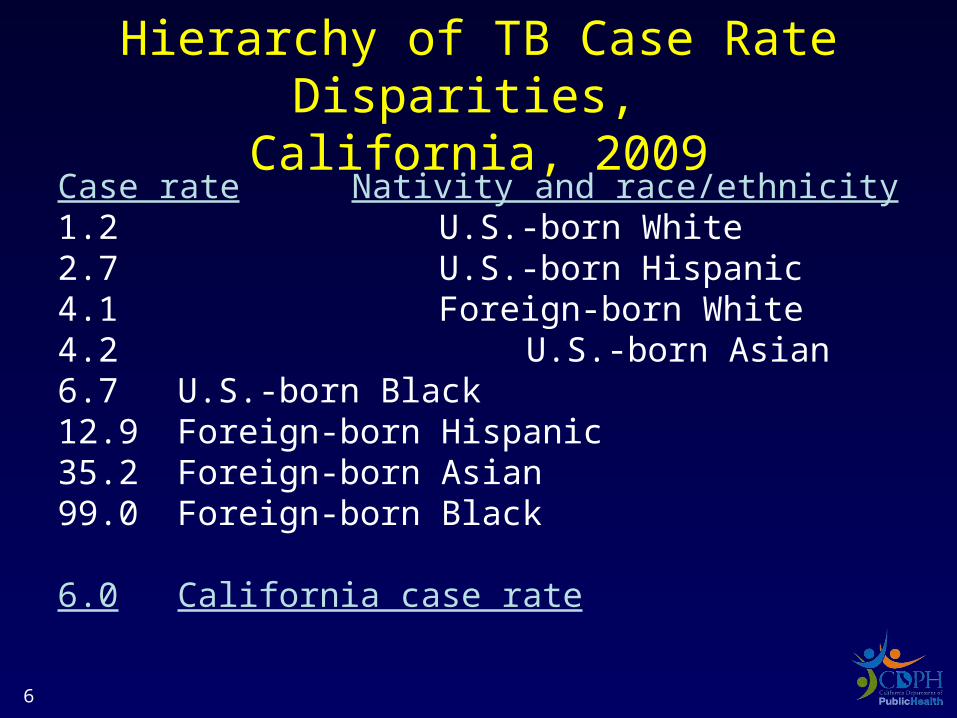
Hierarchy of TB Case Rate Disparities, California, 2009
Case rate Nativity and race/ethnicity1.2 U.S.-born White2.7 U.S.-born Hispanic4.1 Foreign-born White4.2 U.S.-born Asian6.7 U.S.-born Black12.9 Foreign-born Hispanic35.2 Foreign-born Asian99.0 Foreign-born Black
6.0 California case rate
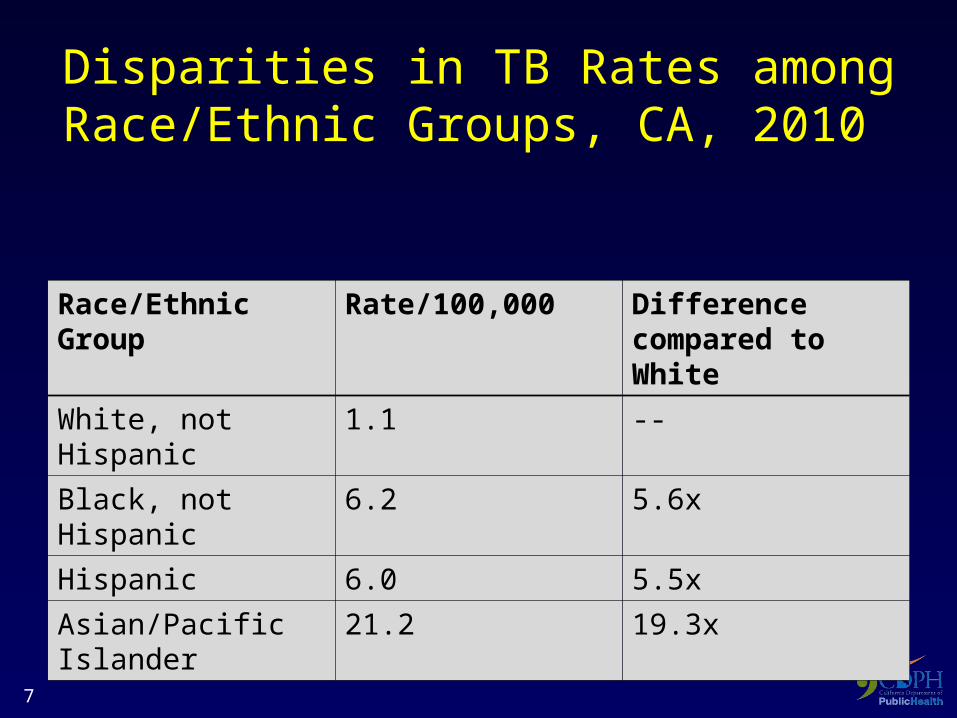
Disparities in TB Rates among Race/Ethnic Groups, CA, 2010
Race/Ethnic Group Rate/100,000 Difference compared to White
White, not Hispanic 1.1 --
Black, not Hispanic 6.2 5.6x
Hispanic 6.0 5.5x
Asian/Pacific Islander
21.2 19.3x
7

TB Case Rate Disparity by Nativity
U.S.-born 1.8
Foreign-born 18.1
8

California’s Population
Compared to US population
•More likely to be
– Asian (13% vs. 5%)
– Hispanic (37% vs. 16%)
– Foreign-born ( 27% vs. 13%)
Changes in CA
•50% increase in persons over 65 in past decade
9

Challenges
• Identify, investigate and aggressively manage cases/outbreaks
• Reduce the pool of LTBI
• Maximize disease prevention
• Focus on Disparities
• Heighten awareness
10
California’s Economy
• California is one of the world’s largest economies: $1.9 trillion in 2009
• For the first time since 1938, in 2009, personal income declined in California
• Between July 2007-2010 , California lost 1.3 million jobs (>12% unemployment)
Source: California FACTS, January 2011, LAO
11
Resource Reductions : CDPH
• ‘08 – ’09: 10% General Fund (GF) reduction
• ‘09 – ’10: Targeted GF Reductions
– HIV
– MCAH
– Immunizations
– MediCal
• Other: Furloughs, Hiring freeze
12

The Economy and Local Health Department TB programs in California
• Many LHDs struggling to provide critical services to uninsured populations
• TB control positions lost
• Some TB control activities have stopped that previously contributed to
– early detection of TB
– prevention of TB spread
13

Trend in Local Health Department TB Program FTEs, 2006-2010
14
Specific impact reported by California local TB programs
• Most experienced: – decrease in funding – reductions in staff
• Resulting in decreased capacity: – to monitor disease trends – to respond to outbreaks
Source: TB Program Assessment Tool
California TB Control Branch, 201015
Impact on CA TB Programs 2010-2011
• 50% experienced increase in case manager patient load
• 25% decreased number of patients on DOT• 30% had delays in contact investigations• 30% decreased clinic services• 35% decreased staff training• 10% decreased reporting capacity to state• Source: TB program assessment tool
16
How may economic pressures affect TB patients?
• Patients delay seeking care• Present with more advanced disease• More patients hospitalized• Patients remain infectious longer and more likely
to spread to families and community
• Patients can’t afford co-pay for drugs and visits• Patients abandon treatment• Patients more likely to develop MDRTB
17

Patient example in California2010
When patients and programs cannot afford TB care:
•Patient with MDR and TB program unable to pay for MDR TB drugs
•Experienced delays in MDR TB treatment initiation
18

Programmatic Priorities in Face of Reduced Budgets
• Re-prioritize programmatic performance targets
• Continue to focus attention/resources on populations at risk
• Prioritize implementation of new evidence-based diagnostics and treatment regimens
• Strengthen partnerships
• Enhance public awareness
19

TB Control Indicators
• Diagnosis
– Culture identification
– HIV status determination
• Treatment
– Recommended Initial Therapy
– Timely Treatment
– Directly Observed therapy
– Culture conversion
– Completion of therapy
• Surveillance
– Timely Reporting
– Complete reporting– Universal genotyping
• Contact Investigation
– Contacts elicited, evaluated, treated
• Adverse Events
– TB Deaths
– Pediatric cases
• TB Control Outcomes
– Case rates
20

21
Program evaluation: California’s Report Card
• Culture conversion within 60 days• COT within 1 year• Contact evaluation• Sputum culture reported• Drug susceptibility results• Universal genotyping• Recommended initial therapy
---------------------------------U.S. average ------------------------------• Contacts elicited• Foreign-born TB case rate • Data reporting: RVCT• U.S.-born TB case rate • Pediatric TB case rate • African-American TB case rate • LTBI treatment completion for contacts• LTBI treatment initiation for contacts• TB case rate (overall)• Known HIV status
Better
Worse

Health Care Reform and TB
• What’s the Problem?
• Opportunities in HCR
• Partnerships
22

The Problem
• Persons with TB need access to prompt medical care and drug treatment to halt transmission to others and prevent TB from spreading in communities
• Uncontrolled TB transmission jeopardizes public health
• Vast population with latent infection is persistent source of future cases
23

The Problem
• TB diagnosis is slow and often tricky
– Many outpatient visits or inpatient days may be needed for a TB diagnosis
• TB treatment is lengthy
– TB treatment requires multiple drugs, frequent medical monitoring, laboratory testing, and interaction with health professionals for up to 24 months
24

The Problem: Gaps Expected in Health Insurance
Coverage
Many California residents will remain uninsured due to:
• residency requirements• income thresholds • lapses in insurance coverage
25
The Problem: Barriers to Affordable Care
• Co-pays and other share of cost provisions are a significant barrier for critical public health services to uninsured as well as insured persons (eg infectious TB evaluation)
26
The Problem: TB services not covered
Public health activities for key uncovered populations not part of HCR:
•TB diagnosis and treatment
•Patient isolation
•DOT/Case management
•Outbreak/contact investigation
27

Opportunities for Public Healthin HCR
– Expanded Access
– Focus on Prevention
– Focus on Quality
28
Expanded Access
• Medicaid expansion
• Insurance Reform
• Expansion of System Capacity
29
Expanded Access: Insurance Reform
• Mandatory individual health insurance• No pre-existing conditions• No dropping coverage for illness• No maximum life-time benefit• Children covered until 26 yrs on parent policy• Mandatory no-cost coverage of CPS• Tax incentive for small employers• Health Insurance exchanges• Subsidized health insurance premiums
30

Expanded Access: System Capacity
• Expansion of Community Clinic Networks
• Expansion of Primary Care
31

Focus on Prevention
• Public Health and Wellness
– Council
– Prevention Framework
– Fund
• No cost coverage of CPS
32

Prevention and Wellness Fund
• Public Health infrastructure improvement
• Epidemiology and laboratory capacity
• HIV reporting
• Home Visitation
• Community transformation
• Public health education/training
33
Mandatory No Cost Coverage of CPS
• ACIP
• USPSTF
• Bright Futures
• Preventive Services for Women
34

Specific Opportunities to Further TB Control
• 3.4 million more Californians will have a regular source of health care
• More people will be under care for conditions that promote TB progression
(eg diabetes, smoking, ESRD, HIV) • Expanded opportunities for early TB
detection and TB disease prevention• LTBI testing and treatment of high risk
groups can become routine35

Focus on Quality: Accountable Care Organizations
ACOs mandated to:
– Improve the efficiency and effectiveness of health services
– Control costs
– Focus on prevention
36

Partnerships
• Community Clinics/FQHCs
• Public Hospitals
• Private Hospitals/practitioners
37

Models for public health care delivery
• Referral of TB patients to public health clinic
• Contract with private or FQHC providers for TB services
• Both models currently in operation within California
38

Challenges with TB service partnership models
• Partners may have less experience with TB case management and prevention
• Difficult to accomplish patient centered management to extent performed by TB programs
• Responsibility for population protections and surveillance needs strong public health infrastructure
39

Charge of Health Departments and FQHCs
LHDs: Population health and health-condition-specific clinical services
FQHCs: Full continuum of primary and preventive care services
40

Populations served by community health centers overlap with populations at risk for
TB
• Overlapping populations means increased access to care for many patients at high risk for TB
• Source: National Association of Community Health Centers 2010
• Disproportionately low-income
• Most uninsured or publically insured
• Most members of racial/ethnic minority
41

Partnership: LHDs and FQHCs
Well positioned to be strong partners with long history of coming together to improve both individual and population health
Common goals:
– Improve health of target populations
– Eliminate health disparities
– Promote health equity
42
Partnerships: Community Health Centers
LHD and FQHC partnership needed to meet ACA goals:•Address health issues of underserved•Eliminate disparities•Improve and document value of interventions/services•Use of health information to improve population health
43

Partnership Examples: promote individual and population health
• Smoking cessation in patients with LTBI prevents TB disease
• Treat LTBI in diabetics- prevent disease progression
• Identification and treatment of LTBI among HIV-infected can prevent TB
• Decrease mortality in TB/HIV- Identify HIV infection in TB patients; promote HAART
44

Partnership: Public Hospitals
• New funds to public hospitals to cover expanded patients and improve care quality
• State and LHDs have lead role to define best practices/standards related to TB care and control– Show what is cost-effective– Role in measuring outcomes and creating
/implementing measures
45
Partnerships: Private Providers
• Private providers care for nearly half of TB patients
• Opportunities for better prevention and case management through partnership
• LHDs needed for TB subject matter expertise and disease control functions
46

47
TB Deaths during Therapy, by Provider Type, 1994-2009
0
2
4
6
8
10
12
14
16
18
20
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
Year
Per
cen
t
Private Provider
Health Department
Role of Public Health Departments
• TB surveillance:
– oversee reporting and case registries
– Epidemiologic trend analysis
– Monitoring TB control /outcome measures
• Define/ promote evidence-based interventions
– Develop and communicate TB control best practices and standards
48

Role of Public Health Departments
• Case management
– DOT
– Expert consultation
– Interjurisidictional transfer of care
• Community disease control
– Response to outbreaks
– Extended contact investigations
– Media releases
– Public and provider education49
Exciting Innovations for TB Dx and Rx
• Rapid diagnostics for TB and LTBI
• Shorter course treatment for LTBI
50

How can public health departments lead the way?
• Ensure these innovations are understood:
– What is the evidence they work?
– Are they better than the old tools?
– Do they improve outcomes?
• Ensure innovations are absorbed and accessible
– Provide technical expertise
– Provide guidance to providers
– Evaluate implementation
51

Summary
• California TB Landscape
• Economic and Budgetary Challenges
• Health Care Reform
• Focus on Partnerships
• Role of Local Health Departments
52

. . I am prejudiced beyond debate
In favor of my right to choose
Who will feel
The stubborn ounces of my weight
--B. Overstreet
53







