
Prof. MUDr. Jan F Vojáček DrSc, FESC, FACC
Iniciace protidestičkové
léčby u pacienta s STE
infarktem myokardu?
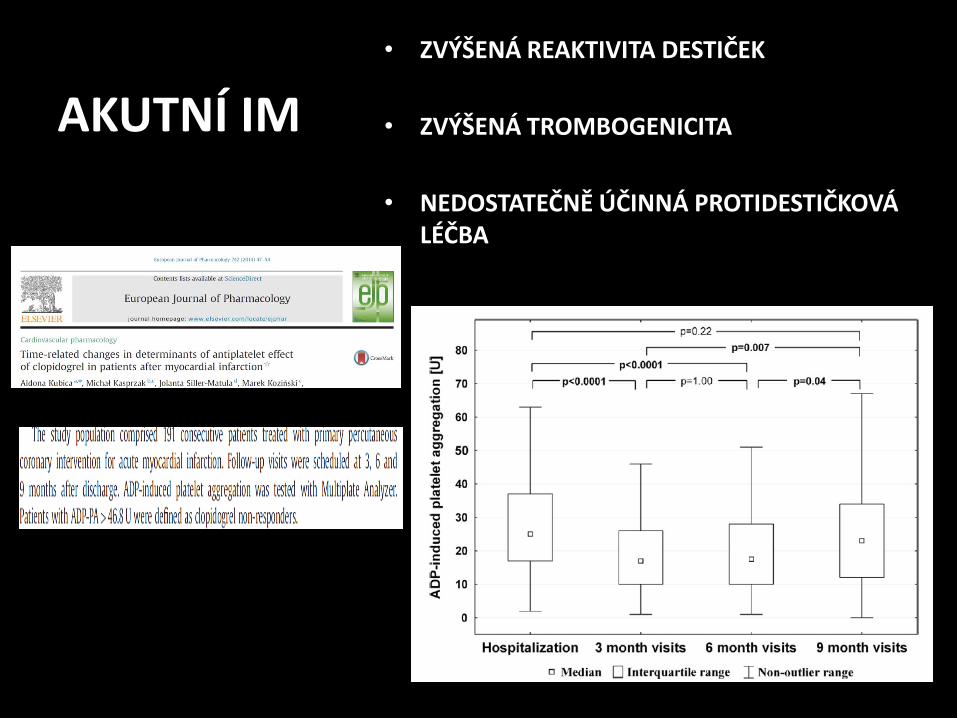
AKUTNÍ IM
• ZVÝŠENÁ REAKTIVITA DESTIČEK
• ZVÝŠENÁ TROMBOGENICITA
• NEDOSTATEČNĚ ÚČINNÁ PROTIDESTIČKOVÁ LÉČBA

AKUTNÍ IM
• ZVÝŠENÁ REAKTIVITA DESTIČEK
• ZVÝŠENÁ TROMBOGENICITA
• NEDOSTATEČNĚ ÚČINNÁ PROTIDESTIČKOVÁ LÉČBA

All patients treated with ticagrelor had PR below 208 PRU cut-off point, whereas more than half of patients (62.50%) receiving high-dose clopidogrel remained non-responsive to clopidogrel.

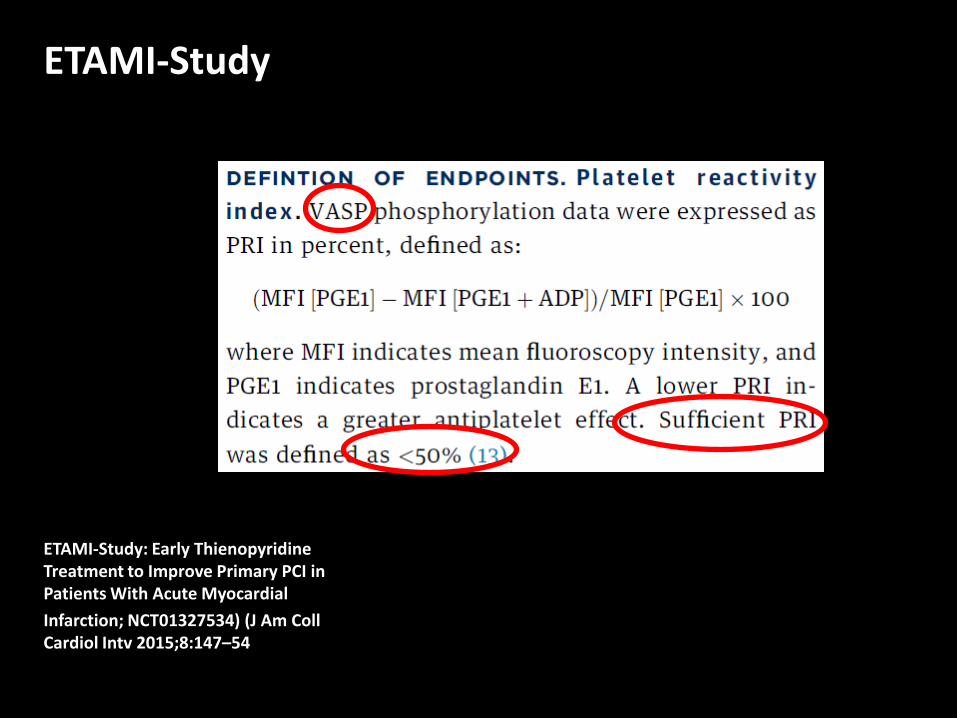
ETAMI-Study
ETAMI-Study: Early Thienopyridine Treatment to Improve Primary PCI in Patients With Acute Myocardial
Infarction; NCT01327534) (J Am Coll Cardiol Intv 2015;8:147–54

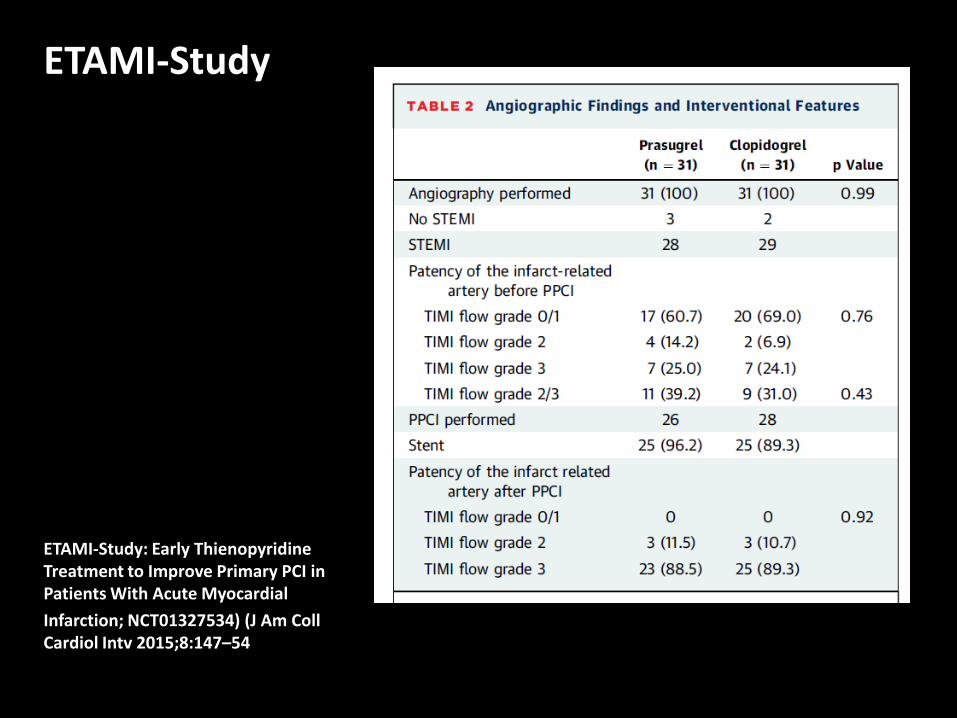
ETAMI-Study
ETAMI-Study: Early Thienopyridine Treatment to Improve Primary PCI in Patients With Acute Myocardial
Infarction; NCT01327534) (J Am Coll Cardiol Intv 2015;8:147–54
ETAMI-Study
ETAMI-Study: Early Thienopyridine Treatment to Improve Primary PCI in Patients With Acute Myocardial
Infarction; NCT01327534) (J Am Coll Cardiol Intv 2015;8:147–54

ETAMI-Study
ETAMI-Study: Early Thienopyridine Treatment to Improve Primary PCI in Patients With Acute Myocardial
Infarction; NCT01327534) (J Am Coll Cardiol Intv 2015;8:147–54
ETAMI-Study
ETAMI-Study: Early Thienopyridine Treatment to Improve Primary PCI in Patients With Acute Myocardial
Infarction; NCT01327534) (J Am Coll Cardiol Intv 2015;8:147–54

ETAMI-Study
ETAMI-Study: Early Thienopyridine Treatment to Improve Primary PCI in Patients With Acute Myocardial
Infarction; NCT01327534) (J Am Coll Cardiol Intv 2015;8:147–54

ETAMI-Study
ETAMI-Study: Early Thienopyridine Treatment to Improve Primary PCI in Patients With Acute Myocardial
Infarction; NCT01327534) (J Am Coll Cardiol Intv 2015;8:147–54

ETAMI-Study
ETAMI-Study: Early Thienopyridine Treatment to Improve Primary PCI in Patients With Acute Myocardial
Infarction; NCT01327534) (J Am Coll Cardiol Intv 2015;8:147–54

ETAMI-Study
CONCLUSIONS The pre-PCI administration of prasugrel in patients with STEMI undergoing PPCI was associated with a significant faster platelet inhibition compared with clopidogrel. Therefore, prasugrel should be preferred to clopidogrel in this setting.
ETAMI-Study: Early Thienopyridine Treatment to Improve Primary PCI in Patients With Acute Myocardial
Infarction; NCT01327534) (J Am Coll Cardiol Intv 2015;8:147–54



PLATELET FUNCTION IN PATIENTS WITH STEMI
full effect of prasugrel or ticagrelor on platelet function may take several hours in patients with STEMI
Alexopoulos D et al. Randomized assessment of ticagrelor versus prasugrel antiplatelet effects in patients with ST-segmentelevation myocardial infarction. CircCardiovasc Interv 2012;5:797-804. Parodi Get al. Comparison of prasugrel and ticagrelor loading doses in ST-segment elevation myocardial infarction patients: RAPID (Rapid Activity of Platelet Inhibitor Drugs) primary PCI study. J Am Coll Cardiol 2013;61:1601-6.

MOŽNOSTI ANTITROMBOTICKÉ LÉČBY
HEPARIN
HEPARIN + GP IIb/IIIa
BIVALURIDIN
ENOXAPARIN i.v.
ENOXAPARIN + GP IIb/IIIa
ASA nasycovací a udržovací
ASA + klopidogrel
ASA + prasugrel
ASA + ticagrelor
ANTITROMBOTIKA VE TŘÍDĚ I U STEMI
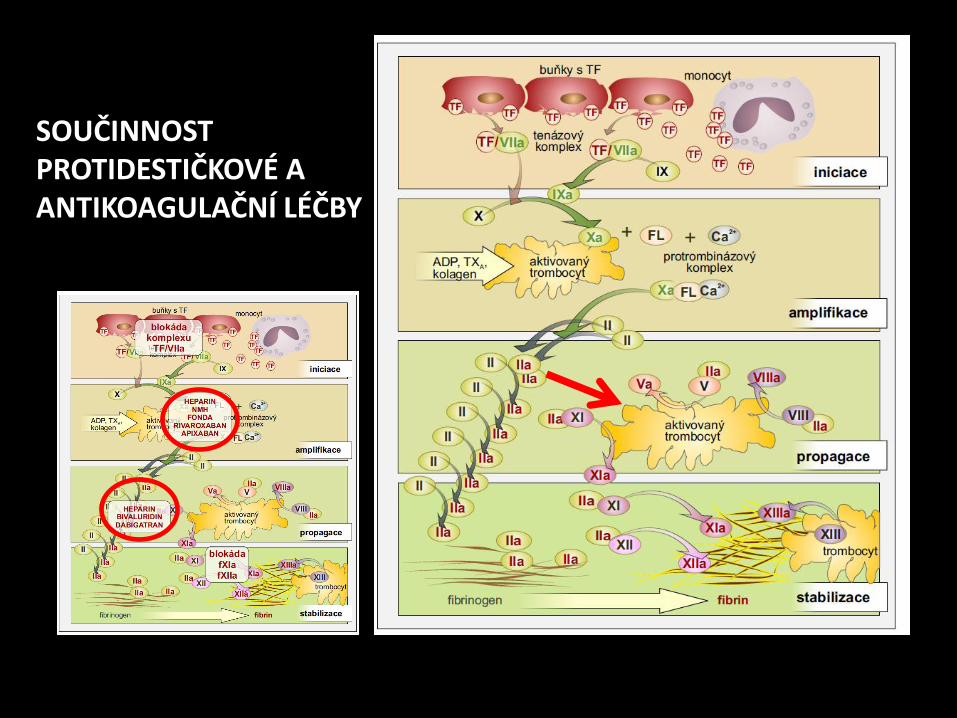
SOUČINNOST PROTIDESTIČKOVÉ A ANTIKOAGULAČNÍ LÉČBY

MOŽNOSTI ANTITROMBOTICKÉ LÉČBY
JAKÁ KOMBINACE ???
KDY ???

čas
trombogenicita
AIM

čas
trombogenicita
ANTITROMBOTIKA
AIM

čas
trombogenicita
riziko krvácení
ANTITROMBOTIKA
AIM

čas
trombogenicita
riziko krvácení
ANTITROMBOTIKA ANTITROMBOTIKA
AIM



ATLANTIC
1862 patients with ongoing STEMI of less than 6 hours’ duration, comparing prehospital (in the ambulance) versus in-hospital (in the catheterization laboratory) treatment with ticagrelor
median time from randomization to angiography was 48 minutes, and the median time difference between the two treatment strategies was 31 minutes

ATLANTIC

ATLANTIC

ATLANTIC
rates of major adverse cardiovascular events did not differ significantly between the two study groups
rates of major bleeding events were low and virtually identical in the two groups

ATLANTIC
absence of ST-segment elevation resolution of 70% or greater after PCI (a secondary end point) was reported for 42.5% and 47.5% of the patients, respectively
rates of definite stent thrombosis were lower in the prehospital group than in the in-hospital group (0% vs. 0.8% in the first 24 hours; 0.2% vs. 1.2% at 30 days)

ATLANTIC

ARIAM-Andalucía Registry
Almendro-Delia M Am J Cardiol 2015;115:1019e1026

ARIAM-Andalucía Registry
The results of our study confirm the benefit of pretreatment
with clopidogrel in reducing ischemic events and mortality during hospitalization, although only in the subgroup with STEMI. This benefit was associated with an increase
in minor bleeding but proving to be a net clinical benefit strategy Almendro-Delia M Am J Cardiol 2015;115:1019e1026

ARIAM-Andalucía Registry
The results of our study confirm the benefit of pretreatment
with clopidogrel in reducing ischemic events and mortality during hospitalization, although only in the subgroup with STEMI. This benefit was associated wih an increase
in minor bleeding but proving to be a net clinical benefit strategy Almendro-Delia M Am J Cardiol 2015;115:1019e1026
t

ARIAM-Andalucía Registry
The results of our study confirm the benefit of pretreatment
with clopidogrel in reducing ischemic events and mortality during hospitalization, although only in the subgroup with STEMI. This benefit was associated wih an increase
in minor bleeding but proving to be a net clinical benefit strategy Almendro-Delia M Am J Cardiol 2015;115:1019e1026
t




Bellemain-Appaix A et al. Association of Clopidogrel Pretreatment With Mortality, Cardiovascular Events, and Major Bleeding Among Patients Undergoing Percutaneous Coronary Intervention: A Systematic Review and Meta-analysis. JAMA 2012;308(23):2507–2516.
Zeymer U et al. Efficacy and safety of a high loading dose of clopidogrel administered prehospitally to improve primary percutaneous coronary intervention in acute myocardial infarction: the randomized CIPAMI trial. Clin Res Cardiol 2012;101(4):305–312.
Koul S. Effect of upstream clopidogrel treatment in patients with ST-segment elevation myocardial infarction undergoing primary percutaneous coronary intervention. Eur Heart J 2011;32(23): 2989–2997.
Dorler J. Clopidogrel pre-treatment is associated with reduced in-hospital mortality in primary percutaneous coronary intervention for acute ST-elevation myocardial infarction. Eur Heart J 2011;32(23):2954–2961.

HEALTH TECHNOLOGY ASSESSMENT VOLUME 19 ISSUE 29 APRIL 2015 ISSN 1366-5278
those aged < 75 years who weighed > 60 kg (no previous stroke or transient ischaemic attack). For the
primary composite end point (death from CV causes, non-fatal myocardial infarction or non-fatal stroke)
statistically significantly fewer events occurred in the prasugrel arm (8.3%) than in the clopidogrel arm (11%)
there was a significant
difference in favour of clopidogrel when major and minor bleeding events were combined (3.0 vs. 3.9%)
Lack of
data precluded a clinical comparison of prasugrel with ticagrelor; the comparative effectiveness of
prasugrel compared with ticagrelor therefore remains unknown.
Well-audited data are needed from a
long-term UK clinical registry on defined ACS patient groups treated with PCI who receive prasugrel,
ticagrelor and clopidogrel.

HEALTH TECHNOLOGY ASSESSMENT VOLUME 19 ISSUE 29 APRIL 2015 ISSN 1366-5278
The results of sensitivity analyses confirmed that it is likely
that, for all four ACS subgroups, within 5–10 years prasugrel is a cost-effective treatment option compared
with clopidogrel at a willingness-to-pay threshold of £20,000 to £30,000 per QALY gained. At the full
40-year time horizon, all estimates are < £10,000 per QALY gained

INICIACE PROTIDESTIČKOVÉ LÉČBY U STEMI
• VYSOKÉ TROMBOTICKÉ RIZIKO V PRVNÍCH FÁZÍCH STEMI
– CO NEJDŘÍVE PO PRVNÍM KONTAKTU S
NEMOCNÝM
– PREFERENČNĚ PRASUGREL nebo TICAGRELOR
– SOUČASNĚ PLNÁ ANTIKOAGULAČNÍ LÉČBA
• V DALŠÍCH FÁZÍCH PŘEVAŽUJE KRVÁCIVÉ RIZIKO A PŘÍPADNÉ JINÉ VEDLEJŠÍ ÚČINKY
– PODLE TOHO ÚPRAVA TRVÁNÍ A ZPŮSOBU
ANTITROMBOTICKÉ LÉČBY
• TÉMA DALŠÍHO SDĚLENÍ
ZÁVĚR


AKUTNÍ IM • CLOPIDOGREL
– POMALÝ NÁSTUP, U IM EFEKTIVITA < 50 %
• PRASUGREL
– NELZE U OSOB > 75 let, < 60 kg, po TIA, CMP
• TICAGRELOR – PŘI DLOUHODOBÉM PODÁVÁNÍ časté
předčasné vysazení, vyšší výskyt rakoviny
Serebruany V L. Ticagrelor shift from PLATO to PEGASUS: Vanished mortality benefit, excess cancer deaths, massive discontinuations, and overshooting target events. International Journal of Cardiology 201, 15 December 2015, Pages 508–512









