
Gauging performance in below-the-knee intervention
Dr. Costantino Del GiudiceVascular and oncological interventional radiology
Paris Descartes University
January 23, 2019

Disclosure
Speaker name:
Costantino Del Giudice
I have the following potential conflicts of interest to report:
X Consulting Boston Scientific

BTK intervention todayPercutaneous transluminal angioplasty (PTA)
compared to surgical bypass allows for multi-
vessel revascularization, using a less invasive
approach with similar outcomes1-3
1) Jaff MR et al, Ann Vasc Dis. 2015;8:343–57.
2) Faglia E et al Diabetes Care. 2009;32:822–7.
3) Gandini R et al Cardiovasc Intervent Radiol. 2013 Feb;36(1):75-83
4) Ferraresi R, et al Eur Soc Vasc Surg. 2009;37:336–42.
Facilitated by :
Improved techniques...
Dedicated devices…

THE BIG PROBLEM
1) Ferraresi R, et al Eur Soc Vasc Surg. 2009;37:336–42.
2) Schmidt et al. Catheter Cardiovasc Interv 2010;76(7):1047–54
3) Iida e al. Eur J Vasc Endovasc Surg 2012;44(4):425–31.
Restenosis is the “Achilles's
heel” of this approach with a
rate of 42% at 1-year follow-
up1
3-month angiographic patency shows a higher rate of
restenosis ranging from 68.8% to 73%2-3

Why doesn’t PTA work?
Immediate technical
results
- Flow limiting
dissection
- Elastic Recoil
Mid and long term outcomes
- Re-stenosis
Prolonged PTA
Stenting
Drug eluting
technologies
Antiplatelet therapy
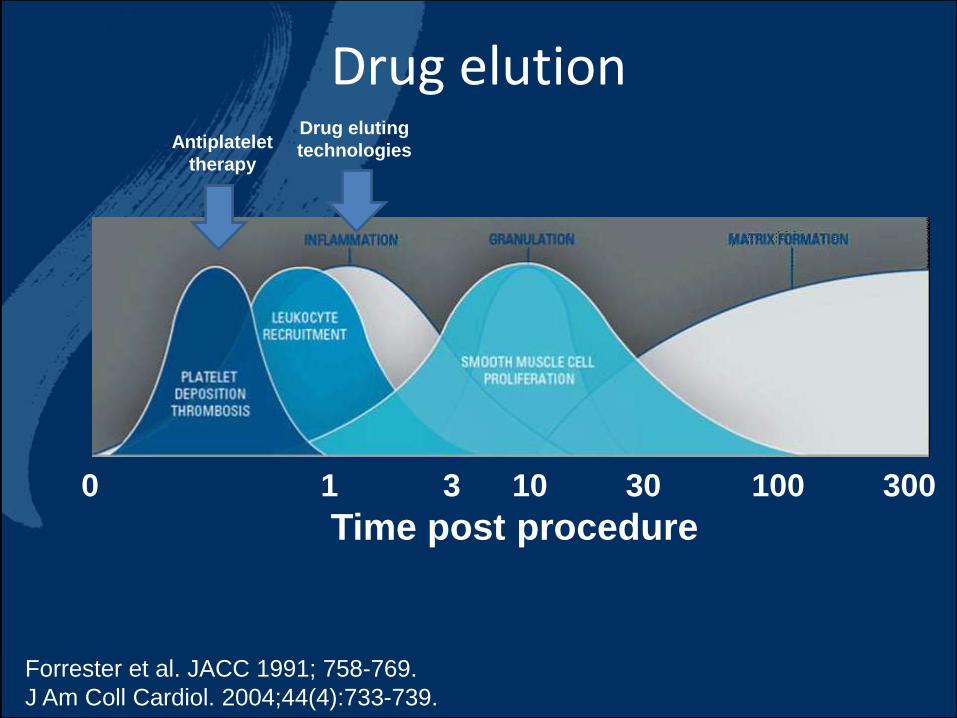
Drug elution
0 1 3 10 30 100 300
Time post procedure
Forrester et al. JACC 1991; 758-769.
J Am Coll Cardiol. 2004;44(4):733-739.
Antiplatelet
therapy
Drug eluting
technologies

How to use drug elution?
DCB DES
Advantages
- No need for scaffold
- Fast procedure
Disadvantages
- Reduced efficacy on recoil/calcification
- No action on dissection
- Loss of drug during implantation
Advantages
- Prolonged release of drug
- Action on dissection, recoil and
calcification
Disadvantages
- Absence of self expandable DES on
market at the moment
- Permanent implant

Actual data on DCB in BTK (1)
Restenosis
TLR
Liu et al Vascular and Endovascular Surgery2017, Vol. 51(2) 72-83
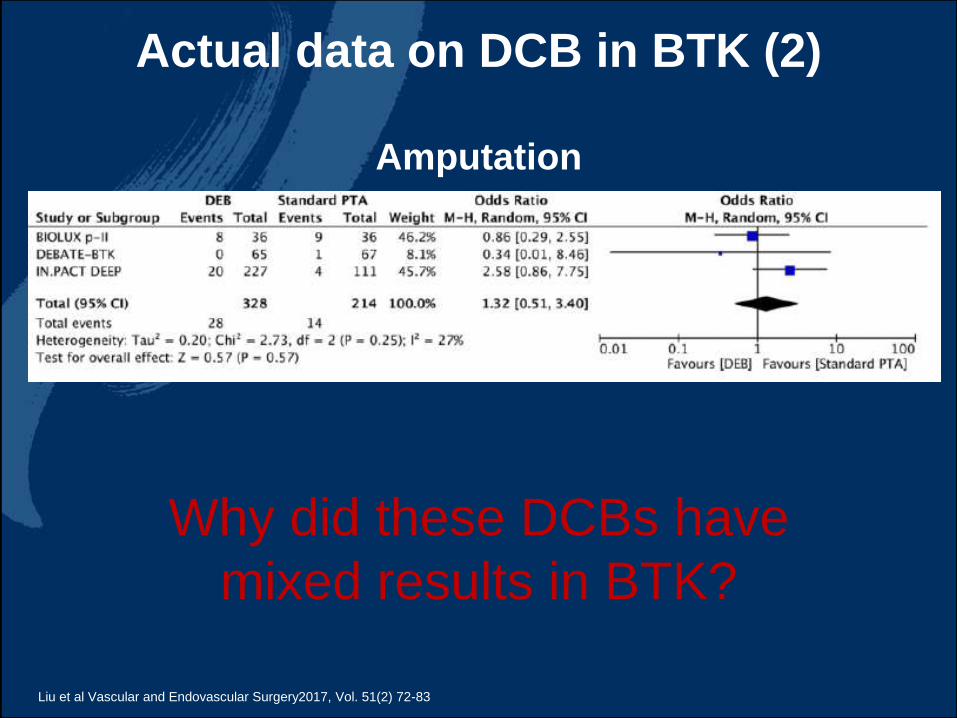
Actual data on DCB in BTK (2)
Liu et al Vascular and Endovascular Surgery2017, Vol. 51(2) 72-83
Why did these DCBs have
mixed results in BTK?
Amputation

• Antiproliferative agent (Paclitaxel)
• Initial dose/dose density
• Tissue transfer efficiency– Coating characteristics (e.g.,
hydrophobicity/hydrophilicity, crystallinity/amorphous morphology)1-4
– Excipient5
– Coating technique6
Determinants of DCB Biological Effect
1. Seidlitz et al. PLOS One 2013; DOI: 10.1371/journal.pone.0083992. 2. Afari & Granada. Endovascular Today August 2012; 53-58.
3. Granada et al. Open Heart 2014;1:e000117. 4. Creel et al. Circ Res; 2000;86:879-884. 5. Radke et al. EuroIntervention 2011;7:
730–737. 6. Buszman et al. JACC Cardiovasc Interv 2013;6(8):883-90.
Xiong GM, et al. J Control Release. 2016;239:92-106.

• Loss to circulation(Insertion-Transit-Inflation)1
and risk of:– Particulate embolization
– Systemic effects
• Paclitaxel tissue residency– Presence in tissue during
restenotic cascade2 (duration of retention)
– Homogeneity of distribution
Determinants of DCB Biological Effect
1-10% to tissue
~70-80% distal circulation
1. Seidlitz et al. PLOS One 2013; DOI: 10.1371/journal.pone.0083992. 2. Forrester et al. J Am Coll Cardiol 1991;17:758-769.
Granada JF, TCT 2014.
Granada JF, TCT 2013.
DCB

HOW to improve DCB
1° generation DCB: UREA + 3µg/mm² crystalline coating structure
2° generation DCB:
polymer acetyl tributyl citrate + 2µg/mm²
non-polymer polysorbate /sorbitol + 2µg/mm²
Reduced crystalline
coating structure
Granada et al. JACC Cardiovasc Interv. 2015 Jul;8(8):1115-1123

• Primary patency at 6-M FU 57,1%
• LLL 0,99±0,6 at 6 months angiographic results
• Freedom from TLR 93,3%
RANGER BTK Outcomes in “all-comer” setting
RANGER BTK
57.1%
31.2% 27%
73%
59%46.9%
0%
20%
40%
60%
80%
Ranger BTK Schmidt et al. Iida et al DEBATE BTK IN.PACT DEEP BIOLUX III
Primary patency (%)
Angiographic results at 3 months
Uncoated Balloons DCB
Angiographic results at 12 months
This investigator-sponsored study is supported by grant funding from Boston Scientific.
Boston Scientific is not responsible for the collection, analysis or reporting of these studies which remain the sole responsibility of the investigators.

The importance of calcium
Calcium represents a barrier to optimal drug absorption.
Circumferential distribution seems to be the most influencing
factor with the worst effect noticed in 360 calcium presence
Sixty patients with de
novo lesions of the
superficial femoral
artery underwent
endovascular treatment
with drug eluting
balloons (DEB).
Fanelli et al Cardiovasc Intervent Radiol (2014) 37:898–907

Roy T, et al. J Endovasc Ther. 2016 Sep 22. pii: 1526602816671135.
Heterogenous Plaque Morphology• CTO plaques may include fat, thrombus, soft tissue, hardened
tissue, and calcium
Popliteal Artery Calcified CTO
MR
IH
isto
logy
Calcium
Thrombus
Fat
Soft tissue(vessel wall reference)
Popliteal Artery “Hard” CTO
Micro-CT
Dense collagen

Plaque modification to facilitate drug uptake.
Atherectomy Lithotripsy
JETSTREAM SC Catheters
Ultrasound
Proof of concept / mechanistic effect established.
Further investigation and RCTs required

DES Efficacy outcomes in BTK
TLR
Restenosis
Amputation
Zhang J et al. Vasc Endovascular Surg. 2017 Feb;51(2):72-83

Long term outcome of TAXUS Liberte in BTK
(Paclitaxel Eluting Stent) vs PTA +/- BMS
Estimated 5-year cumulative incidence rates of major amputation per limb.
PADI, J Am Heart Assoc 2017
Estimated 5-year cumulative incidence rates of amputation free survival per patient.
PADI, J Am Heart Assoc 2017
Van Overhagen et al. JAHA 2017 Vol 6 No 4
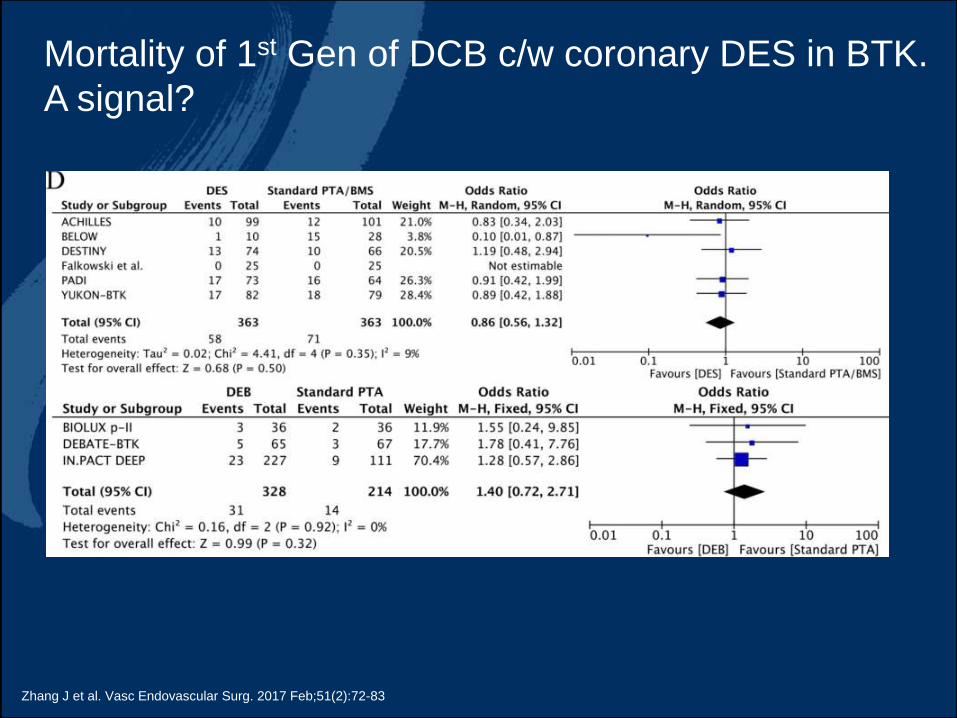
Mortality of 1st Gen of DCB c/w coronary DES in BTK.
A signal?
Zhang J et al. Vasc Endovascular Surg. 2017 Feb;51(2):72-83

Actual data on DES in BTK
In focal disease of infrapopliteal arteries, DES therapy reduces the risk of
reintervention and amputation compared with plain balloon angioplasty or BMS
implantation without any impact on mortality and Rutherford class at 1-y FU
BUT in CLI lesions are frequently long!!!!!Fusaro et al. JACC Cardiovasc Interv. 2013 Dec;6(12):1284-93.
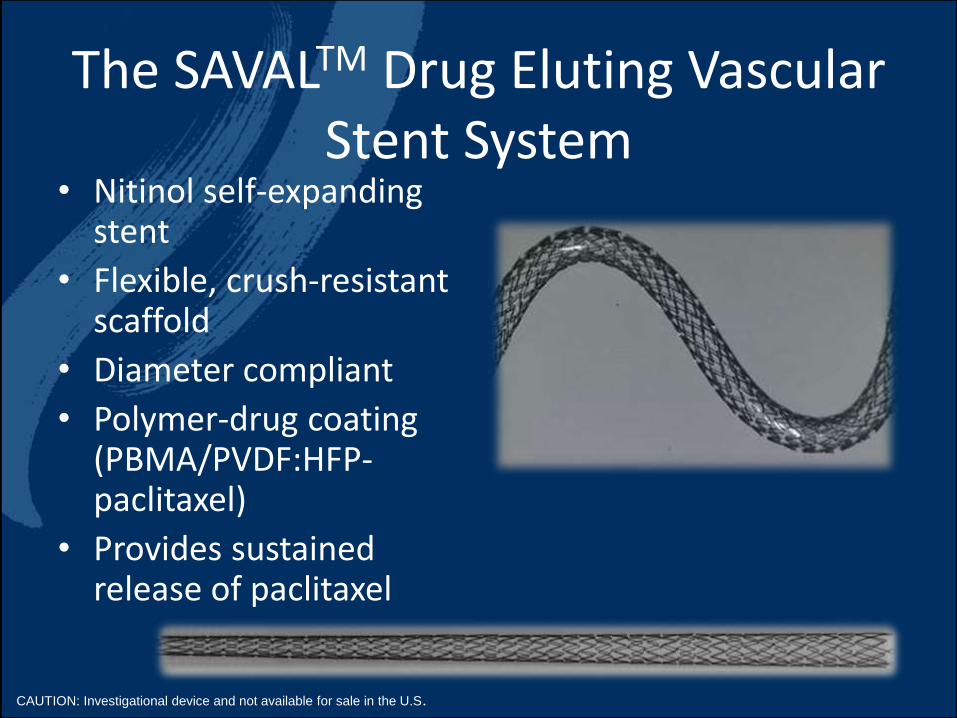
The SAVALTM Drug Eluting Vascular Stent System
• Nitinol self-expanding stent
• Flexible, crush-resistant scaffold
• Diameter compliant
• Polymer-drug coating (PBMA/PVDF:HFP-paclitaxel)
• Provides sustained release of paclitaxel
CAUTION: Investigational device and not available for sale in the U.S.

• Dual Layer System (same as Eluvia)
• Primer Layer (PBMA): Promotes Adhesion of Active Layer to Stent
• Active Layer (PTx, PVDF-HFP)–Controls Release of Paclitaxel
• Tuned low dose: 0.236 µg PTx/mm2
stent surface area
SAVALTM Coating Design
SAVAL is an investigational device and not available for sale in the US. Boston Scientific Data on File.
Stent
PBMA Primer Layer
Paclitaxel/PVDF-HFP Active Layer

Title A Randomized Trial comparing the Drug-Eluting Stent (DES) Below the Knee (BTK) Vascular Stent System vs Percutaneous Transluminal Angioplasty (PTA) Treating Infrapopliteal Lesions in Subjects With Critical Limb Ischemia
Principal Investigators
Global: Jihad Mustapha, MD, FACC FSCA
US: Patrick J. Geraghty, MD, FACS, RPVIEU: Hans van Overhagen, MD, PhD, EBIRJapan: Masato Nakamura, MD, PhD
Objectives Demonstrate a superior patency rate and acceptable safety in below-the-knee arteries with lesions treated with the SAVAL Stent vs PTA.Secondary: To collect additional information on limb salvage and overall quality of life in this patient population.
Study Design Phase A- RCT Phase B- single arm
Global, prospective, multicenter, 2:1 randomized (SAVAL vs PTA)
Stent size 3.5 mm x 80 mm
Sequential, single-arm study to collect ongoing safety and effectiveness dataStent sizes: Diameters 3-4 mm; Lengths 40, 80, 120 mm
Patients ~201 subjects (2:1 randomization) ~100 subjects
• up to 50 study centers in the US, Europe, and Japan
Follow-UpOffice visits at 1, 3, 6, 12, 24, and 36 months post procedureTelephone follow-up at 18 and 30 months post procedure
SAVAL Clinical Study
Enrolling
SAVAL is an investigational device and not available for sale in the US. Boston Scientific Data on File.

A Randomized Trial comparing the Drug-Eluting Stent (DES) Below- the-Knee
(BTK) Vascular Stent System vs Percutaneous Transluminal Angioplasty (PTA)
treating Infrapopliteal Lesions in Subjects with Critical Limb Ischemia
The trial is to be conducted in the United States, Europe, and Japan at up to 50
investigational centers, with up to 35 centers located in the US

Conclusions• 1st Gen DCBs show mixed results in BTK treatment
suggesting an “in class” variation.
• The “all-comer” setting for first evaluation of Ranger BTK
make results more generalizable.
• Plaque modification may help with localized drug uptake in
morphologically challenging anatomy.
• Current (and historic) polymer release ’olimus and PTX
BTK DES are safe and effective but limited in size matrix.
• We await the reporting of SAVAL trial.
Gauging performance in below-the-knee intervention
Dr. Costantino Del GiudiceVascular and oncological interventional radiology
Paris Descartes University
January 23, 2019







