
C O N T E N T SKJOEDITORIAL
339 Waiting for ………………….. Robo 4: The Wonder Protein !!!
Dr. Meena Chakrabarti
MAJOR REVIEW
341 Current approach in diagnosis and management of scleritis
Dr. Zahadur Rahman, Dr. Jyothirmay Biswas
ORIGINAL ARTICLES
349 Natural history of Juxtafoveal Retinal Telangiectasia
Dr. Mahesh .G, Dr. A. Giridhar, Dr. Archis Shedbale,
Dr. Ram Kumar, Dr. Alpesh Rajput
355 Bevacizumab (Avastin) Therapy for macular oedema in
Central Retinal Vein Occlusion – Long term results
Dr. George J. Manayath
362 Ocular Ischemic Syndrome (OIS): A comparative analysis of
Management Options
Dr. Meena Chakrabarti, Dr. Valsa T.Stephen, Dr. Sonia Rani John
Dr. Arup Chakrabarti
367 Primary IVTA with secondary macular laser versus primary macular laser
with secondary IVTA in diabetic macular oedema with
subfoveal sensory detachment
Dr. Gopal S. Pillai, Dr. Niranjan
371 Long term results of surgical management of severe contusion injury
with dislocated lenses
Dr. Meena Chakrabarti, Dr. Valsa T. Stephen, Dr. Arup Chakrabarti,
Dr. Sonia Rani John
OCULAR PHARMACOLOGY
377 Intravitreal Bevacizumab
Dr. Sonia Rani John, Dr. Meena Chakrabarti, Dr. Valsa T. Stephen
Dr. Arup Chakrabarti
OPHTHALMIC INSTRUMENTATION
382 High end phaco systems: A comparison
Dr. Ashley Thomas
385 Spectacles- what we do not know
Dr. Bindu N. Das
OPHTHALMIC SURGERY
392 Management of dislocated PC IOL
Dr. Meena Chakrabarti, Dr. Valsa T. Stephen, Dr. Sonia Rani John
Dr. Arup Chakrabarti

C O N T E N T SKJO397 Pediatric cataract surgery
Dr. Rupal H. Trivedi, Dr. M. Edward Wilson
CURRENT CONCEPTS
408 Investigations in microbial keratitis
Dr. Jyothi P.T.
412 Parasitic keratitis
Dr. Ranjakumar
COMMUNITY OPHTHALMOLOGY
417 ‘’Less than perfect outcomes’’ after an uneventful cataract surgery
Dr. Meena Chakrabarti, Dr. Valsa T. Stephen, Dr. Sonia Rani John,
Dr. Arup Chakrabarti
CASE REPORT
419 Ocular contusion injury due to pelting with hard boiled eggs
Dr. Meena Chakrabarti, Dr. Valsa T. Stephen, Dr. Sonia Rani John,
Dr. Arup Chakrabarti
421 Lacrimal canaliculitis - A case report
Dr. Bindu N. Das, Dr. Sisira
423 Rips after pricks - A case series
Dr. Mahesh G., Dr. A. Giridhar, Dr. Siddarth Pawar, Dr. Ramkumar,
Dr. Alpesh Rajput
425 Combined cilioretinal artery occlusion and
Central Retinal Vein Occlusion - A case report
Dr. Valsa T. Stephen, Dr. Sonia Rani John, Dr. Meena Chakrabarti
Dr. Arup Chakrabarti
PHOTOESSAY
427 Leber’s Multiple Miliary Aneurysm
Dr. Valsa T. Stephen, Dr. Sonia Rani John, Dr. Meena Chakrabarti,
Dr. Arup Chakrabarti
430 CONSULTATION SECTION
434 OPTHALMIC HISTORY
437 JOURNAL REVIEW
440 BOOK REVIEW
445 UPCOMING CME
447 PG TEAR SHEET
451 INSTRUCTIONS TO AUTHORS

EDITORIAL
Waiting for ………Robo 4:
The Wonder Protein!!!
Recent research has shown that Robo 4 may unlock cures for blinding conditions such
as age related macular degeneration (AMD) and Proliferative Diabetic Retinopathy
(PDR). Robo 4, an endogenous protein also called Roundabout gene is a protein that
sits on the surface of cells in the blood vessels and essentially Robo 4 acts to stabilize
the blood vessels.
Blood vessel growth (Angiogenesis) is critical in human development and represents
the body’s natural response to injury or inflammation. Earlier research by Li et al have
conclusively shown that a family of proteins, netrins, induce blood vessel and nerve
growth in mice, a discovery that had great impact for development of potential therapies
to help people with too few blood vessels.
In response to injury or disease, new vessel growth occurs at the wrong place and at
the wrong time. These new vessels are usually very fragile with weak vessel walls
exhibiting a tendency to leak fluid into the surrounding tissues. Everything in biology
has a Yin (negative) to a yang (Positive). In the signaling pathway that induces new
vessels to grow, Robo 4 is the Yin to the yang of netrins. Cloned Robo 4 has been
shown to produce the opposite function of netrins by inhibiting angiogenesis and
stabilizing the walls of blood vessels preventing leakage. Robo 4 is found only in cells
in the interior surface of blood vessels and is activated by a protein called Slit. After
being activated, Robo 4 initiates a chain of biochemical events to stabilize blood vessel
and prevent uncontrolled growth.
Many diseases are caused by injury or inflammation destabilizing the blood vessels
and causing leakage of fluid into the adjacent areas. The Robo 4 pathway is a natural
pathway that acts like an endogenous brake stabilizing the blood vessels. When the
accelerators act (like VEGF) to induce migration, tube formation and permeability of
the capillaries – Robo 4 chips in as an armored brake inhibiting the action of VEGF.
The researchers from the University of Utah tested the power of Robo 4 in mice eyes
because they are very similar to human eyes. They successfully demonstrated that
Robo 4 activation curbed new vessel development.
It is the theorized that some type of of gene therapy involving Robo 4 could be
prescribed for humans at risk for either AMD or PDR – perhaps an injection or an eye
drop. Lengthy clinical studies are underway, and their results alone will prove whether

340 Kerala Journal of Ophthalmology Vol. XX, No. 4
Robo 4 is safe and efficacious for human use. Hence a waiting period of several years
is anticipated before Robo 4 is available for use in AMD and PDR patients. If the study
results prove what has been predicted we can look forward to the dawn of a future
filled with hope.
Dr. Meena Chakrabarti MS DO DNB
Editor

December 2008 Z Rahman et al. - Scleritis 341
M A J O RR E V I EW
Current Approach in Diagnosis and
Management of ScleritisDr. Zahedur Rahman MS, Dr. Jyotirmay Biswas MS
Introduction
Scleritis is a chronic, painful, and potentially blinding
inflammatory disease that is characterized by
edema and cellular infiltration of the scleral and
episcleral tissues. Because of the potentially devastating
ocular complications and possible association with
serious systemic disease, the diagnosis of scleritis
should not be missed. Scleritis most often presents
within 4th–6th decades with a mild preponderance
towards women over men (1.6:1) 1,2,3. Scleritis is
usually suspected from clinical history, and it is
confirmed by its characteristic clinical signs. In a case
of posterior scleritis, ultrasonography and other imaging
studies may be necessary to confirm the diagnosis.
Anatomic considerations
The function of the sclera is to provide a firm protective
coat for the intraocular contents. This coat is resilient
enough to allow for variations in the intraocular
pressure, firm enough to prevent severe distortion of
the contents of the eye on movement or when pressed
on by the muscles or external forces.
The bulbar conjunctiva is a thin transparent mucous
membrane, the epithelium of which is continuous with
the corneal epithelium. Beneath the epithelium lies
stroma which is a loosely arranged connective tissue.
Tenon’s capsule is a dense well defined membrane
which extends backwards from the limbus to ensheath
the extraocular recti muscles and becomes continuous
with the perimysium. It also passes backwards to cover
the globe. Posteriorly it becomes inserted into the dural
sheath of the optic nerve.
The episclera forms the superficial aspect of the sclera.
It is a thin dense, vascularised layer of connective tissue,
the fibers of which are continuous with the underlying
sclera. The episclera is immobile, when viewed with a
slit-lamp microscope. Lamina fusca is the innermost
layer of the sclera adjacent to the uvea.
In order to reliably differentiate episcleritis and scleritis,
an understanding of the anatomy of the vascular
plexuses contained within the conjunctiva, episclera,
and sclera is essential.. The blood supply to this region
is enormous, being derived from the anterior ciliary
arteries, but with extensive collateral arterial
anastomoses to the posterior ciliary arteries at the root
of the iris . The anterior system is readily visible with
the slit lamp and by anterior segment fluorescein
angiography, especially if the eye is inflammed, and its
recognition is of vital importance in the differentiation
of episcleral and scleral conditions. The separation and
displacement of these vascular layers give the most
important clinical clues to the site and the severity of
the inflammation. On slit lamp examination, three
layers of vessels are readily visible. The conjunctival
plexus, which is the most superficial layer of vessels,
can be moved over the underlying structures. The
superficial episcleral capillary plexus is a radially
arranged series of vessels lying within the parietal layer
of Tenon’s capsule. The vessels in this layer anastomoseUvea department, Sankara Nethralaya, 18, College road, Chennai-600 006.

342 Kerala Journal of Ophthalmology Vol. XX, No. 4
at the limbus with the conjunctival vessels, with other
members of the same plexus, and with the deep plexus.
The deep episcleral capillary network is closely applied
to the sclera in the visceral layer of Tenon’s capsule.
The conjunctival and superficial episcleral vessels can
be blanched with 1:1000 epinephrine or 10%
phenylephrine, but the deep vessels are affected slightly.
This is of considerable assistance when attempting to
differentiate deep and superficial scleral inflammation.
Classification
In 1976,Watson and Hayreh proposed a clinical
classification of scleritis based upon the anatomic
location of the inflammation and the observed
alterations in the associated vascular structures .This
categorization of disease entities does not infer etiology,
but provides valuable information regarding severity
of inflammation, prognosis, management options, and
association with systemic diseases and with ocular
complications. Few patients progress to a different form
of scleritis from their initial presentation.
Scleritis is defined as anterior or posterior based upon
the location of inflammation, relative to the equator of
the globe. The majority of scleritis is anterior and can
be categorized as non-necrotizing or necrotizing.
Diffuse and nodular scleritis are non- necrotizing and
represent the most common forms of anterior scleritis.
The necrotizing types of anterior scleritis are less
common ,but represent a more severe disease entity 1, 3.
Necrotizing scleritis is classified as either with
inflammation or without inflammation, with the latter
being synonymous with scleromalacia perforans.
Ultrasonographic classification categorizes posterior
scleritis as diffuse or nodular, based upon increased
eye wall thickness or finding of scleral nodule,
respectively.
Classification of scleritis
I. Anterior scleritis
a) Diffuse
b) Nodular
c) Necrotizing
i) With inflammation
ii) Without inflammation( scleromalacia perforans)
II. Posterior scleritis
a) Diffuse
b) Nodular
Scleritis may be classified etiologically, although it is
most often idiopathic or associated with a systemic
disease, scleritis can also be post surgical or related to
an infectious process. In one study, 25–57 % of scleritis
cases were associated with a known systemic
condition 1,2,3. In the Watson and Hayreh series,
connective tissue disorders were present in 15 % of
the patients, of which rheumatoid arthritis constituted
10 %. In another series with a higher proportion of
necrotizing scleritis cases, half of the patients had an
associated systemic connective tissue or vasculitic
disease 1. Necrotizing scleritis has the highest
association with systemic illness and represents the
most frequent type of scleritis that is the first
manifestation of a systemic condition 1,3. Approximately
two-thirds of patients with scleromalacia perforans have
an associated systemic condition 1, most commonly
longstanding rheumatoid arthritis (47 %) 3. Diffuse
scleritis appears to be the most benign form with the
lowest prevalence of associated systemic illness.
Systemic conditions associated with scleritis are shown
in table 1. Vasculitis is a proposed common factor in
the pathogenesis of both scleritis and the systemic
autoimmune disorders. Scleritis may occur following
ocular trauma . Surgically induced necrotizing scleritis
(SINS) can occur after any type of ocular surgery with
scleral manipulation, including cataract surgery,
strabismus surgery, filtering blebs, pterygium surgery,
and operations for retinal detachments. Many
organisms have been reported as possible causes of
scleritis and these are shown in table 2.
Table 1 Systemic diseases associated with scleritis
Rheumatoid arthritisWegener’s granulomatosisInflammatory bowel disease:Ulcerative colitis and Crohn’s diseaseRelapsing polychondritisSystemic lupus erythematosisPolyarteritis nodosaGiant cell arteritisBehçet’s diseasePolymyalgia rheumaticaReiter’s syndromeRaynaud’s diseaseIgA nephropathyAnkylosing spondylitis

December 2008 Z Rahman et al. - Scleritis 343
GoutSarcoidosisRosaceaPsoriasisLymphoma (Hodgkin’s)Pyoderma gangrenosumCogan’s syndromeNecrobiotic xanthogranuloma
Table-2 Infectious scleritis
BacterialPseudomonasProteus mirabilisStaphylococcus epidermidisStreptococcus pneumoniae
ViralHerpes zosterHerpes simplexMumps
GranulomatousMycobacterium tuberculosisMycobacterium chelonaeMycobacterium lepraeSyphilis
FungalAspergillusPseudallescheria boydiiSporotrichosis
ParasiticAcanthamoebaToxocariasisToxoplasmosisOnchocerciasis
Histopathology
Previous pathologic studies were based upon tissue
obtained from enucleated eyes with advanced
disease 4. Scleral biopsies have rarely been performed
because of the high rate of associated complications.
The pathologic findings of scleritis are classified as
(1) rheumatoid and rheumatoid- like necrotizing
scleritis, (2) idiopathic necrotizing scleritis, (3) post
infectious scleral inflammation, and (4) sarcoidal
inflammation 5,6 .
The typical feature of rheumatoid or rheumatoid-like
scleritis is central scleral necrosis with a distinct
surrounding zone of granulomatous inflammation 5,6,7.
Inflammatory cell infiltration with polymorphonuclear
leukocytes, histiocytes, and lymphocytes within the
episcleral tissue and suprachoroidal area, the presence
of an associated necrotizing vasculitis, and scleral fibre
necrosis between the pars plana and limbus are other
notable findings in rheumatoid scleritis.
In scleritis following a previous herpes zoster
ophthalmicus infection, histologic findings usually
include scleral necrosis, an associated vasculitis, and
surrounding zonal granulomatous inflammation,
primarily in the anterior sclera 5,6. The inflammation
can be non-granulomatous and focal. Although the
scleritis is suspected to be an immune-mediated
response to the prior infection, the presence of a reactive
proliferation of granulation tissue distinguishes this
form from the rheumatoid type. In infectious scleritis,
the presence of microabscesses with or without
histologic identification of a pathogen can be a
distinguishing factor.
Idiopathic necrotizing scleritis is characterized by
chronic, non-granulomatous inflammation and
diffuse lymphocytic infiltration of the anterior sclera,
episclera, and uvea 5,6 The presence of newly formed
vascular channels and focal granulation tissue with
fibroblasts, lymphocytes, and histiocytes in idiopathic
scleritis may be suggestive of a delayed type of
hypersensitivity 8.
Clinical Presentation of Scleritis
The clinical presentation of scleritis depends upon
the anatomic site involved and extent of inflammation.
The characteristic feature of scleritis is the severe
pain that may involve the eye and orbit and radiates
to involve the ear, scalp, face, and jaw. Scleritic pain
is typically dull and boring in nature, exacerbated
by eye movement. It is worse at night often interfering
with sleep, and characteristically wakens the
patient from sleep early in the morning. The pain is
usually severe in nature and resistant to mild
analgesic.
Scleritis typically has a gradual onset of redness with
increasing inflammation over several days 3. In contrast
to the brighter redness of episcleritis, scleritis is usually
a darker violaceous-red hue due to the depth of the
congested vascular plexus.
The patient with anterior scleritis usually notices
redness and tenderness of the globe. There may be
photophobia and lacrimation. Patient with posterior
scleritis may present with reduced vision with or
without pain. Patients may have features of an
underlying systemic disorder.
344 Kerala Journal of Ophthalmology Vol. XX, No. 4
Physical examination: ocular signs
The key clinical observations in patients with scleral
inflammation involve determining the relationship of
the vascular plexuses to each other and the site of
maximum vascular involvement best seen with red-free
light on slit- lamp biomicroscope. Deep discoloration,
extent of scleral edema, and areas of increased
transparency are best appreciated in natural day light 3.
A hallmark finding that distinguishes scleritis from
episcleritis is the presence of scleral edema. Edematous
sclera can bow forward, displacing the deep episcleral
vascular plexus and exacerbating deep vascular
congestion. To assess the degree of scleral involvement,
blanching the superficial conjunctival and episcleral
vasculature with topical 10 % phenylephrine can
improve visualization of the underlying tissue. Further
examination using a red-free filter is instrumental in
evaluating the vascular architecture, areas of
avascularity, and cellular infiltration of the episclera.
The anatomic location of the inflammation and typical
alterations in the vessels form the basis of the
classification of the vascular layers overlying the nodule
are displaced forward 3.
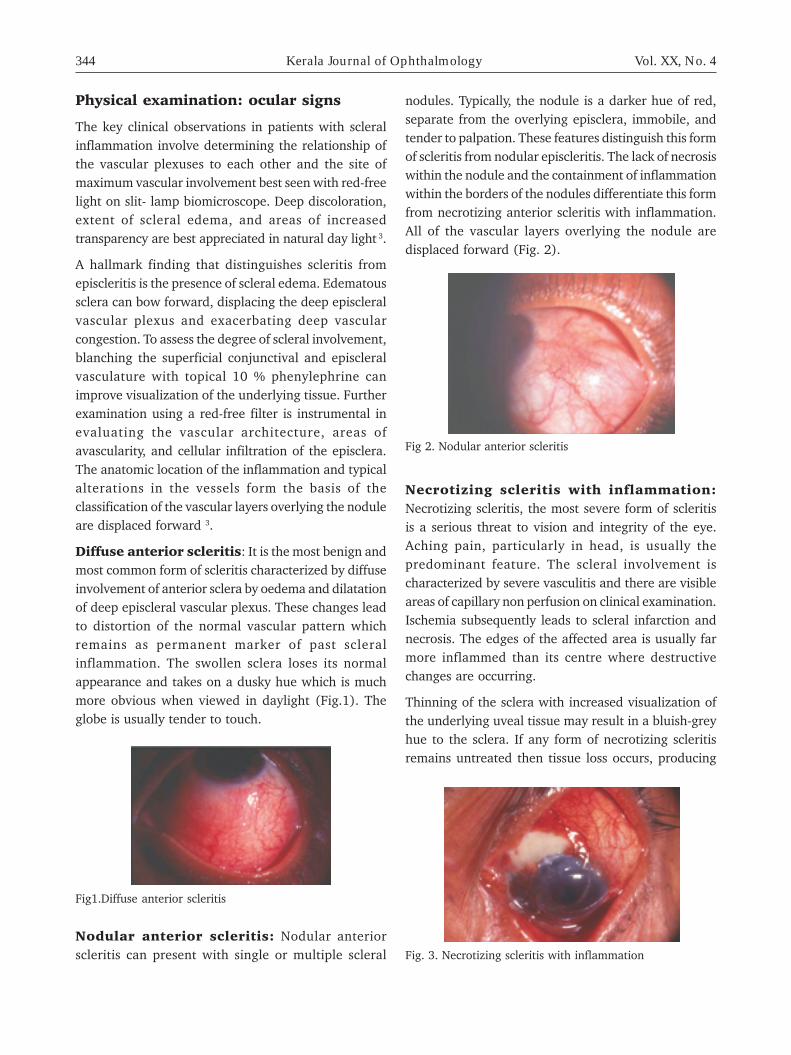
Diffuse anterior scleritis: It is the most benign and
most common form of scleritis characterized by diffuse
involvement of anterior sclera by oedema and dilatation
of deep episcleral vascular plexus. These changes lead
to distortion of the normal vascular pattern which
remains as permanent marker of past scleral
inflammation. The swollen sclera loses its normal
appearance and takes on a dusky hue which is much
more obvious when viewed in daylight (Fig.1). The
globe is usually tender to touch.
nodules. Typically, the nodule is a darker hue of red,
separate from the overlying episclera, immobile, and
tender to palpation. These features distinguish this form
of scleritis from nodular episcleritis. The lack of necrosis
within the nodule and the containment of inflammation
within the borders of the nodules differentiate this form
from necrotizing anterior scleritis with inflammation.
All of the vascular layers overlying the nodule are
displaced forward (Fig. 2).
Fig1.Diffuse anterior scleritis
Fig 2. Nodular anterior scleritis
Necrotizing scleritis with inflammation:
Necrotizing scleritis, the most severe form of scleritis
is a serious threat to vision and integrity of the eye.
Aching pain, particularly in head, is usually the
predominant feature. The scleral involvement is
characterized by severe vasculitis and there are visible
areas of capillary non perfusion on clinical examination.
Ischemia subsequently leads to scleral infarction and
necrosis. The edges of the affected area is usually far
more inflammed than its centre where destructive
changes are occurring.
Thinning of the sclera with increased visualization of
the underlying uveal tissue may result in a bluish-grey
hue to the sclera. If any form of necrotizing scleritis
remains untreated then tissue loss occurs, producing
Fig. 3. Necrotizing scleritis with inflammation
Nodular anterior scleritis: Nodular anterior
scleritis can present with single or multiple scleral

December 2008 Z Rahman et al. - Scleritis 345
overlying serous detachment of the neurosensory retina,
which represents the most common sign of posterior
scleritis 9, 10 . Ultrasound remains the key to diagnosis
with which the thickened posterior coat of the eye
(usually greater than 2 mm) can be identified (Fig. 5.)
Surgically induced necrotizing scleritis :
Surgically induced necrotizing scleritis (SINS) can occur
after any type of ocular surgery with scleral manipulation,
including cataract surgery, strabismus surgery, filtering
blebs, pterygium surgery, and operations for retinal
detachments 11,12,13,14. Inflammation is typically localized
to the site or adjacent to the site of surgery, but may
progress to involve the entire sclera 11,13 . Patients who
have SINS need careful systemic investigation as
62-90 % of patients in one study were later diagnosed
with autoimmune vasculitic disease which required
immunosuppessive therapy. 11,12,13
Investigations :
Because so many patients with scleral disease have
systemic disease, a thorough physical examination is
essential.
The following routine investigations should be
performed:
1. Hemoglobin
2. White blood cell count and differential count
3. Erythrocyte sedimentation rate
4. If connective tissue disease is suspected, full
immunologic investigations are undertaken, including
levels of immunoglobulins and immunofluorescent
studies for autoantibodies (including rheumatoid
factor and antinuclear and anti- ds- DNA antibodies);
circulating immune complexes are searched for.
If Wegener’s granulomatosis or polyarteritis nodosa
are suspected, the anti-nuclear cytoplasmic antibody
(ANCA) tests should be performed. The C-reactive
protein is the best indicator of an active generalized
inflammatory response.
5. Serum uric acid
6. Full serologic tests for syphilis
7. X-ray chest
B-scan ultrasonography should never be omitted from
the examination of patients with scleritis. Now that
high-quality ultrasonography has become available, the
milky white areas of necrotic sclera, episclera, and
conjunctiva. With time this dead tissue is absorbed,
leaving areas of dark choroid covered only by a thin
layer of atrophic conjunctiva (Fig. 3).
Scleromalacia perforans: Scleromalacia perforans
does not produce the acute signs of necrotizing scleritis,
may present with blurred vision from high astigmatism
due scleral thinning leading to loss of scleral rigidity.
The sclera may appear porcelain-like, as the vascularity
diminishes. Necrotic sclera can slough or become
sequestered. With severe scleral thinning, increased
visualization of the dark underlying uvea may occur.
Due to decreased scleral vascularity attributed to
arteriolar vaso-occlusion, large abnormal vessels
may cross and surround the areas of affected region
(Fig. 4).
Fig. 4. Scleromalacia Perforans
Posterior Scleritis: The presentation of posterior
scleritis depends upon the severity, extent, and location
of inflammation. The common signs of posterior scleritis
are posterior extension of anterior scleritis, a serous or
exudative retinal detachment, optic disc edema,
circumscribed subretinal mass, choroidal folds, retinal
striae, elevated intraocular pressure, and a bullous or
annular choroidal detachment 9. Extension of scleral
inflammation to the adjacent choroid can lead to an
Fig.5. Posterior scleritis

346 Kerala Journal of Ophthalmology Vol. XX, No. 4
extent and severity of the inflammation can be
determined with great accuracy. Many patients who
were formerly thought to have only anterior segment
disease have been found to have extensive and sight-
threatening posterior scleritis as well. It also has become
known that many patients with posterior scleritis with
few symptoms and signs have much more extensive
disease than had previously been considered possible.
The hallmark features of posterior scleritis seen with
B-scan ultrasonography are helpful in differentiating
posterior scleritis from other conditions. B-scan
ultrasonography may reveal the characteristic flattening
of the posterior aspect of the globe due to retrobulbar
edema 15. Abnormally increased thickening of the
posterior ocular coats of the globe >2 mm, optic disc
swelling, distension of the optic nerve sheath, retinal
detachments, and choroidal detachments can be
detected. Fluid can accumulate in the posterior
episcleral space and extend around the optic nerve,
forming the characteristic “T-sign”on B-scan 9,15,16.
Ultrasound biomicroscopy :This can be valuable
for better delineation of scleral thinning and ruling out
any malignancy. An underlying squamous cell
carcinoma, medulloepithelioma can extend to the
sclera.
Complications of Scleritis :
Decreased visual acuity, keratitis, cataract, uveitis, and
glaucoma are ocular associations indicating the spread
of scleral inflammation to adjacent tissues 1,2,3 .
Complications are more frequent in severe necrotizing
scleritis and posterior scleritis 1,2,3. Due to potential
ocular complications related to scleritis, early diagnosis
and treatment of scleritis and its associated ocular
manifestations are critical.
Vision may be limited due to keratitis, anterior uveitis,
cataract, change of refractive status, macular oedema,
optic disc oedema, or atrophy, retinal detachment,
epiretinal membrane formation, macular cyst or hole, or
raised intraocular pressure. Decreased vision occurs most
frequently with posterior scleritis (45-84 %), necrotizing
scleritis (74-82 %), nodular scleritis (26 %) and least
often with diffuse anterior scleritis (9 %) 1,2
A mild to moderate anterior uveitis has been observed
in 30–42 % of patients with scleritis, most frequently
(69 %) with necrotizing scleritis 3,17. Almost half of the
patients with posterior scleritis have an anterior uveitis.
Corneal changes are most frequently seen in patients
with necrotizing scleritis including peripheral corneal
thinning, stromal keratitis, and peripheral ulcerative
keratitis 18. Patients with scleritis and keratopathy have
more chance of being associated with systemic diseases.
During any stage of scleral inflammation, the
intraocular pressure may be elevated due to several
different mechanisms, such as obstruction of the
aqueous outflow channels, elevated episcleral pressure,
angle closure, or secondary to a steroid response.
Cataract formation may be accelerated by long-standing
inflammation or secondary to steroid use. Scleral
thinning most commonly occurs in necrotizing scleritis
and may progress to staphyloma in the presence of
raised intraocular pressure.
Medical management:
The aim of treatment is to treat the cause, to control
the inflammatory process and thereby reduce the
damage to the eye. Treatment almost always requires
systemic therapy. Patients with an associated disease
need specific treatment.
� Treatment of noninfectious scleritis:
Nonsteroidal anti-inflammatory drugs (NSAIDs),
corticosteroids, or immunomodulatory drugs are
indicated. Topical therapy is routinely insufficient.
This treatment must be individualized for the
severity of the scleritis, response to treatment,
adverse effects, and presence of the associated
disease.
Diffuse scleritis or nodular scleritis:
� The initial therapy consists of an NSAID (eg:
Indomethacin 75mg twice daily after meal). In case
of therapeutic failure, 2 different NSAIDs should be
tried in succession with the first drug. In high-risk
patients, consider appropriate gastrointestinal
protection with misoprostol or omeprazole.
� If NSAIDs are not effective or have untoward
complications, oral corticosteroids (tab:
Prednisolone) at doses of 1 mg/ kg body weight
can be substituted. Remission may be maintained
with continued NSAIDs.

December 2008 Z Rahman et al. - Scleritis 347
� Periorbital and subconjunctival steroid injections
(Inj.Triamcinolone acetonide 40 mg/ml) are
also effective in non-necrotizing anterior scleritis
(Fig. 6, Fig.7, Fig. 8). In case of therapeutic failure
of corticosteroids, immunosuppressive drugs
should be added or substituted. Methotrexate (initial
dose-15 mg/week and tapered monthly) can be the
first choice, but azathioprine, cyclophosphamide,
or cyclosporine may be helpful. Tumor necrosis
factor alpha (Tumour necrosis factor (TNF)-alpha)
inhibitor infliximab, may be effective, although
further investigation is warranted.
Necrotizing scleritis :
� Cyclophosphamide(100 mg per day orally and
tapered monthly) should be the first choice in
treating patients with associated potentially lethal
vasculitic diseases, such as Wegener’s granulomatosis
or polyarteritis nodosa.
� The initial therapy consists of immunosuppressive
drugs that are supplemented with corticosteroids
during the first month; the latter is tapered slowly,
if possible. Cyclophosphamide is the most effective
drug.
� In case of therapeutic failure, another
immunomodulatory drug, such as infliximab, may
be effective. Other alternatives are daclizumab and
rituximab, although their efficacy awaits further
study.
� Periocular steroid injections should be applied with
great caution in cases of necrotizing scleritis or
peripheral ulcerative keratitis. Some authors believe
that depot steroids actually may exacerbate
necrotizing disease or an underlying infection.
� Pulse intravenous cyclophosphamide with or
without pulse intravenous corticosteroids may be
required in case of emergencies and may be followed
by maintenance therapy.
Treatment of infectious scleritis: Systemic
treatment with or without topical antimicrobial therapy
always is required. Differentiating infectious scleritis
from non-infectious scleritis is important because
corticosteroid therapy and immunosuppressive therapy
(often used in noninfectious autoimmune scleritis) are
contraindicated in active infections.
Surgical care:
Tectonic surgical procedures rarely may be required to
preserve the integrity of the globe.
� Scleral grafts are fresh sclera or glycerin-preserved
sclera that is available through eye banks. Grafts
may be performed in cases of pending perforation
during the time before the effects of systemic
immunosuppressive agents manifest (Fig.9).
� Corneal tissue may be used for associated corneal
disease.
Fig. 6. Sub-conjuntival triamcinolone acetonide injection ina case of anterior scleritis
Fig. 7. Diffuse anterior scleritis before giving subtenoninjection of triamcinolone acetonide.
Fig. 8. Resolution of diffuse anterior scleritis two days aftergiving sub-conjunctival injection triamcinoloneacetonide.

348 Kerala Journal of Ophthalmology Vol. XX, No. 4
2. Tuft SJ, Watson PG. Progression of scleral disease.Ophthalmology. 1991 ;98:467-71
3. Watson PG, Hayreh SS. Scleritis and episcleritis. Br JOphthalmol 1976;60:163-91
4. Fraunfelder FT, Watson PG.Evaluation of eyesenucleated for scleritis. Br J Ophthalmol. 1976;60:227–230
5. Rao NA, Marak GE, Hidayat AA.Necrotizing scleritis: aclinico-pathologic study of 41 cases. Ophthalmology.1985; 92: 1542–1549
6. Riono WP,Hidayat AA, Rao NA. Scleritis: aclinicopathologic study of 55 cases. Ophthalmology.1999;106:1328–1333
7. Fong LP, Sainz de la Maza M, Rice BA, Kupferman AE,Foster CS. Immunopathology of scleritis. Ophthalmology.1991;98:472–479
8. Rao NA, Phillips TM,Wong VG, et al. (1985) Etiologyof scleritis. In: O’Connor GR, Chandler JW (eds)Advances in immunology and immunopathology of theeye. Masson, New York, pp 54–57
9. McClusky PJ, Watson PG, Lightman S. Posterior scleritis:clinical features, systemic associations, and outcomein a large series of patients. Ophthalmology. 1999; 106:2380–2386
10. Watson PG. The diagnosis and management of scleritis.Ophthalmology. 1980;87:716–720
11. Karia N, Doran J, Watson SL, et al. Surgically inducednecrotizing scleritis in a patient with ankylosingspondylitis. J Cataract Refract Surg.1999;25:597–600
12. O’Donoghue E, Lightman S, Tuft S, et al. Surgicallyinduced necrotizing sclerokeratitis (SINS) –precipitating factors and response to treatment. Br JOphthalmol.1992;76:17–21
13. Sainz de la Maza M, Foster CS. Necrotizing scleritisafter ocular surgery: a clinicopathologic study.Ophthalmology. 1991;98:1720–1726
14. Salamon SM, Mondino BJ, Zaidman GW. Peripheralcorneal ulcers, conjunctival ulcers, and scleritis aftercataract surgery. Am J Ophthalmol. 1982;93:334–33
15. Benson WE. Posterior scleritis. Surv Ophthalmol. 1988;32: 297–316
16. Biswas J, Mittal S, Ganesh SK, Shetty NS, Gopal L:Posterior scleritis: Clinical profile and imagingcharacteristics. Ind J ophthal 1998;46: 195-202
17. Sainz de la Maza M, Foster CS, Jabbur NS. Scleritis-associated uveitis. Ophthalmology.1997;104: 58–63
Sainz de la Maza M, Foster CS, Jabbur NS, Baltatzis S.Ocular characteristics and disease associations inscleritis-associated peripheral keratopathy. ArchOphthalmol. 2002 ;120:15-9.
Fig.9. Scleral patch graft
Consultations
� Rheumatology or internal medicine consultation for
associated disease
� Hematology, oncology, or internal medicine
consultation for immunosuppressive therapy
Conclusions
Scleritis is highly associated with potentially sight
threatening ocular complications and serious systemic
diseases. Early diagnosis and treatment of scleritis is
important in preventing and diminishing ocular and
systemic morbidity. Hence, attempts should be made
to achieve excellent long-term prognosis with careful
clinical history, detailed ocular examination, and use
of immunosuppressant drugs whenever necessary.
References
1. Sainz del la Maza M, Jabbur NS, Foster CS. Severity ofscleritis and episcleritis. Ophthalmology. 1994 ;101:389-96.

December 2008 Mahesh G. et al. - Juxtafoveal Retinal Telangiectasia 349
Natural History of Juxtafoveal Retinal
TelangiectasiaDr. Mahesh G FRCS Ed, Dr. A. Giridhar MS, Dr. Archis Shedbale MS, Dr. Ram Kumar DO, Dr. Alpesh Rajput DO
Idiopathic juxtafoveal retinal telangiectasia (IJRT) has
been considered a separate clinical entity since it was
first described by Gass in 1968 1. In 1993, Gass and
Blodi 2 examined 140 such cases seen at Bascom Palmer
Eye Institute, Miami over a 28-year period and
established a classification of these entities with
subgroups and stages. In recent years, newly recognized
manifestations have expanded and refined the clinical
spectrum of these macular vasculopathies. Furthermore,
the use of high-speed angiography and optical
coherence tomography (OCT) have provided a better
understanding of the nature of the vascular
abnormalities and their secondary effects in the macula,
to some degree paralleling histopathological
observations described in the ophthalmic literature 3-9.
There are few reports on the long term natural history
of IJRT 2,10,11.
We describe a retrospective series of 35 eyes of
20 patients with IJRT with special emphasis on visual
acuity.
Methods
We analyzed the case records of 35 eyes of 20 patients
diagnosed with IJRT between January 1, 1998 and
December 31, 2004. The standard for recruitment was
unilateral or bilateral presence of abnormal juxtafoveal
vessels documented by fundus fluorescein angiography
(FFA). At the follow-up visits, patients were questioned
about visual symptoms. Each patient underwent
complete ophthalmologic examination, including
biomicroscopy and indirect ophthalmoscopy. Colour
fundus photographs were taken during follow up visits.
Vision was assessed by using the standard eight steps
Snellen test charts; measurements were made on the
first and follow-up visits and recorded in the clinical
records. Comparative visual change between visits was
reported as lines of loss or gain. We assessed the clinical
photographic and fundus fluorescein angiography (FFA)
characteristics of eyes with type II A disease at first
visit and during follow-up using the stages of
development of parafoveal telangiectasis as described
by Gass and Blodi 3 : stage 1 is characterized by no
biomicroscopic abnormality, but staining and leakage
at the level of retinal pigment epithelium (RPE); Stage
2, by slight retinal graying and capillary telangiectasis
visible only by FFA; stage 3 by parafoveolar dilated and
right angled venules; stage 4 by RPE hyperplasia within
the retina; stage 5 by subretinal neovascularisation.
Results
There were 8(40 %) male and 12 female (60 %)
patients. Age in years ranged from 41 to 72 (Mean
49.65).Ten patients (50 %) were diabetic and
8(40 %) were hypertensive. Of the 20 study patients,
5 had Gass type IA disease and 15 had Gass type IIB
disease. Follow-up period varied from 4 months to 102
months (mean 35.6 months). Best corrected visual
acuity (BCVA) remained same in 16 eyes(45.71 %),
deteriorated by 1 or more lines in 11 eyes( 31.42 % ),
deteriorated by 3 or more lines in 3 eyes (8.57 %),
improved by 2 lines in 4 eyes (11.42 %), improved byGiridhar Eye Institute, Ponneth Temple Road, Kadavanthra, Cochin-682020,
Kerala. E-mail:[email protected]
ORIGINAL
A R T I C L E

350 Kerala Journal of Ophthalmology Vol. XX, No. 4
1 line in 1 eye.(2.85 %). The cause for deterioration
included progression of IJRT in 9(64.28 %) eyes
,progression of cataract in 4 (28.57 %) eyes, branch
retinal vein occlusion (BRVO) in 1 (7.14 %)eye. Two
eyes showed improvement in BCVA as a result of
cataract surgery, 1 eye because of resolution of macular
edema, 2 eyes as a result of regression of corneal
disease. None of the eyes had diabetic retinopathy in
the beginning, but 6 eyes (15 %) developed changes of
mild NPDR and 4 eyes (10 %) moderate NPDR during
follow-up. None of these eyes had features of diabetic
macular edema/maculopathy
Type I B: Unilateral idiopathic, focal juxtafoveolar
telangiectasis
There were 5 patients (3 males and 2 females) who
had type I B disease. Mean age was 51.4 years. All these
patients had unilateral focal area of capillary
telangiectasis in the parafoveal area as evidenced by
fluorescein angiography. Of these 5 eyes, best corrected
visual acuity (BCVA) dropped by 1 line in 1 eye (20 %)
due to progression of IJRT, remained stable in 3 eyes
(60 %) one of which had poor vision due to BRVO,
which was confirmed by FFA (Patient 2; Table 1).BCVA
improved by 2 lines in 1 eye (20 %) as a result of
resolution of macular edema in eye(20 %) over a period
of 72 months follow-up (Patient 1; Table1)
Type IIA: Bilateral idiopathic acquired juxtafoveolar
telangiectasis
Thirty eyes of 15 patients were classified as having type
IIA disease. There were 5 male (33.33 %) and 10 female
patients (66.66 %) BCVA remained stable in 13 eyes
(43.33 %). BCVA dropped by 1 line in 7 eyes. (23.33%)
(all due to progression of IJRT).deteriorated by 2 lines
in 3 eyes (10%) (all due to progression of cataract),
deteriorated by 5 lines in 2 eyes (6.66%) (one due to
development of SRNVM and other due to BRVO).One
eye (3.33%) showed deterioration by 10 lines due to
progression of cataract to maturity. Three eyes (10%)
showed improvement in BCVA by 2 lines (2 eyes as a
result of cataract surgery and 1 eye because of
regression of corneal oedema).BCVA improved by 1 line
in 1 eye (3.33%) due to regression of corneal problem.
Case 10 (Patient10, Table 1) exemplifies progression
of disease to subretinal neovascularisation. This patient
was a 43 years old woman who noted gradual loss of
central vision first in the right eye and then in the left
eye for 6 months. She was neither diabetic nor
hypertensive. She was examined in December 2000 and
BCVA was 6/36 in right eye and 6/12 in left eye.
Parafoveal whitening, RPE proliferation and
pigmentation temporal to fovea was seen in right eye.
Fluorescein angiography of right eye showed leakage
of dye. (Stage 4 disease) Left eye showed retinal graying
and dilated and blunted retinal venules. FFA confirmed
this and showed leakage. (Stage 3 disease) In September
2001, her vision was stable at 6/36 in right eye and
6/12 in the left eye. There was increased pigmentation
and proliferation in the right eye. FFA showed about
same amount of intraretinal leakage in both eyes. She
was not seen again until March 2007. Her BCVA had
dropped to 2/60 in right eye and was stable at 6/12 in
left eye. Fundus photograph of right eye (Fig. 1a)
showed a scarred CNVM (Stage 5 disease) which was
confirmed by FFA (Fig 1c). Left eye fundus photograph
(Fig 1b) showed no significant change and FFA
Fig. 1e. OCT showing scarredmembrane in righteye
Fig. 1f. OCT showingpseudocyst in left
eye
Fig. 1c. FFA of right eyeshowing a scarred
CNVM
Fig. 1d. FFA showingincreased intra-retinalleakage in the left eye
Fig. 1a. Fundus photograph ofright eye showing ascarred CNVM
Fig. 1b. Normal left eyefundus photograph

December 2008 Mahesh G. et al. - Juxtafoveal Retinal Telangiectasia 351
(Fig. 1d) showed increased intra-retinal leakage
(stage 3 disease). OCT examination (horizontal line
scan) at this visit showed a scarred membrane in right
eye (Fig 1e) and pseudocyst in left eye (Fig 1f).
Case 15 (Patient15, Table 1) is an example
highlighting the slow rate of progression of the disease.
This 52 years old man complained of defective vision
in both the eyes of 6 years duration. He was a known
diabetic. On examination in December 2003, he was
missing letters of the Snellen‘s chart in both eyes and
his BCVA was 6/ 12 in right eye and 6/18 in left eye.
Anterior segment examination revealed immature
senile cataract in both eyes. Colour fundus photograph
of both eyes (Fig. 2a, 2b) showed parafoveal retinal
graying and crystals and left eye in addition showed
RPE hyperplasia and pigmentation. FFA of both eyes
(fig. 2c, 2d) showed telangiectatic capillaries and late
intra-retinal leakage of dye in both eyes. He was
followed up and in July 2005, his BCVA was stable at
6/12 in right eye and 6/18 in left eye. Anterior segment
examination was almost unchanged .Colour fundus
photo of right eye showed parafoveal retinal graying
and crystals. Left eye colour fundus photograph was
significant for the increase in the pigmentation. In June
2007 he presented with drop in visual acuity, BCVA
being 6/24 in right eye and 6/36 in left eye. Anterior
segment examination revealed significant progression
of cataract in both eyes. On colour fundus photography
(Fig 2e, 2f), both eyes were status quo. FFA was
significant only for the increase in the intra-retinal
leakage of dye (Fig 2g, 2h).There was no evidence of
subretinal neovascularisation in either eye. The
deterioration of visual acuity was mainly due to
progression of cataract.
Case 20 (Patient 20, Table 1) is another example which
highlights the very slow progressive nature of the
disease. This patient was 44 years old woman who had
Fig. 2 (a. & b.) showing parafoveal retinal graying andcrystals in both eyes and RPE hyperplasia andpigmentation in the left eye
Fig. 2. (c & d) FFA of both eyes showing telangiectaticcapillaries and late intra-retinal leakage of dye in botheyes
Fig. 2 (e & f) status quo colour fundus photograph of both
eyes on review
Fig. 2 (g & h) increase in the intra-retinal leakage of dye inboth eyes
Fig. 3 (a & b) showing parafoveal graying with crystals in
both the eyes
(c) (d)
(a) (b)
(e) (f)
(g) (h)
Fig. 3c. FFA showing lateleakage of dye in theright eye
Fig. 3d. FFA showing minimal
leakage of dye in theleft eye
(a) (b)
(c) (d)

352 Kerala Journal of Ophthalmology Vol. XX, No. 4
noted gradual loss of vision first in right eye and then
in left eye since 6 months. She was examined in
September 2004. BCVA was 6/18 in right eye and 6/6
in left eye. There was parafoveal graying along with
crystals in both the eyes. (Fig 3a and Fig 3b). On FFA,
there was late leakage of dye in right eye (Fig. 3c) and
minimal leakage in left eye (Fig. 3d). She was followed
up and during her last visit in March 2007; BCVA was
stable in both eyes, 6/18 in right eye and 6/6 in left
Table 1. Long-Term Follow-up of Patients With Juxtafoveal Retinal Telangiectasia
Patient Age Sex Eye(s) Vision at Fundus Gass Duration Vision at Fundus Change Miscellainvolved first visit findings type of follow-up follow-up findings in visual neous
(months) acuity (cause forchange in Vn)
1 50 M RE 18-Jun MA, ME I B 72 9-Jun MA 2 Resolution ofME
2 49 M LE Jun-60 MA, ME,HE I B 12 Jun-60 MA 0 BRVO3 49 F LE 18-Jun HE, Hm.,TV I B 24 24-Jun Hem.,TV -1 Progression
of IJRT4 52 M RE Jan-60 Pigm.,HE II A 4 Jan-60 Pigm,HE 0
LE 6-Jun Pigm.,HE 6-Jun Pigm.,HE 05 50 F RE Jun-36 Pigm,HE,Hm II A 102 Jun-36 Pigm, 0 Progression
of IJRTLE 12-Jun Pigm 18-Jun Pigm, -1
6 49 M LE 6-Jun MA I B 8 6-Jun MA 07 66 F RE 6-Jun MA II A 48 Jun-60 ST BRVO -5 BRVO, ME
LE 6-Jun MA 12-Jun MA -2 Progressionof IJRT
8 45 F RE 12-Jun Whitng II A 48 18-Jun Whitng,MA -1 Progressionof IJRTProgressionof IJRT
LE 6-Jun Whitng 6-Jun Whitng,MA -1
9 57 F LE Jun-36 HE, Hm I B 36 Jun-36 HE 010 43 F RE Jun-36 Pigm II A 72 Feb-60 Scarred CNVM -5 Progression
of IJRTCrystals
LE 12-Jun Pigm 12-Jun 011 44 M RE 18-Jun Hm II A 12 9-Jun Whitng 2 Regression of
cornea
guttata in BELE 9-Jun Whitng 6-Jun Whitng 1
12 72 M RE Jun-36 Pigm., II A 42 Jun-36 Pigm., 0
LE 6-Jun Pigm 6-Jun Pigm -1 Progressionof IJRT
13 53 M RE 9-Jun Whitng II A 4 9-Jun Whitng 0 Progressionof IJRT
LE 6-Jun Whitng 9-Jun TV -114 57 F RE 18-Jun Whitng II A 30 18-Jun Whitng 0
LE 6-Jun Whitng 6-Jun Whitng 0
15 52 M RE 12-Jun Crystals II A 48 24-Jun Crystals,TV -2 ProgressionLE 18-Jun Crystals Jun-36 Crystals,TV -2 of Cataract in
BE
Fig. 3 (e & f) status quo fundus photograph in both eyes on
review
(e) (f)

December 2008 Mahesh G. et al. - Juxtafoveal Retinal Telangiectasia 353
16 58 F RE 24-Jun ME,Crystals, II A 24 18-Jun ME,Crystals, -1 Progressionof IJRT
Piigm Piigm MSCLE 9-Jun ME,Crystals, Jan-60 -10
Piigm17 61 F RE 12-Jun Whitng II A 6 12-Jun Whitng 0 Progression
of IJRTLE 9-Jun Whitng 9-Jun Whitng -1
18 50 F RE 24-Jun Crystals, Whitng II A 12 9-Jun TV, Crystals 2Cataractsurgery in BE
Whitng 2LE 24-Jun 9-Jun Whitng
19 41 F RE 12-Jun TV II A 72 12-Jun TV,Crystals 0LE 9-Jun TV 9-Jun TV 0
20 44 F RE 18-Jun Whitng II A 36 18-Jun Whitng 0
LE 6-Jun Whitng 6-Jun Whitng 0
Pigm : Pigmentation, MA : Microaneurysm, ME: Macular oedema, Whitng: Whitening TV: Telangiectatic vessels, Hm : Haemorrhage,BRVO: Branch retinal vein occlusion. CNVM: Choroidal neovascular membrane, RE : Right eye, LE : Left eye, BE: Both eyes Vn:Vision
eye. Colour fundus photography showed the disease
to be status quo in both eyes. (Fig. 3e & 3f)
Discussion
There were 5(25 %) patients with type 1B disease and
15(75 %) patients with type 2A disease confirming that
type 2a is the most common form of IJRT 12. Majority
(16 eyes, 45.71 %) maintained a stable visual acuity
and vision loss in patients with IJRT is generally mild
and occurs over many years 11.
When we analyzed each disease type, there were
5 patients with type I B disease, of which majority
(60 %) were male and mean age was 51.4 years. This
pattern in which middle-aged men are most commonly
affected correlates well with the demographic
characteristics described earlier 2,11. Regarding type 2A
disease, there were 15 patients and majority was
female. (66.66 %). This slight female preponderance
was in contrast to an earlier report 13 of equal sex
distribution.
Among the eyes in our study that lost vision, progression
of IJRT was responsible only in 64.28 % of cases. Loss
of central vision occurs slowly over many years and is
associated with atrophy of the foveolar retina 12. Visual
disturbance in retinal telangiectasia is usually due to
vascular leakage, with intra-retinal edema and exudate
accumulation and later cystic degeneration 13. However,
the development of neovascular membrane in the
vicinity of a black hyperplastic retinal pigment epithelial
plaque or a dilated vein passing at right angles into the
depth of the retina and indicative of a retinochoroidal
anastomosis can lead to rapid and severe visual
loss 2,14,15. None of the patients in our series developed
macular hole. The two recent reports 16,17 of full
thickness macular hole development in IJRT have
opened up a new dimension in the pathogenesis and
natural history of IJRT. The pronounced central foveal
structural abnormalities (for excavitation) could be due
to loss of the structural aspects afforded by Muller cells,
particularly the Muller cell cone. Hence loss of Muller
cells could be an important factor in the pathogenesis
of IJRT 17.
No intervention was done in any of the patients in our
series. Park and associates 16 attempted grid laser
photocoagulation for macular edema in IJRT but found
that it neither improved nor stabilized long-term visual
acuity. The role of any intervention arises only in
type 2 stage 5 diseases when there is development of
subretinal neovascularisation. Intravitreal injection of
triamcinolone acetonide has been found to be of some
benefit in few reports, but there are no randomized
controlled trials. The potential role of photodynamic
therapy with Verteporfin in IJRT with subretinal
neovascularisation has been well substantiated in
literature22-25. IJRT is a slowly progressive disease and
visual acuity remains stable for quite a long time.

354 Kerala Journal of Ophthalmology Vol. XX, No. 4
Conclusion
IJRT has favourable prognosis unless there is
development of subretinal neovascular membrane 12.
References
1) Gass JD. A fluorescein angiographic study of macular
dysfunction secondary to retinal vascular disease. V.
Retinal telangiectasis. Arch Ophthalmol. 1968 Nov;
80(5):592-605.
2) Gass JD, Blodi BA. Idiopathic juxtafoveolar retinal
telangiectasis. Update of classification and follow-up
study. Ophthalmology. 1993 Oct;100(10):1536-46
3) Puliafito CA, Hee MR, Lin CP, et al. Imaging of maculardiseases with optical coherence tomography.Ophthalmology. 1995;102:217-229
4) Hee MR, Izatt JA, Swanson EA, et al. Optical coherencetomography of the human retina. Arch Ophthalmol.
1995;113:325-332.
5) Voo I, Mavrofrides EC, Puliafito CA. Clinical applicationsof optical coherence tomography for the diagnosis andmanagement of macular diseases. Ophthalmol Clin
North Am. 2004;17:21-31
6) Berger AS, McCuen BW II, Brown GC, Brownlow RL Jr.
Surgical removal of subfoveal neovascularization in
idiopathic juxtafoveolar retinal telangiectasis. Retina.
1997;17:94-98.
7) Davidorf FH, Pressman MD, Chambers RB. Juxtafoveal
telangiectasis: a name change? Retina. 2004;24:
474-478.
8) Green WR, Quigley HA, De la Cruz Z, Cohen B. Parafoveal
retinal telangiectasis: light and electron microscopy
study. Trans Ophthalmol Soc U K. 1980;100:162-170
9) Eliassi-Rad B, Green WR. Histopathologic study of
presumed parafoveal telangiectasis. Retina. 1999; 19:
332-335.
10) Watzke R C et al., Long-term juxtafoveal retinal
telangiectasia.Retina. 2005 Sep;25(6):727-35.
11) Gass JD, Owakara RT. Idiopathic juxtafoveolar
telangiectasis. Arch Ophthalmol 1982;100;769-780.
12) Engelbrecht NE, Aaberg TM Jr, Sung J, Lewis ML.
Neovascular membranes associated with idiopathic
juxtafoveolar telangiectasis. Arch Ophthalmol. 2002
Mar;120(3):320-4.
13) Albert DM and Jacobiec A. Principles and practiceof Ophthalmology. W B Saunders Co. 2000; 1957-1965
14) Gitter KA, Yannuzzi LA, Schatz H. The macula : acomprehensive text and atlas.Baltimore: Williams and
Williams,1979:118-26
15) Gass JDM. Retinal capillary diseases, In:.Stereoscopic
atlas of macular diseases. 4th ed. St. Louis;Mosby;
1997;504-12
16) Koizumi H, Slakter JS, Spaide RF.Full-thickness macular
hole formation in idiopathic parafoveal telangiectasis.
Retina. 2007 Apr-May;27(4):473-6
17) Olson JL, Mandava N.Macular hole formation associated
with idiopathic parafoveal telangiectasia. Graefes Arch
Clin Exp Ophthalmol. 2006 Mar;244(3):411-2
18) Park DW, Schatz H, McDonald HR, Johnson RN.Grid
laser photocoagulation for macular edema in bilateral
juxtafoveal telangiectasis. Ophthalmology. 1997 Nov;
104(11):1838-46.
19) Maia Junior OO, Takahashi WY, Bonanomi MT,
Nascimento VP, Melo CS.Intravitreal triamcinolone
injection in the treatment of idiopathic juxtafoveal
telangiectasis] Arq Bras Oftalmol. 2006 Nov-Dec; 69(6):
941-4
20) Li KK, Goh TY, Parsons H, Chan WM, Lam DS.Use of
intravitreal triamcinolone acetonide injection in
unilateral idiopathic juxtafoveal telangiectasis.Clin
Experiment Ophthalmol. 2005 Oct;33(5):542-4.
21) Cakir M, Kapran Z, Basar D, Utine CA, Eroglu F, Perente
I.Optical coherence tomography evaluation of macular
edema after intravitreal triamcinolone acetonide in
patients with parafoveal telangiectasis. Eur J
Ophthalmol. 2006 Sep-Oct;16(5):711-7.
22) Alldredge CD, Garretson BR. Intravitreal triamcinolone
for the treatment of idiopathic juxtafoveal telangiectasis.
Retina. 2003 Feb; 23(1):113-6.
23) Snyers B, Verougstraete C, Postelmans L, Leys A,
Hykin P. Photodynamic therapy of subfoveal neovascular
membrane in type 2A idiopathic juxtafoveolar retinal
telangiectasis. Am J Ophthalmol. 2004 May;137(5):
812-9
24) Potter MJ, Szabo SM, Sarraf D, Michels R, Schmidt-Erfurth
U.Photodynamic therapy for subretinal neovascularization
in type 2A idiopathic juxtafoveolar telangiectasis. Can
J Ophthalmol. 2006 Feb;41(1): 34-7.
25) Hershberger VS, Hutchins RK, Laber PW.Photodynamic
therapy with verteporfin for subretinal
neovascularization secondary to bilateral idiopathic
acquired juxtafoveolar telangiectasis. Ophthalmic Surg
Lasers Imaging. 2003 Jul-Aug;34(4):318-20.
26) Hussain N, Das T, Sumasri K, Ram LS.Bilateral
sequential photodynamic therapy for sub-retinal
neovascularization with type 2A parafoveal telangiectasis.
Am J Ophthalmol. 2005 Aug;140(2): 333-5.
27) Abujamra S et al., Idiopathic juxtafoveolar retinal
telangiectasis: clinical pattern in 19 cases.
Ophthalmologica. 2000;214(6):406-11.

December 2008 G.J. Manayath - Avastin in CRVO 355
Bevacizumab (Avastin) Therapy for Macular
Oedema in Central Retinal Vein Occlusion –
Long Term ResultsDr. George J Manayath MS
Introduction
Although central retinal vein occlusion (CRVO) is one
of the most frequent retinal vascular disorders in clinical
practice, its pathogenesis is still not fully understood.
Green et al. 1 found venous thrombi in nearly all
rubeotic eyes after CRVO, but it remains unclear
whether venous thrombus formation represents the
beginning or rather the endpoint of the pathogenetic
cascade.
The development of macular edema is one of the most
common findings and the main reason for decreased
visual acuity (VA) in early CRVO. An impaired
Abstract
Background: There is no proven treatment for vision loss in central retinal vein occlusion (CRVO).
Bevacizumab has been reported in small series with limited followup to have a positive effect in
reducing macular edema (CME) and improving vision in central retinal vein occlusion . We report
long term results of Bevacizumab in central retinal vein occlusion.
Methods: Prospective interventional case series included 15 patients, serially evaluated with ETDRS
BCVA, OCT, FFA and Tonometry. Results were statistically analysed.
Results: Mean followup was 12 +/-3.6 months (range 6 -18 months). Mean number of injections
2.2 (range 1- 4) per patient. Statistically significant reduction of macular thickness (P<0.001) was
seen at 6 weeks (mean 346μ), 3months (353μ), 6months (348μ) and final followup (342μ).
Significant BCVA improvement seen at 6 weeks (Mean - .27 logmar), 3 months (.3 logmar),
6 months (.15 logmar) and final followup (.21 logmar) (P=0.009). 73.3 % patients had > 2 lines
of BCVA improvement at last followup.
Conclusion: Intravitreal Bevacizumab is an effective treatment option for CME in CRVO patients.
Re-injections at appropriate timing based on the OCT findings are important for better visual outcome
microcirculation and reduced blood flow lead to a
dysfunction of the endothelial blood-retinal barrier with
increased permeability and plasma exudation into the
central retina. A causative therapy to normalize the
retinal perfusion is desirable, but only hemodilution
therapy has shown limited benefit in randomized
studies 2,3,4.
It seems reasonable to reduce the macular edema as
soon as possible as irreversible damage of the
photoreceptors occurs as early as 3 months after the
development of macular edema 5,6. GRID laser
photocoagulation is an evidence-based therapeutic
option to reduce the macular edema in patients with
branch retinal vein occlusion (BRVO), but not in centralChaithanya Eye Hospital, Kochi
ORIGINAL
A R T I C L E

356 Kerala Journal of Ophthalmology Vol. XX, No. 4
retinal vein occlusion (CRVO) 7,8. Another option is the
injection of triamcinolone (IVTA) into the vitreous
cavity, which seems to be effective in early RVO.
However, recent results suggest that this effectiveness
is not maintained beyond 1 year despite repeated
injections. The main drawback of IVTA use is the high
rate of possible side effects such as glaucoma, cataract
formation or endophthalmitis 9,10,11,12. As in CRVO
patients the macular edema is thought to be at least
partly triggered by hypoxia-induced expression of
vascular endothelial growth factor (VEGF) 13,
intravitreally administered anti-VEGF antibodies have
recently been introduced into the treatment regime for
RVO patients 14.
Bevacizumab (Avastin, Genentech) was ,along with
pegaptanib,among the first anti-VEGF substances used
to treat macular edema in patients with CRVO 15,16,17.
Initial reports on intravitreal injections of bevacizumab
showed a significant reduction of central retinal
thickness and improved VA 14, 18. To date, only
retrospective studies and short term reports have been
published on bevacizumab treatment of CRVO 14, 18.
In this study we evaluate the safety,visual acuity changes
and morphologic response to bevacizumab treatment
in a prospective case series of CRVO patients.
Patients and Methods
Fifteen consecutive CRVO patients with central macular
oedema (CME) were included in this study.
Inclusion criteria
1. Funduscopically and angiographically diagnosed
CRVO duration of more than 4 weeks with CME of
more than 250 μm (measured by OCT 3, macular
thickness program).
2. Best corrected VA by ETDRS equal to or worse than
0.3 Logmar (Snellen = 6/12)
3. Age older than 18 years
4. Patient able to give informed consent
Exclusion criteria
1. Patients with retinal, angle or disc neovascularization
needing photocoagulation at first presentation
2. Other eye diseases that reduced VA
3. Not able to give informed consent
4. History of allergic reaction to bevacizumab
5. Pregnancy
6. History of Stroke/IHD/ uncontrolled HT
Study endpoints
The primary outcome was the improvement in visual
acuity (VA). Baseline visual acuity was measured using
ETDRS charts a few hours prior to injection as well as
on each follow-up visit (1 week and then 6 weekly after
injection). For ease of comparison and purpose of
statistical analysis, VA was converted to logMAR as well
as Snellen equivalents.
Secondary study outcomes were:
1. Central retinal thickness measured by optical
coherence tomography (OCT 3; macular thickness
program)
2. Complication rate (i.e., endophthalmitis, inflammation,
increased intraocular pressure, retinal tears, retinal
detachment and thromboembolic events)
3. To determine the best time point for re-injection
depending on the course of VA development as well
as central retinal thickness.
Patient examinations
The following data were registered: duration of CRVO
before injection, ophthalmologic and medical history,
patient age and sex, best corrected visual acuity (ETDRS
charts) and full ocular examination including OCT and
Applanation tonometry. We also documented retinal
changes by color fundus photographs and fluorescein
angiography (Topcon Imagenet, Japan) preoperatively
and between 6 and 12 weekly after injection.
All other parameters were evaluated on the day of
injection (baseline) as well as at 2 weeks and 6 weekly
after injection. On each follow-up visit, possible side
effects of the injection were ruled out.
Methods
All patients underwent intravitreal injection of 1.25 mg
bevacizumab (Avastin) in 0.05 ml total volume over

December 2008 G.J. Manayath - Avastin in CRVO 357
the inferior pars plana area, under strict aseptic
precautions. After 6 weeks of follow-up time, re-
injection of 1.25 mg bevacizumab was considered
depending on the individual treatment response and
OCT findings.
Study design
Our study design is that of a nonrandomized
interventional case series. All patients gave their
informed consent with specific emphasis on the off-
label character and possible systemic side effects as well
as unknown long-term ocular complications of
bevacizumab.
Statistics
Wilcoxon Signed Ranks test was used to calculate the
statistical significant difference between the paired
groups. Mann Whitney-U Test was used to calculate
the statistical significant difference between the two
independent groups. Friedman Multiple comparison
test was used to calculate the overall significance. The
level of significance was 0.05 (2-sided) in all statistical
testing. All these Statistical Analysis was performed
using the statistical software Stata 8.1 (College Station,
TX, USA).
Results
Table 1 displays the demographic data for all patients
enrolled in this study.
Table 1 Demographic data
No: of patients 15
Mean Age 64 years (40-82yrs)
Sex 13 Male / 2 Female
Duration of CRVO 3.3 months (range 1-10)
Type of CRVO 11 NICRVO / 4 ICRVO
The mean follow up was 12.2 ± 3.6 months (range -
6months to 18 months). All patients except one had
completed atleast 3 months since the last injection.
The mean number of injections per patient was
2.2 ± 0.884 (range – 1 to 4 injections per patient).
Visual acuity changes
The mean best corrected visual acuity at base line was
0.9 ± 0.31 Logmar units. Statistically significant BCVA
improvement (P = 0.009) was seen at 6 weeks 0.63 ±
0.34 (Mean improvement 0.27 logmar), at 3 months
0.60 ± 0.32 (mean improvement 0.31 logmar), at
6 months 0.74 ± 0.43 (mean improvement 0.15
logmar) and final followup 0.68 ± 0.54 (mean
improvement 0.21 logmar).
Overall there was a statistically significant improvement
in BCVA over time (P - 0.009) -FRIEDMAN test.
73.3 % patients had 2 or more lines of visual acuity
improvement and 60 % patients had 3 or more lines of
improvement. Table 2 shows the visual acuity change
distribution among the study patients at the final
follow up.
Fig. 1. changes in visual acuity over the study period
Table 2: Final BCVA (in logmar)
Frequency Percent
>2 lines improvement 9 60.0<=2 lines imporvement 2 13.3Remained same 2 13.3
Worsened 2 13.3Total 15 100.00
Macular thickness reduction
The mean central macular thickness (OCT) at baseline
was 615.7 ± 158.2 microns. Statistically significant
reduction of macular thickness (P<0.001) was seen at
6 weeks 269 ± 105μ (mean improvement 346μ), at
3 months 262 ± 129μ (mean improvement 353μ), at
6 months 261 ± 142μ (mean improvement 348μ) and
at final followup 273 ± 149 (mean improvement 342μ).
Overall there is a statistically significant difference in
macular thickness (p<0.001) - Friedman Test
73.3 % patients had a central macular thickness (CMT)
less than or equal to 250 microns at final followup visit.

358 Kerala Journal of Ophthalmology Vol. XX, No. 4
Table 3 shows the macular thickness distribution among
the study group at final followup.
There was no direct correlation found between macular
thickness reduction and BCVA improvement, as macular
macular thickness(CMT) reduction, throughout the
study period (Figure 3).
Subgroup analysis was done to assess if early injection
was associated with better final visual outcome and
patients injected before 12 weeks since the onset of
CRVO(Gp 1) was compared with those injected after
12 weeks (Gp2) of disease onset. However, early
injection group was not found to be significantly
associated with better final BCVA improvement
(P= 0.557). (Table 4)
Subgroup analysis was done to assess if ischemic (Gp1)
and non ischemic (Gp2) nature of the disease has
impact on visual outcome. Ischemic CRVO was
significantly associated with poor final visual acuity
outcome (P= 0.026) (Table 5).
No ocular complications were noted during the entire
study period including glaucoma, cataract,
endophthalmitis, vitreous haemorrage or retinal
detatchment. However, a 55year old patient reported
an episode of ischemic heart disease 3 weeks following
his first injection . He was a hypertensive on treatment
with single drug and no other systemic diseases. It is
unsure if this was a coincidence or complication.
Discussion
Although the exact pathological sequence of CRVO is
unknown, visual acuity seems to be not only dependent
on macular ischemia, but mainly on CME and
photoreceptor damage in the early period of the disease.
The aim in RVO treatment should therefore include
different therapeutical aspects: (1) causal therapy for
improved blood circulation and (2) prevention of
secondary changes such as CME and neovascular
complications. Besides hemodilution 2,3,4, additional
treatment options have been evaluated for the
improvement of blood circulation without conclusive
results so far.
With bevacizumab a new treatment option has been
introduced for early intervention against the formation
Fig. 2. Reduction in macular thickness over the study period
Table 3. Central macular thickness reduction in the studygroup at final followup
Final CMT
Frequency Percent
<=250 microns 11 73.3>250 microns 4 26.7
Total 15 100.0
thickness reduction was more pronounced, preceded
BCVA improvement and due to the multiple factors
determining the latter. However, there was a general
trend of BCVA improvement associated with central
Table 4. Duration of Disease vs final BCVA - (p. 0.557) - Mann - Whitney U Test
Duration of Disease N Minimum Maximum Mean Std. Deviation
12 weeks Final BCVA (in logmar) 8 .00 2.00 .6500 .66117
12 weeks Final BCVA (in logmar) 7 .00 1.17 .7243 .50113
Fig. 3. Correlation of post injection best corrected visual
acuity (BCVA) and central macular thickness (CMT)

December 2008 G.J. Manayath - Avastin in CRVO 359
of CME. Although the intravitreal injection of bevacizumab
has already gained high clinical relevance for the
treatment of retinal vascular diseases, to date only few
short term studies have evaluated the course of CRVO
after bevacizumab treatment.One retrospective study
with 16 eyes found an improvement of visual acuity in
87.5 % of the eyes treated after 3 months 14 . A second
retrospective study with 15 eyes found an increase in
visual acuity of more than 3 lines in 40 % of the patients
treated 18. In a prospective study by Schaal et al with 6
months follow-up, 2.5 mg Bevacizumab was reported
to improve visual acuity in 73.3 % eyes with CRVO 19.
The present prospective case series of 15 patients with
CRVO evaluates the 1 year course of visual acuity and
central retinal thickness after bevacizumab injection.
Peak VA was reached between 3 and 6 weeks after
injection and ranged from 1 to 5 lines. Of the treated
patients, 60 % gained 3 or more lines. This number is
in line with published data from retrospective and
shorter term studies 14, 18,19,20. 73.3 % eyes resolved CME
at final follow up and maximum reduction of macular
thickness was achieved by 1-2 weeks following the
injection. Central macular thickness reduction preceded
improvement in BCVA. But, no direct correlation was
found between VA and CMT reduction.
Both patients with low as well as high baseline
VA benefited from bevacizumab injection. Patients with
good initial visual acuity showed a tendency to gain
1–2 lines, whereas majority of patients with moderate
visual loss (up to 6/60) gained more than 2 lines.
Stahl et al 20 in their prospective study reported
significantly better visual outcome in patients receiving
bevacizumab within first 3 months of onset of CRVO
compared to CRVO older than 4 months. However, in
the present study and in a recent prospective study by
Priglinger SG et al 21, no statistically significant
difference in the final visual outcome was found
between the early and late injection groups. This could
be due to multiple factors influencing the visual
outcome or a small sample size.
A subgroup analysis for different occlusion types
revealed less visual acuity improvement for Ischemic
CRVO patients compared to Non Ischaemic CRVO
patients. Only 1 of the 4 eyes of Ischemic CRVO had
3 line improvement, mainly due to macular ischaemia
or neovascular complications like vitreous haemorrage.
Three of the 4 ischaemic CRVO eyes developed
neovascularization and 2 eyes with non ischemic CRVO
had ischaemic conversion, while on treatment with
Bevacizumab. Therefore, the current dose of 1.25 mg
doesn’t prevent neovascular complications in CRVO.
Dose escalation studies like that of Costa et al 22 with
2mg bevacizumab in Ischemic CRVO also has not shown
improvement in the avascular or ischaemic status of
the retina and further dose escalation studies are
required to answer this issue. It must also be noted
that due to the small patient number, subgroup analyses
can only indicate tendencies and do not reflect
statistically significant results.
The improvement of visual acuity after bevacizumab
injection was concordant with a decrease in central
retinal thickness. Regular OCT examinations can thus
be regarded helpful for early detection of an impending
drop in visual acuity after bevacizumab injection. An
increase in central retinal thickness should be
interpreted as an indication for re-injection. Regarding
the number of re injections required to achieve a stable
condition,this study showed a mean of 2.2 injections
per patient (range 1- 4 injections) during the study
period. From the natural course of RVO, however, it is
known that the imbalance between inflow and outflow
of the retinal circulation can prevail for several months
or even years. The formation of a new blood flow
balance is presumably supported by the formation of
collateral disc vessels with a new drainage route 23. It
is likely that bevacizumab treatment must be upheld
until a new balance between inflow and outflow in the
retinal circulation is reached.
The main challenge in bevacizumab treatment is to
maintain patients within the initially reached range of
visual acuity by means of well-timed reinjections in
Table 5. Diagnosis Vs Final BCVA - (p-0.026) - Mann-Whitney U Test
Diagnosis N Minimum Maximum Mean Std. Deviation
ICRVO Final BCVA (in logmar) 4 .90 2.00 1.2675 .50089
NICRVO Final BCVA (in logmar) 11 .00 1.00 .4727 .44518

360 Kerala Journal of Ophthalmology Vol. XX, No. 4
combination with laser treatment for the treatment of
secondary complications. Careful timing of bevacizumab
injection and laser treatment for ischemic complications
could have a beneficial effect.
The positive effect of bevacizumab injection on central
retinal thickness and visual acuity is evident when mean
values are considered, as was done in the present as
well as other studies 17, 19, 32. However, it should be
emphasized that within our study population some
individual treatment courses are not adequately reflected
by the presentation of the mean values discussed above.
Although most patients showed a good and reproducible
response to bevacizumab treatment, a certain inter
individual variability could be noted. In some patients,
a decrease of central retinal thickness was accompanied
by only a mild increase in visual acuity (due to macular
ischemia, foveal haemorrage with later
RPEdegeneration etc). In other patients, bevacizumab
injection neither diminished central retinal thickness,
nor improved visual acuity beyond week 3. These
patients did not differ from the rest of the study
population in terms of occlusion type, age of occlusion
or patient age. It can only be assumed that the degrees
of ischemia as well as other individual factors have an
impact on treatment response.
The causes and mechanisms for treatment failure with
bevacizumab injection have to be elucidated further in
vitro as well as in clinical studies. The question whether
bevacizumab might have negative long-term effects on
collateral vessel formation due to its anti-VEGF action
also needs to be addressed in these studies.
Conclusion
In summary, bevacizumab injection seems to
improve the visual acuity in the majority of CRVO
patients. This effect is probably due to a reduction of
blood vessel permeability similar to the effect of
intravitreally administered corticosteroids. In contrast
to intravitreal corticosteroids, however, a rise in
intraocular pressure was not observed in patients
treated with intravitreal bevacizumab. In the present
study, no other possible complications such as cataract,
pseudo-endophthalmitis, endophthalmitis, central
artery occlusion or retinal detachment were observed.
We therefore suggest bevacizumab treatment for
patients with CRVO under close postoperative
observation. Around week 6 after bevacizumab
treatment, re-injection should be considered based on
the OCT and visual acuity findings, until the disease
compensates.
References
1. Green WR, Chan CC, Hutchins GM, Terry JM (1981)
Central retinal vein occlusion: a prospective histopathologic
study of 29 eyes in 28 cases. Retina 1:27–55
2. Glacet-Bernard A, Zourdani A, Milhoub M, Maraqua
N, Coscas G, Soubrane G (2001) Effect of isovolemic
hemodilution in central retinal vein occlusion. Graefes
Arch Clin Exp Ophthalmol 239:909–914
3. Hansen LL, Wiek J, Wiederholt M (1989) A randomised
prospective study of treatment of non-ischaemic central
retinal vein occlusion by isovolaemic haemodilution.
Br J Ophthalmol 73:895–899
4. Wolf S, Arend O, Bertram B, Remky A, Schulte K,
Wald KJ, Reim M (1994) Hemodilution therapy in
central retinal vein occlusion. One-year results of a
prospective randomized study. Graefes Arch Clin Exp
Ophthalmol 232:33–39
5. Kalogeropoulos C, Donati G, Pizzolato GP, Pournaras
CJ (1996) [Morphology of early retinal lesions after
experimental venous occlusion]. Klin Monatsbl
Augenheilkd 208:375–376
6. Larsson J, Bauer B, Andreasson S (2000) The 30-Hz
flicker cone ERG for monitoring the early course of
central retinal vein occlusion. Acta Ophthalmol Scand
78:187–190
7. Branch Vein Occlusion Study Group (1984) Argon laser
photo coagulation for macular edema in branch vein
occlusion. J Ophthalmol 98:271–282
8. The Central Vein Occlusion Study Group (1995)
Evaluation of grid pattern photocoagulation for macular
edema in central vein occlusion. M report.
Ophthalmology 102:1425–1433
9. Goff MJ, Jumper JM, Yang SS, Fu AD, Johnson RN,
McDonald HR, Ai E (2006) Intravitreal triamcinolone
acetonide treatment of macular edema associated with
central retinal vein occlusion. Retina 26:896–901
10. Greenberg PB, Martidis A, Rogers AH, Duker JS,
Reichel E (2002) Intravitreal triamcinolone acetonide
for macular oedema due to central retinal vein
occlusion. Br J Ophthalmol 86:247– 248
11. Gregori NZ, Rosenfeld PJ, Puliafito CA, Flynn HW Jr,
Lee JE, Mavrofrides EC, Smiddy WE, Murray TG,
Berrocal AM, Scott IU, Gregori G (2006) One-year safety
and efficacy of intra- vitreal triamcinolone acetonide
for the management of macular edema secondary to
central retinal vein occlusion. Retina 26:889–895
12. Ip MS, Gottlieb JL, Kahana A, Scott IU, Altaweel MM,
Blodi BA, Gangnon RE, Puliafito CA (2004) Intravitreal
triamcinolone for the treatment of macular edema
December 2008 G.J. Manayath - Avastin in CRVO 361
associated with central retinalvein occlusion. Arch
Ophthalmol 122:1131–1136
13. Aiello LP, Avery RL, Arrigg PG, Keyt BA, Jampel HD,
Shah ST, Pasquale LR, Thieme H, Iwamoto MA, Park JE
et al (1994) Vascular endothelial growth factor in ocular
fluid of patients with diabetic retinopathy and other
retinal disorders. N Engl J Med 331:1480–1487
14. Iturralde D, Spaide RF, Meyerle CB, Klancnik JM,Yannuzzi LA, Fisher YL, Sorenson J, Slakter JS, FreundKB, Cooney M, Fine HF (2006) Intravitreal bevacizumab(Avastin) treatment of macular edema in central retinalvein occlusion: a short-term study. Retina 26:279–284
15. Moshfeghi AA, Puliafito CA (2005) Pegaptanib
sodium for the treatment of neovascular age-related
macular degeneration. Expert Opin Investig Drugs
14:671–682
16. Rosenfeld PJ, Fung AE, Puliafito CA (2005) Optical
coherence tomography findings after an intravitreal
injection of bevacizumab(avastin) for macular edema
from central retinal vein occlusion. Ophthalmic Surg
Lasers Imaging 36:336–339
17. Rosenfeld PJ, Moshfeghi AA, Puliafito CA (2005) Optical
coherence tomography findings after an intravitreal
injection of bevacizumab (avastin) for neovascular age-
related macular de-generation. Ophthalmic Surg Lasers
Imaging 36:331–335
18. Jaissle GB, Ziemssen F, Petermeier K, Szurman P,
Ladewig M, Gelisken F, Volker M, Holz FG, Bartz-
Schmidt KU (2006) [Bevacizumab for treatment of
macular edema secondary to retinal vein occlusion].
Ophthalmologe 103:471–475
19. Schaal KB,Hoh AE, ScheuerleA, Schutt F, Dithmar S
(2007) Bevacizumab for the treatment of macular
edema secondary to retinal vein occlusion.
Ophthalmologe 104(4):285-9
20. Stahl A,Agostini H,Hansen LL, Feltgen N (2007)
Bevacizumab in retinal vein occlusion-results of a
prospective case series.Graefes Arch Clin Exp
Ophthalmol 14:141-49.
21. Priglinger SG, Wolf AH, Kreutzer TC, Kook D,
Hofer A, Strauss RW ( 2007). Intravitreal bevacizumab
injections for treatment of central retinal vein occlusion:
six-month results of a prospective trial. Retina
27(8):1004-12.
22. Costa RA, Jorge R, Calucci D, Melo L A,Cardillo JA,
Scott IU (2007) Intravitreal Bevacizumab (avastin) for
central and hemicentral retinal vein occlusions :IBeVO
Study. Retina 27(2): 141-49.
23. Takahashi K, Muraoka K, Kishi S, Shimizu K (1998)
Formation of retinochoroidal collaterals in central
retinal vein occlusion. Am J Ophthalmol 126:
91–99.
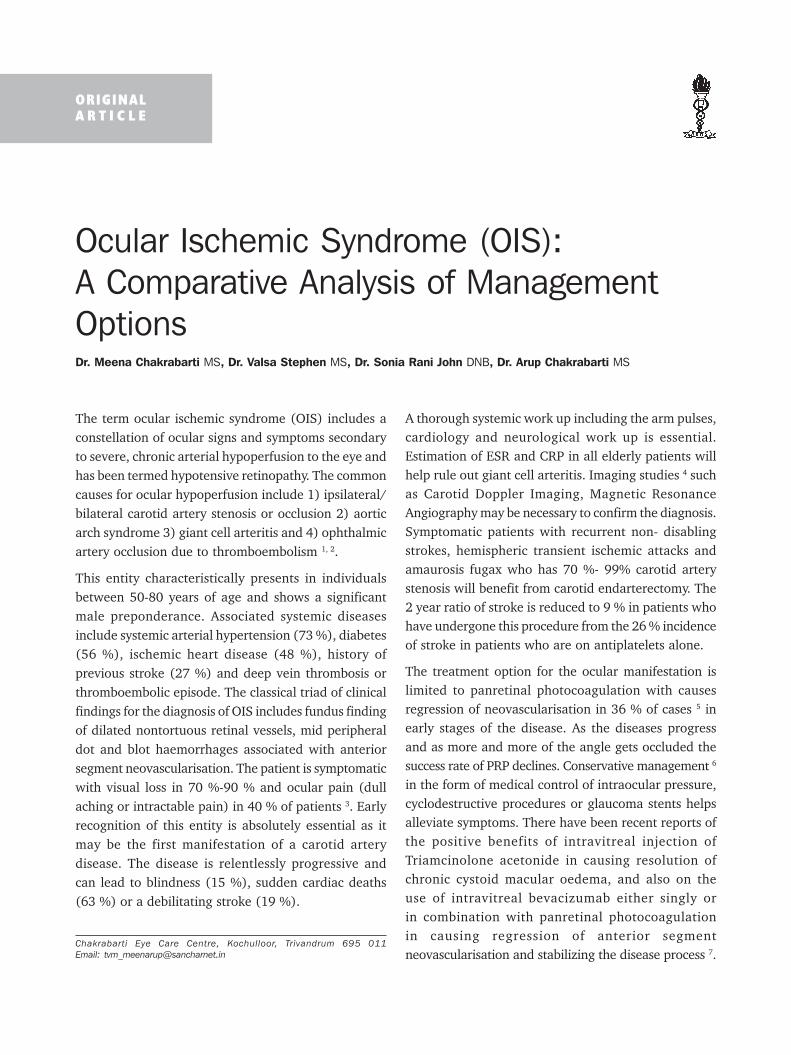
362 Kerala Journal of Ophthalmology Vol. XX, No. 4
Ocular Ischemic Syndrome (OIS):
A Comparative Analysis of Management
OptionsDr. Meena Chakrabarti MS, Dr. Valsa Stephen MS, Dr. Sonia Rani John DNB, Dr. Arup Chakrabarti MS
The term ocular ischemic syndrome (OIS) includes a
constellation of ocular signs and symptoms secondary
to severe, chronic arterial hypoperfusion to the eye and
has been termed hypotensive retinopathy. The common
causes for ocular hypoperfusion include 1) ipsilateral/
bilateral carotid artery stenosis or occlusion 2) aortic
arch syndrome 3) giant cell arteritis and 4) ophthalmic
artery occlusion due to thromboembolism 1, 2.
This entity characteristically presents in individuals
between 50-80 years of age and shows a significant
male preponderance. Associated systemic diseases
include systemic arterial hypertension (73 %), diabetes
(56 %), ischemic heart disease (48 %), history of
previous stroke (27 %) and deep vein thrombosis or
thromboembolic episode. The classical triad of clinical
findings for the diagnosis of OIS includes fundus finding
of dilated nontortuous retinal vessels, mid peripheral
dot and blot haemorrhages associated with anterior
segment neovascularisation. The patient is symptomatic
with visual loss in 70 %-90 % and ocular pain (dull
aching or intractable pain) in 40 % of patients 3. Early
recognition of this entity is absolutely essential as it
may be the first manifestation of a carotid artery
disease. The disease is relentlessly progressive and
can lead to blindness (15 %), sudden cardiac deaths
(63 %) or a debilitating stroke (19 %).
A thorough systemic work up including the arm pulses,
cardiology and neurological work up is essential.
Estimation of ESR and CRP in all elderly patients will
help rule out giant cell arteritis. Imaging studies 4 such
as Carotid Doppler Imaging, Magnetic Resonance
Angiography may be necessary to confirm the diagnosis.
Symptomatic patients with recurrent non- disabling
strokes, hemispheric transient ischemic attacks and
amaurosis fugax who has 70 %- 99% carotid artery
stenosis will benefit from carotid endarterectomy. The
2 year ratio of stroke is reduced to 9 % in patients who
have undergone this procedure from the 26 % incidence
of stroke in patients who are on antiplatelets alone.
The treatment option for the ocular manifestation is
limited to panretinal photocoagulation with causes
regression of neovascularisation in 36 % of cases 5 in
early stages of the disease. As the diseases progress
and as more and more of the angle gets occluded the
success rate of PRP declines. Conservative management 6
in the form of medical control of intraocular pressure,
cyclodestructive procedures or glaucoma stents helps
alleviate symptoms. There have been recent reports of
the positive benefits of intravitreal injection of
Triamcinolone acetonide in causing resolution of
chronic cystoid macular oedema, and also on the
use of intravitreal bevacizumab either singly or
in combination with panretinal photocoagulation
in causing regression of anterior segment
neovascularisation and stabilizing the disease process 7.Chakrabarti Eye Care Centre, Kochulloor, Trivandrum 695 011
Email: [email protected]
ORIGINAL
A R T I C L E

December 2008 M. Chakrabarti et al. - OIS: Management options 363
There is no general consensus on the management of
the ocular manifestation in patients with OIS and hence
several modalities of treatment have been tried.
This paper investigates the clinical features, and
compares the results of various management options
in 25 patients with suspected ocular ischemic syndrome.
Materials and Methods
A retrospective case study in which 34 eyes of
25 patients were included in the study group if
they had at least three of the five inclusion criteria
[(a) asymmetric retinopathy (b) elderly patient with
NVI of unknown cause (c) asymptomatic anterior
uveitis in elderly (d) presence of dilated retinal vessels
with no tortuosity (e) presence of mid peripheral dot
and blot haemorrhages in an ischemic featureless
retina], necessary for a diagnosis of ocular ischemic
syndrome.
Patients with a diagnosis of ocular ischemic syndrome
underwent a detailed medical and ocular histories,
complete ophthalmic evaluation, carotid evaluation by
Doppler and a through cardiology and neurological
work up. The management options used and its
outcome were assessed and compared. The patients
were divided into two groups based on the treatment
options chosen 1) PRP alone, 2) Combination of PRP
and intravitreal Bevacizumab.
The outcome measures assessed included post
treatment visual acuity, variation in the intraocular
pressure, fluorescein angiographic findings and
complications. The patients were followed up at
monthly intervals for 12 months.
Results
We analyzed the clinical features and management options
in 34 eyes of 25 patients with a diagnosis of Ocular
Ischemic Syndrome. Analysis of the demographic data
showed that the patients were of age group ranging
from 60 years to 85 years (mean 63 ± 8 years). The
male female ratio in our study population was 2:1.
Associated systemic diseases included arterial
hypertension: 28.6 %, diabetes: 85.7 %, coronary artery
disease: 20 %, history of previous stroke: 30 % and
10 % of patients were on haemodialysis.
Thus in our study population, majority of the patients
had associated diabetes (85.7 %) and had presented
with features of both proliferative diabetic retinopathy
and chronic ocular ischemia out of proportion to the
retinal changes in the contralateral eye. The
presentation was unilateral in 64 % of patents while
bilateral involvement was seen in 36 %.
Presenting visual symptoms included gradual visual loss
in 82.5 %, sudden visual loss (17.5 %); dull aching
ocular pain in 30 % of patients. At initial presentation,
eyes with Ocular Ischemic Syndrome had a visual acuity
ranging from hand movements to 6/6. 50 % of patients
presented with a visual acuity of hand movements only.
Ophthalmic evaluation included slit lamp
biomicroscopy, applanation tonometry, fluorescein
fundus angiography, field charting and optical
coherence tomography. Results of ophthalmic
evaluation in our study population is listed in Table 1
Table 1: Ocular Findings in OIS
1 Corneal Oedema 5 %2 Hypotony 10 %3 Elevated IOP ( NVG ) 42 %4 NVI 88 %5 AS inflammation 20 %6 Cataract 30 %7 Optic Disc Pallor 30 %8 AION 10 %9 CRAO 12 %10 Combined OIS and DR 5.7 %11 Ischemic featureless retina 88 %12 Extensive CNP on FFA 40 %13 CME on OCT 10 %14 Classical triad of dot h/ages
in mid periphery, NVI and dilatednon tortuous veins 24 %
15 NVD and NVE 13 % and 8 %
NVG: Neovascular Glaucoma; NVI: Neovascularisation of Iris; IOP:Intraocular pressure; AS: Anterior segment; AION: Anterior IschemicOptic Neuropathy, CRAO : Central Retina Artery Occlusion, DR:Diabetic Retinopathy; CNP: Capillary Non perfusion, FFA: Fluorosceinangiography; CME: Cystoid Macular edema; OCT: Optical Coherence
Tomography
Corneal oedema was the presenting feature in 5 % of
our patients and these patients presented with visual
blurring and foreign body sensation as well as ocular
pain. Ocular hypotony was present in 10 % of patients
who had associated corneal striae, anterior chamber
inflammation and new vessels on the iris. Low arterial
pressure to the ciliary body with resultant decrease in
aqueous production is responsible for paradoxical
lowering of IOP in the presence of neovascularisation.

364 Kerala Journal of Ophthalmology Vol. XX, No. 4
42 % presented with neovascular glaucoma out of the
88 % who had NVI at presentation. Anterior segment
inflammatory signs characterized by flare and cells in
the anterior chamber were present in 2 % of the study
population at initial presentation. Optic disc findings
included uniformly pale disc (30 %); anterior ischemic
optic neuropathy (10 %) and central retinal artery
occlusion (12 %). Majority of our patients (85.7 %)
were diabetic and presented with features of diabetic
retinopathy on an ischemic featureless background
associated with gross asymmetry in the fundus findings
between the 2 eyes. An ischemic featureless retina with
out much neovascular proliferation associated with mid
peripheral dot and blot haemorrhages, and venous
dilatation, as well as multiple intraretinal microvascular
anomalies (Fig. 1) was seen in 88 % of our patients
with suspected OIS. 40 % of patients had extensive
capillary non perfusion areas in the fluorescein
angiograms (Fig. 2). 10 % of patients had demonstrable
cystoid macular oedema in OCT images.
Neovascularisation of the disc was present in 13 % of
patients while only 8 % had neovascularisation
elsewhere in the retina. Carotid Doppler showed
significant occlusion due to atheromatous plaques in
40 % of patients. The degree of stenosis produced by
the plaques was less than 70 % on an average and hence
none of our patients where counseled to undergo
carotid endarterectomy.
A retrospective analysis of the treatment options and
the results were compared between the 2 treatment
groups. The post treatment visual acuity, intraocular
pressure, regression of NVI, need for repeat treatments
were compared in all three treatment groups. Table 2
gives a comparative analysis of results of treatment.
Table 2 Comparative Analysis of Treatment Options
Criteria PRP alone Combined(30 eyes) PRP with IVB
(4 eyes)
1 Post Rx BVCA Not affected Not affected2 IOP 7mm reduction 20 mm ±3 mm
at 3 months reduction at3 months
3 Regression of NVI + +++4 Time to regression 4 weeks 1 week5 Repeat Treatment Necessary in Not given
4 % for
recurrent VH
None of the treatment options produced any visual
improvement. Pan retinal photocoagulation was
effective in controlling the neovascular process in
36 % of the treated 30 patients. It had no effect on the
visual acuity and did not produce significant lowering
of IOP in patients with NVG (7 mm ± 2mm Hg).
Conservative treatment had to be continued along with
maximal anti glaucoma medication to keep the patient
Fig. 1. Classical clinical features of OIS in an unilateral caseshowing mid-peripheral dot and blot hemorrhagesand extensive capillary non perfusion in thefluorescein angiography
Fig. 2. Showing a featureless ischemic retina with extensiveCNP areas, NVI and macular ischemia

December 2008 M. Chakrabarti et al. - OIS: Management options 365
comfortable. PRP had to be repeated in 40 % of patients
for recurrent vitreous haemorrhage.
Combination of PRP with IVB was the treatment option
in 4 patients. This group had maximum reduction of
NVI, with regression occurring within 1 week. The IOP
dropped by 20 mm ± 8 mm Hg from the baseline.
Repeat treatment was not necessary. This combination
may prove valuable in patients who are detected early.
In addition to local treatment all patients continued
their regular medications for hypertension and diabetes
along with antiplatelet medications and were kept
under regular follow up with the cardiologist and
neurologist. In one patient there was progressive optic
disc pallor with decreased vision at 6 months following
IVB injection.
Discussion
We present a retrospective series of patients with ocular
ischemic syndrome. The characteristic features of our
series are
1. Early cases of OIS were included.
2. 87.5 % had associated diabetes and diabetic
retinopathy.
3. Carotid Doppler showed atheromatous plaque with
stenosis < 70 % in 40 % of patients.
4. 10 % of our patients presented with hypotony, NVI
and anterior segment reaction
5. 22 % of patients had acute visual loss either due to
AION (12 % ) or CRAO (10 % )
6. Aching orbital pain was present in 40 %
7. The incidence of NVG was 40 % in our series.
8. Ischemic featureless retina with mid peripheral dot
and blot haemorrhages was the commonest ocular
fundus finding.
9. Neovascular proliferation in the fundus was not
common with NVD in (13 %) and NVE in (8 %).
confirming with other series.
10. PRP as a treatment option was able to stabilize the
ischemic process in 36 % of patients. Recurrence
in the form of recurrent VH necessitated repeat
treatment in all patients in this group.
11. Combining IVB with PRP proved to be the most
efficacious treatment modality and should be
considered in all early cases with OIS.
12. Presence of NVI indicated as poor treatment out
come and hence early detection and initiation of
treatment is mandatory.
Thus eyes with asymmetric retinopathy with an
ischemic featureless background fundus appearance
will definitely benefit from combining IVB with PRP
especially if they also have diabetic retinopathy.
Conclusion
Early detection of features of OIS needs a high index
of suspicion 8. OIS should be suspected in the following
situations.
1. Elderly patients presenting with non specific and
asymptomatic anterior segment inflammation
2. Presence of asymmetric retinopathy
3. Presence of NVI of unknown cause in an elderly
patient.
4. Ocular hypotony in elderly in presence of NVI and
inflammation
5. Non tortuous dilation of retinal vessels.
6. Elderly patient with h/o non deblitating stroke,
transient ischemic attacks and amaurosis fugax
A thorough ophthalmic evaluation in addition to a
detailed systemic work up and imaging studies is
necessary in all patients. Control of systemic risk factors,
regular use of anti-platelet medication combined with
vigorous local treatment of the ocular condition, may
help safeguard the patient. Presence of iris
neovascualrisation heralds a point of no return
indicating progress of disease which will continue
unabated unless early intervention in the form of
combined PRP and IVB is given. Combining anti VEGF
therapy with PRP helps stabilize disease progression,
speeds control of anterior segment neovascualarisation
and eliminates need for subsequent surgeries.
Carotid Endarterectomy is necessary in symptomatic
patients with 70 - 99 % 9, 10 stenosis especially in the
presence of non disabling stroke, amaurosis and
hemispheric transient ischaemic attacks. Carotid

366 Kerala Journal of Ophthalmology Vol. XX, No. 4
endarterectomy has been shown to reduce the 2 year
rate of stroke to 9 % in comparison to the 26 % incidence
in patients who are on anticoagulants alone. Bypass
procedures in the form of Superficial Temporal Artery
to Middle Cerebral Artery (STA-MCA by pass) can be
considered in patients with 100 % carotid stenosis.
5 % – 15 % of patients with carotid artery occlusive
disease develop ocular ischemic syndrome and this
condition can become bilateral in 20 % patients. Early
detection is mandatory to ward off permanent
blindness, debilitating stroke and sudden death.
Reference
1. Antebana N.H, Brown GC; et al. Ocular IschemicSyndrome, Duanes Clinical Ophthalmology, Ed.Tasman W, Jaeger EA, 1998, Vol:3, 12,1-19
2. Hamed L M, Guy JR, Moster ML, Bosely et al. Giant cellArteritis in Ocular Ischemic Syndrome. Am. J.Ophthalmol 1992, 113: 702-5
3. Johnson M A. Use of electroretinographic ratios inassessment of vascular occlusion and ischaemia,Principles and Practice of clinical electrophysiology of
vision Ed. Hickenlively J and Arden G, Ed by MosbyYear Book, 1991, 613-618
4. H O AC, Lieb WE, Flaharty PM et al. Color DopplerImaging of the ocular ischemic syndrome. Ophthalmol1992,99,1453-62
5. Mizeber JB, Podhajsky P, Hayreh SS. Ocular IscheamicSyndrome. Ophthalmology 1997;104:859-64
6. Ryan S J, Schachart AP, Murphy RP, Patz A. The OcularIschemic Syndrome. Retina, Vol II , Ed SJ Ryan; 1989;88; 547-59
7. Luis Amselemab, Javier Montero, Manual Daiz- Llopisb;S. Pulido et al. Intravitreal Bevacizumab injection inocular ischemic syndrome. Am J. Ophthalmol, 2007;Vol 144 (1): 122-124
8. Sivalingam A, Brown GC, Magargal LE. The OcularIschemic Syndrome III The visual Prognosis andthe effect of treatment. Intl. Ophthalmol 1991;15:15-20
9. Story JL, Held K, Harrison JM, Cleland TP, Eubanks KDet al. The Ocular Ischemic Syndrome in carotid arterydisease. Ophthalmic Color Doppler flow velocity andelectroretinographic changes following carotid arteryreconstruction. Surg Neurol 1995; 44:534-5
10. Winter Korn J M, Beckman RL et al. Recovery fromOcular Ischemic Syndrome after treatment withVerapamil J Neuro-Ophthalmol 1995;15:209-11

December 2008 Gopal S. Pillai et al. - IVTA and Macular Laser in DME 367
Primary IVTA with Secondary Macular Laser
versus Primary Macular Laser with
Secondary IVTA in Diabetic Macular Edema
with Subfoveal Sensory DetachmentDr Gopal S. Pillai MD DNB FICO FRCS, Dr Niranjan P. MBBS DNB
acetonide (IVTA) injection. There is continuing debate
about which treatment modality is superior.
In this study we tried to look at this subject in a selective
subset of diabetic macular edema patients having a
subfoveal sensory neural detachment (SFSND).
Methods:
No of patients: 22 consecutive patients
Inclusion criteria: Presence of diabetic maculopathy
irrespective of the status of diabetic retinopathy and
optical coherence tomography (OCT) showing
subfoveal sensorineural detachment.
Randomisation: Patients were randomly allocated
to one of the groups: one group receiving IVTA as
primary treatment and other group treated primarily
with focal macular laser.Dept. of Ophthalmology, Amrita Institute of Medical Sciences, Kochi
Abstract
22 eyes with subfoveal sensory detachment were randomized into primary IVTA and primary focal
macular laser and studied for 6 months
Macular thickness reduced and visual acuity increased significantly more in primary IVTA than in
primary laser after the first treatment. At the end of 6 months, there was still a statistically significant
difference between the two groups.
Primary IVTA gives better results in subfoveal sensory detachment than primary laser therapy.
Introduction
Nearly 171 million people worldwide have diabetes.
This figure is likely to double by 2030. India holds 31.7
million diabetic patients ranking first in the world. This
number is projected to increase to 79.4 million by 2030 1.
Diabetic Retinopathy (DR) is a common complication
of diabetes which accounted for 5 million blind in year
2002. 2 The increasing incidence of diabetes has caused
diabetic retinopathy to be included in the “priority list”
as a part of “Vision 2020” 2. Among the various types
of diabetic retinopathy, diabetic maculopathy is the
commonest cause of visual impairement 3.
The different modalities of treatment for diabetic
macular edema include focal macular laser
photocoagulation and intravitreal triamcinolone
ORIGINAL
A R T I C L E

368 Kerala Journal of Ophthalmology Vol. XX, No. 4
Preoperative evaluation: Best corrected visual
acuity (BCVA) for distance and near, Fundus Fluorescein
Angiography (FFA), Optical Coherence Tomography
(OCT) of macula measuring central foveal thickness
and total macular volume.
Operative intervention:
IVTA: 4mg (0.1ml) triamcinolone acetonide injection
into vitreous cavity under all aseptic precautions in
inferotemporal quadrant 4mm from limbus in phakic
patients, 3mm in aphakes and 3.5mm in pseudophakes.
Patients were advised sitting up position for 24 after
injection.
Focal macular laser: No of burns: 200, strength of
burns: 150-200 mw, size of burns: 100-150 microns,
Site of burns: Leaking microaneurysms.
Post intervention follow-up: Schedules for next
day, after one week and then after one month and
6 months. At each visit BCVA for distance and near,
intraocular pressure and status of lens transparency
(especially in IVTA group), OCT of macula measuring
central foveal thickness and total macular volume was
obtained.
At the end of 1 month, if response to primary treatment
was not found to be adequate, either IVTA (for cases
who had focal macular laser as primary treatment) or
focal macular laser ((for cases who had IVTA as primary
treatment) was given.
Main outcome:
Improvement in best corrected visual acuity (BCVA)
for distance and near, central foveal thickness and total
macular volume.
Results:
Out of 22 patients, 12 were women and 10 were men.
The mean age was 63 years (range 49-70 years). All of
them were type II diabetics and 18 of them on insulin.
The average duration of diabetes was 20 years (range
5-29 years). 10 patients also had associated diabetic
nephropathy, 12 had hypetension and 8 had dyslipidemia.
During the course of study, these comorbidities were
monitored and were found to be stable.
The baseline mean foveal thickness in group I was
444.9 microns and 486.9 microns in group II.
The change in foveal thickness at the end of 1 month
and 6 months is shown in the following table 1.
Table 1: showing change in foveal thickness at 1 month and6 months
Mean foveal thickness Group I Group II
(microns)
Baseline 444.9 486.9
After I month 250.2 438.7
(Change) (-194.7) (-61.2)
After 6 months 212.6 312.6
(Change) (-241.7) (-177.5)
The drop in mean central foveal thickness was markedly
higher in group I than group II at the end of 1 month
and 6 months. This difference had strong statistical
significant (P < 0.005)
The baseline BCVA for distance and at I month & 6
month follow up is shown in following table 2.
Table 2: showing baseline BCVA at 1 month and 6 months
Mean BCVA for Group I Group IIdistance (in decimal)
Baseline 0.36 0.31
After I month 0.51 0.32
(Change) (+0.15) (+0.1)
After 6 months 0.62 0.44
(Change) (+0.26) (+0.13)
As seen from the above table, the improvement in
BCVA for distance is much more faster and better in
group I compared to group II. This is also statistically
significant. ( P < 0.05)
The near vision in both the groups had increased at 1
month and 6 months, the change between them was
not statistically significant.
IOP had risen from 2-8 mm of Hg in both the groups.
But there was no statistically significant rise at the end
of 6 months in either of the groups.
There was no significant cataract progression in either
of the groups till 6 months.
Discussion
Although several treatment modalities are currently
under investigation for diabetic macular oedema , the
only demonstrated means to reduce the risk of vision
loss from diabetic macular edema are laser
photocoagulation, as demonstrated by the ETDRS, and

December 2008 Gopal S. Pillai et al. - IVTA and Macular Laser in DME 369
intensive glycemic control, as demonstrated by the
Diabetes Control and Complications Trial (DCCT) 4 and
the United Kingdom Prospective Diabetes Study
(UKPDS) 5.
Recently, the managament of diabetic macular oedema
(DME) has significantly changed with the availability
of optical coherence tomography. It helps to classify the
DME in different types which guides the treatment 6.
We looked at the subset of patients who had a subfoveal
sensorineural detachment as shown by OCT. The reason
being these are the most visually significant cases and
we wanted to find out the best way of dealing with
these specific group of cases.
The frequency of an unsatisfactory outcome following
laser photocoagulation in some eyes with diabetic
macular edema has prompted interest in other
treatment modalities. One that has recently generated
interest is intravitreal injection of triamcinolone
acetonide.
How does IVTA act?: Diabetic macular edema results
from abnormal leakage of macromolecules, such as
lipoproteins, from retinal capillaries into the
extravascular space followed by an oncotic influx of
water into the extravascular space 7. The increase in
retinal capillary permeability and subsequent retinal
edema may be the result of a breakdown of the blood
retina barrier mediated in part by VEGF, a 45 kD
glycoprotein 8. The normal human retina contains little
or no VEGF; however, hypoxia causes upregulation of
VEGF production 9. So attenuation of the effects of
VEGF provides a rationale for treatment of macular
edema associated with diabetic retinopathy.
Corticosteroids, a class of substances with anti-
inflammatory properties, have been demonstrated to
inhibit the expression of the VEGF gene 10.
Intravitreal injection has been proposed as a way to
deliver corticosteroid (triamcinolone acetonide) to the
posterior segment. Triamcinolone acetonide is readily
available (Kenacort). However, it is not specifically
formulated for intraocular use. The most common dose
of triamcinolone acetonide used to treat eyes with
diabetic macular edema is 4mg 11. This dose is typically
used because at a shelf dosage of 40mg/cc, it is easily
aliquoted to a 4mg/0.1cc dose. A volume of 0.1cc is
readily injected into the vitreous cavity. Other than the
convenience of this dose, there are no data that support
the use of 4mg over any other alternative dose. The
use of 25mg of triamcinolone acetonide has less
commonly been used to treat eyes with diabetic macular
edema.12 However, there are no data that compare the
efficacy and safety of the 4mg vs. the 25mg dose.
Side effects of IVTA: Elevation of intraocular pressure,
progression of cataract and endophthalmitis are the
known side effects of this treatment.
Comparison of our results with other studies:
There was no study which compared the role of IVTA
and focal laser both in a specific population of patients
with subfoveal sensorineural detachment.
Kang SW & et al found that visual acuity and decrease
in foveal thickness was significantly better in patients
receiving IVTA followed by focal laser than patients who
receive only IVTA. 13
Our results were also similar.
We did not have any significant adverse effects apart
from transient elevation of IOP.
Shortcomings
Long term follow up data should be available to find
out the stability of these effects.
Conclusion
In cases of CSME with subfoveal sensorineural
detachment, first IVTA followed by focal macular laser
after a month gives significantly better outcome than
focal laser followed by IVTA.
References
1. “Diabetes Action now: An Initiative of the World Health
Organization & the International Diabetes Federation”
A WHO publication, 2004 pg: 10
2. “Blindness: vision 2020- control of major blinding
disease & disorders”, A WHO publication, Feb.2000.
3. ‘Retina’, Volume II Medical Retina, Editor in Chief:
Stephen Ryan, Fourth Edition, Elsevier Mosby publishers
2006, page no 1275.
4. Diabetes Control and Complication Trial Research
Group. The effect of intensive treatment of diabetes on
the development and progression of long-term
complications in insulin-dependent diabetes mellitus.
N Engl J Med 1993; 329:977-986.

370 Kerala Journal of Ophthalmology Vol. XX, No. 4
5. UK Prospective Diabetes Study Group. Intensive blood-glucose control with sulphonylureas or insulincompared with conventional treatment and risk ofcomplications in patients with type 2 diabetes.UKPDS 33. Lancet 1998; 352:837-853
6. Atlas Optical Coherence Tomography of MacularDiseases, Vishali Gupta, Amod Gupta, Mangat Gupta,Jaypee brothers, First edition 2004.
7. Ferris F, Patz A. Macular edema: a complication ofdiabetic retinopathy. Surv 1640 Ophthalmol 1984; 28(suppl):452-61.
8. Aiello L, Bursell S, Clermont A, et al. Vascularendothelial growth factor-induced retinal permeabilityis mediated by protein kinase C in vivo and suppressedby an orally effective beta-isoform-selective inhibitor.Diabetes 1997; 46:1473-80.
9. Vinores S, Youssri A, Luna J, et al. Upregulation ofvascular endothelial growth factor in ischemic and
non-ischemic human and experimental retinal disease.Histol Histopathol 1997; 12:99-109.
10. Nauck M, Karakiulakis G, Perruchoud A,Papakonstantinou E, Roth M. Corticosteriods inhibit theexpression of the vascular endothelial growth factorgene in human vascular smooth muscle cells. Euro JPharmacol 1998; 341:309-15.
11. Martidis A, Duker J, Greenberg P, et al. Intravitrealtriamcinolone for refractory diabetic macular edema.Ophthalmology 2002; 109:920-7. 1696
12. Jonas J, Sofker A. Intraocular injection ofcrystalline cortisone as adjunctive treatment ofdiabetic macular edema. Am J Ophthalmol 2001;132:425-7.
13. Kang SW, Sa HS,Cho HY,Kim JI. Macular gridphotocoagulation after intravitreal triamcinoloneacetonide for diffuse diabetic macular edema. ArchOphthalmol. 2006 May;124(5):653-8.

December 2008 Kerala Journal of Ophthalmology 371
Long -Term Results of Surgical
Management of Severe Contusion Injury
With Dislocated LensesDr. Meena Chakrabarti MS, Dr. Valsa T.Stephen MS, Dr. Arup Chakrabarti MS, Dr. Sonia Rani John DNB
Introduction
Traumatic cataracts and subluxated or dislocated
crystalline lenses are frequently encountered in the
settings of severe ocular trauma. Traumatic cataracts
are thought to develop secondary to equatorial
expansion with rupture of the lens capsule. This
equatorial expansion may also cause a significant
amount of zonules to dehisce with subsequent
subluxation or dislocation 1. Dislocation implies a
complete displacement of the lens from the pupillary
region either posteriorly into the vitreous cavity or
anteriorly into the anterior chamber. Management of
these commonly encountered entities first requires a
thorough evaluation for any other associated pathology
such as herniation of vitreous into the anterior chamber,
angle recession, vitreous haemorrhage, retinal breaks
or retinal detachments 2.
History and Clinical Evaluation: - The evaluation of the
crystalline lens after injury requires a thorough
ophthalmic examination to look for an occult posterior
scleral perforation, vitreous herniation into anterior
chamber, gonioscopy for traumatic angle recession,
dilated indirect ophthalmoscopy for retinal tears, retinal
detachments or vitreous haemorrhage 3.
In the presence of traumatic hyphema or vitreous
haemorrhage, B. Scan ultra sonography 4 may be of a
great value in delineating the dislocated lens as well as
for evaluating for other associated posterior segment
pathologies.
We present the results of a retrospective analysis of 25
cases of severe contusion injury with dislocated
crystalline lenses, which was managed, at our centre
with lens removal and anterior chamber ACIOL
implantation.
Methods
A retrospective case sheet analysis of all cases managed
by us with a diagnosis of blunt injury severe enough to
cause dislocation of crystalline lens into the vitreous
cavity was performed. The data retrieved from the case
sheets included the mechanism of injury, the best
corrected visual acuity, biomicroscopic examination of
the anterior segment, tension applanation, associated
posterior segment findings, details of the surgical
procedure performed including the technique used for
lens removal and the type of IOL implanted, as well as
the intraoperative difficulties and post operative
complication both immediate and long term. The
duration of follow up was 24 months to 60 months.
All patients had undergone a thorough preoperative
evaluation, which included a detailed history to elicit
the mechanism of trauma, the time of presentation for
treatment and a thorough evaluation of both anterior
and posterior segment of the eye. The surgical
procedure depended on the results of the preoperative
evaluation. Patients with associated retinal detachment,Chakrabarti Eye Care Centre, Kochulloor, Trivandrum - 695 011,
E-mail: [email protected]
ORIGINAL
A R T I C L E

372 Kerala Journal of Ophthalmology Vol. XX, No. 4
underwent a combined scleral buckling, pars plana
vitrectomy, use of perflurocarbon liquid to achieve
mechanical retinal flattering and also to elevate the
lens to the pupillary area. Lens removal was performed
using the ocutome cutter in 8 eyes, by using the
phacofragmatome hand piece in 9 eyes or though a
limbal incision in 9 eyes. In 22 of the 25 eyes an anterior
chamber Kelman multiflex AC IOL was implanted. In
three patients who had an associated retinal
detachment, underwent repair of the detachment along
with lens removal and were left aphakic. The presence
or absence of intraoperative problems, short and long
term postoperative complications were noted and
analyzed.
Results
A retrospective analysis of the case records of all
patients managed at our centre (between March 1999-
2007 March) for traumatic dislocation of crystalline
lens were analyzed. 25 patients with a postoperative
follow up varying from 24 months to 60 months formed
the study group (Mean 42 m).
The patients were of the age group 30-70 years of age
(Mean age = 50 years). The patients were
predominantly males (19 patients) and there were 6
female patients in the study population. The mechanism
of injury is listed in Table 1.
Table 1: Mechanism of Injury
1 Mango falling on face 42 Struck while cutting firewood 43 Soda bottle blast injury 14 Domestic Violence 35 Stone throw 86 Injury with Idiyappam makers spring
(Rice hopper) 27 Assault (MLC) 3
Majority of patients were referred within a week of
sustaining the blunt injury (20 eyes). 5 cases reported
within 2 weeks of sustaining injury. Associated anterior
segment findings included traumatic hyphema (3 eyes;
12 %); Sphincter tears (2 eyes; 8 %); angle recession
(5 eyes; 20 %); traumatic glaucoma (7 eyes; 28 %);
vitreous herniating into anterior chamber (3 eyes;
12 %); uveitis (2 eyes; 8 %); and traumatic mydriasis
in 4 eyes (16 %) (Table 2). Patients were taken up for
surgery after controlling the intraocular inflammation
and achieving medical control of IOP before surgical
intervention.Table: 2: Anterior Segment Findings
Findings No of eyes %
1 Hyphema 3 12%2 Sphincter Tear 2 8 %3 Angle recession 5 20 %4 Glaucoma 7 28 %5 Vitreous in AC 3 12 %6 Uveitis 2 8 %7 Tr Mydriasis 4 16 %
A dilated posterior segment evaluation was performed
and whenever Indirect Ophthalmoscopic view was poor,
a B.Scan USG was performed. Associated posterior
segment findings included vitreous haemorrhge (9 eyes;
36 %). Berlins oedema (2 eyes ; 8 %); Avulsed vitreous
base (1 eye ; 4 %), Retinal tear (3 eyes ; 12 %); Retinal
detachment (2 eyes; 8%), Choroidal rupture (1 eye ;
4 %) Fig. 1. (a-d). The preoperative best corrected visual
Fig. 1. (a-d) : Preoperative ocular findings. (a). Total
hyphema b) Dislocated lens (c) Bullous retinaldetachment (d) Choroidal rupture with organizedsubretinal blood
acuity ranged from Hand movements (HM) to 6/6 with
aphakic correction.
In all patients the surgery was performed under local
anaesthesia. Two patients with retinal detachment
underwent retinal detachment repair along with lens
removal and were left aphakic. In these 2 eyes
Perflurocarbon liquid (PFCL) was used to float the
dislocated lens into the pupillary area for where it was
removed through a limbal incision. The soft lens
dislocation was managed by performing a parsplana

December 2008 M. Chakrabarti et al. - Surgical Management of Dislocated lenses 373
lensectomy using an outcome cutter in 7 eyes. Phaco
fragmentation was performed in 9 eyes after floating
the lens on a small PFCL bubble. In the remaining 7
patients, the hard dislocated lens was floated up into
the pupillary space by injecting PFO after a thorough
vitrectomy.
In 22 patients a multiflex open loop ACIOL was
implanted into the anterior chamber under adequate
viscoelastic cover and the limbal section closed with 90
Nylon sutures. The residual PFO was aspirated and a
fundus examination with scleral depression was
performed before closure of sclerotomies.
Intraoperative complications encountered were an
iatrogenic retinotomy in one patient in whom an
intraoperative endolaser barrage retinopexy was
performed, residual retained PFCL and intraoperative
hyphema. Postoperative complications are listed in
Table 2.
Table 2: Post operative Complications
Macular Hole 1 4 %Epiretinal Membrane 4 16 %Macular Degeneration 4 16 %CME 1 4 %OD pallor 1 4 %Residual PFCL 1 4 %ILM folds 1 4 %
Retinal Detachment 1 4 %
15 patients achieved a final visual acuity of > 6/18. A
final visual acuity between 6/24 – 6/60 was possible
in 8 eyes and in 2 patients the final vision was less
than 6/60. Traumatic glaucoma was seen in 1 patient
who achieved adequate control with medical
management. The commonest cause for subnormal
vision was epimacular membrane and post traumatic
macular degeneration. Other caused included cystoid
macular oedema, optic disc pallor, choroidal rupture
and macular ILM folds. One eye developed a total RD
with advanced PVR, 5 years after the procedure. All
22 patients who underwent an ACIOL implant showed
clear corneas and no evidence of corneal endothelial
decompensation.
All patients were followed up and at each followup
visit their best corrected visual acuity, intraocular pressure,
degree of anterior segment inflammation, PAS formation
and macular integrity for presence of CME were assessed.
All eyes maintained good corneal clarity, no evident
anterior segment inflammation or PAS formation.One
patient each developed CME & Retinal detachment.
Discussion
If the crystalline lens dislocation is not associated with
other problems, it does not lead to any complications
on follow-up. The eye can be rehabilitated by contact
lenses or aphakic glasses. However, in some eyes the
dislocated crystalline lens has to be removed because
of some complications.
In general, the indications 5 for removal of a dislocated
crystalline lens includes impaired visual acuity, resulting
from obstruction of the visual axis by the dislocated
lens, development of complications such as phacolytic
uveitis, or glaucoma, retinal detachment, and vitreous
herniation into the anterior chamber resulting in a
cystoid macular oedema. A relative indication for
surgery is severe monocular diplopia.
Surgical techniques: Numerous surgical techniques 6,7,8
have been described for the management of dislocated
crystalline lenses, however, most have been abandoned
because of their limitations, complications and
complexities. The common technique currently used
to remove a crystalline lens dislocated into the vitreous
cavity includes performing a three port pars plana
vitrectomy 9. With this technique a thorough pars plana
vitrectomy with removal of as much of the basal vitreous
gel is performed using vitrectomy cutter The lens is
lifted into the midvitreous cavity and fragmented.
Frequently it may be necessary to crush the lens
between the endoilluminator and the fragmatome into
smaller fragments which can be easily emulsified and
aspirated. This procedure, though easy to perform can
be hazardous in view of the mechanical retinal damage
from falling lens fragments, or due to high energy of
the ultrasonic probe. There is also an added danger of
vitreous traction as the vitreous gets sucked into the
probe, if the vitrectomy has not been completed Retinal
damage is particularly likely to occur if these maneuvers
are performed when the retina is detached and mobile.
Therefore to remove the posteriorly dislocated crystalline
lens safely and effectively, the use of prefluorocarbon
liquids have been recommended 10,11,12. The advantage
of using perfluoro carbon liquid in removing crystalline
lenses dislocated into the vitreous cavity are as follows,

374 Kerala Journal of Ophthalmology Vol. XX, No. 4
Disloc-dislocated, Tr-Traumatic, GRT-Gient Retinal Tear, Vit-Vitreous, AC-Anterior Chamber, VH-Vitreous
haemorrhage, Ret-Retinal, RT-Retinal tear, Chor: Choroidal, SB-Scleral buekh, PPV-parsplana vitrectomy,
PPL-Parsplana lensectomy, C3F
8-perflusopropane gas, LR-Lens removal, AC IOL- Anterior Chamber intraocular
lens, Frag- Fragmatome OD-Optic disc, ERM- Epiretinal membrane, Mac degn -Macular degeneration,
PFCL-Parsflurocarbon liquid, ILM-Internal limiting membrane

December 2008 M. Chakrabarti et al. - Surgical Management of Dislocated lenses 375
1. The perfluoro carbon liquid lifts the dislocated lens
from the retinal surface into the anterior vitreous.
2. In the presence of a retinal detachment, their high
specific gravity mechanically flattens out the retina.
3. The PFCL bubble forms a cushion which supports
the lens and prevents mechanical retinal damage
from falling lens fragments.
Therefore with the use of PFCL, the potential for
retinal damage is reduced. The surgical technique
includes performing a pars plana vitrectomy with
removal of as much basal vitreous gel, prior to lens
removal. After the completion of vitrectomy, PFCL is
injected into the vitreous cavity over the optic disc
floating up the dislocated lens into the anterior vitreous.
If the dislocated lens is associated with a retinal
detachment, the PFCL injection mechanically flattens
the retina against the retinal pigment epithelium,
displacing the subretinal fluid through a pre-existing
inferior retinal break into the vitreous cavity. The
dislocated lens is then fragmented in the anterior
vitreous cavity while floating on the PFCL. Small
fragments of lens matter that drop, float on the surface
of the perflurocarbon bubble and are easily aspirated.
Lens particles can get entangled in the basal vitreous
making its removal difficult. Damage to the peripheral
retina can occur in an attempt to remove these
entangled fragments.
If the dislocated crystalline lens is very hard it is
preferable to remove it through the anterior (limbal
route) using either a cryo or an irrigating vectis 13.
If the eye with the dislocated crystalline lens also has
an associated rhegmatogenous retinal detachment, the
scleral buckle is placed prior to the lens removal. After
removal of the lens, endolaser retinopexy is performed
around the tear and a PFCL air exchange is carried out
to achieve pneumohydraulic retinal reattachment.
Three elements are key to a successful lens
fragmentation techniques 13 are
1. Adequate vitrectomy avoids unintended vitreous
traction during phaco fragmentation.
2. Reducing fragmentation power to only 5 % to 10 %
facilitates nuclear extraction by continuous
occlusion of the suction ports and avoids projectile
fragments. This maneuver also minimizes the risk
of fragments dropping on to retinal surface.
3. Fragments should be aspirated and brought to
midvitreous cavity before ultra sonic fragmentation,
if PFCL is not used.
There are several reports comparing various IOL
fixation techniques in aphakic eyes 14,15,16,17,18. Results
of these studies have conclusively shown that there is
no statistically significant difference between the
various IOL types with respect to postoperative
vision,central corneal thickness and intraocular
pressure. Implanting a multiflex open loop design AC
IOL into the anterior chamber is a viable option provided
there is no corneal endothelial decompensation,
compromised angles or loss of iris tissue.
In this study, all patients with ACIOL implants were
followed us for atleast a minimum period of 24 months.
Corneal clarity, endothelial cell counts, central corneal
thickness, presence or absence of anterior chamber
inflammation, peripheral anterior synchiea formation,
intra ocular pressure, and presence of cystoid macular
oedema were assessed as each follow up visit and found
stable expect for CME in one patient.
Thus successful management of severe blunt injury
involves a thorough preoperative work up, proper
surgical planning and meticulously tailored
postoperative management and follow up.
References
1. William A Townsend; Pico MP; Hilel Lewis MD.
Vitreoretinal Surgery for Ocular Trauma Chapter 117.
2. Higget PE; Pince KJ; Barlow. W et al. Ocular Trauma in
an Urban Population; Study of 1132 cases. Ophthalmol
1992; 97: 581-596.
3. Maguire AM; Enger. C; Elliot et al. Computerized
Tomography in the Evaluation of Penetrating Ocular
Injuries. Retina 1991; (II): 405 -410.
4. Nicholas MH; Brophy D. P et al. Ocular Trauma –
Evaluation with Ultra Sound. Radiology 1995; 195:
423 -427.
5. Lewis H Blumenkraz; Chang. S .Treatment of Dislocated
Crystalline Lenses and Retinal Detachment with
Perfluoro carbons. Retina 1992; 12:299-
6. Demeler. U; Sautter. H . Surgery in Subluxated Lenses
in Adults. Dev Ophthalmol 1985 ; 11 : 162-
7. Illif CE; Kramar. T. A working guide for the management
of Dislocated Lens. Ophthalmic Surg. 1971 ; 2: 251-
8. Urrets; Zavalia. A Displacement of the Crystalline Lens.
Dev. Ophthalmol Vol 59, 1989.

376 Kerala Journal of Ophthalmology Vol. XX, No. 4
9. Hutton W L; Snyder WD; Vaiser A. Management ofSurgically Dislocated Intra Retinal Lens Fragments byPars Plana Vitrectomy.
10. Liu.K; Peyman G.A; Chen. M; Chang.K . Use of HighDensity Vitreous Substitute in Removing PosteriorlyDislocated Crystalline Lens or Intraocular Lenses.Ophthalmic Surg 22: 503; 1991
11. Shapiro M.J; Resnick K. I; Kim. S. H; Weinberg. A.Management of Dislocated Crystalline Lens with aPerfluoro Carbon Liquid. Am. J. Ophthalmol 112; 401;1991
12. Hilel Lewis. MD; German Sanchez MD. The use of PFCLin the repositioning of posteriorly dislocated IOLs.Ophthalmol 1993; 100; 1055-1059.
13. W. Smiddy; H. J. Flynn. Managing lens fragments anddislocated PCL’s after Cataract Surgery. Focal Points:1996
14. Implantation of Kelman Style Open loop AC IOLs duringKeratoplasty for aphakic and pseudophakic bullouskeratopathy – A comparision with Iris Sutured PC IOLs.Ophthalmol 1991; 98:875-880.
15. Richard .M.Davis MD, Douglas Best, Gregory E Gilbert.Comparison of IOL fixation techniques performedduring penetrating Keratoplasty. Am.J.Ophthalmol.111,June 1991:743-749.
16. Oliver.D.Schein MD, MPH, Kenneth.R.Kenyon MD,Roger .F. Steenert MD, et al A randomised trail of IOLfixation techniques with penetrating Keratoplasty.Ophthalmol 1993, 100, 1437-1443
17. Leaming DV. Practice styles and preferences of ASCRSmembers – 1994 survey. J Cataract Refract Surg 1995;21:378-385
18. Lawrence E Weene MD. Flexible Open Loop AC IOLImplants .Ophthalmol 1993, 100; 1636-1639

December 2008 Kerala Journal of Ophthalmology 377
Intravitreal BevacizumabDr. Sonia Rani John DNB, Dr. Meena Chakrabarti MS, Dr. Valsa Stephen MS, Dr. Arup Chakrabarti MS
Angiogenesis is a highly complex, dynamic process
regulated by a number of pro and anti antiogenic
molecules. The vascular endothelial growth factor
(VEGF) and its receptors play a vital role in normal
and pathologic angiogenesis. Activation of the VEGF
receptor pathway triggers a network of signaling
processes that promote endothelial cell growth,
migration and survival from pre existing vasculature,
differentiation, and mobilization of endothelial
progenitor cells from the bone narrow into the
peripheral circulation. In addition, VEGF increases
vascular permeability leading to deposition of proteins
in the interstitium that facilitate the process of
angiogenesis.
There are many ocular diseases in which angiogenesis
plays a major role; for example, proliferative diabetic
retinopathy, age - related macular degeneration
(ARMD), retinal vascular occlusion, sickle cell
retinopathy and retinopathy of prematurity. VEGF has
been identified in neovascular membranes in both
diabetic retinopathy and ARMD and intraocular levels
of the factor correlate with the severity of
neovascularization in diabetic retinopathy. Therapeutic
antagonism of VEGF in animal models result in
significant inhibition of both retinal and choroidal
neovascualrisation as well as a reduction in vascular
permeability 1, 2.
Bevacizumab (Avastin; Genentech Inc, South San
Francisco, CA) is a full length humanized murine
monoclonal antibody against the VEGF molecule. The
amino acid sequence of this monoclonal antibody is
93 % of human origin and 7 % murine 3. Bevacizumab
is approved by the Food and Drug Administration for
treatment of metastatic colorectal cancer in 2004 and
is in phase III trial for advanced breast cancer and
advanced renal cancer. VEGF selectively stimulates
endothelial cells by binding to two receptors, VEGFR -
1 and VEGFR-2, which respond in a typical fashion to
ligand binding by activation of signal transduction
cascades. Bevacizumab can theoretically inhibit the
activity of both receptors.
The labelled indication of Avastin is for the treatment
of colon cancer. Its use in the eye is therefore off-label;
no robust scientific data exist on its safety and efficacy,
all the positive reports have short follow- ups. Off-label
use of drugs is not illegal. Physicians and surgeons are
allowed to do this. The fact that it is a common practice
does not make it safe. There may be a risk of unexpected
adverse outcomes, but this is also true of labelled use
of new drugs.
Bevacizumab is a clear to slightly opalescent, colorless
to pale brown solution with a pH of 6.2. It is supplied in
100 mg and 400 mg preservative free single use vials
to deliver 4 ml or 16 ml of Bevacizumab (25 mg/ ml).
It is formulated in trehalose dihydrate, sodium
phosphate (monobasic, monohydrate), sodium
phosphate polysorbate and water for injection. The
most commonly used dose for intravitreal injection
currently is 1.25 mg (0.05 ml) although upto 2.50 mg
(0.1 ml) may be used 4. The stability and anti VEGF
activity of bevacizumab that was drawn up from the
vial and refrigerated or frozen for later use is currently
not known. The question as to how long the withdrawn
samples can be stored in a syringe, without affecting
the stability of the product, is relevant to our clinicalChakrabarti Eye Care Centre, Kochulloor, Trivandrum - 695 011,
E-mail: [email protected]
O C U L A R
PHARMACOLOGY

378 Kerala Journal of Ophthalmology Vol. XX, No. 4
practices. In addition, as clinical trials are designed, it
is important to maintain consistency between samples
of bevacizumab, to assess its efficacy and establish the
optimum dose for each disease. Studies have shown
that there is minimal change in concentration of
bevacizumab in the samples at 3 months and minimal
further change from 3 months to 6 months. Given the
potential error in accurately dosing 0.05 mL of drug in
a clinical setting, a 10 % change in drug concentration
at 3 months is insignificant. It is interesting to note
that at 3 months and 6 months, bevacizumab in both
the vial and stored syringes degrades minimally. The
manufacturer’s guidelines state that bevacizumab vials
must be refrigerated at 20 C to 80 C ( 360 F to 460 F),
should be protected from light, and should be stored
in the original carton until time of use. The
manufacturer recommends that bevacizumab be used
within 8 hours of being opened when diluted for
intravenous administration and that it should be neither
frozen nor shaken.
While ranibizumab (Lucentis) is derived from
bevacizumab, the 2 molecules have quite different
pharmacokinetics and VEGF–binding affinity.
Ranibizumab (48 K Da) 2 is an antibody fragment
approximately one–third the size of bevacizumab (148
K Da) 3 that penetrated the retina much better than a
full sized antibody after intravitreal injection in
monkeys. In June 2006, the FDA approved Lucentis
for the treatment of patients with neovascular AMD.
Ranibizumab has also been modified to increase 100
times its affinity for the VEGF-A receptor binding
domain. The vitreous and serum half lives of
bevacizumab are much longer than those of
ranibizumab (5.6 Vs 3.2 days ; < 21 days Vs 15 hours
respectively) raising the possibility of both local and
systemic over dosage if bevacizumab is used in the same
way as ranibizumab. Because subretinal
neovascularisation causes breakdown of blood retinal
barrier, it is inevitable that drugs injected into the eye
will appear to inhibit important physiological functions
of VEGF such as wound healing and the formation of
collateral circulations in myocardium and peripheral
vascular ischemia.
The last two years heralded the use of intravitreal anti-
VEGF injections especially the use of intravitreal
Bevacizumab (Avastin) injection in the management
of ocular neovascularization arising from diverse
etiologies. Age Related Macular Degeneration
(ARMD) is a common cause of blindness that has a
pathogenic link to neovascularization. The tell tale signs
of AMD include the presence of drusen, thickening of
Bruch’s membrane and hypo and hyper pigmented
areas of RPE cells. The development of choroidal
neovascular membrane in the form of wet AMD leads
to the growth of incomplete vessels. Leakage from these
vessels cause accumulation of subretinal exudates and
hemorrhages and brings about cell death and reactive
gliosis with severe vision loss. Excellent results of
regression of choroidal neovascular membranes
associated with age related macular degeneration 5, 6
following intravitreal Bevacizumab has been reported
by various authors. Age related macular degeneration
is the leading cause of irreversible vision loss among
the elderly and macular neovascularisation is the most
common cause of severe vision loss 7. Photodynamic
therapy is one current treatment for neovascular AMD
patients with subfoveal neovascularisation. Although
photodynamic therapy (PDT) is superior to placebos
for preventing moderate vision loss in patients with
relatively small minimally classic and occult lesions,
there is little chance of visual improvement in these
patients. Of all the angiogenic factors, VEGF is
implicated as the major stimulus responsible for
neovascularisation in AMD. Once injected into the eye,
the proposed mechanism of action of anti VEGF agents
involve penetration of the drug through the retina
followed by competitive inhibition of VEGF in the extra
cellular space 8.
In a recent off -label study, patients with neovascular
ARMD were treated systematically with bevacizumab
(5 mg/kg) 9. An open label prospective clinical study,
the systemic Avastin for Neovascular AMD (SANA)
study, proposed that systemic (B) could leak from CNV
and blind extra cellular VEGF and that inhibition of
extracellular VEGF could improve visual outcomes.
Systemic (intravenous) bevacizumab was associated
with a significant increase is visual acuity and decrease
in central retinal thickness by OCT 1 week after therapy.
These preliminary results are promising 9. In addition
to the ocular side effects, there were some systemic
disadvantages associated with systemic administration
of bevacizumab; the most significant disadvantage was

December 2008 S.R. John et al. - Intravitreal Bevacizumab 379
the possibility of life threatening adverse events. There
was an increased risk of potentially fatal
thromboembolic events in patients with advanced
metastatic colorectal cancer receiving concomitant
chemotherapy and bevacizumab when compared to
patients receiving chemotherapy alone. Other potential
systemic side effects included hypertension, epistaxis,
hemoptysis, proteinuria, wound healing complications
and gastrointestinal haemorrhage.
Another study has enrolled more than 250 patients to
date for intravitreal Avastin therapy and data for the
first 53 patients with 3 - month follow-up is now
available. The first set of data released in this ongoing
study shows similar efficacy to that of Lucentis with
notably 44 % of patients gaining greater than or equal
to three lines of visual acuity.
The major reservation for the off-label use of Avastin
in treatment of CNV continues to be debate over the
possible systemic side effects. During the initial
investigational studies of Avastin for the treatment of
colon cancer, patients were found to have significant
side effects including increases in blood pressure and
doubling of the risk for thromboembolic events
including myocardial infarctions and cerebral vascular
accidents. Proponents of Avastin contend that those
complication rates were based on systemic administration
of much larger dosages every 2 weeks for upto a year
or longer. The use of Avastin intravitreally with a
substantially lower dose would result in lower systemic
peak levels and monthly dosing would have lower total
dosage, both of which can reasonably be expected to
induce fewer systemic side effects. Moreover, the
reported risk of thromboembolism with Avastin therapy
is based on a cancer population receiving concomitant
chemotherapy, clearly at great risk for such events. An
increase in thromboembolic events has not been
observed in the intravitreal study thus far; however,
further studies are needed to provide more conclusive
data on the safety and efficacy of Avastin. In February
2008, the National Eye Institute (NEI) announced the
start of a multicenter clinical trial to compare the
relative safety and effectiveness of Lucentis and Avastin
to treat advanced AMD.
Recent studies 10 show that intravitreal bevacizumab
leads to rapid regression of iris and angle
neovascularization and should be investigated
thoroughly as an adjunct in the management of
neovascular glaucoma. These studies have
demonstrated the safety and efficacy of intravitreal
Bevacizumab in causing regression of ocular
neovascularization. Kahook MY et al 10 and Davidorf
F H 12 et al have, in 2006, proved the efficacy of intravitreal
Avastin injection as an adjunct in the management of
neovascular glaucoma. In these studies rapid regression
of iris neovascularization and clearing of corneal
oedema occurred within 48 hours giving symptomatic
relief to the patient along with short term IOP control.
Thus IVB as an adjuvant in the management of
neovascular glaucoma may offer a more scientific
rationale for the treatment of the causative neovascular
trigger, might prevent further PAS formation and extension
of secondary angle closure. It also facilitates early
initiation of PRP, further dampening the neovascular
trigger. Prospective randomized trials are required to
validate the efficacy of IVB alone as monotherapy and
its use in conjunction with maximal anti glaucoma
medications, ARC, CPC and cyclo cryotherapy. Long
term results, chances of recurrence and the options to
manage them can only be answered by a prospective
trial in a larger series with longer follow up data.
Recalcitrant diabetic macular edema is
characterized by the accumulation of plaques of hard
exudates in a grossly oedematous retina not amenable
to the standard modalities such as photocoagulation,
intravitreal injection of triamcinolone acetonide or
vitrectomy and showing a very poor visual potential.
These patients usually have a poorly controlled glycemic
status of long duration with associated co-morbid
conditions such as systemic hypertension, dyslipidemia
and chronic renal failure 13. Studies 6 reveal reduction
in central retinal thickness by OCT scan and
improvement in visual acuity in these patients after
intravitreal injection of bevacizumab.
Intravitreal bevacizumab results in significant decrease
in macular edema due to central retinal vein
occlusion 14, 15. Retinal vein occlusion is associated
with increased intravitreal levels of VEGF, particularly
in cases complicated by neovascularisation. Eyes with
CRVO show evidence of intraretinal VEGF mRNA
expression. Inhibition of VEGF by anti sense oligo deoxy
nucleotide or anti VEGF monoclonal antibody resulted
in reduction or complete prevention of iris

380 Kerala Journal of Ophthalmology Vol. XX, No. 4
neovascularisation in animal models of CRVO 16. Since
intraocular injection of VEGF causes retinal
microvascular abnormalities and retinal ischemia, and
since retinal vein occlusion itself causes increased intra
ocular VEGF that varies with disease severity, inhibition
of VEGF in human CRVO has therapeutic potential.
The lack of controlled studies leaves open questions
regarding the safety of intravitreal injection of
Bevacizumab. The literature to date suggests that IVB
is relatively safe in the short term with few severe ocular
and systemic side effects. The systemic risk from
intravitreal injections of drugs in adults are relatively
low because the amount of drug that is absorbed into
the systemic circulation is then diluted substantially
by blood volume. Nevertheless, beneficial cross over
effects have been reported (eg; as a reduction in
neovascularization of the disc in the fellow eye of an
eye that received anti VEGF agent). Published ocular
side effects include uveitis, subconjunctival
haemorrhage, transient blurred vision, vitritis, lid
irritation, ocular discomfort, foreign body sensation,
corneal abrasion, elevated IOP, cataract, posterior
vitreous detachment, endophthalmitis, subretinal
haemorrhage, RPE tears, and retinal detachment 17. Anti
VEGF agents act by reducing angiogenesis and arresting
the CVNM 18. The same pathology of fibrovascular tissue
contraction may be at work in RPE rips following anti-
VEGF therapy. The risk of an RPE rip should be
considered with treatment for anti VEGF agents in cases
with fibrovascular PED. The lack of controlled studies
leaves questions as to the frequency of the various
reported side effects.
Kernt et al 19 measured IOP in 45 patients undergoing
IVB and reported 2 cases of elevated IOP (22 and 28
mm of Hg) immediately following injection, both of
which resolved without therapy. Although the frequency
of elevated IOP after IVB appears to be low, the long
term consequences of transient IOP elevation could be
significant not only for those with already compromised
optic nerves, such as in patients with glaucoma, but
also in terms of risk of vascular occlusive events, such
as retinal venous or arterial occlusion. The mechanism
for acute elevation in IOP has been postulated to be
mechanical, secondary to increased vitreous volume.
If this is the case, in high risk cases one might consider
anterior chamber tap prior to injection. Certain
precautions have to be taken to limit the risks and
complications associated with intravitreal injection of
anti- VEGF agents. So to reduce the risk of
endophthalmitis associated with intravenous injections,
5 % povidone iodine can be applied to the conjunctival
cul de sac. To avoid cataract or possible injury should
the patient move, forceps is used to stabilize the globe
in the region anesthetised before administering the
injection and ensure that the angle of the needle path
into the vitreous cavity avoids the lens. After the
injection, the intraocular pressure is measured and the
patency of central retinal artery (CRA) is checked by
indirect ophthalmoscopy. If there is loss of vision, or
the patency of the CRA is compromised, a paracentesis
has to be performed.
It should be explained to the patients that the drug is
approved for use in the human body, but has either not
been approved by intravitreal route or not for use in
this particular disease. A large scale study has not been
conducted, and therefore the data to support this use
of the agent are limited and also there are small case
series that suggest the agent may be benefit.
Intravitreal bevacizumab did not appear toxic to the
retina in albino rabbits at a concentration of 2.5 mg
based on electrophysiologic studies 20, 21. Maturi R K et
al 12 in his study concluded that intravitreal use of
Bevacizumab resulted in improvement of mf – ERG
macular function responses and relatively stable G -
ERG responses. The macular electrophysiologic
response suggested that macular function improved
with treatment. G -ERG suggested that there is no
significant measurable photoreceptor toxicity with the
use of IVB over short term 22.
The use of intravitreal bevacizumab for the treatment
of chorioretinal diseases mediated by VEGF has spread
throughout the globe in less than six months from the
time of the first case reports. The most obvious reasons
for the rapid adoption of intravitreal Avastin include
the rational scientific basis of treatment, the
overwhelming efficacy reported for the closely related
drug known as Lucentis (Ranibizumab, Genentech Inc),
the presence of an enormous unmet need to prevent
blindness from VEGF–mediated diseases, the visual
acuity and anatomic improvements appreciated by
patients and treating physicians, the apparent short
term safety and the affordable low cost of the drug.

December 2008 S.R. John et al. - Intravitreal Bevacizumab 381
Neovascularization is a key pathophysiologic mechanism
of a wide variety of diseases, making the factors that
mediate angiogenesis an attractive therapeutic target.
Although the brunt of clinical research in the inhibition
of ocular neovascularization has been on CNV related to
AMD, researchers are exploring the potential for benefit
from the utilization of these drugs in other diseases
such as diabetic retinopathy, vascular occlusion, and
macular edema. While the gamunt of retinal and
choroidal neovascular diseases varies greatly, the
common source of pathogenesis, incompetent vessels and
the compromise of the blood retinal barrier, has
provided for significant advancement in the treatment
of these diseases. Despite all the advancements in
treatment discussed here, the collection of ocular
diseases caused by neovascularization continues to
create significant morbidity among patients.
References
1. Aeillo LP, Pierce EA, Foley ED, et al. Suppression ofretinal neovascularisation in vivo by inhibition ofvascular endothelial growth factor (VEGF) using solubleVEGF receptor chimeric proteins. Proc Natl Acad SciUSA 1995;92:10457-10461.
2. Quam T, Xu Q, Joussen AM, et al. VEGF initiated blood-retinal barrier breakdown in early diabetes. InvestOphthalmol Vis Sci 2001; 42:2408-2413.
3. Sophie J.Bakri, MD, Melissa R, Snyder. PhD, et al. Sixmonth stability of Bevacizumab (Avastin) binding tovascular endothelial growth factor after withdrawal intoa syringe and refrigerator or freezing.Retina 26:519-522, 2006.
4. Rosenfeld PJ, Schwartz SD, Blumenkranz MS, et al.Maximum tolerated dose of a humanized anti-vascular
endothelial growth factor antibody fragment for treatingneovascular age-related macular degeneration.
Ophthalmology 2005; 112:1048–1053.
5. Rosenfeld P J, Moshefeghi A et al. OCT findings after
intravitreal Bevacizumab (Avastin) for neovascular agerelated macular degeneration. Ophthalmic Surg LasersImaging 2005; 36:331-5.
6. Haritoglou C, Kook D, Neubauer A, Wolf A, Priglinger
S, Strauss R, Gandorfer A Avery R L, Pieramici D J,Rabena MD et al. Intravitreal Bevacizumab (Avastin)for neovascular age related macular degeneration.
Ophthalmol 2006; 113: 363-372.
7. Rosenfeld PJ, Moshfeghi AA, Puliafito CA. Opticalcoherence tomography findings after an intravitrealinjection of bevacizumab (Avastin®) for neovascular
age-related macular degeneration. Ophthalmic SurgLasers Imaging 2005; 36:331–335.
8. Avery RL, Pieramici D, Rabena M, Castellarin A,Nasir M, Giust M. Intravitreal bevacizumab (Avastin)for neovascular age-related macular degeneration.Ophthalmology 2006.
9. Michels S Rosenfield PJ, Puliafite CA. Systemic
Bevacizumab therapy (Avastin) for neovascular ARMD,
12 week results of an uncontrolled open- label study.
Ophthalmology 2005; 112: 1035-1047.
10. Milko E, Hiev, Diego, Domig MD, Intravitreal
Bevacizumab (Avastin) in the treatment of Neovascular
Glaucoma. Am J. Ophthalmol 2006; 142:1054-1056.
11. Haritoglou C, Kook D, Neubauer A, Wolf A, Priglinger S,
Strauss R, Gandorfer A, Ulbig M, Kampik A. IVB
(Avastin) therapy for persistent diffuse diabetic macular
edema. PMID: 17151486 [PubMed - indexed for
MEDLINE]
12. Maturi R K, Bleau LA, Wilson DL, Retina 2006 Mar;
26 (3): 270-274.
13. Reichel E. Intravitreal bevacizumab for choroidal
neovascularization and cystoid macular edema: a cost-
effective treatment? Ophthalmic Surg Lasers Imaging
2005; 36:270–271.
14. Ip MS, Gottlieb JL, Kahana A, et al. Intravitreal
triamcinolone for the treatment of macular edema
associated with central retinal vein occlusion. Arch
Ophthalmol 2004; 122: 1131–1136.
15. Pe’er J, Folberg R, Itin A, et al. Vascular endothelialgrowth factor upregulation in human central retinalvein occlusion. Ophthalmology 1998; 105:412–416.
16. Tolentino MJ, Miller JW, Gragoudas ES, et al.Intravitreous injections of vascular endothelial growthfactor produce retinal ischemia and microangiopathyin an adult primate. Ophthalmology 1996; 103:1820–1828.
17. Lynch SS, Cheng CM. Bevacizumab for neovascularocular diseases. Ann Pharmacother 2007; 41:614-25.
18. Adamis AP, Shima DT. The role of vascular endothelial
growth factor in ocular health and disease. Retina 2005;
25: 111-118.
19. Kernt M, Nuebauer A S, Kampila a. Intravitreal
Bevacizumab (Avastin) treatment is safe in terms of
intraocular and blood pressure. Acta Ophthalmol Scand
2007; 85: 119-20.
20. Loewenstein A, Zemel E, Lazar M, Perlman I. Drug-
induced retinal toxicity in albino rabbits: the effects of
imipenem and aztreonam. Invest Ophthalmol Vis Sci
1993; 34:3466–3476.
21. Han DP. Intravitreal human immune globulin in a rabbit
model of Staphylococcus aureus toxin-mediated
endophthalmitis: a potential adjunct in the treatment
of endophthalmitis. Trans Am Ophthalmol Soc 2004;
102:305–320.
22. Hood DC, Birch DG. A computational model of the
amplitude and implicit time of the b-wave of the human
ERG. Vis Neurosci 1992; 8:107–126.

382 Kerala Journal of Ophthalmology Vol. XX, No. 4
High-End Phaco Systems: A ComparisonDr. Ashley Thomas Jacob MS DNB MRCOphth
High End Phaco: Excellence at your finger
tips
There are several high end phaco designs available in
the market today. I have ventured to analyze only those
that offer some value and uniqueness that would help
the individual surgeon in bettering his technique and
enable superior marketing of his surgical unit.
In this issue, the spot light is on three designs that have
superior degree of innovation and have dominated
scientific meetings in US, Europe and in India.
Oertli Os3
Country of Origin: Switzerland
Website: www.oertli-instruments.com
Sold & Serviced by: Toshbro Medical Equipments
Oertli has been a leader in innovative concepts that
are rarely well marketed in India. The quality of its
product range has been never justified by the various
distributors handling its products. This has been the
failure of an otherwise exceptional product.
Oertli has several innovations to its name like the 6-
crystal Handpiece, Co-MICS (coaxial micro phaco), dual
linear foot pedal, etc.
User Interface: Large LED display and push button
control &Audio. The display unit is a dated design that
cries out for change.
I/A System: The OS3 fluidics system comes with the
TwinVac cassette (250ml) and integrated pressure
sensor. The cassettes are available as single use or
autoclavable and these can be emptied.
Venturi and peristaltic double pump switchable (from
pedal, remote control or panel) during surgery with
the dual function cassette that supports both pumps.
Air free fluidics system: The absence of air in the
aspiration path has multiple advantages like immediate
response to pressure changes, instant build up of suction
power and stable anterior chamber.
Oertli claims to employ an AC Guard system that eliminates
vacuum surges completely even at highest levels of
vacuum. The company says that there is no possibility
of contaminations from pressure sensor as pressure is
sensed without contacting the aspiration liquid.
Reflux function is selectable, from bottle or with pump
reverse (150ml).
Ultrasound Phaco: Six-Crystal Design Phaco hand
piece.
CMP - cool phaco mode for bimanual cool micro incision
phaco.
Bipolar Klöti RF-capsulotomy: This form of
capsulotomy is unique to Oertli designs.
Anterior Segment Vitrectomy: Single use
guillotine cutter with selectable cutting rate of upto
1200cuts/minute. Extendable to Vitreoretinal Surgery
Dual Linear Pedal: The programmable dual linear
pedal is equipped with its own controller. Not only can
you assign preferred functions to the various pedal
elements, you can also individually set the position
points and the resistance at the position points.
*Skill Enhancement needed: NONEMulamoottil Eye Hospital, Kozhencherry
O P H T H A L M I C
INSTRUMENTATION

December 2008 A. Thomas - High end phaco systems 383
Alcon Infiniti
Country of Origin: USA
Website: www.alconlabs.com
Sold & Serviced by: Alcon India
Alcon has consistently provided surgeons with
innovative technologies in the field of cataract micro
surgery. Although expensive to purchase and maintain,
the quality is unmistakable. The groundbreaking Legacy
is a case in point. Now, with the Infiniti, we have a
worthy successor.
The Infiniti has several innovations like the Ozil
Torsional Phaco, AquaLase system, and Alcon’s own
version of the micro phaco (Intrepid).
User Interface: Touch screen & Audio
I/A System: Alcon calls it the Fluidic Management
System.
Alcon claims that the FMS has a low-compliance (rigid)
design with molded fluid paths and thick-wall polymer
aspiration tubing that decrease post-occlusion surge and
increase fluidic response and accuracy.
The pump mechanism has tapered rollers designed for
instantaneous, smooth peristaltic response and has
greater pumping capability, with forward and reverse
actuation up to 100cc per minute.
Ultrasound Phaco: OZil Torsional Handpiece:
The hand piece delivers side-to-side oscillating
ultrasonic movement. With virtually no repulsion, it
delivers a level of followability that is unmatched.
Torsional phaco utilizes ultrasonic oscillatory movement
that can benefit lens removal for all lens densities. The
unique movement of torsional phaco shears the lens
material, providing decreased repulsion (no jack hammer
effect) while improving the thermal safety profile over
traditional ultrasound. There are multiple surgical
benefits to decreased repulsion: increased followability,
reduced turbulence, and increased cutting efficiency.
Side-to-side movement delivers increased cutting
efficiency by emulsifying lens material with both
directions of movement which has the potential to
reduce fluid usage and increase your surgical efficiency.
Less frictional movements within the incision and lower
frequency (32kHz) reduce the risk for thermal injury
thus allowing the use of sealed incisions and continuous
torsional modes increasing surgical efficiency.
The design facilitates the emerging trend of micro-
coaxial phaco.
The titanium hand piece with 4 crystals weighs only
60 grams.
AquaLase Liquefaction Device: The innovative
AquaLase Liquefaction Device offers an alternative to
ultrasound in soft to medium density cataract lenses
while claiming reduced surgical complications.
Warmed pulses of BSS sterile irrigating solution are
delivered through a smooth polymer tip to delaminate
and separate lens tissue. Each pulse is only 4 mL and is
delivered in a “scoop-like” energy pattern. The smooth
capsule-friendly tip is designed to improve your ocular
safety with a “more in the bag” technique. The fluidic
pulses are individually made and delivered with no
mechanical motion of the tip and the pulse energy
density is quickly dampened within the fluid of the
anterior chamber, reducing risk to surrounding tissue.
AquaLase allows change of pulse strength by altering
volume and velocity; vary pulse rate, and activate burst,
with variable rest intervals and decreased repulsion of
nuclear material.
INTREPID Micro-Coaxial System: Micro-coaxial
System delivers a complete micro-incision solution,
allowing the surgeon to perform surgery safely and
efficiently through a single incision without altering
the normal technique.
*Skill Enhancement needed: Since the Ozil works
only with the Kelman tip, the surgeon would have to
devote time to re-train himself if used to working with
straight tips.
AMO Whitestar Signature
Country of Origin: USA
Website: www.amo-inc.com
Sold & Serviced by: AMO India
User Interface: Touch screen & Audio
I/A System: AMO calls it the Fusion Fluidics. It claims
to provide increased chamber stability and safety by
anticipating intraocular changes and proactively

384 Kerala Journal of Ophthalmology Vol. XX, No. 4
adjusts, so chamber stability is never compromised -
even at higher vacuum and flow settings, with any
technique, on any lens type.
The Fusion Fluidics surge-prevention technology allows
the use of high vacuum and flow settings to reduce
phaco time and increase efficiency while improving
chamber stability by anticipating occlusions and
preemptively adjusting vacuum before occlusion breaks.
The system has the ability to switch between a true
peristaltic pump and true venturi pump on-the-fly.
During a procedure, the surgeon can switch instantly
into venturi mode for additional vacuum and holding
power. This capability can be extremely useful in
teaching institutions, allowing the flexibility to use both
modalities in one system.
WHITESTAR ICE Technology
Cavitation is a recognized source of ultrasonic cutting
power. When bubbles strike, high energy manifesting
as a localized implosion destroys nuclear material.
WHITESTAR ICE Technology is designed to maximize
the cavitational potential of phaco energy to optimize
surgical technique
Theoretically, an initial punch at the beginning of each
ICE Pulse allows gas-rich BSS to flow between the phaco
tip and cataract material, acting as a transient cavitation
accelerator
The ICE Pulse amplitude punch can be from 0% to 12%
of total pulse power and can be set to increase, decrease
or stay constant in each phaco setting.
Ultrasound Phaco: Ellips Transversal
Ultrasound
The Signature System now comes with Ellips
Transversal Ultrasound as an answer to Alcon’s Ozil.
To work around Alcon’s patent, the longitudinal and
transversal ultrasound has been simultaneously
blended. This, AMO claims, has been designed for
efficient cutting that doesn’t require a change in
technique and works with any tip style—straight or
curved. And it’s true! There is no skill enhancement
required unlike with Ozil.
The system is optimized with Micropulse Technology
for followability and to minimize the risk of thermal
damage.
*Skill Enhancement needed: NONE
Conclusion
Buying a High End phaco system involves a lot of
money. So it is wise that such a decision is reached
after careful deliberations on the feasibility of such an
investment. The bare truth is that the purchase is most
often made to satisfy one’s own ego (which is important,
but cannot be the sole point on which to base the
purchase).
The purchase would be deemed financially viable if
the surgeon would be performing a minimum of 30
cases a month. As with any surgical unit, break even
has to be achieved by 12-18 months.
Alcon Infiniti would be a good buy if considered purely
on the merit of the investment. The unit has a fairly
good number of installations and has proved to be
largely trouble free. AMO Signature with Ellips would
come a close second losing out on the number of
installations. Oertli would raise concerns on the
distributor’s ability to sustain the unit and their
distributorship which could change hands.
Whatever your choice, it has be complimented by good,
ethical in-house marketing activities.
(To be continued)

December 2008 A. Thomas - High end phaco systems 385
Spectacles- What We Do Not KnowDr. Bindu N. Das MS DO MBA(HM)
Introduction
Spectacles is a common, cheap and easy method of
prescribing corrective lenses in patients with refractive
errors and presbyopia.
Working knowledge about spectacle lenses , frames and
process of dispensing will help an ophthalmologist to
give exact instructions to the optician. This will go a
long way in ensuring patient satisfaction with glasses.
What is a Spectacle?
Spectacle is defined under British standard as an optical
appliance comprising lenses and a frame with sides
extending towards ears (Fig 1).
I .Spectacle Frames
A. Parts of a Spectacle frame
Each frame has two main parts - Front & Side.
� Front consist of rims, bridge,joints and lugs.
� Rims
May be complete or incomplete or full rim, rimless(3ps)
and half rim(supra)
Lenses are supported by nylon or steel wires.
� Bridge
Is that part of front which forms the connection between
two rims (Fig. 2). Bridges may be of three basic types
1. Regular:-it rest on the nose with full surface in
contact.
2. Insets bridge/Keyhole:-Projects behind the frame
plane so that area of contacts has behind the lenses
plane.
3. Saddle Bridge:-Combination of regular and insets
bridges. It mainly distributes the weight of
spectacles on top as well as side of nose.
4. Modified saddle bridge
5. Adjustable nose pads:-Allow for good fit.
Different types of bridges
� Lugs: Projection on sides to which side pieces are
attached.
� Side Pieces / Temples are the principal parts
that fix spectacles to ear. They are made up of
metals and plastic in combination.
B. SPECTACLE FRAME MATERIALS
An ideal spectacle material must be durable , adjustable,
non allergic, non inflammable, non corrosive and
preferably of low cost.
� Plastic frames � Shell frames
� Nylon frames � Metallic
� CombinationRegional Institute of Ophthalmology, Calicut
Fig. 1. Parts of a Spectacle
O P H T H A L M I C
INSTRUMENTATION

386 Kerala Journal of Ophthalmology Vol. XX, No. 4
a) Plastic Frames:-Thermoplastic material is are used
usually as these can be heated and cooled without losing
their plasticity. Cellulose acetate, Cellulose nitrate,
Cellulate propionate, Perspex(Synthetic acrylic resin-
PMMA),Epoxy resins are examples
b)Shell frames:-Made from shell of Hawks bill turtle
found in West Indies and Seychelles. They are durable,
have attractive colours and mottling and are easy to
maintain.
c) Nylon:-were used in making spectacles for children
where chances of breaking were high.
d)Metallic frames:-These are stable, quite adjustable,
non inflammable and non allergic (except nickel) and
pleasing. They are inexpensive and can be mass produced.
Variety of materials like stainless steel, nickel, silver
(German Silver), anodized aluminum, gold, titanium
and memory metal are used for making frames.
e)Combination frames
C. FRAME STYLES
Spectacle frames are available in different styles. They
include Full Frame, Combination Frame, semi rimless
and Rimless (Drill mount).
D.FRAME SELECTION
Correct fit and selection of frames is an essential part
of accurate dispensing. Frames must be rigid, strong,
and light and must be comfortable for the wearer.
Points to be taken into account:- (Fig. 3)
- Temporal hairline margin distance
- IPD
- Shape of the face
- Physical features of face.
- Nose bridges and suitable side arms.
- FTB
- Pantoscopic tilt
- Fitting triangle
Computer software programs are available by which
we can match the facial form with different type of
spectacle styles and select the suitable frames.
FTB: Distance between back surfaces of the front to
the ear. Too large FTB will cause the frame to sag.
Pantoscopic Tilt:-Lower end of the frame is tilted
backwards towards the face. In this way optical center
of spectacle lenses coincides with the fixation axis. This
is needed because, most of the time eyes are looking in
downward direction.Pantoscopic tilt reduces chromatic
aberration of a high power lens and has better cosmesis.
Fitting triangle:-is an important criterion of good
fit.Properly fit frames should touch the patient in only
three places – bridge and the top of each ear.An
imaginary line drawn from each point of contact with
the wearer’s face results in an triangular shaped form
and this is called as “Fitting triangle” (Fig. 4).
II SPECTACLE LENSES
Spectacle lenses consist of a transparent material that
has two polished opposing surfaces with ability to focus
light rays in an expected manner.For proper
understanding of the requisite features of lenses, one
needs to be familiar with critical properties like
Fig. 2: Different types of bridges
Fig. 3. Points to be taken into account before dispensingspectable frames

December 2008 B.N. Das - Spectacles 387
refractive index, dispersion expressed by Abbe value
and specific gravity.
Refraction: Bending of light when it passes from one
medium to another.
Power : Power of an ophthalmic lens is determined
by the difference between the front and back curve of
the lenses expressed in dioptre.
Refractive index: is the ratio of velocity of light in
vacuum to the velocity in a given medium at a given
wave length.
Increasing the refractive index reduces the edge
thickness of minus lens and centre thickness of a plus
lens. The volume of the material is reduced and also
we get flatter surfaces.
Specific gravity: is the ratio of the weight of a
substance to the weight of water with the same volume.
A high index lens will be heavier due to high specific
gravity.
Abbe value: indicates the ability of a lens material to
refract white light without chromatic aberration. Abbe
value runs between 1 and 100. Higher the Abbe value
the better but only upto a point. Abbe value of the
human eye is 45,hence it becomes difficult to perceive
above this value. Optimum Abbe value is necessary for
optical efficiency of a lens.
Optical center: of a lens is the position along the
optic axis where no prismatic effect is found.
Visual axis: is an imaginary line from an object of
fixation in the field to the fovea. The best and least
distorted image is obtained when optic centre matches
the visual axis.
A. Types of Spectcle Lenses
a. Can be classified as spheres, cylinders, and prisms.
b. Can be grouped based on choices of lenses.
1. Single Vision
2. Bifocals
3. Lenticular
4. Aspheric
5. Multifocals/Progressives
c.Can be grouped based on the purpose for which they
are given
1. Optical Purposes
2. Sunglasses
3. Vocational Spectacles
- Half eye reading
- Safety spectacles
- Swimming goggles
- Spots glasses
- Driving mask
- Computer glasses
- Welding goggles
- Lorgnette, quizzer
(held before eyes by a handle)
B. Lens Materials
Lenses like frames are made up of a variety of materials.
Common materials:-
Glass, plastics.
Special Materials:
-Poly carbonate
-Hi-index lenses
-Trivex
An ideal ophthalmic lens material should satisfy several
parameters and requirements.
Visual requirement:-Abbe value and other visually
related concerns are to be considered.
Cosmetic:- should be cosmetically acceptable to the
wearer - “People should see the wearer’s eye than the
glasses”.
Safety:-particularly for children, individuals involved
in sports, special jobs and monocular individuals.
Health:-In terms of UV and other occupational
hazards.
Fig. 4. “Fitting Triangle”

388 Kerala Journal of Ophthalmology Vol. XX, No. 4
1. Glass
Crown glass :-with RI of 1.5223 is used mostly
Abbe value 58.5. They are highly transparent, scratch
resistant and low cost but they are thick, heavy and
can break easily
Flint glass:-has high RI of 1.62. Due to high specific
gravity and low abbe value, flint glass has the
disadvantage of being heavier and has high chromatic
aberration.
2. CR 39 (Columbia resin)
Chemically it is allyl digtycol carbonate and was created
by chemists at Columbia Southern Corporation in 1942.
39 indicates that the 39th test resin produced by the
company was successful
RI 1.498, 1.58, 1.6, 1.74. As it is a thermosetting
material it can be ground and polished after
manufacturing without risk of deformity.
Advantages:-
a. Good optics and chemical resistance.
b. Comfortable due to light weight.
c. Safer than glass lenses.
d. Unlimited designs,coating and tinting.
e. Photo chromatic options available.
Disadvantages:-
a.Poor structural integrity
b.Unstable at high temperature
c.Scratches more easily
d.More expensive
e.Not suitable for rimless frame as they can wreck.
f.Difficult to drill without cracking
3. Polycarbonate Lenses
RI 1.586 is an amorphous material and is the lens of
choice when safety is an issue.
Advantages:-
a. Thinner as they have high refractive Index.Centre
thickness can be ground to 1.2 mm.
b. Lighter (26% Lighter than CR 39) due to low
density.
c. They can bend easily without getting deformed
therefore they have got high impact resistance.
d. Has built in UV protection.
e. Bullet proof.
Disadvantages:-
a. Soft so very low scratch resistance.
b. Tinting not possible.
c. Cause peripheral chromatic aberration in high
minus power.
d. Low abbe value and needs ARC.
It is the lens of choice in children, athletes and people
working in industry.
4. Hi-index Lenses
Are made of denser materials than conventional
materials. They are available in plastic resin(Mitsui
Resin-MR-8, MR-10, MR-11) and glass. They can be
made thinner hence useful in high powers. RI - 1.6,
1.7, 1.8, 1.9. They can be anti reflection coated.
Disadvantages:
a) Not necessarily lighter even though thinner.
b) Costly.
c) Low Abbe value.
d) ARC is a must.
5. Photochromatic Lenses
Has the property to change the colour when the sunlight
or UV light strike the lens surfaces .They are also called
variable tint/Day and Night /Transition lenses.
The darkening process takes as little as 45 seconds but
the reverse lightening process takes up to 20 mts. For
this reason it is not advisable to prescribe them as a
routine.
Photo grey (PG) photo brown (PB), Photopink (PP)
are the available colours. They are available in glass
and plastic. They provide UV protection and some relief
from glare.
6. Trivex (Trilogy) – (Essilor)
This is an alternative to polycarbonate lenses.TRIVEX
material has good optics and inherent UV protection.

December 2008 B.N. Das - Spectacles 389
Antireflective coating and Scratch resistance coating
can be done. Tinting is possible. It has less chromatic
aberration compared to polycarbonate lenses. They are
the lightest lens available, are unbreakable and resistant
to chemicals. Easy drilling and mounting is possible
hence it is the ideal material for rimless spectacles. Abbe
value of human eyes and Trilogy is 45 which is the
reason for its excellent clarity.
III) LENS ENHANCEMENTS
� UV protection
� Scratch resistance coating (SRC)
� Anti reflection coating (ARC)
� Tinting
� Hydrophobic coating
UV Protection:
In the electromagnetic spectrum we are capable of
seeing wavelengths between 400nm-760nm
(VIBGYOR). Rays above 700 and below 400nm are
harmful to the eyes.
UVC (250-286), are filtered by Ozone layer of earth
UVB (286-320nm) are primarily absorbed by cornea
and can lead to snow blindness, photokeratitis etc,
UVA (320-40nm) are absorbed by crystalline lens and
cause cataract.
Plastic lenses are treated chemically for obtaining UV
protection.
Scratch Resistance Coating (SRC)
Done to prevent easy scratching of plastics. This clear
coating hardens to provide a durable, tougher lens.
Scratch resistant does not mean scratch proof.
Anti Reflection Coating (ARC)
This reduces reflection from the surface of lens and
increase transmission of light. Maximum transmission
gives maximum clarity. This helps to eliminate “shop
window” effect and road blindness (temporary
blindness caused by high beam head lights of oncoming
vehicles). It also reduces eye fatigue in artificially
lit environment. Available in yellow, green and blue
colour.
Hydrophobic Coating:
Is a water resistant coating which prevents staining and
smudging on the lens surface making it easy to clean.
Essilor Crizal Alize and TMC Satin (Titanium Multi
Coating with Satin) are examples of superior ARC with
hydrophobic properties.
Tinting:
Can cut the amount of light that reaches your eyes and
provide relief. Lenses can be tinted in a solid pattern,
meaning entire lens is tinted the same colour or they
can be tinted in a gradient pattern. Several tints like
pink, brown, grey, green, blue etc are available.
Drive Wear Technology: combines ARC,UV
protection and tinting effectively. In addition to glare
and excessive light protection, drive wear enhances red
and green traffic signal recognition. It blocks 100 %
UV light also. They are available as prescriptions for
plano, single vision and as progressives.
IV) Lenses For Correction of Presbyopia
Single vision lenses: Corrects for one focal length.
ie., for distance or near only.
Bifocal lenses – correct vision at two distances ie
Distance and near
Can be kryptok bifocals, or as Univis / D bifocals
Disadvantages : No clear vision for intermediate
distance, has a disturbing dividing line and has “image
jump”.
Progressive Lenses: These are aspheric lenses in
which power gradually changes from distance
Fig. 5. Demonstrates the beneficial effect of anti refractivecoating

390 Kerala Journal of Ophthalmology Vol. XX, No. 4
correction at the top through intermediate powers to
the near prescription at the bottom of the lens.
Progresssive design
Advantages:
a) No lines in the way of vision
b) Convenience of having a single pair
c) Available in a variety of materials
progressives.It is available in general & customized
designs.
Customized designs- have no preconceived design.
They utilize each patients unique head and eye
movements which are measured using a device called
“Vision Print System” for optimal visual
performance.eg:varilux ipseo, rodenstock pure life, sola-
1etc
Occupational Progressives: are multifocal aspheric
progressives, designed for both near and intermediate
vision. The lower half is for NV correction and upper
half for mid range vision upto 2.5 metres.
They are an ideal solution for CVS as computer users
benefit from a natural head and neck position, and form
a wide intermediate area for computer use.
Eg: AO compact, Zeiss RD, Panorama Mini, Essilor
Ellipse, Kodak Precise
Spectacles for Kids:
- Choose colourful/trendy/sturdy frames
- Not unisex, separate for boys / girls
- Give special attention to frame material, nose bridge,
nose pads, hinges etc. High quality spring
temples,silicone nose pads,elastic straps etc are good
options
- Lens material can be CR39 or Polycarbonate
- Use aspheric design
- Provide SRC, ARC and avoid tinting
- The lens should cover the eyes
Points to be considered in lens fitting:
1. Vertex Distance - Should be specified for higher
prescription.
Pupillary alignment : Pupils should be close to the
optic centre of each lens to take full advantage of
refractive correction given.
2. IPD : Interpupillary distance should be measured
both for distance and near.
3. Fitting plane of lenses – lenses should be in a plane
perpendicular to the visual axis, ideally fitted
15.7mm in front of cornea which corresponds to
Suitable for people who have intermediate
requirements like Computer use, typist etc.
Disadvantages:
a) Peripheral distortion (Swimming & Swaying effects)
b) Narrow field of view
c) Expensive
d) Needs adaptation period
Different companies have come forward with newer
designs which offer wider field of vision & binocular
vision, short corridors, smooth transition and easy
adaptation Eg: Varilux Panamic, Solamax from SOLA,
Concise from KODAK, Internal Progressives from SEIKO,
Progressive Life series from Rodenstock and
Progressives from NOVA.
Internal Progressives are backside progressives –
providing expanded field of vision, wider near vision
and considerable reduction in distortion. Eg; Seiko,
Nova.
Wave front assisted PALs : wavefront analysis used
in LASIK and astronomy is used to detect and eliminate
high order aberrations inherent in conventional
Fig. 6. Progressive lens

December 2008 B.N. Das - Spectacles 391
anterior principal focus, but practically fitted as
close to the eye as possible.
4. Optical centres: Marking is very important for
proper fitting as it should coincide with visual axis.
Hold the lens against a cross line chart horizontally
or vertically and move until one gets an unbroken
cross
Conclusions
Spectacles still form a major share in optical correction
of refractive errors and presbyopia. Wider choices are
available in frames and lenses. Selection depends on
taste and budget of the patient, occupational condition
and requirement – Finally the wearer should see
well and look good.
References
1. Theory and Practice of Optics & Refraction, AK Khulana
2. Ophthalmic Prescription Work, Arthur G Bennet.
3. Spectacle Glass Technology, Horne DF, Adam Hilger andBristol.
4. Fannin TE & Grosvenor T. Clinical Optics. Aberrationsand Ophthalmic Lens Design.
5. T.B. of Ophthalmology, Vol.I, Optics & Refraction., auser friendly guide. D.Miller, S.Podos, M.Yanoff, 1991.
6. Duke Elder, Practice of Refraction.
7. Optician’s guide-Ajay kumar bhootraFig. 7. Measurement of Interpupillary distance
Fig. 8. Marking of optical centre of the lens

392 Kerala Journal of Ophthalmology Vol. XX, No. 4
Management of Dislocated PC IOLDr. Meena Chakrabarti MS, Dr. Valsa T. Stephen MS, Dr. Sonia Rani John DNB, Dr. Arup Chakrabarti MS
Inadequate posterior capsular support or zonular
rupture may allow IOL decentration or dislocation.
Decentered IOLs may occur in 0.2 % to 1.2 % of cases
postoperatively 1. The specific cause of the displacement
may not be always evident 1,2.
Various mechanisms include the following
1. Inadequate posterior capsular support due to
posterior capsular rent.
2. Zonular rupture.
3. Accidental placement of IOL through posterior
capsular rent into the anterior vitreous face.
4. Late haptic rotation out of a zone of thin capsular
remnant.
The cause of late spontaneous IOL rotation is
unclear 3,4. It may follow accidental changes in position,
gravitational effect, accidental finger rubbing or other
contact with the eye. Late dislocation of the IOL can
occur spontaneously or following trauma.
Generally posterior chamber IOL placement is safe if
at least 180 degree of the capsular remnant is intact 5.
More extensive support is necessary if the capsular
remnant is missing inferiorly or if the capsular margin
on which the haptics are to be positioned is inadequate.
Indications for subsequent surgery 3,4,5: The
indications for surgical removal include decreased
visual acuity, chronic intraocular inflammation, retinal
detachment and vitreous in the cataract wound
associated with cystoid macular oedema. Although a
dislocated IOL may be well tolerated for a considerable
period of time by some patients, visual rehabilitation
is usually difficult and surgical intervention may become
necessary.
Surgical Technique: For a subluxated IOL 6,7,8
associated with symptoms, surgery may be performed
by a limbal or parsplana approach. In patients with
less extensive subluxation and posterior capsule that is
intact for most of its part, repositioning can be done
via the limbal route, after minimal or no anterior
vitrectomy. However, in the presence of a sizeable
posterior capsular rent, or posterior dislocation of the
IOL into the vitreous cavity, a parsplana approach is
prefered to acheive the goals of surgery 1. A thorough
preoperative assessment of the posterior capsular
integrity is necessary to plan the surgical procedure.
The first step of the procedure is to bring the dislocated
IOL into the anterior vitreous in the plane of the pupil.
Fig. 1. After completion of the vitrectomy, injection of
perfluorocarbon liquid between the retina and theintraocular lens, floats the dislocated intraocular lensoff the retina.
Chakrabarti Eye Care Centre, Kochulloor, Trivandrum - 695 011,
E-mail: [email protected]
OPH TH A LM I C
S U R G E R Y

December 2008 M. Chakrabarti et al. - Management of Dislocated PC IOL 393
This is achieved after a complete vitrectomy and release
of vitreous adhesions to the IOL. The IOL is then lifted
off the retinal surface using foreign body forceps or
with the help of perflurocarbon liquids (fig 1).
Late spontaneous in - the - bag intra ocular lens and
capsular tension ring dislocation 9,10 has been reported
in pseudoexfoliation syndrome. Capsular tension ring
implantation in “pseudoexfoliation associated zonular
weakness” does not guarantee long term zonular
stability and capsular bag / IOL positions. In these
patients, parsplana vitrectomy, perflurocarbon liquid
injection to lift up the CTR-IOL-CB complex, grasping
this complex with forceps and bringing it to the
pupillary space transfer across pupil, and with a Mc
Phersons forceps the complex can be explanted through
the cornea scleral incision as a single unit.
Alternatively after PFCL injection 11,12, the vitrectomy
cutter is used to cut the capsular bag after supporting
it with an illuminated hook followed by removal of the
CTR and IOL separately through a smaller scleral
tunnel.
Once the PC IOL is in the pupillary plane depending on
the integrity of the capsulozonular remnant there are
three options available to the surgeon. These
include 1,2,
1. IOL repositioning.
2. IOL explanation
3. IOL exchange.
IOL Repositioning: is performed when adequate
capsulo zonular support is present. The lens may be
repositioned without sutures on to the residual posterior
capsule or fixated by sutures to the iris or the sclera.
Surgical success depends on accurate placement of the
haptics into the ciliary sulcus and this requires
visualization of the residual posterior capsule.
In patients with insufficient pupillary dilatation iris
hooks or retractors may be used to allow a more
accurate assessment of the posterior capsule. Since
the use of capsulorhexis has become wide spread,
the peripheral anterior capsule is left intact and
frequently serves as adequate support for the
sulcus fixation of the dislocated PC IOL. Repositioning
of a posterior chamber IOL into the anterior chamber
has also been reported, but this approach is not
recommended due to chronic chafing of the iris by
the IOL.
IOL removal and or exchange options 13 are
usually exercised during surgery when the IOL has been
damaged (e.g. broken haptic), when appropriate
instrumentation to reposit the IOL is unavailable, or
when highly flexible haptics make the IOL unsuitable
for sulcus fixation. IOL exchange may sometimes be
appropriate for plate haptic IOL which are slippery and
difficult to grasp than PMMA lenses. Serrated or
diamond dusted forceps are recommended when
handling these IOLs. Repositioning may be particularly
challenging with silicon plate haptic lenses because they
are extremely floppy and difficult to manipulate. Also,
since they are non expansible and sized for capsular
fixation, centration with sulcus placement may be sub
optimal because it requires a longer dimension.
Implantation of a second IOL without removing the
first IOL has been reported, but this approach is not
generally recommended.
In patients for whom repositioning of posterior chamber
IOLs proves problematic, an intraoperative decision
may be made to remove or replace the lens with an
anterior chamber IOL or a scleral suture-fixated
posterior chamber IOL. Exchanging for a scleral
sutured- IOL has been simplified by new IOL designs
that incorporate positioning holes at the point of
maximum haptic curvature. Alternatively, exchange for
an anterior chamber IOL may be a faster, easier and
less traumatic to the corneal endothelium 14,15,15,17.
Newer AC IOL designs avoid mechanical side effects
that accompanied earlier designs.
Scleral fixated PC IOLs are technically more complex
than AC IOL implants. They carry a high risk of intra
ocular hemorrhage because of penetration of the ciliary
body. The major disadvantage of this technique is that
it leaves a potentially permanent partial thickness fistula
through the sclera, around the 100 prolene suture. This
surgical technique requires a thorough anterior
vitrectomy. IOL power calculation is difficult due to
posteriorly placed optic of the IOL.
It is important to verify the position of the scleral fixated
IOL because 2 prolene sutures are its sole support and
the position of the lens is the most important factor
contributing to post-operative refraction. A one piece,

394 Kerala Journal of Ophthalmology Vol. XX, No. 4
all PMMA, 100 vaulted, 13.5 mm haptic spread IOL
provides excellent optic centration and haptic
stabilization, when the haptic positioning holes are
placed at the point of greatest haptic spread and one
trans-scleral suture pass per haptic is made. A scleral
entry point 18,19,20 0.50 mm to 0.75 mm from the surgical
limbus avoids the major arterial circle and the entire
ciliary body and provides true ciliary sulcus placement
of the IOL.
Scleral fixation sutures 21,22,23 were first introduced for
implantation of secondary IOLs from the limbal or
parsplana approach or even for placement of a primary
PC IOL in the absence of adequate capsulozonular
support. Although a wide variety of techniques have
been described, all have the following common
objectives:-
1. Proper suture attachments to the IOL haptic.
2. Proper scleral sutures positioned to avoid
torsion,decentration or damage to intraocular
structures.
3. Proper scleral flap sutures to avoid externalization
of the fixation sutures and reduce the risk of
endophthalmitis.
In any scleral suture fixation procedures, the IOL is
first retrieved, then a suture loop is introduced through
the pars plana region into the vitreous cavity and
around the IOL and the suture is firmly secured to the
sclera. The technique that is commonly used for
repositioning the dislocated PC IOL with scleral sutures
in given below 24,25 (Fig. 2)
IOL torsion and decentration can be avoided by accurate
ciliary sulcus placement and adequate excision of bulky
capsular remnant and cortical matter. Histopathological
studies have shown little or no fibrosis around the
a b
c d
Fig. 2 a-d Technique for scleral suture fixation. (2a) Suture isthreaded through a 27-guage straight needle with ahole in the bevel. Needle and suture are introduced
into the vitreous cavity 1mm posterior to the limbusthrough the bed of a partial thickness scleral flap.Slack is created in the suture along the shaft of the
needle by withdrawing it slightly. Under directvisualization the haptic is threaded through the loopalong the shaft of the needle, using an intraocularforceps to grasp the optic. (2b) The needle iswithdrawn, and the suture is tied under the scleral
flap. (2c) Similar procedure is performed for the otherhaptic (2d). Side view of 2c.
Fig. 3. 10-0 prolene suture on an STC6 plus (ethicon) needle.Is passed at 10’o clock, docked on a 30 guage needleat 4’o clock (a) and pulled out with the later diagonally
(b). A Sinskey hook pulls out the suture from superiorcorneo-scleral section. The prolene suture is then tiedto the PC IOL haptic(d). The PC IOL is then delivered
into the posterior chamber with Mc Phersonforseps(e). The sutures are pulled at 4’o clock and10’o clock meridians (f). A single posterior scleral biteis taken and sutures are tied to themselves (g)
a b c
ed
f g

December 2008 M. Chakrabarti et al. - Management of Dislocated PC IOL 395
sutured PC IOL haptics. Therefore, a non dissolving
suture material must be used since it provides the sole
means of support at the ciliary sulcus 24.
Iris fixation sutures 25 requires passing a suture through
the cornea, iris, around the IOL haptic and back through
cornea and iris. Placement of the needle is not accurate
making IOL centration a challenging task. Other
disadvantage includes the increased risk of inviting a
chronic iris mediated intra ocular inflammation 12.
Fig 3 a-g describes the technique of two point scleral
fixator that we have been using for several years and it
has given us predictable results 12,13.
Alternatively a 4 –point scleral fixation can be
performed where the suture passage is made twice,
ensuring adequate anchorage, centration and
eliminating torsion.
Boris Malyugin 26 et al described a technique for
repositioning and trans scleral fixation of a dislocated
plate – haptic foldable collamer posterior chamber
intraocular lens. The displaced IOL was positioned in
the anterior chamber, and a double armed suture or a
curved needle was fixed to the sclera at 10.30 O’ clock
position. The needle then entered the globe and passed
through the superior haptic eyelet of the IOL and was
withdrawn through the scleral wound on the opposite
side. The inferior haptic was fixed at 4.30 and 7.30 o’
clock and provided the mirror reflection of the suture
path of the upper fixed haptic. This technique may be
an useful alternative to lens removal and exchange.
Richard Hoffman 27 et al decribed a technique of scleral
fixation without conjuctival dissection. The scleral
tunnel technique for scleral fixation utilizes a scleral
pocket initiated through a peripheral clear corneal
incision. Full thickness passage of a doubled arm suture
through scleral pocket and conjunctiva with subsequent
retrieval of the suture ends through the external corneal
incision for tying avoids the need for conjunctival
dissection, and a sutured wound closure.
A new technique that relies on glue 28 to implant IOLs
in eyes that lack posterior capsular support was
described by Agarwal et al. They used biological glue
(a quick acting surgical fibrin sealant derived from
human plasma with both hemostatic and adhesive
properties) to perform scleral fixation in a case of
dislocated IOL. Using microrhexis forceps the haptic of
the PMMA non-foldable IOL is grasped and externalized
under the previously prepared scleral flap. Fibrin glue
is applied on the bed of the flap and the flap is closed
in position. In the 12 eyes in their series there were no
notable postoperative complications such as
postoperative inflammation, hyphema, decentration,
glaucoma or corneal oedema on regular follow up.
However a long term follow up is necessary to validate
the efficacy of the procedure.
Surgical Results: The incidence of retinal
detachment following vitrectomy for dislocated PC IOLs
is given in Table 1. In recent series,approximately
70 % of patients achieved a final visual acuity ³
20/40. But surgical series are difficult to compare
accurately due to nonhomogenicity of the variety of
management techniques used.
Table 1. Results of PPV for Dislocated PC IOLs
Study Total RD before RD after Cumulative
(Year) patients PPV PPV
1. Blodi et al 32 4 3 7(1992) (12.5 %) (9.3 %) (21.9 %)
2. Scott 343 25 19 44(2003) (7.3 % ) (5.5 %) (12.8 %)
3. Smiddy 100 4 4 8
(2003) (4.0 %) (4.0 %) (8.0 %)
References
1. W. Smiddy; H. J. Flynn Managing lens fragments anddislocated posterior chamber lenses after CataractSurgery. Focal Points: 1996
2. William E Smiddy; Gonzalo V Ibanez; Eduardo Alfonso;Harry Flynn Surgical Management of dislocatedIOLs.JCRS; Vol 21; Jan 1995, 64-69.
3. Randy V Campo; Kelly D Chung; Ray T Oyakaura. Parsplana vitrectomy in the management of dislocatedposterior chamber lenses. Am. J Ophthalmol; 108;529-534; Nov 1989
4. Harry W Flynn Jr MD; Delyse Buus MD; William WCulbertson MD. Management of Subluxated andPosteriorly Dislocated IOLs using Pars plana VitrectomyInstrumentation. JCRS; Vol 16, Jan 1990; 51-56
5. Flynn H W Jr . Pars Plana Vitrectomy in the managementof subluxated and posteriorly dislocated intra ocularlens. Graefes Arch Clin Exp Ophthalmol 225; 169; 1987
6. Richard J Duffey; Edward J Holland et al. AnatomicStudy of Transsclerally sutured intra ocular lensimplantation.Am. J. Ophthalmol 108; 300-309, Sept1989.
7. Michael Cahane MD; Varda Chen; Issac Avni.Dislocation of scleral fixated PC IOL after fixation sutureremoval . JCRS, Vol 20, March 1994.

396 Kerala Journal of Ophthalmology Vol. XX, No. 4
8. Fransic W Price, Jr. MD, William E Withson MD. Visualresults of suture fixated PCIOLs during PKP. Oph 96,1989:1234-1240,
9. F.Haken Oner, Nilufer Kocak, Osman Saatis. Dislocationof capsular bag with IOL and capsular tension ring. J.Cataract Refract Surg 2006; 32:1756-1758
10. Schneidermann TE, Johnson MW et al. Surgicalmanagement of dislocated plate haptic IOLs. Am. J.Ophthalmol 1997;123:629-635
11. William E Smiddy, Gonzalo V Ibanez, Edward Alfons,Haerry Hynn. Surgical management of Dislocated IOLs.JCRS.Vol 21, Jan 1995. 64-69.
12. Hilel Lewis. MD; German Sanchez MD. The use of PFCLin the repositioning of posteriorly dislocatedIOLs.Ophthalmol 1993; 100; 1055-1059.
13. Randy .V. Campo, Kelly .D. Chung, Ray. T. Oyakawa. ParsPlana Vitrectomy in the management of posterior chamberlenses. Am.J.Ophthalmol 108, Nov 1989; 529-534.
14. Edward .S. Lim, MD, David .J. Apple MD, Jolie C. TsaiMD et al. An analysis of Flexible Anterior Chamberlenses with special reference to the normalised rate oflens explanation. Ophthalmol 1991, 98: 243-246
15. Tarek.S.Hassen, Kaz Soong, Alan Sugar et al.Implantation of Kelman-Style open loop AC IOLs duringKeratoplasty for aphakic and pseudophakic bullouskeratopathy – A comparison with iris sutured posteriorchamber lenses. Ophthalmol 1991,98:875-880
16. Lawerence .E. Weene MD. Flexible open-loop AC IOLimplants. Ophthalmol 1993, 100, 1636-1639
17. Jonathan .H. Lass, Deana .M. Desentis, Wiliam J.Reinhart. Clinical and morphometric results of PKPwith one piece AC or suture fixted PCIOLs in theabsence of lens capsule. Arch. Ophthalmol 1990,108:1427-1430.
18. Richard .J. Duffey, Edward .J, Holland et al. Anatomicstudy of trans sclerally sutured intraocular lens
implantation. Am. J. Ophthalmol 108, Sept 1989:300-309
19. Surendra Basti, P.C. Tejaswi et al. Outside – inTransscleral fixation for ciliary sulcus IOL placement.JCRS Vol 20, Jan 1994, 89-92.
20. Anthony .J. Lubniewski MD, Edward J Holland MD,Woodford .S. Van Meter MD et al. Histological study ofEye with Trans sclerally sutured posterior chamber IOLs.Am. J. Ophthalmol.110, Sept 1990:237-243
21. Emigdio A Navia- Aray MD. A technique for knotting asuture around the loops of a dislocated IOL within theeye for fixation in the ciliary sulcus. Oph Surgery Oct1993, Vol 24, No:10 :702-707
22. Steven .M. Bloom, Richard .E. Wyszynske Alexander.J. Brucker. Scleral fixation suture for dislocated PCIOLS.Ophthalmic surgery Dec 1990, Vol 21, No:12
23. Martin .S. Arkin, Roger F Stenert. Sutured posteriorchamber intraocular lenses. J Cataract Refract Surg.Dec. 1991, Vol. 21.
24. Kerry Solomon, MD, Joseoh .R. Gussler, Carter Gussler,Woodford S. Van Meter. Incidence and management ofcomplications of transsclerally sutured PCIOLs.J.Cat.Refract Surgery Vol 19, July 1993; 488 -493
25. S.Gregory Smith MD, Wilmengton Deluerare FrankShowden et al. Topographical anatomy of the ciliarysulcus. J. Cataract Refract Surg. Vol 13, Sept 1984:543 -547
26. Boris Malyugin et al. Technique for respositioning andtrans –scleral fixation of a dislocated plate hapticfoldable posterior chamber intraocular lens. J.CataractRefract Surg 2008
27. Richard S Hoffmann, Howard Fine et a .Scleral fixationwithout conjunctival dissection .J.Cataract Refract Surg2006;32:1907-1912
28. Amar Agarwal et al. PCIOL fixed by Fibrin glue. OcularSurg News Europe/ Asia-Pacific Edition March 2008

December 2008 R.H. Trivedi et al. - Pediatric Cataract Surgery 397
Pediatric Cataract SurgeryDr. Rupal H. Trivedi MD MSCR, Dr. M. Edward Wilson MD
Cataract surgery in children remains complex and
demanding. It is quite different from surgery for
cataracts in the elderly. A propensity for increased
postoperative inflammation and capsular opacification,
constantly changing refraction, difficulty in examining
child due to poor compliance, and a tendency to develop
amblyopia are among the factors that make the
management of childhood cataract different from that
in the adult. The aim of pediatric cataract surgery is
not only to provide but also to maintain a clear visual
axis and a focused retinal image.
Preoperative evaluation: A detailed history
including current age, age at onset of symptoms, birth
weight; evidence of maternal infection (especially the
TORCH infections), rash or febrile illness during
pregnancy (may be suggestive of intrauterine infection),
any other prenatal and perinatal history that may be
pertinent (e.g., alcohol, tobacco, drug use, ionizing
radiation during pregnancy), history of ocular trauma
(unless cataract appears to be purely non-traumatic),
ocular status on previous eye examinations (can be
helpful in assessing visual prognosis after treatment),
history of corticosteroid therapy (especially in posterior
subcapsular cataract) and family history (especially for
bilateral cataract) should be documented.
The method of evaluating visual function will vary
according to the age of the child and the level of
cooperation. Documentation of the child’s level of
cooperation with the examination can be useful in
interpreting the results and in making comparisons
among the examinations over time. In infant and
preverbal child the assessment strategy is to determine
whether each eye can fixate on an object, maintain
fixation, and then follow the object into all directions.
The assessment should be performed binocularly and
then monocularly. The force with which the child objects
to alternate occlusion of the eyes is useful to judge the
relative vision in each eye. In an awake and alert child,
if poor fixation and following are noted binocularly after
3-4 months of age, a significant visual loss is suspected.
For strabismic children, an assessment of binocular
fixation pattern is performed in which the examiner
determines the length of time that the non-preferred
eye can hold fixation. It can be reported as, will not
hold fixation with non-preferred eye, holds fixation
briefly with non-preferred eye, or no fixation
preference. With a straight-eyed child and those with
small angle deviation, 20 diopter base-down prism
induced-tropia fixation test can be used to optically
separate the two eyes. Quantitative VA assessment in
cooperative verbal children can be assessed using
optotype VA testing (identifying or matching symbols
or letters), allowing quantification of VA on a Snellen
or preferably, a logMAR scale. Distance VA should be
determined monocularly whenever possible. The fellow
eye should be completely covered (with adhesive
occluder to prevent peeking). In children with posterior
subcapsular cataracts who complain of intolerable glare,
but have good Snellen VA, glare testing should be
performed to evaluate the need for surgery.
The red reflex test can be used to detect the density
and extent of the opacity in the visual axis. Details on
strabismus and nystagmus help when explaining
Department of Ophthalmology, Storm Eye Institute, Miles Center for Pediatric
Ophthalmology, Medical University of South Carolina, Charleston, SC, U.S.A.
The authors have no financial or proprietary interest in any product mentioned
herein. Supported in part by the Grady Lyman Fund of the MUSC Health Sciences
Foundation, Charleston, S.C.
OPHTHALMIC
S U R G E R Y

398 Kerala Journal of Ophthalmology Vol. XX, No. 4
prognosis to the parents and to prepare them for
patching or further surgeries. Strabismus at
presentation is often an indication that the cataract is
long-standing and that significant amblyopia is likely
to be present. Infants with profound bilateral dense
cataracts develop nystagmus at approximately 3 months
of age because the fixation reflex normally develops
by that time. If manifest nystagmus does develop, the
visual prognosis is worse.
Microphthalmia and poorly dilating pupils increase the
risk of a poor anatomical outcome after cataract surgery.
After dilation, a slit-lamp evaluation should be carried
out if the child is old enough to be cooperative. The
morphology of the cataract may affect prognosis and
give a clue to the etiology. Unilateral PSC should prompt
a careful search for evidence of trauma. Bilateral PSC
cataract may result from chronic uveitis, prolonged
corticosteroid treatment for chronic disease, radiation
treatment for malignancy, or nonaccidental injury (child
abuse). Children with juvenile idiopathic arthritis may
have associated band shaped keratopathy and posterior
synechaie. Lens subluxation, iridodonesis, and aniridia
should be looked for. Total cataract involving the whole
lens can occur in Down syndrome, Type 1 diabetes
mellitus, in congenital rubella (where shaggy nuclear
cataracts are more common), and posterior lentiglobus.
In cases of unilateral cataract, examination of the fellow
eye after pupil dilation is essential to rule out
asymmetric bilateral findings. Anterior lenticonus is
most often associated with Alport syndrome and should
be investigated accordingly. A sudden onset of total
cataract may be an indication of unsuspected trauma,
diabetic cataract or preexisting ruptured anterior
(reported in anterior lenticonus) or posterior capsule
(reported in posterior lentiglobus).
For children approximately above 5-6 years of age,
ability of child to cooperate for slit-lamp examination
is also an indirect indicator that child will cooperate
for YAG-laser capsulotomy if needed. In children above
5-6 years of age with intact posterior capsule and
AcrySofR IOL implantation, visually significant posterior
capsule opacification (PCO) is known to develop after
18-24 months of surgery. If child in this age range seems
to be cooperative for slit-lamp examination during
preoperative evaluation, the surgeon may decide to
leave behind an intact posterior capsule (assuming high
odds of getting child’s cooperation for YAG if needed).
A slit-lamp examination of both parents, if possible,
helps to establish the presence of familial cataracts and
cataract-associated conditions. These findings can be
subtle and the parents may not have been told that
they have any pathology at all.
As compared to unilateral cataract, laboratory
investigation of bilateral cases is more rewarding.
Exhaustive lists of possible laboratory investigations for
a child with cataract can be found in several text books,
however, in an otherwise healthy child, most physicians
do not advise extensive laboratory and genetic
investigations. After detailed evaluation, 86% of
unilateral and 68% of bilateral cataract have no
discernible cause 1. Based on history and examination,
customized laboratory investigations can be advised.
Deciding list of laboratory investigations to detect the
cause can be occasionally based on logistic issues,
financial considerations and parent’s enthusiasm and
willingness to spend time and effort to do so. It is
important to keep in the mind that the common causes
of cataract in children include intrauterine infections,
metabolic disorders, and genetically transmitted
syndromes. Since cataracts can be the presenting sign
of diabetes, children with acquired cataracts of
unknown etiology should be questioned about classic
symptoms of diabetes and evaluation for hyperglycemia
should be performed. Children with Lowe syndrome
have hypotonia, mental retardation, aminoaciduria and
an abnormal facial appearance with frontal bossing,
and chubby cheeks. The lens typically has a reduced
anterior-posterior diameter 2. In addition, these eyes
have frequent association with glaucoma. If Lowe
syndrome is suspected, the urine should be screened
for amino acids. If there is history of maternal rash,
fever, flu-like symptoms, or neonatal physical signs of
intrauterine infection, then acute and convalescent
TORCH titers should be obtained. Developmental
pediatricians and clinical geneticist are experts in
selective investigation based on characteristics of the
child and they should be consulted when appropriate.
Indication for surgery: Indications for cataract
surgery include cataracts obstructing the examiner’s
view for fundus examination in the nondilated pupil
or a blackened retinoscopic reflex preventing refraction
of patient. It is often difficult to decide when to remove

December 2008 R.H. Trivedi et al. - Pediatric Cataract Surgery 399
a partial cataract in non-verbal children. The loss of
accommodation after the cataract is removed may
negatively affect visual functioning more than the
partial cataract was. For verbal children, cataract
surgery is contemplated if Snellen VA is 20/50 or worse,
if the child is intolerant to glare or resistant to
amblyopia therapy with gradually deteriorating visual
function. Since a subjective VA cannot be obtained in
infants with cataracts, greater reliance is placed on the
morphology of the cataract; other associated ocular
findings, and the visual behavior of the child, in order
to ascertain whether the cataract is visually significant
or not. The degree of visual impairment induced by
lens opacity differs markedly depending on the location
of the opacity. Generally, the more posterior and more
central location of the opacity is more amblyogenic.
Generally speaking, a cataract that blackens the
retinoscopic reflex for 3mm or more in the center of
the pupil is considered visually significant. If a partial
cataract is being treated conservatively, it is important
to carefully follow these children. Conservative
treatment using mydriatics drops necessitates the
patient’s wearing glasses for reading if any cycloplegic
effect is induced. This has not found widespread
acceptance. Associated glare and loss of accommodation
are the most common obstacles. Visual outcome has
also been unimpressive. Despite these limitations, the
use of mydriatics drops may be kept in reserve in eyes
with slowly progressive cataracts or para-central
cataracts less than 3mm and, especially, in patients for
whom cataract surgery needs to be deferred for any
reason, - be it medical (high risk for anesthesia), social
or economical.
Timing of surgery: Deciding on the appropriate
timing of surgery is most critical during early infancy.
In the case of a unilateral dense cataract diagnosed at
birth, the surgeon can wait until 4-6 weeks of age.
Waiting until this age decreases anesthesia-related
complications and facilitate the surgical procedure.
Waiting beyond this time, however, adversely affects
visual outcome. 3, 4 In the case of a bilateral cataract
diagnosed at birth, a good visual outcome can be
achieved if the child is operated before 10 weeks
of age. 5 The first eye surgery can be offered at 4-6
weeks of age, and the second eye surgery after another
1-2 week’s time. It is important to keep the time interval
to a minimum between the two eye surgeries. For older
children, timing of surgery is not as crucial. In children
beyond the amblyopic age, surgery can often be decided
based on convenience and other logistic issues.
Sequential cataract surgery, more popularly known as
simultaneous bilateral cataract surgery (SBCS), remains
controversial. Almost every discussion on SBCS either
starts or ends with a comment on the disagreement
surrounding its use. The important question is not “can
it be done?” but, more properly, “should it be done?”
Even conservative surgeons, who vote against routine
use of SBCS in children, are more likely to use this
approach when anesthesia poses more than average
risks or the patient lives far away and a visit for surgery
on the second eye would be difficult. In eyes with
penetrating trauma and cataract, primary repair of the
corneal or scleral wound is usually preferred as the
initial step. Cataract surgery with IOL implantation
should be performed 1-4 weeks after a complete
evaluation of damage to intraocular structures (e.g.
posterior capsule rupture, vitreous hemorrhage and
retinal detachment) with ancillary methods such as B-
scan ultrasonography.
Aphakic rehabilitation: For bilateral cataracts,
aphakic glasses and/or contact lens use may be a
reasonable option. However, for unilateral cataracts in
infancy, the issue of when to implant an IOL is
unresolved. We await the results of ongoing multi-
center clinical trial research to help guide us. For
children beyond infancy, IOL implantation is less
controversial. Both IOLs and aphakic contact lenses may
support similar VA after surgery for unilateral cataract
in the presence of good compliance with contact lens.
However, IOLs support better VA when compliance with
contact lens wear is moderate or poor 6.
Intraocular lens implantation in children has the benefit
of reducing dependency on compliance with other
external optical devices (aphakic glasses and contact
lens) and providing at least a partial optical correction.
These are important advantages to the visual
development in amblyopia-prone eyes. However,
concerns about primary IOL implantation are the
technical difficulties of implanting an IOL in the eyes
of children, selecting an appropriate IOL power, and
the risk of visual axis opacification (VAO) after
implantation. Despite performing primary posterior
capsulectomy and vitrectomy, the rate of VAO is higher

400 Kerala Journal of Ophthalmology Vol. XX, No. 4
in pseudophakic infantile eyes as compared with
aphakic infantile eyes. 7 On the other hand, although it
is possible for an eye with a unilateral infantile cataract
to achieve good visual outcome following contact lens
correction, it has continued to be the exception rather
than the rule.
Parental counseling: Surgeons who perform
pediatric cataract surgery should be prepared for
sometimes a quite lengthy discussion with parents. A
coordinated plan of action can best be developed when
the parents understand the reasons for, goals of, and
the advantages and potential complications of cataract
surgery. When properly informed preoperatively, the
parents and the physician become partners with the
common goal of doing what is best for the child. Time
spent establishing this partnership is not wasted,
because a better informed family is much more likely
to comply with the frequent follow-ups, medications,
patching, glasses wear, etc., that are so essential to the
eventual visual outcome. The parents/caregivers play
a critical role in the postoperative care of the eye and
treatment of amblyopia. They must understand that a
successful visual outcome depends on more than the
surgical procedure; it also depends on their ability to
maintain adequate aphakic correction and follow
through with amblyopia therapy. It is important to
discuss the major pros and cons of the available options
with the parents/legal guardian. Parents should be
made aware that surgery is only one component of the
treatment. Visual prognosis can be explained to the
parent based on preoperative evaluation.
The changing refraction will require frequent follow-
up examinations. Glaucoma is known to develop even
years after cataract surgery. Parents need to understand
that their child may need serial examinations under
anesthesia until the child is cooperative enough to get
examined in the office. The parents should also be
explained about treatment of VAO, strabismus,
glaucoma, and rarely, decentered IOL, synechiolysis,
or removal of a loose stitch. For eyes operated during
early infancy, parents should be made aware that the
first 6-month follow-up is very crucial. Despite
performing primary posterior capsulectomy and
vitrectomy, many infant eyes develop VAO, and most
eyes that develop VAO, develop it in the first six
postoperative months. Earlier detection (and treatment
if needed) can help to achieve a better visual outcome.
For eyes operated with an intact posterior capsule,
parents should be made aware that the child would
require a secondary procedure for PCO. Parents of
children with lens implants are also made aware that
glasses will likely still be needed postoperatively even
when an IOL is implanted. In addition, glasses power
may need to be changed frequently after surgery,
because of changing refraction. Useful web resources
for parents: http://www.pgcfa.org/cataract.htm and
http://www.ich.ucl.ac.uk/factsheets/families/
F020023/ (information for families with cataract).
Examination under anesthesia: We routinely
perform an EUA during the same session as the cataract
surgery. However, to do an EUA as a separate session is
also an acceptable approach. Intraocular pressure
should be checked as soon as possible after induction
of anesthesia. Although we routinely use the tonopen,
if in doubt, we recheck IOP using the Perkins tonometer.
In addition to high IOP, a difference of IOP between
the two eyes is alarming. Cataracts and glaucoma are
associated with congenital rubella and Lowe Syndrome.
The next step for us is to take keratometry
measurements. We use the Nidek handheld
keratometer. However, many other centers uses an
autorefractokeratometer for this purpose. The
remaining examinations listed below can be performed
in any chronology: examine the eye using the operating
microscope, immersion A-scan ultrasound for globe
axial length, horizontal corneal diameter, retinoscopy
(if possible), and fundus examination. Some physicians
use a slit lamp attachment to operating microscope for
evaluating location of the cataract. Immersion A-scan
performed by a skilled ultrasonographer helps to reduce
the incidence of postoperative refractive surprises. A
shorter or longer axial length in the eye with the
cataract can be sign of poor prognosis. In the case of
no view on fundus examination, we perform a B-scan
ultrasound examination. Although it is often not
possible to do a preoperative cycloplegic refraction of
an eye with a dense cataract, an uninvolved or less
involved fellow eye should be refracted. The presence
of refractive error in the fellow eye may help when
deciding on an IOL power.
Preoperative and Intraoperative Medications:
It is important to apply antibiotic drops to the eye prior

December 2008 R.H. Trivedi et al. - Pediatric Cataract Surgery 401
to beginning surgery. We begin topical application of
antibiotics approximately 1 hour prior to surgery. The
drop is given every five minutes for a total of four times.
While it would be ideal to start the antibiotic earlier
than 1 hour before surgery, it is logistically difficult.
Dilating drops are also given preoperatively on check-
in every five minutes times three. We make up a peds
combination drop that consists of 2 mL 2 %
cyclopentalate, 0.5 mL 10 % phenylephrine, and 0.5
mL 1 % tropicamide in every 3 mL of drops. In essence,
each drop delivered to the patient contains 1.3 %
cyclopentalate, 1.67 % phenylephrine, and 0.17 %
tropicamide. To aid in maintaining dilation of the pupil
throughout surgery, 0.5 mL epinephrine 1:1000 solution
is added to each 500 mL bottle of irrigating solution.
We recently published a pediatric case of intraoperative
floppy iris syndrome IFIS in one eye and no IFIS in the
other eye as a result of the inadvertent absence of
epinephrine in the irrigating fluid of the eye
demonstrating signs of IFIS 8. We strongly recommend
epinephrine in the irrigation fluid for all pediatric
cataract surgeries. Povidone iodine, diluted to a 5 %
solution, is applied to the eye at the end of the surgical
skin and lash prep. An additional drop is placed at the
conclusion of surgery.
Surgical Steps:
Incision: Pediatric cataracts can be removed through
a relatively small wound, as the lens has no hard
nucleus. Therefore, wounds should be constructed to
provide a snug fit for the instruments that pass into
the anterior chamber. When an IOL is not being
implanted, two stab incisions are usually made at or
near the limbus. These incisions should not be larger
than necessary for the instruments being used. For
instance, a micro vitreoretinal (MVR) blade can be used
that creates a 20-gauge opening for a 20-gauge
vitrector/aspirator to enter the anterior chamber. A 20
gauge blunt tipped irrigating cannula can also be used
through a separate MVR blade stab incision. If the
instrument positions need to be reversed, the snug fit
is maintained. If 23 gauge or 25 gauge instruments are
used, an MVR for that gauge opening can be utilized.
While some surgeons prefer phaco-aspiration
(aspiration utilizing a standard phacoemulsification
hand-piece), bimanual technique using an irrigating
hand-piece and a separate aspiration hand-piece is
preferred by the authors. Anterior chamber stability is
maintained by limiting wound leak and using a high
irrigation setting. When a foldable IOL is being
implanted, a corneal tunnel is preferred since it leaves
the conjunctiva undisturbed. In infants, a scleral tunnel
is sometimes used because it heals more transparently
than a corneal tunnel. In addition, a rigid IOL is
implanted occasionally when sulcus placement over a
large pre-existing posterior capsulotomy is desired. In
these instances, a scleral tunnel is utilized.
Unlike adults, corneal incisions do not usually self-seal
in children. Our 2001 survey indicated that only 20%
and 3 % of the American Society of Cataract and
Refractive Surgeons (ASCRS) and American Association
for Pediatric Ophthalmology and Strabismus (AAPOS)
respondees, respectively, left both tunnel and
paracentesis incisions unsutured. 9 According to one
study 10, self-sealing wounds failed to remain watertight
in children below 11 years of age, especially when an
anterior vitrectomy was combined with cataract
extraction. Even in older children, suturing is
recommended since postoperative eye rubbing is
common. The recommended closure material is a 10-0
synthetic absorbable suture. The use of non-absorbable
sutures occasionally calls for an EUA for suture removal.
Even when economic issues are a deciding factor in
choice of suture material, it is better to use absorbable
sutures rather than subject the child to additional
anesthesia.
Anterior Capsulotomy: The anterior capsule in
children is highly elastic and poses challenges in the
creation of the capsulotomy 11, 12, 13 While a manual
continuous curvilinear capsulorhexis (CCC) is ideal for
adults, it is more difficult to perform in young eyes.
When performing a manual CCC in a child, the
following technical recommendations are offered. Use
of a highly viscous ophthalmic-viscosurgical-device
(OVD) is recommended to fill the anterior chamber and
flatten the anterior capsule. A slack anterior capsule
will be easier to tear in a controlled fashion. Re-grasp
the capsulorhexis edge frequently and begin with a
smaller capsulotomy than desired. Because of the
elasticity, the opening will be larger than it appears
once the capsular flap is released. In order to control
the turning of the CCC edge along a circular path, the

402 Kerala Journal of Ophthalmology Vol. XX, No. 4
tear must often be directed more toward the center of
the pupil than would be necessary in an adult eye. If
the capsule begins to extend peripherally, stop before
the edge is out of sight under the iris. Re-grasp the
capsule edge and pull directly toward the center of the
pupil to recover the tear. Converting to a vitrectorhexis
or a radio frequency diathermy capsulotomy may also
be warranted. Using small incision capsulorhexis
forceps that fits easily through a paracentesis will allow
conversion to vitrector instruments when needed
without leakage around the vitrector hand-piece during
use. While a CCC using the techniques described above
is a reasonable option beyond age 4, it will be more
difficult when attempted on children aged 4 and
younger. The vitrectorhexis is an alternative anterior
capsulotomy method that will be more consistently
successful than manual CCC in the youngest patients.
When creating a vitrectorhexis, the following surgical
caveats are offered. Use a vitrector supported by a
Venturi pump, if possible. A bi-manual technique with
a separate infusion port is recommended. Maintain a
snug fit of the instruments in the incisions through
which they are placed. The anterior chamber of these
soft eyes will collapse readily if leakage occurs around
the instruments, making the vitrectorhexis more
difficult to complete. A MVR blade can be used to enter
the eye. The vitrector and a blunt-tip irrigating cannula
fit snugly into the MVR openings. We recommend either
a 20 gauge Grieshaber irrigation handpiece (Alcon) or
a Nichamin cannula (Storz). An anterior chamber
maintainer can also be used if the surgeon prefers. We
have found that it is not necessary to begin the
capsulotomy with a bent-needle cystotome. Merely
place the vitrector, with its cutting port positioned
posteriorly, in contact with the center of the intact
anterior capsule. Turn the cutter on and increase the
suction using the foot pedal until the capsule is engaged
and opened. A cutting rate of 150 to 300 cuts per minute
and an aspiration maximum of 150 to 250 are
recommended. These settings are for currently utilized
Venturi-pump machines. Adjustments may be needed
for other machines. With the cutting port facing down
against the capsule, engage the capsule and enlarge
the round capsular opening in a spiral fashion to the
desired shape and size. Any lens cortex that escapes
into the anterior chamber during the vitrectorhexis is
aspirated easily without interrupting the capsulotomy
technique. Care should be taken to avoid leaving any
right-angle edges, which could predispose to radial tear
formation. A third option for creating an anterior
capsulotomy in a child is available with the use of high
frequency endodiathermy (Kloti radio frequency
endodiathermy). This instrument cuts capsule
efficiently but results in an edge that tears easily if
stretched. The Fugo plasma blade has also been used
to make an anterior capsulotomy. Our experience with
the Fugo blade in children is only a few cases, but the
capsulotomy edge created in those cases was not very
different clinically from that produced by the Kloti
instrument mentioned above. Use of capsular dyes has
started attracting pediatric cataract surgeons, also.
Visualization of the capsular flap is important to
maintain control of any tears and to ensure that the
edge is continuous. A report from the American
Academy of Ophthalmology 14 has concluded that “it is
reasonable to consider the use of dye in cataract surgery
in cases in which inadequate capsule visualization or
inexperience with capsule visualization may
compromise the outcome. The use of dye in routine
cases cannot be recommended until a lack of toxicity is
more clearly demonstrated in the event of longer
duration exposure or posterior segment exposure”. Both
trypan blue and indocyanine green dyes provide
excellent visualization of the anterior capsule flap
during CCC. When injecting under air, the dye should
be injected after the paracentesis, but prior to creating
the main incision, to help with anterior chamber
stability. Staining under air versus under OVD was
reported similar efficacy and safety. In addition to better
visualization, trypan blue has been reported to
minimize epithelial cell proliferation in pediatric
cataract surgery. The staining the anterior capsule with
trypan blue affected the density and viability of
LECs. 15 The use of dyes is not advised when using
hydrophilic IOLs, to avoid permanent discoloration of
the IOL. 16
Lens substance aspiration (Phacoaspiration):
Thorough removal of lens substance is especially crucial
for pediatric eyes. When any cortical matter, which
clinically may resemble a harmless strand or fiber, is
left behind, it actually leaves behind a large number of
mitotically active cells. These cells have the potential
to grow and cause a proliferative form of VAO. The

December 2008 R.H. Trivedi et al. - Pediatric Cataract Surgery 403
best means of reducing the incidence of this is to remove
as many of these cells as possible at the time of surgery.
Since VAO is one of the most frequent postoperative
complications in pediatric cataract surgery, meticulous
removal of the lens substance is a crucial step in the
management of pediatric cataracts. Pediatric cataracts
are soft but they may be “gummy.” Phacoemulsification
is not needed. Lens cortex and nucleus can be aspirated
in every case with an irrigation/aspiration or vitrectomy
hand-piece. We prefer the bimanual approach using
separate irrigation and aspiration. Separate irrigation
and aspiration help maintain the anterior chamber
stability, decrease fluctuations of the anterior chamber
and help thorough removal of lens substance. When
using the vitrector, bursts of cutting can be used
intermittently to facilitate the aspiration of the more
“gummy” cortex of young children. The advantage of
using the vitrector is that it is possible to perform
vitrectorhexis, irrigation/aspiration, posterior
capsulectomy and vitrectomy – all with one instrument
(the setting needs to be changed appropriately). This
avoids extra manipulation and repeated entry into and
exit from the eye. In older children, after a manual
CCC we prefer 20-gauge bimanual irrigation/aspiration
hand-pieces that are tapered and curved (Alcon/
Grieshaber 170-01 for irrigation and Alcon/Grieshaber
170-02 for aspiration). Maintenance of the anterior
chamber is critical when removing lens substance.
Aspiration of fluid from the anterior chamber must be
balanced by adequate infusion. Although we do not
have personal experience of using heparin sodium in
the irrigating fluid, reports showing a beneficial role in
preventing postoperative inflammation have appeared
in the literature. 17 The use of heparin should be avoided
in eyes with a compromised blood-aqueous barrier (e.g.,
previous ocular surgery) as they are at high risk of
developing postoperative hyphema.
Hydrodissection has been thought to be less useful in
children than in adults. However, one study has shown
the intraoperative benefits of performing multiquadrant
hydrodissection. 18 The potential benefits are an overall
reduction in the operative time and a reduction in the
amount of irrigating solution used to facilitate lens
substance removal. A fluid wave can sometimes be
generated in older children but not reliably in infants
and toddlers. Cortical material strips easily from the
pediatric capsule even in the absence of hydrodissection
if the proper technique is used. Hydrodissection should
not be done in children with posterior polar cataracts
in children because of the fragility in the posterior
capsule in these cases.
Posterior Capsulectomy and Vitrectomy: In
young children who undergo pediatric cataract surgery,
PCO is rapid and virtually inevitable if the posterior
capsule is left intact. 19-22 PCO occurs much faster and
is much more amblyogenic in younger children as
compared with older children. The advent of vitreous
suction cutting devices for removing the center of the
posterior capsule and a portion of the anterior vitreous
during the initial surgery in young children undergoing
cataract surgery dramatically decreased the need for
secondary surgery. A primary posterior capsulectomy
and anterior vitrectomy during IOL implantation in the
pediatric cataract gives the best chance for maintaining
a long-term clear visual axis. Nd: YAG laser posterior
capsulotomies are usually necessary in children when
the posterior capsule is left intact. Larger amounts of
laser energy are often needed as compared to adults,
and the posterior capsule opening may close, requiring
repeated laser treatments or a secondary pars plana
membranectomy. At present primary posterior
capsulectomy and anterior vitrectomy is common
practice while managing younger children with
cataract. An important question that remains is, when
should the posterior capsule be left intact? We answer
this question looking at several factors (age, association
of posterior capsule plaque or defect, availability of YAG
laser, expected cooperation of child approximately 12-
24 months after cataract surgery for YAG). As a rough
guideline, in children below 5 years of age, we prefer
to do primary posterior capsulectomy and vitrectomy.
In children, 5-8 years of age, we will do a posterior
capsulectomy with or without vitrectomy, as needed.
In children above 8 years of age, we keep an intact
posterior capsule more often. Anterior segment
surgeons are often more accustomed to, and more
comfortable with, a limbal (or anterior) approach. Our
current strategy is to perform these procedures via the
pars plana/plicata preferentially, whenever we intend
to use a primary vitrectomy in pediatric eyes receiving
IOL implantation. The size of the posterior capsule
opening should be large enough to help avoid VAO,
but small enough that sufficient peripheral capsular
support remains for capsular fixation of an IOL. Even

404 Kerala Journal of Ophthalmology Vol. XX, No. 4
if the surgeon is not planning to implant an IOL in a
specific eye, it is important to leave behind sufficient
anterior and posterior capsular support at the time of
cataract surgery to facilitate subsequent in-the-bag or
sulcus-fixated IOL implantation (if needed). 23 Ideally,
the surgeon should aim for a central, circular opening
in the posterior capsule about 1-1.5 mm smaller than
the IOL optic. On the Accurus machine (Alcon
Laboratories, Fort Worth, Texas), an irrigation rate of
30+ cc/min and a cutting rate of 600 cuts/min have
proven effective at our setting. Readers should follow
the manufacturer’s instruction manual for using a
specific machine and setting. When the pars plana/
plicata approach is chosen, the IOL should be inserted
into the capsular bag using OVD, while the posterior
capsule is still intact. The OVD can be removed without
fear of engaging vitreous, because removal precedes
the posterior capsulectomy. While the irrigation cannula
remains in the anterior chamber, a MVR blade is used
to enter the pars plana/plicata 2-3 mm (2-mm in
patients less than 1-year old, 2.5-mm in patients 1-4
years old, and 3-mm in patients over 4 years old)
posterior to the limbus. The vitrector is then inserted
through this incision and used to open the center of
the posterior capsule. The endpoint for the vitrectomy
is difficult to define. Sufficient vitreous should be
removed centrally so that the LEC cannot use the
vitreous face as a scaffold for VAO. Any vitreous that
tracks forward past the plane of the posterior
capsulectomy needs to be removed. VAO after primary
posterior capsulectomy and vitrectomy is often blamed
on an inadequate posterior capsule opening or an
inadequate vitrectomy. These assertions have not been
verified scientifically. In cataract with associated blood
vessel anomalies, such as persistent fetal vasculature,
vitrectomy instrumentation is used to remove the
posterior lens capsule, abnormal membrane, and
anterior vitreous. Intraocular scissors and intraocular
cautery are also used as needed. Intracameral
triamcinolone (Kenalog) may have a potential benefit
in the management of pediatric cataract. Kenalog
injection into the anterior chamber provides the anterior
segment surgeon a means to localize and identify if
any vitreous strands remaining in anterior chamber that
otherwise might have gone unnoticed. Sutureless, pars
plana vitrectomy through self-sealing sclerotomies has
been reported in the literature. No difference in the
amount of visible vitreous incarceration between
sutured and sutureless sclerotomies was reported, using
ultrabiomicroscopy. However, wound leakage,
extension, dehiscence, hemorrhage, vitreous and/or
retinal incarceration, retinal tear and dialysis have been
reported with this technique. Difficulty with the passage
of instruments has also been observed when tunnel
incisions are used.
IOL implantation: A general consensus exists that
IOL implantation is appropriate for most older children
undergoing cataract surgery. In contrast, the advisability
of IOL implantation during the first year of life is still
being questioned. 24 We showed a nearly 5-fold increase
in the number of the ASCRS respondents and more
than a 13-fold increase in the number of the AAPOS
respondents implanting IOLs in children 2-years old
and younger from 1993 to 2001. It is well known that
the majority of the eye’s axial growth occurs during
the first two years of life. This rapid eye growth makes
selection of an IOL power for an infant difficult.
Selecting the best IOL power to implant in a growing
child presents unique challenges. While Gordon and
Donzis 25 have documented the axial growth pattern of
normal eyes in children, the axial growth of cataractous
eyes is different. 26 In the normal phakic child, there is
little change in refraction (0.9 diopters from birth
through adulthood on average) because the power of
the natural lens decreases dramatically as the eye grows
axially. However, an IOL placed in a child’s eye cannot
change in power to match the growth of the eye. An
IOL chosen for emmetropia in early childhood is likely
to leave the patient highly myopic in adulthood. For
children beyond age 2, studies are available to help
the surgeon predict average growth of the eye. When
operating on children, many surgeons have advised
selecting an IOL power that will leave mild to moderate
hyperopia, leaving less hyperopia with increasing age.
Details on IOL power selection has been provided in
earlier issue of this journal.
When placing an IOL in a child’s eye, in-the-bag
implantation is strongly recommended. Care should be
taken to avoid asymmetrical fixation with one haptic
in the capsular bag and the other in the ciliary sulcus.
This can lead to decentration of the IOL. In contrast to
adults, dialing of an IOL into the capsular bag can be
difficult in children. Often the IOL will dial out of the

December 2008 R.H. Trivedi et al. - Pediatric Cataract Surgery 405
capsular bag rather than into it. This tendency can be
blunted somewhat by the use of highly viscous OVDs.
Foldable hydrophobic acrylic IOLs are used increasingly
in children. The AcrySof® hydrophobic acrylic IOL
(Alcon Laboratories, Ft. Worth, Texas) has been shown
to be very biocompatible for the pediatric eyes. 27
Tassignon and colleagues 28 reported the outcome of a
surgical procedure they called “bag-in-the-lens” in eyes
with pediatric cataract. In this technique, the anterior
and posterior capsules are placed in the groove of a
specially designed IOL after a capsulorhexis of the same
size is created in both capsules. The authors reported a
clear visual axis in all pediatric patients with an average
follow-up of 17-months.
The ongoing development in adjustable IOL technology
may prove very useful in the future of the surgical
management of pediatric cataracts. The possibility of a
lens that could be adjusted to counter the myopia
induced by ocular growth is potentially exciting. An
ideal pediatric adjustable IOL implant should be
biocompatible, allow for safe repeatable adjustment
procedures performed at any time after cataract
surgery; and have an adequate refractive error
adjustment range. As of today, this ideal adjustable IOL
does not exist. However, the concept of such and IOL
is being developed and after certain modifications, such
an IOL may become available.
Each of the multifocal IOLs represents a compromise
based upon the simultaneous vision principle. Two or
more images are formed on the retina at the same time,
one image at near and the other at distance focus. The
brain selects the image it wants to see. Some loss of
contrast is inherent to simultaneous vision since the
available light is split between the near focus and the
distance focus. Uncorrected refractive error (cylinder
of more than 1 diopter or the changes in sphere that
occur with eye growth) may result in more significant
blur because of the simultaneous vision concept.
Alternating vision, which is provided by a monofocal
IOL and bifocal glasses, results in only one object being
in focus at a time and all incoming light is directed to
this focus. While the increased use of multifocal and
accommodative IOLs for implantation during the
teenage years is predictable, we would caution surgeons
that these lenses may not be advantageous in growing
or amblyopic eyes. With residual refractive error,
especially the myopia that develops after eye growth,
multifocality may (ironically) result in more spectacle
dependence compared to a monofocal IOL with residual
myopia. This deserves further study.
The vast majority of children undergoing secondary IOL
implantation have had a primary posterior capsulotomy
and anterior vitrectomy. If adequate peripheral capsular
support is present, the IOL is placed into the ciliary
sulcus or in the reopened capsular bag. Viscodissection
and meticulous clearing of all posterior synechiae
between the iris and the residual capsule is mandatory.
The most common IOL used in secondary implantation
is the 3-piece AcrySof® IOL. However, decentrations
can occur, especially in eyes with large anterior
segments and axial length measurements greater than
23 mm. When inadequate capsular support is present
for sulcus fixation in a child, implantation of an IOL is
not recommended unless every contact lens and
spectacle option has been explored fully. Anterior
chamber IOLs and scleral or iris-fixated posterior
chamber IOLs are used in children when other viable
options are absent but the long-term consequences of
these placements are unknown.
Postoperative medications and Follow-up: A
drop of dilute (5 %) Povidone iodine should be placed
on the operative eye immediately after surgery. An
antibiotic steroid and atropine ointment should be
placed. A patch and Fox shield are placed over the eye.
We prefer to secure the shield with 2 Tegaderm sheets
instead of standard tape. The patch and shield should
remain on the eye until the morning after surgery. We
remove it in the office, examine the eye and show the
parents how to apply the postoperative drops. There
are some variances from the protocol in certain
situations. With older children, the atropine may be
deleted. Babies who are left aphakic do not receive the
ointment. We use topical drops for these eyes, and
rather than patching the eye, we apply a Silsoft contact
lens (usually a 7.5 base-curve and +32 D or +29 D
power) at the end of surgery. The parents can then begin
the drops right away. For older children (above age 6-
7 years), the parents are allowed to remove the patch
and shield 4-5 hours after the surgery and begin the
postoperative drops. The eye is still examined on the
first postoperative day. Topical atropine (0.5% in
children less than 1 year of age, and 1% thereafter) is

406 Kerala Journal of Ophthalmology Vol. XX, No. 4
utilized once per day for 2 - 4 weeks in children up to
age 6 years. Topical steroid is used topically 6 times
per day for 2 weeks and then 3 - 4 times per day for an
additional 2 weeks. An antibiotic drop (the same
fluoroquinolone used pre-operatively) is used for one
week after surgery. Any residual refractive error is
corrected after the wound stabilizes and the synthetic
absorbable sutures dissolve. We rarely use oral steroids
except in some uveitis patients or some trauma cases.
We schedule postoperative examinations at 1 week, 4
weeks, 3 months, and 6 months postoperatively. We
also consider a yearly EUA in order to measure
intraocular pressure, examine the peripheral retina,
monitor eye growth using A-scan ultrasound and
examine the position of the IOL and detect any
secondary membrane or after-cataract formation. Once
children become old enough and cooperative enough
to undergo these examinations awake, the yearly EUA
becomes unnecessary.
In summary, pediatric cataract surgery is a complex
issue best left to surgeons that are familiar with its long-
term complications and lengthy follow-up. Cataract
surgery in children is the first stepping-stone in the long
road to visual rehabilitation, not the end of the journey.
Consideration of a clear visual axis and corrected
refractive error are very important to the visual outcome
of children as they grow and develop. Postoperative
complications may develop in the early postoperative
period, or after many years, making it crucial to follow
these children closely on a long-term basis after
pediatric cataract surgery. Management of residual
refractive error, amblyopia, and strabismus must be
customized to each child based on measurements that
can be a challenge to obtain, and which can change
over time. Despite these uncertainties, diligent
teamwork involving the physician and the parents can
result in a gratifying outcome for the long-life of the
child.
References
1. Johar SR, Savalia NK, Vasavada AR, Gupta PD.Epidemiology based etiological study of pediatriccataract in western India. Indian J Med Sci. 2004Mar;58(3):115-21.
2. Tripathi RC, Cibis GW, Tripathi BJ. Pathogenesis ofcataracts in patients with Lowe’s syndrome.
Ophthalmology. 1986;93(8):1046-51.
3. Birch EE, Stager DR. The critical period for surgical
treatment of dense congenital unilateral cataract. Invest
Ophthalmol Vis Sci. 1996;37(8):1532-8.
4. Wilson ME, Jr., Trivedi RH, Hoxie JP, Bartholomew LR.
Treatment outcomes of congenital monocular cataracts:
the effects of surgical timing and patching compliance.
Journal of Pediatric Ophthalmology & Strabismus.
2003;40(6):323-9.
5. Lambert SR, Lynn MJ, Reeves R, Plager DA, Buckley
EG, Wilson ME. Is there a latent period for the surgical
treatment of children with dense bilateral congenital
cataracts? J AAPOS. 2006;10(1):30-6.
6. Birch EE, Cheng C, Stager DR, Jr., Felius J. Visual acuity
development after the implantation of unilateral
intraocular lenses in infants and young children. J
AAPOS. 2005;9(6):527-32.
7. Lambert SR, Lynn M, Drews-Botsch C, Loupe D, Plager
DA, Medow NB, et al. A comparison of grating visual
acuity, strabismus, and reoperation outcomes among
children with aphakia and pseudophakia after unilateral
cataract surgery during the first six months of life. J
AAPOS. 2001 Apr;5(2):70-5.
8. Wilson ME, Trivedi RH, Mistr S. Pediatric intraoperative
floppy-iris syndrome. J Cataract Refract Surg.
2007;33(7):1325-7.
9. Wilson ME, Jr., Bartholomew LR, Trivedi RH. Pediatric
cataract surgery and intraocular lens implantation:
practice styles and preferences of the 2001 ASCRS and
AAPOS memberships. J Cataract Refract Surg.
2003;29(9):1811-20.
10. Basti S, Krishnamachary M, Gupta S. Results of
sutureless wound construction in children undergoing
cataract extraction. Journal of Pediatric Ophthalmology
& Strabismus. 1996;33(1):52-4.
11. Trivedi RH, Wilson ME, Jr., Bartholomew LR.
Extensibility and scanning electron microscopy
evaluation of 5 pediatric anterior capsulotomy
techniques in a porcine model. Journal of Cataract &
Refractive Surgery. 2006;32(7):1206-13.
12. Wilson ME, Jr., Trivedi RH, Bartholomew LR, Pershing
S. Comparison of anterior vitrectorhexis and continuous
curvilinear capsulorhexis in pediatric cataract and
intraocular lens implantation surgery: a 10-year
analysis. J AAPOS. 2007 Oct;11(5):443-6.
13. Wilson ME, Jr. Anterior lens capsule management in
pediatric cataract surgery. Trans Am Ophthalmol Soc.
2004;102:391-422.
14. Jacobs DS, Cox TA, Wagoner MD, Ariyasu RG, Karp CL,
American Academy of O, et al. Capsule staining as an
adjunct to cataract surgery: a report from the American
Academy of Ophthalmology. Ophthalmology.
2006;113(4):707-13.
15. Nanavaty MA, Johar K, Sivasankaran MA, Vasavada AR,
Praveen MR, Zetterstrom C. Effect of trypan blue
staining on the density and viability of lens epithelial
cells in white cataract. J Cataract Refract Surg.
2006;32(9):1483-8.

December 2008 R.H. Trivedi et al. - Pediatric Cataract Surgery 407
16. Werner L, Apple DJ, Crema AS, Izak AM, Pandey SK,Trivedi RH, et al. Permanent blue discoloration of ahydrogel intraocular lens by intraoperative trypan blue.J Cataract Refract Surg. 2002 Jul;28(7):1279-86.
17. Wilson ME, Jr., Trivedi RH. Low molecular-weightheparin in the intraocular irrigating solution in pediatriccataract and intraocular lens surgery. Am J Ophthalmol.2006;141(3):537-8.
18. Vasavada AR, Trivedi RH, Apple DJ, Ram J, Werner L.Randomized, clinical trial of multiquadranthydrodissection in pediatric cataract surgery. Am JOphthalmol. 2003;135(1):84-8.
19. Vasavada AR, Trivedi RH, Singh R. Necessity ofvitrectomy when optic capture is performed in childrenolder than 5 years. Journal of Cataract & RefractiveSurgery. 2001;27(8):1185-93.
20. Vasavada AR, Trivedi RH, Nath V. AcrySof intraocularlens implantation in children. J Cataract Refract Surg.2004;In press.
21. Vasavada AR, Trivedi RH, Nath V. Visual axis opacificationafter AcrySof intraocular lens implantation in children.J Cataract Refract Surg. 2004;30(5):1073-81.
22. Vasavada AR, Trivedi RH. Role of optic capture incongenital cataract and intraocular lens surgery in
children. J Cataract Refract Surg. 2000;26(6):824-31.
23. Trivedi RH, Wilson ME, Jr., Facciani J. Secondaryintraocular lens implantation for pediatric aphakia. JAAPOS. 2005;9(4):346-52.
24. Trivedi RH, Wilson Jr ME, Bartholomew LR, Lal G,Peterseim MM. Opacification of the visual axis aftercataract surgery and single acrylic intraocular lensimplantation in the first year-of-life. J AAPOS.2004;8:156-64.
25. Gordon RA, Donzis PB. Refractive development of thehuman eye. Arch Ophthalmol. 1985;103(6):785-9.
26. Trivedi RH, Wilson ME. Biometry data from caucasianand african-american cataractous pediatric eyes.Investigative Ophthalmology & Visual Science.2007;48(10):4671-8.
27. Wilson ME, Jr., Trivedi RH, Buckley EG, Granet DB,Lambert SR, Plager DA, et al. ASCRS white paper.Hydrophobic acrylic intraocular lenses in children. JCataract Refract Surg. 2007 Nov;33(11):1966-73.
28. Tassignon MJ, De Veuster I, Godts D, Kosec D, Van denDooren K, Gobin L. Bag-in-the-lens intraocular lensimplantation in the pediatric eye. J Cataract RefractSurg. 2007;33(4):611-7.

408 Kerala Journal of Ophthalmology Vol. XX, No. 4
Investigations in Microbial KeratitisDr. Jyothi P T MS
Microbial keratitis is a common cause of ocular
morbidity and blindness. Different types of bacteria,
virus, fungus, parasites can invade the cornea if the
normal corneal defense mechanism is compromised.
Although some keratitis have very distinctive
appearance, it is not easy to identify the responsible
organisms based on the morphological appearance of
the corneal lesion alone. Since the clinical appearance
of infective keratitis may sometimes be misleading
(eg. A ring infiltrate can be caused by fungus,
acanthamoeba, herpes simplex or even pseudomonas),
laboratory investigations are often required for
identifying the causative organisms.
Different steps in the microbiological diagnosis of
Corneal infections are
1) Proper specimen collection
2) Direct microscopic examination of the smear
3) Innoculation of material into various culture media
and isolation of organisms
4) Demonstration of antigen and antibodies.
Proper Specimen collection
The technique of proper specimen collection is very
important in the recovery of organisms. This can be
done under slit lamp biomicroscope or by using a simple
magnification device with the patient lying supine.
Sterile precaution should be taken to avoid
contamination. Proparacaine 0.5 % is the ideal local
anaesthetic since it has the least inhibitory effect on
organism recovery. Scrapings should be taken from the
edges and base of the ulcer using blunt spatula, No. 15
Bard Parker blade or hypodermic needle.(Fig 1) All
overlying loose material should be removed before
scraping. The scraped material is smeared on to glass
slide and inoculated into the culture media. Deep
stromal lesions and progressive lesions with initial
negative cultures may require corneal biopsy to obtain
adequate specimen.
Department of Ophthalmology, Calicut Medical College
Corneal scrapings not only provides material for
microbiologic diagnosis, but also debrides the necrotic
tissues and enhances antibiotic penetration.Other than
corneal scrapings, contact lens case and solutions,F.B’s
on the cornea, corneal biopsy specimen and corneal
button after keratoplasty are some of the useful samples
for microbiological examinations in certain situations.
Direct microscopic examination
Direct microscopic examination of smear is important
because it help us to determine the type of organism
(whether bacteria, fungus, acanthamoeba) is present
and to start appropriate treatment.
Commonly used stains for evaluation of smears are
gram stain, giemsa stain and Ziehl-Neelson stain.
Flurochromic stains like acridine orange and Calcoflour
white requires a fluorescent microscope.
Fig. 1. Method of corneal scraping
CURRENT
CONCEPTS

December 2008 Jyothi P.T. - Investigation in Microbial Keratitis 409
Gram stain is used to detect bacteria, fungal hyphae,
yeasts and cysts of acanthamoeba. It differentiates
bacteria into two groups based on the difference in the
cell wall: gram positive gram +ve appears bluish purple
and gram negative –ve appears pink.
Giemsa stain is useful to detect bacteria, fungi, cysts of
acanthamoeba, viral and chlamydial inclusion bodies.
Also detects cellular response. In viral keratitis Giemsa
stained smears will show mononuclear cells, PMNs and
eosinophilic intranuclear inclusion bodies.
Ziehl-Neelson stain detects mycobacteria as well as
nocardia.
Acridine Orange detects bacteria, fungi and
acanthamoeba
Calcoflour white detects fungi and acanthamoeba
Potassium Hydroxide (KOH) wet mount – 10 %
Highly sensitive and very reliable test for recognition
of fungal filaments (fig 2) and acanthamoeba cysts.
Thin branching filaments of nocardia can also be seen.
Scraped material is spread on a clean glass slide, one
drop of 10 % KOH is added. Coverslip placed on it and
examined under low power and high power. 10 % KOH
clears the cellular debris and make the hyphae
fragments more refractile and prominent. It can be used
alone or with ink or lactophenol cotton blue (LPCB)
Gomori Methenamine Silver stain is the best stain for
visualization of fungi. Cell wall and septa stain black
against the light green background. It is time consuming
and difficult to perform. (Fig. 4)
Lactophenol Cotton Blue mount - very useful to detect
fungi and acanthamoeba. (Fig. 3)
Identification of organisms by culture
Corneal infections usually yields very small quantities
of material for culture.Therefore direct innoculation
of scraped material onto the culture medium improves
the yield of culture.
Commonly used media and organisms isolated
Standard media
1. Blood agar plate- Standard media for the isolation
of aerobic bacteria It also supports the growth of
many fungi . Fusarium grows well in blood agar.
(Fig. 5).
2. Chocolate agar- Haemophilus,Neisseria and
Moraxella grows well in Chocolate agar
3. Sabouraud’s dextrose agar-Universal media for the
fungus.Most ocular fungi demonstrates growth
within 2-3 days, but wait for atleast 2 weeks before
considering culture as negative.
4. Thioglycollate broth - Supports the growth of a
number of aerobic and anaerobic bacteria. Contains
basic nutrients supporting the growth of aerobic
Fig. 2: KOH Mount
Fig. 3. Lactophenel cotton blue mount showing a new of
Aspergillus
Fig. 4: Gomori Methenamine silver stain
Fig. 5: Aerobic bacteria in blood agar

410 Kerala Journal of Ophthalmology Vol. XX, No. 4
bacteria and sulfhydril compounds that act as
oxygen reducing agent to facilitate growth of
anaerobic bacteria.
Additional media
5. Non nutrient agar plate with E coli overlay-This
media is used for the growth of acanthamoeba.The
organisms consumes E coli and the migrating
organisms are seen as tracks.
6. Thayer martin agar plates-Chemically enriched
chocolate agar that suppress the growth of inhibitory
contaminants and allows isolation of Neisseria.
7. Brain Heart Infusion broth with Gentamicin-Liquid
media. Enhances the recovery of filamentous fungi
and yeasts
8. Lowenstein Jenson Agar plate-Supports the growth
of mycobacteria
Innoculation in plates should be done in multiple “C”
Streak pattern (Fig. 6)which facilitates differentiation
of valid growth from contaminants.Growth of the C
streak is considerd significant whereas growth outside
C streak is considerd as contaminants.
in viral transport medium and sent to the
laboratory.With herpes simplex, cytopathic effects are
seen within 24- 48 hrs, but may take as long as 7 days.
Detection of antigens and antibodies
Detection of various microbial antigens in tissue
specimens help in the rapid diagnosis of infection.Direct
immunofluorescence staining of smears with fluorescein
conjugated monoclonal antibody against HSV
glycoprotein is a rapid diagnostic test, but requires a
fluorescent microscope. Enzyme linked immunosorbent
assay (ELISA) tests identify different antigens in
specimens.Serological tests to detect IgG and IgM
antibodies are useful for the detection of viruses and
microsporidia
Limulus lysate test
It is a fairly accurate and quick test for detecting
endotoxins in corneal specimens. Endotoxin is a
lipopolysaccharide in the cellwall of gram negative
enteric organism and its detection would indicate that
one of these organisms were present in the specimen.
The horseshoe crab limulus polyphemus produces cells
coelomic amoebocytes which cause clotting when
exposed to endotoxin. The endotoxin activation of the
coagulation pathway has been adapted as a sensitive
in-vitro assay for the presence of bacterial
lipopolysaccharide. Corneal scrapings are emulsified
in a test tube with amoebocyte lysate reagent. If
endotoxin is present, a visible clot is formed.
Polymerase Chain Reaction(PCR)
PCR is an effective method of detecting very small
quantities of microbial DNA or RNA in samples. Any DNA
or RNA that matches the probe DNA sequence is amplified.
Appropriate probes must be determined for each
organism tested.The DNA or RNA sequence of the probe
must be unique to the organism.Very useful test for the
detection of viruses, acanthamoeba and microsporidia.
Test is expensive and false negatives can occur.
Confocal microscopy
Confocal microscopy is a new imaging technique which
provides an optical section of the tissues and provides
An isolate is likely to be significant if
1. Smear results are consistent with culture.
2. Same organism is grown in more than one media
3. Same organism is grown in repeated samples
In all cases, the results should be correlated with the
clinical features
Cell culture for isolation of Viruses
The isolation of virus in tissue culture provides a
definitive diagnosis.The lesion is swabbed and placed
Fig. 6. Innoculation as C Streak pattern

December 2008 Jyothi P.T. - Investigation in Microbial Keratitis 411
images from different depths. Although not widely
used, it is useful in the detection of cysts of
acanthamoeba and fungal filaments in vivo. It can also
detect parasites like microsporidia and certain bacteria.
In the diagnosis of microbial keratitis, use
tests which are sensitive, specific and
affordable and use them selectively. Careful
clinical examination and direct miscroscopy of
corneal scrapings stained by simple methods
allows a rapid presumptive aetiological
diagnosis. Where facilities are available,
culture of organism should be done in all cases
of moderate to severe microbial keratitis.
References
1. Daniel M. Albert,Frederick A Jakobiec Priciples andpractice of Ophthalmolgy. vol 2
2. Graysons disea se of cornea
3. Krachmer, Mannis, Holland, Fundamentals of corneaand external diseases
4. Jayahar M.Bharathi, M.Sreenivasan, R. Meenakshi,S.Padmavathy, Prajna M. Lalitha A study of spectrumof acanthamoeba keratitis, IJO 2007; 55: 37-42.
In a lighter vein
Of Protocols, Procedures and PracticesRRV
Let me assure you, the words in the title are not
used in a clinical sense. It is actually part of the title
of a book dealing with conduct of official meetings.
This fictious book invented by yours truly in self
defense has saved the situation (and my face) more
than once.
Our Society conducts a lot of meetings now. The
bigger of them are conducted with more formalities
and protocols. Many are the funny moments
generated in some of them. The non-Ophthalmic
MCs and speakers stumbling on ophthalmic terms
are one category. Ophthalmic MCs and speakers
doing the same with general terms are equally
hilarious.
The first ritual in any major meeting would be the
investiture of the President. Surprisingly many of
our MCs are not familiar with the term ‘invest’ or
‘investiture’. Many may know that it is something to
do with the Presidential collar. The funniest usage
was heard in the SROC meeting in a provincial town
in A.P., where the MC invited the Secretary to “collar”
the President. He definitely must have been unaware
of the nuances of the many meanings of ‘collaring’.
In another venue I heard the Secretary being invited
to “put the collar on the President”. Really it invoked
canine images! In one of our annual conferences
the MC (a senior Ophthalmologist who wouldn’t
listen to any advice) preferred a more flowery and
regal sounding “adorning the president with the
collar”. Two terms back, our local IMA Secretary
solved the problem in simple and straight-forward
way by announcing, “With your permission I am
putting ‘this thing’ on the President”. (But then he
substituted ‘this thing’ for any word/phrase that did
not occur to him in time).
Many of our MCs and speakers seem to feel that
stage is for performances and a meeting is conducted
on a dais. Rightly so; but most of them pronounce it
as ‘dias’ and as ‘diayas’ once in a while.
Another word which is most usually mispronounced
is ‘memento’, meaning things given away to
remember the occasion by. Recently in a ‘mega’ CME
conducted hereabouts, a willowy MC with ‘convent’
English and a put on accent took on the floor. First
she got the name of the chief guest wrong and later
blithely announced, “Now Dr. So and so will give a
MOMENTO to the chief guest”. The chief guest gave
me, who was supposed to do the honours, a startled
look. Later, realising the true meaning, murmured:
“Thank God, it is not MOMENTUM”.

412 Kerala Journal of Ophthalmology Vol. XX, No. 4
Parasitic KeratitisDr. Ranjakumar MS MBA(HM)
Various parasitic infections are important causes of
ophthalmic diseases worldwide.Most parasitic
infections are spread by insect vectors or consuming or
getting contact with contaminated water.There are
fairly obvious reasons why parasitic diseases are found
mainly in tropics:
� The warm climate encourages the growth and
survival of the parasites
� The warm climate encourages the insect vectors
� Poor sanitation and poor water supply makes the
food/water contaminated
� People live in close contact with domestic animals
which are involved in the life cycle of some
parasites
Various organisms producing keratitis are the following:
Acanthamoeba
Microsporidia
Onchocerca
Leishmania-
Trypanosoma bruci
Echinococcus granulosus
Crab louse –Marginal Keratitis(IJO 1976-Dr.Ittyerah)
Other free living amoeba –Vahikampia/Hartmanella
Acanthamoeba keratitis
Background
These amoebae are distinct from other pathogenic
protozoa. They have a free living existence, have no
human carrier state(which is important in disease
transmission), and have no insect vector.
The pathogenic species of Acanthamoeba known to
produce keratitis are the following
1. A castellani
2. A polyphaga
3. A hatchetti
4. A culberstoni
5. A rhysodes
6. A griffina
Out of these castellani and polyphaga are commonly
associated with keratitis whereas culberstoni is rarely
encountered but highly virulent.
Life Cycle
The life cycle consists of 2 stages:
1. Trophozoite (14-40 μm in diameter)
2. Cyst (12-16 μm diameter & a double layered wall)
Dept. of Ophthalmology, Medical college, Kozhikode
Acanthamoeba genus causes 3 clinical syndromes .
Granulomatous amoebic encephalitis, Disseminated
granulomatous amoebic disease (eg- skin, sinus, and
pulmonary infection) Amoebic keratitis.
Patients who develop the first two are usually
immunocompromised whereas those who develop
keratitis are immunocompetent.
Fig. 1. Isophozotic and Cyst of Acanthamoeba
CURR EN T
CONCEPTS

December 2008 Ranjakumar - Parasitic Keratitis 413
Acanthamoeba was first established as a case of human
disease in1973
This vision threatening corneal disease was first
recognized in contact lens wearers.
There was a sharp increase in the recognition(and
perhaps incidence ) of this disease in the late 1980’s.
First case of Acanthamoeba keratitis from India was
reported in 1987 from Aravind Eye Hospital, Madurai
Epidemiology
Acanthamoeba are free living, ubiquitous pathogenic
protozoa. They are isolated from soil,water(including
natural and treated) air and dust. Most persons appear
to have been exposed to this organism during their life
time as 50-100 % of healthy people have serum
antibodies against acanthamoeba. Studies have also
demonstrated that this amoeba can be cultured from
nasopharynx of healthy individuals. Acanthamoeba
cysts are very resistent to chlorine. It converts from
trophozoites to more durable cyst form during
unfavourable conditions, making the organism highly
resistant to killing by desiccation, irradiation or
chlorination. Acanthamoeba thrives in soil, ponds,
swimming pools and contact lens solution.
Despite widespread prevalence in nature, the incidence
of keratitis is low because, it is a weak pathogen and
there is a high degree of innate host resistance.
Trophozoites are probably more important than cysts
in initiating keratitis.
The incidence of Acanthamoeba keratitis accounts
for 1-4 % of proved keratitis. Mud as a cause for corneal
trauma resulting in Acanthamoeba keratitis is
significantly more than any other material. Contact lens
wear does not emerge as an important risk factor for
the development of Acanthamoeba keratitis in our
population.
Pathophysiology
The occurrence of infection is multifactorial. .Keratits
occurs in patients with minor corneal trauma. Minor
trauma in western countries is due to content lens wear.
Amoeba are introduced via contaminated solution or
wearing lenses while swimming. All types of content
lens can predispose to this. In our country, people
belonging to poor socio economic strata are affected
(who are using unclean, contaminated water for
washing eyes). 60 % of cases in our country are due to
ocular trauma. Humans come into contact with amoeba
while swimming in lakes, pools, sea water and also on
contact with mud and tap water. This direct exposure
combined with minor trauma leads to corneal infection
Clinical features
Patients will have similar symptoms as with other forms
of keratitis, but pain will be out of proportion to the
findings.
Clinical signs are discussed in three stages
1. Early stage Epithelial defects, epithelial haze,
pseudodendrites
2. Late stage Epithelial defects, stromal
infiltrates, nummular keratitis
3. Advanced stage Ring infiltrate, satellite lesions,
stromal abscess (Fig. 2 a-d)
Other features
- Severe anterior and posterior uveitis
- Nodular or Diffuse scleritis
- Corneal stromal infiltrates (single,multiple,ring shape)
- Anterior uveitis (transient hypopyon)
- Radial keratoneuritis
- Disciform keratitis
Fig. 2. Clinical findings in acanthamoeba keratitis
(a) epithelial haze (b) pseudo dendrites (c) Ringinfiltrate (d) stromal abscess

414 Kerala Journal of Ophthalmology Vol. XX, No. 4
Clinical characteristics that help to distinguish
Acanthamoeba keratitis from other keratitis include the
following:
1. Ring infiltrate
2. Elevated epithelial lesion
3. Relative lack of vascularisation even in chronic and
severe cases
Clinical Diagnosis
Acanthamoeba keratitis poses a diagnostic challenge
because of its similarity to fungal and viral keratitis.
Most often Acanthamoeba keratitis in early stage is
misdiagnosed as herpes simplex keratitis, and in late
stage as fungal keratitis. There will be a history of
trauma with soiled water, organic matter, and rarely
contact lenses. Adults engaged in outdoor work are
affected mainly. Suspect when the response to antiviral
or antibiotic drugs is poor or absent. Patient might
have had several consultations with different
Ophthalmologists before a proper diagnosis is
established.
Laboratory Diagnosis
Acanthamoeba trophozoites or cysts can be
demonstrated in corneal scrapings or a biopsy sample
via wet mount, stains, histopathologic examination or
culture
10% KOH wet mount is used routinely as an initial
procedure to identify cysts and to exclude fungi.
Sesitivity of this test is almost equal to Calcoflour white.
Motile trophozoites may be seen in a wet mount
preparation.
Stains commonly used are
Geimsa Cysts & Trophozoites stain
purple
Lactophenol cottonblue Cyst wall stains green/
Trophozoite red
Gram Cysts show as multisided
gram positive crystals
Calcoflour white Cyst wall stains green/
trophozoite red
PAS
Other diagnostic options :
Indirect fluorescent antibody staining
Confocal microscopy: This provides in vivo views
of the cornea and delineates both trophozoites and
cysts. The double walled cysts are particularly prominent
and radial keratoneuritis can be appreciated. This can
also be used to monitor the patient on treatment.
Equipment is costly and is available only in specialized
centres. If corneal specimens are unremarkable consider
culturing contact lens or cleansing solution for amoeba
Culture Acanthomeba could be isolated by inoculating
the specimen on non nutrient agar with E.coli overlay.
The plate should be incubated for more than a week.
Acanthamoeba feed off the bacteria, leaving linear
tracks(migration tracks/snail tracks) in the plates.
Tissue specimens.corneal smears, contact lenses and
swabs may be kept in Page’s saline (phosphate buffered
saline) and sent to lab, if materials for culturing are
not available (fig 7)
An alternative to non nutrient agar has also been
described.Corneal scrapings may be inoculated in
tissue culture flask containing suspension of E.coli in
¼ Ringer solution. The flask is incubated at 37ºC and
examined daily for trophozoites using an inverted
microscope.
Superinfecting bacteria can complicate the diagnosis and
isolation of bacterial pathogen does not exclude
Acanthamoeba as the cause for keratitis
Treatment
There is no consensus on treatment. Various regimens
are described. Treatment is required for 6-12 months.
Prolonged medication results in corneal vascularisation
and toxic keratitis.
Fig. 7. Acanthomeba in culture on non nutrient agar withE. Coli overlay

December 2008 Ranjakumar - Parasitic Keratitis 415
Drugs used are:
1. Aromatic diamidines - Propamidine isethionate
0.1 %
Dibromopropamidine
ointment 0.15 %
(Brolene eye ointment,
not avialble in India)
2. Aminoglycosides - Neomycin
3. Imidazole & Triazole antifungals
4. Polymyxins
5. Cationic antiseptics - Polyhexamethylene
biguanide (PHMB)
0.02 %
Chlorhexidine 0.02 %
Primary agents used are biguanides as they are both
trophocidal and cysticidal and also less toxic to cornea
than aminoglycosides and antifungals.
Drug Trophicidal Cycticidal
Chlorhexidine + +
PHMB 0.025% + +
Propamidine 0.1% + +
Neomycin + -
Clotrimazole + -
Initial approach can be-
1. Cationic antiseptics in combination with neomycin
and propamidine.
2. A combination of topical biguanide and diamidine
therapy.
(Pentamidine is not available in India)
Treatment is divided into three phases
1. Loading dose - On days 1 to 3.The patient is given
chlorhexidine or PHMB and propamidine with or
without neomycin. Each drug is given hourly.
2. Intensive treatment - On days 4 to 7.Above
regimen is repeated, 2hrly during day and 4hrly at
night.
3. Maintenance phase. From day 8 onwards for
atleast 4 months-chlorhexidine or PHMB with or
without propamidine 6hrly.
A regimen which can be advocated here is as follows:
PHMB 0.02% hrly for 1week, 2 hrly for 2 weeks, 4 hrly
upto 8 weeks.
If no toxicity,continue 4-6 hrly till it heals,which may
require nearly 1 year.
(Prolonged use of PHMB promotes corneal vascularistion
which is reversible when drug is tapered/withdrawn)
Combine Adjuvant therapy
Topical steroids is controversial as it will foster
conversion of cyst to trophozoite
Systemic therapy
Itraconazole/ketaconazole 600mg/day orally
Pentamidine IV in recalcitrant cases 4 mg/kg/d i/v. After
first 3 doses reduce to 3mg/kg/d to minimise toxicity
Surgical treatment
Epithelial debridement: Effective in early phase
in combination with antimicrobials.
This will improve penetration of the drug and facilitates
removal of pathogen
Penetrating keratoplsty: Timing of sugery is
critical. It is unwise to perform keratoplasty before
infection is controlled or organism is fully eradicated,
otherwise graft recurrence will occur. But if impending
perforation is seen, keratoplasty may be done,with risk.
Optical graft may be done after complete resolution of
infection.
In general,treatment of Acanthamoeba keratitis has
been disappointing, partly because the infection is
frequently well advanced before diagnosis and partly
because the available treatment is suboptimal.
Successful treatment requires early diagnosis and
aggressive medical and surgical management.
Conclusion
Acanthomeba keratitis is a challenging disease to
Ophthalmologists. Prevention is the only method till
we get a specific drug. Contaminated water is the source
of infection in our region hence prevention is a difficult
task.

416 Kerala Journal of Ophthalmology Vol. XX, No. 4
Microsporidiosis
Microsporidians are obligate intracellular parasites and
are omnipresent (fig 8)
Microsporidial keratitis was first described in 1973
Three species are known to cause keratitis
Encephalitozoon hellum Imuno compromised cases
Nosema corneum Immunocompetent cases
Nosema ocularum Immunocompetent
10 mg/ml suspension of fumagillin can be applied
hourly for 24 hrs and then tapered. Complete
resolution of symptoms has been reported in a period
of 3 days.
Onchocerciasis (River blindness)
The causative organism is a filarial nematode
Onchocerca volvulus which is transmitted by the
Simulium black fly. There is transplacental
transmission also
Eye disease is related with inflammatory response
generated by nematodes, which can be found in the
conjunctival epithelium, corneal stroma, iris, ciliary
body, sclera, extra ocular muscles and optic nerve sheath
Manifestations
Inter palpebral marginal keratitis, Sub epithelial
opacities, Stromal oedema due intrastromal worm are
some of its clinical manifestations. Cornea may contain
large numbers of living microfilaria. Worms are
visualized in the slit lamp on retro illumination. Calcific
band keratopathy and both anterior and posterior
uveitis may be associated with river blindness.
Microfilaria may be observed in the anterior chamber
especially in the inferior angle on gonioscopy, or seen as
moving shadows against red background with
ophthalmoscope.
Diagnosis Based upon the identification of the worm
from skin snips
Diagnosis is also confirmed by Mazzoti test: 30 minutes
after oral administration of diethyl carbamazepine
patient develops pruritis, erythema, flu like symptoms.
After the drug administration microfilaria can be
recovered from urine and blood.
Treatment
The mainstay of treatment is oral Ivermectin as single
dose (150 μgm/kg) and repeated every 6 months to
1 year.
Because of the more complex scenario as well as wide
variety of pathological manifestations,each ocular
disease has to be addressed individually, including
epidemiology, pathogenesis, diagnosis and treatment.
Fig. 8. Microsporidial spore
Microsporidial infection produces -
stromal keratitis and iritis in immunocompetent
individuals, conjunctivitis and epithelial keratitis in
immunocopromised patients.
Epithelial lesions are characterized by multiple
coarse white grey opacities and decreased corneal
luster. In addition there will be a fusiform swelling
in the inferior fornix from which microsporidia are
recovered
Microsporidians are difficult to culture, hence diagnosis
is made by direct observation of organism.On gram stain
microsporidians appear as gram positive, ovoid
intracytoplasmic iclusions
Confocal microscope can reveal the organisms,but
these organisms approach the resolution limits of this
instrument
Electron microscopy is considered the gold standard
for diagnosis
Treatment
Itraconazole Orally
Propamidine Topically
Fumagillin Topically

December 2008 Ranjakumar - Parasitic Keratitis 417
“Less-Than-Perfect Outcomes”
After An Uneventful Cataract SurgeryDr. Meena Chakrabarti MS, Dr. Valsa Stephen MS, Dr. Sonia Rani John DNB, Dr. Arup Chakrabarti MS
Astute and self absorbed patients will usually find a lot
of “little things” to feel disappointed about. Most often
lending a sympathetic ear and offering scientific reasoning
of their complaints reassures this group of trouble makers.
In the present cataract surgery scenario the patient
expectations are very high, and doubly so, for those patients
who opt to have “premium” IOLs implanted in their eyes.
When a patient complains of decreased visual function
after an uneventful cataract surgery you should have a
definite game plan. Typically we have to look for 3
things- ocular surface disease, early posterior capsular
opacification, and cystoid macular oedema. All these
causes are magnified and multiplied in the unfortunate
multifocal IOL patient.
My vision is coming and going .…..group
Posterior lid margin disease and Meibomian Gland
Dysfunction (MGD) are recognized as significant causes
of decreased quality of vision in a cataract patient. The
meibomian gland can become inflamed, the oil
abnormal or unstable, both of which may cause the
tear film to become unstable with rapid tear break-up-
time. If your cataract patient complaints that his vision
is “coming and going”, it is consistent with posterior
lid margin disease. Other tell tale signs include
telengiectasia around the gland orifice, gland dropouts,
or ‘foam’ in the tears.
Other OSDs that may cause subnormal vision includes
1. Aqueous deficiency dry eye.
2. Epithelial basement membrane debasement
A very common scenario in our day to day practice is a
disgruntled and grumpy post operative patient. This
article will focus on how to handle such a situation,
what to look for and to effectively streamline our
management options.
Majority of the cataract surgeons perform uneventful
surgeries (no intraoperative surprises) most of the time.
On few occasions we anticipate a particular intra
operative difficulty, and with good prior planning we
are able to efficiently manage the complication and give
an excellent outcome. In this situation the patient is
already counseled on the less-than-perfect outcome and
usually he willingly accepts the final visual result.
Imagine the scenario where you have performed an
uneventful cataract surgery in an uncomplicated eye
and contrary to your patient being another of your
success stories, you have a pessimistic disgruntled
individual in your OPD infecting other waiting clients
with his pessimism.
Assuming an uncomplicated procedure, some outcomes
are going to be due to patient –specific factors. For
example patients with diabetes have higher risks of
postoperative macular oedema as are patients with
preexisting uveitis and retinitis pigmentosa.
Age is also a major determinant. Wound healing is
faster in younger patients and hence there is a higher
incidence of wound dehiscence, or leaks in the
elderly.
Chakrabarti Eye Care Centre, Kochulloor, Trivandrum - 695 011
Email: [email protected]
C O M M U N I T Y
OPHTHALMOLOGY

418 Kerala Journal of Ophthalmology Vol. XX, No. 4
3. Salzmann’s disease
4. Subtle corneal oedema
Patients with aqueous deficiency, complain that their
vision gets worse as the day progresses. Salzmann’s
disease typically affects women in 95 % of cases. In the
classic form subepithelial fibrosis is easily distinguished.
However the more subtle forms of this entity may be
entirely missed unless the cornea is examined by
oblique illumination.
“Fine till I had my cataract surgery” group
“Fine until I had my surgery” group of patients
attribute all their preexisting little complaints to the
cataract surgery. A common complaint is seeing floaters-
possibly the patient just did not notice their floaters
until they had the surgery. The cataract surgery is not
the cause but may be it brought this complaint to the
forefront.
The Keratitis Medicamentosa patient
Many of our cataract patients are toxically exposed
to preservatives such as BAK present in the steroid
and nonsteroidal anti-inflammatory drops that we
prescribe. Keratitis Medicamentosa is seen in a fairly
large subset of elderly postoperative patients.
Remember also to check the patients IOP regularly-
you may never know that you have a ‘steroid –
responder’ in your hands.
The Borderline OSD patient
Beware of the cataract patient who firmly believes that
the cause of his foreign body sensation is “the cataract”
and is hell bent on a surgical procedure. A good dose
of strong and effectively loaded worded counseling will
have the desired effect of dispelling the patient’s assumptions
and gives him a realistic expectation of the postoperative
outcome. In majority of this subset of patients, their
“borderline OSD” goes unrecognized before surgery. In
the surgeons eagerness ‘to cut’ he erroneously assumes
that the patients vague complaints are due to his
cataract! and the procedure tips the scale towards a
frank OSD and a disgruntled symptomatic patient.
Undetected preexisting astigmatism
Irregular astigmatism may be missed preoperatively or
we might be faced with a patient who has a subtle
Keratoconus.
The unhappy Multifocal patient
A subtle change or wrinkling in the posterior capsule
goes unnoticed by majority of patients. But for the
multifocal patient even if he is reading 6/5, subtle
changes yield visual complaints. Early Yag capsulotomy
can be advised in these patients if their visual
complaints persist.
Subtle Macular pathologies
Any one from any of the major institutes around the
world will tell you that even in patients who look
normal, OCT will pick up subtle macular pathologies
such as ripe cyst, macular drusen, partial thickness
macular hole or a vitreo macular traction. The
presentation can be very subtle and the clinician may
miss it during biomoicroscopy.
Know – your - Patient well
Retinal photo toxicity and CME are 2 other diagnosis
to ‘look- at’ in patients who have subnormal
postoperative vision.
Preoperative topography, OCT and angiography should
be used judiciously before surgery to detect subtle
changes that causes subnormal vision in a predisposed
patient. It goes a long way to ‘know your patient’ well
before subjecting him to the knife. An unhappy patient
spoils the day for you and your team and it really takes a
lot of effort to pacify him and even more hard work to make
him come back to you for his other eye cataract surgery.
A thorough preoperative evaluation, meticulous
examination of the ocular surface, reliable refraction
and Keratometry, ocular imaging to rule out subtle
macular pathogenesis all go a long way in ensuring
that your patient’s postoperative recovery is free of
surprises. The role that preoperative counseling plays
needs no emphasis especially in patients who opt for
premium multifocal IOLs.

December 2008 M. Chakrabarti et al. - Less than perfect outcomes after cataract surgery 419
Ocular Contusion Injury Due to Pelting with
Hard Boiled EggsDr. Meena Chakrabarti MS, Dr. Valsa Stephen MS, Dr. Sonia Rani John DNB, Dr. Arup Chakrabarti MS
Blunt injuries account for 51 % of all ocular injuries 1
with the majority of the retinal lesions being unilateral.
Reports in literature have included injury with bungee
cords, water balloons, golf balls, paint balls 2, 3,4 etc.
In this case report, we present the clinical features
and management of a rather severe blunt injury in a
young man following a surprisingly trivial
trauma………….a thrown hard boiled egg that hit
his eye.
Mr. X; a 22 year old computer operator was cooking
his dinner when a difference of opinion occurred
between himself and his friend. He was pelted
with several unshelled hard boiled eggs one of which
struck him in his right eye. Although he had pain
and the eye became red, he sought medical aid only
after 2 days.
Ocular examination revealed a visual acuity of 6/60 in
the right eye, a soft eye with unrecordable intraocular
pressure, uveitis with 1 mm hypopyon, and fundus
showing an increased physiological cupping, traumatic
retinal whitening and evidence of retinal contusion at
the macula ( Fig 1). Optical coherence tomography
showed evidence of intra retinal oedema with increased
retinal thickening and a subfoveal serous retinal
detachment Fig(2). He was started on topical and
systemic steroids, cycloplegics and topical as well as
systemic nonsteroidal anti inflammatory agents. When
the patient was reviewed after one week he had
symptomatic improvement, his visual acuity was 6/36
Chakrabarti Eye Care Centre, Kochulloor, Trivandrum 695 011
Email: [email protected]
Fig 1 a showing traumatic
retinal whitening inthe right
Fig 1 b showing normal retinain the left
Fig 2 Optical coherence tomography showing subfovealserious detachment in the right eye
improving with pin hole to 6 /24, N8;
the anterior
segment reaction had subsided well and his tension
applanation reading was 16 in the injured eye. He was
kept under follow up while the medication 5 were
tapered. Within a period of 2 weeks he showed
remarkable improvement with a visual acuity of 6/9
N6, no evidence of anterior chamber reaction and a
fairly normal appearance of the macula. (Fig. 3). Repeat
optical coherence tomographic scan showed good
resolution of subfoveal serous retinal detachment in
the macula
C A S E
R E P O R T

420 Kerala Journal of Ophthalmology Vol. XX, No. 4
angiography shows blocked choroidal fluroscence in
the early phases of the angiogram followed by intense
retinal pigment epithelial staining.
Histopathological studies 5, 6, 7 have shown that in severe
forms of contusion, the retinal opacification
corresponded to the areas of fragmented photoreceptor
outer segments. There was associated intracellular
oedema of the retina glia, loss of apical processes of
the retinal pigment epithelium, disruption of RPE
plasma membrane and formation of microcystic spaces.
No specific treatment has been found beneficial in either
retinal concussion or contusion.
Conclusion
This case is presented as a novel cause of ocular
contusion injury due to pelting with a hard boiled egg.
Since the patient had only a retinal contusion,
spontaneous recovery with good visual results and no
permanent sequlae was observed.
References
1. Ligget PE, Pince KJ, Barlow W et al Ocular trauma inan urban population: review of 1132 casesOphthalmology 97:581-584, 1990
2. Bullock J D, Ballal DR et al. Ocular and Orbital traumafrom water balloon sling shots: a clinical,epidemiological and experimental study.Ophthalmology 104:878- 887, 1997
3. Cooney MJ, Pieramici DJ. Eye injuries caused by Bungeecords. Ophthalmology 104 : 1644- 1647, 1997
4. Fireman MS, Fischer DH et al. Changing trends in paintball sport –related ocular injury. Arch Ophthalmol 118;60- 65, 2000
5. Lien AT, Keunen JE et al. Reversible cone photoreceptorinjury in commotio retinae of the macula Retina 15:58- 61, 1995
6. Mansour AM, Green WR et al. Histopathology of
commotio retinae Retina 12:24- 48, 1992
7. Pulido JS, Blaur NP et al. The blood retinal barrier in
Berlin’s oedema. Retina J 233-236, 1987.
Fig 3 showing resolution a macular oedema after 2 weeks
Discussion
Berlin in 1873 invoked the Latin term for retinal
contusion ‘commotio retinae’ to describe a transient
whitening of the retina resulting from blunt trauma.
It can occur peripherally or within the posterior
pole region in which case it is refered to as Berlin’s
oedema.
Commotio retinae consist of two variants: retinal
concussion or the more severe retinal contusion.
Retinal concussion may be regarded as one end of the
spectrum of traumatic opacification. The initial vision
following trauma is fairly good, the grey-white changes
less dramatic and haemorrhage less frequent. The
clinical changes are reversible, with no visible late
pigment scarring and good final visual acuity. Fluroscein
angiography may show blockage of the choroidal
fluorescence by the retinal opacification. There is no
leakage of dye into or under the retina. The retinal
whitening clears spontaneously in a few days.
Retinal contusion represents the other end of the
spectrum of traumatic retinal opacification. The visual
loss is more profound, the retinal whitening more
intense and haemorrhage common. These changes are
often irreversible leading on to permanent visual loss,
macular stippling, macular hole formation or an
epimacular membrane formation. Fluorescein

December 2008 M. Chakrabarti et al. - Ocular Contusion Injury 421
Lacrimal Canaliculitis, A Case ReportDr. Bindu N. Das MS, Dr. Sisira MS
Introduction
Canaliculitis is a chronic unilateral infection of the
lacrimal canaliculus which is often overlooked and
treated unsatisfactorily. Bacteria, fungi and viruses may
all produce such infection , the most common agents
reported being actinomyces. Here we report a case of
culture positive bilateral actinomyces canaliculitis
involving both upper and lower puncti.
Case Report
A 40 year old male patient presented to us with
complaints of watering and purulent discharge from
left eye of 1 year duration, pain and swelling of the left
eyelids for 2 months. On examination his vision was
6/6 in right eye and 6/12 in left eye. Examination of
left eye showed a tender fusiform swelling in the medial
one third of left upper and lower eyelids. The
neighbouring part of the conjunctiva was inflammed.
(Fig.1) There was no tenderness and swelling in the
lacrimal sac area. The upper and lower puncti were
found to be pouting with expression of tenacious pus
on pressure over the swelling. The right eye also showed
pouting of lower puncta though it did not show
swelling. Patient was asymptomatic in the right eye.
Rest of the anterior and posterior segment was normal.
He was a known diabetic on irregular treatment.
The punctum was split under topical anaesthesia using
a fine scissors taking aseptic precautions and a thick,
tenacious purulent material was expressed from the
canaliculus. (Fig.2) The casts were removed by
performing a 3- snip procedure (Fig.3) followed by
irrigation with penicillin solution (100, 000 units). The
patient was also treated with fortified penicillin eye
drops and a course of oral penicillin. The casts collected
were sent for microbiological investigations. Repeated
irrigation with crystalline penicillin drops was done in
the right eye. A portion of collected material was
inoculated on blood agar and brain heart infusion broth.
On Gram staining the organisms appeared as gram-
Dept of Ophthalmology, Kozhikode Medical College, Kozhikode Fig. 3. The casts removed after 3-snip procedure
Fig. 2a-b showing thick tenacious purulent material expressedfrom canaliculus
Fig. 1. showing conjunctivalinflammation
C A S E
R E P O R T

422 Kerala Journal of Ophthalmology Vol. XX, No. 4
positive beaded, coccoid, thin branching filaments.
(Fig.4) The patient recovered rapidly and was left with
a slit punctum and adjoining canaliculus. The remaining
portion of the lower canaliculus was intact and was
patent. Post-operatively, the swelling, conjunctivitis and
discharge disappeared (Fig.5).
Discussion
Actinomyces israelii species is a gram-positive, cast-
forming, non–acid-fast, non–spore-forming anaerobic
bacillus. Its filamentous growth and mycelia like
colonies have a striking resemblance to fungi. They are
soil organisms, often found in decaying organic matter
(eg, wet hay, straw). It is primarily a commensal
microbe found in normal oral cavities, in tonsillar
crypts, in dental plaques, and in caries teeth and enters
the lacrimal system through the nasal passage or
indirectly by means of saliva into the conjunctiva. The
anaerobic environment also helps in the growth of the
Actinomyces in the canaliculus.
Other ocular manifestations include keratitis,
conjunctivitis, blepharitis, dacryocystitis, postsurgical
endophthalmitis, and infected porous orbital implant.
Cervico-facial actinomycosis has also been reported.
Canaliculitis usually presents as chronic watering,
redness and discharge from eye. A pouted punctum is
clinically diagnostic, although it occurs in less than
50 % of all patients who are affected. Typically, the
discharge is particulate and contains concretions.The
plica may be swollen and congested, and canalicular
swelling and overlying lid erythema are often
present.The lower lid is more commonly affected, and
the lacrimal sac and the duct are usually not
involved.The disease is most commonly unilateral.
Among the reported cases almost all were unilateral,
involving the lower lid. Bilateral and upperlid
involvement as in this case is a rare presentation.
Concretions on the lacrimal canaliculus can also be due
to Candida albicans , Aspergillus niger , Fusobacterium
species, and Nocardia asteroids.
Lab Studies
Canalicular discharge and canaliculiths may be sent for
the following studies:
� Gram stain/Giemsa stain
� Culture and sensitivity (ie, blood agar, Sabouraud,
anaerobic media)
� Special stains (ie, calcofluor white)
Treatment
Actinomycetes are usually susceptible to penicillins and
cephalosporins.
Surgical Care
Failure of resolution of canaliculitis by topical treatment
necessitates surgical exploration of the canalicular
system and removal of any casts. Extensive surgery is
not always required. A 2-snip punctoplasty, cast
removal, curettage, and probing is usually done.
Subsequent lacrimal irrigation with 1 MU of penicillin
in 10 mL of sterile water may be helpful.
References
1. Jordan DR. Dacryoadenitis, Dacryocystitis, and
Canaliculitis, chapter 57. In: Cornea- Cornea andExternal Disease: Clinical Diagnosis and Management.Krachmer JH, Mannis MJ, Holland EJ, Eds. (St. Louis,Mosby). 1997;687-693.
2. Richards WW. Actinomycotic lacrimal canaliculitis.American J Ophthalmol 1975;75:155-157.
3. Pine L, Hardin H, Turner L, Roberts SS. Actinomycoticlacrimal canaliculitis - A report of two cases with areview of the characteristics which identify the causalorganism. American J Ophthalmol 1960;49:1278-1298.
4. Sridhar MS, Gopinathan U, Garg P, Sharma S, Rao GN.Ocular Nocardia infections with special emphasis onthe cornea. Surv Ophthalmol 2001;45:361-378.
5. Sharma S. Ocular Microbiology. 1st ed. (Aravind EyeHospitals Publication, Madurai) 1988:79-84.
Fig. 4. showing positivebeaded, coccoid, thinbranching filamentson gram staining
Fig. 5. P o s t - o p e r a t i v eappearance of the eye

December 2008 Kerala Journal of Ophthalmology 423
Rips After Pricks – A Case SeriesDr. Mahesh G. MS DO DNB FRCS Ed, Dr. A. Giridhar MS, Dr. Siddharth Pawar DNB,
Dr. Ramkumar DO, Dr. Alpesh Rajput DO
Case 1: 78 year old female presented with complaints
of defective vision in right eye (OD) of 3 years duration
and recent onset of defective vision in left eye (OS)
since 3 weeks. Her best corrected visual acuity (BCVA)
in OD was 1/60 and in OS was 6/18 N6. Indirect
ophthalmoscopy and biomicroscopic examination of
right macula showed a submacular scar. Left macula
showed hemorrhagic pigment epithelial detachment
(PED) suggestive of occult choroidal neovascular
membrane (CNVM) (Figure 1a). Fundus fluorescein
angiogram (FFA) and Indocyanine green angiogram
(ICG) were done and ICG showed a plaque measuring
6.14 mm in OS (Figure 1b). During the next 2 months
visual acuity in OS dropped to 6/60 N 12. It was at this
time we advised photodynamic therapy (PDT) with
Visudyne due to sudden drop of vision in the only useful
eye. She underwent PDT followed by intravitreal
triamcinolone acetonide (IVTA) in OS. Following PDT
and IVTA, visual acuity in OS was stabilized to 6/36 N
12. Repeated fluorescein angiography confirmed the
diagnosis of RPE rip (Figure 1c and 1d).
Case 2: 72 year old gentleman came with complaints
of defective vision OD of 10 days duration and in OS of
8 years duration. His BCVA in OD was 6/36, N 36 and
in OS was 3/60. Indirect ophthalmoscopy and
biomicroscopic examination of right macula showed
haemorrhagic PED (Figure 2 a) and left eye macula
showed scarred CNVM. Digital fluorescein angiogram
(DFA) and optical coherence tomography (OCT)
confirmed the diagnosis of occult CNVM in right eye
(Figure 2b). He was advised 3 injections of intravitreal
Giridhar Eye Institute, Ponneth Temple Road. Kadavanthra. Cochin.682020
Email: [email protected]
Fig. 1. (a & b) Left macula showing hemorrhagic pigmentepithelial detachment (PED) with CNVM (c & d)showing RPE rip
Bevacizumab. First injection was given on 2.6.2008.
On follow up examination on 2.7.2008, patient came
with vision of CF at 3 meter. Clinical examination, FFA
and OCT confirmed the diagnosis of RPE rip (Figure
2c and d).
Fig. 2. (a & b) showing haemorrhagic PED with occult CNVM
in right macula (c & d) showing RPE rip
C A S E
R E P O R T

424 Kerala Journal of Ophthalmology Vol. XX, No. 4
Case 3: 69 year old female was referred here for retinal
evaluation. On presentation she complained of defective
vision left eye of 2 years duration and right eye of 15
days duration. Her BCVA was 6/24 N 18 in the right
eye and 3/60 N36 in left eye. Detailed fundus
examination by slit lamp biomicroscopy and indirect
ophthalmoscopy revealed fibrovascular PED in the right
eye (Figure 3a) and disciform scar in the left eye. DFA
and OCT confirmed occult CNVM (Figure 3b). Patient
was advised intravitreal injection of anti VEGF
Ranibizumab. On one month after the first injection
her BCVA was 6/36. On completion of third dose her
visual acuity was noted to be deteriorated to 6/60.
below the detachment is usually not visible due to the
lack of optical penetration. Also there is enhanced
reflectivity and optical penetration of the choroid in
the region with the lack of retinal pigment epithelium.
Initial good vision may deteriorate later after RPE rips.
Presence of sub RPE blood is a good indicator of rip. In
cases with RPE rip there is a substantial risk of AMD
related visual loss in the fellow eye. The risk is 37 % -
1yr, 59 % - 2 yr, 80 % - 3 yr due to PED, CNV, and RPE
tear. This is evident in our cases where there are large
scars at the macula in the fellow eyes of all the three
cases.
Anti-VEGF agents act by reducing angiogenesis and
arresting the CNVM.
The same pathology of fibrovascular tissue contraction
may be at work in RPE rips following anti-VEGF therapy.
The risk of an RPE rip should be considered with
treatment with anti-VEGF agents in cases with
fibrovascular PED.
Treatment of CNVM is aimed at regressing the vascular
elements of CNVM. Once there is conversion of vascular
network into fibrous tissue it contracts due to the
inherent property. If this is attached to the PED RPE
tear can result. Same mechanism acts in PDT and anti
VEGF treatment. This is to be kept in mind when there
is a large fibrovascular PED.
Conclusion
RPE rip can result from treatment for CNVM especially
in cases of occult CNVM with very large fibrovascular
PED in which other eye also shows severe involvement.
References
1 Schoeppner et al. Am J Ophth. 1989; 108:683-685.
2. Subramanyam A, Phatak S, Chudgar D. Large retinalpigment epithelium rip following serial intravitrealinjection of Avastin in a large fibrovascular pigment
epithelial detachment. Indian J Ophthalmol 2007;55:483-6.
Deterioration of visual acuity led to suspicion of RPE
rip (Figure 3c), which was diagnosed later with the
help of fluorescein angiography.
Discussion
RPE rip was first reported in 1981 by Hoskin et al (BJO
1981; 65:147) as a complication of serous PED in
ARMD patient. It is usually seen to occur at or along
the border of the serous RPE detachment on the side
opposite to the location of the choroidal neovascular
membrane (CNVM). FFA shows marked early
hyperfluorescence at denuded area without leak and
staining of the choroid and sclera later. Folded
epithelium mound blocks fluorescence which may leak
later. The lack of leak differentiates rip from classic CNV.
OCT image exhibits a well-defined elevation of the
neurosensory retina and double layered highly reflective
pigment epithelium. The choroidal neovascularization
Fig. 3. (a) Fibrovascular PED in the right eye (b) DFAshowing occult CNVM (c) showing RPE rip in the righteye on follow up

December 2008 Kerala Journal of Ophthalmology 425
Combined Cilioretinal Artery Occlusion and
Central Retinal Vein Occlusion -
A Case ReportDr. Valsa T. Stephen MS, Dr. Sonia Rani John DNB, Dr. Meena Chakrabarti MS, Dr. Arup Chakrabarti MS
Cilioretinal artery occlusion present in 5 % of patients
with central retinal vein occlusion giving an erroneous
picture of a poor visual prognosis. However in majority
of patients the occlusion is transient as demonstrated
in the case history given below.
A 37 year old male with no systemic illness presented
with sudden loss of vision in his left eye. On
examination, best corrected visual acuity was 6/6, N6
in the right eye and CF ½ m in the left. Applanation
tonometry was 16mm Hg in both eyes. Anterior
segment was within normal limits. Dilated fundus
evaluation showed dilated and tortous veins in the left
with few superficial haemorrhages and an area of
whitening in the superior macular region below the
superotemporal vessel.The right eye was normal
(Fig 1a & b).
The patient was started on Tab. Trental 400 mg twice
daily and dorzox eye drops 3 times. A digital fluorescein
fundus angiogram was done which revealed a non
ischemic central retinal vein occlusion in the left eye
with cilioretinal artery occlusion (Fig 2a & b). The right
Fig. 1. (a & b): Normal fundus in the right (a) and centralretinal vein occlusion and cilioretinal artery occlusion
in the left eye
Fig. 2. (a & b) FFA in the left showing non-ischaemic CRVOwith cilioretinal artery occlusion
Fig 3 Normal FFA in the right eye
eye was within normal limits(Fig 3). Blood
investigations including ESR, serum lipid profile, ANA
and LE cell were performed. He was advised a
cardiology consultation following which inj. heparin
was given. On review after 2 days, his vision and fundus
were status quo. All investigations including cardiology
work up were within normal limits. On review after
one month, his vision had recovered to 6/6 B in the
left with near complete resolution of the central retinalChakrabarti Eye Care Centre, Kochulloor, Trivandrum - 695 011,
E-mail: [email protected]
C A S E
R E P O R T

426 Kerala Journal of Ophthalmology Vol. XX, No. 4
vein occlusion and complete resolution of the
cilioretinal artery occlusion (Fig. 4).
Discussion
Cilioretinal artery usually enters the retina from the
temporal aspect of the optic disc separate from the
central retinal artery and can be seen clinically in about
20 % of eyes. Fluorescein angiographically, they are
visible in approximately 32 % of eyes 1. In a normal
flurescein angiographic sequence, they usually fill with
the choroidal circulation, about 1-2 seconds before filling
of the retinal artery.
Ophthalmoscopically, a cilioretinal artery obstruction
appears as an area of superficial retinal whitening along
the course of the vessel. The following clinical variants
have been described 2. 1) isolated ciliio retinal artery
obstruction 2) cilioretinal artery obstruction associated
with central retinal artery obstruction 3) cilioretinal artery
obstruction associated with anterior ischemic optic
neropathy. Cilioretinal artery obstruction along with
central retinal vein obstruction makes up just greater
than 40 % of cases of cilioretinal atery obstruction 2.
The venous obstruction are generally non ischemic and
therefore do not usually lead to rubeosis iridis and
neovascular glaucoma 2, 3, 4. However, it is possible for
a cilioretinal artery obstruction to be difficult to detect
in the presence of an ischemic central retinal vein
obstruction causing the incidence of rubeosis iridis to
be falsely low in this subgroup with cilioretinal artery
obstruction. Approximately 70 % of these eyes achieve
20/40 or better vision 2 with the venous obstructive
component accounting for the greatest degree of visual
loss. Fong and colleagues 5 have noted that 5 % of
patients with central retinal vein obstruction also have
cilioretinal artery occlusion. The reasons for this
association are unclear. Reduced hydrostatic pressure
in the cilioretinal artery, as compared to the central
retinal artery, may predispose the cilioretinal artery to
stasis and thrombosis in the setting of increased hydrostatic
pressure within the retinal venous system 3, 4. In addition,
swelling of the optic disc may compromise the cross
sectional area of the cilioretinal artery and lead to
reduced flow. According to Poiseulle’s law, the flow
within a blood vessel is proportional to the fourth power
of the radius of the vessel. Thus flow within a vessel
with twice the radius of a second vessel will be 16 times
that with the similar vessel.
The systemic work up for causes of cilioretinal artery
obstruction is similar to that for central retinal artery.
An extensive work up for the embolic sources is probably
not indicated however for cases of associated with CRVO.
Ocular treatment is not usually given. Studies have
shown that eyes with combined CRVO and CRAO with
recent visual loss respond well to superselective
ophthalmic artery fibrinolytic therapy with urokinase 6.
Another study showed no alternation on course of the
disease with intravitreal tissue plasminogen activator 7.
In this case, the obstruction resolved completely in one
months time with return of vision to 6/6.
References
1. Justice, J Jr, and Lehmann, RP: Cilioretinal arteries: Astudy based on review of stereo fundus photographsand fluorescein angiographic findings, Arch Ophthalmol94:1355-1358, 1976.
2. Brown, GC, Moffat, K, Cruess, AF, Magargal, LE, andGoldberg, RE: Cilio retinal artery obstruction, Retina3: 181-187, 1983.
3. Mc Leod, D, and Rig , CP : Cilio- retinal infarction afterretinal vein occlusion, Br. J. Ophthalmol 60:419-427,1976.
4. Schatz, H, Fong, ACO, McDonald, HR, Johnson, RN, Jeffe,L, Wilkinson, CP, deLaey, JJ, Yannuzzi, LA, Wendel, RT,Joondeph, VC, Angioletti, LV, and Meredith, TA: Cilioretinalartery occlusion in young adults with central retinal
vein occlusion, Ophthalmology 98: 594 - 601, 1991.
5. Fong, ACO, Schatz, H, McDonald, HR, Burton, TC,
Meberly, AL, Joffe, L, Zegarra, H, Nadel, AJ, andJohnson, RN: Central retinal vein occlusion in youngadults, Retina 12:3-11, 1992.
6. M Pagues, J N Vallee et al. Super selective ophthalmic
artery fibrinolytic therapy for treatment of CRVO. Br. J.Ophthalmol 2000 84(12) 1387-91
7. A Glacet Bernard, D Kahn et al - Treatment of recentonset CRVO with intravitreal tissue plasminogenactivator. A pilot study Br. J. Ophthalmol 2000 June84(6) : 609-13
Fig. 4. showing complete resolution of cilioretinal arteryocclusion with partial resolution of CRVO

December 2008 Kerala Journal of Ophthalmology 427
Leber’s Multiple Miliary AneurysmDr. Valsa T. Stephen MS, Dr. Sonia Rani John DNB, Dr. Meena Chakrabarti MS, Dr. Arup Chakrabarti MS
In 1912 and 1915, Theodor Leber described a disease
with similar vascular findings to Coats but which lacked
the massive subretinal exudates described by Coat. This
syndrome was later named Leber’s multiple miliary
aneurysm disease. In 1915, Leber concluded that what
he had described was merely an earlier stage of Coats
disease1. This conclusion was later reinforced by Reese2 who described an eye with Leber’s miliary aneurysm
that progressed into a clinical case of Coats disease
during long term follow up. Most authors today clarify
Leber’s disease as an early or non progressive form of
Coats 1.3. This photoessay describes the classical features
Chakrabarti Eye Care Centre, Kochulloor, Trivandrum - 695 011, E-mail: [email protected]
Fig. 1. (a) Right fundus showing multiple hard exudates in the macular region with the extensive exudation extending intothe infero temporal retina and numerous vascular anomalies. (b) Normal left fundus
Fig 3a & b Fundus fluorescein angiography showing multiple miliary aneurysms,intra retinal shunts and nonperfusion areas
in the macula and inferotemporal retina in the right eye
P H O T O
E S S A Y

428 Kerala Journal of Ophthalmology Vol. XX, No. 4
Fig 4a&b showing stable retina post sector photocoagulation in the right on review after 1 month
Fig 5a&b Right and left fundus on review after 3 months
Fig 6a&b showing new vessel anomalies in the right eye on FFA after 3 months.
of Leber’s multiple miliary aneurysm in a 34 year old
school teacher.
Case History:
A 34 year old female presented in our OPD with
complaints of blurring of vision in the right eye of 3
days duration. She had no history of any systemic
illness. On examination, her best corrected visual acuity
was 6/18, N12
in the right eye and 6/6, N6 in the left
eye. Her external eyes were within normal limits. On
dilated examination, the right fundus showed multiple
hard exudates in the macular region with the extensive
exudation extending into the infero temporal retina and
numerous vascular anomalies (Fig. 1a) suggestive of
Leber’s multiple miliary aneurysm. The left retina was
normal (Fig. 1b). A fundus fluorescein angiography
showed multiple miliary aneurysms,intra retinal shunts
and nonperfusion areas in the macula and infero
temporal retina in the right eye (Fig. 2). The left eye

December 2008 Kerala Journal of Ophthalmology 429
was normal. She underwent a sector laser
photocoagulation in the right eye. On review, the vision
had improved 6/9, N6 in the right. Fundus was stable
with no new lesion(Fig. 3). On review, after 3 months;
vision was 6/6, N6 in both eyes. Fundus looked status
quo (Fig. 4). On repeat angiogram, more aneurysms
were seen(Fig. 5) for which focal laser was repeated.
On review after 3 months, her vision and fundus are
stable. She has been advised 6 monthly review.
Discussion
Leber’s miliary aneurysm is a form of retinal
telengectasia. The retinal telengectasia are a group of
rare, idiopathic congenital, retinal vascular anomalies
characterized by dilation and tortusity of retinal vessels,
formation of multiple aneurysms, varying degrees of
leakage and deposition of lipid exudates. Retinal
telengectasia always involves the capillary bed,
although arteries and venules may also be affected. The
vascular malformations frequently progress and may
become symptomatic later in life as a result of
hemorrhage, oedema or lipid exudation. This condition
is not associated with any other systemic or ocular
disease.
Leber’s is a relatively severe form of telengectasia which
usually present in adult life with unilateral impairment
of central vision. Fusiform and saccular dilatation of
venules and arteries most commonly involving the
temporal retinal periphery are seen with chronic
leakage resulting in intra retinal hard exudate
formation. Fluorescein angiography highlights the
vascular anomalies. The treatment is by cryotherapy
or photocoagulation to ablate the vascular anomalies.
References
1. Asdourian G: Vascular anomalies of the retina. InPeyman, GA, Sanders, DR, Goldberg, MF, eds: Principlesand practices of Ophthalmology, Vol 2, Philadelphia,1980, WB Saunders.
2. Reese, AB : Telangiectasis of the retina and Coat’sdisease, Am J Ophthalmol 42:1,1956
3. Blodi, FC: Vascular anomalies of the fundus. In Duane,T, ed: Clinical ophthalmology, Vol 3, Hangerstown, MD,1980, Harper & Row.
4. Jack J Kanski.Clinical Ophthalmology-A SystemicApproach 4 th edition.1999 Butterworth Heineman

430 Kerala Journal of Ophthalmology Vol. XX, No. 4
Managing V Pattern ExotropiaDr. T.S. Surendran MS 1, Dr. Elizabeth Joseph MS 2, Dr. K. Ravisankar MS 3, Dr. Suma Ganesh MS 4,
Dr. Santhan Gopal KS MS 5, Dr. Meenakshi Dhar MS 6
Case1
A case of V pattern exotropia with inferior oblique
overaction in a young patient.
She had a best corrected visual acuity of 6/6 in both
eyes with –1.25 D Sphere given after a cycloplegic
refraction. She had a normal fundus with extorsion of
the macula. On PBCT [Prism bar cover test] in upgaze
horizontal, gaze and downgaze it was 60, 35 and
10 prism diopters on repeated examinations. Patient
had alternate suppression with free alternation.
Bilateral inferior oblique overaction was present.
The plan for surgery was decided. The clinical management
of this patient is based on the following factors:
How is it decided what component of the “V’ is
contributed by the oblique muscle overaction?
How do we decide the surgical plan- The options being
1. Two horizontal muscle surgery with vertical shift of
the horizontal muscles insertion-either bilateral
lateral rectus (LR) muscle recession, or unilateral
medial rectus (MR) resection with LR muscle recession
2. Inferior oblique muscle weakening procedure
3. Both a weakening procedure on inferior oblique with
horizontal muscle recession or resection procedure
with vertical shift of the muscle insertion
If both then what component of the exotropia would
be corrected by the inferior muscle weakening and
horizontal correction should be planned with which
PBCT value in mind.
Strabismus surgery dictums have more or less been well
estabilished, but this is one situation that may be tricky.
Experts in the field of strabismus were consulted and
their views are outlined below. To illustrate the variability
in presentation Case 2 pictures are also attached.
Dr. T.S. Surendran
A good result can be achieved in such patients by taking
the PBCT in horizontal gaze as base line subtracting
15-20 dioptres for inferior oblique overaction and then
correct the horizontal muscles and shift the insertion
1Paediatric Ophthalmolgy, Sankara Nathralaya, Chennai. 2Pediatric ophthalmology
& Strabismus services, Little Flower Hospital, Angamaly 3Sri Ramana Eye Centre,
Chennai, 4Dr. Shroff’s Charity Eye Hospital, Delhi, 5 Strabismus Consultant,
Bangalore, 6 Professor, Amrita Institute of Medical Sciences, Cochin
Case 2: Primary position 30 PD XT, upgaze 40 PD XT, downgaze- 20 PD with bilateral I O overaction.
Case 1:Primary position exotropia 35 PD, down gaze 10 pd,upgaze 60 pd. bilateral inferior oblique overactionpresent.
CONSULTATION
S E C T I O N

December 2008 Consultation Section 431
downwards in case of medial rectus and upwards in
case of lateral rectus one half of its width of insertion.
Do surgery in one sitting combining the horizontal
muscle procedure and oblique muscle weakening.
For a basic exotropia lateral rectus recession 6mm and
medial rectus resection 5mm can be done. Differential
recession of horizontal recti is another useful way of
tackling V pattern. In This for V exotropia the lateral
rectus recession would be more for the superior fibres
so that in upgaze the abduction is weakened more -
exotropia is well controlled.
Dr. Elizabeth Joseph
V pattern eso deviation or exo deviation may be with
or without inferior oblique overaction and success of
surgical procedure depends on accurate assessment and
titration of surgery. Accurate tables are not available
to guide towards proper planning of surgery and every
case should be assessed individually.
First is assessment of the angle of deviation in primary
position, 25 degrees up and down gazes and lateral
gazes to find out the horizontal deviation, amount of V
and whether obliques are overacting. Examine the
versions in extreme 9 positions of gaze to identify any
oblique overaction or underaction and do double
Maddox rod test, to document torsion. In patients with
inferior oblique overaction, there will be extorsion of
fovea as demonstrated by by indirect ophthalmoscope
or fundus photography.
Bilateral weakening of inferior oblique by recession or
myectomy can correct 15 to 20 PD of pattern and will
not affect the horizontal angle in primary position.
Vertical transposition of horizontal recti can correct
about 15 PD of pattern strabismus.
Her Surgical Straegy Is As Follows-
In a patient with primary position horizontal squint
with inferior oblique overaction and the pattern around
20 pd (difference between gaze up and gaze down =20
PD) (as in the second patient whose pictures are shown)
I will correct the deviation in primary position by
horizontal muscle surgery without any vertical shift and
tackle the V pattern by inferior oblique recession. If
the inferior oblique are not tackled in such a patient
the pattern deviation will remain.
If the difference between upgaze and downgaze is as
high as 30-40 PD in a patient with V pattern and inferior
oblique overaction (as in the first patient whose pictures
are given). I will prefer to do inferior oblique weakening
and vertical transposition of horizontal recti to change
the force vector. Some of these patients with a very
large V may have primary superior oblique paresis and
secondary inferior oblique overaction, these patients
present with very large V pattern and may require 6
muscle surgery including superior oblique tucking.
In those patients without oblique overaction , horizontal
muscle supraplacement or infraplacement along with
recess /resect procedure is good enough to correct a
moderate A OR V pattern. Horizontal transposition of
vertical recti combined with horizontal muscle surgery
in large patterns of 40 PD is associated with problems
of anterior segment ischaemia and should be
undertaken only if a vessel sparing technique is
resorted to.
Dr. K. Ravisankar
In this patient 2 aspects of the problem are correction
of the V phenomena and that of the exotropia. Bilateral
inferior oblique weakening procedures correct 15-20º
of the horizontal squint. .Bilateral lateral rectus
recession will correct the horizontal squint, if exotrpia
at distance is 15 PD more than near in primary gaze.
The primary gaze PBCT should be used to calculate
the amount of recession needed. This can be combined
with differential recession of the horizontal recti, where
the superior and inferior ends are recessed in differing
amounts making the musle insertion slanting and not
parallel to the limbus which implies that recession for
superior end of the lateral rectus is more than inferior
end. This further corrects the V pattern strabismus.
The medial rectus is always moved towards the closed
end of the ‘V’ i.e. shifted downwards if its resection is
done. Further the recessed lateral rectus is always
shifted towards the open end of the “V”.
Dr. Suma Ganesh
She also affirmed the viewpoint of doing one stage
procedure - bilateral inferior oblique weakening with
horizontal muscle surgery. Recessing the inferior oblique
would correct 15-20" of exotropia and amount of

432 Kerala Journal of Ophthalmology Vol. XX, No. 4
horizontal muscle surgery has to be calculated in
primary gaze. The insertion can be shifted half the
muscle width downwards for medial rectus and
upwards for lateral rectus.
Dr. Santhan Gopal KS
In V exotropia with inferior oblique overaction, first
thing is to note the way the recti are inserted.
If one was to imagine a line passing thru the centre of
the eye horizontally, and then see how much of the
insertion of the horizontal recti were above and below
it. There would be the following situations.
A. If LR insertion was either way more superiorly,
i.e. the horizontal line passed through the lower
half of the insertion, there is no point in further
shifting up this insertion for a patient of ‘V’
Exotropia, instead one needs to do the inferior
oblique weakening.
B. If MR insertion was either way more inferiorly,
i.e. the horizontal line passed through the upper
half of the insertion, there is no point in further
shifting down this insertion for a patient of ‘V’
Exotropia, instead one needs to do the inferior
oblique weakening.
C. If the imaginary line passes thru the centre of each
horizontal muscle insertion, shifting the insertions
vertically will help in rectifying the V pattern. The
LR insertion gets shifted half width of the insertion
upwards, and the MR insertion gets shifted
downwards.
D. If LR insertion was either way more inferiorly,
i.e. the horizontal line passed through the upper
half of the insertion, there is point in further shifting
up this insertion for a patient of ‘V’ Exotropia, thus
vertical displacement of the LR insertion would
improve V pattern exotropias.
E. If MR insertion was either way more superiorly,
i.e. the horizontal line passed through the lower
half of the insertion, there is point in further shifting
down this insertion for a patient of ‘V’ Exotropia,
thus vertical displacement by one half of insertion
width would help correcting the V pattern exotropia
He was of the opinion that shifting the horizontal
muscle insertions vertically to correct ‘V’ pattern would
help only if their insertions were either horizontal
orsuperior in MR and inferior in LR.
Exotropia can be corrected as usual with either bilateral
LR weakening or unilateral combined LR rescession and
MR resection, done at the same sitting.
Dr. Meenakshi Dhar
Decision regarding a V pattern exotropia should be
made on the table to a certain extent. Correcting only
the horizontal muscles can help in correcting a small V
pattern in many cases of exotropia, provided all the
check ligaments are released during surgery. This can
be combined with vertical displacement of the insertions
keeping in mind Dr. Santhan’s ideology (as illustrated
above) on muscle insertions. The amount of recession
and resection needed can be calculated taking the PBCT
in primary straight gaze.
Then at a second stage inferior oblique weakening can
be planned if needed. It is surprising to see how many
V patterns get corrected by just doing horizontal muscle
surgery. This leads to lesser surgical manipulation. It is
the long term results with minimal surgical handling,
which should be the goal. Neither the surgeon nor the
patient should be in a hurry.
Of course if the V pattern is large as in case 1, one
stage procedure of horizontal muscle weakening taking
the PBCT in horizontal gaze after subtracting 15 PD
can be done. The simultaneously performed bilateral
IO recession would correct the 15 PD XT.
Conclusion
15-25 % exotropias have pattern strabismus. While
assessing V pattern exotropia oblique muscle overaction
should be looked for. Measurements of deviation should
be taken in all 9 gazes. It could be due to inferior oblique
muscle overaction or superior oblique muscle
underaction or increased action of LR in upgaze or
decreased MR action in downgaze.
Primary and reading positions are functionally the
important positions of gaze. Orbital configuration can
change the force vectors of the extra ocular muscles as
in cases of Crouzon’s and Apert Syndrome. Correction
of these may alter the extra ocular muscle alignment
and action. Thus this should precede muscle alignment.

December 2008 Consultation Section 433
In all cases of strabismus the difference between
primary up and down gaze needs to be calculated.
A difference of 15 PD between up and down gaze makes
it a clinically significant V pattern , while in A pattern
strabismus the difference should be 25 PD.
The presence or absence of inferior oblique muscle
overaction determines the surgical plan. Weakening
inferior oblique corrects 15-20 PD of V pattern.
The horizontal mucles are operated keeping in mind
their original insertions, after good surgical dissection
during their disinsertion for recession or resection
procedures. The musle is reinserted with either slanting
insertions or vertical displacement of one half or both.
A useful mnemonic for the surgical procedures is
‘MALE’: Medial rectus to the apex of the pattern and
Lateral rectus muscles to the empty space.[fig.]. Some
surgeons realign the rectus muscle insertion by placing
the superior corner of say LR and inferior corner of MR
further away from the limbus and other end vice versa-
This is called slanted insertion.
Cases contributed by Dr Elizabeth Joseph, Little Flower Hospital, Angamaly
Compiled and edited by Dr. Meenakshi Dhar, Amritha Institute of Medical Sciences, Cochin
Surgical results are good with functional development
of binocularity, correction of extorsion of the fovea and
decrease in the pattern strabismus of course.
References:
A. Biglan AW. Pattern Strabismus,IN : Rosenbaum AL,
SantiagoAP,eds. Clinical Strabismus Management:
Principles and Surgical Techniques, Philadelphia:
Saunders1999:202-215
B. Ohba M, Nakagawa T. Treatment for A and V strabismus
by slanting muscle insertions. [Binocul Vis Strabismus
Q. 2004] Jpn J Ophthalmol. 2000 Jul-Aug;44(4):
433-8
C. Caldeira JA Some clinical characteristics of V-pattern
exotropia and surgical outcome after bilateral recession
of the inferior oblique muscle: a retrospective study of
22 consecutive patients and a comparison with V-pattern
esotropia. Binocul Vis Strabismus Q. 2004 19(3):
139-50
D. Kamlesh, Dadeya S, Kohli V, Fatima S Primary
inferior oblique overaction-management by inferior
oblique recession. Indian J Ophthalmol. 2002 Jun;
50(2): 97-101

434 Kerala Journal of Ophthalmology Vol. XX, No. 4
Ernst Fuchs
(1851-1930)Dr. Padmaja Krishnan, Calicut
(In the same year that Helmholtz invented the
ophthalmoscope was born a child destined to be one
of our great ophthalmologists. This is his story…….)
Ernst Fuchs was born in Vienna on 14th November 1851.
He was the eldest of three children.
His ancestors were poor farmers, but his grandfather
was sent to Germany to study Theology initially; he
gave it up to become instead a
Professor of History in Vienna. Fuchs’
father, Adalbert, had an even more
varied career. He started as a medical
student, did a PhD, taught Natural
Science, Zoology and finally
Agriculture in Vienna.
Ernst began his scholastic career at
Scott’s Gymnasium in Vienna in1860,
graduating in 1868. He had an
insatiable thirst for knowledge and
often related the story of how he had,
as a college student, jumped into a
whirlpool to find out for himself if it
were true that the current was strong enough to pull
down the strongest swimmer. He was lucky to survive
this foolhardy experiment.
Fuchs’ father wanted Ernst to be an engineer but the
lad had other ideas. Although his interests included
Physics and Astronomy, he opted to study Medicine.
This he did in the heyday of the Vienna school, being
taught by such luminaries as Joseph Hyrtl, Ernst
Wilhelm von Brücke, Karl Rokitansky, Joseph Skoda,
Christian Billroth, and Carl Ferdinand von Arlt.
While still a medical student, von Brücke recognised
Fuchs’ interest in Ophthalmology and got him a post
as assistant to Otto Becker in Heidelberg, Germany.
Fuchs however chose to go for a year to the
Physiological Institute in Innsbruck.
Here in the Austrian Alps, he developed
his passion for mountaineering, which
remained with him throughout his life.
He returned to Vienna in the fall of
1873 and graduated with honours a
year later.
He began his medical career as an
unpaid intern with von Arlt for whom
he had the greatest respect and
admiration. A few months later von Arlt
suggested that Fuchs start his formal
training in surgery under Billroth,
whose outstanding contributions as a
surgeon were already recognised across Europe. Billroth
was Fuchs’ teacher and mentor for the next two years
at the end of which time Fuchs was tempted to become
a general surgeon himself.
Von Arlt now asked Fuchs to become his assistant and
probably regretting his decision not to train under
Becker the previous year, Fuchs accepted the offer and
returned to Ophthalmology. Five years later and just
30 years of age, he became Professor of OphthalmologyComtrust Hospital, Calicut
OPHTHALMICH I S T O R Y

December 2008 Ophthalmic History 435
at Liege, Belgium; at that time he was the youngest
Austrian-trained graduate to become a professor.
In 1885 he succeeded Eduard Jaeger Ritter von Jaxtthal
as Clinical Director of the Second Vienna Eye Hospital.
Fuchs had already published his prize winning book
on the causes and prevention of blindness. His
worldwide reputation as a lecturer and physician
started with this appointment.
In 1915, aged 64 years, Fuchs resigned as clinical
director of the Second Vienna Eye Hospital. The main
motive for his relatively early retirement was apparently
to escape from the time-consuming obligations of
teaching and examining. Nevertheless, following
retirement he published a further 99 articles.
During the time he was at Vienna, ophthalmologists
from around the world came there to learn from the
man considered the master of their profession. Fuchs’
extensive clinical studies and histopathologic
observations provided the first descriptions and
definitions of many conditions and diseases of the eye,
including Fuchs endothelial dystrophy, Fuch’s
heterochromic cyclitis, Dalen –Fuch’s nodules and
Fuch’s coloboma to name a few. He changed the custom
of keeping patients in a dark room with both eyes
covered for a whole week before changing dressings
after a cataract operation. He also introduced early
ophthalmoscopic examinations in these patients and
thus found that choroidal detachment was far more
common than previously believed.
His Textbook of Ophthalmology, first published in 1889,
was regarded as the “bible of ophthalmology” for more
than 50 years. He developed this from his lectures to
ensure that his students listened to him rather than be
distracted making notes. It was a classic in its time and
published in all European languages as well as Japanese
and Chinese. Fuchs employed the then new technique
of using large print for material suitable for students
and small prints for that which he felt was important
for people who were continuing to study ophthalmology
as a postgraduate exercise. It ran into eighteen editions
in German within the next twenty-one years. Of these,
twelve were edited by Fuchs himself and the later ones
by his oldest pupil, Salzmann. And the rapid progress
made by ophthalmology in that period made Fuchs
write in his preface to the tenth edition, “Nothing shows
me the speed of scientific progress better than to leaf
through the first editions of my book. I come across
opinions that I shared with other experts and that now
seem to have aged half a century. I would prefer not to
admit to these opinions, would the proof not lie in front
of me.”
This text proved to be a very important work at that
time and was translated into various languages
including Japanese, Chinese and Russian. The last
German edition was published in 1945. Ten British
editions appeared between 1892 and 1933. In 1903,
Alexander Duane translated and published this in the
United States as Fuchs’ Textbook of Ophthalmology –
this popular text ran into eight editions.
Ernst Fuchs was famed for his teaching abilities
throughout his career but especially during the last 15
years of his life, which he spent traveling to teach and
visit his pupils around the world.Thanks to numerous
invitations by international colleagues, scientific
societies, and governments, Fuchs was able to escape
the Austrian winters (of which he had a growing dislike
with age) by speaking in countries as far away as
Indonesia and East Africa. Remarkably, besides some
knowledge of Latin and Greek, Fuchs was fluent in
English, French, and Italian. To present his work in
Spain and South America, he also began to learn
Spanish at age 70 years and subsequently produced
several publications in that language.
Fuchs was a tall man with a slight stoop. He embodied
Osler’s ideals of equanimitas by never being angry or
impatient and maintaining a calm and unruffled
exterior. He was fluent in English and German and this
helped him to communicate with and present papers
to scientists all over the world.
Apart from his interest in medicine, Fuchs was
interested in Botany, Geography, Literature, Art and
History. He enjoyed travelling till the very end and was
a member of the Vienna Geographical Society. He
regularly gave talks to a wide audience on his many
travels around the globe. In 1875 he returned from
Scandinavia with a pair of “snow shoes” and thus
introduced skiing to Vienna.
In recognition of Fuchs’ worldwide reputation a special
banquet was held in his honor by the American
delegation at the Amsterdam International
Ophthalmological Congress in 1929. It was at this

436 Kerala Journal of Ophthalmology Vol. XX, No. 4
congress that the International Association for the
Prevention of Blindness was established and Fuchs was
elected it’s first honorary member. From the
Netherlands, he traveled to Canada and then to
Baltimore, where he was guest speaker for the opening
of the Wilmer Ophthalmic Institute. Fuchs then
journeyed through Mexico and Central America.
A few months after his return to Vienna and following
an outstanding, dynamic career, Ernst Fuchs died of a
heart attack on November 21, 1930, at age 79 years.
He was buried in Kritzendorf, a small Austrian village
on the Donau River.
During the funeral oration held by the Austrian
Ophthalmological Society, of which he had been
President of Honor, Fuchs was described as a serious
teacher and physician who was never dogmatic and
never taught anything he was not certain of. Great
encomiums indeed!!

December 2008 Journal Review 437
Prevalence of Glaucoma in Patients With
Obstructive Sleep Apnoea -
A Cross-Sectional Case-SeriesRE Bendal, J Kaplan, M Heckman, PA Fredrickson, Eye 2008, 22: 1105-1109.
Loss of integrity of the optic nerve is the key in the
pathogenesis of glaucoma. Several reports suggest the
importance of vascular risk factors, especially in normal
tension glaucoma. Obstructive sleep apnoea (OSA) is
a condition characterized by recurrent upper airway
obstruction accompanied by hypoxemia, hypercapnia,
and sleep disruption. Untreated OSA has been
implicated in the development of cerebral ischemia,
myocardial infarction, pulmonary hypertension, and
cardiac rhythm disturbances, all potential factors in
optic nerve ischemia.
In this study the authors from Mayo Clinic, aim to
determine the prevalence of glaucoma in patients with
obstructive sleep apnoea. This is a cross sectional case
series and includes one hundred patients with moderate
to severe obstructive sleep apnoea. Within 48 hrs of
the polysomnographic diagnosis of obstructive sleep
apnoea, patients underwent following tests: intraocular
pressure, gonioscopy, automated perimetry,
stereoscopic biomicroscopy, and fundoscopic
assessment for the presence of glaucomatous optic
nerve changes.
Glaucoma was diagnosed in 27 of 100 patients yielding
an estimated prevalence of 27 %.(95 % CI 19-37 %).
The presence of glaucoma did not correlate with sex,
body mass index, or AHI, but did appear to be
associated with age (P=0.014). There was no evidence
of a relationship between intraocular pressure and
either the apnoea plus hypopnoea index or age.
This study revealed an unexpected high rate of
glaucoma in patients with obstructive sleep apnoea.
The authors admit that the study design has the
potential to introduce bias since the eye examinations
were carried out with the knowledge that all the
patients had obstructive sleep apnoea.
J OURNALR E V I E W

438 Kerala Journal of Ophthalmology Vol. XX, No. 4
Fibrin Glue Versus Sutures for Conjunctival
Autografting in Pteryium Surgery:
A Prospective Comparative StudyA karalezil, C Kucukerdonmez, Y A Akova, R Altan-Yaycioglu, M Borazan
Br J Ophthalmol 2008;92:1206-1210.
Conjunctival autografting after pterygium excision is
associated with very low rates of recurrence and
complications when compared with other techniques.
The surgeon’s skill and experience affect the recurrence
rate, which varies between 2 % and 39 % with this
technique. Nevertheless, because of graft suturing, this
method has the disadvantage of a relatively longer
surgery time when compared with the bare sclera
technique; also it carries the risk of complications such
as granuloma formation and giant papillary conjunctivitis,
as well as significant patient discomfort after surgery.
In the this study, the authors from Ankara,Turkey,
sought to determine the safety and efficacy of using
fibrin glue (Tisseel VH, Baxter AG, Vienna) to attach
conjunctival autografts and to the results of such with
the use of Vicryl sutures in patients undergoing
pterygium excision. This is a prospective, randomised
study to evaluate operation time, postoperative patient
comfort and pterygium recurrence.
Fifty consecutive patients (50 eyes) with primary nasal
pterygium were enrolled in this prospective study.
Patients with immune system, eyelid or ocular surface
diseases (eg, blepharitis, Sjögren syndrome and dry
eye), with a history of previous ocular surgery or trauma
or known hypersensitivity to any component of fibrin
glue were excluded from the study. Patients were
randomised to two groups. To reduce intra-observer
bias and minimise the influence of the known surgical
technique on the extent of removal and size of the graft,
the randomisation was done after the surgeon (AK)
had harvested the graft. Postoperatively, patients used
dexamethasone 0.1 % and tobramycin 0.3 % eye-drops
four times a day for 7 days, and three times a day for
the following 10 days. All eyes in both groups were
covered with an eye shield for 10 days. Patients were
examined on the first and 10th days, and also at the
first, third, sixth and 12th months after surgery. In the
suture group, sutures were removed 10 days after the
surgery.
Patients were asked to fill out a questionnaire on
postoperative day 1 and during every follow-up
examination until the first month, grading their symptoms
(pain, foreign body sensation, irritation and epiphora)
using a five-point scale adapted from Lim-Bon-Siong
and associates, in which 0 means none, or no symptoms;
1 means very mild, or presence of the symptom but
that it is easily tolerated; 2 means mild, or that the symptom
causes some discomfort; 3 means moderate, or that
the symptom partially interferes with usual activities
or sleep; and 4 means severe, or that the symptom
interferes completely with usual activities or sleep.
Statistical analyses were done with SPSS software. The
Mann-Whitney U and chi-square tests were used for
statistical analyses. A p value less than 0.05 was
considered statistically significant. No significant
difference was found between the two groups with
regard to sex or age (p > 0.05). The mean duration of
surgery was 15.7 (SD 2.4) min (range 12-18 min) in
the fibrin glue group, and 32.5 (6.7) min (range 25-40
min) in the suture group. The operation time was
significantly shorter in the fibrin glue group than it was
in the suture group (p < 0.001). The intensity of the
postoperative complaints including pain, foreign-body
sensation, irritation and epiphora was significantly
lower in patients treated with fibrin glue than in those
treated with sutures at both postoperative days 1 and
10 (p < 0.001). Also, the intensity of itchy sensation
at the first two postoperative visits was lower among
patients in the fibrin glue group (five patients, 20 %)
than in the suture group (12 patients, 48 %) (p < 0.05).
After suture removal in the suture group at
postoperative day 10, all symptoms disappeared quickly.

December 2008 Journal Review 439
None of the patients had any complaints of epiphora
or pain at day 30. Only a few patients in both groups
still had mild irritation and foreign-body sensation in
their eyes at day 30; however, there was no statistically
significant difference between the two groups (p > 0.05).
Reviewed by Dr. Radha Ramanan DO DNB, Little Flower Hospital & Research Center, Angamaly
The authors conclude that, the use of fibrin glue in
pterygium surgery with conjunctival autografting
significantly reduces surgery time, improves postoperative
patient comfort and results in a lower recurrence rate
compared with suturing.
Changes in Angle Configuration After
Phacoemulsification Measured by Anterior
Segment Optical Coherence TomographyWinifred P. Nolan, Jovina L See, Tin Aung, David S Friedman, Yiong-Huak Chan,
Scott D Smith, Ce Zheng, david Huang, Paul J Foster, Paul T K Chew
Journal of Glaucoma. 17(6):455-459, September 2008.
Cross-sectional imaging of the anterior segment and
angle has become more sophisticated over the last 5 to
10 years. Recently optical coherence tomography (OCT)
technology has been adapted for the use in imaging
the anterior segment (AS-OCT). The aim of the study
was to measure changes in angle width after
Phacoemulsification and intraocular lens (IOL)
implantation using anterior segment optical coherence
tomography (AS-OCT).
Twenty-one patients undergoing cataract surgery were
recruited from the National University Hospital,
Singapore. AS-OCT images were obtained of nasal and
temporal angle quadrants before and at 1-month after
surgery. Optical measurements of central anterior
chamber depth were obtained, and gonioscopic
measurement of angle width was recorded. AS-OCT
angle width parameters measured in the nasal and
temporal quadrants included the angle opening
distance at 500 [μm] (AOD500) anterior to the scleral
spur and the trabecular iris surface area at 750 [μm]m
(TISA750) anterior to the scleral spur. Preoperative and
postoperative measurements were compared using
paired samples t tests.
Data were collected from 21 eyes of 21 subjects with
cataract. Seven subjects also had gonioscopic evidence
of primary angle closure. Mean anterior chamber depth
increased from 2.92 (+/-0.54) to 4.24 (+/-0.57) mm
(P=0.044) after cataract extraction. There was a
significant increase in AS-OCT parameters for both
nasal and temporal angles after surgery. An 88.2%
increase in AOD500 was measured for the nasal angle
quadrant with a mean difference of 213.9 (+/-173)
[μm] (P<0.001). TISA750 increased by 94.4% in the
nasal angle with a mean difference of 0.134 (+/-0.104)
[μm] (P<0.001).
This study demonstrates how AS-OCT imaging can be
used to measure changes in angle configuration after
cataract surgery. It confirms that angle widening of up
to 80% can occur when the lens is removed. The authors
conclude that AS-OCT imaging quantitatively
demonstrates increases in angle width after cataract
extraction.

440 Kerala Journal of Ophthalmology Vol. XX, No. 4
Mastering the Techniques of LASIK,
EPILASIK and LASEK (Techniques and
Technology with DVD-ROM)Edited by Ashok Garg, Jorge L Alio, Bojan Pajic, Cyres K Mehta
Published by Jaypee Brothers New Delhi
First edition-2007
Price Rs: 1795/-
Rapid strides have been made in the field of Corneal
Refractive Surgery in the relatively short span of the
last decade. With the advent of new laser machines
and techniques a new paradigm shift in Ophthalmology
was introduced regarding refractive surgery. Excimer
Laser Surgery provides an accurate tool to reshape the
cornea to correct refractive errors in a successful
manner. Ten years ago only Excimer Lasers were
available but now Broad beam, Slit beam, Spot Lasers
and Solid State Laser have revolutinized the Corneal
Refractive Surgery Treatment. The leading factors that
have influenced the changing phase of Corneal
Refractive Surgery have been knowledge gained from
the experience and improvements in technology that
have implemented that knowledge. New Wavefront and
Topography guided Lasik system, Epilasik and Lasek
techniques that have evolved in recent years have not
only helped design better ablation profiles for individual
patients but also provided a more objective means of
measuring outcome resulting in improved algorithms
for future treatments.
With accumulated experience and with the application
of more sophisticated techniques, the safety and efficacy
of refractive surgery has considerably increased during
the recent years. In addition, patient’s satisfaction and
complaints together with the doctor’s clinical
suggestions are being long-term investigated in order
to determine the maximum efficacy after refractive
surgery. The initial enthusiasm is replaced by a more
systematic approach, which contributes to better results
leading to increasing patient’s satisfaction and
physician’s confidence. In this concept, this book is
timely and concise on the many interesting entities of
LASIK technique while the large collection of esteemed
authors and chapters stimulate the reader to search in
the literature for additional contents. It is thoroughly
researched and easy to read.
This international book contains 46 chapters covering
all aspects of practical Lasik, Epilasik and Lasek techniques.
A galaxy of top international Lasik Experts have shared
their experiences in form of chapters for the benefit of
those ophthalmologists who want to start these techniques
in their practice. A video DVD Rom is being given with
this book showing latest Lasik, Epilasik and Lasek
techniques by International Master of this field. As the
clinical practice of Lasik, Epilasik and Lasek is on the
rise world wide, this book shall provide useful practical
tips and guidance to every interested ophthalmologist.
B O O KR E V I E W

December 2008 Book Review 441
The Sankara Nethralaya
Atlas of Ophthalmic UltrasoundEdited by; Muna Bhende, Sriram Gopal, Anuj Gogi, Tarun Sharma, Lingam Gopal,
Lekha Gopal, Parveen Sen, Smitha Menon
Published by Jaypee Brothers New Delhi
First Edition- 2006
Price Rs: 1595/-
Although ophthalmic ultrasound is now widely
accepted as an important tool for the diagnosis and
management of many ocular and orbital disorders, most
academic centers do not have formal training programs
to teach the skills necessary for performing precise and
accurate ultrasound examinations. Unless an individual
can spend several months or more at one of the few
centers in the world that have an expert echographer,
most ophthalmic ultrasound is self-taught by attending
lectures, reading articles and studying one of the few
textbooks available in this field. A welcome addition
to the collection of teaching materials currently
available for ophthalmic ultrasound is The Sankara
Nethralaya Atlas of Ophthalmic Ultrasound.
The Ultrasonography department at Sankara
Nethralaya consists of ophthalmologists, most of whom
are trained vitreoretinal surgeons. The department
performs about 40 procedures every day and has been
doing so far almost two decades. The atlas is a
compilation of the numerous classic and unusual cases
that have been here, along with a brief outline of the
salient clinical and ultrasound features. The nuggets
at the end of the chapters are intended to serve as a
quick reference in difficult situations.
This group, consisting of mainly vitreoretinal surgeons
who are also experienced echographers, has put
together a concise, yet comprehensive text that is
extremely well illustrated very readable. Excellent
examples of almost every ocular and orbital disorder
one might expect to encounter in the clinical practice
of ophthalmic echography are represented in this atlas.
The reader’s understanding of the ultrasound illustrations
is enhanced with color fundus photographs and external
photos, as well as CT scans and MRI scans of the orbit.
One of the text’s outstanding features is the use of
“nuggets” in most of the chapters; charts which provide
pearls of information that are important for the
differentiation and diagnosis of particular conditions.
This book have 50 chapters in 9 sections which includes
topics like getting started, Vitreo-retinal diseases,
Trauma, Infections and inflammations, Tumors,
Congenital anomalies-Disorders of Paediatric age group,
Surgical considerations and Orbital lesions.
This atlas is meant as both a basic text as well as reference
tool for both students of ophthalmology, practicing
ophthalmologists and will be of great interest to those
already familiar with ultrasound of the eye and orbit.

442 Kerala Journal of Ophthalmology Vol. XX, No. 4
Sankara Nethralaya’s Atlas of Uveitis and
ScleritisEdited by: Sudha K Ganesh, Mamta Agarwal, Amala E George, Jyotirmoy Biswas
Published by: Jaypee Brothers, New Delhi
First edition: 2006
Price Rs: 1695/-
Anterior Segment Imaging in
Ophthalmology Ultrasound Biomicroscopy,
Anterior Segment OCT, Pentacam with
DVD- ROMEdited by Tanuj Dada, Ritu Gadia, Sujith Vengayil, Anand Aggarwal, Ramanjit Sihota
Published by Jaypee Brothers New Delhi
First Edition; 2008
Price Rs: 995/-
surface disorders, Lens, Glaucoma, Imaging of ocular
neoplasms, Evaluations of ocular trauma, Vitreoretinal
applications, Utility in cornea and lens based refractive
surgery, corneal transplant surgery and cataract surgery
with over 200 illustrations and photographs.
This text is well- structured, clearly written, well
illustrated and includes a DVD demonstrating the “how
to” of these techniques in a practical and helpful
manner. Trainees, ancillary eye care workers and
ophthalmologists alike will find this publication useful,
easy to read and helpful as a clinic reference manual.
Hospital and clinic administrators will be able to judge
the value of adding these new technologies to the
service they currently provide.
The readers will find the present text informative,
helpful in their clinical practice, will enjoy and benefit
from this publication.
Innovative technology for anterior segment imaging has
become available in recent times that have
revolutionized diagnostic ophthalmology. The three
major technologies that are now in use include
Ultrasound Biomicroscopy (UBM), Anterior Segment
Optical Coherence tomography (ASOCT) and
Seheimpflug photography using the Pentacam. These
investigations have impacted several ophthalmic
subspecialties and now play a vital role in the diagnosis
and management of various corneal and ocular surface
disorders, congenital and acquired lenticular abnormalities,
ocular neoplasia, ocular trauma and glaucoma.
The topics of this text includes; Basic principles of
imaging, Salient features of machine, Methods of
examination, Quantitative evaluation and biometry,
Indications for use, Clinical applications in congenital
disorders, Ocular adnexal imaging, Corneal and Ocular
Uveitis is an emerging subspeciality of ophthalmology
that presents with a constellation of clinical findings.
Accurate diagnosis of uveitis and successful treatment
of these patients remain a challenge. The field of uveitis
has been revolutionized over the past 50 years. Our
understanding of the ocular inflammatory diseases has

December 2008 Book Review 443
progressed rapidly and we can accurately diagnose and
treat these disease. Basic science and research in
immunology has led to new therapeutic approaches to
the patient with uveitis and scleritis.
In recent years, molecular diagnostic procedures have
detected infectious agents in some cases wherein
organisms could not be cultured or detected by
microbiological procedures. Among the various
molecular procedures used, the analysis of intraocular
fluid by polymerase chain reaction (PCR) in uveitis has
shown great promise in detecting traces of an infectious
agent in the form of a microbial specific DNA sequence.
This procedure has been successfully used by several
laboratories including laboratory of Sankara Nethralaya
to detect bacteria, viruses and protozoa in intra ocular
inflammation.
This atlas gives the reader a concise overview of the
clinical manifestations, investigations, diagnosis and
management of uveitis and scleritis. The authors
emphasize on careful clinical assessment and accurate
diagnosis. This book is not intended to be a textbook
but a practical guide to the diagnosis, in obtaining
appropriate investigations and management. The uvea
department of Sankara Nethralaya has a team of four
consultants and they examine about a thousand new
cases of uveitis every year. The emphasis on maintaining
good clinical record with digital archiving was an
excellent source for selecting pictures for this atlas. All
cases included were patients seen at Sankara
Nethralaya, Chennai.
Based on well documented clinical findings, laboratory
investigations including PCR analysis, the authors of
this well illustrated atlas provide succinctly, the main
clinical diagnostic features and management of various
uveitic entities. Profusely illustrated clinical examples
of both anterior and posterior uveitis and scleral
inflammation serve as a guide to postgraduate students
who are in the process of acquiring knowledge in the
field of uveitis, a leading cause of blindness in the
developing world.
Mastering the Techniques of
Presbyopia SurgeryEdited by: Ashok Garg, Jairo E Hoyos, Guillermo Avalos Urzua, Roberto Pinelli, Keiki R Mehta, Matteo Piovella
Published by: Jaypee brothers, New Delhi
First Edition: 2006
Price Rs 1595/-
The mechanism and cause of presbyopia are not fully
understood. In fact competing theories about what is
happening to the lens and the zonules during
accommodation have led to very different cures.
There is sizable population of presbyopics in the world.
Majority of them are not interested in wearing
presbyopic glasses or contact lenses in the long run.
The restoration of reading vision in presbyopia is one
of the most important component of modern refractive
surgery. For the last five years a massive research work
is being done on lenticular, corneal and scleral
modifications to correct presbyopia with encouraging
results. Multifocal Presbyopic LASIK, Conductive
Keratoplasty, Multifocal Presbyopic Lenses are in
widespread use already. A lot of work is being done on
laser and injectable intraocular lenses for restoration
of accommodation which has met with initial success.
Use of accommodative implants, multifocal implants,
Refractive Lens Exchange and Blended Vision Implants
are lenses based refractive surgery procedures which
are quite successful in restoring reading vision in
presbyopic patients.
This book on presbyopia has been written through a
team effort of leading International refractive surgeons
with the purpose of providing latest knowledge on
modern lens and corneal based refractive techniques
of presbyopic correction to ophthalmologists who are
interested in presbyopia surgery practice. Forty-one

444 Kerala Journal of Ophthalmology Vol. XX, No. 4
chapters in four section of this book are written by well
known international refractive surgeons sharing their
knowledge and skill covering all aspects from
physiology to various LASIK/lens based techniques,
complications management, recent advances and future
prospects. An Interactive CD Rom is being provided
with this book showing various operative techniques
in presbyopia by masters of this field.
In the first section of this textbook, leading experts from
around the world discuss presbyopia as a condition and
look at appropriate preoperative evaluation and
considerations in recommending treatments for the
presbyopic patient. In section II, more than two dozen
authors explore the rich variety of techniques for
correcting presbyopia. These include lenticular, corneal
and scleral approaches to restoring accommodation or
pseudo-accommodation. Some of them including
conductive keratoplasty and multifocal LASIK are in
widespread use already. Others are still early in the
developmental stages, but one can find excellent ideas
and pearls from the top authorities on the subject in
these pages. Finally, the book closes with a section on
complication management in presbyopia surgery, and
future considerations for technology that may be the
next big step.
This book provides comprehensive and latest
information on presbyopia correction to every
interested ophthalmologist.
Compiled by Dr. C. V. Andrews Kakkanatt, JMMC Thrissur
December 2008 Book Review 445
NATIONAL CONFERENCE
Vitreo Retinal Society of India Conference
4th -6th December 2008
Venue: Raichak, West Bengal
Contact: Dr.Mangat R.Dogra
AIOS
67th All India Ophthalmological Conference
(Maru Jyothi)
5th – 8th February 2009,
Venue: Jaipur
Contact: Dr.P.K.Mathur (Organising Secretary)
C-126, Moti Marg, Bapu Nagar, Jaipur
Ph:0141-5131236/37
Fax 0141-2221695
Upcoming CME
INTERNATIONAL CONFERENCE
ASIA-ARVO 2009
International Meeting on Research in
Vision and Opthalmology
January 15-18, 2009
Venue: Hyderabad International Convention Center
Hyderabad, India
Contact: Santosh G Honavar
MEACO 2009
Middle East African Council of Ophthalmology
26-30 March 2009
Bahrain
www.meaco.org
UPCOMING
C M E

446 Kerala Journal of Ophthalmology Vol. XX, No. 4

December 2008 Kerala Journal of Ophthalmology 447
OCT IN MACULAR DISORDERS
• Non Invasive, Non Contact• High Resolution
• Cross Sectional Imaging Technique
• Morphology of OD, Fovea, Layers of Retina
• 2.1 /3/10 micron Resolution
• Valuable in Teaching
• Optical Biopsy Imaging - Without Excisional Biopsy
UTILITY
• To Identify ERM
• Confirm Presence of Macular Hole
• Differentiate MH From Simulating Lesions
• Identify - Macular Holes
- Macular Cysts
- Vitreomacular Traction
- Presence of SRF ;PED;CNVM
• Quantify Macular Oedema
• Measure Retinal Thickness Changes in Responseto Therapy
Optical Coherence Tomography in
Macular DiseasesOCT
� Based on Principle of Optical Reflectometry
� Ultrasound using Light
� Original Concept was Optical Biopsy : Non –
Invasive Way to Define Ultrastructure of Optical
Tissue
� OCT 1,2,3,& 4 : Resolution Of 8-10 micron
…………….Still Unable to Perform a True Optical
Biopsy
P G T E A R
S H E E T

448 Kerala Journal of Ophthalmology Vol. XX, No. 4
SURGICAL DECISION MAKING
• Characterises ERM: Location, Extent, Thickness,Attachment Points, Multilaminar, Pseudoholes
• Visualising Surgical Approach• Prognosticate Post op Visual Acuity• Macular edema, Asso Lamellar MH, Degree &
Location of Perifoveal Traction, Presence of CMERisk of Iatrogenic MH
• Post op Evaluation of Slow Visual Recovery• ERM :Presence / Regrowth,Macular Oedema
OCT IN MACULAR HOLES
• As an Adjunct in the Diagnosis ofDifficult to examine patient
• Certain Media Opacities• Coexistent ERM• Suspicion of a tiny hole• Lamellar vs Full Thickness Hole• Thin walled Cyst vs Hole
OCT IN MACULAR HOLES
• Macular Pseudoholes &Lamellar Holes� Contour of Foveal Pit� Thickening of Edges� Steep Foveal Contour� Presence of Normally
Reflective Retinal Tissueat Base
DEFORMATION OF RETINAL PROFILE
• Macular Holes
• Pathogenesis
� Staging
� Natural Course
� Treatment Implication
� Differential Diagnosis
� Patient Education
� Post Surgical Confirmation of Closure
PATHOPHYSIOLOGY• Importance of
VitreomacularTraction inthe creation ofMacular HolesHas Been Recognised For Years
Anteroposterior Transvitreal Traction
• Tangential Traction Theory of Gass
SCREENING : FELLOW EYE• Can Document Progression of VMT• Progression to MH
in Fellow EyeWithout PVD
4.6 % in 3 Years6.5% in 5 years7.1 % in 6 years
With PVD : 0%
MEASUREMENT OF HOLE FORM FACTORa = BASE DIAMETER OF HOLE = 932 micronb = MINIMUM HOLE DIAMETER = 649 micronc = LENGTH OF LEFT ARM = 280 micrond = LENGTH OF RIGHT ARM = 333 micronHFF = c+d/a = 280 + 333 /613 = 0.65
OCT VALUE IN MHS• Operative Planning & Prognosis• Hole size & centration• Presence & degree of surrounding cystoid change• Degree of macular detachment• Asso ERM• Degree of underlying RPE change
POST MHS
• Confirmation of Hole Closure• Visual Prognosis
(Imaii .M , Iijima,H,Gotoh .TAm .J. Oph 1992,128,621 – 627)� U Pattern : Normal Foveal Contour� V Pattern ; Steep Foveal Contour� W Pattern: Foveal Defect Of Neurosensory
Retina U>V>W (Visual Prognosis)

December 2008 Kerala Journal of Ophthalmology 449
ROLE OF OCT IN DME
Sensitive Diagnostic Test
� Early Detection of DME
� Monitor DME
� Prognosticate
� Can Reveal CME, Subfoveal Serous RD,VMT
which cannot be detected by FFA
Detects Mechanical Contribution
VM Interface Abnormalities
Thickness of Macula
Presence of ERM
Compiled by Dr. Meena Chakrabarti MS DO DNB, Chakrabarti Eye Care Centre, Trivandrum
OCT IN DME
• Separates DME with VR Interface abnormality :VMT, Coincident ERM, Taut ILM
• Explains why these eyes respond poorly topharmacological & Laser therapy
• Defines indications for PPV• Longitudinal tracking of tissue changes following
an intervention
OCT IN VMT• Points of attachment• Evaluation of clinically inapparent VMT• Preop Counseling: cystoid
change, foveal traction,schisis, distorsion of fovealarchitecture, intra retinaloedema, foveal detachment
ARTIFACTS & LIMITATIONS Preintepretation check list
REPRODUCIBILITY
HUMAN• Operator experience• Pt co-operation• C o m m u n i c a t i o n
between doctor &operator regardingarea of interest
MACHINE• Registration
• Scan type: points, fastscan, scan length,horizontal/vertical
• Image quality & signalstrength (<5 : do notjudge), iris clip,capture error
• Measurements :algorithm confidence
• Serial OCT in Followup of Retinal Diseases
• Post OperativeConfirmation of• Accurate• MH Closure• Release of VMT• Resolution of DME• Inter Observer
Reproducibility• FP - OCT Overlay
• Accurate• Precise• Repeatable• Reproducible
DISADVANTAGES OF OCT
• Degradation of ImagesIn Presence of Media Opacities
• Scan Quality = depend on Skill of Operator• Impossible in Uncooperative
Children• Measurements Incorrect if
Scan is Not Centered
OCT & MHS : POSTOP ISSUES
• Suboptimal Visual Results• Persistent foveal detachment• Persistent macular oedema• Reduced central foveal thickness• Late Drop in Vision• ERM formation• Distorsion of foveal architecture• Hole reopening
DECISION MAKING IN AMD
• FFA can determine lesion size, location, type &leakage
• OCT : shows compartmentalisation of fluid thatleaks from CNVM : ME, SRF, PED
• OCT : an adjunct to FFA …….interpretation ofleakage, response to therapy
• Useful in ambiguous cases: ME,Early RAP, EarlyRPE tears,Location of blood: subretinal /subRPE
• Non AMD causes of vision loss : MH,VMT,ERM• Conditions Mistaken for AMD : CSR,IPFT
OCT IN AMD
• In the age of antiangiogenic therapy
• Ideal for designing treatment strategies : When
to stop ? When to restart?
• OCT : can identify leakage from CNVM,
resolution of, recurrence of leakage
• What is the future of FA?
• Anti Angiogenic Therapy is effective across all
lesion types ……..it is not the lesion but the
leakage that has to be monitored……..if it is the
leakage that matters …….OCT is all that is really
needed to plan treatment strategies & for
followup

450 Kerala Journal of Ophthalmology Vol. XX, No. 4

December 2008 Kerala Journal of Ophthalmology 451
GENERAL INSTRUCTIONS TO AUTHORS
The Kerala Journal of Ophthalmology (KJO) is a quarterly; peer reviewed one, devoted to dissemination
of the latest in ophthalmology to the general ophthalmologists as well as to specialists in the various
subspecialties of this discipline. It invites submission of original work dealing with clinical and laboratory
materials.
Authors submitting materials to this journal are requested to adhere STRICTLY to the norms laid down
below. The matter must be typed on one side of the paper. A margin of I” must be left all around and the
material must be double-spaced. A page should contain not more than 25 lines. Two copies of the text in
paper and one copy in a CD must be submitted to the Editor and the corresponding author is advised to
keep another copy with him. The corresponding author must give it in writing in his covering letter that
the same matter will not be submitted elsewhere if accepted. He must also enclose the copyright transfer
of his work to this journal. The papers sent will be subjected to peer review. The accepted manuscripts
become the permanent property of this Journal. The author is informed that, if his work is returned to him
for correction / clarification after peer review, he should effect the same and send the manuscript back to
the Editor within one month. Each manuscript component mentioned here under must begin with a new
page and the pages are to be numbered at the right tip corner starting from the Title page.
1. TITLE: The title of the work must be brief and precise. It should not exceed two lines and 40 characters
(including comma, period) Author (s) full name (s) must be given along with his (their) degree and
the affiliations. Corresponding author’s name, correct address (including e-mail and Fax, if available)
and phone number must be mentioned at the bottom left hand corner of the first page.
2. ABSTRACT: The abstract is to be given in the beginning itself. It should not exceed 200 words. It must
contain the aim, methodology, results and conclusion. For case report, summary / conclusion alone is
to be given.
KEY WORDS (maximum five) in capitals are to be included at the end of Abstract.
3. INTRODUCTION: Describe the aim of the study, along with the hypotheses that were tested. Only
necessary references are to be given
4. METHOD: Give in detail the materials used and the methods employed. Describe the type of study.
Pharmacological names only must be mentioned for the drugs used and, if proprietary name is used,
then the manufacturers name must be given in parentheses. Except for standard, well-accepted
abbreviations (Including SI Units), all others must be introduced in parentheses when the full term is
used for the first time in the article.
5. RESULTS: Give only the results obtained by the study under discussion. State the statistics in the
correct scientific form (P value, mean etc). Results based on assumptions must not be given. Indicate
in the text the place where the tables have to be inserted
6. DISCUSSION: The discussion should be to the point and relevant to the subject under discussion.
This section can be combined with the previous one if the author desires. Avoid speculations. Use
only standard abbreviations or the abbreviations already introduced.
7. ACKNOWLEDGEMENT: This is to be made only to those who were directly and scientifically involved
with the preparation of the paper. Permitting authorities, technicians, photographers who assisted in
the work need not be mentioned.

452 Kerala Journal of Ophthalmology Vol. XX, No. 4
8. REFERENCES: The references should be given in numerical order in which they first appear in text
and not in alphabetical order (Citation Order System). It should be numbered consecutively in the
text. The references will not be checked by the Editor or by the Peer reviewer and hence the author is
solely responsible for its completeness and the accuracy. Period should not be employed anywhere in
the references. Personal communication, unpublished data and poster references, if mentioned, should
be in the text itself and the source mentioned in parentheses. References should be in the following
form:-
Journal reference: Author(s) full title, Journal name (as abbreviated in Index Medicus), volume number,
pages and year. If there are more than three authors, then mention the first three authors and then ‘et
al’.
Book reference: Authors(s) (& Editor, if any), title of book (and chapter), publisher, place of publication,
page number (s) of the cited portion and year.
9. THE LEGEND: The legend for the illustrations (and tables, if necessary) must be given in a separate
sheet of paper and should be typed double-spaced.
Illustrations: The photos and figures should be prepared in glossy prints with good contrast and of the
size 6” x 4”. Only salient details should be included. On the back of the illustration, the figure number
in text, title of the paper, the first author’s name and the top side (marked with an arrow) must be
specified. Except for arrows, no text is to be on the photos. It is the duty of the author(s) to get the
patient’s written permission when the subject is identifiable in the photo. Submit two sets of illustrations.
Illustrations from other Journals and books are usually not accepted. If used, it rests with the author(s)
to get the copy right permission from the original author / publisher and this permission letter must
be sent to the Editor at the time of submitting the manuscript. For Histological figures the stain and
magnification used should be noted e.g.: - H & E Stain x 70.
10. TABLE: It should be in double space. Each table must have an Arabic numeral (except for single
table) and a title both in a single line. Each column in the table must have a short heading. If a table
is large, then it must be continued in a second page, which also must have the table number and the
title. Avoid vertical lines in the tables. Two sets must be submitted.
The manuscripts are to be sent to The Editor by Courier Mail or by Registered post. The corresponding
author will receive communication from the Editor within two weeks of receiving the manuscript.
11. All manuscripts are subjected to editorial board review.
12. Other Categories of Manuscript
a) Original Articles should generally not exceed 3,000 words or 12 double – spaced pages.
b) Review Articles: can be on topics of relevance to clinical practice, research methodology, community
ophthalmology or investigative work, of relevance to visual science. These articles should include
up to date review of existing literature, and summarize the current status / preferred practice for
that particular topic.
Brief reports are short communication of new instruments, new laboratory techniques or surgical
techniques as well as interesting case reports with unique findings. These should not exceed 1000
words with a maximum of 2 illustrations. They should follow the format - introduction, case, and
discussion. No more than 8 references should be cited. Each brief report must begin with a 75-100
word summary that highlights the significance of the articles.

December 2008 Kerala Journal of Ophthalmology 453








