Download - In association with Diabetes UK

MAKING BEST PRACTICE EVERYDAY PRACTICE
Best practice in diabetes
Professor Michael Kirby & Jane Diggle
Chair: Fola Omotunde
In association with Diabetes UK
Delivering best practice: 5 Steps / Interactive Case Study

Making Best Practice, Everyday Practice 4th November 2016
Delivering Diabetes Care
in General Practice Professor Mike Kirby
Jane Diggle

Professor Mike Kirby MK has received funding for research, conference attendance, lecturing and advice from the pharmaceutical industry including Astellas, Pfizer, Takeda, Bayer, MSD, BI, Lilly, GSK, AZ and Menarini. Editor PCCJ. Also on several NHS advisory boards including the Prostate cancer Risk Management Programme and the Prostate Cancer advisory Group. Jane Diggle Associate Editor-in-Chief for Diabetes and Primary Care , Board Member of the Primary Care Diabetes Society (PCDS) Committee, the Forum for Injection Technique(FIT) and Associate Member of TREND-UK. Received funding for participation in Advisory Boards, presentations and preparation of educational materials for Boehringer Ingelheim, BMS/Astra Zeneca, Eli Lilly, Janssen, MSD, Takeda, Novo Nordisk and Sanofi.
Disclosures

What are we trying to achieve? ● To alleviate symptoms ● Maintain Quality of Life
● Prevent or slow the progression of complications
Best Practice Diabetes Care

1. Kaplar M, et al. J Nucl Med 2009; 50:1993–1998. 2. Diabetes in the UK. Diabetes UK. Available at http://www.diabetes.org.uk/Documents/Reports/Diabetes-in-the-UK-2012.pdf. April 2012. Last accessed October 2013. 3. Mealey BL. JADA 2006; 137 (Suppl 10):26S–31S. 4. Tolman KG, et al. Diabetes Care 2007;30(3):734–43.
Microvascular complications Macrovascular complications
Diabetic nephropathy2
Diabetic retinopathy2
Diabetic neuropathy2
Brain and cerebral circulation1
Periodontal disease3
Erectile dysfunction2
Peripheral vascular disease2
Heart disease2
Stroke2
Liver disease4
The complications associated with diabetes

What is Best Practice?

What percentage of people registered with diabetes achieved the NICE defined treatment targets for glucose control, blood pressure and blood
cholesterol?
Type 1 Type 2 and other 2009-10 2010-11 2011-12 2012-13 2013-14 2014-15 2009-10 2010-11 2011-12 2012-13 2013-14 2014-15
HbA1c < 58 mmol/mol 28.7 28.1 27.0 27.2 29.4 29.9 66.6 66.5 65.8 64.9 66.8 66.1 Blood Pressure < 140/80* 68.5 68.8 72.2 73.4 76.4 76.4 60.8 61.4 66.6 68.6 73.6 74.2 Cholesterol < 5mmol/L 72.6 72.0 71.1 70.2 71.5 71.3 78.2 78.0 77.4 76.7 77.8 77.5
Meeting all three treatment targets 16.9 16.5 16.5 16.1 18.6 18.9 35.0 35.1 37.4 37.3 41.4 41.0
Percentage of people with diabetes in England and Wales achieving their treatment targets by diabetes type and audit year
* The blood pressure target does not exactly match NICE (<140/80) but was changed to align with the relevant QOF indicator (<140/80) . More information can be found here

What are the challenges?
• Progressive condition requiring treatment intensification.
• Often associated with co-morbidities (polypharmacy – complex regimens)
• Often asymptomatic - difficult to convey the benefits of treating now to reduce
future risks (especially where drugs cause side effects)
• Poor medication adherence
• Encouraged to involve patients in shared decision-making but patient
knowledge may be poor.
• Patient expectations are rising – with ever-expanding choice of therapies.
• Prescribing costs are escalating but pressure to reduce prescribing costs.
• New evidence emerging all the time.

“Clinical guidelines are recommendations on the appropriate treatment and care of people with specific conditions that are based on the best available evidence. They are designed to help healthcare professionals in their work, but do not replace their knowledge and skills.”
NICE (2014) Clinical guidelines. NICE, London. Available at: www.nice.org.uk/CG (accessed: 23.05.2014)
NICE Clinical Guidelines – NG28: Type 2 diabetes in adults: management http://www.nice.org.uk/guidance/ng28
New Guidelines for Type 2 diabetes

Meet Margaret
57yrs old - on routine screening found to have diabetes. HbA1c is 72mmol/mol. Mild symptoms
• Polyuria • Recurrent thrush ( 3 episodes over past year)
BMI 32 Kg/m2
BP 155/85 mmHg Cholesterol 5.2mmol/l
• Non HDL Cholesterol 3.4mmol/l ALT 92mmol/l eGFR 68ml/min/1.73m2 ACR 5mg/mmol Family history
• Mother Type 2 diabetes diagnosed at 54yrs when admitted with an MI.
• Father CVA aged 78yrs.

What are the issues?
Margaret’s medical issues
• 57yr old • Mild symptoms • Overweight • Raised BP • Dyslipidaemia • Albuminuria • Abnormal LFT • FH premature CVD
Clinical scenario
• BMI 32 Kg/m2
• BP 155/85mmHg • HbA1c 72 mmol/mol • Cholesterol 5.2mmol/l
– Non HDL Cholesterol 3.4mmol/l
• eGFR 68ml/min/1.73m2
• ALT 92mmol/l • ACR 5mg/mmol

Tackling her CV risk
• QRisk2
• Consider 24 hour ABPM • Need to establish if there are microvascular complication (repeat ACR) as this
will impact BP target • preferred target is ≤ 140/80 • CKD/proteinuria the target is ≤ 130/80
• Lifestyle Interventions (Diet and physical activity including weight
management, alcohol consumption, caffeine & salt intake, smoking cessation advice for smokers, referral to health trainer if appropriate)
• Consider anti-hypertensive therapy: ACE inhibitor first-line.
• Consider Lipid-lowering therapy (if QRisk2 is above 10%) : Atorvastatin 20mg – Aim for a 40% reduction in non-HDL.

Key NICE Updates
• Hypertension CG 127 (August 2011). • Lipid Modification CG 181 (July 2014). • Chronic Kidney Disease CG 182 (July 2014).

• Agree an individualised HbA1c target.
• Where appropriate, aim for the targets on the algorithm.
• Measure HbA1c at 3 or 6 monthly intervals.
• Choose from the full range of oral treatments. – Base treatment choice on effectiveness, safety, tolerability, individual
circumstances, preferences, needs, indications and costs
– If 2 drugs in same class, choose the lowest acquisition cost option.
• SMBG guidance not changed (not routinely unless person is on insulin, on oral medication that may increase their risk of hypoglycaemia while driving or operating machinery, is pregnant or planning to become pregnant or if there is evidence of hypoglycaemic episodes).
Tackling her HbA1c

UKPDS=United Kingdom Prospective Diabetes Study Holman RR et al (2008) N Engl J Med 359: 1577–89 UKPDS Group (1998) Lancet 352: 854–65
Med
ian
HbA
1c (%
)
0 6
7
8
9
UKPDS 1998
Conventional Approach More intensive approach
Holman et al 2008
Drives the “legacy effect”
1997
Difference in HbA1c was lost after first year but those in the initial intensive arm still had lower incidence of any complication 10 years
later (the legacy effect): • 21% reduction in any diabetes-related endpoint (P=0.01) • 33% reduction in myocardial infarction (P=0.005) • 27% reduction in death from any cause (P=0.002)
2007
UKPDS: early, intensive control of hyperglycaemia is important

But tackling lifestyle is a real challenge…….
Lifestyle modification is key

Telling people what to do doesn’t work!

We have to hand over responsibility to the patient, explore their attitudes & beliefs & find more effective ways to support them to make healthier
and less risky lifestyle decisions.
THE CHANGE EQUATION (Gleicher – Beckard & Harris 1987)
Dissatisfaction x Vision x First Steps > Resistance to change
To change behaviour a person has to: • be dissatisfied with their current situation (D) • want to change it (V) • know how to make the first step towards this (F) • feel confident in their ability to make the change.
Metformin
+
Sulphonylurea
+
Insulin
• Thiazolidinediones (Glitazones)
• DPP4-inhibitors
• SGLT2-inhibitors
• GLP-1 RA’s
• New insulin Strengths
• Biosimilar Insulin
But ultimately most people will need blood glucose lowering drugs…


Metformin

Metformin
• Mechanisms of action – ↓ hepatic glucose production, ↑ gut glucose uptake, ↑ GLP-1, alters bile acids and microbiome.
• NICE - First-line unless contraindications • Build dose – start low, go slow, aim for 1g twice daily • No hypoglycaemia, weight neutral; CVD benefit (UKPDS) • GI side effects – allow to settle; trial Metformin MR • Consensus - Reduce dose if eGFR <45; stop if <30 • Stop therapy temporarily if fluid depletion eg vomiting diarrhoea • B12 deficiency - ? significance
Available in combination with other oral drugs to reduce pill burden/cost McCreight, Bailey and Pearson Diabetologia 2016; 59: 426-35 Inzucchi et al Diabetes Care 2015; 38: 140-49

“I feel well thanks”
“Metformin gave me a bit of diarrhoea”
“I want to do something about my weight”
4 months later …..
HbA1c is 65mmol/mol
Margaret is on maximum tolerated metformin (Metformin MR 1g daily)
What next?
• Revisit lifestyle – scope to make more changes?
• Offer structured education. • Check medication
adherence!

What next after metformin?
Metformin
Sulphonylurea DPP-4 inhibitor Pioglitazone SGLT-2 inhibitor
Agree a target and aim for HbA1c of 53mmol/mol (7%).

What next after metformin?
Metformin
Sulphonylurea DPP-4 inhibitor Pioglitazone SGLT-2 inhibitor

DPP-4 inhibitors
• Sitagliptin, saxagliptin, vildagliptin, linagliptin, alogliptin • Glucose-dependent ↑ insulin secretion and ↓ glucagon secretion • Low risk of hypoglycaemia. • Weight neutral. • Excreted by kidney apart from linagliptin – may reqwuire dose adjustment
according to eGFR. • CVD safety studies
– sitagliptin – no HF (TECOS) – saxagliptin (SAVOR TIMI) and alogliptin (EXAMINE) – possible ↑ heart
failure hospitalisations • Well tolerated; possible risk pancreatitis
Scirica et al. N Engl J Med 2013;369:1317-26. White et al. N Engl J Med 2013;369:1327-35. Inzucchi et al Diabetes Care 2015; 38: 140-49

Causes of Mortality in Patients With Diabetes

UK/DIA/00315 | February 2016
Heart failure and T2D share risk factors Independent risk factors for developing heart failure or T2D1–5
*Synthesised based on data from 2 clinical studies – see notes page for details Please see notes page for references 28
People with diabetes have a 2–3-fold higher risk of developing heart failure8
Diabetes increases the risk of all-cause mortality and cardiovascular death in the heart failure setting9*
Age,4,6 ethnicity,4,6 family history,4,6 obesity,2–4 fat distribution,4,7
hypertension,3 smoking3
T2D is an independent
risk factor for heart failure1
Heart failure is an independent
risk factor for T2D1,2
UK/DIA/00315 | February 2016
0.8 -
0.6 -
0.4 -
0.2 -
1.0 -
0.0 - 0 2 4 6 8 10 12
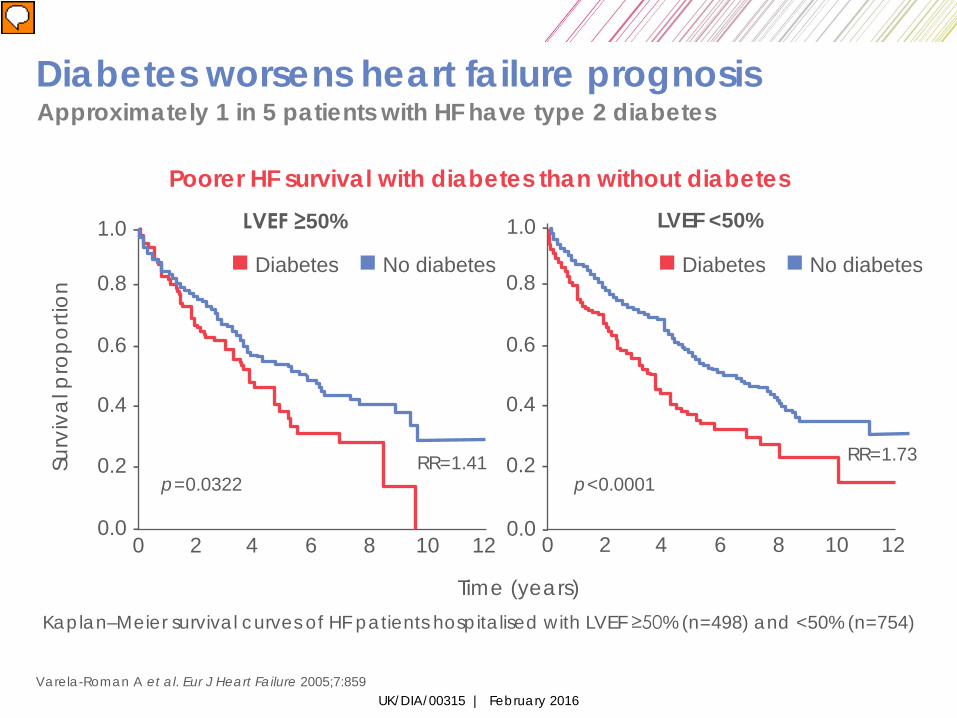
Varela-Roman A et al. Eur J Heart Failure 2005;7:859
Poorer HF survival with diabetes than without diabetes
Kaplan–Meier survival curves of HF patients hospitalised with LVEF ≥50% (n=498) and <50% (n=754)
1.0 -
0.8 -
0.6 -
0.4 -
0.2 -
0.0 - 0 2 4 6 8 10 12
Surv
iva
l pro
por
tion
Time (years)
p=0.0322 RR=1.41
p<0.0001 RR=1.73
LVEF ≥50% LVEF <50%
Diabetes No diabetes Diabetes No diabetes
Diabetes worsens heart failure prognosis Approximately 1 in 5 patients with HF have type 2 diabetes

UK/DIA/00315 | February 2016
The presence of diabetes increases the risk of hospitalisation or death in patients with heart failure
Aguilar D, et al. Am J Cardiol. 2010;105:373–377.
Adjusted HR 1.68 95% CI: 1.26–2.25; p < 0.01
0.00
0.05
0.10
0.15
0.20
0.25
0.30
0.35
0.40
HF
hosp
italis
atio
n or
HF
dea
th
0 12 24 36 48 Months
No diabetes
Diabetes
Number of patients at risk 285 702
234 613
193 559
121 366
47 136

UK/DIA/00315 | February 2016
Life expectancy is reduced by 12 years in diabetes patients* with previous CV disease
In this case, CV disease is represented by MI or stroke *60 years of age The Emerging Risk Factors Collaboration. JAMA. 2015;314:52. 31
60 End of life yrs
-6 yrs
-12 yrs
No diabetes
Diabetes
Diabetes + MI


33
CV = cardiovascular; DPP-4 = dipeptidyl peptidase-4; CAD = coronary artery disease; CVD = cardiovascular disease; PAD = peripheral artery disease; ACS = acute coronary syndrome; EXAMINE = Examination of Cardiovascular Outcomes: Alogliptin vs Standard of Care in Patients With Type 2 Diabetes Mellitus and Acute Coronary Syndrome; SAVOR-TIMI 53 = Saxagliptin Assessment of Vascular Outcomes Recorded in Patients With Diabetes Mellitus Trial-Thrombolysis in Myocardial Infarction 53; TECOS = Trial Evaluating Cardiovascular Outcomes With Sitagliptin; CARMELINA = Cardiovascular and Renal Microvascular Outcome Study With Linagliptin in Patients With Type 2 Diabetes Mellitus at High Vascular Risk. 1. White W et al. N Engl J Med. 2013;369:1327–1335. 2. Scirica BM et al. N Engl J Med. 2013;369:1317–1326. 3. Bethel MA et al. Diabetes Obes Metab. 2015; 17:395–402. 4. Green JB et al. N Engl J Med. 2015 Jun 8.[Epub ahead of print]. 5. CARMELINA: Cardiovascular and renal microvascular outcome study with linagliptin in patients with type 2 diabetes mellitus at high vascular risk. ClinicalTrials.gov web site. http://clinicaltrials.gov/ct2/show/ NCT01703298. Accessed September 12, 2014.
Baseline Risk of Patient Populations Enrolled in CV Safety Trials of DPP-4 Inhibitors
Vildagliptin does not have an ongoing CV safety trial
Linagliptin CARMELINA (N=8,300)5
Pre-existing CVD + albuminuria or impaired renal function End Jan 2018
Sitagliptin TECOS (N=14,671)3,4
Pre-existing CVD Presented Jun 2015
Alogliptin EXAMINE (N=5,380)1
ACS within 15–90 days
Presented Sept 2013
Saxagliptin SAVOR-TIMI 53 (N=16,492)2
Pre-existing CVD or multiple risk factors for CVD
Presented Sept 2013
Risk Factors Stable CAD-CVD-PAD Post ACS patients

The Truth Is Not So Sweet
Cardiovascular safety of diabetes drugs
• The goal of marely lowering blood glucose levels in diabetes is too simplistic
• With respect to CVD it appears important how you lower blood sugar as well as how much
• Diabetes drugs, even within the same “class” may yield dramatically different CV outcomes

35
EXAMINE = Examination of Cardiovascular Outcomes: Alogliptin vs Standard of Care in Patients With Type 2 Diabetes Mellitus and Acute Coronary Syndrome; SAVOR-TIMI 53 = Saxagliptin Assessment of Vascular Outcomes Recorded in Patients With Diabetes Mellitus Trial-Thrombolysis in Myocardial Infarction 53; TECOS = Trial Evaluating Cardiovascular Outcomes With Sitagliptin. CV = cardiovascular; MI = myocardial infarction; UA = unstable angina. 1. White WB et al. N Engl J Med. 2013;369:1327–1335. 2. Scirica BM et al. N Engl J Med 2013;369:1317–1326. 3. Green JB et al. Am Heart J. 2013;166:983–989.e7. 4. Bethel MA et al. Diabetes Obes Metab. 2015; 10.1111/dom.12441. 5. Green JB et al. New Engl J Med 2015 Jun 8.[Epub ahead of print].
DPP4 EXAMINE, SAVOR-TIMI 53, and TECOS CV Safety Trials
Median Duration of Follow-up
SAVOR- TIMI 532
TECOS3–5
EXAMINE1
6.5–8.0
CV death, Nonfatal MI,
Nonfatal stroke, or UA req. hospitalization
Randomization Year 3 Year 2 Year 1
CV death, Nonfatal MI, or Nonfatal stroke
CV death, Nonfatal MI, or Nonfatal stroke
Saxagliptin
Alogliptin
Placebo
Placebo
6.5–12.0
6.5–11.0
HbA1c Range, % Primary End point Duration of Treatment (as part of usual care)
R
R
R
Sitagliptin
Placebo

Heart failure • Insulin, induces sodium retention and thiazolidinediones
increase the risk of heart failure.
• Increase in the risk of admission to hospital for heart failure in patients treated with the dipeptidylpeptidase-4 (DPP4) inhibitor, saxagliptin, compared with placebo. (SAVOR TIMI- 53)
• There was also a trend toward an increased risk of heart-failure events among type 2 diabetic patients treated with alogliptin (Nesina, Takeda) in the EXAMINE study.
• TECOS: No CVD Risks or Heart Failure With Sitagliptin in High-Risk Diabetic Patients

What next after metformin?
Metformin
Sulphonylurea DPP-4 inhibitor Pioglitazone SGLT-2 inhibitor

SGLT-2 inhibitors • Sodium-glucose co-transporter 2 inhibitors – reduce reabsorption glucose in
kidney; lose up to 80g glucose daily • Insulin independent – use at any stage • Weight reduction (2kg+), BP benefits (2-4/1-2mmHg) • Empagliflozin positive CVD study (EMPA-REG); others awaited • Less effective when eGFR <60 (canagliflozin, empagliflozin can continue
lower dose to eGFR 45) • Caution with loop diuretic; fluid depletion, elderly • Increased fungal and urinary infections • Emerging euglycaemic DKA risk – rare
– Must warn patients (partners/other professionals) – Ensure practice systems to test for ketones – PCDS statement
• Increased toe amputations (canagliflozin)
Inzucchi et al Diabetes Care 2015; 38: 140-49

UK/DIA/00282b | October 2015
Primary outcome: 3-point MACE
HR 0.86 (95.02% CI 0.74, 0.99)
p=0.04*
Cumulative incidence function. MACE, Major Adverse Cardiovascular Event; HR, hazard ratio: RRR: Relative risk reduction; ARR: Absolute risk reduction. * Two-sided tests for superiority were conducted (statistical significance was indicated if p≤0.0498) RRR: 14%; ARR: 1.6% (CER – EER): Incidence of 3P-MACE: 10.5% (empagliflozin) vs. 12.1% (placebo). CER: Control event rate; EER: Experimental event rate. Zinman B et al. N Engl J Med 2015 DOI: 10.1056/NEJMoa1504720

UK/DIA/00282b | October 2015
CV death
HR 0.62 (95% CI 0.49, 0.77)
p<0.001
RRR: 38%; ARR: 2.2%. (CER – EER) Rates of CV death: 3.7% (empagliflozin) vs. 5.9% (placebo) Cumulative incidence function HR, hazard ratio. Indicated with 95% confidence intervals; RRR: Relative risk reduction; ARR; Absolute risk reduction; CER: Control Event Rate; EER: Experimental Event rate. Zinman et al N Engl J Med 2015; doi: 10.1056/NEJMoa15047201

UK/DIA/00282b | October 2015
Hospitalisation for heart failure
HR 0.65 (95% CI 0.50, 0.85)
p=0.002
Cumulative incidence function. HR, hazard ratio; RRR: Relative risk reduction; ARR: Absolute risk reduction; CER: Control Event Rate; EER: Experimental Event rate. RRR: 35%; ARR: 1.4% (CER – EER). Incidence of HHF: 2.7% (empagliflozin) vs. 4.1% (placebo) Zinman B et al. N Engl J Med 2015 DOI: 10.1056/NEJMoa1504720

UK/DIA/00282b | October 2015
All-cause mortality
HR 0.68 (95% CI 0.57, 0.82)
p<0.001
Kaplan-Meier estimate. HR, hazard ratio; RRR: Relative risk reduction; ARR: Absolute risk reduction. CER: Control Event Rate; EER: Experimental Event rate. RRR: 32%; ARR: 2.6% (CER – EER). Incidence of All-cause mortality: 5.7% (empagliflozin) vs. 8.3% (placebo) Zinman B et al. N Engl J Med 2015 DOI: 10.1056/NEJMoa1504720

Empagliflozin modulates several factors related to CV risk
Adapted from Inzucchi SE,Zinman, B, Wanner, C et al. Diab Vasc Dis Res 2015;12:90-100 45
BP Arterial stiffness
Glucose Insulin
Albuminuria
Uric acid
Other
↑LDL-C ↑HDL-C
Triglycerides
Oxidative stress
Sympathetic nervous system
activity
Weight Visceral adiposity

What next after metformin?
Metformin
Sulphonylurea DPP-4 inhibitor Pioglitazone SGLT-2 inhibitor

Thiazoledinediones - Pioglitazone
• Increases insulin sensitivity • Pioglitazone – start 15mg; can increase to 45mg daily • No hypoglycaemia; durable action • Weight gain, fluid retention, peripheral oedema and heart failure • Bladder cancer possibly increased – avoid if undiagnosed
haematuria/previous bladder cancer • Increased fracture risk especially in women • Possible decreased CVD (PROactive study) • Not restricted in renal disease • May improve LFTs – possible benefits in NAFLD
Inzucchi et al Diabetes Care 2015; 38: 140-49 Tuccori et al BMJ 2016;352:i1541 Charbonnel et al Diabetes care 2004; 27: 1647-1653

What next after metformin?
Metformin
Sulphonylurea DPP-4 inhibitor Pioglitazone SGLT-2 inhibitor

Sulphonylureas and meglitinides
• Increase insulin secretion • Effective at reducing HbA1c; long-term experience; ↓ microvascular risks
(UKPDS) • Significant hypoglycaemia risks (monitoring/ driving). • Weight gain; low durability • Meglitinides – ‘prandial glucose regulators’ - complex dosing, still significant
hypoglycaemia risk
Inzucchi et al Diabetes Care 2015; 38: 140-49
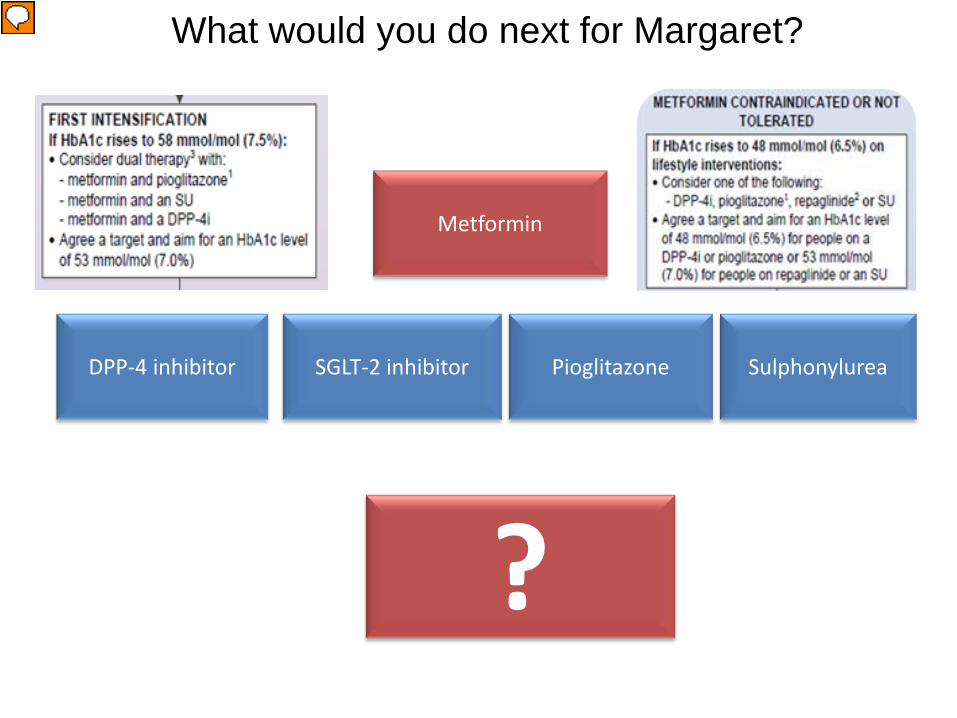
What would you do next for Margaret?
Metformin
Sulphonylurea DPP-4 inhibitor Pioglitazone SGLT-2 inhibitor
?

And later…..
Metformin
Sulphonylurea
DPP-4 inhibitor
Pioglitazone
SGLT-s inhibitor
GLP-1 agonist
Insulin

LEADER trial: Primary Outcome
15
10
20
5
0
0 6 12 18 24 30 36 42 48 54
Placebo Liraglutide
Pat
ient
s w
ith a
n ev
ent (
%)
Months since randomisation
Hazard ratio, 0.87 (95% CI, 0.78–0.97) P<0.001 for noninferiority P=0.01 for superiority
First occurrence of CV death, nonfatal myocardial infarction, or nonfatal stroke in the time-to-event analysis in patients with type 2 diabetes and high CV risk.
Liraglutide Effect and Action in Diabetes: Evaluation of cardiovascular outcome Results (LEADER) trial
Adapted from: Marso SP et al., NEJM 2016

LEADER trial: Death from Cardiovascular Causes
15
10
20
5
0
0 6 12 18 24 30 36 42 48 54
Placebo Liraglutide
Pat
ient
s w
ith a
n ev
ent (
%)
Months since randomisation
Hazard ratio, 0.78 (95% CI, 0.66–0.93) P=0.007
Liraglutide Effect and Action in Diabetes: Evaluation of cardiovascular outcome Results (LEADER) trial
Adapted from: Marso SP et al., NEJM 2016

Results of the sodium-glucose-lithium transporter 2 (SGLT-2) inhibitor empagliflozin trial (EMPA-REGS) 11
AND The results of the glucagon-like peptide-1 (GLP-1) agonist liraglutide (LEADER-6) 12 trial showed reduced CVD events and mortality !! Will lead to the order of different classes of hypoglycaemic therapy in the pathway being rearranged.
11 Zinman B et al Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med 2015 ; 373 : 2117 – 28 . 12 Marso SP et al . Liraglutide and
cardiovascular outcomes in type 2 diabetes . N Engl J Med 2016 ; DOI: 10.1056/NEJMoa1603827.
Diabetes

Individualisation is the key!

Factors to be taken into consideration when selecting an appropriate drug
? Therapy for diabetes
Age Occupation
Hobbies
Sex
Past medical history (e.g. haematuria/
cancer)
Renal function
Fasting
Live alone / nutrition
Driving
Liver function
BMI / body
weight
Fracture risk
? Therapy for
diabetes

ADA/EASD position statement: Intensiveness of glucose lowering should be individualised
ADA=American Diabetes Association; EASD=European Association for the Study of Diabetes. Inzucchi SE et al (2015) Diabetes Care 38: 140–9
Few/mild
Few/mild
Usually not modifiable
Potentially modifiable
More stringent HbA1c 7% Less stringent
Risks potentially associated with hypoglycaemia and other drug adverse events Disease duration Life expectancy Important comorbidities Established vascular complications Patient attitude and expected treatment efforts Resources and support system Readily available Limited
Less motivated, non-adherent, poor self-care capacities
Severe
Severe
Short
Long-standing
High
Highly motivated, adherent, excellent self-care capacities
Absent
Absent
Long
Newly diagnosed
Low
Patient/disease features

Current glycaemic control
Frail elderly control often too tight
Younger and early disease often not tight
enough
Glycaemic control

• When caring for older people with type 2 diabetes, consider their broader health and social care needs.
• They are more likely to have co-existing conditions (dementia, mobility &
sensory problems) and are likely to be on more medications. • Their ability to benefit from risk-reduction interventions in the longer term
may be reduced. • Much of the evidence base used to inform guidelines has been generated
from studies involving younger adults (under 70 years).
• Avoidance of hypoglycaemia should take priority.
• Relax HbA1c targets (worth auditing this – especially for those in care homes or living alone)
Older People

Clinical inertia
Retrospective Cohort Study 2 2004-2011 n= 81,573 In those with HbA1c >7% it took: • 1.6 years before a second oral agent was added. • >6.9 years before a third oral agent was added.
• HbA1c typically reached 8.7 – 9.7% (71.6 - 82.5mmol/mol) before insulin was
initiated.
“Clinical inertia may be defined as a failure to initiate or intensify treatment in a timely manner in people with diabetes whose health is likely to improve with this intensification” 1
1. Strain WD, et al. Diabetes Research and Clinical Practice 105. 2014;302–312. 2. Khunti K, et al. Diabetes Care 2013;36:3411–7

In conclusion….. 5 Key Messages
1. Guidelines are not absolutes (we need to individualise targets and treatment).
Ref. Page 56 of NG28

2. Diabetes management is not just about blood glucose.

EVERY 1% reduction in HbA1c
REDUCED RISK*
1%
UKPDS Lancet 1998; 352: 837–853.
Deaths from diabetes
Heart attacks
Microvascular complications
Peripheral vascular disorders
*p<0.0001
Lessons from UKPDS: better control means fewer complications

3. We need to encourage and support patients to self-manage and be actively involved in treatment decisions through education and motivational approaches.

4. We all need to be properly trained
Now, chuck out your uni books, pop this on and everything will be just like the good old days……
http://www.trend-uk.org/documents/TREND_4th%20edn_V9.pdf

Six SMART Steps to Insulin Safety
5. You can’t do an annual diabetes review in 10 minutes!
• Consider skill mix (HCA) • Share results with patient prior to the consultation • Encourage patient to consider what issues they want to discuss
and what they need more information about and focus on that.








