
J. Hogan has documented that he has no relevant financial relationships to disclose or conflict of interest to resolve.

Why do girls with end-stage renal
disease wait longer for
transplantation than boys?Dr Julien Hogan
Pediatric Nephrology, Robert Debré Hospital, APHP, Paris, France
REIN Registry, France
On behalf of the ESPN/ERA-EDTA Registry

Introduction
– Study of inequality in access to renal transplantation:
• 852 references on Pubmed
– In Europe such inequalities have been found:
• Between countries1
• Between centers2,3
• Between patients : age, racial disparities4,5, socio-economic
status, educational level6
…… AND GENDER7,8,9
[1] Harambat et al. AJT 2013; [2] Oniscu et al. BMJ 2003; [3] Hogan et al. NDT 2014
[4] Furth et al. Pediatrics 2000; [5]Soucie et al. AJKD 1992; [6] Schaeffner et al. AJKD 2008
[7] Couchoud et al. Transplantation 2012; [8] Ravanan et al. BMJ 2010;
[9] Segev et al. JASN 2009
Introduction
• In both Europe and USA female gender has been
associated with:
– Lower access to transplantation
– Lower rate of registration on the waiting-list
– Longer time from start of dialysis to wait listing
• Factors contributing to these differences:
– Longer transplantation work-up1
– Lower willingness to undergo transplantation2
– Higher DSA level
[1] Alexander et al. JAMA 1998; [2] McCauley et al. AJKD 1997
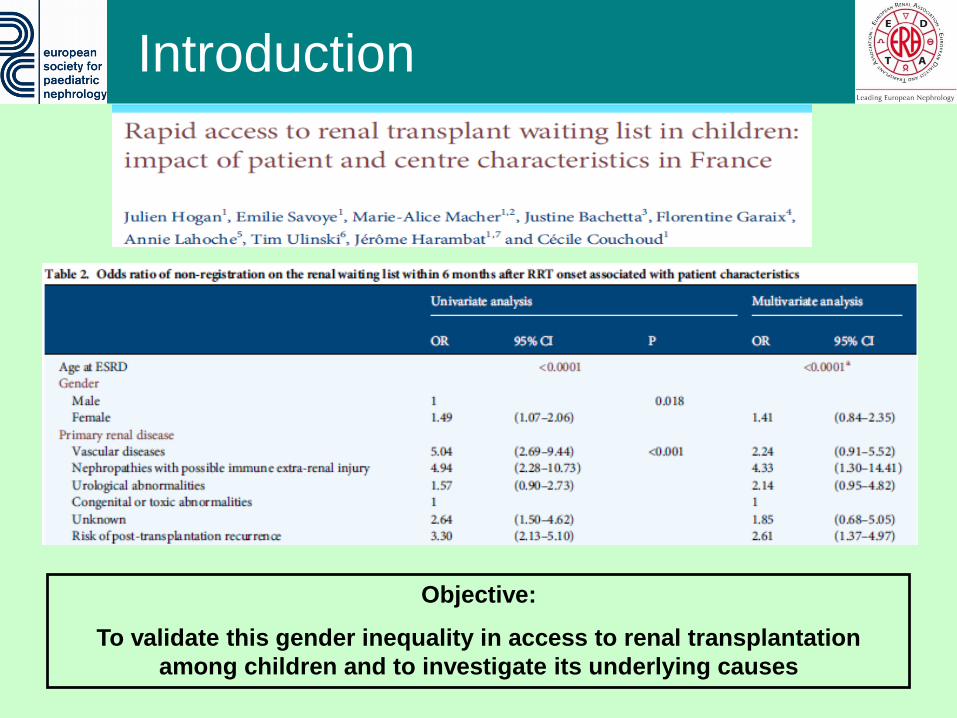
Introduction
Objective:
To validate this gender inequality in access to renal transplantation
among children and to investigate its underlying causes

Methods
• Population
6454 patients <18, starting RRT between 01/01/2000 and 31/12/2012,
from 35 countries, recorded in the ESPN/ERA-EDTA registry
• Statistical analysis
•Time from RRT start to transplantation
Survival analysis: KM, Proportional Hazard
Frailty model
•Probability of pre-emptive transplantation
Hierarchical logistic regression
•Study of the time of follow-up prior RRT
T-test and Linear regression

Results

Time to Access to Renal
Transplantation
Time to Access to Renal
Transplantation
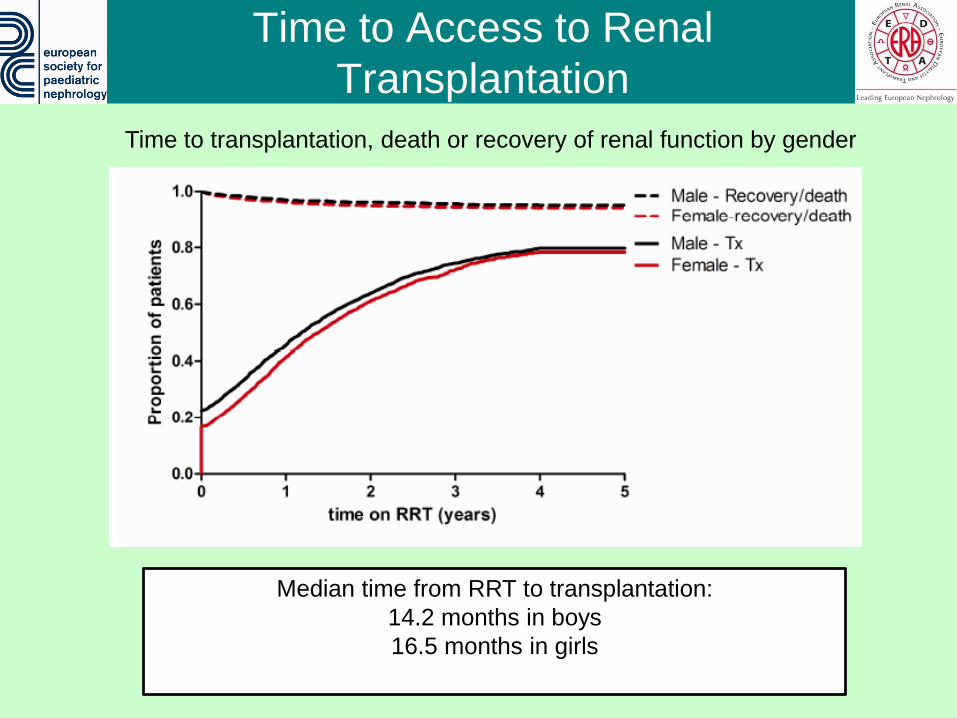
Time to transplantation, death or recovery of renal function by gender
Median time from RRT to transplantation:
14.2 months in boys
16.5 months in girls

Time to Access to Renal
Transplantation
Access to transplantation by gender adjusted for age after excluding
preemptive transplantations
HR girls vs boys: 0.99, 95%CI: 0.92-1.06
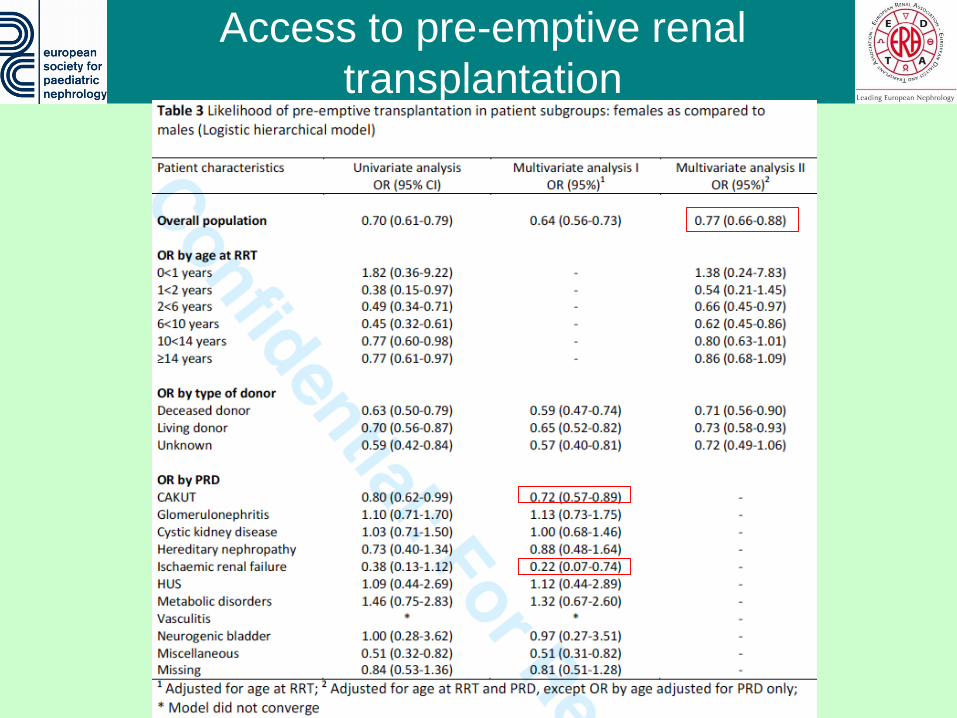
Access to pre-emptive renal
transplantation

Follow-up time before RRT
Median follow-up time:
23.0 months [2.4-68.6] in boys
14.4 months [0.6-53.6] in girls
Longer follow-up time is associated
with a higher chance of receiving
preemptive transplantation
OR 1.19 [1.15-1.24] per year
Possible explanations:
1. Girls are diagnosed later
1. Girls progress faster towards
ESRD
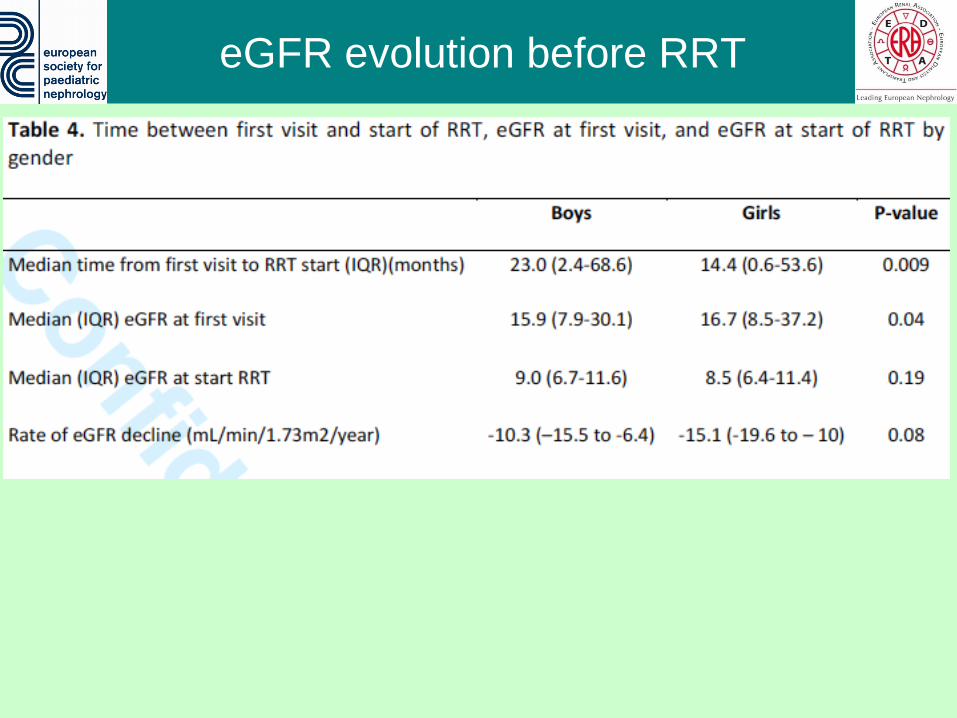
eGFR evolution before RRT
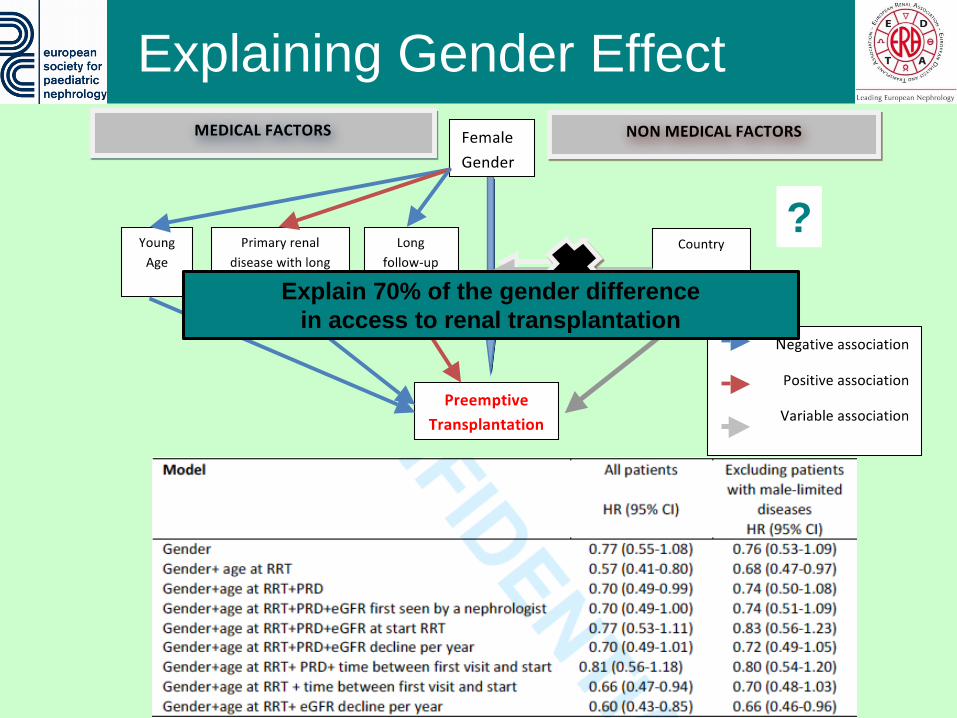
Explaining Gender Effect
Explain 70% of the gender difference
in access to renal transplantation
?
Conclusion (1)
• Gender difference in access to renal transplantation
is explained by a 23% decreased likelihood of
preemptive transplantation in girls.
• This difference is only partially explained by medical
factors such as age and primary renal disease
• A much shorter follow-up time prior RRT in girls
explains part of the gender difference in access to
renal transplantation
• A trend towards more rapid decline of eGFR in girls
Conclusion (2)
• Medical factors only partially explain gender
difference in access to transplantation
• Non-medical factors need to be considered:
– Patient willingness for early transplantation1
– Parents willingness to donate their kidney
– Health care professionals attitude towards pre-
emptive transplantation and living donor
transplantation2
– Fear of non-adherence to IS treatement3
…..
[1] McCauley et al. AJKD 1997; [2] Thamer et al. Transplantation 2001; [3] Chisholm et al. cJASN 2013
#
Transplant
Our Girls

Acknowledgments
• Cécile Couchoud
• Karlijn van Stralen
• Marjolein Bonthuis
• Jaap Groothoff
• Kitty Jager
• Franz Schafer

Acknowledgements
Albania D Shtiza Lithuania A Jankauskiene, B Pundziene
Austria R Kramar, R Oberbauer Malta V Saied-Conti
Belarus S Baiko, A Sukalo Moldova S Gatcan, O Berbeca, N Zaikova
Belgium K van Hoeck, F Collart, JM des Grottes Montenegro S Pavićević
Bosnia Herzegovina D Pokrajac Norway T Leivestad, A Bjerre
Bulgaria D Roussinov Poland A Zurowska, I Zagozdzon
Croatia D Batinić, M Lemac, J Slavicek Portugal C Mota, M Almeida, C Afonso
Czech Republic T Seeman, K Vondrak Romania G Mircescu, L Garneata
Denmark J Heaf Russia EA Molchanova, NA Tomilina, BT Bikbov
Estonia U Toots Serbia M Kostic, A Peco-Antic, B Spasojevic-Dimitrijeva,
G Milosevski-Lomic, D Paripovic, S Puric, D Kruscic
Finland P Finne, C Grönhagen-Riska Slovakia L Podracka, G Kolvek
France C Couchoud, M Lasalle, J Harambat Slovenia N Battelino, G Novljan, J Buturovic-Ponikvar
FYR of Macedonia E Sahpazova, N Abazi, N Ristoka Bojkovska Spain A Alonso Melgar and the Spanish Pediatric Registry
Germany F Schaefer, G von Gernsdorff, C Scholz,
B Tönshoff, K Krupka, B Höcker, L Pape
Sweden S Schön, KG Prütz, L Backmän, M Stendahl,
M Evans, B Rippe
Greece N Afentakis, A Kapogiannis, N Printza, C Stefanidis Switzerland G Laube, CE Kuehni, H Chehade, C Rudin
Hungary G Reusz Cs Berecki, A Szabó, T Szabó,
Zs Györke, E Kis
The Netherlands A Hoitsma, A Hemke, JW Groothoff, and all centres
participating in the RICH-Q study
Iceland R Palsson, V Edvardsson Turkey R Topaloglu, A Duzova
Italy B Gianglio, S Maringhini, C Pecoraro, S Testa,
E Vidal, E Verrina
Ukraine D Ivanov
Latvia V Strazdins, I Andersone United Kingdom R Pruthi, F Braddon, S Mannins, A Cassula, MD Sinha







