Kevin Svancara DO PGY3 Jennifer Peterson DO PGY3Advanced Desert DermatologyMidwestern University AZCOM


http://www.aocd.org/?page=GranulomaAnnulare
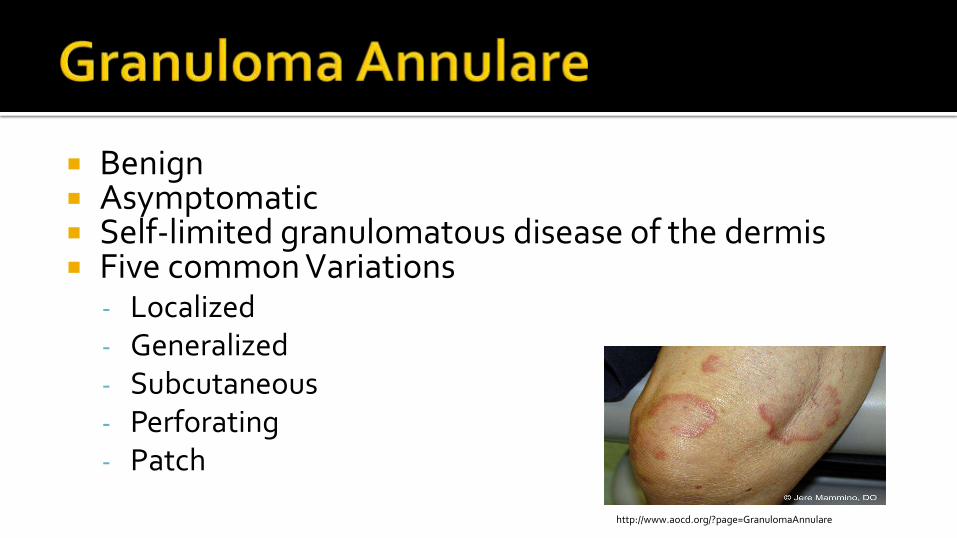
Benign Asymptomatic Self-limited granulomatous disease of the dermis Five common Variations
- Localized- Generalized- Subcutaneous- Perforating- Patch
http://www.aocd.org/?page=GranulomaAnnulare
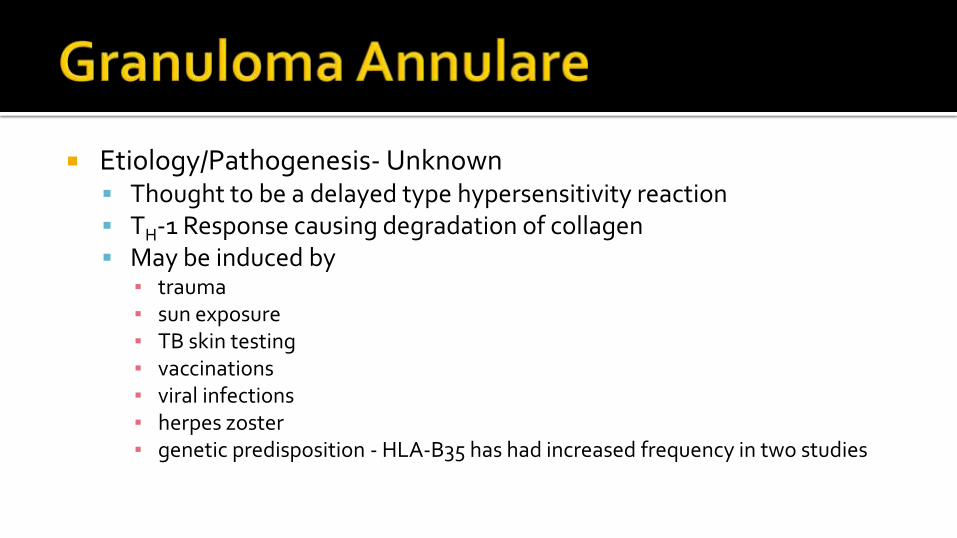
Etiology/Pathogenesis- Unknown Thought to be a delayed type hypersensitivity reaction TH-1 Response causing degradation of collagen May be induced by
▪ trauma▪ sun exposure▪ TB skin testing▪ vaccinations▪ viral infections▪ herpes zoster▪ genetic predisposition - HLA-B35 has had increased frequency in two studies
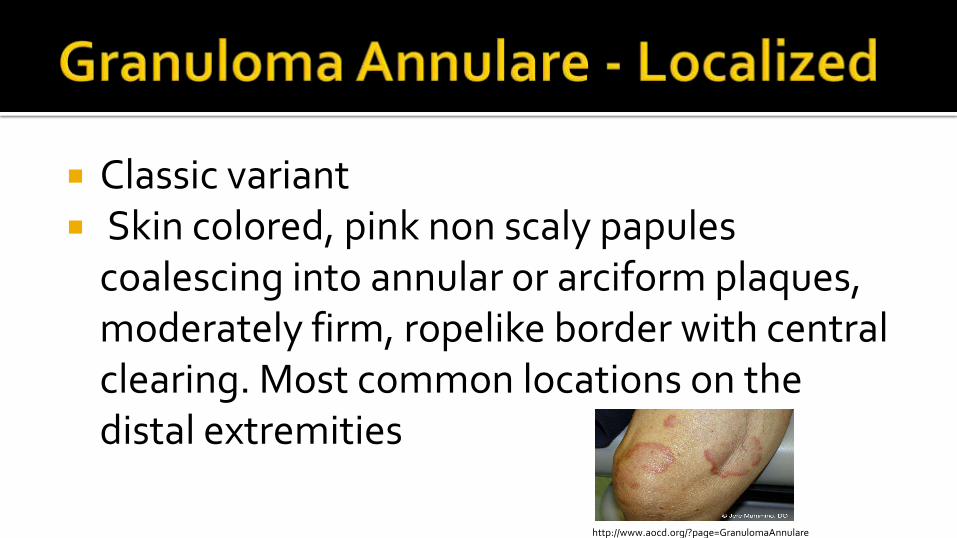
Classic variant Skin colored, pink non scaly papules
coalescing into annular or arciform plaques, moderately firm, ropelike border with central clearing. Most common locations on the distal extremities
http://www.aocd.org/?page=GranulomaAnnulare

Generalized 15% of cases 10 or more lesions 45% have lipid abnormalities More chronic and relapsing course
Subcutaneous Most common form in children Scalp and extremities Painless
http://drcamisasblog.com/2013/11/17/granuloma-annulare-5/
http://dermnetnz.org/dermal-infiltrative/granuloma-annulare.html

Rare variants include –Perforating, Patch Histology
Palisading Granuloma with a necrobiotic foci in the dermis
Mucin present
lymphocytic infiltrate
http://www.dermpedia.org/case-type/9?page=65
Associated Disorders Diabetes Mellitus
The relationship between diabetes and GA is controversial Earlier studies presented a relationship, more recent studies
have failed to find the association previously reported Autoimmune Thyroiditis Hodgkin's and Non Hodgkin's Lymphoma Hyperlipidemia and Hypercholesterolemia HIV Hep B and C
Treatments Often self-limited – 50% resolve within the first 2 years
First Line – High potency topical or intralesional steroids
Destructive▪ Cryotherapy: 25/31 patients had resolution with 1 treatment (10-60
sec)
▪ Biopsy – controversial
Lasers – PDL, CO2, Excimer

Treatments Oral antibiotics
▪ Doxycycline 100mg bid▪ Dapsone
Antimalarials▪ Hydroxychloroquine, Chloroquine
Immunosuppressants▪ Methotrexate, Cyclosporine, TNF-a
Light Therapy▪ NBUVB, PUVA, PDT
Take home points Benign – self limited in 50% of cases
Delayed type hypersensitivity reaction – TH-1
Localized form – most common
Subcutaneous form – most common in children
Can be associated with autoimmune thyroiditis
Consider checking triglycerides in generalized GA

http://www.dermis.net/dermisroot/en/37834/image.htm
Clinical DM associated –65% of patient’s have DM. Only
found in 0.3% of DM patients
average age of 25 in patients with DM
Non-DM associated in mid 40s
Most commonly located on the anterior shins.
Red, brown or violaceous papules. Progress to yellow, brown, atrophic telangiectatic plaques.
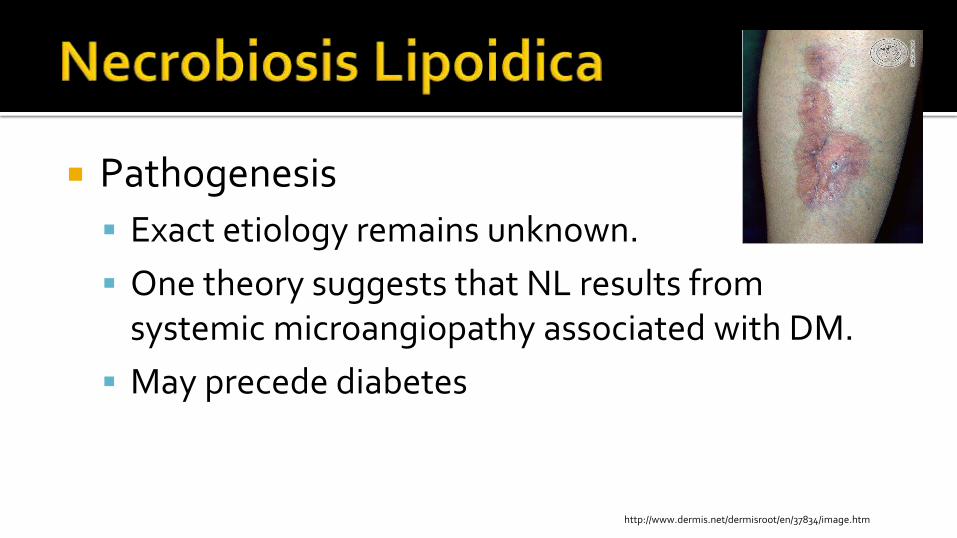
Pathogenesis
Exact etiology remains unknown.
One theory suggests that NL results from systemic microangiopathy associated with DM.
May precede diabetes
http://www.dermis.net/dermisroot/en/37834/image.htm
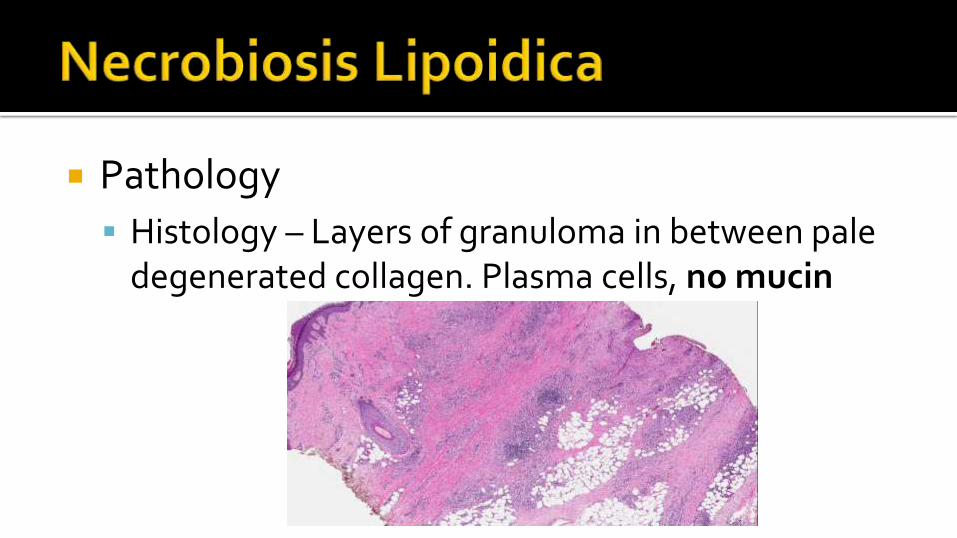
Pathology
Histology – Layers of granuloma in between pale degenerated collagen. Plasma cells, no mucin
Treatment First Line – High potency (Class I) topical steroids under
occlusion
Intralesional steroids – Use caution not to cause ulceration
Topical PUVA
Antimalarials – Hydroxychloroquine 200mg qd
Fumaric Acid Esters – Not approved by the FDA
Pentoxifylline

Take home points
Only a small portion of patients with DMII (0.3%) will develop Necrobiosis Lipoidica
Histology: Palisading Granuloma
without mucin
Located on anterior shins
http://www.dermis.net/dermisroot/en/37834/image.htm

http://www.aocd.org/resource/resmgr/ddb_high/sarcoidosis_2_high.jpg
http://www.aocd.org/?page=Sarcoidosis
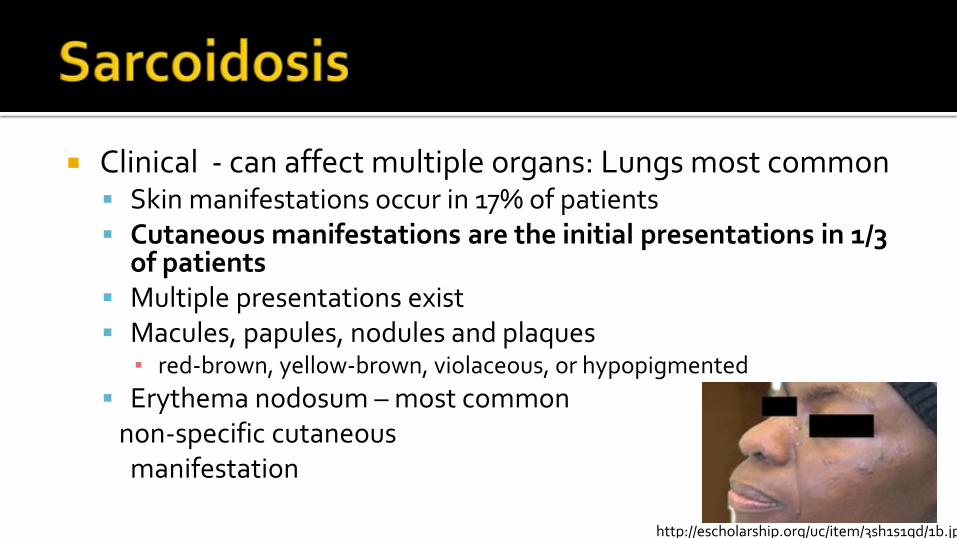
Clinical - can affect multiple organs: Lungs most common Skin manifestations occur in 17% of patients Cutaneous manifestations are the initial presentations in 1/3
of patients Multiple presentations exist Macules, papules, nodules and plaques
▪ red-brown, yellow-brown, violaceous, or hypopigmented
Erythema nodosum – most commonnon-specific cutaneousmanifestation
http://escholarship.org/uc/item/3sh1s1qd/1b.jpg
Pathogenesis - Unknown Thought to involve genetically influenced
dysregulation of the Th-1 immune response to one or more extrinsic antigens
May lead to over activation of inflammatory pathways and subsequent granuloma formation
Case control study of 700 patients was unable to find any single etiologic agent.
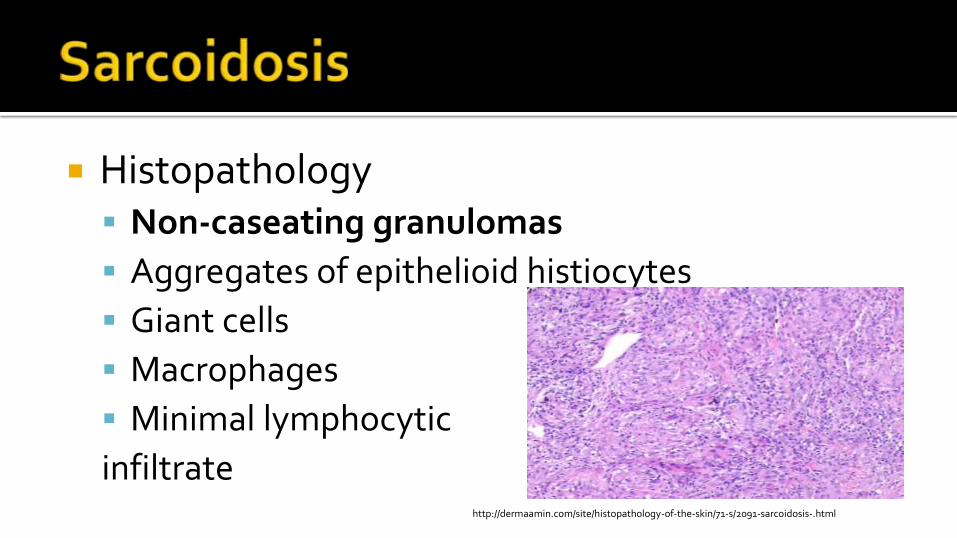
Histopathology Non-caseating granulomas
Aggregates of epithelioid histiocytes
Giant cells
Macrophages
Minimal lymphocytic
infiltratehttp://dermaamin.com/site/histopathology-of-the-skin/71-s/2091-sarcoidosis-.html
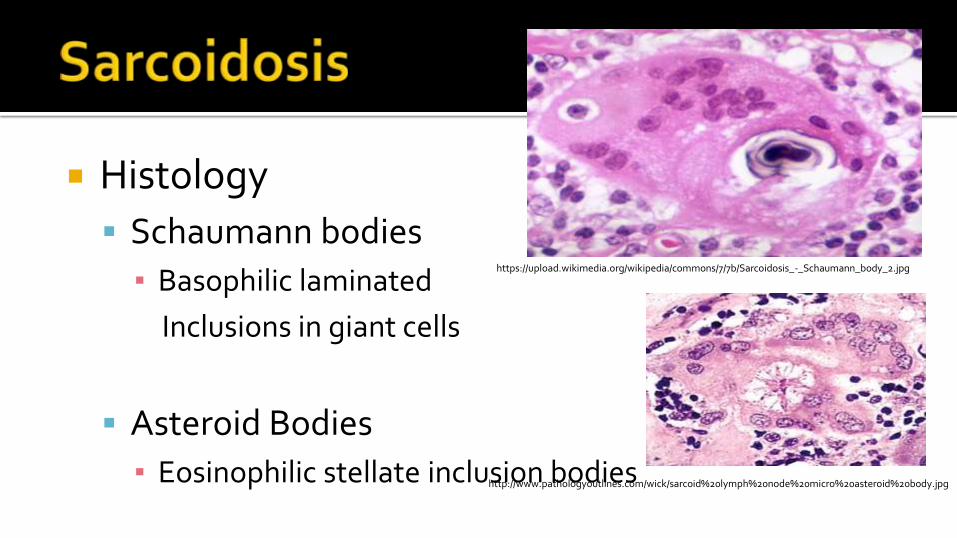
Histology
Schaumann bodies
▪ Basophilic laminated
Inclusions in giant cells
Asteroid Bodies
▪ Eosinophilic stellate inclusion bodies
https://upload.wikimedia.org/wikipedia/commons/7/7b/Sarcoidosis_-_Schaumann_body_2.jpg
http://www.pathologyoutlines.com/wick/sarcoid%20lymph%20node%20micro%20asteroid%20body.jpg

Variants Lupus Pernio – violaceous infiltration of the nose,
cheeks or earlobes, often
associated with a chronic
course▪ Can cause scarring after resolution
▪ Often associated with upper
respiratory tract disease
http://www.dermis.net/bilder/CD183/550px/img0053.jpg

Lofgren’s Syndrome
Triad
▪ Erythema nodosum - Most common non-specific cutaneous finding, 25% of patients with sarcoidosis
▪ bilateral hilar adenopathy
▪ migrating polyarthritis
https://escholarship.org/uc/item/8rg7v60g/lofgren2.jpeg
http://www.hindawi.com/journals/crirh/2013/125251.fig.001.jpg
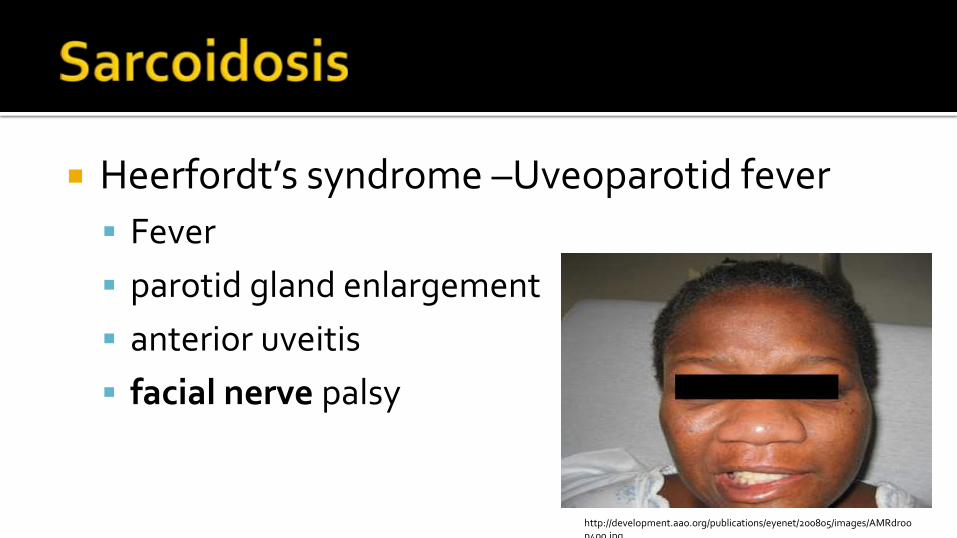
Heerfordt’s syndrome –Uveoparotid fever
Fever
parotid gland enlargement
anterior uveitis
facial nerve palsy
http://development.aao.org/publications/eyenet/200805/images/AMRdroop400.jpg
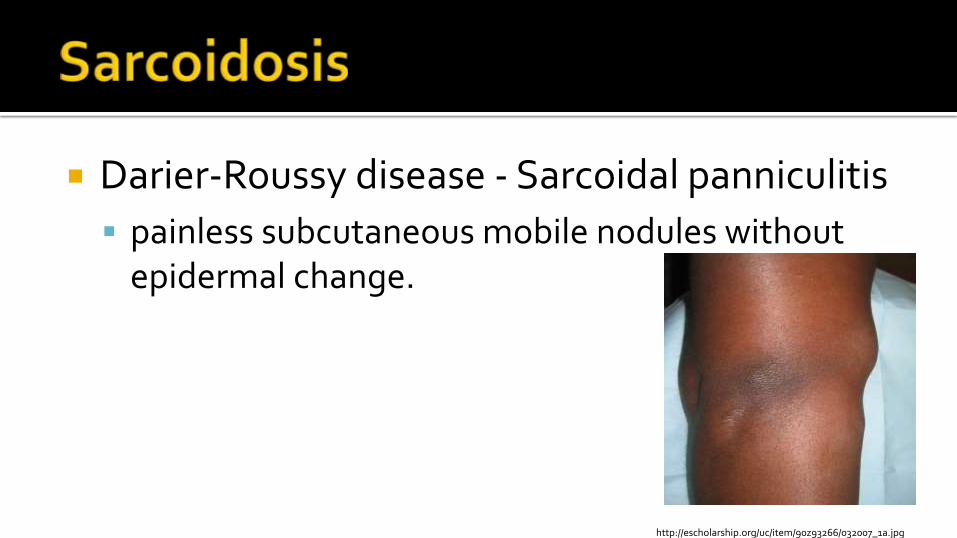
Darier-Roussy disease - Sarcoidal panniculitis
painless subcutaneous mobile nodules without epidermal change.
http://escholarship.org/uc/item/90z93266/032007_1a.jpg
Treatment – lack of high quality evidence to support efficacy
Topicals - super potent steroids, mid potency for face.
Intralesional injections systemic corticosteroids for severe disease
20-40mg/kg/day with a slow taper May add hydroxychloroquine 200-400mg/day or
methotrexate 25mg/week, tapered to 5-15mg

minocycline – retrospective study of 27 patients, 14 had partial improvement while 6 had complete improvement on 1-6 months of minocycline
Refractory treatments Biologics - TNF – alphas – notably infliximab but
data has been conflicting in larger studies
Take home points
Lesions that develop within a scar or tattoo should be ruled out for sarcoidosis
Erythema Nodosum – positive prognosis, associated with acute sarcoidosis
TH1 response to unknown antigen

https://www.dermquest.com/imagelibrary/large/044989HB.JPG
http://dermaamin.com/site/images/clinical-pic/m/macular-amyloidosis/macular-amyloidosis2.jpg
Cutaneous Macular Lichen Nodular Secondary
Systemic Primary systemic Secondary systemic Hemodialysis- associated
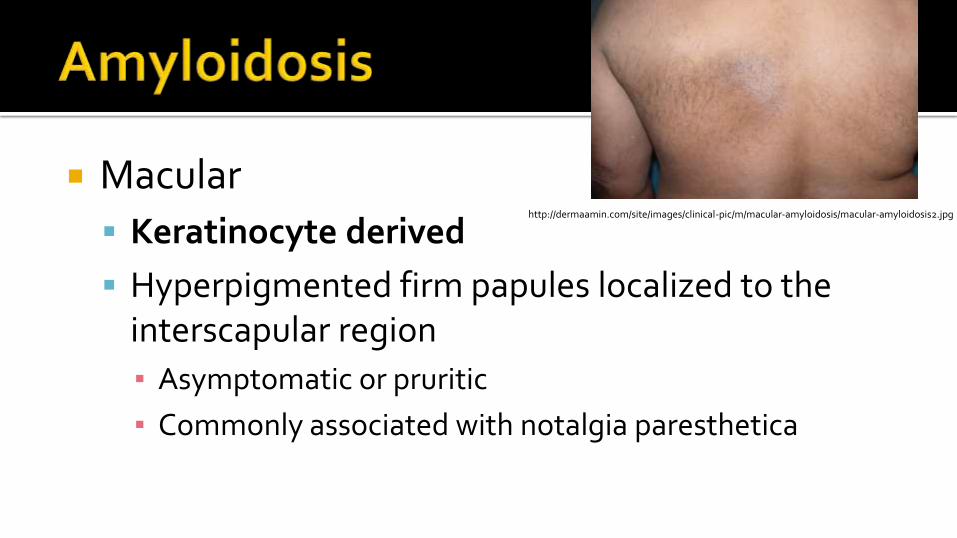
Macular
Keratinocyte derived
Hyperpigmented firm papules localized to the interscapular region
▪ Asymptomatic or pruritic
▪ Commonly associated with notalgia paresthetica
http://dermaamin.com/site/images/clinical-pic/m/macular-amyloidosis/macular-amyloidosis2.jpg

Lichen amyloidosis
Keratinocyte derived
Flat topped shiny papules
Commonly over the shins
Pruritic
Seen in MEN 2A
http://dermaamin.com/site/images/clinical-pic/L/lichen-amyloidosis/lichen-amyloidosis10.jpg
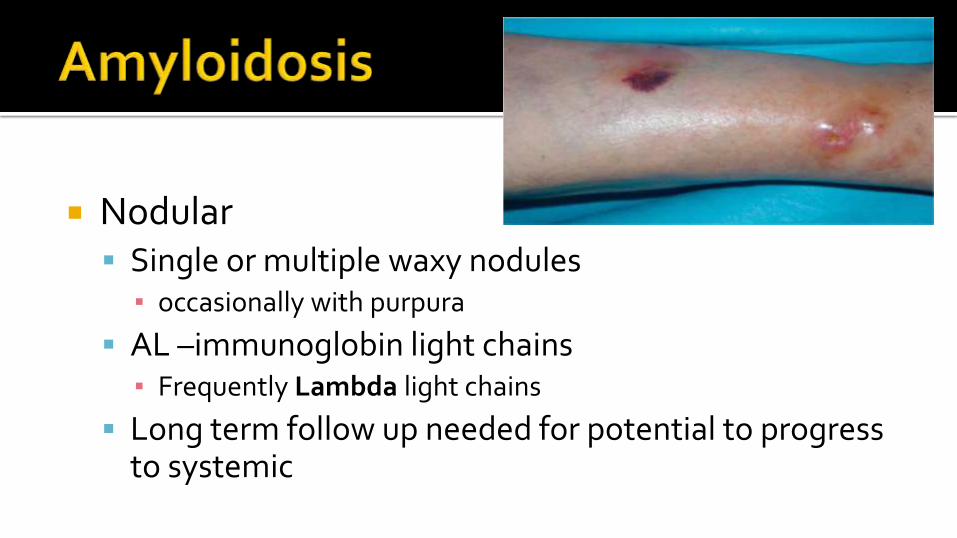
Nodular Single or multiple waxy nodules
▪ occasionally with purpura
AL –immunoglobin light chains▪ Frequently Lambda light chains
Long term follow up needed for potential to progress to systemic
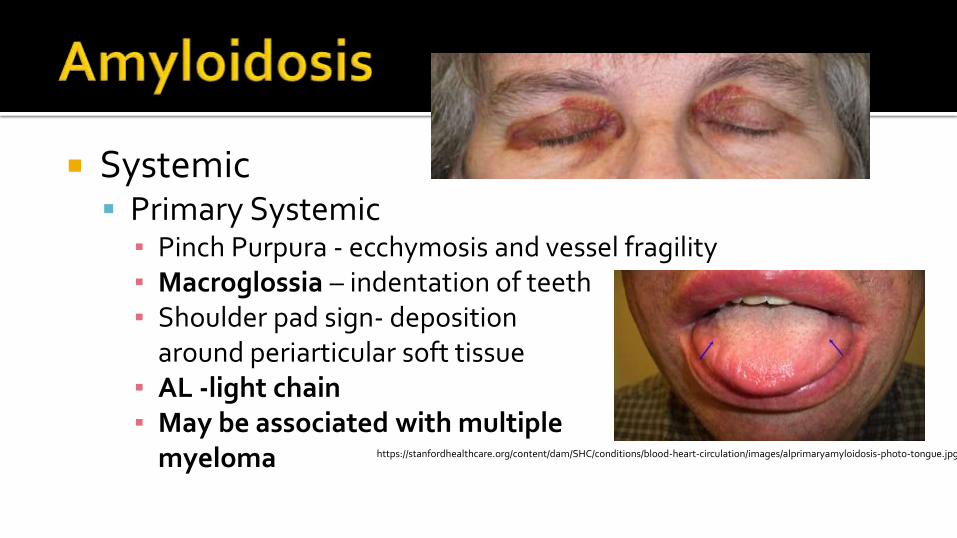
Systemic Primary Systemic
▪ Pinch Purpura - ecchymosis and vessel fragility ▪ Macroglossia – indentation of teeth▪ Shoulder pad sign- deposition
around periarticular soft tissue▪ AL -light chain▪ May be associated with multiple
myeloma https://stanfordhealthcare.org/content/dam/SHC/conditions/blood-heart-circulation/images/alprimaryamyloidosis-photo-tongue.jpg
Hemodialysis associated amyloidosis Long term hemodialysis Beta 2 microglobulin Deposition in synovial membranes
▪ Carpal Tunnel Senile Systemic amyloidosis
Late onset in elderly patients ATTR - Transthyretin
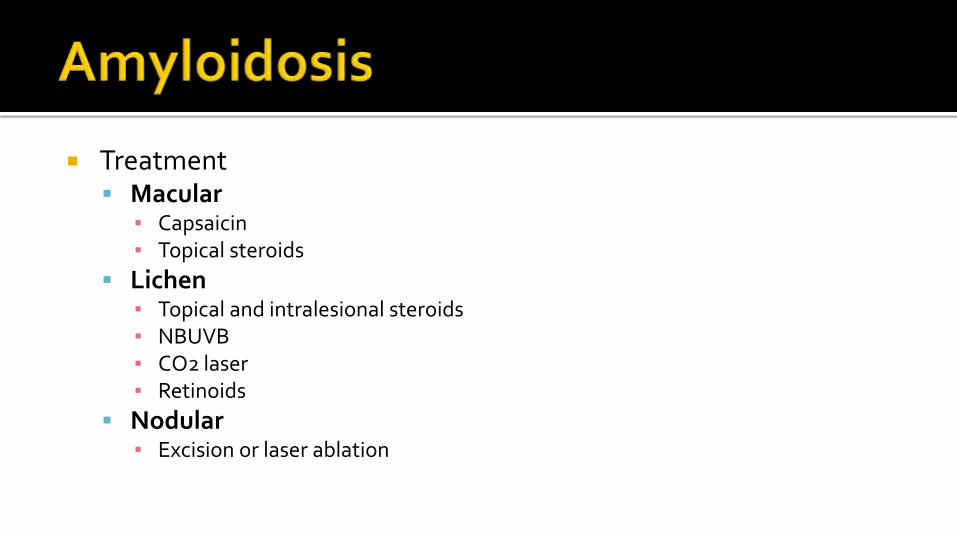
Treatment Macular
▪ Capsaicin▪ Topical steroids
Lichen▪ Topical and intralesional steroids▪ NBUVB▪ CO2 laser▪ Retinoids
Nodular▪ Excision or laser ablation
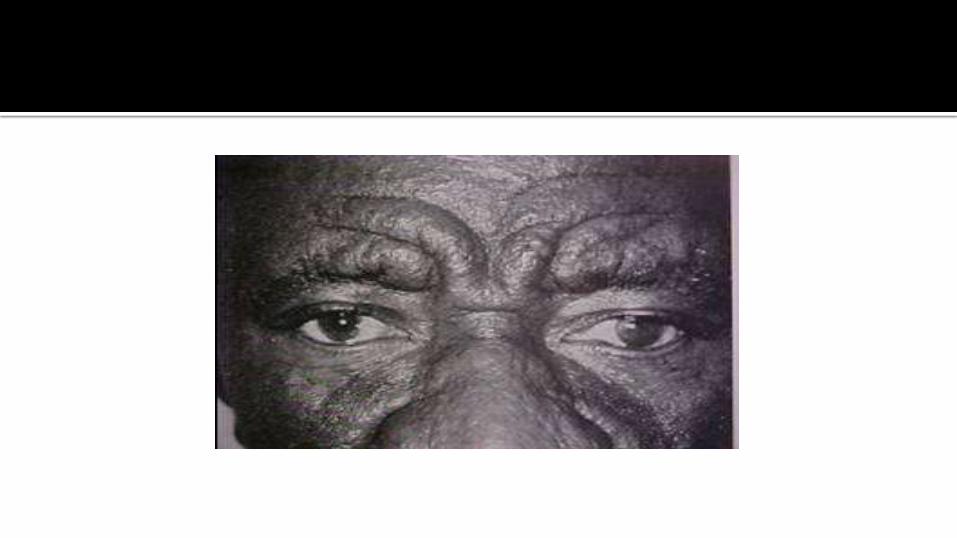
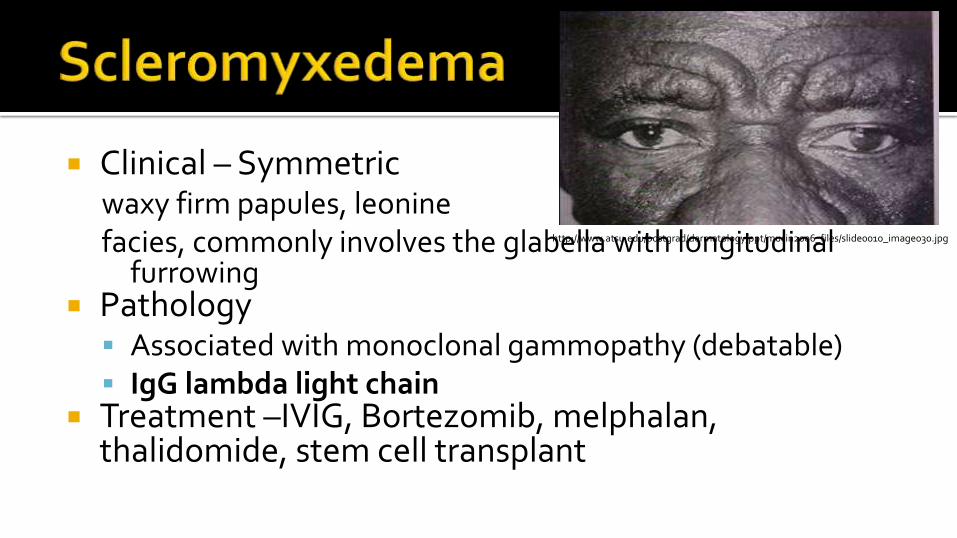
Clinical – Symmetricwaxy firm papules, leoninefacies, commonly involves the glabella with longitudinal
furrowing Pathology
Associated with monoclonal gammopathy (debatable) IgG lambda light chain
Treatment –IVIG, Bortezomib, melphalan, thalidomide, stem cell transplant
http://www.atsu.edu/postgrad/dermatology/ppt/mucin2006_files/slide0010_image030.jpg
http://images.rheumatology.org/image_dir/album75672/md_04-10-0056.jpg
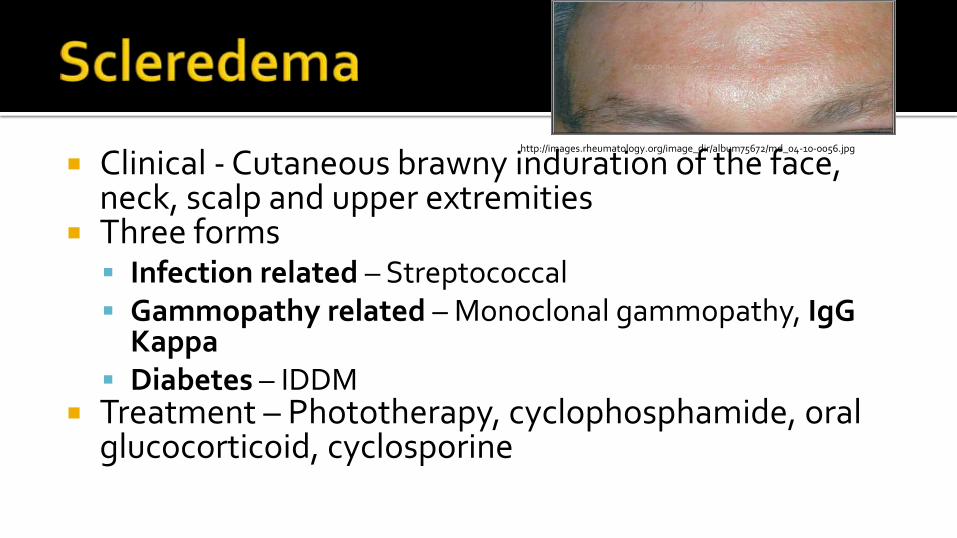
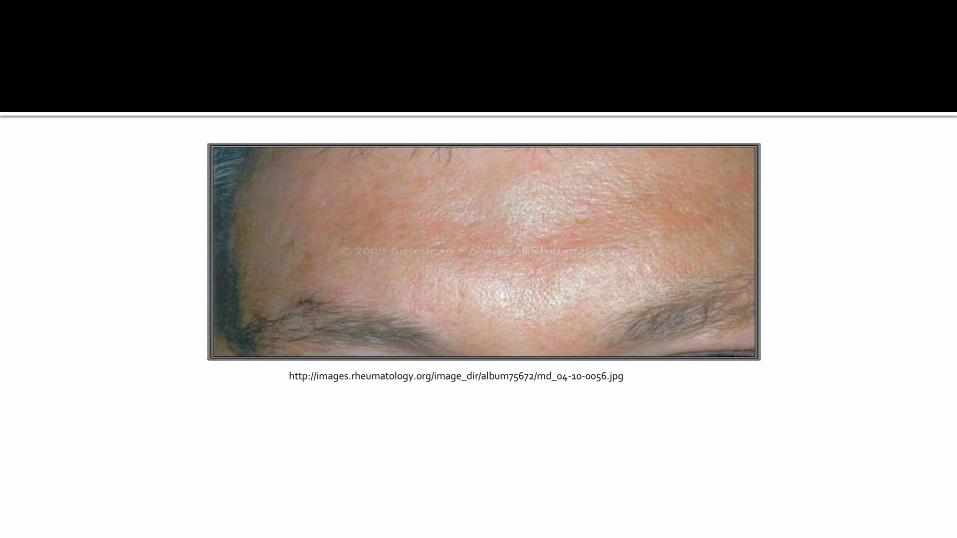
Clinical - Cutaneous brawny induration of the face, neck, scalp and upper extremities
Three forms Infection related – Streptococcal Gammopathy related – Monoclonal gammopathy, IgG
Kappa Diabetes – IDDM
Treatment – Phototherapy, cyclophosphamide, oral glucocorticoid, cyclosporine
http://images.rheumatology.org/image_dir/album75672/md_04-10-0056.jpg

http://www.dartmouth.edu/~thabif/weeklyclinic111901/pictures/19porphyriacthands.jpg
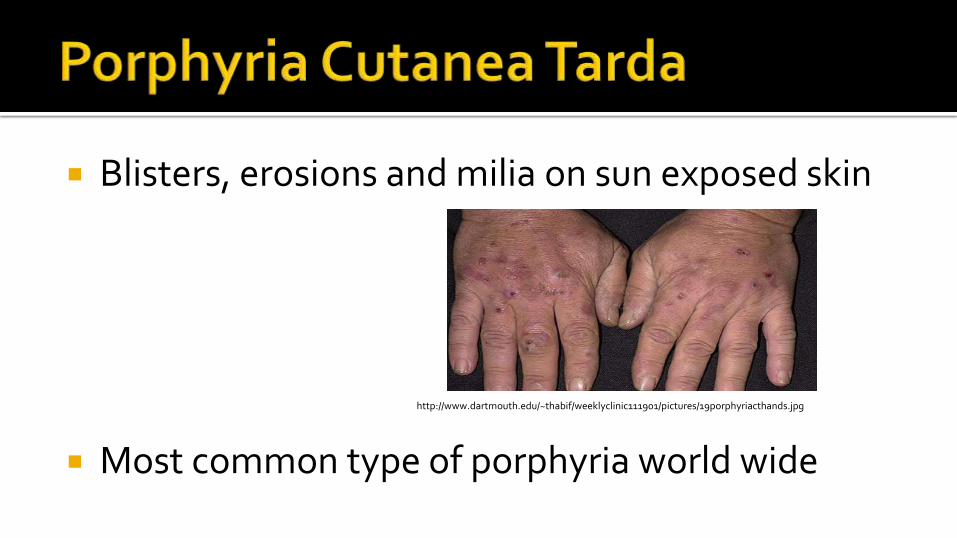
Blisters, erosions and milia on sun exposed skin
Most common type of porphyria world wide
http://www.dartmouth.edu/~thabif/weeklyclinic111901/pictures/19porphyriacthands.jpg

Defect – Uroporphyrinogen Decarboxylase
Triggers Alcohol HCV Estrogen Iron Over load Hemochromatosis
Labs: Total plasma porphyrins with reflex Then stool, plasma and RBC fractionation

Treatment - Phlebotomy every 2 weeks, may combine with antimalarials
Hydroxychloroquine: 100mg BIW
Takes on average 6.5 months to reach therapeutic levels with hydroxychloroquine and phlebotomy
Better compliance than phlebotomy

http://dermaamin.com/site/images/clinical-pic/e/erythropoietic_protoporphyria/erythropoietic_protoporphyria5.jpg

Most common porphyria in children Clinical – erythema, edema, crust, purpura and
skin thickening Labs – Total erythrocyte protoporphyrin
Urine porphyrin levels normal Complications
Protoporphyric hepatopathy Gallstones
http://dermaamin.com/site/images/clinical-pic/e/erythropoietic_protoporphyria/erythropoietic_protoporphyria5.jpg
Treatment Broad Spectrum Sunscreen, Photo protective
Clothing
Avoidance of sunlight exposure from 11:00 AM –3:00PM
Beta-Carotene 30-90mg/day in children
Cysteine supplements, 500mg bid
Afamelanotide
1. Kapoor R, Piris A, Saavedra AP, et al. Wolf isotopic response manifesting as postherpetic granuloma annulare: a case series. Arch Pathol Lab Med. 2013; 137(2):255-258.
2. Muhlemann MF, Williams DR. Localized granuloma annulare is associated with insulin-dependent diabetes mellitus. Br J Dermatol. 1984;111(3):325.
3. Li A, Hogan DJ, Sanusi ID, Smoller BR. Granuloma annulare and malignant neoplasms.. Am J Dermatopathol. 2003;25(2):113. 4. Keimig E, Louise E. Granuloma Annulare. Dermatol clin. 2015;33(3):315-329. 5. Kosaka S, Kowana S. Case of necrobiosis lipoidica diabeticorum successfully treated by photodynamic therapy. J Dermatol. 2012;39(5):497-499. 6.Lecha M, Puy G, Deybach JC. Erythropoietic Protoporphyria. Orphanet J Rare Dis. 2009; 4:19. 7. Thornsberry, L, English, A. Etiology, diagnosis, and therapeutic management of granuloma annulare: an update. AM J Clin Dermatol. 2013;
14(4):279-290. 8. Alexandrescu, Doru T; Kauffman, C Lisa; Ichim, Thomas E; Riordan, Neil H; Kabigting, Filamer; & Dasanu, Constantin A. (2011). Cutaneous
sarcoidosis and malignancy: An association between sarcoidosis with skin manifestations and systemic neoplasia. Dermatology Online Journal, 17(1)
9. Steen, T, English JC, Oral Minocycline in Treatment of Cutaneous Sarcoidosis. Jama Dermatol. 2013. 149(6): 758-760. 10. Rose AS, Tielker MA, Knox KS. Hepatic, ocular, and cutaneous sarcoidosis. Clin Chest Med. 2008;29(3):509 11. Salas-Alanis JC, Martinez-Jaramillo B, Gomez-Flores M, et al. Scleromyxedema, a therapeutic dilemma. Indean J Dermatol. 2015; 60(2): 215. 12. Dereure O, Jumez N, Bessis D,e t al. Measurement of liver iron content by magnetic resonance imaging in 20 patients with overt porphyria
cutanea tarda before phlebotomy therapy: a prospective study. Acta Derm Venereol. 2008;88(4):341. 13.. Harms JH, Lautenschlager S, Minder CE, et al. Photosensitivity of erythropoietic protoporphyria patients by an agonistic analog of alpha-
melanocyte stimulating hormone. Photochem Photobiol. 2009 Nov;85(6):1434-9. 14. Mathews-Roth MM, Rosner B, Benfell K, et al. A double-blind study of cysteine photoprotection in erythropoietic protoporphyria. Photodermatol Photoimmunol Photomed. 1994 Dec;10(6):244-8. 15. Jain, S. 2012. Dermatology:Illustrated Study Guide and Comprehensive Review. New York, NY: Springer. 16. Sanchez M, Haimovic A, Prystowsky S. Sarcoidosis. Dermatol Clin. 2015; 33(3): 389-416. 17. Ladizinski B, Lee KC. Lichen Amyloidosis. CMAJ. 2014; 186(7): 532.







