
1
Hypersensitivity Pneumonitis
DR.S.H.HASHEMI

2
INTRODUCTION
HP known as extrinsic allergic alveolitis
Granulomatous, interstitial, bronchiolar and alveolar-filling lung diseases
Caused by repeated exposure and subsequent sensitization to a variety of organic and chemical antigens.

3
ETIOLOGYThree main categories:
Microbial agents Bacteria
Farmer’s lung Bagassosis Mushroom
worker’s lung Fungi
Wood pulp worker’s lung
Cheese washer lung
Ameba Humidifier lung
Animal proteinsAvian proteins
Bird breeder’s lung
Urine,Serum,Pelts Animal handler’s lung
Wheat weevil Wheat weevil lung
Chemicals Isocyanate
TDI,MDI,HDI
TMA Trimellitic
anhydride

4

5
PATHOGENESIS
Immunology: Cell-mediated immunity
Repeated inhalation of antigens → sensitization → immunology response(type III,IV) → influx of neutrophiles → shift T lymphocytes (~70%)(predominantly of CD8)(↓CD4/CD8 )
BAL → activated T lymphocytes
Lung biopsy: Interstitial mononuclear cell infiltration Granulomatous inflammatory response
Antibodies in HP are IgG class

6
PATHOGENESIS . . .
Host factors: Host susceptibility or resistance factors may
influence individual responses to inhaled antigens. Non smokers > smokers No association with HLA
Exposure factors: Ag concentration Duration of exposure Frequency & intermittency of exposure Particle size Use of respiratory protection
Farmer's lung disease: winter Bird breeder's lung: summer
7
CLINICAL FEATURES
Acute HP: Fever ,chills ,myalgia ,cough , dyspnea (4-12 h
after heavy exp. )
Ph/E : basilar rales , peripheral leukocytosis
Recurrent febrile episodes (most frequent presentation)

8
CLINICAL FEATURES . . .
Subacute and chronic HP: Temporal relationship between symptoms and
exposure is difficult to elicit.
Insidious onset of respiratory symptoms
Non-specific systemic symptoms Malaise, fatigue, weight loss, cough, dyspnea, low
grade fever
Ph/E: normal or basilar crackles & wheezing
End-stage disease: cyanosis & right-sided HF

9
L/D
↑ Specific IgG ( no sensitive , no specific ) ↑ ESR & CRP ↑ IgM , IgA, IgG ↑ ACE ↑ ANA

10
PFT
There is no single characteristic pattern of pulmonary function abnormalities .
Acute HP : restrictive pattern
Subacute and chronic HP : air way obstruction or mixed
↓ DLCO (most sensitive physiologic test in early HP )
Methacholine challenge test : increased non-specific bronchial hyper-reactivity

11
CXR
Acute HP: Diffuse ground glass opacification Fine nodular or reticulonodular pattern( lower lung
field) Consolidation ( rarely )
Subacute HP: Reticulonodular pattern
Chronic HP: Fibrosis with upper lobe retraction Reticular opacity Volume loss Honeycombing Mediastinal lymphadenopathy (up to 50%)

12
Ground glass pattern
Most common in acute HP (but may also be seen in subacute and chronic HP)
Middle lung zone PFT: restrictive , ↓DLCO May resolve with removal from exposure

13
Acute HP: pigeon breeder’s lung shows ground-glass haziness and associated air-trapping

14
Airspace consolidation
Only reported in acute HP
Bilateral ill-defined areas of consolidation

15
Subacute HP: bilateral alveolar and reticular pattern

16
Centrilobular nodules
Round, poorly defined, less than 5 mm in diameter
Typically centrilobular
Profuse throughout the lung,but a middle to lower lung zone predominance.
Most frequent HRCT finding in HP
Centrilobular nodules + ground glass opacification are highly suggestive for HP.
PFT : normal

17
Fibrosis
Chronic HP (subacute HP) Irregular linear opacities Traction bronchiectasis Honeycombing

18
Emphysema
Chronic HP Emphysema occurred more commonly than
fibrosis in chronic farmer’s lung.

19
Chronic HP: upper lobe fibrosis

20
Chronic HP: farmer’s lung disease showing bibasilar end-stage fibrosis

21
HRCT
Sensitivity of HRCT is significantly better than CXR Ground glass Centrilobular nodules Fibrosis Emphysema Mediastinal lymphadenopathy (> 20 mm )

22
Centrilobular ground-glass nodules uniformly distributed throughout the lung.Lobular air-trapping also frequently present.

23
Multiple low density ill-defined centrilobularnodules

24
Extensive areas of grand-glass attenuation.Decreased perfusion (arrows)representing associated air-trapping.
25
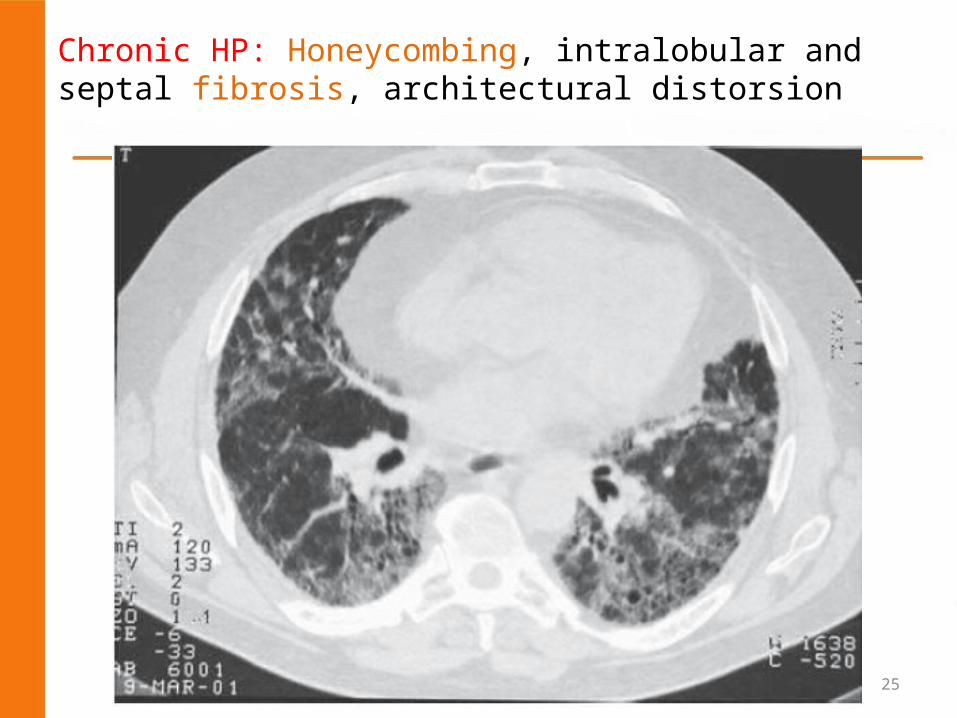
Chronic HP: Honeycombing, intralobular and septal fibrosis, architectural distorsion

26
Mosaic pattern
Patchwork of regions of differing attenuation Due to patchy areas of ground glass or
airtrapping

27
Histopathology
Classic triad: Cellular bronchiolitis Lympho-plasmocytic interstitial infiltration Non-necrotizing granulomas

28
Diagnosis
Temporal relationship between symptoms and certain activities is often the first clue to the diagnosis of HP

29
Diagnostic criteria
Required Appropriate exposure Dyspnea on exertion Inspiratory crackles Lymphocytic alveolitis
Supportive Recurrent febrile episodes Infiltration on CXR Decreased DLCO Precipitating antibodies Granulomatous on lung
biopsy Improvement with contact
avoidance

30
DDx

31
Comparison HP& Inhalation fever

32
Comparison HP& Inhalation fever . . .

33
Comparison HP& Inhalation fever . . .

34
PROGNOSIS
The clinical course of HP is variable
Acute HP generally resolves without sequelae But progressive impairment may occur with recurrent
attacks or with a single severe attack.
Subacute or chronic forms of HP present with insidious symptoms More subtle clinical abnormalities Frequently recognized later in the disease course
Long-term mortality rates for patients with chronic HP range from 1% to 10%.

35
Prognostic factors
Age Duration of exposure after onset of symptoms Time of exposure prior to diagnosis

36
TREATMENT
Cornerstone of therapy → removal from exposure
Respirators are used when removal from exposure is impossible.
Oxygen (hypoxemic patients)
Airflow limitation: Inhaled steroids β-agonists
Oral corticosteroids (40–60 mg/day of oral prednisone) in severe or progressive disease.
In refractory cases: Cyclophosphamide & Azathioprine

37


![Alveolitis Seca[1]](https://cdn.vdocuments.site/doc/165x107/55cf9d9b550346d033ae5e07/alveolitis-seca1.jpg)




