Download - Invasive Candida Infections in the ICU B. Guery Lille Infectious Diseases Summit: Fungal Series

Invasive Candida Infections in the ICU
B. GueryLille
Infectious Diseases Summit: Fungal Series

Invasive Candida infections in the ICU
Epidemiology and pathophysiology Diagnosis The molecules Key studies Available guidelines
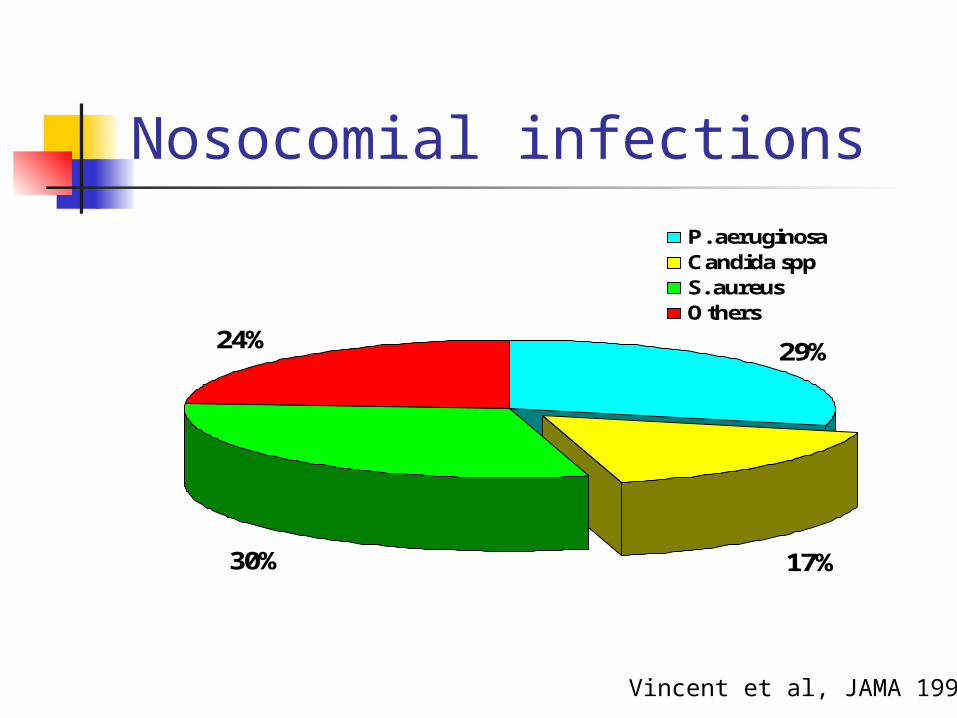
Nosocomial infections
29%
17%30%
24%
P. aeruginosaCandida sppS. aureusOthers
Vincent et al, JAMA 1995
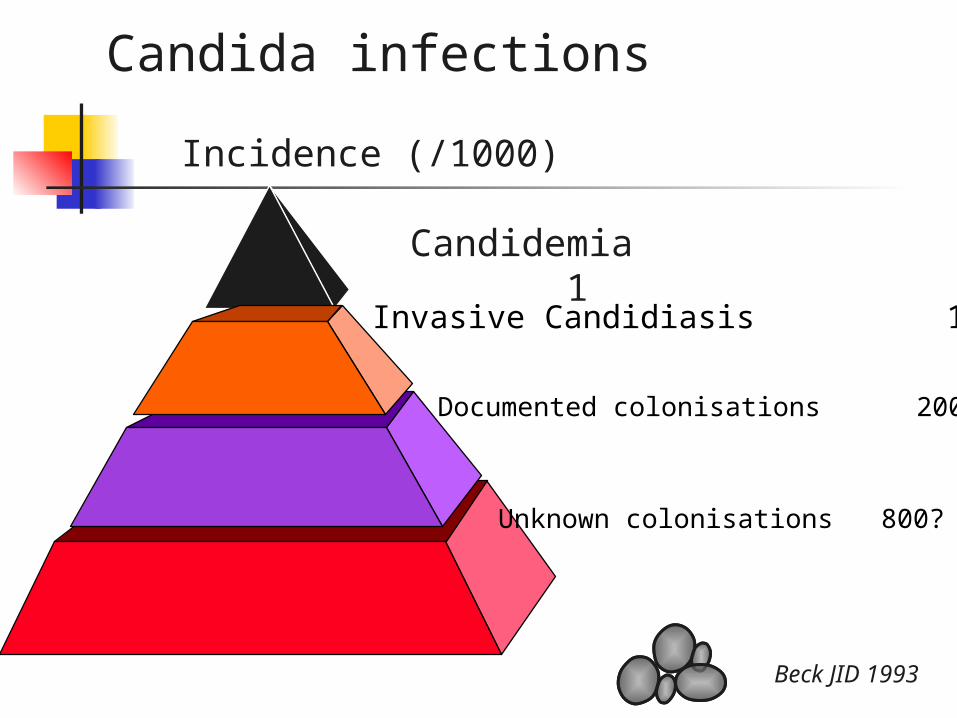
Incidence (/1000)
Beck JID 1993
Candida infections
Invasive Candidiasis 10
Documented colonisations 200 ?
Unknown colonisations 800?
Candidemia 1
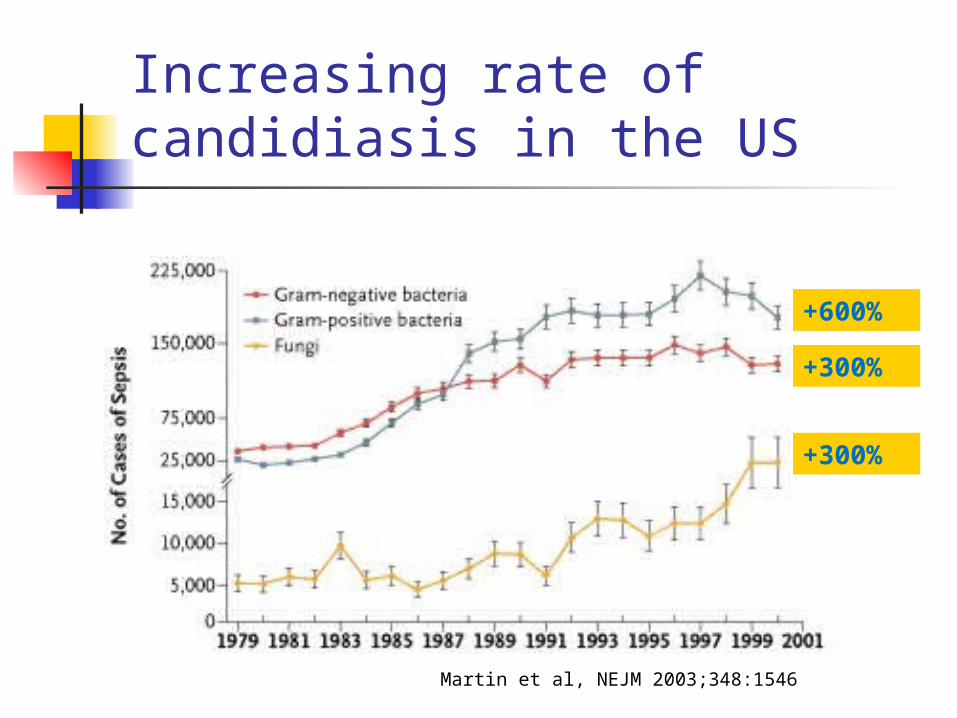
Increasing rate of candidiasis in the US
Martin et al, NEJM 2003;348:1546
+300%
+300%
+600%

Viridans streptococci
E. coli
S. aureus
Coag neg staph
P. aeruginosa
Enterobacter spp
Candida spp
Klebsiella spp
Enterocci
Serratia spp
0 5 10 15 20 25
22,5 days
Edmond et al, Clin Inf Dis 1999

Epidemiology of candidemia
Tortorano Trick Diekema Richet Pfaller Marchetti
(n=569) (n=2759) (n=254) (n=377) (n=1134) (n=1137)
J Hosp Infect CID J Clin Microbiol CMI J Clin Microbiol CID
2002 2002 2002 2002 2002 2004
C.albicans 58,50% 59% 58% 53% 55% 66%
C.glabrata 12,80% 12% 20% 11% 15% 15%
C.parapsilosis 14,60% 11% 7% 16% 15% 1%
C.tropicalis 6,10% 10% 11% 9% 9% 9%
C.krusei 0,90% 1,20% 2% 4% 1% 2%
Miscellaneous 7,10% 7% 2% 6% 1% 7%
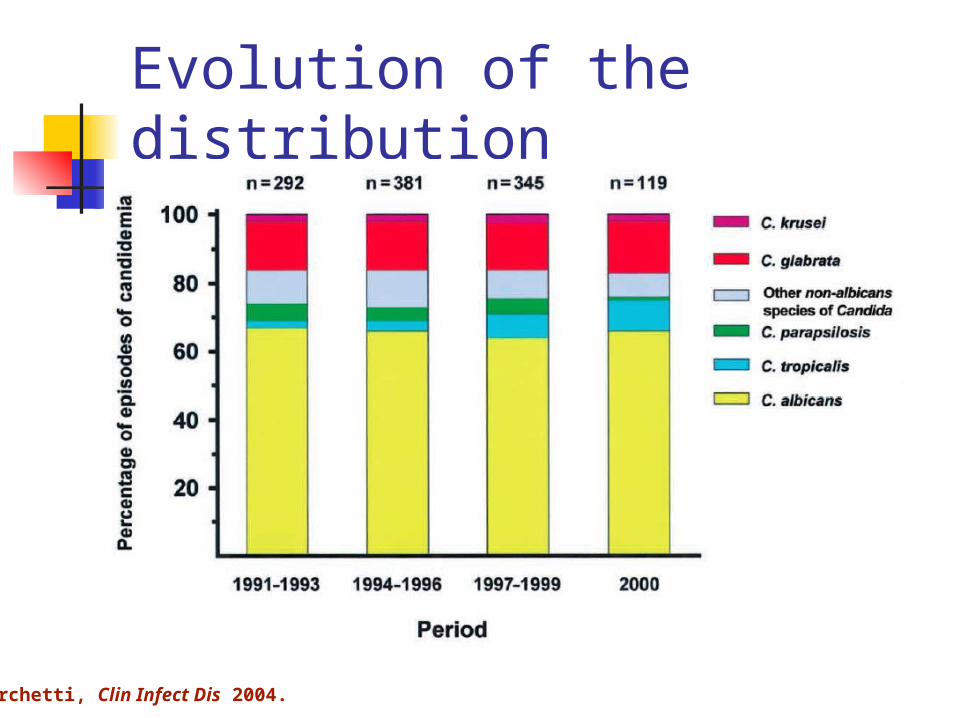
Evolution of the distribution
Marchetti, Clin Infect Dis 2004.

300 patients with proven invasive candida infection
Main risks factors of invasive candidiasis
Colonisation Abdominal (Solomkin, Surgery 1980) Independant risk factor(Wey, Pittet, Karabinis,…) 5-15% patients colonized on admission, 50-86% if
prolonged LOS, 5-30% develop a candidemia Antibiotics
Major risk factor (Wey, Arch Intern Med 1989) Wide spectrum, increase with time (Pittet, Ann Surg 1994)
Neutropenia Venous access:
Candidemia directly related to the IVL in 35-80% of the cases (Luzzati, Eur J Clin Microb Inf Dis 2002)
ICU, surgery, ARF, steroids, anti-H2, high Apache score…


Physiopathology
12 may
16 may
21 may
25 may
Blood culture
27 mayendogenous >> exogenous
Pittet Am J Med 1991 / Ann Surg 1994 / Nucci & Anaissie CID 2001

Invasive Candida infections in the ICU
Epidemiology and pathophysiology Diagnosis The molecules Key studies Available guidelines

Colonisation/Infection
1,0
0,8
0,6
0,4
0,2
0,00 20 40 60 140
Length of colonisation (d)
Colonisation IndexInfectedColonized • Prospective cohort study in the ICU
• 5,3 distincts sites /patient
• Colonisation Index : Prospectively definedMeasured 3 times/we
nb distincts colonized sites nb distincts sampled sites
(Pittet et al, Ann Surg 94 ; 220 : 751-8)

(Pittet et al, Ann Surg 94 ; 220 : 751-8)(Pittet et al, Ann Surg 94 ; 220 : 751-8)
Se Se SpSp PPV PPV NPVNPV
>2 colonized sites >2 colonized sites 100100 2222 44 44 100 100
≥≥3 colonized sites 3 colonized sites 4545 7272 50 50 68 68
Index >0,5Index >0,5 100100 6969 66 66 100 100
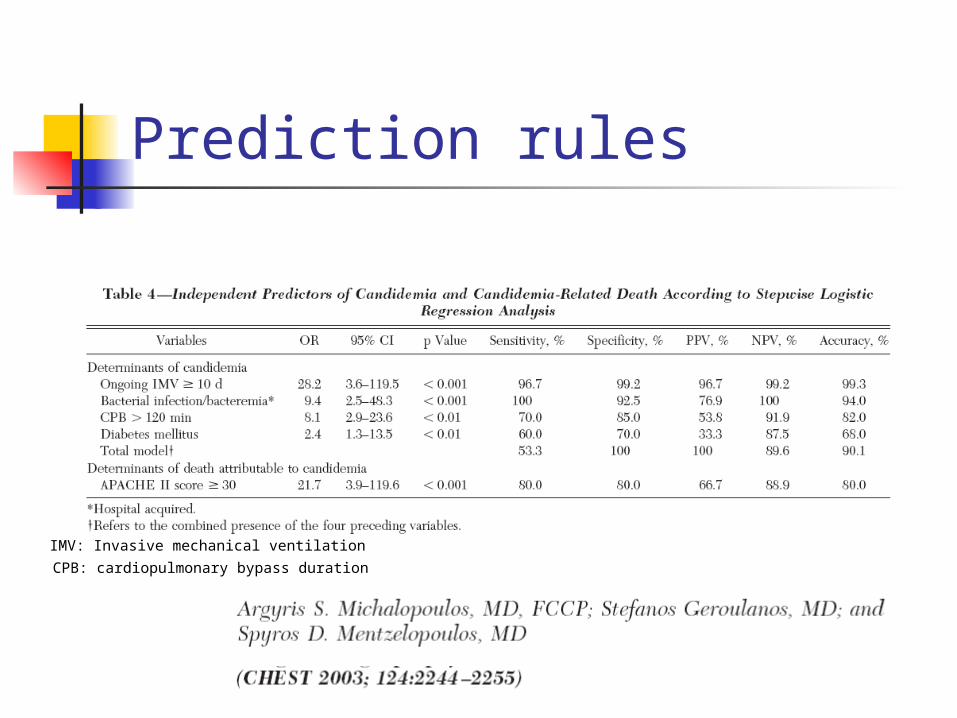
Prediction rules
IMV: Invasive mechanical ventilation
CPB: cardiopulmonary bypass duration

Prediction rules
Se: 81%Sp: 74%

Prediction rules
The CS - total parenteral nutrition 1- surgery 1, - multifocal Candida colonization 1 - severe sepsis 2

Prediction rules
In this cohort of colonized patients staying >7 days, with a CS <3 and not receiving antifungal treatment, the rate of IC was <5%. Therefore, IC is highly improbable if a Candida-colonized non-neutropenic critically ill patient has a CS <3.

Diagnosis
Positive blood culture or isolation from a normaly sterile site (except urine)
Surrogate markers 1,3 D glucan Mannans Germ tube antibody Hyphal wall protein 1 PCR

Invasive Candida infections in the ICU
Epidemiology and pathophysiology Diagnosis The molecules Key studies Available guidelines

Mecanisms of action
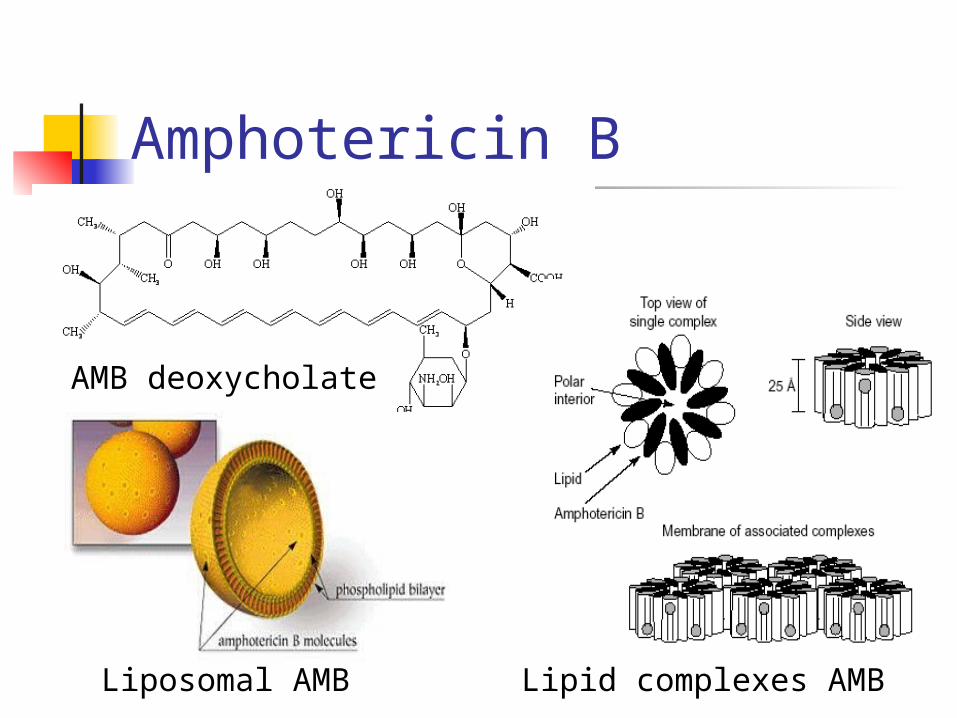
Amphotericin B
Lipid complexes AMBLiposomal AMB
AMB deoxycholate

Fluconazole Good oral absorption CNS diffusion Half life 25-30 h Side effects
Nausea, vomiting Rash Liver toxicity (lower compared to other
azoles)

Voriconazole
Oral and IV Large distribution volume Half life 6h (200mg) CSF concentration ≈ 50% serum
Side effects: Photopsia, abdominal pain, rash, nausea, diarrhea, Liver toxicity
Johnson et al, Clin Infect Dis 2003

Echinocandins
Only intravenously Fungicidal 3 molecules
Caspofugin Anidulafungin Micafungin
Different metabolisms

AnidulafunginCaspofungin MicafunginGlarea lozoyensis Aspergillus nidulansColeophoma empetri
Adapted from Micafungin US Prescribing Information; Anidulafungin US Prescribing Information; Debono M, Gordee RS. Annu Rev Microbiol. 1994;48:471–497; Debono M et al. J Med Chem. 1995;38:3271–3281.
Echinocandins
N O
O
O
NH
O
H
HH H
OH
CH3
O
O
H2N
OH
NHHO
H2N
HO NHHN
OH
OH
HN OH
NH
HO
H3CCH3 CH3
O
O
ON
O
O
HN
NO
O
O
O
ON
O
H3C
SOO
HO
OHHO
HO
OH
HN
NH
NHH3CH2N
HOHO
OH
NH
OH
OH
CH3O
ON
H3C
O
NO
O
O
O
O
HO
HO
HO
OH
HN
NH
OH
HOHO OH
NH
HN
CH3
OH
NH
H3C
H3C
• Side chains are key determinants of lipophilicity, solubility, antifungal activity, and toxicity

Pharmacology: Metabolism, Elimination, Bioavailability, and Protein Binding
Caspofungin Micafungin Anidulafungin
Metabolism Hepatic metabolism by hydrolysis and
N-acetylation
Spontaneous nonhepatic chemical degeneration
Hepatic metabolism by arylsulfatase and
catechol-O-methyltransferase
Nonhepatic chemical degradation
Elimination/excretion Urine 41%Feces 34%
Urine + feces 82.5%Feces 71%
Urine <1%Feces ≈30%
Protein Binding 97% >99% >99%
Oral Bioavailability <5% <5% <5%
Dialyzable No No No
Adapted from Micafungin US Prescribing Information; Anidulafungin US Prescribing Information; Dodds Ashley ES et al. Clin Infect Dis. 2006;43:S28–S39.

Pfaller et al, JCM 2008
No evidence of emerging resistance

Invasive Candida infections in the ICU
Epidemiology and pathophysiology Diagnosis The molecules Key studies Available guidelines
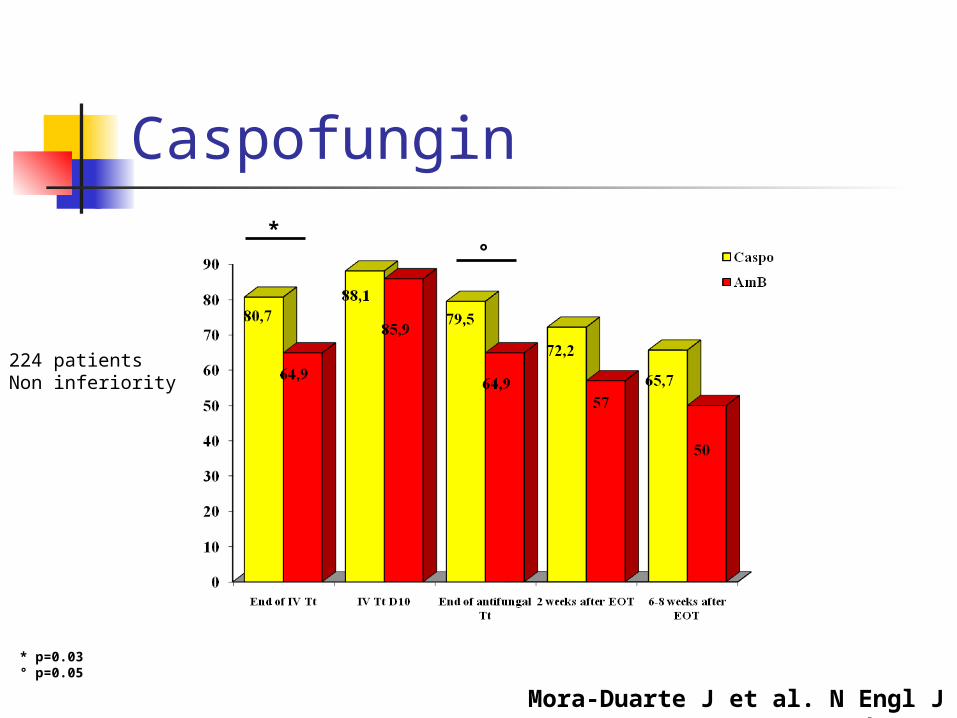
Caspofungin
Mora-Duarte J et al. N Engl J Med 2002
*°
* p=0.03° p=0.05
224 patientsNon inferiority

Primary analysis (ITTm*)Success at 12 weeks
Kullberg BJ et al, Lancet 2005
Su
cess
rate

Voriconazole
VoriconazolVoriconazolee
(n = 248)(n = 248)
AmB fluconazol
e(n = 122)
p
End of treatment
70 % (173)70 % (173) 74 % (90)0,42 ;
NS
2 weeks after EOT
52 % (130)52 % (130) 53 % (64)0,99 ;
NS
6 weeks after EOT
44 % (110)44 % (110) 46 % (56)0,78 ;
NS
Kullberg BJ et al, Lancet 2005
Secondary Analysis (ITTm*)
on inferiority

Voriconazole
Amphotericin B/Fluconazole
Caspofungin
Note: Data on file. Pfizer. Adapted from Kullberg BJ, et al. N Engl J Med. In pressSources: Candidemia 1 (Rex, 1994); Candidemia 2 (Rex, 2003); Caspofungin (Mora-Duarte, 2002); Itraconazole (Tuil, 2003; ISICEM); Global Candidemia Study
Pro
bab
ilit
y o
f P
osi
tive
Cu
ltu
re
0 2520151054321 6 987 11 141312 16 191817 21 2423220.0
0.2
1.0
0.8
0.6
0.4
Time to First Negative Blood Culture

Investigator-Assessed Responses
Improved at EOT
Success at2 Weeks
Success at6 Weeks
Success at12 Weeks
72%
50%
42% 42%
72%
51%45%
42%
73%
51%
43%
Voriconazole
Amphotericin B Fluconazole
Cancidas
NA
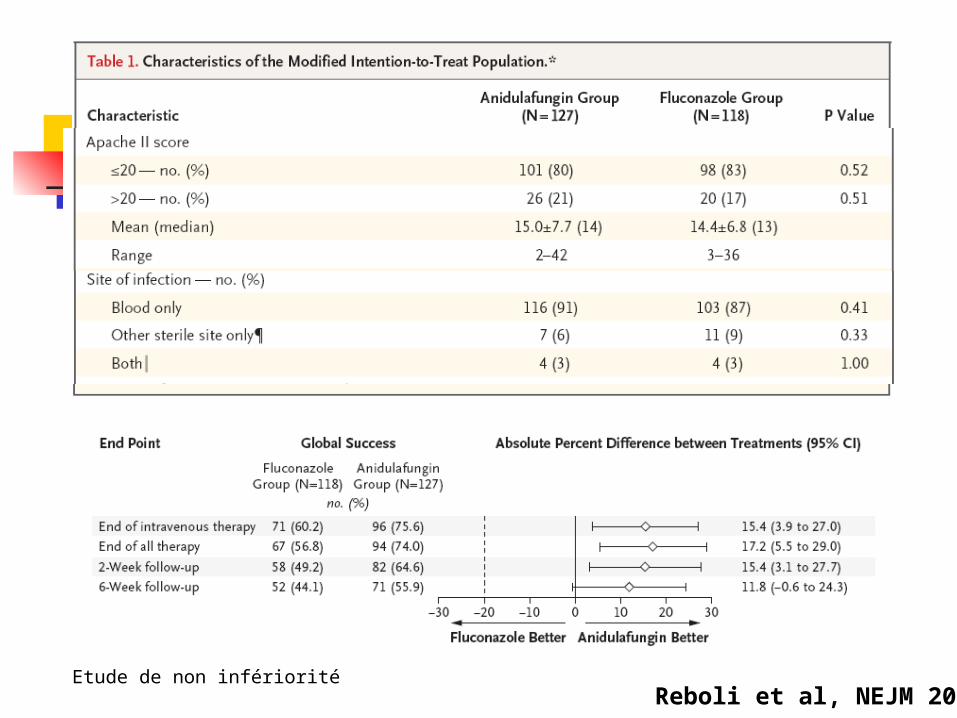
Reboli et al, NEJM 2007Etude de non infériorité


Invasive Candida infections in the ICU
Epidemiology and pathophysiology Diagnosis The molecules Key studies Available guidelines





Nonneutropenic patients Transition to
fluconazole Isolates likely to be
susceptible and stable Glabrata:
echinocandin preferred
Parapsilosis: fluconazole preferred
Catheter removal Duration: 2 wk post
clearance
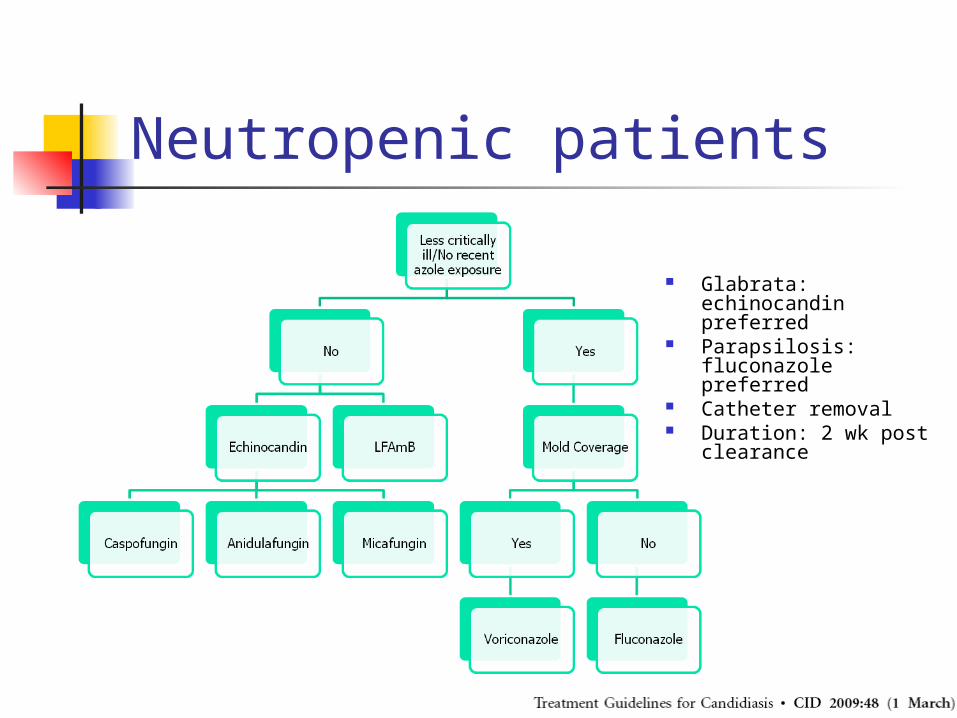
Neutropenic patients
Glabrata: echinocandin preferred
Parapsilosis: fluconazole preferred
Catheter removal Duration: 2 wk post
clearance

Conclusion
Epidemiology and pathophysiology Increased rate of non albicans
Diagnosis Remains difficult
The molecules Echinocandins have a proeminent place
Available guidelines Association?




![UNDERSTANDING CANDIDA - Amazon S3 · Understanding Candida Yeast and Fungal Infection by Donna Gates [transcript] Page | 3 And it is contagious: Men and women can pass it back and](https://cdn.vdocuments.site/doc/165x107/5f058f457e708231d4139072/understanding-candida-amazon-s3-understanding-candida-yeast-and-fungal-infection.jpg)


