Download - Mandibular fractures

MANDIBULAR FRACTURES

Contents.
Introduction.
Surgical anatomy
History.
Epidemiology.
Classification systems
Clinical features and diagnosis
Radiographic features
Conclusion.
References.

Introduction.
Maxillofacial injuries.
Mandibular fractures –
prominence of mandible
Occlusion
Management.
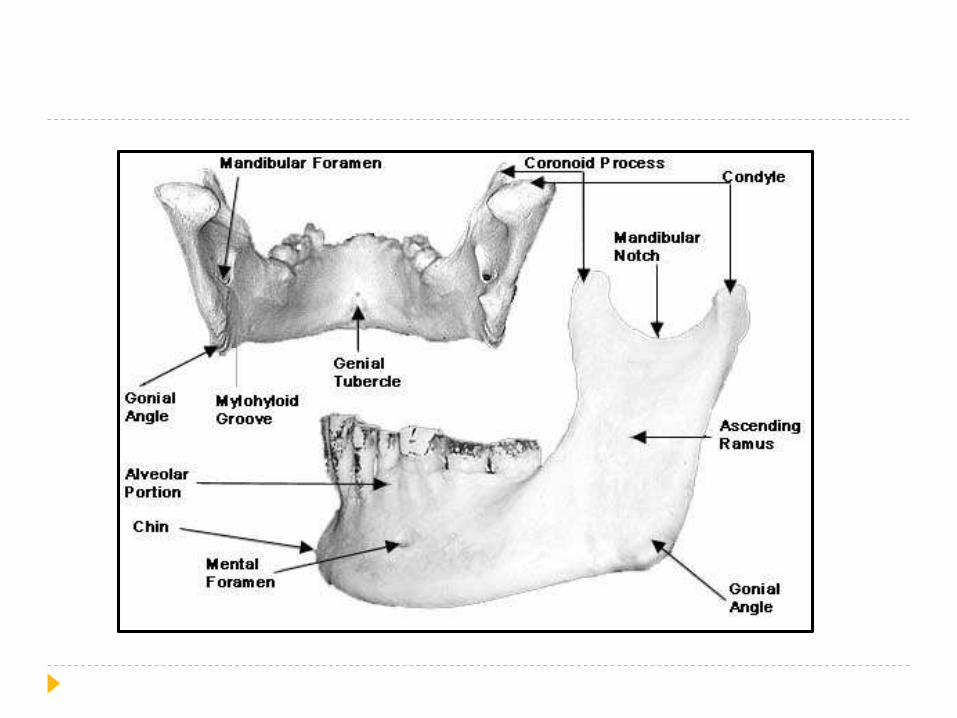
Surgical anatomy
Strongest facial bone
Parabola shaped bone
Angle of curvature is 110-140°
Mandible is the 2nd bone to ossify
Energy of 44.6-74.4 kg/m required to fracture the
mandible.
Weak areas of mandible
Junction between alveolar bone & basal mandibularbone.
Symphysis region - junction of two individual bones.
Parasymphyseal region - lateral to the mentalprominence, incisive fossa and mental foramen.
Junction of the ramus and the body are fracturedcommonly.
Presence of impacted tooth, canine with long roots.
Age changes of mandible.
Mental foramena.
child – near inferior border.
old age – near alveolar ridge.
Ramus angle.
child & old – obtuse
Alveolar ridge
Blood supply
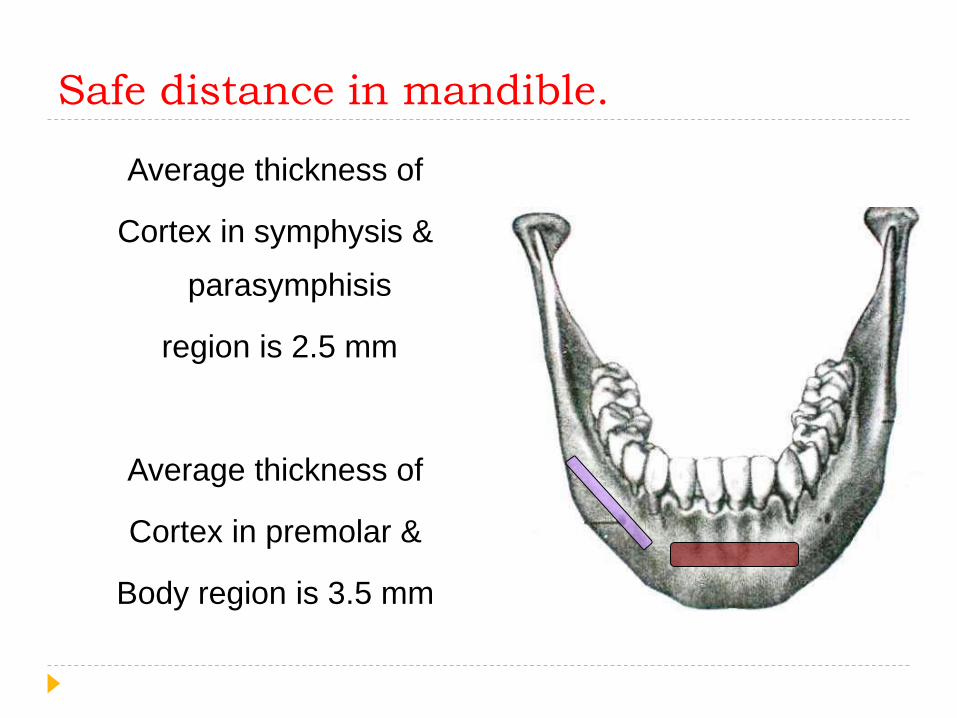
Safe distance in mandible.
Average thickness of
Cortex in symphysis &
parasymphisis
region is 2.5 mm
Average thickness of
Cortex in premolar &
Body region is 3.5 mm
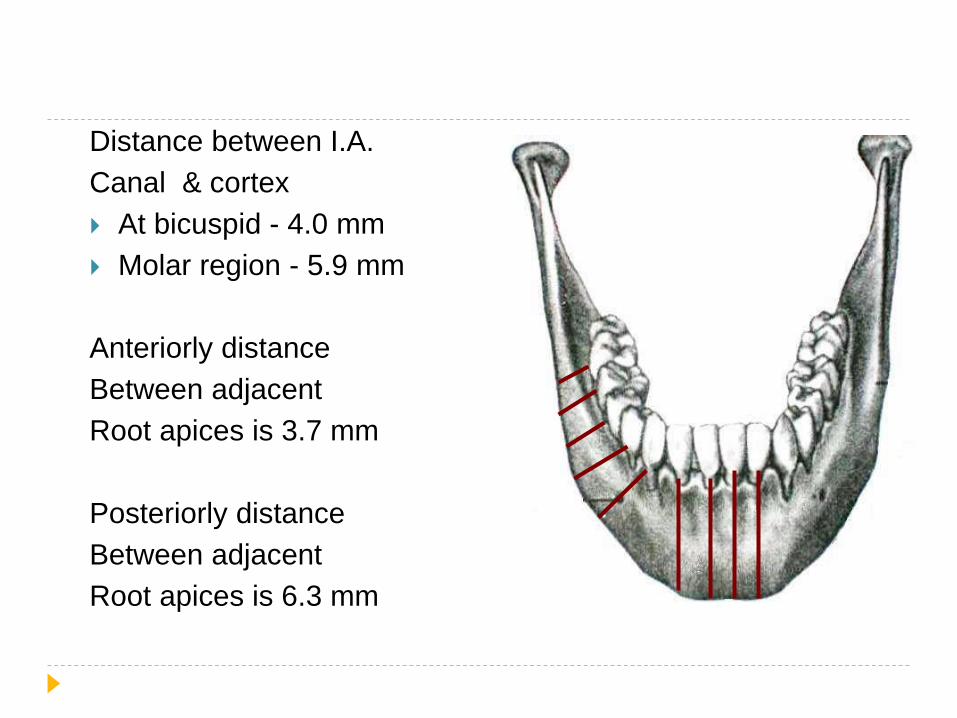
Distance between I.A.
Canal & cortex
At bicuspid - 4.0 mm
Molar region - 5.9 mm
Anteriorly distance
Between adjacent
Root apices is 3.7 mm
Posteriorly distance
Between adjacent
Root apices is 6.3 mm
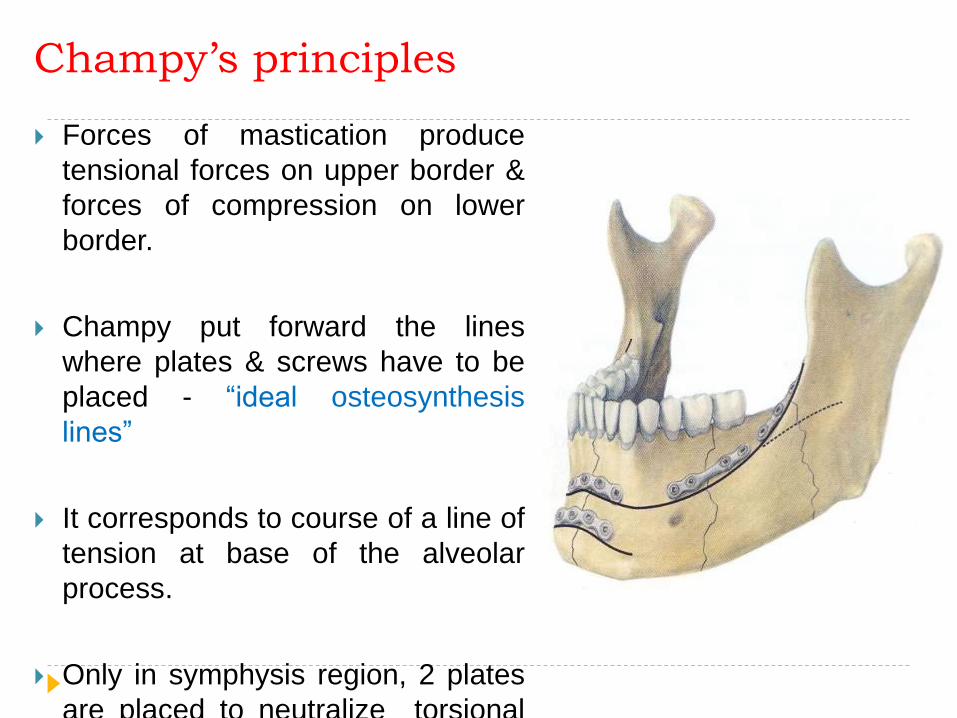
Champy’s principles
Forces of mastication produce
tensional forces on upper border &
forces of compression on lower
border.
Champy put forward the lines
where plates & screws have to be
placed - “ideal osteosynthesis
lines”
It corresponds to course of a line of
tension at base of the alveolar
process.
Only in symphysis region, 2 plates
are placed to neutralize torsional
forces.
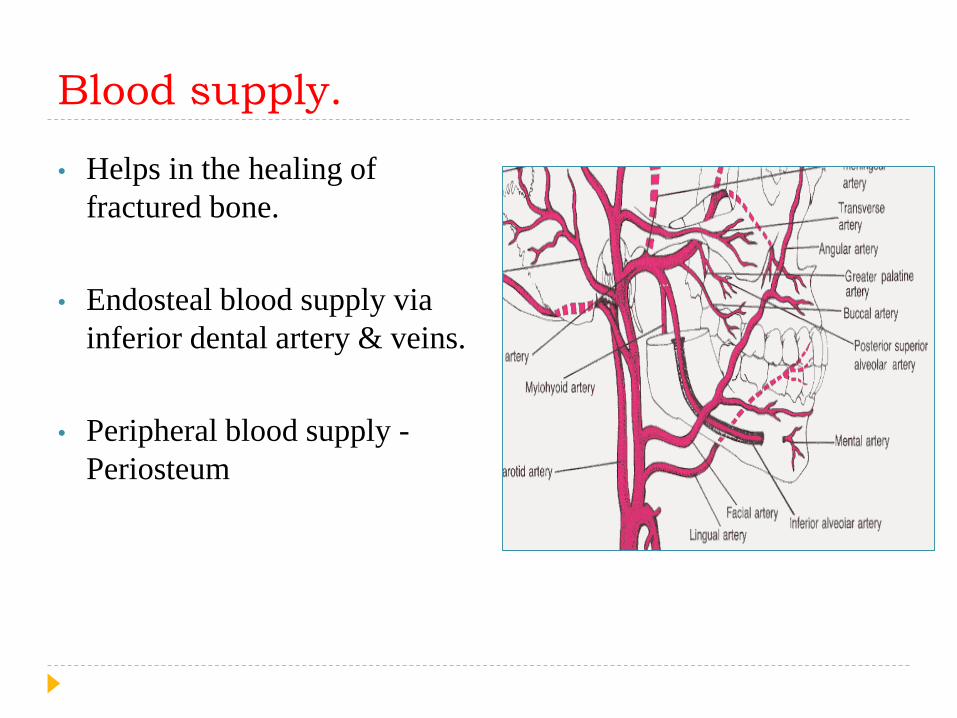
Blood supply.
• Helps in the healing of
fractured bone.
• Endosteal blood supply via
inferior dental artery & veins.
• Peripheral blood supply -
Periosteum

Nerve supply.
• Inferior alveolar nerve
• Damage - angle & body #
• Anesthesia or parasthesia of
the nerve
• Recovery / regeneration - 3 to
12 months
History. Egyptian Papyrus (1650 BC) –
Examination, diagnosis & treatment.
Hippocrates – Approximation of # segments.
Salerno, Italy (1180) – Proper occlusion.
1492, the book Cyrurgia by Guglielmo Salicetti – use of IMF.
John Barton - Barton Bandage
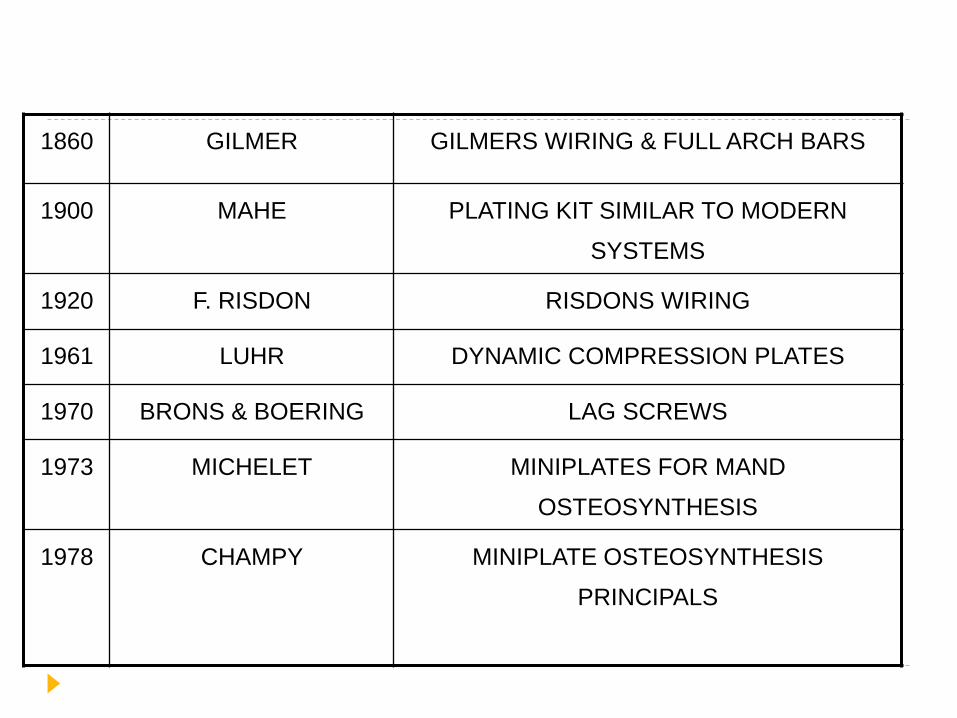
1860 GILMER GILMERS WIRING & FULL ARCH BARS
1900 MAHE PLATING KIT SIMILAR TO MODERN
SYSTEMS
1920 F. RISDON RISDONS WIRING
1961 LUHR DYNAMIC COMPRESSION PLATES
1970 BRONS & BOERING LAG SCREWS
1973 MICHELET MINIPLATES FOR MAND
OSTEOSYNTHESIS
1978 CHAMPY MINIPLATE OSTEOSYNTHESIS
PRINCIPALS
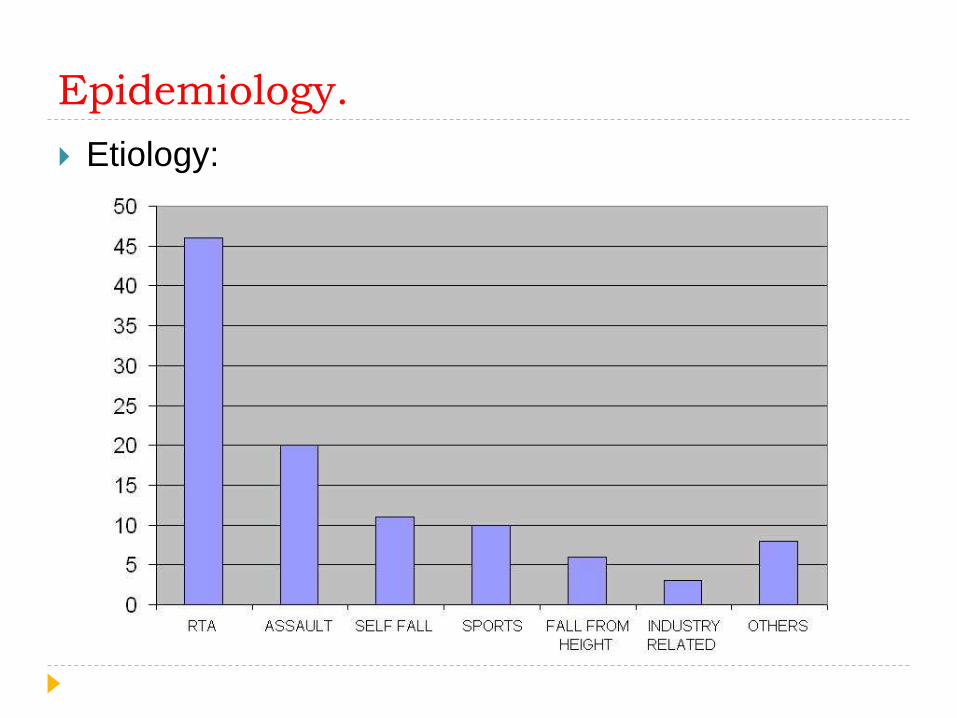
Epidemiology.
Etiology:
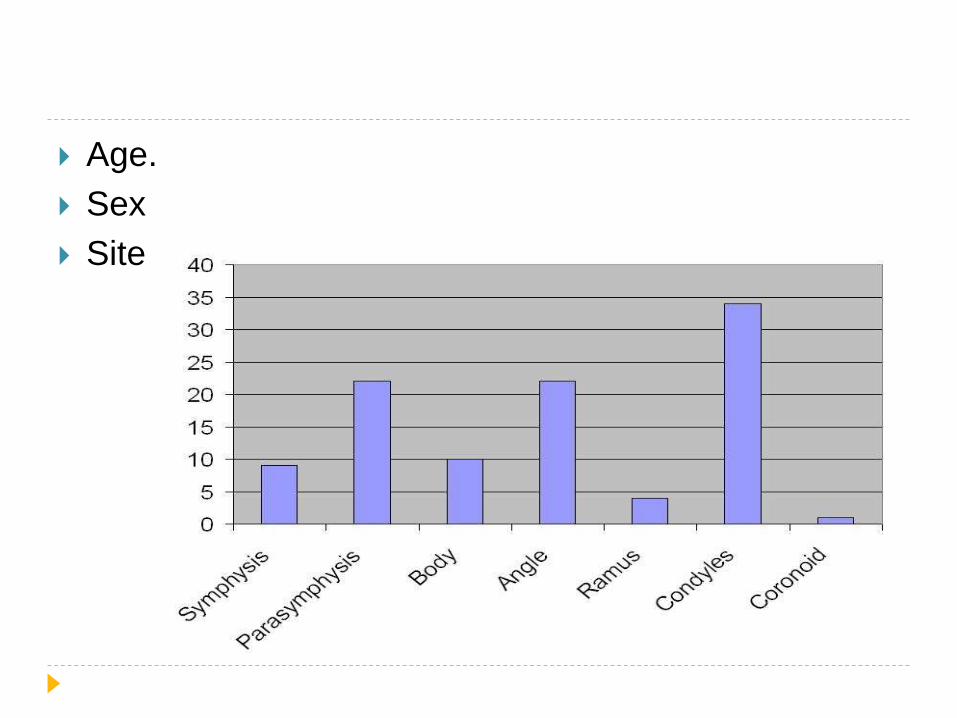
Age.
Sex
Site
CAR ACCIDENTS
ASSAULTS
BIKE ACCIDENTS

Classification
General
Anatomical
Completeness
Mechanism of injury
Number of fragments
Shape of fracture
Direction & favorability of treatment
Presence or absence of teeth
AO classification.
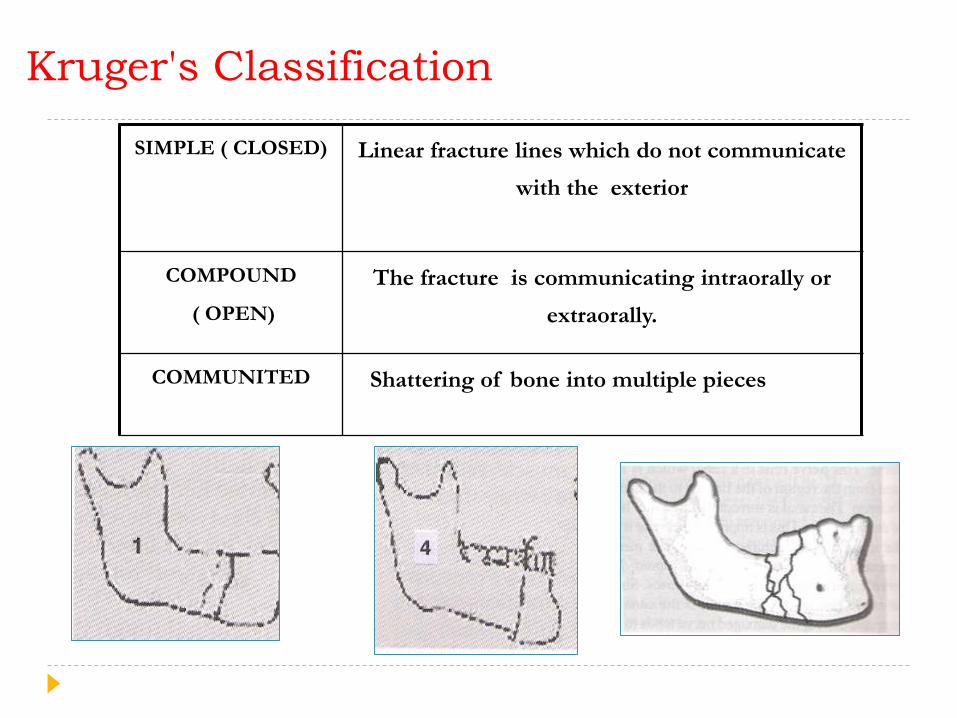
Kruger's Classification
SIMPLE ( CLOSED) Linear fracture lines which do not communicate
with the exterior
COMPOUND
( OPEN)
The fracture is communicating intraorally or
extraorally.
COMMUNITED Shattering of bone into multiple pieces
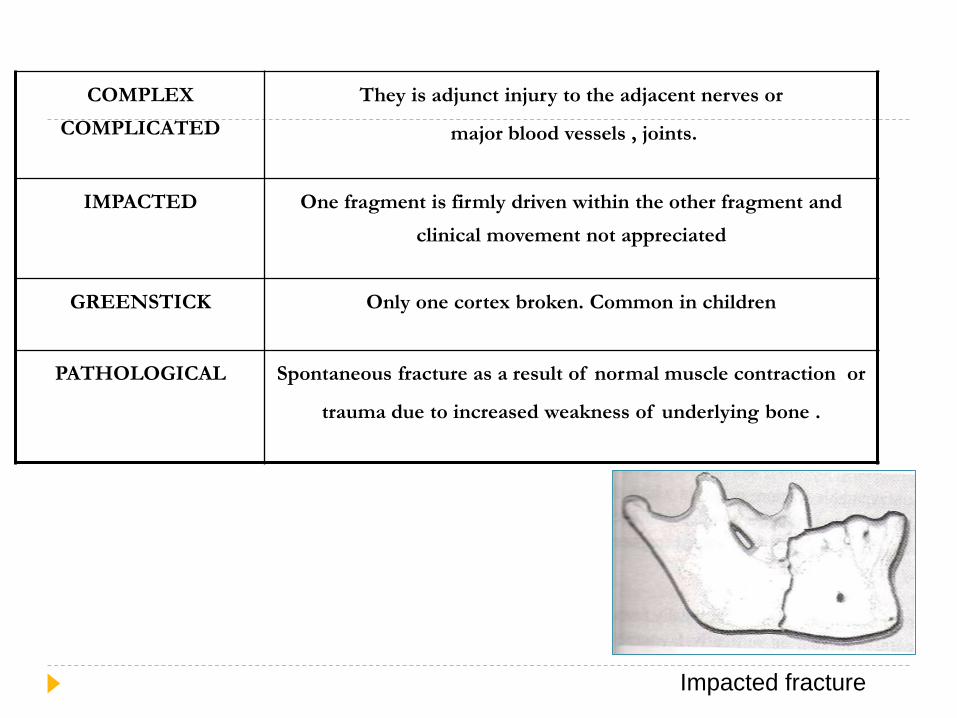
COMPLEX
COMPLICATED
They is adjunct injury to the adjacent nerves or
major blood vessels , joints.
IMPACTED One fragment is firmly driven within the other fragment and
clinical movement not appreciated
GREENSTICK Only one cortex broken. Common in children
PATHOLOGICAL Spontaneous fracture as a result of normal muscle contraction or
trauma due to increased weakness of underlying bone .
Impacted fracture
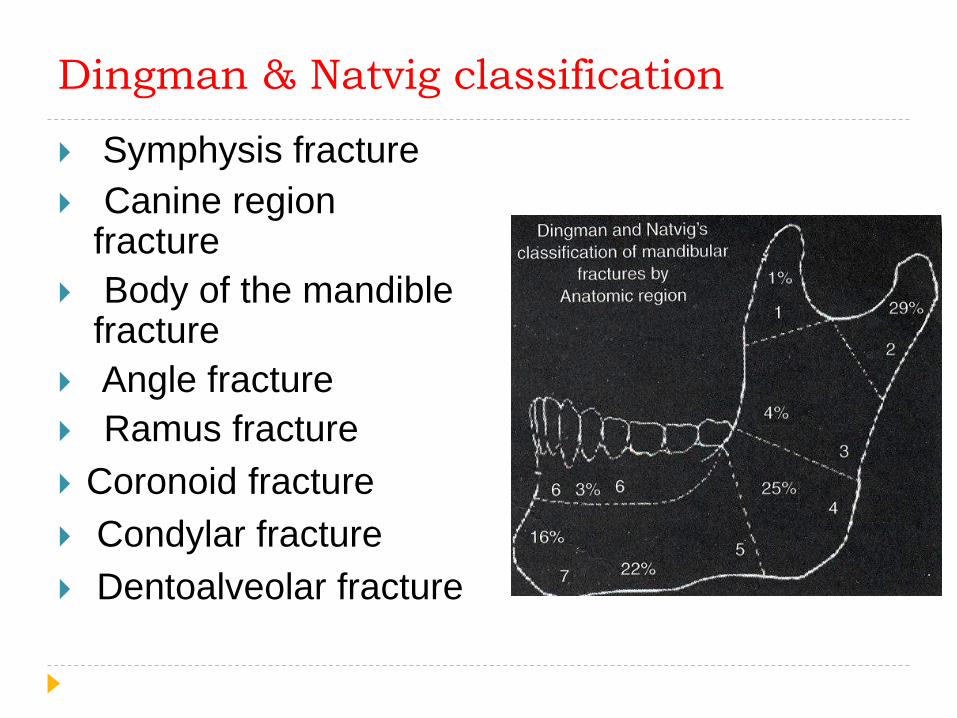
Dingman & Natvig classification
Symphysis fracture
Canine region fracture
Body of the mandible fracture
Angle fracture
Ramus fracture
Coronoid fracture
Condylar fracture
Dentoalveolar fracture

Direction & favorability of treatment
Horizontally Favourable
Fracture line runs
downward & forward so
upward displacement
avoided
HorizontallyUnfavourable
Fracture line runs Down
Wards and Back Wardsso
upward Displacement
Unrestricted
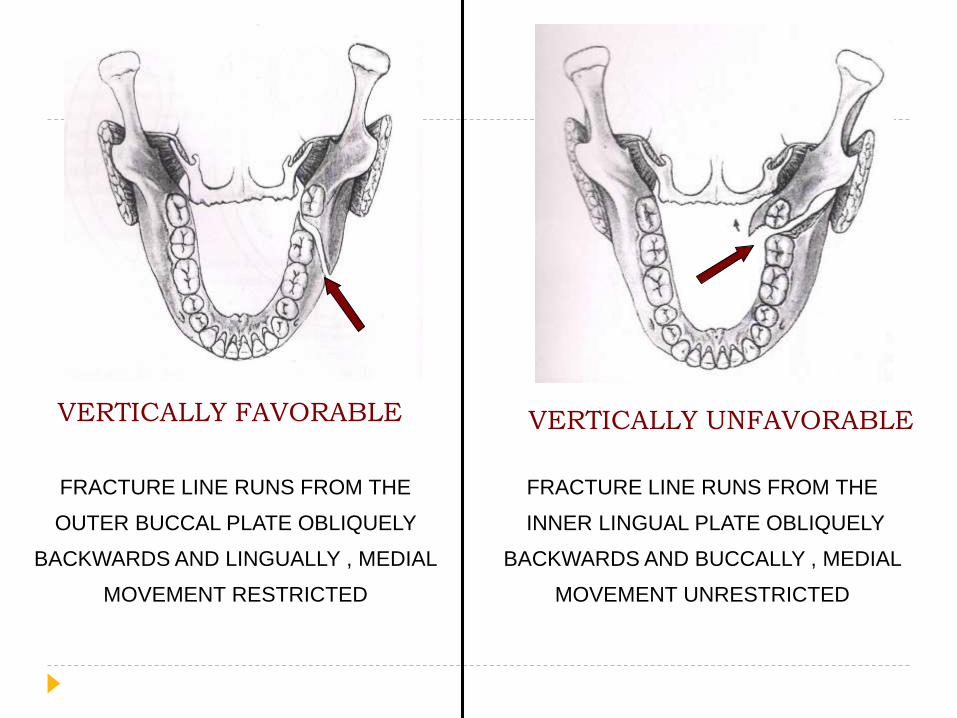
VERTICALLY FAVORABLE VERTICALLY UNFAVORABLE
FRACTURE LINE RUNS FROM THE
OUTER BUCCAL PLATE OBLIQUELY
BACKWARDS AND LINGUALLY , MEDIAL
MOVEMENT RESTRICTED
FRACTURE LINE RUNS FROM THE
INNER LINGUAL PLATE OBLIQUELY
BACKWARDS AND BUCCALLY , MEDIAL
MOVEMENT UNRESTRICTED
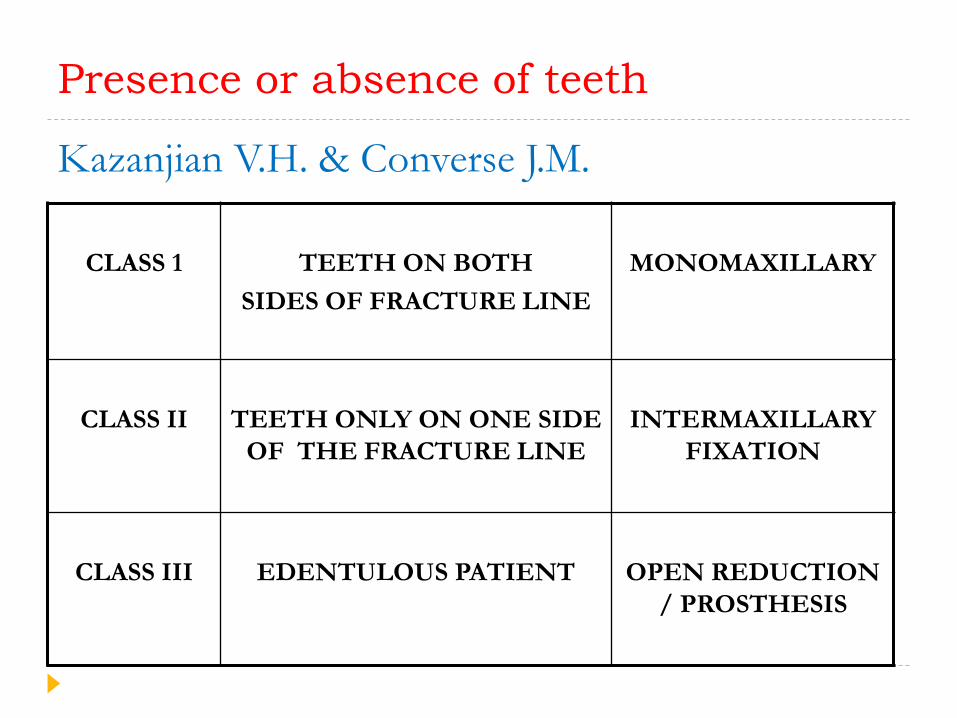
Presence or absence of teeth
Kazanjian V.H. & Converse J.M.
CLASS 1 TEETH ON BOTH
SIDES OF FRACTURE LINE
MONOMAXILLARY
CLASS II TEETH ONLY ON ONE SIDE
OF THE FRACTURE LINE
INTERMAXILLARY
FIXATION
CLASS III EDENTULOUS PATIENT OPEN REDUCTION
/ PROSTHESIS
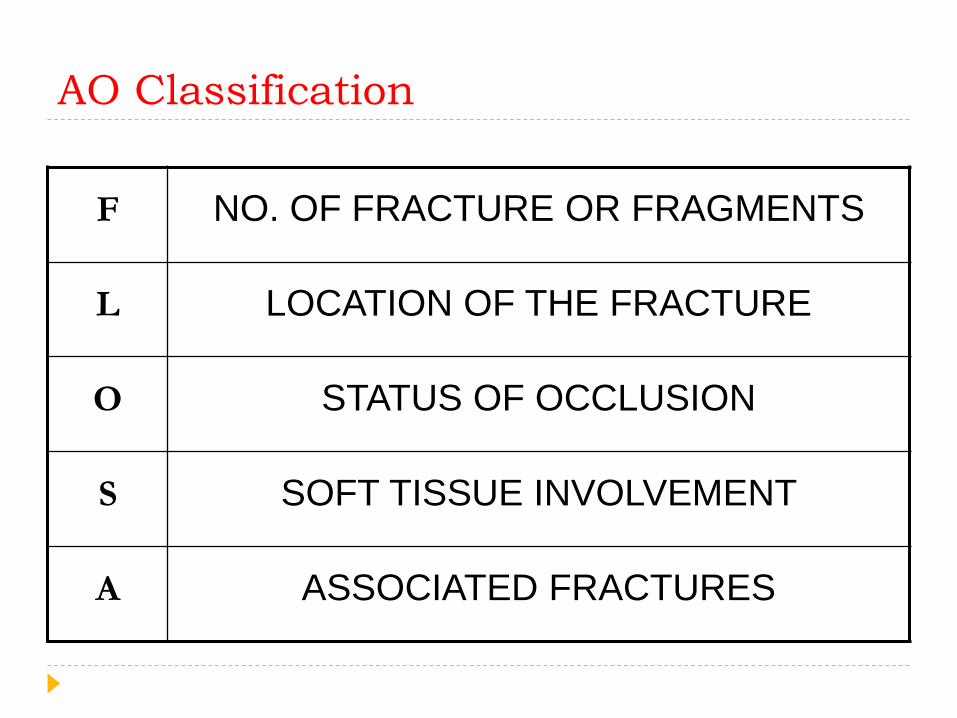
AO Classification
F NO. OF FRACTURE OR FRAGMENTS
L LOCATION OF THE FRACTURE
O STATUS OF OCCLUSION
S SOFT TISSUE INVOLVEMENT
A ASSOCIATED FRACTURES
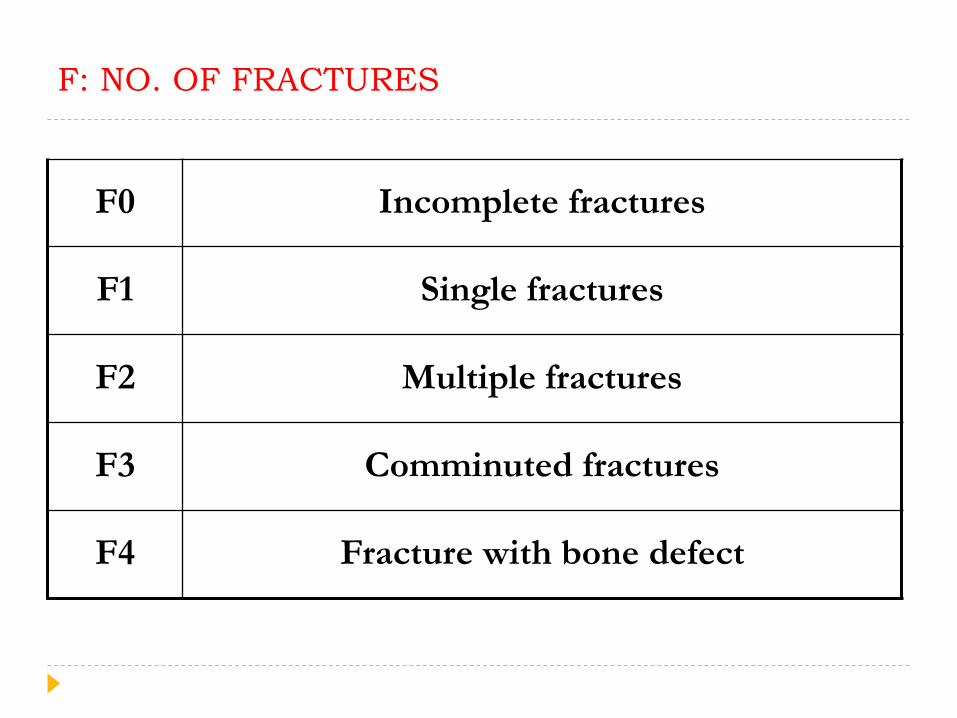
F: NO. OF FRACTURES
F0 Incomplete fractures
F1 Single fractures
F2 Multiple fractures
F3 Comminuted fractures
F4 Fracture with bone defect

L: Location of fracture
L1 Pre-canine
L2 Canine
L3 Post-canine
L4 Angle
L5 Supra-angular
L6 Condyle
L7 Coronoid
L8 Alveolar process

O: Status of occlusion
O 0 No malocclusion
O 1 Malocclusion
O 2 Edentulous mandible
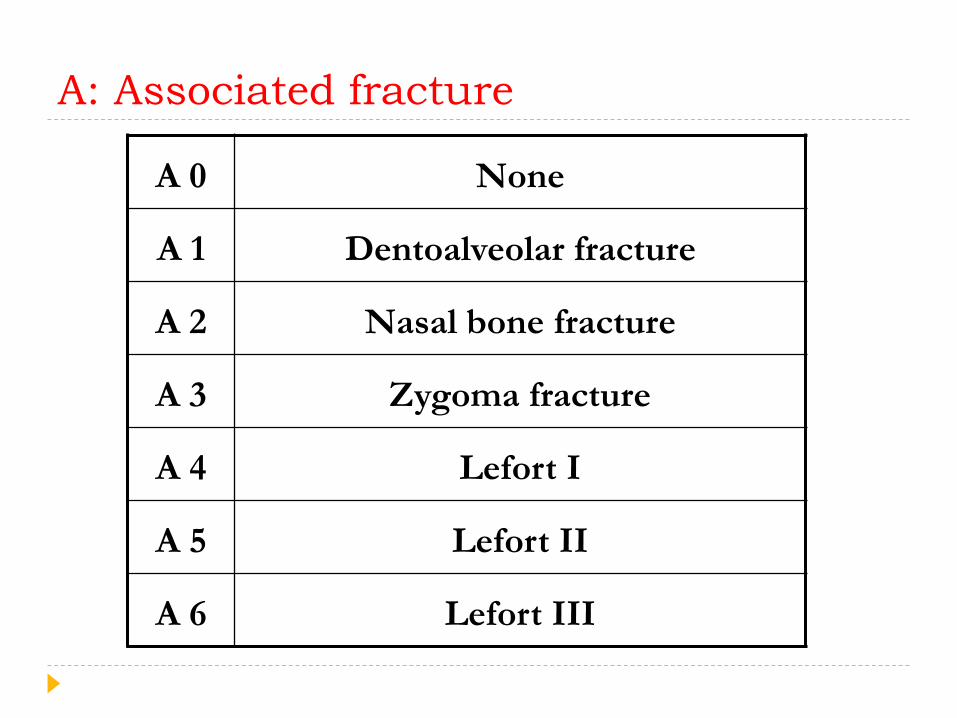
A: Associated fracture
A 0 None
A 1 Dentoalveolar fracture
A 2 Nasal bone fracture
A 3 Zygoma fracture
A 4 Lefort I
A 5 Lefort II
A 6 Lefort III
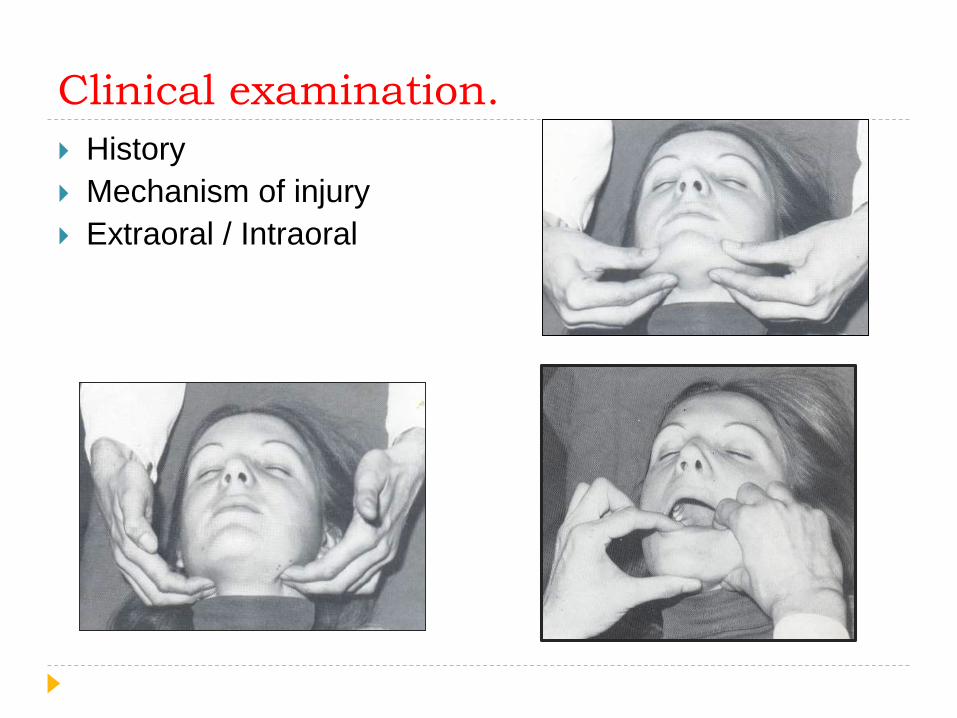
Clinical examination.
History
Mechanism of injury
Extraoral / Intraoral
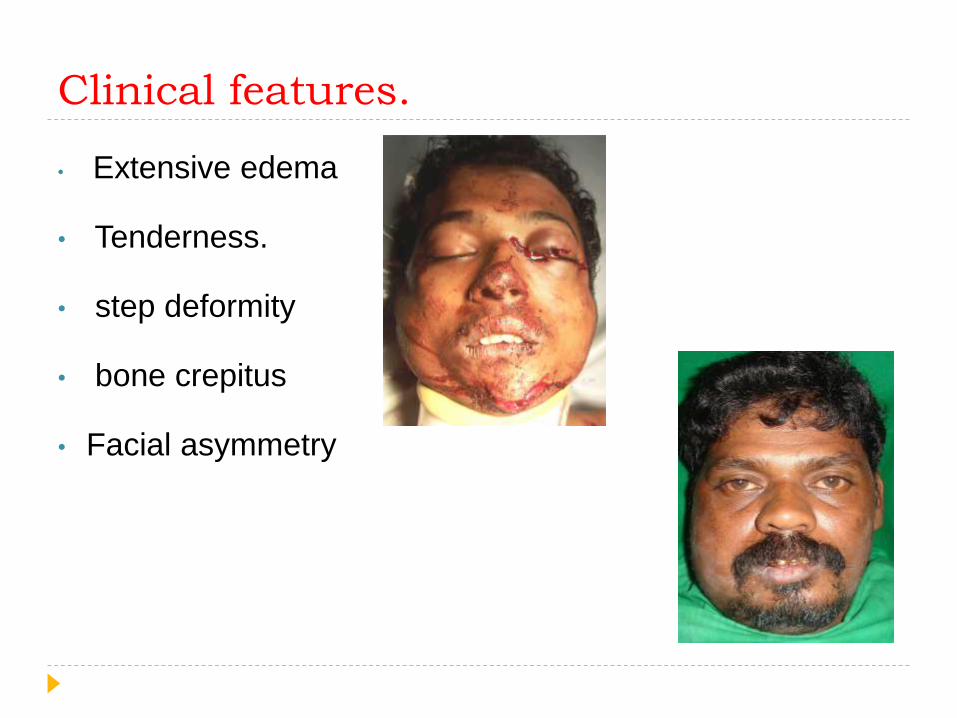
Clinical features.
• Extensive edema
• Tenderness.
• step deformity
• bone crepitus
• Facial asymmetry

Deviation of jaw Restriction of mouth
opening
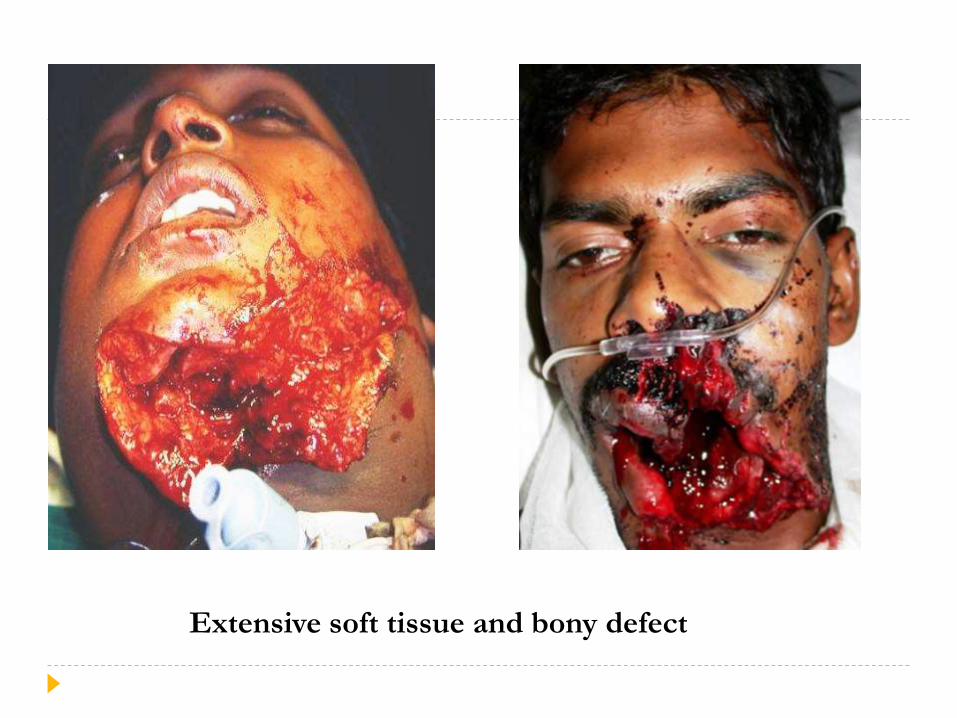
Extensive soft tissue and bony defect
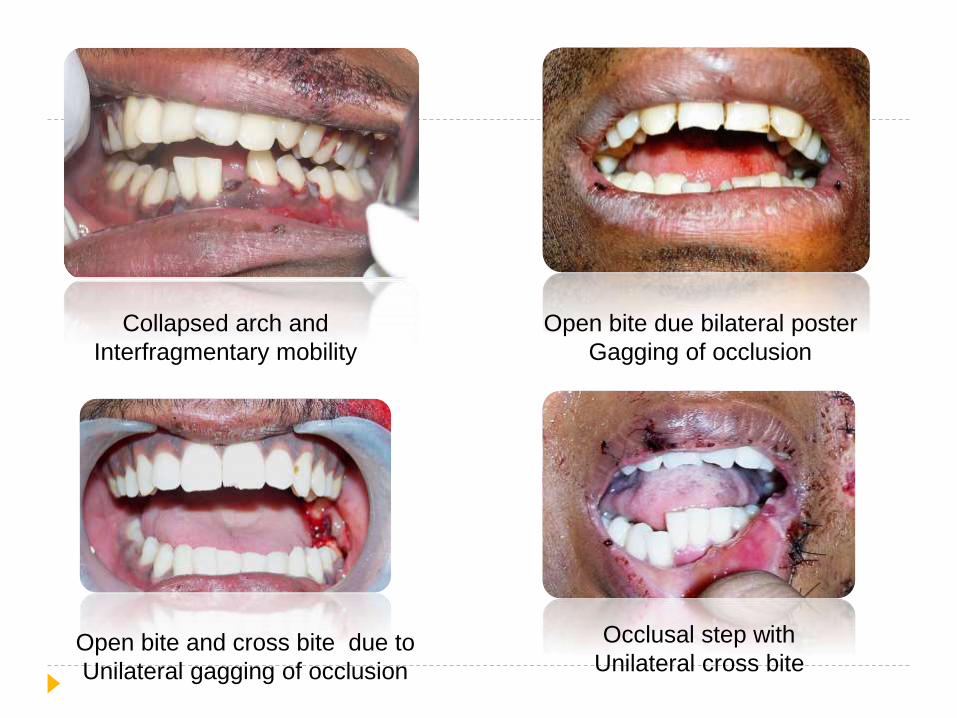
Collapsed arch and
Interfragmentary mobility
Open bite due bilateral poster
Gagging of occlusion
Open bite and cross bite due to
Unilateral gagging of occlusion
Occlusal step with
Unilateral cross bite

Mandibular fracture has to be differentiated from extensive
Soft tissue injury and dentoalveolar trauma
UNILATERAL CROSS BITE UNILATERAL OPEN BITE
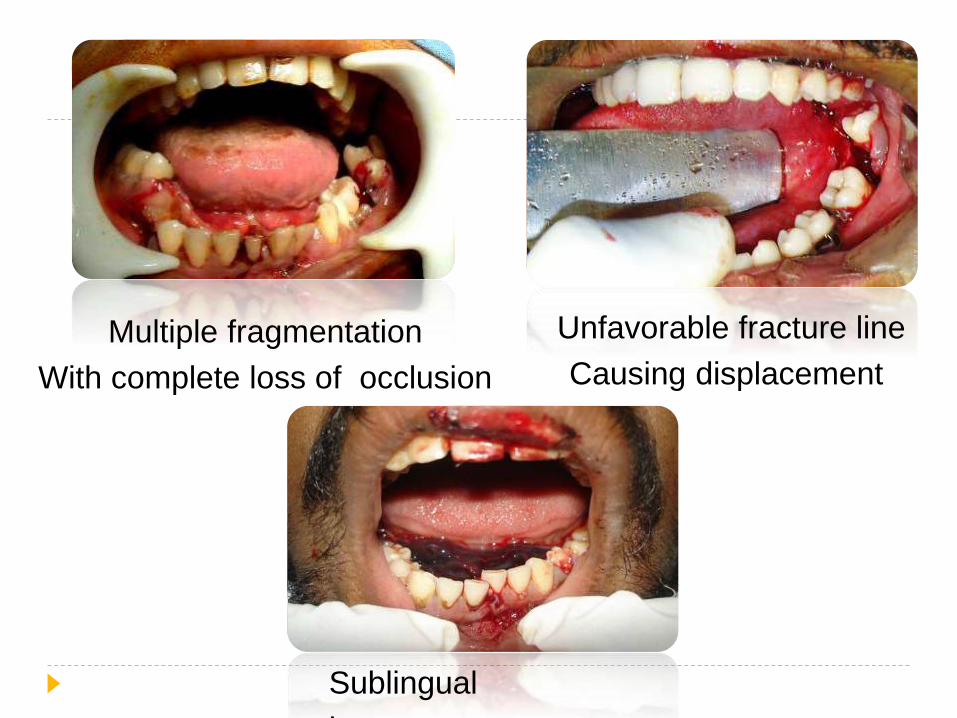
Multiple fragmentation
With complete loss of occlusion
Sublingual
hematoma
Unfavorable fracture line
Causing displacement
Displacement of fracture
Direction and intensity of the traumatic force.
Site of fracture.
Direction of fracture line.
Muscle pull exerted on fractured fragments.
Presence or absence of teeth.
Extent of soft tissue wound.
Radiographic features
OPG
PA View
PNS View
Lateral oblique Radiograph
Occlusal view
CT scan.
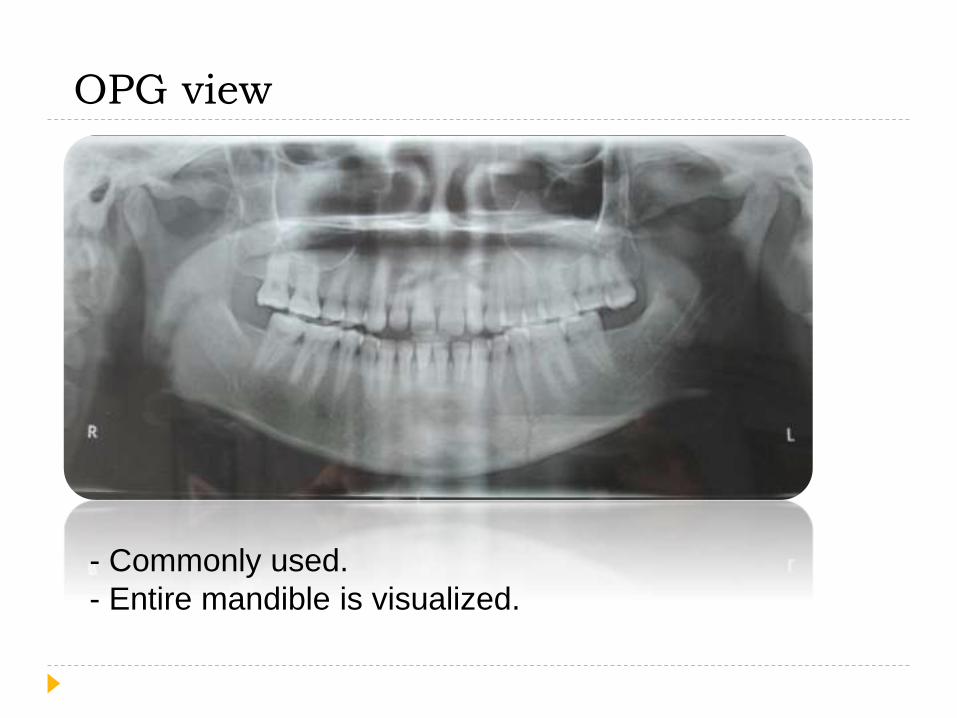
- Commonly used.
- Entire mandible is visualized.
OPG view
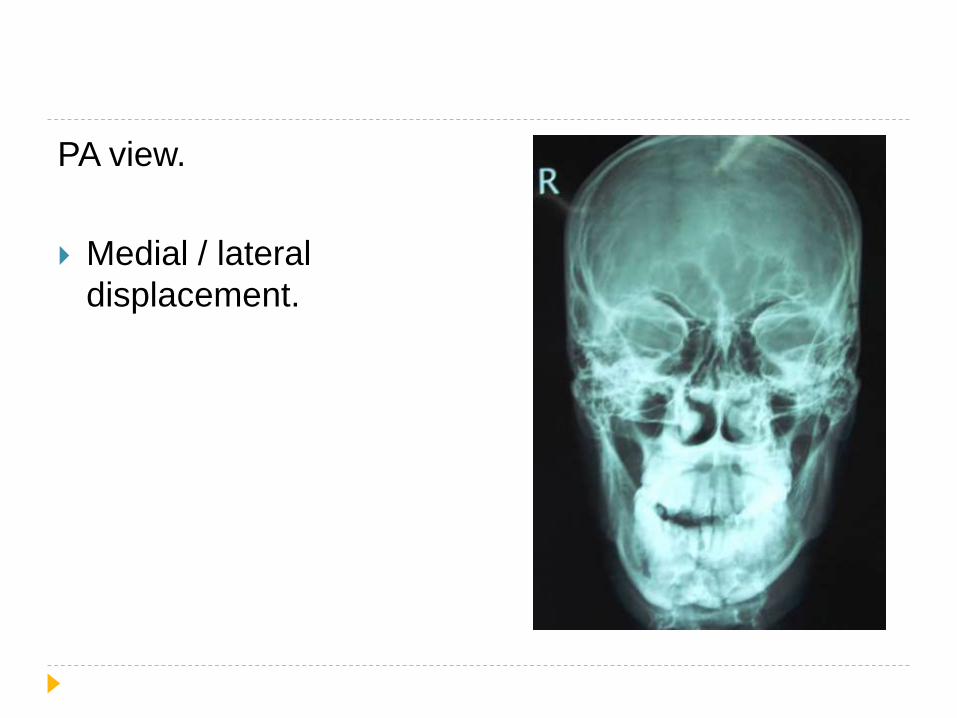
PA view.
Medial / lateral
displacement.
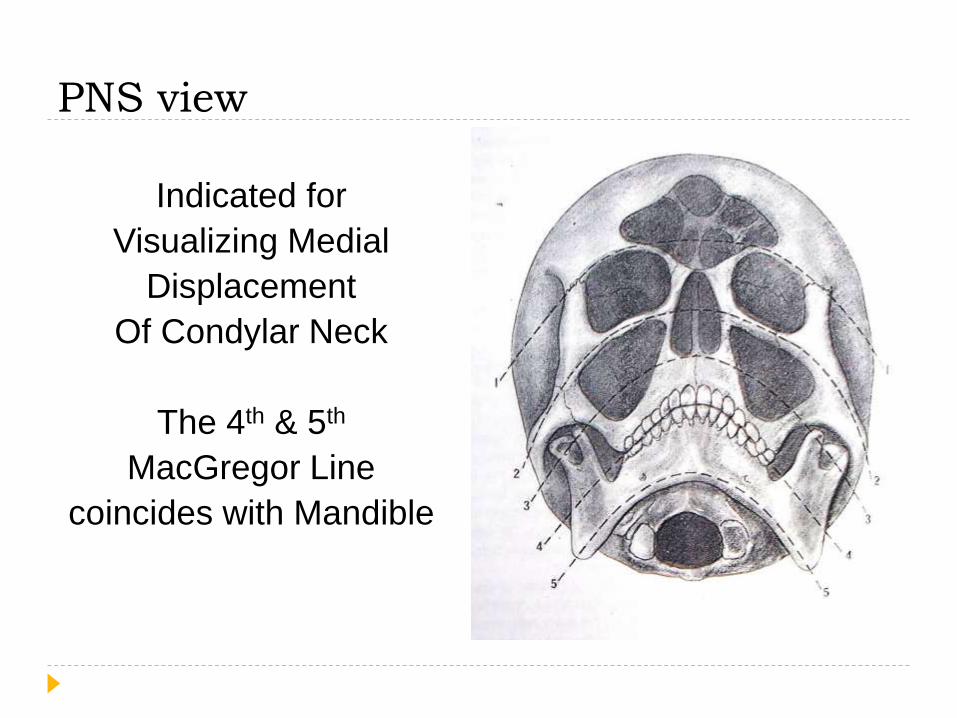
Indicated for
Visualizing Medial
Displacement
Of Condylar Neck
The 4th & 5th
MacGregor Line
coincides with Mandible
PNS view
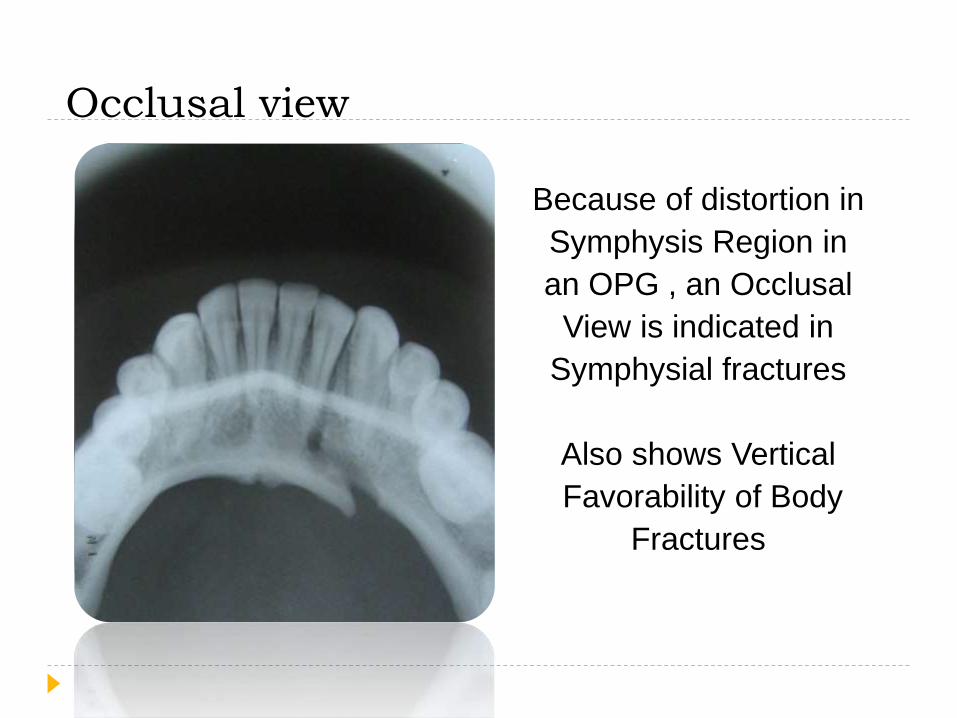
Because of distortion in
Symphysis Region in
an OPG , an Occlusal
View is indicated in
Symphysial fractures
Also shows Vertical
Favorability of Body
Fractures
Occlusal view
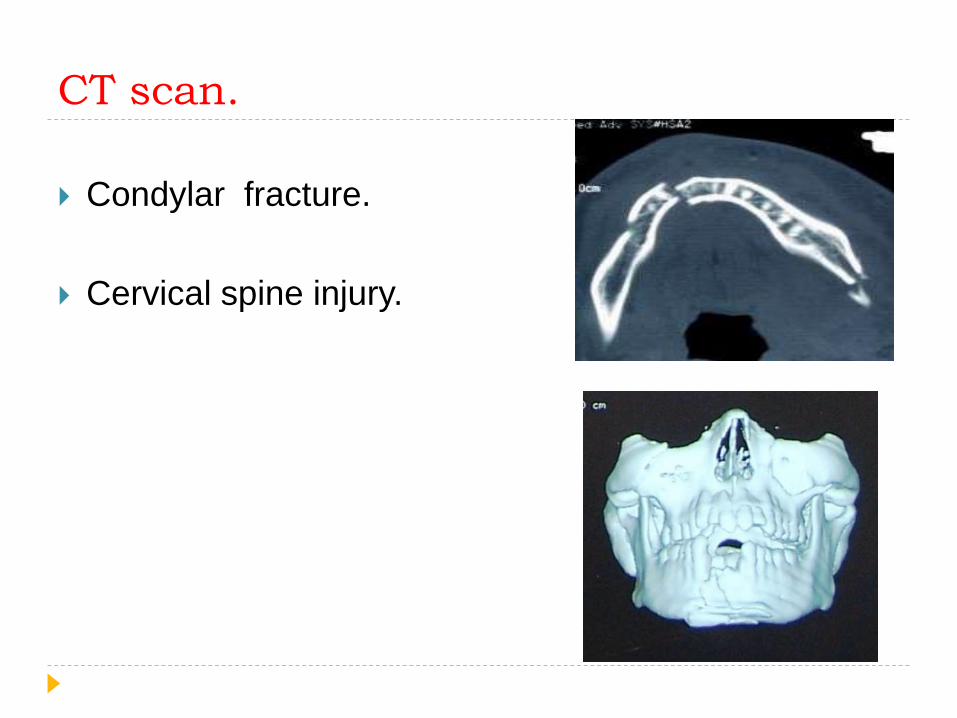
CT scan.
Condylar fracture.
Cervical spine injury.

Management of mandibular fractures.
To be continued…..
References.
Oral & maxillofacial trauma- Fonseca,vol 1
Maxillofacial Injuries- Rowe & Williams
Textbook of oral & maxillofacial surgery by Peter Ward
Booth.
Textbook of oral & maxillofacial surgery by Neelima
malik.
Killeys - fractures of the mandible







