Illinois Breastfeeding Blueprint
Quantitative Data Appendix:
Data Sources, Methodology, and Additional Analyses
Table of Contents
Section 1. Illinois Breastfeeding Data Sources…………………………………………………………………………………………1
Section 2. Notes about Race/Ethnicity………………………………………………….……………………………………………….. 2
Section 3. Creation of Low Income Index………………………………………………………………………………………………..3
Section 4. Hispanic Sub-Group Analyses………………………………………………………………………………………………… 4
Section 5. WIC Client Breastfeeding Continuation Analysis……………………………………………………………………. 8
Section 6. Effect of Hospital Practices on Breastfeeding Continuation and Exclusivity………………………….10

1
Section 1: Illinois Breastfeeding Data Sources ** indicates data source used in the Illinois Breastfeeding Blueprint report
Birth Certificates (starting with 2010 births)
As of 2010, Illinois revised the birth certificate to include a question about breastfeeding. The question is worded:
““Is the infant being breastfed at discharge?” with the option of responding yes or no. Once 2010 birth certificate
data are complete, the Illinois Department of Public Health will be able to examine the responses and report
differences in breastfeeding rates throughout the state, including by delivery hospital. This will provide the state
with important information about geographic and demographic differences in early breastfeeding behaviors, as
well as documenting the association of early breastfeeding with later infant and child health. Hospital level data
on the birth certificate breastfeeding question is publically available on the Illinois Hospital Report Card website
(http://www.healthcarereportcard.illinois.gov).
Cornerstone
Cornerstone is the administrative database for many Illinois Department of Human Services programs, including
the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) and Family Case
Management (FCM). For infants enrolled in WIC, breastfeeding information is recorded and updated over time,
so this system can provide information about breastfeeding initiation, duration, and length of exclusive
breastfeeding.
Maternity Practices in Infant Nutrition and Care (mPINC) **
mPINC is a survey of hospital representatives about policies and practices related to breastfeeding conducted
biannually by the Centers for Disease Control and Prevention (CDC). Questions are asked about specific practices
related to: labor and delivery care, feeding of breastfed infants, breastfeeding assistance, contact between the
mother and infant, facility discharge care, staff training, and structural/organizational aspects of care. The results
of this survey are publicly available by state, so Illinois’ scores may be compared to those of other states and the
nation overall. The first version of the survey was administered in 2007 and all hospitals in Illinois were invited to
participate. Illinois, however, had a low response rate compared to other states, with only 59% of hospitals
completing the survey compared to a national average of 80%. The mPINC survey was repeated in 2009, and data
will be publicly available in summer 2011. Please check the CDC mPINC website for updated data
(http://www.cdc.gov/breastfeeding/data/mpinc/index.htm).
National Immunization Survey (NIS)
NIS is an annual survey conducted by the Centers for Disease Control and Prevention. It surveys a representative
sample of families of children 19-35 months old. While the major focus of the survey is immunizations, NIS asks
questions about breastfeeding initiation, duration, and exclusivity. Estimates of breastfeeding for all women
giving birth in each State are available yearly and may be compared to those in other states and the nation
overall.
Pregnancy Risk Assessment Monitoring System (PRAMS) **
PRAMS is an annual survey of Illinois women who recently delivered a live birth that collects information about
maternal attitudes and experiences before, during, and shortly after pregnancy. Participants are typically
surveyed by mail or phone 3 to 6 months after delivery. Women are asked about their breastfeeding behaviors
(such as initiation, duration, and length of exclusivity), reasons why they chose not to breastfeed or to stop
breastfeeding, and whether or not they experienced specific hospital practices during their delivery
hospitalization. There is a rich amount of information available in this survey, which is linked to the birth
certificate for infants of participating mothers.
2
Section 2: Notes about Race/Ethnicity
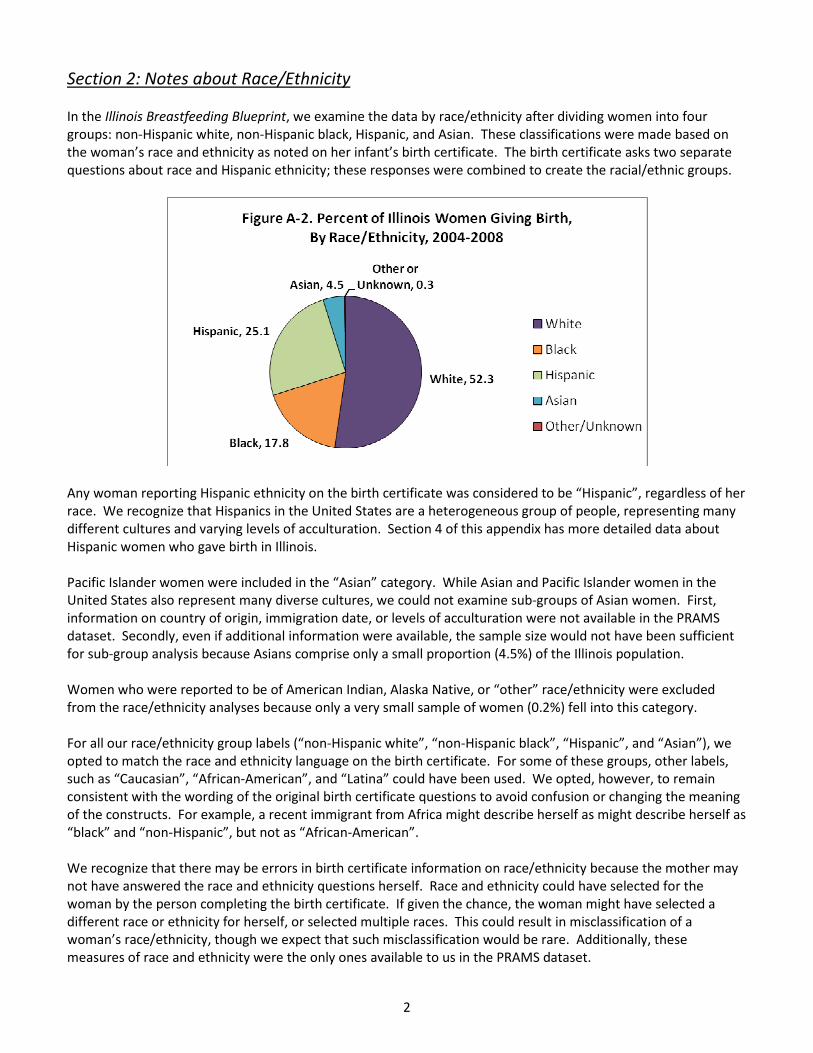
In the Illinois Breastfeeding Blueprint, we examine the data by race/ethnicity after dividing women into four
groups: non-Hispanic white, non-Hispanic black, Hispanic, and Asian. These classifications were made based on
the woman’s race and ethnicity as noted on her infant’s birth certificate. The birth certificate asks two separate
questions about race and Hispanic ethnicity; these responses were combined to create the racial/ethnic groups.
Any woman reporting Hispanic ethnicity on the birth certificate was considered to be “Hispanic”, regardless of her
race. We recognize that Hispanics in the United States are a heterogeneous group of people, representing many
different cultures and varying levels of acculturation. Section 4 of this appendix has more detailed data about
Hispanic women who gave birth in Illinois.
Pacific Islander women were included in the “Asian” category. While Asian and Pacific Islander women in the
United States also represent many diverse cultures, we could not examine sub-groups of Asian women. First,
information on country of origin, immigration date, or levels of acculturation were not available in the PRAMS
dataset. Secondly, even if additional information were available, the sample size would not have been sufficient
for sub-group analysis because Asians comprise only a small proportion (4.5%) of the Illinois population.
Women who were reported to be of American Indian, Alaska Native, or “other” race/ethnicity were excluded
from the race/ethnicity analyses because only a very small sample of women (0.2%) fell into this category.
For all our race/ethnicity group labels (“non-Hispanic white”, “non-Hispanic black”, “Hispanic”, and “Asian”), we
opted to match the race and ethnicity language on the birth certificate. For some of these groups, other labels,
such as “Caucasian”, “African-American”, and “Latina” could have been used. We opted, however, to remain
consistent with the wording of the original birth certificate questions to avoid confusion or changing the meaning
of the constructs. For example, a recent immigrant from Africa might describe herself as might describe herself as
“black” and “non-Hispanic”, but not as “African-American”.
We recognize that there may be errors in birth certificate information on race/ethnicity because the mother may
not have answered the race and ethnicity questions herself. Race and ethnicity could have selected for the
woman by the person completing the birth certificate. If given the chance, the woman might have selected a
different race or ethnicity for herself, or selected multiple races. This could result in misclassification of a
woman’s race/ethnicity, though we expect that such misclassification would be rare. Additionally, these
measures of race and ethnicity were the only ones available to us in the PRAMS dataset.

3
Section 3: Creation of Low Income Index
To compare women of different social situations and explore the relationship between social class and
breastfeeding, we classified women as either low income or non-low income. This classification was made on the
basis of responses to several questions in the PRAMS survey. Women were classified as low income if they
reported at least one of the following: 1) Medicaid as the health insurance payer for prenatal care and/or delivery,
2) Supplemental Nutrition Program for Women, Infants, and Children (WIC) participation during pregnancy and/or
after delivery, 3) Temporary Assistance for Needy Families (TANF) receipt during pregnancy, 4) Food Stamps
receipt during pregnancy, or 5) an annual household income less than $25,000 per year. If women reported that
they did not participate in any of the listed programs and that their household income was $25,000 or higher,
they were classified as non-low income.
As shown in Figure A-1, low income status varied across racial/ethnic groups in the population of women
surveyed. Thirty-seven percent (37%) of non-Hispanic white women who gave birth and 36% of Asian women
who gave birth were considered low income by our classification scheme. In contrast, 91% of non-Hispanic blacks
who gave birth and 88% of Hispanics who gave birth were classified as low income by our index. This reveals the
strong correlation between race/ethnicity and income in our state, particularly among women of reproductive
age, and should be taken into consideration when comparing racial groups overall.

4
Section 4: Hispanic Sub-Group Analyses
Hispanics in the United States are a heterogeneous group of people, representing many different cultures. Many
studies have demonstrated the association of country of origin, immigration status, and level of acculturation with
health behaviors, utilization of health services, and the health status of Hispanics in the U.S.
To try to capture the differences among Hispanics, we wanted to find a way of examining Hispanic sub-groups for
our analysis. We did not have country of origin, immigration status, or primary language available from the
PRAMS survey. We did, however, know which language the mother chose to take the survey in. PRAMS may be
taken in either English or Spanish and women are given the option of which survey language they prefer. While
survey language may serve as an indication of Hispanic women’s comfort with English, it is clearly not a
comprehensive measure for acculturation. Because it was the only option available to us, we used survey
language as a way of dividing Hispanic women who gave birth into two groups.
Overall, Hispanic women made up about 25% of women who give birth in Illinois each year. Of Hispanic women
who took the PRAMS survey, about 35% took the survey in English and 64% took the survey in Spanish.
The charts on the following pages show the differences in breastfeeding initiation, duration, and exclusivity for
Hispanic women based on their survey language. These results demonstrate that not all Hispanic women are
equal in terms of breastfeeding.

5
In 2008, approximately 88% of the
Hispanic women who took the
Spanish survey started
breastfeeding their infants,
compared to 84% of Hispanic
women who took the English
survey. This difference was not
statistically significant and both
groups met the Healthy People
2020 objective of 81.9% for
breastfeeding initiation.
Over time, the breastfeeding
initiation rates for both groups of
Hispanics increased.
Among low income Hispanic
women, 78% of those who took
the English survey and 88% of
those who took the Spanish survey
started breastfeeding their infants.
This difference was statistically
significant.
Among higher income Hispanic
women, there was no difference in
breastfeeding initiation by survey
language. Both groups had high
initiation rates, meeting the
Healthy People 2020 objective.
Additionally, among Hispanic
women who took the Spanish
survey, income did not affect
breastfeeding initiation. For those
who took the English survey, lower
income was associated with lower
breastfeeding rates.
6
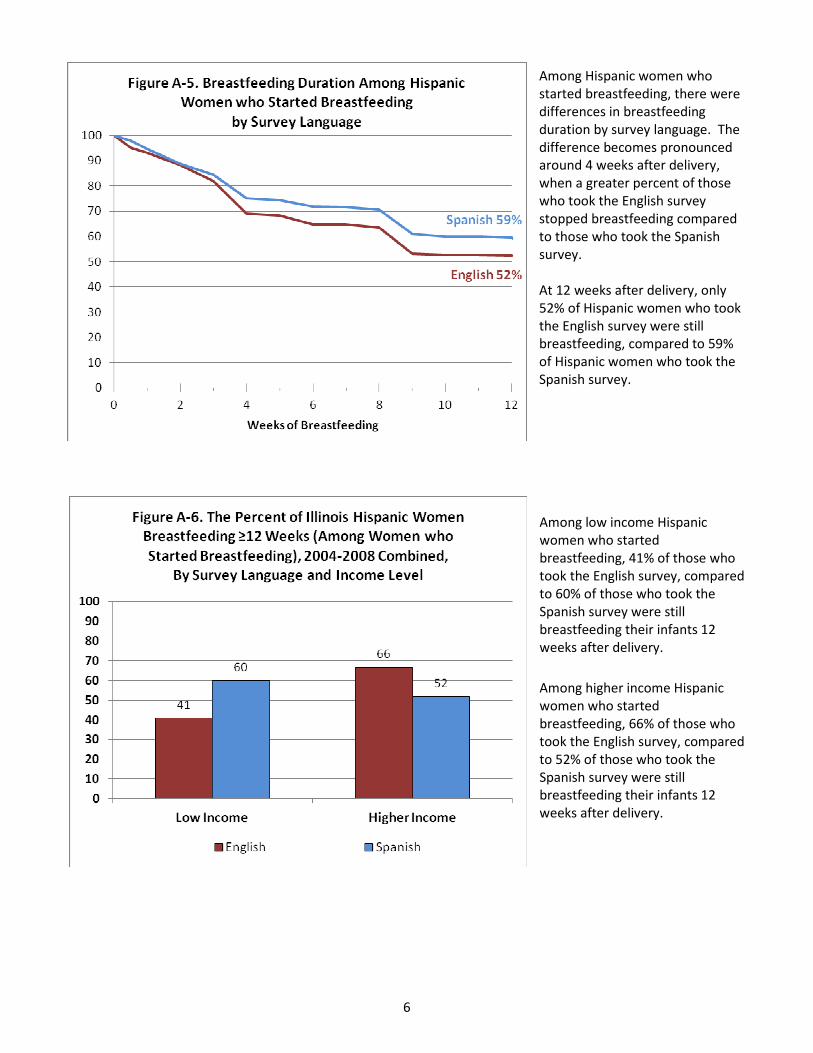
Among Hispanic women who
started breastfeeding, there were
differences in breastfeeding
duration by survey language. The
difference becomes pronounced
around 4 weeks after delivery,
when a greater percent of those
who took the English survey
stopped breastfeeding compared
to those who took the Spanish
survey.
At 12 weeks after delivery, only
52% of Hispanic women who took
the English survey were still
breastfeeding, compared to 59%
of Hispanic women who took the
Spanish survey.
Among low income Hispanic
women who started
breastfeeding, 41% of those who
took the English survey, compared
to 60% of those who took the
Spanish survey were still
breastfeeding their infants 12
weeks after delivery.
Among higher income Hispanic
women who started
breastfeeding, 66% of those who
took the English survey, compared
to 52% of those who took the
Spanish survey were still
breastfeeding their infants 12
weeks after delivery.

7
Survey language did not make a
difference in breastfeeding
exclusivity among Hispanic women
who started breastfeeding.
At 12 weeks after delivery, among
Hispanic women who started
breastfeeding, 23% of those who
took the Spanish survey were
exclusively breastfeeding their
infants compared to 21% of those
who took the English survey.
Survey language and income made
very little difference in the
proportion of Hispanic women
who exclusively breastfed their
infants for at least 12 weeks.
Among low income Hispanic
women who started
breastfeeding, 22% of those who
took the English survey and 23% of
those who took the Spanish survey
were exclusively breastfeeding
their infants 12 weeks after
delivery.
Among higher income Hispanic
women who started
breastfeeding, 24% of those who
took the English survey and 28% of
those who took the Spanish survey
were exclusively breastfeeding
their infants 12 weeks after
delivery.
8
Section 5: WIC Client Breastfeeding Continuation Analysis
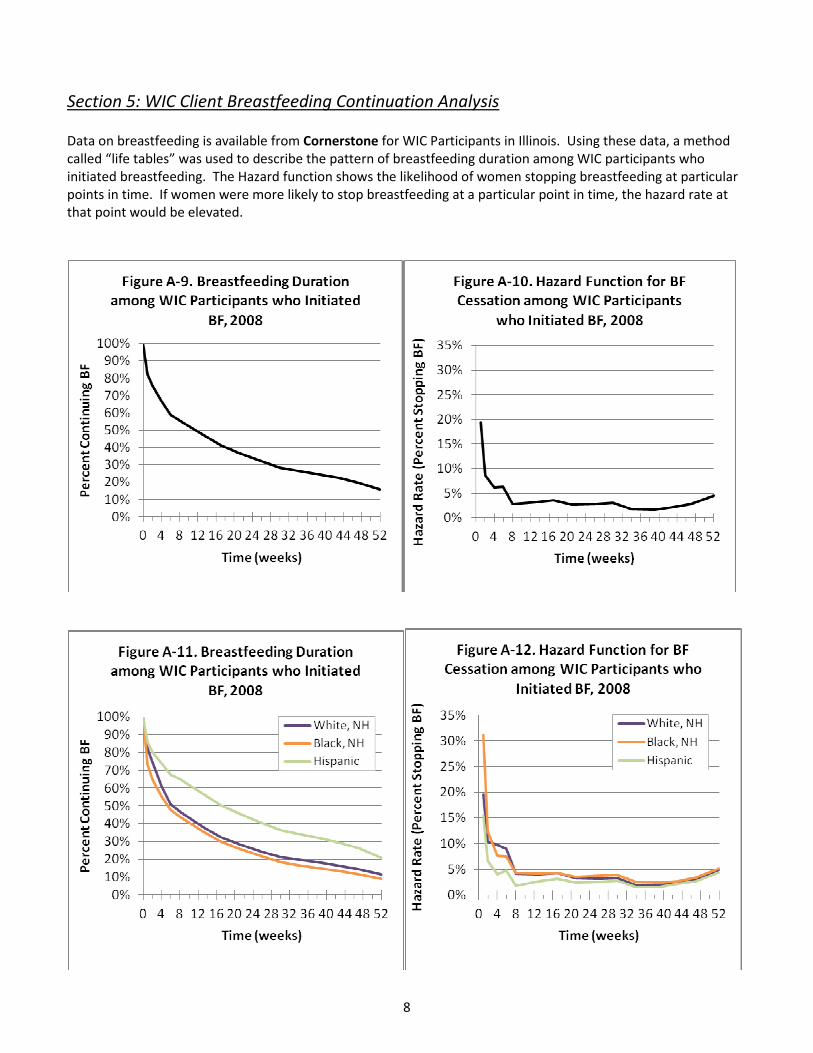
Data on breastfeeding is available from Cornerstone for WIC Participants in Illinois. Using these data, a method
called “life tables” was used to describe the pattern of breastfeeding duration among WIC participants who
initiated breastfeeding. The Hazard function shows the likelihood of women stopping breastfeeding at particular
points in time. If women were more likely to stop breastfeeding at a particular point in time, the hazard rate at
that point would be elevated.
9
Results
Among WIC participants who initiated breastfeeding:
• Less than 50% overall continued for 12 weeks
• Less than 20% overall continued for at least one year
• There were differences in breastfeeding continuation by race/ethnicity
• Black infants were least likely to continue breastfeeding and Hispanic infants were most likely to
continue breastfeeding
• More than 50% of black and white infants had already stopped breastfeeding by 8 weeks
• Only about 10% of black and white infants breastfed for at least one year, compared to 20% of
Hispanic infants
• Within each racial-ethnic group, the hazard rate is highest in the first six weeks. This demonstrates that
the fastest drop-off in breastfeeding occurs during this time period.
• The differences in hazard rates between racial/ethnic groups decrease the longer breastfeeding is
continued
Conclusions
• The majority of Illinois infants born to mothers who participate in WIC are not benefiting from the
recommended duration of breastfeeding.
• Even among WIC infants who start breastfeeding, disparities in duration exist. Black infants are least
likely to continue breastfeeding, though white infants are not far behind them. Hispanic infants are most
likely to continue breastfeeding.
• The first 6 weeks after delivery is when all groups of women are most likely to stop breastfeeding.
• The early postpartum period sets the trajectory for the continuation curve. Helping women continue
breastfeeding through this early period will improve overall breastfeeding duration.

10
Section 6: Effect of Hospital Practices on Breastfeeding Continuation and Exclusivity Women who initiated breastfeeding were included in a study of how maternity care practices impact
breastfeeding duration and exclusivity at 6 weeks postpartum. Among these women who started breastfeeding,
women who reported experiencing certain maternity hospital practices were compared to women did not
experience those practices.
Table A-1. Adjusted Odds Ratios (a-OR) of Continuing Breastfeeding and Exclusive Breastfeeding for at
Least 6 Weeks among Women Who Initiated Breastfeeding
Delivery Hospital Practice
BF ≥6 Wks
a-OR*
(95% CI)
Exclusive BF ≥6 Wks
a-OR*
(95% CI)
Breastfed in the hospital 2.32
(1.89 - 2.84)
1.79
(1.44 - 2.22)
Breastfed in the first hour after delivery 1.79
(1.57 - 2.05)
1.82
(1.61 - 2.06)
Baby fed only breast milk in the hospital 3.42
(2.93 - 3.99) Not assessed**
Hospital staff gave a BF support phone number 1.31
(1.10 - 1.57)
1.22
(1.03 - 1.45)
Hospital gave information about breastfeeding 0.90
(0.68 - 1.19)
0.90
(0.70 - 1.16)
Baby stayed in mom's hospital room 1.41
(1.20 - 1.65)
1.45
(1.25 - 1.69)
Hospital helped with breastfeeding 0.85
(0.72 - 1.02)
0.87
(0.75 - 1.01)
Hospital told mother to breastfeed on demand 1.51
(1.29 - 1.77)
1.39
(1.19 - 1.62)
Hospital gave a formula gift pack 0.74
(0.64 - 0.99)
0.62
(0.53 - 0.73)
Baby given pacifier in hospital 0.62
(0.54 - 0.71)
0.60
(0.54 - 0.68)
*Final regression models adjusted for: maternal race/ethnicity, age, education, marital status, parity, and pregnancy
intention. No race/ethnicity*hospital practice interaction terms were statistically significant.
**This relationship could not be assessed because infants fed anything other than breast milk in hospital were all not
exclusively breastfed at six weeks postpartum
11
About Odds Ratios: Odds Ratios (OR) show the strength of the relationship between maternity care practices and
breastfeeding continuation and exclusivity. ORs higher than 1 indicate that a hospital practice is associated with improved
breastfeeding continuation and exclusivity; ORs lower than 1 indicate that a hospital practice is associated with reduced
breastfeeding continuation and exclusivity. An OR shown in bold indicates that the finding is statistically significant.
Eight delivery hospital practices were significantly associated with improved breastfeeding duration for WIC
participants:
• Breastfeeding in hospital
• Breastfeeding within first hour after delivery
• Feeding infant only breast milk in hospital
• Giving a breastfeeding support phone number
• Rooming-in
• Encouraging breastfeeding ‘on-demand’
• NO formula gift pack
• NO pacifier use
Seven delivery hospital practices were significantly associated with improved exclusive breastfeeding duration for
WIC participants:
• Breastfeeding in hospital
• Breastfeeding within first hour after delivery
• Giving a breastfeeding support phone number
• Rooming-in
• Encouraging breastfeeding ‘on-demand’
• NO formula gift pack
• NO pacifier use
Illinois hospitals can support breastfeeding by encouraging these practices that are shown to be effective at
improving breastfeeding continuation and exclusivity.







