
REVIEW ARTICLE
Ketamine: Teaching an Old Drug New Tricks
Rainer Kohrs, MD, and Marcel E. Durieux, MD
Department of Anesthesiology, University of Virginia Health Center, Charlottesville, Virginia
K etamine has a special position among anesthetic drugs. It was introduced into clinical practice >30 yr ago with the hope that it would function
as a “monoanesthetic” drug: inducing analgesia, am- nesia, loss of consciousness, and immobility. This dream was not fulfilled because significant side effects were soon reported. With the introduction of other IV anesthetic drugs, ketamine’s role diminished rapidly. However, it is still used clinically for indications such as induction of anesthesia in patients in hemodynamic shock; induction of anesthesia in patients with active asthmatic disease; IM sedation of uncooperative pa- tients, particularly children; supplementation of in- complete regional or local anesthesia; sedation in the intensive care setting; and short, painful procedures, such as dressing changes in burn patients.
However, recent insights into ketamine’s anesthetic mechanism of action and its neuronal effects, as well as a reevaluation of its profound analgesic properties, offer the potential of expanding this range of indica- tions. In addition, studies with the S(+) ketamine isomer suggest that its use may be associated with fewer side effects than the racemic mixture. In this article, we review the mechanism of action of ket- amine anesthesia, the pharmacologic properties of its stereoisomers, and the potential uses of ketamine for preemptive analgesia and neuroprotection. Several as- pects discussed herein have been reviewed previously (l-4).
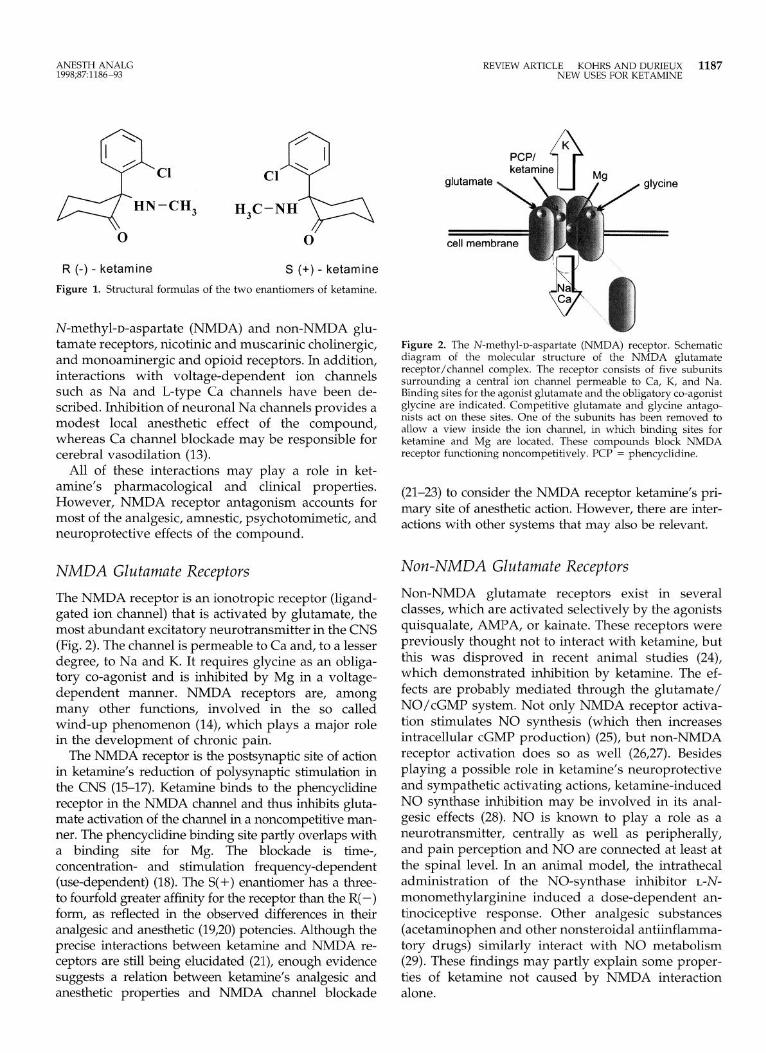
Clinical Pharmacology Commercial ketamine is a racemic mixture consisting of two optical enantiomers, R( -) and S( +) (Fig. l), and the preservative benzethonium chloride. Pharmacoki- netically, ketamine has relatively short distribution and elimination half-lives: the a-elimination phase lasts only a few minutes, and the p-elimination half life is 2-3 h. The compound is metabolized extensively
This work was supported in part by National Institutes of Health Grant GMS52387 to MED.
Accepted for publication July 31, 1998. Address correspondence to Marcel E. Durieux, MD, Department
of Anesthesiology, University of Virginia Health Center, PO Box 10010, Charlottesville, VA 22906-0010.
1186 An&h Analg 1998;87:1186-93
by the hepatic cytochrome ~450 system; its primary metabolite norketamine is only one-third to one-fifth as potent as the original compound but may be in- volved in the prolonged analgesic actions of ketamine. The metabolites of norketamine are excreted by the kidneys.
Classic ketamine anesthetic effects are best de- scribed as a dose-dependent central nervous system (CNS) depression that leads to a so-called dissociative state, characterized by profound analgesia and amne- sia but not necessarily loss of consciousness. Although not asleep, the subject seems completely unaware of the environment. Suggested mechanisms for this form of catalepsy include electrophysiologic inhibition of thalamocortical pathways and stimulation of the lim- bit system.
Ketamine has other effects besides analgesia and amnesia. Effects on the respiratory system are gener- ally beneficial: it is a well documented bronchodilator (5), it causes minimal respiratory depression with only mild hypercapnia (6) in clinically relevant doses, and protective airway reflexes are more likely to be pre- served than with other IV anesthetics. However, in- creased oral secretions can occur. Ketamine often pro- duces significant increases in blood pressure and heart rate (7), and increases in pulmonary artery pressure have been reported, especially in patients with preex- isting heart disease (8,9). These effects are due to sym- pathetic stimulation; ketamine’s direct effect on the heart is depressant, S(+) less than R(-) (10). Recovery time is dose-dependent, and emergence is, at times, complicated by psychotomimetic reactions (hallucina- tions, vivid dreams), which can be highly unpleasant. The manufacturer lists the presence of uncontrolled arterial hypertension or hypersensitivity to the drug as contraindications to the use of ketamine. However, caution has also been suggested when the drug is used in patients with coronary artery disease (11) or right heart failure (12).
Mechanisms of Action Ketamine’s neuropharmacology is complex. The com- pound interacts with multiple binding sites, including
01998 by the International Anesthesia Research Society 0003.ZYY9/98/$5.00
ANESTH ANALG 1998;87:1186-93
REVIEW ARTICLE KOHRS AND DURIEUX 1187 NEW USES FOR KETAMINE
HN-CH, H,C -NH
0 0
R (-) - ketamine S (+) - ketamine
Figure 1. Structural formulas of the two enantiomers of ketamine.
N-methyl-D-aspartate (NMDA) and non-NMDA glu- tamate receptors, nicotinic and muscarinic cholinergic, and monoaminergic and opioid receptors. In addition, interactions with voltage-dependent ion channels such as Na and L-type Ca channels have been de- scribed. Inhibition of neuronal Na channels provides a modest local anesthetic effect of the compound, whereas Ca channel blockade may be responsible for cerebral vasodilation (13).
All of these interactions may play a role in ket- amine’s pharmacological and clinical properties. However, NMDA receptor antagonism accounts for most of the analgesic, amnestic, psychotomimetic, and neuroprotective effects of the compound.
NMDA Glutamate Receptors
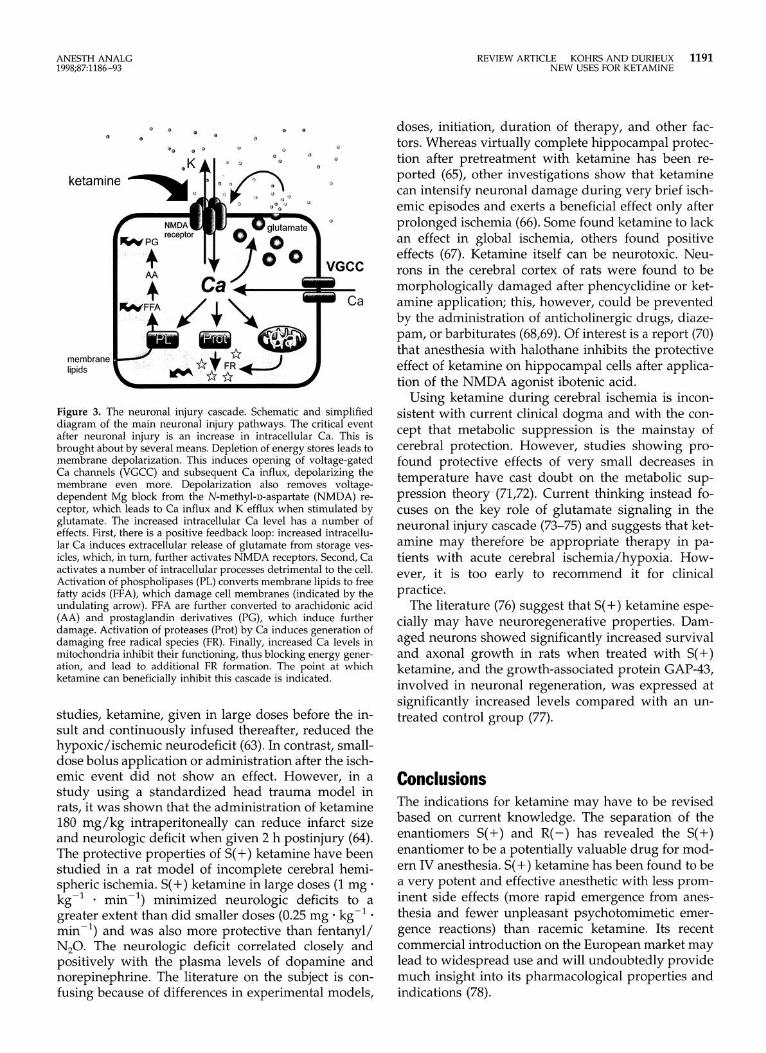
The NMDA receptor is an ionotropic receptor (ligand- gated ion channel) that is activated by glutamate, the most abundant excitatory neurotransmitter in the CNS (Fig. 2). The channel is permeable to Ca and, to a lesser degree, to Na and K. It requires glycine as an obliga- tory co-agonist and is inhibited by Mg in a voltage- dependent manner. NMDA receptors are, among many other functions, involved in the so called wind-up phenomenon (14), which plays a major role in the development of chronic pain.
The NMDA receptor is the postsynaptic site of action in ketamine’s reduction of polysynaptic stimulation in the CNS (15-17). Ketamine binds to the phencyclidine receptor in the NMDA channel and thus inhibits gluta- mate activation of the channel in a noncompetitive man- ner. The phencyclidine binding site partly overlaps with a binding site for Mg. The blockade is time-, concentration- and stimulation frequency-dependent (use-dependent) (18). The S(+) enantiomer has a three- to fourfold greater affinity for the receptor than the R( -) form, as reflected in the observed differences in their analgesic and anesthetic (19,20) potencies. Although the precise interactions between ketamine and NMDA re- ceptors are still being elucidated (21), enough evidence suggests a relation between ketamine’s analgesic and anesthetic properties and NMDA channel blockade
Figure 2. The N-methyl-D-aspartate (NMDA) receptor. Schematic diagram of the molecular structure of the NMDA glutamate receptor/channel complex. The receptor consists of five subunits surrounding a central ion channel permeable to Ca, K, and Na. Binding sites for the agonist glutamate and the obligatory co-agonist glycine are indicated. Competitive glutamate and glycine antago- nists act on these sites. One of the subunits has been removed to allow a view inside the ion channel, in which binding sites for ketamine and Mg are located. These compounds block NMDA receptor functioning noncompetitively. PCP = phencyclidine.
(21-23) to consider the NMDA receptor ketamine’s pri- mary site of anesthetic action. However, there are inter- actions with other systems that may also be relevant.
Non-NMDA Glutamate Receptors
Non-NMDA glutamate receptors exist in several classes, which are activated selectively by the agonists quisqualate, AMPA, or kainate. These receptors were previously thought not to interact with ketamine, but this was disproved in recent animal studies (24), which demonstrated inhibition by ketamine. The ef- fects are probably mediated through the glutamate/ NO/cGMP system. Not only NMDA receptor activa- tion stimulates NO synthesis (which then increases intracellular cGMP production) (25), but non-NMDA receptor activation does so as well (26,27). Besides playing a possible role in ketamine’s neuroprotective and sympathetic activating actions, ketamine-induced NO synthase inhibition may be involved in its anal- gesic effects (28). NO is known to play a role as a neurotransmitter, centrally as well as peripherally, and pain perception and NO are connected at least at the spinal level. In an animal model, the intrathecal administration of the NO-synthase inhibitor L-N-
monomethylarginine induced a dose-dependent an- tinociceptive response. Other analgesic substances (acetaminophen and other nonsteroidal antiinflamma- tory drugs) similarly interact with NO metabolism (29). These findings may partly explain some proper- ties of ketamine not caused by NMDA interaction alone.

1188 REVIEW ARTICLE KOHRS AND DURIEUX NEW USES FOR KETAMINE
Opioid Receptors
Agonist actions of ketamine on opioid receptors, members of the G-protein-coupled receptor class, seem to play a minor role in its analgesic effects (30). However, the psychotomimetic side effects of ket- amine may be explained by the interaction with K
opioid receptors, because K-agonists induce similar effects. Several investigations show likely interactions between ketamine and opioid receptors (31,32). Its affinity for these receptors ranks p > K > 6 (32). S(+) ketamine binds approximately two- to fourfold stron- ger to TV and K-receptors than does R(-). Still, the affinity of ketamine for these receptors is 10 (p) to 20 (K) times less than for the NMDA channel, which suggests that the interaction is not of major clinical importance. This is confirmed by findings that nalox- one does not reverse the analgesic effect of ketamine in humans (30). However, in an animal study, ketamine-induced small bowel smooth muscle con- traction could be partially reversed by naloxone (33).
ANESTH ANALG 1998;87:1186-93
GABA, Signaling
Cholinergic and Advenergic Signaling
Both nicotinic and muscarinic acetylcholine receptors are affected by ketamine (34), and, in clinical concen- trations, ketamine inhibits NMDA receptor-mediated acetylcholine release. The postsynaptic inhibitory ef- fect of ketamine on nicotinic acetylcholine receptors in skeletal muscle is not necessarily noticeable clinically, as ketamine increases muscle tone by central mecha- nisms. However, the additional administration of muscle relaxants can uncover this ketamine effect (34). Muscarinic receptors are also inhibited (35). S(+) ket- amine shows a twofold greater affinity for the musca- rinic receptor than does R(-) (30), although this was not confirmed in functional studies (36). Overall, how- ever, affinity for the muscarinic receptor is lo- to 20-fold less than NMDA receptor binding (37). Emer- gence side effects may be partly related to inhibition of cholinergic transmission.
R(-) ketamine inhibits the neuronal uptake of nor- epinephrine, and S( +) ketamine additionally inhibits extraneural uptake, thus inducing a prolonged synap- tic response and increased transfer of norepinephrine into the systemic circulation (34). The uptake of dopa- mine and 5-HT is inhibited similarly (38), which could lead to an increase in central dopaminergic activity. The 5-HT antagonist methysergide antagonizes the analgesic effects of intrathecal ketamine, implicating serotonergic mechanisms in ketamine analgesia (39). These mechanisms may also be involved in ketamine- related emesis, as ondansetron inhibits ketamine- induced currents through 5-HT receptors. Thus, influ- ences of ketamine on monoaminergic transmission seem very likely, although their role in the clinical effects of the compound are not yet clear.
GABA is the most common inhibitory neurotransmit- ter in the CNS, and GABA signaling neurons account for approximately 30% of all synaptic connections in the CNS. Investigations using GABA, receptors ex- pressed recombinantly in Xenopus laevis oocytes re- vealed a significant increase of GABA-induced Cl cur- rent after ketamine application (40). Similar effects were observed in olfactory cortex and hippocampal slices (41). Although an effect of ketamine on GABA signaling seems established (42), the concentrations used were higher than those used clinically. Based on current knowledge, this interaction seems to be of minor importance for clinical practice (34).
S( +) Ketamine In 1992, the Food and Drug Administration stated that separation of stereoisomers had not received appro- priate attention in commercial drug development and that, despite technical difficulties and high cost, focus- ing on this issue could open new horizons in thera- peutics. The isomers of ketamine are a good example. It has been known since the late 1970s that the ket- amine enantiomers exhibit pharmacologic and clinical differences. Receptor studies in animal models show that S( +) ketamine has approximately fourfold greater affinity at phencyclidine binding sites on the NMDA receptor than does R(-) ketamine.
Not all of ketamine’s effects are stereoselective. Nor- epinephrine release is inhibited in a nonstereoselective manner at clinically relevant concentrations. How- ever, its uptake is influenced stereoselectively: both isomers inhibit neuronal uptake, whereas S(+) ket- amine additionally inhibits extraneuronal uptake. Muscarinic receptors (36) and Ca channels (43) are inhibited nonstereoselectively. Interestingly, serotonin transport is inhibited twofold more potently by R(-) ketamine.
Animal studies have not revealed significant phar- macokinetic differences between the enantiomers and the racemic mixture. After subcutaneous application, similar plasma and brain concentration curves have been found. In a clinical study, however, a signifi- cantly higher elimination rate was observed for S(+) ketamine compared with the racemate (44).
The increased inhibitory potency at the NMDA re- ceptor combined with similar pharmacokinetics sug- gest that S(+) ketamine may be an interesting clinical drug, and its pharmacological properties have been studied in some detail. Table 1 summarizes the clini- cally relevant differences between the isomers.
Anesthetic/Hypnotic/Analgesic Effects
In rats and mice, S(+) ketamine exhibits 1.5- to 3-fold greater hypnotic and 3-fold greater analgesic potency

ANESTH ANALG 1998;87:1186-93
REVIEW ARTICLE KOHRS AND DURIEUX 1189 NEW USES FOR KETAMINE
Table 1. Effects of S( +) and R( -) Ketamine
Variable SC+) WI
NMDA receptor 4 1 affinity
Plasma concentration 1 1 Cerebral concentration 1 2-3 Elimination rate 1 0.8-l Side effect profile Similar to racemic ketamine LDs,/ED,o 2.5 1 Anesthetic potency 3 1
Data are expressed as relative effects. NMDA = N-methyl-D-aspartate, LD,,, = 50% lethal dose, ED,,, = 50%
effective dose.
than the R( -) compound. Compared with the racemic mixture, S(+) ketamine is twice as potent. The calcu- lated therapeutic index of S(+) ketamine seems to be 2.5-fold greater than that of the mixture or R( -) alone (45). A double-blind study with 60 patients (20) rein- forced these findings: S(+) ketamine was 3.4-fold more potent an anesthetic than R(-) and 2-fold more potent than the racemate.
Studies in rats and mice show that S(+) ketamine induces less spontaneous movement than does R(-) ketamine in comparable anesthetic doses. An explana- tion may be that, whereas plasma levels are equal after administration of S( +) or R( -) ketamine, cerebral lev- els of R(-) norketamine are two- to threefold greater than those of S( +) norketamine. In mice, R( -) induces more prominent CNS stimulation than does S( +) ket- amine, thus making spontaneous movements more likely.
As to hemodynamic response, no significant differ- ences between the compounds could be demon- strated, despite the fact that catecholamine plasma levels are significantly lower after S(+) than R(-) ketamine anesthesia (46,47).
Emergence from Anesthesia and Psychotomimetic Effects
S( +) ketamine and R( -) ketamine have a clinical po- tency ratio of approximately 2:l. Thus, only one-half the dose of S(+) ketamine should suffice for the in- duction of anesthesia, possibly affecting recovery time. Several clinical studies have assessed the dura- tion of recovery after administration of the racemic mixture or S( +) ketamine. R( -) was excluded because its clinical potency is insufficient (44). In virtually every study, the recovery phase was clearly shortened when S( +) ketamine was used compared with racemic ketamine. This was true regardless of whether the compounds were administered as a single IV bolus, as a bolus followed by continuous infusion, or by IM injection (46,48,49).
Classical side effects after ketamine anesthesia (am- nesia, altered short-term memory, decreased ability to
concentrate, decreased vigilance, altered cognitive performance, hallucinations, nightmares, nausea and vomiting) were observed with similar incidence after S(+) or racemic mixture administration (19). At least for the racemic mixture, it was found that the inci- dence of these effects is clearly related to the ketamine plasma concentration (50), making psychedelic effects less likely (although still possible) at lower drug concentrations. Convincing evidence for a lower inci- dence of psychotomimetic side effects after S(+) ket- amine administration could not be documented. Nonetheless, the patients felt more comfortable after S( +) ketamine (49), and a larger proportion of patients would be willing to have a repeat anesthetic with S( +)compared with the racemic mixture (85”/0 vs 65%), mainly because of decreased agitation, disorientation, and anxiety (19). The additional administration of a benzodiazepine provided both drugs with a signi- ficantly higher rate of acceptance, but the duration of recovery also increased significantly with this regimen.
Taken together, these data suggest that S(+) ket- amine allows the use of significantly smaller doses, with a resultant faster recovery and (possibly) some diminution in side effects. As a result, the compound has been approved for clinical use in Europe; there- fore, additional clinical experience will soon be available.
Ketamine and Preemptive Analgesia At small doses (0.1-0.5 mg/kg), ketamine has a no- ticeable analgesic action, which can be used to supple- ment regional or local anesthesia. A number of studies have suggested that administration of ketamine be- fore the noxious stimulus occurs is even more effec- tive (51-53). This effect is referred to as preemptive analgesia.
The goal of preemptive analgesia is to prevent or reduce the development of a “memory” of the pain stimulus in the nervous system (54,55), thereby less- ening postoperative analgesic requirements. When a massive barrage of afferent nociceptive impulses reaches the spinal cord, a hyperexcitable state of CNS sensitization known as wind-up results (55). NMDA receptors seem to be responsible for pain memory (as they are responsible for other forms of memory), and their blockade can contribute significantly to the pre- vention of pain (56). NMDA antagonists prevent the induction of central sensitization and even abolish hypersensitivity once it is established (56). Ketamine is the only NMDA antagonist approved by the Food and Drug Administration (although magnesium also has significant NMDA receptor-blocking properties), and several studies have demonstrated the effect of pre- emptive administration of small doses of ketamine on

1190 REVIEW ARTlCLE KOHRS AND DURIEUX NEW USES FOR KETAMINE
ANESTH ANALG lYY8;87:1186-93
postoperative pain, measured as a reduction in opioid requirements (57,58). These effects require remarkably small doses of the drug and last for a relatively pro- longed period of time (~6 h). For example, patients undergoing gallbladder surgery who received ket- amine were found to have diminished analgesic re- quirements after a single dose of 0.25 mg/kg IV ket- amine versus patients who did not receive ketamine (58). When presurgery versus postsurgery administra- tion was compared, ketamine administered before skin incision (0.5 mg/kg bolus followed by continuous rate of 10 PLg * kg-’ * mini’) provided better pain control than ketamine given after wound closure (57).
Although the administration schedule and dose var- ies among studies, preoperatively (preemptively) ad- ministered ketamine seems to reduce the amount of narcotics required postoperatively for pain control. Opioid requirements were reduced 40%60% on av- erage (57,58). Whether this translates to a lower inci- dence of opioid-related adverse effects is as yet un- known, although it seems likely. Psychotomimetic responses to these small ketamine doses have not been found troublesome. The role of S(+) ketamine in pre- emptive analgesia has not yet been studied.
Ketamine and Neurosurgery Historically, ketamine has been felt to be contraindi- cated in patients at risk of increases in intracranial pressure (ICI’). However, reports about its neuropro- tective actions have led to a reevaluation of this issue.
Effects on ICP
ICI’ can increase after the administration of racemic ketamine (no data are available yet for S( +) ketamine). This is especially true when the ICI’ is already in- creased before ketamine administration and when the drug is given at doses >l mg/kg IV. Two reasons are provided for the effect on ICI’: cerebral blood volume may increase passively, caused by increased arterial pressure during a period of impaired cerebrovascular autoregulation; and (probably more important) in- creases in arterial Pco,, due to ketamine-induced ven- tilatory depression, may contribute (59). It could be shown that, independent of the preexisting ICI’, ket- amine administration (0.5-5 mg/kg) did not increase ICI’ when normocapnia was maintained with con- trolled ventilation (60). Although some studies show an ICI’ increase during normocapnia after the admin- istration of 2 mg/kg ketamine, this increase could be avoided by mild hyperventilation or the administra- tion of benzodiazepines. This is not different from the situation with most volatile drugs, which are used routinely in patients with increased ICI’. It has been shown that neither 1.5, 3, nor 5 mg/kg IV ketamine increased ICI’ in patients with head trauma during
controlled ventilation and sedation with propofol; in- stead, the ICI’ decreased after ketamine administra- tion (61).
Effects on Cerebral Blood Flow
Studies in dogs have shown that racemic ketamine increases cerebral blood flow (CBF) in the presence of the cerebral vasodilator N,O. In contrast, other animal studies using barbiturates as a background anesthetic showed a decrease in CBF after ketamine administra- tion. This suggests that the cerebrovascular effects of ketamine are related to the preexisting cerebrovascu- lar tone. When ventilation is not controlled, part of the vasodilatory effect may result from increased Pco,. However, ICI’ can increase even when the Pco, is constant, and stimulation of cerebral metabolic rate by ketamine has been suggested to explain the increase in CBF. Ketamine inhibits certain cerebral regions and stimulates others at the same time, changes which are reflected as decreased CBF in areas with reduced me- tabolism and increased CBF in areas with higher me- tabolism (62). The net balance of these determines the total effect on CBF. In addition, ketamine acts in zlitvo as a Ca channel antagonist and increases blood flow by direct vasodilation.
In summary, racemic ketamine can increase CBF dependent on preexisting vascular resistance. The mechanisms most likely involve hypercapnia, region- ally specific stimulation and inhibition of cerebral me- tabolism, and direct vasodilation by Ca channel block. The response of the cerebral autoregulation to racemic ketamine has not been systemically studied yet, but S(+) ketamine does not affect this autoregulation. It also has been proven that ketamine does not trigger seizure activity but, much more likely, prevents sei- zures by NMDA receptor antagonism.
Neuvopvotection and Neuroregeneration
Cerebral hypoxia/ischemia initiates a pathophysio- logic cascade that leads to membrane and cell destruc- tion and neuronal death (Fig. 3). In this cascade, the activation of NMDA and non-NMDA receptors plays an important role. If these receptors are stimulated by very high levels of glutamate or aspartate, the result- ant transmembrane flux and intracellular accumula- tion of Na and Ca leads to cell swelling and activation of cellular pathways, eventually inducing cell death. In particular, NMDA receptor antagonists have re- ceived attention as neuroprotective drugs, although neuronal degeneration correlates more closely with the distribution of AMPA than of NMDA receptors, and AMPA antagonists prevent the degeneration at least as effectively as NMDA antagonists. In animal
ANESTH ANALG 1998;87:1186-93
REVIEW ARTICLE KOHRS AND DURIEUX 1191 NEW USES FOR KETAMINE
lipids
VGCC 3 FL
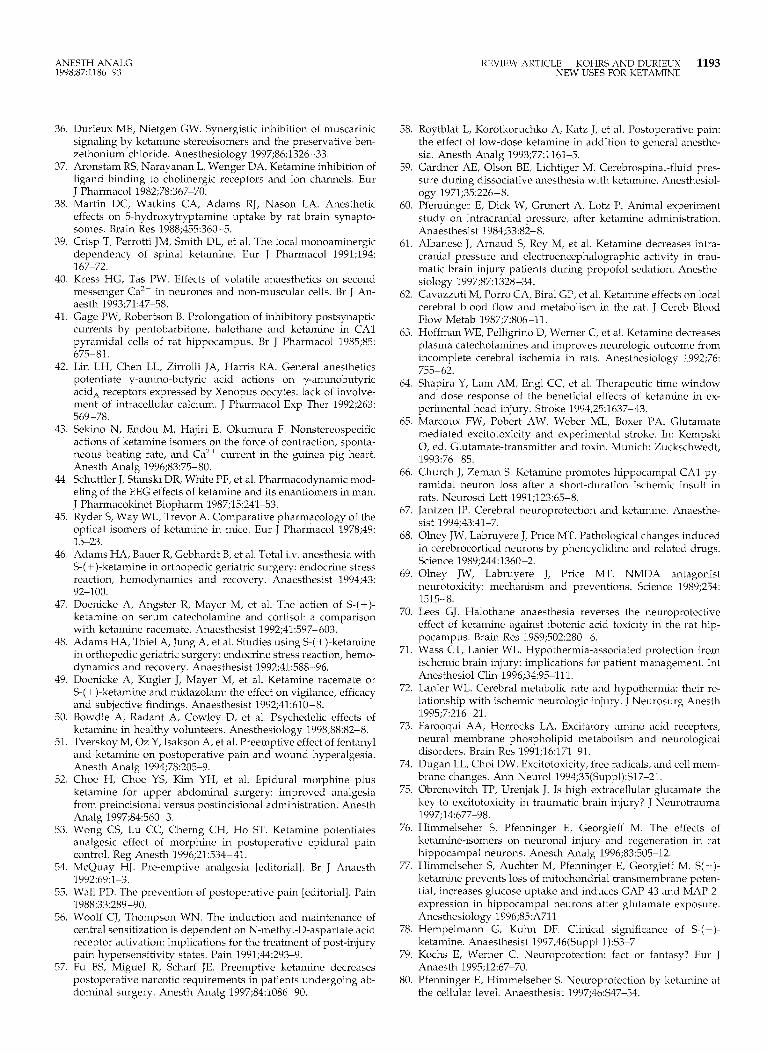
Figure 3. The neuronal injury cascade. Schematic and simplified diagram of the main neuronal injury pathways. The critical event after neuronal injury is an increase in intracellular Ca. This is brought about by several means. Depletion of energy stores leads to membrane depolarization. This induces opening of voltage-gated Ca channels (VGCC) and subsequent Ca influx, depolarizing the membrane even more. Depolarization also removes voltage- dependent Mg block from the N-methyl-o-aspartate (NMDA) re- ceptor, which leads to Ca influx and K efflux when stimulated by glutamate. The increased intracellular Ca level has a number of effects. First, there is a positive feedback loop: increased intracellu- lar Ca induces extracellular release of glutamate from storage ves- icles, which, in turn, further activates NMDA receptors. Second, Ca activates a number of intracellular processes detrimental to the cell. Activation of phospholipases (PL) converts membrane lipids to free fatty acids (FFA), which damage cell membranes (indicated by the undulating arrow). FFA are further converted to arachidonic acid (AA) and prostaglandin derivatives (PG), which induce further damage. Activation of proteases (Prot) by Ca induces generation of damaging free radical species (FR). Finally, increased Ca levels in mitochondria inhibit their functioning, thus blocking energy gener- ation, and lead to additional FR formation. The noint at which ketamine can beneficially inhibit this cascade is indicated.
studies, ketamine, given in large doses before the in- sult and continuously infused thereafter, reduced the hypoxic/ischemic neurodeficit (63). In contrast, small- dose bolus application or administration after the isch- emit event did not show an effect. However, in a study using a standardized head trauma model in rats, it was shown that the administration of ketamine 180 mg/kg intraperitoneally can reduce infarct size and neurologic deficit when given 2 h postinjury (64). The protective properties of S( +) ketamine have been studied in a rat model of incomplete cerebral hemi- spheric ischemia. S( +) ketamine in large doses (1 mg * kg-’ . min-‘) minimized neurologic deficits to a greater extent than did smaller doses (0.25 mg * kg-i * min-‘) and was also more protective than fentanyl/ N,O. The neurologic deficit correlated closely and positively with the plasma levels of dopamine and norepinephrine. The literature on the subject is con- fusing because of differences in experimental models,
doses, initiation, duration of therapy, and other fac- tors. Whereas virtually complete hippocampal protec- tion after pretreatment with ketamine has been re- ported (65), other investigations show that ketamine can intensify neuronal damage during very brief isch- emit episodes and exerts a beneficial effect only after prolonged ischemia (66). Some found ketamine to lack an effect in global ischemia, others found positive effects (67). Ketamine itself can be neurotoxic. Neu- rons in the cerebral cortex of rats were found to be morphologically damaged after phencyclidine or ket- amine application; this, however, could be prevented by the administration of anticholinergic drugs, diaze- pam, or barbiturates (68,69). Of interest is a report (70) that anesthesia with halothane inhibits the protective effect of ketamine on hippocampal cells after applica- tion of the NMDA agonist ibotenic acid.
Using ketamine during cerebral ischemia is incon- sistent with current clinical dogma and with the con- cept that metabolic suppression is the mainstay of cerebral protection. However, studies showing pro- found protective effects of very small decreases in temperature have cast doubt on the metabolic sup- pression theory (71,72). Current thinking instead fo- cuses on the key role of glutamate signaling in the neuronal injury cascade (73-75) and suggests that ket- amine may therefore be appropriate therapy in pa- tients with acute cerebral ischemia/hypoxia. How- ever, it is too early to recommend it for clinical practice.
The literature (76) suggest that S(+) ketamine espe- cially may have neuroregenerative properties. Dam- aged neurons showed significantly increased survival and axonal growth in rats when treated with S(+) ketamine, and the growth-associated protein GAP-43, involved in neuronal regeneration, was expressed at significantly increased levels compared with an un- treated control group (77).
Conclusions The indications for ketamine may have to be revised based on current knowledge. The separation of the enantiomers S(+) and R( -) has revealed the S(+) enantiomer to be a potentially valuable drug for mod- ern IV anesthesia. S( +) ketamine has been found to be a very potent and effective anesthetic with less prom- inent side effects (more rapid emergence from anes- thesia and fewer unpleasant psychotomimetic emer- gence reactions) than racemic ketamine. Its recent commercial introduction on the European market may lead to widespread use and will undoubtedly provide much insight into its pharmacological properties and indications (78).

1192 REVIEW ARTICLE KOHRS AND IIURIEUX NEW USFS FOR KETAMINF
ANESTH ANALG lYY8;87:1186-93
K&amine may have neuroprotective and even neu- roregenerative effects (76,77). Some authors are re- served or even skeptical, others see the results ob- tained thus far more positively (79) and even propose new indications (80). Although many issues (such as time of administration and dose) remain to be re- solved, the preponderance of evidence favors a neu- roprotective action. Inconsistencies among studies probably arise from the complexity of the injury cas- cade initiated after brain injury. It seems likely that neither racemic nor S(+) ketamine will be clinically successful if used as sole therapy; only when used in combination with other drugs and treatments can sec- ondary injury be effectively limited. It seems con- firmed that ketamine does not increase ICI’ when the blood pressure is controlled and mild hypocapnia is achieved. Thus, the contraindication for ketamine use in neurosurgical patients is only a relative one, and when further preclinical and clinical studies confirm a neuroprotective effect of the compound, ketamine and, more likely, S( +) ketamine may well find a place in the neuroanesthesiology drug cart.
Finally, the analgesic properties of small-dose ket- amine have been rediscovered. Current data strongly suggest that the preemptive administration of ket- amine can have profound effects on postoperative analgesic requirements (57,58) with minimal risk and side effects. This provides the anesthesia practitioner with another useful tool in the management of peri- operative pain.
We thank John C. Rowlingson, MD, for his critical review of the manuscript.
References 1. Hirota K, Lambert DG. Ketamine: its mechanisms of action and
unusual clinical uses. Br J Anaesth 1996;77:441&4. 2. Hudspith MJ. Glutamate: a role in normal brain function, an-
aesthesia, analgesia and CNS injury. Br J Anaesth 1997;78: 731-47.
3. White PF. Ketamine: its pharmacology and therapeutic uses. Anesthesiology 1982;56:119-36.
4. Reich DL. Ketamine: an update on the first twenty-five years of clinical experience. Can J Anaesth 1989;36:186-97.
5. Haas DA, Harper DG. Ketamine: a review of its pharmacologic properties and use in ambulatory anesthesia. Anesth Prog 1992; 39:61-S.
6. Werner C, Reeker W, Engelhard K. Ketamine racemate and S-(+)-ketamine: cerebrooascular effects and neuroprotection following focal ischemia. Anaesthesist 1997;46:55-60.
7. Zielmann S, Kazmaier S, Schnull S, Weyland A. S-(+)-ketamine and circulation. Anaesthesist 1997;46(Suppl 1):43-6.
8. Gutzke GE, Shah KB, Glisson SN. Cardiac transplantation: a prospective comparison of ketamine and sufentanil for anes- thetic induction. J Cardiothorac Anesth 1989;3:389-95.
9. Berman W Jr, Fripp RR, Rubler M, Alderete L. Hemodynamic effects of ketamine in children undergoing cardiac catheteriza- tion. Pediatr Cardiol 1990;11:7226.
10. Graf BM, Viccnzi MN, Martin E, et al. Ketamine has stereospe- cific effects in the isolated perfused guinea pig heart. Anesthe- siology 1995;82: 1426-37.
11. Felts JD, Afonso S, Rowe GG. Systemic and coronary hemody- namic effects of ketamine in intact anaesthetized and unanaes- thetized dogs. Br J Anaesth 1975;47:686-94.
12. Johnstone M. The cardiovascular effects of ketamine in man. Anaesthesia 1976;31:873-82.
13. Wong BS, Martin CD. Ketamine inhibition of cytoplasmic cal- cium signalling in rat pheochromocytoma (PC-12) cells. Life Sci 1993;53:359-64.
14. Woolf CJ. Recent advances in the pathophysiology of acute pain. Br J Anaesth 1989;63:139946.
15. Brockmeyer DM, Kendig JJ. Selective effects of ketamine on amino acid-mediated pathways in neonatal rat spinal cord. Br J Anaesth 1995;74:79984.
16. MacDonald JF, Nowak LM. Mechanisms of blockade of excita- tory amino acid receptor channels. Trends Pharmacol Sci 1990; 11:167-70.
17. Yamamura T, Harada K, Okamura A, Kemmotsu 0. Is the site of action of ketamine anesthesia the N-methyl-D-aspartate re- ceptor? Anesthesiology 1990;72:704-10.
18. MacDonald JF, Milikovic Z, Pennefaher P. Use-dependent block of excitatory amino acid currents in cultured neurons by ket- amine. J Neurophysiol 1987;58:251-66.
19. White PF, Ham J, Way WL, Trevor AJ. Pharmacology of ket- amine isomers in surgical patients. Anesthesiology 1980;52: 231-9.
20. White PF, Schuttler J, Shafer A, et al. Comparative pharmacol- ogy of the ketamine isomers: studies in volunteers. Br J Anaesth 1985;57:197-203.
21. Irifune M, Shimizu T, Nomoto M, Fukuda T. Ketamine-induced anesthesia involves the N-methyl-D-aspartate receptor-channel complex in mice. Brain Res 1992;569:1-9.
22. Nasstrom J, Karlsson U, Post C. Anti-nociceptive actions of different classes of excitatory amino acid receptor antagonists in mice. Eur J Pharmacol 1992;212:21&9.
23. Oye I, Paulsen 0, Maurset A. Effects of ketamine on sensory perception: evidence for a role of N-methyl-D-aspartate recep- tors. J Pharmacol Exp Ther 1992;260:1209-13.
24. Gonzales JM, Loeb AL, Reichard PS, Irvine S. Ketamine inhibits glutamate-, N-methyl-D-aspartate- and quisqualate-stimulated cGMP production in cultured cerebral neurons. Anesthesiology 1995;82:205513.
25. Garthwaite J. Glutamate, nitric oxide and cell-cell signalling in the nervous system. Trends Neurosci 1991;14:60-7.
26. Marin P, Quignard JF, Lafon-Cazal M, Bockaert J. Non-classical glutamate receptors, blocked by both NMDA and non-NMDA antagonists, stimulate nitric oxide production in neurones. Neu- ropharmacology 1993;32:29-36.
27. Wood PL, Emmett MR, Rao TS, et al. Inhibition of nitric oxide synthase blocks N-methyl-D-aspartate-, quisqualate-, kainate-, harmaline-, and pentylene-tetrazole-dependent increases in cer- ebellar cyclic GMP in 7k~. J Neurochem 1990;55:346-8.
28. Gordh T, Karlsten R, Kristensen J. Intervention with spinal NMDA, adenosine and NO systems for pain modulation. Ann Med 1995;27:229-34.
29. Bjorkman R, Hallman K, Hedner J, et al. Acetaminophen blocks spinal hyperalgesia induced by NMDA and substance P. Pain 1994;57:259-64.
30. Hustveit 0, Maurset A, Oye 1. Interaction of the chiral forms of ketamine with opioid, phencyclidine, and muscarinic receptors. Pharmacol Toxic01 1995;77:355-9.
31. Finck AD, Ngai SH. Opiate receptor mediation of ketamine analgesia. Anesthesiology 1982;56:291--7.
32. Smith DJ, Bouchal RL, desanctis CA, et al. Properties of the interaction between ketamine and opiate binding sites in viva and in vitro. Neuropharmacology 1982;26:1253-60.
33. Bansinath M, Warner W, Tang CK, et al. On the mechanism of the interaction of ketamine and halothane in vitro. Gen Pharma- co1 1992;23:1183-7.
34. Kress HG. Actions of ketamine not related to NMDA and opiate receptors. Anaesthesist 1994;43(Suppl 2):S15-24.
35. Durieux ME. Inhibition by ketamine of muscarinic acetylcholine receptor function. Anesth Analg 1995;81:57-62.
ANESTH ANALG 1998;87:1186-93
REVIEW ARTICLE KOHRS AND DURIEUX 1193 NEW USES FOR KETAMTNE
36. Durieux ME, Nietgen GW. Synergistic inhibition of muscarinic signaling by ketamine stereoisomers and the preservative ben- zethonium chloride. Anesthesiology 1997;86:1326-33.
37. Aronstam RS, Narayanan L, Wenger DA. Ketamine inhibition of ligand binding to cholinergic receptors and ion channels. Em J Pharmacol 1982;78:367-70.
38. Martin DC, Watkins CA, Adams RJ, Nason LA. Anesthetic effects on 5-hydroxytryptamine uptake by rat brain synapto- somes. Brain Res 1988;455:360-5.
39. Crisp T, Perrotti JM, Smith DL, et al. The local monoaminergic dependency of spinal ketamine. Eur J Pharmacol 1991;194: 167-72.
40. Kress HG, Tas PW. Effects of volatile anaesthetics on second messenger Ca ‘+ in neurones and non-muscular cells. Br J An- aesth 1993;71:47-58.
41. Gage PW, Robertson B. Prolongation of inhibitory postsynaptic currents by pentobarbitone, halothane and ketamine in CA1 pyramidal cells of rat hippocampus. Br J Pharmacol 1985;85: 675-81.
42. Lin LH, Chen LL, Zirrolli JA, Harris RA. General anesthetics potentiate y-amino-butyric acid actions on y-aminobutyric acid, receptors expressed by Xenopus oocytes: lack of involve- ment of intracellular calcium. J Pharmacol Exp Ther 1992;263: 569-78.
43. Sekino N, Endou M, Hajiri E, Okumura F. Nonstereospecific actions of ketamine isomers on the force of contraction, sponta- neous beating rate, and Ca’+ current in the guinea pig heart. Anesth Analg 1996;83:75-80.
44. Schuttler J, Stanski DR, White PF, et al. Pharmacodynamic mod- eling of the EEG effects of ketamine and its enantiomers in man. J Pharmacokinet Biopharm 1987;15:241-53.
45. Ryder S, Way WL, Trevor A. Comparative pharmacology of the optical isomers of ketamine in mice. Eur J Pharmacol 1978;49: 15-23.
46. Adams HA, Bauer R, Gebhardt B, et al. Total iv. anesthesia with S-( +)-ketamine in orthopedic geriatric surgery: endocrine stress reaction, hemodynamics and recovery. Anaesthesist 1994;43: 92-100.
47. Doenicke A, Angster R, Mayer M, et al. The action of S-(+)- ketamine on serum catecholamine and cortisol: a comparison with ketamine racemate. Anaesthesist 1992;41:597-603.
48. Adams HA, Thiel A, Jung A, et al. Studies using S-( +)-ketamine in orthopedic geriatric surgery: endocrine stress reaction, hemo- dynamics and recovery. Anaesthesist 1992;41:588-96.
49. Doenicke A, Kugler J, Mayer M, et al. Ketamine racemate or S-( +)-ketamine and midazolam: the effect on vigilance, efficacy and subjective findings. Anaesthesist 1992;41:610-8.
50. Bowdle A, Radant A, Cowley D, et al. Psychedelic effects of ketamine in healthy volunteers, Anesthesiology 1998;88:82-8.
51. Tverskoy M, Oz Y, Isakson A, et al. Preemptive effect of fentanyl and ketamine on postoperative pain and wound hyperalgesia. Anesth Analg 1994;78:205-9.
52. Choe H, Choe YS, Kim YH, et al. Epidural morphine plus ketamine for upper abdominal surgery: improved analgesia from preincisional versus postincisional administration, Anesth Analg 1997;84:560-3.
53. Wong CS, Lu CC, Cherng CH, Ho ST. Ketamine potentiates analgesic effect of morphine in postoperative epidural pain control. Reg Anesth 1996;21:534441.
54. McQuay HJ. Pre-emptive analgesia [editorial]. Br J Anaesth 1992;69:1-3.
55. Wall PD. The prevention of postoperative pain [editorial]. Pain 1988;33:289-90.
56. Woolf CJ, Thompson WN. The induction and maintenance of central sensitization is dependent on N-methyl-D-aspartate acid receptor activation: implications for the treatment of post-injury pain hypersensitivity states. Pain 1991;44:293-9.
57. Fu ES, Miguel R, Scharf JE. Preemptive ketamine decreases postoperative narcotic requirements in patients undergoing ab- dominal surgery. Anesth Analg 1997;84:1086-90.
58. Roytblat L, Korotkoruchko A, Katz J, et al. Postoperative pain: the effect of low-dose ketamine in addition to general anesthe- sia. Anesth Analg 1993;77:1161-5.
59. Gardner AE, Olson BE, Lichtiger M. Cerebrospinal-fluid pres- sure during dissociative anesthesia with ketamine. Anesthesiol- ogy 1971;35:226-8.
60. Pfenninger E, Dick W, Grunert A, Lotz I’. Animal experiment study on intracranial pressure, after ketamine administration. Anaesthesist 1984;33:82-8.
61. Albanese J, Arnaud S, Rey M, et al. Ketamine decreases intra- cranial pressure and electroencephalographic activity in trau- matic brain injury patients during propofol sedation. Anesthe- siology 1997;87:1328-34.
62. Cavazzuti M, Porro CA, Biral GP, et al. K&amine effects on local cerebral blood flow and metabolism in the rat. J Cereb Blood Flow Metab 1987;7:806~11.
63. Hoffman WE, Pelligrino D, Werner C, et al. Ketamine decreases plasma catecholamines and improves neurologic outcome from incomplete cerebral ischemia in rats. Anesthesiology 1992;76: 755- 62.
64. Shapira Y, Lam AM, Engl CC, et al. Therapeutic time window and dose response of the beneficial effects of ketamine in ex- perimental head injury. Stroke 1994;25:1637-43.
65. Marcoux FW, Pobert AW, Weber ML, Boxer PA. Glutamate mediated excitotoxicity and experimental stroke. In: Kempski 0, ed. Glutamate-transmitter and toxin. Munich: Zuckschwedt, 1993:76-85.
66. Church J, Zeman S. Ketamine promotes hippocampal CA1 py- ramidal neuron loss after a short-duration ischemic insult in rats. Neurosci Lett 1991;123:65-8.
67. Jantzen JP. Cerebral neuroprotection and ketamine. Anaesthe- sist 1994;43:41-7.
68. Olney JW, Labruyere J, Price MT. Pathological changes induced in cerebrocortical neurons by phencyclidine and related drugs. Science 1989;244:1360-2.
69. Olney JW, Labruyere J, Price MT. NMDA antagonist neurotoxicity: mechanism and preventions. Science 1989;254: 1515-8.
70. Lees GJ. Halothane anaesthesia reverses the neuroprotective effect of ketamine against ibotenic acid toxicity in the rat hip- pocampus. Brain Res 1989;502:280-6.
71. Wass CT, Lanier WL. Hypothermia-associated protection from ischemic brain injury: implications for patient management. Int Anesthesiol Clin 1996;34:95-111.
72. Lanier WL. Cerebral metabolic rate and hypothermia: their re- lationship with ischemic neurologic injury. J Neurosurg Anesth 1995;7:216-21.
73. Farooqui AA, Horrocks LA. Excitatory amino acid receptors, neural membrane phospholipid metabolism and neurological disorders. Brain Res 1991;16:171-91.
74. Dugan LL, Choi DW. Excitotoxicity, free radicals, and cell mem- brane changes. Ann Neurol 1994;35(Suppl):S17-21.
75. Obrenovitch TP, Urenjak J. Is high extracellular glutamate the key to excitotoxicity in traumatic brain injury? J Neurotrauma 1997;14:677-98.
76. Himmelseher S, Pfenninger E, Georgieff M. The effects of ketamine-isomers on neuronal injury and regeneration in rat hippocampal neurons. Anesth Analg 1996;83:505-12.
77. Himmelseher S, Auchter M, Pfenninger E, Georgieff M. S(+)- ketamine prevents loss of mitochondrial transmembrane poten- tial, increases glucose uptake and induces GAP-43 and MAP-2- expression in hippocampal neurons after glutamate exposure. Anesthesiology 1996;85:A711
78. Hempelmann G, Kuhn DF. Clinical significance of S-( +)- ketamine. Anaesthesist 1997;46(Suppl l):S3-7
79. Kochs E, Werner C. Neuroprotection: fact or fantasy? Eur J Anaesth 1995;12:67-70.
80. Pfenninger E, Himmelseher S. Neuroprotection by ketamine at the cellular level. Anaesthesist 1997;46:S47-54.






