
Diagnosis of Ectopic Pregnancy in the Emergency Department
Ralph Wang/Brian ChinnockUCSF/Fresno DEM
learning objectives
• understand the problem of EP
• become familiar with roles of US and bHCG
• learn how to perform bedside pelvic US
• integrating BPU into your practice
• recognize common pitfalls of BPU
key points
• r/o EP by identifying IUP (with caveat)
• IUP is defined by GS + YS surrounded by myometrium
• interrogate the uterus thoroughly
• bedside US is the test of choice in unstable patients
• TVS and TAS are complementary

who are we talking about?
• pregnant patients in the 1st trimester
• UPT + (with exceptions)
• VB +/or pelvic pain
• no prior US with IUP • does this patient have an ectopic pregnancy?
• 3-13% prevalence in ED studies
• EP was leading cause of 1st trimester mortality (10%)
• increased pre-rupture detection = declining mortalityBarnhart, K. T. Clinical practice. Ectopic pregnancy N Engl J Med 2009
advances in diagnostic modalities
• pelvic ultrasound
• ICT = high resolution (5-8Mhz)
• serum bHCG
basic strategy
• identify location of pregnancy
• identification of IUP = r/o EP
• rate of heterotopic = 1/30000 >1/5000*
• IVF rate = 1/100
ididentify location of pregnancy
ididentification of IUP = r/o EP
rarate of heterotopic = 1/30000 >1/5000*
IVIVF rate = 1/100

possible findings
• IUP (GS + YS) = discharge
• EP (-IUP, FF, adnexal mass) = ob/gyn
• indeterminate (-IUP) = correlate with bHCG
• abnormal IUP
• molar pregnancy
the intermediate result
• approx 10-20% of all pts
• location of pregnancy is unknown
• ddx = early IUP, miscarriage,
• approx 10-20% of all pts
• location of pregnancy is unknown
• ddx = early IUP, miscarriage, EP
narrowing the differential
• enter bHCG/DZ concept
• correlate bHCG to indeterminate result
• bHCG = gestational age
• DZ = level of bHCG at which operator is certain to see IUP (if IUP exists)
• enenteter r bHbHCGCG/D/DZ Z Z Z coconcncepepepeptt
• correlate bHCGCGCGCG t t t to indeterminate result
• bHbHCGCG = = g g gesestatatitiononononalal a agegege
• DZ = level of bHbHbHbHCG at which opopoperator is s certain to see IUP (i(i(i(if f f f IUIUIUIUP P P P exexisisisistststs))))
Gestational Age bHCG IUP visualized by US
3w 25-50
5w 1000-2000 gestational sac
5-6w >2000 GS+YS
6w >5000 GS+FP
7w >10000 cardiac activity
8w >100000
intermediate result
• bHCG<DZ: IUP, EP, embryonic demise
• bHCG>DZ: EP, embryonic demise
Kadar, N.Combined use of serum HCG and sonography in the diagnosis of ectopic pregnancy AJR American journal of roentgenology 1983
, IUP

USI
IUP - D/CEP - C/S OB
intermediate - correlate bHCG with DZI
low B - F/U 48hhi B - C/S OB
Moore, C. Ultrasound in pregnancy. Emerg Med Clin North Am. 2004
problems with protocol
• RUS unavailability
• increased ED LOS
• transport of unstable patients
• sending patients home with EP***
EPPU for EP
• US at the bedside performed by EP
• focused question: do I see an IUP ?
• components:
• transabdominal
• RUQ of FAST
• transvaginal
getting ready - 4P’s
• probe selection
• patient pee’s - bladder should be emptied for TVS
• position - pelvic exam
• probe cover - cover the ICT with condom

TASTAS
B
A
TAS
U V
TAS

TVS sagittal
TVS US
Ucul-de-sac
ES
full bladder

TVS coronal
interrogation - visualize the entire uterus

TVS - left adnexa TVS

recognizing IUP
• IUP =
• GS +YS or FP +
• surrounded by myometrium
gestational sac
pseudogestational sac
• EP may present with pseudo-GS (10%)
• NO DDSS, irregular border, may contain echogenic material
• yolk sac?
psuedogestational sac

GS + YS + surrounded IUP = GS + YS in uterus
location, location
• GS should be within uterus
• beware peripherally placed GS
• may represent interstitial EP
• 5mm rule
• importance of TAS
fetal pole
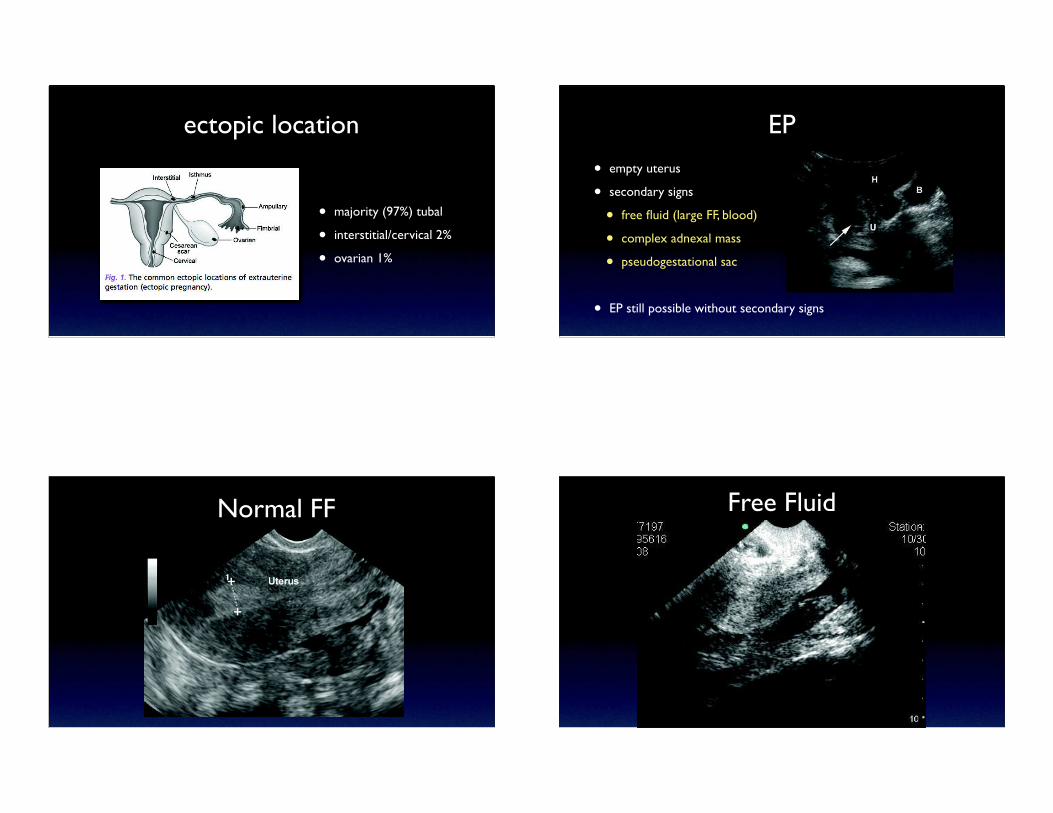
ectopic location
• majority (97%) tubal
• interstitial/cervical 2%
• ovarian 1%
EP
• empty uterus
• secondary signs
• free fluid (large FF, blood)
• complex adnexal mass
• pseudogestational sac
• EP still possible without secondary signs
Normal FF Free Fluid

TAS - ectopicTAS eecctoppicc ectopic pregnancy
ectopic Morison’s pouch
• FF in RUQ scan predicts need for OR for ruptured EP
• Moore, C. Free Fluid in Morison's Pouch on Bedside Ultrasound Predicts Need for Operative Intervention in Suspected Ectopic Pregnancy Academic Emergency Medicine 2007

abnormal
• large GS without YS, or FP
molar pregnancy
outcomes of EPPU
IUP70%
Demise~50%
IUP~30%
EP15%
Unknown3%
Indeterminant20%
Embrionic demise8%
EP2%
Molar preg<1%
N=1490pts w/ 1st trimester symptoms
Mateer, J. R. Outcome analysis of a protocol including bedside endovaginal sonography in patients at risk for ectopic pregnancy. Ann Emerg Med 1996
risk of ectopic according to subclass
• empty uterus = strongest predictor for EP
• normal GS (no yolk sac) = EP very unlikely

accuracy of EPPU
in 10 trials of EPPU TVS, 1 miss (heterotopic)excellent specificity = when we detect IUP > almost always correct
safe to discharge pts with IUP
McRae, A. Diagnostic accuracy and clinical utility of emergency department targeted ultrasonography in the evaluation of first-trimester pelvic pain and bleeding: a systematic review.
CJEM 2009
ED LOS
4 studies showing 1-2hr decreased LOS if EP identifies IUP
MICHAEL BLAIVAS, MD. Do Emergency Physicians Save Time When Locating a Live Intrauterine Pregnancy with Bedside Ultrasonography? ACADEMIC EMERGENCY MEDICINE 2000
perform EPPUI
IUP - D/CEP - C/S OB, RUS
indeterminate - RUSI
compare BHCG with DZ
Moore, C. Ultrasound in pregnancy. Emerg Med Clin North Am.2004
pitfalls - errors in thinking
• “lets wait for the bHCG before performing the US”
• “I’ve never sent home a pt with EP”

“lets wait for the bHCG”
•EP mean bHCG below DZ
•if only pt with bHCG>DZ scanned - miss 1/3-1/2 EPs
•discriminatory zone and bHCG only apply to IUP, not EP
•IUP and EP can be visualized below DZ
Kohn, M. A. Beta-human chorionic gonadotropin levels and the likelihood of ectopic pregnancy in emergency department patients with abdominal pain or vaginal bleeding. Academic emergency medicine. 2003
pitfalls
• heterotopic pregnancy
• cornual ectopic pregnancy
• pseudo-gestational sac
• state of the bladder
• TVS vs TAS - performing one without the other (see image)
summary
• EPPU for possible EP is a valuable screening tool
• In most instances, IUP rules out EP, dec LOS
• definition IUP = GS + YS surrounded by myometrium
• bedside US is test of choice in unstable pts
• TAS and TVS are complimentary studies

selected bibliography
1. Barnhart, K.T., Clinical practice. Ectopic pregnancy. N Engl J Med, 2009. 361(4): p. 379-87
2. Blaivas, M., et al., Do emergency physicians save time when locating a live intrauterine pregnancy with bedside ultrasonography? Academic emergency
medicine : official journal of the Society for Academic Emergency Medicine, 2000. 7(9): p. 988-93.
3. Mateer, J.R., et al., Outcome analysis of a protocol including bedside endovaginal sonography in patients at risk for ectopic pregnancy. Annals of emergency
medicine, 1996. 27(3): p. 283-9.
4. Moore, C. and S.B. Promes, Ultrasound in pregnancy. Emerg Med Clin North Am, 2004. 22(3): p. 697-722.
5. Moore, C., et al., Free Fluid in Morison's Pouch on Bedside Ultrasound Predicts Need for Operative Intervention in Suspected Ectopic Pregnancy. Academic
Emergency Medicine, 2007. 14(8): p. 755-758.
6. Tayal, V., Outcome of Patients with an Indeterminate Emergency Department First-trimester Pelvic Ultrasound to Rule Out Ectopic Pregnancy. Academic
Emergency Medicine, 2004. 11(9): p. 912-917.
7. Kohn, M.A., et al., Beta-human chorionic gonadotropin levels and the likelihood of ectopic pregnancy in emergency department patients with abdominal pain or
vaginal bleeding. Academic emergency medicine : official journal of the Society for Academic Emergency Medicine, 2003. 10(2): p. 119-26.
8. Adhikari, S., M. Blaivas, and M. Lyon, Diagnosis and management of ectopic pregnancy using bedside transvaginal ultrasonography in the ED: a 2-year
experience. The American journal of emergency medicine, 2007. 25(6): p. 591-6.
9. Shih, C.H., Effect of emergency physician-performed pelvic sonography on length of stay in the emergency department. Annals of emergency medicine, 1997.
29(3): p. 348-51; discussion 352.
10. McRae, A., H. Murray, and M. Edmonds, Diagnostic accuracy and clinical utility of emergency department targeted ultrasonography in the evaluation of first-
trimester pelvic pain and bleeding: a systematic review. CJEM : Canadian journal of emergency medical care = JCMU : journal canadien de soins médicaux
d'urgence, 2009. 11(4): p. 355-64.







